1. Introduction
The coordination between postural control and visual system is essential for successfully performing multiple tasks and achieving environmental goals [
1]. Young adults are able to control body sway to facilitate eye movements during visual search tasks [
1] and to use reliable visual information to enhance body sway control [
2]. People with Parkinson’s disease (PD) experience challenges in the control of both balance [
3] and eye movements [
4].
People with PD display larger body sway magnitude [
5,
6,
7], higher body sway acceleration and velocity, and lower complexity and adaptability [
8] in postural control function while standing upright compared to age-matched neurologically healthy controls [
9]. In addition, their limits of stability are reduced [
10] due to a disruption of the precisely coordinated execution of agonist and antagonist muscles [
11]. These postural impairments are problematic because they can lead to falls [
12], which are related to asymmetric control of posture in people with PD [
13]. The postural sway of people with PD is higher during challenging upright postural tasks, such as tandem position [
14,
15]. Poor postural control performance in people with PD is not surprising, considering the many changes in sensory systems [
16].
It is known that individuals with PD particularly rely on visual information to compensate for deficits in postural sway control [
17]. However, eye movement abnormalities in people with PD are extensively discussed in the literature, including a decreased range of eye movements and prolonged saccadic latency [
4,
18]. In addition, this population shows hypometria during the execution of voluntary saccades (remembered, predictive, and antisaccades) [
19] and impairment of antisaccade latencies, which is an indirect marker of impaired anticipatory postural adjustments [
20]. The deficits in voluntary saccade movements in PD are attributed to pathological involvement at the brainstem and basal ganglia levels [
20]. While the basal ganglia mediate saccade amplitude and latency [
18], the cerebellum is involved in saccade accuracy [
21]. However, it is not clear yet whether and how aspects of saccade and postural control are conjointly impaired in PD. A better understanding of how eye movements and postural sway are linked in PD should help to develop more effective strategies to minimize balance impairments in this population.
In both young adults [
22,
23] and healthy older adults [
24,
25], it has been shown that body sway is reduced when performing saccadic eye movements. This reduction in postural sway allows the brain to shift gaze accurately, indicating a functional connection between posture and gaze control [
1]. However, the impact of saccadic eye movements on body sway depends on the direction of the saccadic eye movements (horizontal vs. vertical) and the level of difficulty of the standing posture in both young and older adults. Vertical saccadic eye movements are more challenging for the eye movement system than horizontal saccade ones, leading to a delayed gaze response [
26]. Greater postural instability seems to impair eye movements in the vertical direction, particularly in older adults [
25]. When exposed to a challenging standing position (e.g., tandem stance), older adults exhibited greater variability in gaze during vertical saccadic eye movements, which is associated with larger head movements compared to young adults [
25]. Furthermore, older adults experience an increase in the effects of saccadic eye movements on body sway when performing a more challenging postural task, adopting a more rigid postural control strategy [
24].
This stabilization of postural control could be attributed to both afferent and efferent mechanisms for eye movements. In fact, the afferent motion perception mechanism occurs when the central nervous system uses optic flow information to minimize retinal slip and stabilize the distance between the eye and the visual scene; while the efferent motion perception mechanism occurs when the central nervous system uses the copy of motor commands (i.e., “efference copy”) or extraocular muscle afferents that follow eye movements to stabilize posture [
2]. Another explanation for the reduction in body sway during saccadic eye movements in healthy adults may be associated with the achievement of a goal in a supra-postural task [
27]. This type of activity includes tasks or behavioral goals that are subordinated to the control of posture [
27]. In this case, postural coordination and supra-postural performance have a hierarchical relationship, where posture coordination serves as a means to succeed in supra-postural tasks. The main viewpoint is that the neurologically healthy individual improves postural stability to facilitate, at least in part, the performance of this type of task [
28]. Both explanations consider additional resources available, such as sensory cues, attentional efforts, and cognitive engagement, as essential for decreasing postural sway and favoring the spatial accuracy of the saccade in terms of target location [
23,
29].
Considering that postural sway is decreased in performing saccadic eye movements in healthy young and older adults, testing the impact of such saccadic eye movements is important in people with PD who often experience larger body sway, especially in challenging stances (i.e., semi-tandem position) [
14,
15], and deficits in voluntary saccade movements [
4,
18], which increase the risk of falls [
12]. In this study, we investigated the effects of horizontal and vertical saccadic eye movements on body sway in people with PD (under dopaminergic medication) and neurologically healthy individuals (control group) during quiet stance tasks in two bases of support positions (side-by-side and tandem stances).
We hypothesized that (i) the brain would decrease body sway to perform horizontal saccadic eye movement compared to the eye fixation condition in neurologically healthy individuals, with a greater reduction during tandem stance than side-by-side stance [
24], but we did not expect changes in body sway in people with PD during horizontal saccadic eye movement due to their postural [
14,
15] and visual deficits [
4,
18]; (ii) the brain would not reduce body sway during vertical saccadic eye movement compared to the eye fixation condition in both neurologically healthy individuals and people with PD because of the weaker functional connection between posture and gaze control in this scenario [
25]; (iii) people with PD would show poorer gaze performance, with an increased number of fixations and decreased mean duration of fixations during both horizontal and vertical saccadic eye movements compared to neurologically healthy individuals, with a greater impact during tandem stance than side-by-side stance; and iv) both groups would show worse gaze performance during vertical saccadic eye movements compared to horizontal saccadic eye movements, considering that the first type of eye movement is more challenging for the eye movement system [
26].
2. Materials and Methods
2.1. Participants
Ten individuals diagnosed with PD (PD group) (8 men/2 women) and 11 neurologically healthy individuals (7 men/4 women) participated in this study. The number of participants was determined using a power analysis that used an alpha level of 0.05, effect size of 0.93 and a power of 90% (G-power
®). The analysis was based on the mean velocity of the center of pressure (CoP) from Polastri and colleagues’ study [
25], which determined that a minimum of nine participants in each group was needed for the study.
All participants included in this study were over the age of 60 and were able to stand independently during the postural task. The PD group included only those who had received a confirmed diagnosis of idiopathic PD from a specialist according to the criteria of the UK Parkinson’s Disease Brain Bank Field [
30], classified between stages 1 and 3 on the Hoehn and Yahr (H&Y) scale [
31] and treated with dopaminergic medication. Participants with cognitive deficits (defined as a score below 24 on the Mini-Mental State Examination [
32]) (for both groups), rheumatic or orthopedic diseases that impaired the performance of the postural task (for both groups), or any neurological diseases (for the control group) or other neurological diseases (for the PD group) were excluded from the study. To ensure consistent visual acuity among participants, we conducted the Snellen test and only selected individuals with visual acuity scores between 20/20 and 20/30 to participate in the study. Five individuals with PD and three neurological healthy individuals did not meet the inclusion/exclusion criteria and were therefore excluded from the study.
All participants signed an informed consent form and heard a thorough explanation of the research procedures before signing the document. The study received approval from the University Ethics and Research Committee (#11322/46/01/12).
2.2. Clinical Evaluation
A specialist in movement disorders conducted a cognitive evaluation of both the control group and the PD group. The control group was evaluated using the Mini-Mental State Examination and an anamnesis. The PD group was evaluated using a procedure similar to that for the control group, in addition to the H&Y scale and the Unified Parkinson’s Disease Rating Scale—UPDRS-III [
33]. The PD group was assessed under dopaminergic medication (“ON” state) [
34].
2.3. Postural Task and Eye Movements
During the experiment, each participant was asked to stand barefoot on a force plate (AMTI-AccuGait). An LCD monitor (37.5 cm × 30 cm, LG, Faltron L1952H, 50/60 Hz, 0.8 A) was placed at eye level, and a red dot with a 2 cm diameter was displayed on the monitor, which was 1 m away from the participant’s eyes. The target was presented on a white background, and its subtended visual angle was 1.15° (relative to looking straight ahead). The stimulus was generated using Flash Mx 7.2 software (Macromedia, Portland, OR, USA).
The participants completed the trials of the two postural tasks in a sequential order, and the three visual conditions in a randomized order. The protocol for each postural task consisted of one block of six trials, making a total of 12 trials. After every three trials, the participant was given a one-minute rest period to avoid fatigue or tiredness that could potentially deteriorate their performance. Each trial lasted 70 s.
The participants performed two types of postural tasks under eye movement conditions: (1) to stand with the feet in a side-by-side stance, with the feet parallel and aligned with the shoulders; (2) to stand with the feet in a tandem stance, with the least affected or dominant foot aligned in front of the most affected or non-dominant foot (
Figure 1d,e). The three visual tasks were (a) fixation, where the participant fixed their gaze on a single target displayed at the center of the screen (
Figure 1b); (b) horizontal saccadic eye movements to the right and left, with the subject tracking the targets in those directions on the screen (
Figure 1a); (c) vertical saccadic eye movements up and down, with the individual keeping their eye on the target positioned above or below the screen (
Figure 1c). During horizontal and vertical saccadic eye movements, (i) the angle between targets was 11° to avoid head movements, and (ii) the target appeared first on the left side of the monitor, 9.75 cm away from the center, and then disappeared and reappeared immediately on the opposite side (i.e., the right side), also 9.75 cm away from the center.
To determine the lower-limb preference of the control group, the participants were asked to kick a ball. The limb used to kick the ball was considered the preferred limb [
35]. For the people with PD, the most affected limb was determined using items 20–23 and 25–26 of UPDRS-III. The value of the right limb was subtracted from the value of the left limb in each item. If the result of this calculation was positive or negative, the most affected limb was the right or left limb, respectively [
35].
2.4. Data Analysis
The force plate measures the forces (Fx, Fy and Fz) and moment components (Mx, My and Mz) to calculate the displacement of the CoP in the anterior–posterior (AP) and medial–lateral (ML) axes. The CoP displacement was filtered using a second low-pass Butterworth filter with a 5 Hz cutoff frequency and a fourth-order zero-lag. A head-mounted eye tracking system (model H6, Applied Science Laboratory, Billerica, MA, USA) was used to measure eye movements with a precision of 1° of visual angle. The system calibration was performed from the fixation of nine points displayed in a 3 by 3 grid and checked in each trial. The sampling frequency was 60 Hz. Although each trial lasted 70 s, the first 10 s were not considered in the analyses.
The following CoP variables were calculated for both AP and ML directions: displacement of sway—the total path length of the CoP along the support base in each direction; mean velocity of sway—the division of the total sway in each direction by the duration of the trial; and root mean square (RMS)—the mean variability of the displacement along the trial. In addition, the area was calculated as 95% of the ellipse area that the CoP covered. To analyze the data from the force platform, a group of specific programs written in MATLAB R_2022a (MathWorks, Inc®, Natick, MA, USA) was used.
Eye movement analysis was conducted using Applied Sciences Laboratories Results Plus software® (Billerica, MA, USA) and MATLAB (MathWorks, Inc®). The following gaze parameters were calculated for both conditions: number of fixations (the total number of fixations during the trials), and mean duration of fixations (the average of all fixation durations in each trial). To calculate these gaze parameters, an eye fixation occurred when the value of two times point of gaze standard deviation was less than one degree of visual angle in the horizontal axis and one degree of visual angle in the vertical axis over 100 ms.
2.5. Statistical Analysis
CoP and gaze variables were pre-tested with the Shapiro–Wilk test to verify the normality of the data and with Levene’s test to verify the equality of variance. Independent t-tests were performed to compare anthropometric and cognitive status between the PD group and the control group. Three-way ANOVAs were conducted to test differences between groups, and within-group conditions, for each CoP- and gaze-dependent variable. The study examined the effects of groups (PD vs. control), visual tasks (fixation, horizontal, and vertical saccadic eye movements) and base of support (side-by-side vs. tandem). The last two factors were measured repeatedly. When the ANOVA showed significant differences between variables, post hoc tests with Bonferroni adjustments were performed. For gaze-dependent variables, visual tasks had only two levels (horizontal and vertical saccadic eye movements). The effect size (η
2, partial eta-squared) was also calculated for each statistical analysis and was interpreted as a small effect if it was <0.06, moderate if it was within >0.06 and <0.14, and large if it was >0.14 [
36]. The significance level was
p < 0.05 (SPSS, version 26.0).
3. Results
Table 1 depicts the anthropometric and clinical status of the PD group and control group. There were no significant differences in age, body mass, height and cognitive status between the two groups (all
p > 0.05).
3.1. CoP Parameters
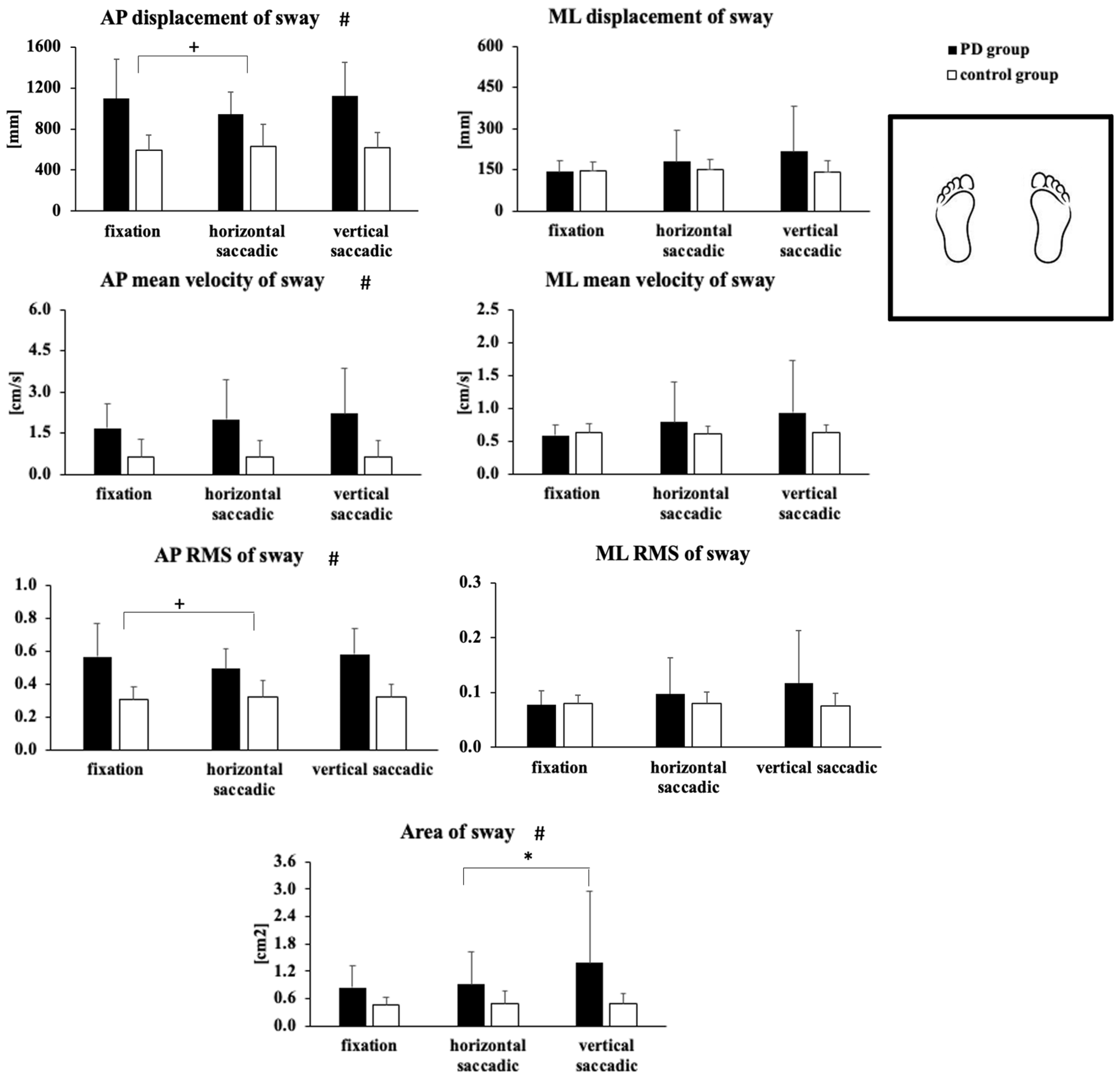
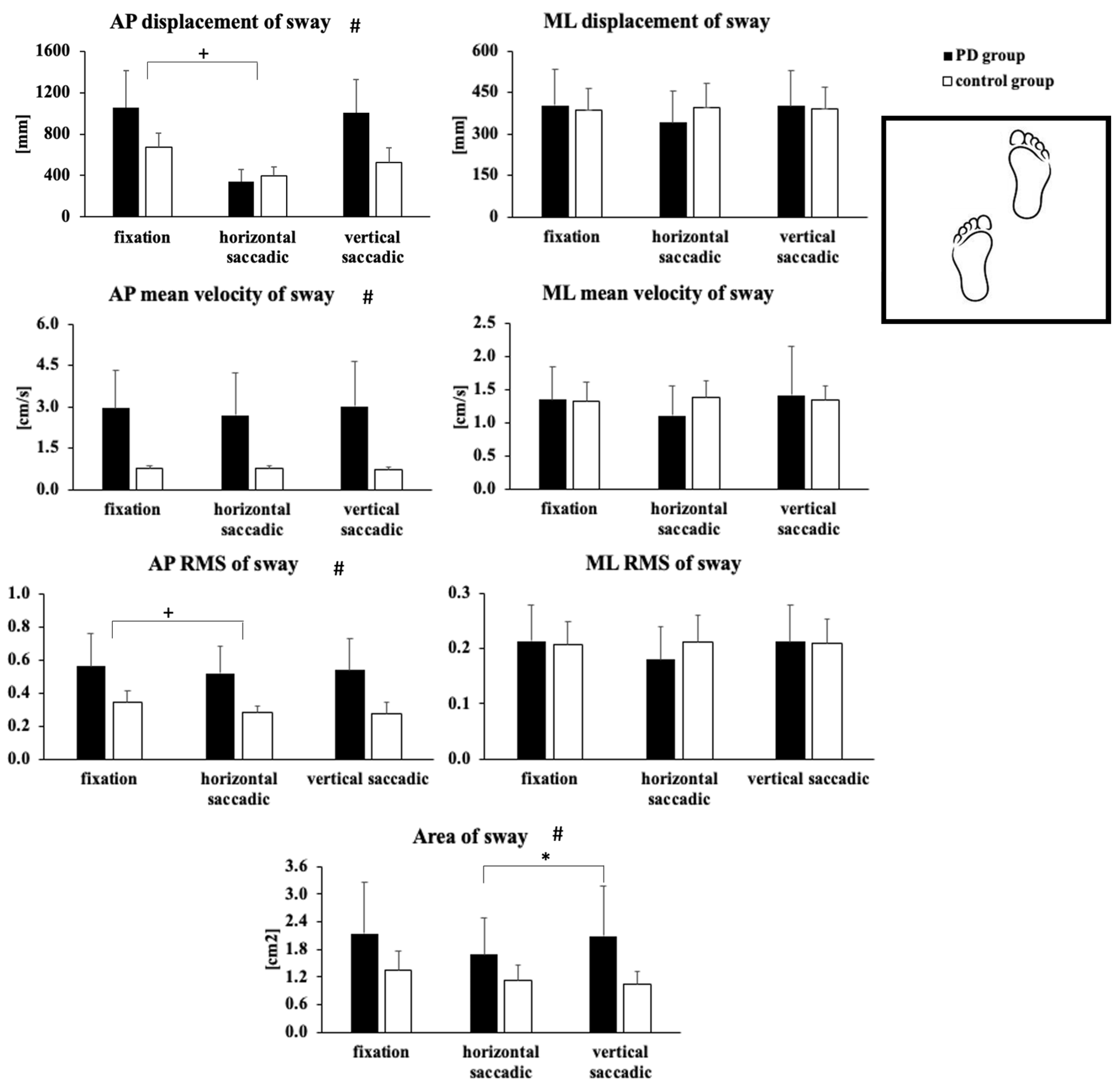
Figure 2 and
Figure 3 depict the CoP variables for side-by-side and tandem support positions during fixation and eye movements in horizontal and vertical directions. ANOVAs did not reveal a significant three-factor interaction for the group and base of support and visual task (
p > 0.05).
ANOVAs indicated a significant group effect for AP displacement (F1,18 = 24.23, p < 0.001, η2 = 0.57), mean velocity of sway (F1,18 = 18.39, p < 0.001, η2 = 0.50) and RMS (F1,18 = 24.96, p < 0.001, η2 = 0.58), and area of sway (F1,18 = 9.80, p < 0.006, η2 = 0.35). The PD group showed higher levels of AP displacement, mean velocity of sway and RMS, and area of sway compared to the control group.
ANOVAs indicated a significant visual task effect for AP displacement (F1,18 = 6.29, p < 0.005, η2 = 0.25) and RMS (F1,18 = 6.76, p < 0.004, η2 = 0.24). During the horizontal saccadic movements, the participants in both groups reduced AP displacement and RMS compared to the fixation condition.
ANOVAs also indicated a significant base of support effect for ML displacement (F1,18 = 64.49, p < 0.001, η2 = 0.78), mean velocity of sway (F1,18 = 47.61, p < 0.001, η2 = 0.72) and RMS (F1,18 = 61.21, p < 0.001, η2 = 0.77), AP mean velocity of sway (F1,18 = 17.13, p < 0.01, η2 = 0.48), and area of sway (F1,18 = 18.30, p < 0.001, η2 = 0.50). In both groups, the tandem stance resulted in higher levels of ML displacement and RMS, AP and ML mean velocity of sway, and area of sway than the side-by-side stance.
A group by base of support interaction was indicated in ANOVAs for AP mean velocity of sway (F1,18 = 9.21, p < 0.007, η2 = 0.33). The PD group showed greater AP mean velocity of sway during the tandem stance compared to the side-by-side stance (p < 0.001), which was not found for the control group.
A group by visual task interaction was indicated in ANOVAs for the area of sway (F2,36 = 3.59, p < 0.04, η2 = 0.16). Only for the PD group, the area of sway was higher when performing vertical saccadic eye movements compared to horizontal saccadic eye movements (p < 0.005), but there was no significant difference in comparison to fixation condition (p = 0.124).
3.2. Gaze Parameters
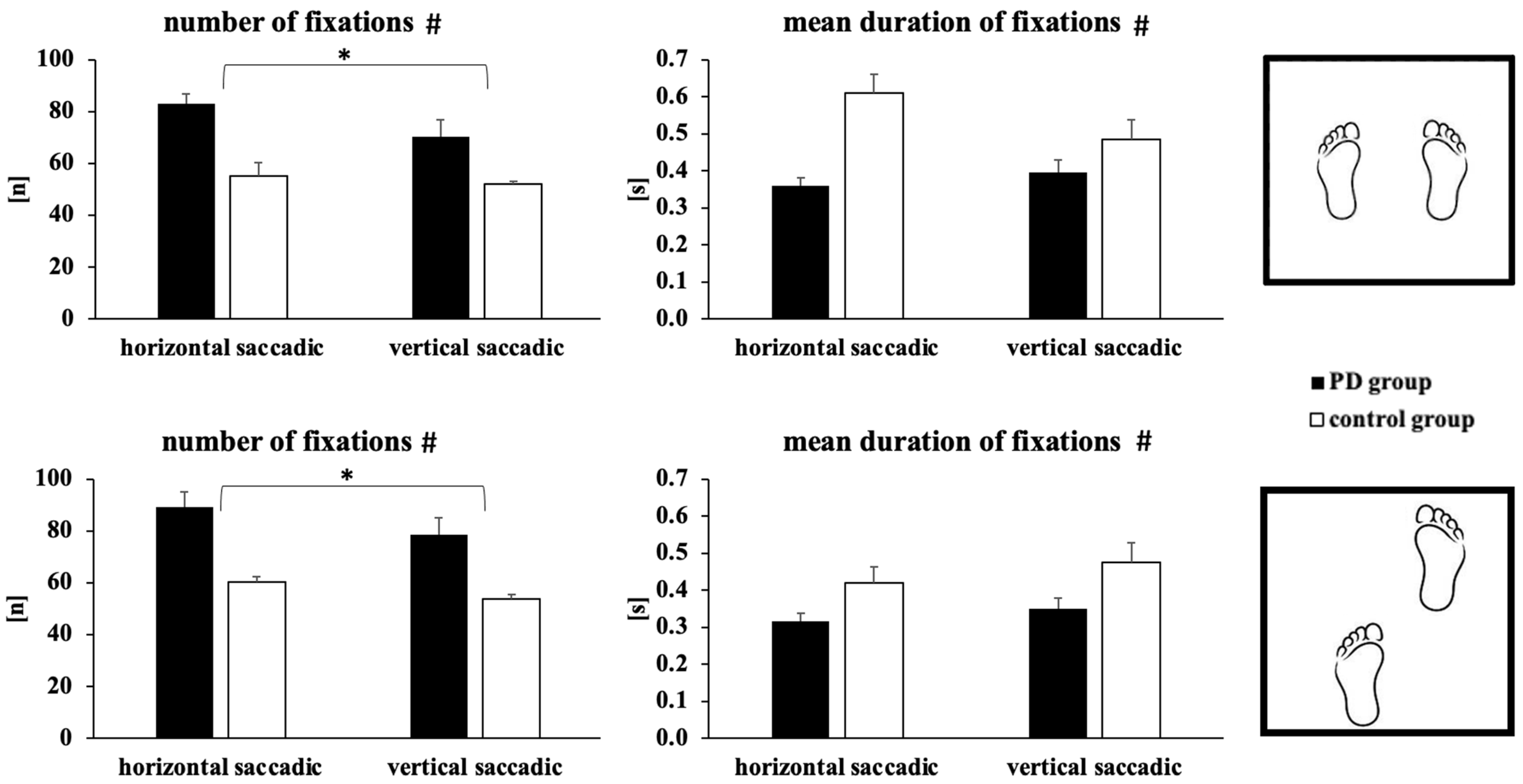
Figure 4 shows the gaze parameters for side-by-side and tandem stances during saccadic eye movements in horizontal and vertical directions. ANOVA did not reveal a significant interaction for (i) group and base of support, (ii) group and visual task, (iii) base of support and visual task, and (iv) group and base of support and visual task (
p > 0.05).
ANOVAs indicated a significant group effect for the number of fixations (F1,17 = 24.60, p < 0.001, η2 = 0.59) and mean duration of fixations (F1,18 = 5.19, p < 0.03, η2 = 0.23). In all tasks, the PD group exhibited a higher number of fixations and shorter mean duration of fixations compared to the control group.
ANOVAs indicated a significant visual task effect for the number of fixations (F1,17 = 4.37, p < 0.05, η2 = 0.21). The participants in both groups exhibited a lower number of fixations in the vertical saccadic eye movements compared to horizontal saccadic conditions.
ANOVAs also indicated a significant base of support effect for the number of fixations (F1,17 = 6.02, p < 0.02, η2 = 0.26). For both groups, the tandem stance resulted in a higher number of fixations than the side-by-side stance.
4. Discussion
We conducted a study to test whether people with PD are able to reduce their body sway when performing horizontal and vertical saccadic eye movements while standing with feet in a side-by-side or tandem stance. Our findings partially supported our first hypothesis, showing a reduction in body sway for both groups when performing horizontal saccadic eye movement compared to the eye fixation condition (we expected reduction only for neurologically healthy individuals). However, we did not find significant effects of the base of support on body sway during horizontal saccadic eye movements as we proposed in the first hypothesis. In addition, our second, third, and fourth hypotheses were fully supported by our findings: vertical saccadic eye movements did not reduce body sway for both people with PD and neurologically healthy individuals, gaze performance was poorer in people with PD compared to neurologically healthy individuals, especially during tandem stance, and vertical saccadic eye movements led to poorer gaze performance compared to horizontal saccadic eye movements, respectively. It is important to note that all significant effects had a large effect size, indicating that eye movements had a noteworthy impact on postural stability.
During horizontal saccadic eye movements, people with PD were able to reduce body sway during both side-by-side and tandem postural tasks by coupling eye movements and postural sway (
Figure 2 and
Figure 3). This finding was unexpected and invalidated our main hypothesis. A posteriori, the literature also showed that neurologically affected populations are able to reduce their sway to perform gaze shift tasks as well as older healthy and younger populations [
22,
23,
24]. The afferent and efferent mechanisms of visual stabilization of posture can explain these results [
2]. On the one hand, the afferent mechanism involves minimizing changes in the projected image on the retina to maintain a relationship between visual information and body posture during fixation [
23,
29]. On the other hand, the efferent mechanism, particularly efference copy, attenuates body sway in an attempt to connect pre-saccadic and post-saccadic views of the scene, thus enhancing the spatial accuracy of the saccade concerning the target location [
23,
29]. Since the eye saccade condition requires greater postural stability to allow spatially more accurate gaze shifts, there seems to be a functional integration of postural and gaze control [
1]. Also, similarly to neurologically healthy individuals, the achievement of a goal in a supra-postural task may explain the reduction in body sway during saccadic eye movements [
27]. Therefore, there is an improvement in postural stability to facilitate, at least in part, the performance of this type of task [
28].
One possible reason for the similar findings in people with PD, under dopaminergic medication, and healthy controls in our study (or other populations in other studies) could be related to subcortical control of posture. During horizontal saccadic eye movements, it is believed that the control of posture shifts to a more subcortical level [
27]. It means that the brain uses the brainstem/cerebellum to control the body/head position, while other lower structures take control of eye movements. This hypothesis puts postural control on a “second goal”, making it more “automatic” and reducing body sway during horizontal saccadic eye movement. Consistent with this argument, Bonnet et al. [
37], Cruz et al. [
7], and Feller et al. [
38] showed that PD may not affect a person’s ability to control their posture automatically in simple environments (e.g., when looking at a blank target). It means that people with PD are able to control their posture as well as healthy people in quiet stance. Furthermore, and based on our results, PD individuals are also able to improve their postural control, and thus show functional gaze and posture connection when performing horizontal saccadic eye movements. In other words, performing horizontal saccadic eye movements might be a useful strategy to help the central nervous system in people with PD to counter impairments in basal ganglia related to both gaze shift and postural control.
As expected, vertical saccadic eye movements did not reduce body sway and worsened gaze performance in both groups in comparison to the control fixation task. Therefore, people with PD did not show any functional coupling between gaze and posture but also did not show any impairment when performing vertical saccadic eye movements. As complementary information, vertical saccadic eye movements increased the area of sway in people with PD but only when contrasting the horizontal and vertical saccadic eye movements. Hence, this finding only shows that the coupling between gaze shift and postural control is significantly better when performing horizontal saccadic eye movements than vertical saccadic eye movements and not that there is a PD-related impairment in vertical saccadic eye movements (as again, there was no significant difference between body sway in vertical saccadic eye movements and fixation). We can provide some reasons to explain why the coupling between gaze shift and postural control was not functional when performing vertical saccadic eye movements.
Firstly, we need to acknowledge that the control of horizontal and vertical eye saccadic movements is distinct. In fact, on one hand, the cortical areas mainly involved in horizontal saccade generation are the contralateral parietal and frontal eye fields [
26]. On the other hand, the circuits required to execute vertical saccades involve a higher level of activation in the right frontal eye field, cerebellar posterior lobe, and superior temporal gyrus [
4]. Secondly, vertical eye movements are more variable compared to horizontal eye movements [
25]. Our results seem to confirm that gaze performance is poorest during vertical eye movements. We found a lower number of fixations during vertical saccadic eye movements compared to horizontal saccadic conditions for both groups. However, we did not assess the variability of eye movements to fully confirm the existing literature. Thirdly, the direction of vertical gaze movement could have promoted slight up/down head rotations, which would have increased sway because the head is a heavy segment. Even if head rotations had been similar in left/right and up/down directions, they have clearly different effects on postural sway [
39]. In fact, on one hand, in left/right head rotations, the head center of mass stays in line with the body center of mass, thus not creating any couple of rotations and ultimately not increasing postural sway. On the other hand, in up/down head rotations, the head center of mass is not aligned with the body center of mass anymore [
39], thus creating couples of rotations that increase postural sway. Unfortunately, we cannot verify this a posteriori hypothesis, as we did not record head rotation. We can only suggest, from the results, that both groups were able to significantly reduce their sway when performing horizontal saccades but not vertical saccades. One relevant finding, though, is that due to the specificity of 90% in discriminating PD and healthy individuals, vertical saccades could be a biomarker for early diagnosis of PD [
26] and postural impairments.
Our results validated the hypothesis that people with PD would have a worse gaze performance than neurologically healthy individuals. In fact, they revealed that people with PD used a higher number of fixations in all visual tasks in both postural tasks compared to healthy individuals, which could be an indication of reduced goal-directed control [
40]. This suggests that people with PD have difficulty maintaining their visual attention and may shift their gaze toward irrelevant information, which could increase the number of fixations in the visual scene. This behavior can be dangerous, as shown by Gotardi et al. [
41], who found that people with PD had an increased number of collisions while driving due to an overall increase in gaze fixations and a shift in visual attention toward task-irrelevant information. People with PD tend to have difficulties in processing temporal information, leading to deficits in temporal judgment [
42]. According to Cruz et al. [
43], individuals with PD exhibit delayed body sway to visual stimuli during continuous and predictable driving frequency compared to the control group, indicating some disruption in the visual–motor coupling. The pedunculopontine nucleus area, which is responsible for both saccades and posture functions, may explain some of the dysfunction seen in PD patients [
20].
Although novel findings were presented above, some limitations of our study need to be discussed. First, the sample size was small but still fitted with the required minimum sample size. Additionally, all significant differences exhibited large effect sizes, which confirms that the number of participants in the study was adequate. A second limitation is that we refrained from the inclusion of patients in H&Y 4 and 5. So, our findings can be valid only for initial and moderate levels of PD. An extension of the study population to the late stages of PD would be relevant in future studies.


 ,
, 

{kind=link}
{kind=link}
{kind=link}
{kind=link}