
Ballroom Dance as a Form of Rehabilitation: A Systematic Review


Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Flow of Studies through The Review Process
3.2. Characteristics of the Studies

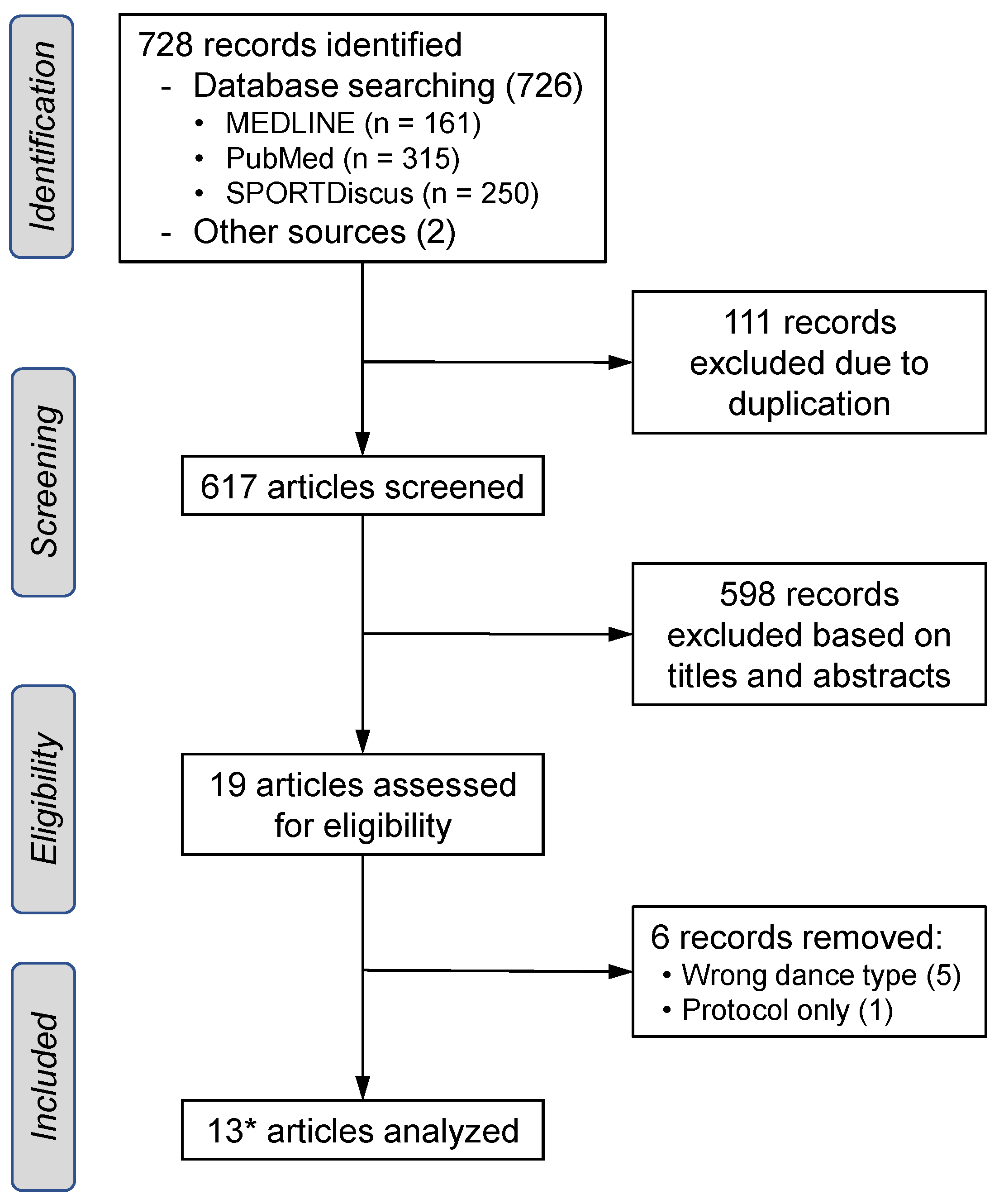{kind=link}
| Study | Study Design | Disease/Disorder | Participants (n; Age (SD)) | Type of Dance | Frequency of Intervention | Intensity |
|---|---|---|---|---|---|---|
| Blandy et al, 2015 [28] | Single-group pre-post test | PD | 6 people with PD (3 male), age: 64 (6.28) | Argentine Tango | 1 hour, twice per week, for 4 weeks | Not reported |
| Hackney & Earhart, 2010 [16] | Randomized, pre-post without control | PD | 39 people with PD—15 partner (13 male), age: 69.6 (8.5); 16 non-partner (15 male), age: 69.6 (9.5) | Partnered and non-partnered Argentine tango | 1 hour, twice per week, for 10 weeks | Not reported |
| Hackney et al, 2012 [30] | Case Study | Stroke | 73-year-old male | Tango | 20 sets of 1.5-hour dance class over 12 weeks | Not reported |
| Hulbert et al, 2017 [27] | Randomized controlled | PD | 27 people with PD: intervention (15)—7 male, age: 73.4 (4.9); control (12)—5 male, age: 71.7 (5.1) | Fox trot, Waltz, Tango, Rumba, Cha Cha, Rock-n-roll, Social dance | 1 hour, twice per week, for 10 weeks | Not reported |
| Kunkel et al, 2017 [15,26] * | Randomized controlled trial | PD | 51 people with PD: intervention (36)—19 male, age: 71 (7.7); control (15)—6 male, age: 69.7 (6) | Fox trot, Waltz, Tango, Cha Cha, Rock-n-roll, and Rumba | 1 hour, twice a week, for 10 weeks | Not reported |
| Lazarou et al, 2017 [13] | Single-blinded randomized controlled, pre-post trial | Dementia | Intervention Group—66 (13 male), age: 65.9 (10.8); Control Group—63 (15 male), age: 67.9 (9.5) | Tango, Waltz, Viennese Waltz, Fox Trot, Rumba, Cha Cha, Swing, Salsa, Merengue, Hustle | 60 minutes, twice per week for 40 weeks | Not reported |
| Mandelbaum et al, 2016 [12] | Pre-post study with no control | MS | 8 people with MS (3 male), aged 32 to 63 | Salsa | 60 minutes, twice per week for 4 weeks | Moderate |
| Mangeri et al, 2014 [7] | Longitudinal | Diabetes | 100 people—47 with type 2 diabetes, 53 with obesity (52 male), age: 59 | Latin and Standard Ballroom | 2 hours, twice per week for 6 months | 4–7 METs (depending on dance type) |
| Masters et al, 2013 [29] | Uncontrolled pilot study | Spinal Cord | 7 paraplegia and 8 tetraplegia individuals | Salsa, Tango, Rumba | 4 hours a week for 6 weeks | Not reported |
| Ng et al, 2019 [11] | Pre-post study with control | MS | 13 people with MS—7 intervention, age: 49; 6 control, age: 55 | Rumba, Fox trot, Waltz, and Push-pull | 1 hour, twice per week for 8 weeks | Not reported |
| Pisu et al, 2017 [8] | Pre-post study with control | Cancer | 31 couples: cancer survivors—age: 57.9 (9.3); partners—age: 60.7 (9.9) | Foxrot, Waltz, Cha Cha, and East Coast Swing | 45 minutes, 10 private and 2 group lessons over 12 weeks | 5 METs/hr |
| Schmidt et al, 2018 [31] | Unspecified | Cancer | 11 couples—Age: 6 were 56–65 years, 6 were 66–75 years, and 1 was over 75 | Ballroom-unspecified | 90 minutes, offered once a week for 8 months | Varied |
| Study | Dropouts | Adverse Events | Outcome Measures | Findings |
|---|---|---|---|---|
| Blandy et al., 2015 [28] | 89% adherence, and 1 dropout | None | Safety, adherence, overall health, and depression scores | Health and depression scores improved, and intervention was deemed safe with high adherence |
| Hackney & Earhart, 2010 [16] | 20% withdrew (4 from each condition) | None reported | BBS, tandem stance, one-leg stance, TUG, 6MWT, comfortable and fast walking examined gait velocity, cadence, stride length, swing %, and double support %, program experience | Improved BBS, comfortable and fast walking velocity, one-leg and tandem stance time, cadence, double support %, fast walking swing %, stride length, 6MWT, and reported physical well-being |
| Hackney et al., 2012 [30] | NA | None reported | 30 s chair stand, walking speed and variability, step length variability, and single support time during habitual, backward, and fast walking, 6MWT, BBS, FRT, TUG, TUGc, balance confidence, physical, mental and visual QOL, and depression using self-report questionnaires | Improved chair stand, BBS, FRT, TUGc, TUG, and 6MWT, decreased balance confidence, unchanged mental health and visual QOL, reported feeling improved walking, coordination, strength, endurance, and mood. |
| Hulbert et al., 2017 [27] | 3 dance participants dropped out | 1 adverse event (leg pain) was linked to the participant’s condition, and 1 participant fell in class with no injury | SS180 | Controls had longer latencies between segments, and increased rotation. Dancers showed shorter latency between segments, decreased rotation throughout the body segments, and increased weight transfer |
| Kunkel et al., 2017 [15,26] | 5 dance participants dropped out | None reported | BBS, Spinal Posture, SS180, TUG, PDQ39, ABC, Phone-FITT, Euroqual-5D, 6MWT | Improved 6MWT, TUG, and SS180. Study demonstrated feasibility |
| Lazarou et al., 2017 [13] | 3 (due to family problems) | None reported | Neuropsychological battery of tests to evaluate attention, working memory, memory, executive functioning, and language—MMSE, RBMT, FAS, NPI, GDS, BDI, Hamilton Scale for Depression, PSS, Beck Anxiety Inventory, FRSSD, FUCAS, TRAIL-B, ROCFT, RAVLT, and TEA | Improved MMSE, MOCA, TEA, NPI, RAVLT, FAS, RBMT1, RBMT2, ROCFT, and GDS in the dance group. No improvements in the control group. |
| Mandelbaum et al., 2016 [12] | 1 participant completed 7 of 8 dance sessions due to scheduling | None | T25FW, MSWS-12, TUG, DGI, BBS, MSSS, ABC, MPAM-R, PDDS, GLTEQ, MS symptom checklist | Improved TUG, MSWS-12, DGI, MS symptom checklist, and time spent exercising |
| Mangeri et al., 2014 [7] | 2% dropped out, 77% attended over 70% of the planned sessions | None reported | MET-hours/week, anthropometric data, weight, waist circumference, 6MWT, EMME-3 | Both groups decreased body weight, waist circumference, fasting glucose, and liver enzymes. Both groups improved 6MWT and MET-hours/wk. |
| Masters et al., 2013 [29] | Not reported | None reported | Weight, subjective pain at rest, isometric strength, upper body ROM, reaction time, wheelchair agility, 6-min distance, and coordination | Improved upper extremity and trunk ROM, upper body strength, 6-min distance, coordination, and decreased weight, resting pain, and reaction time |
| Ng et al., 2019 [11] | 0 | None reported | PROMIS-GH, FIS, BDI, MSSS, T25FW, 9-HPT, PASAT, BBS, DGI | Improved PROMIS-GH, FIS, BDI, BBS, MS Functional Composite Score, and PASAT in the dance group. Control group showed no changes. |
| Pisu et al., 2017 [8] | 20% | None reported | GLTEQ, 6MWT, SF-36, Dyadic Trust Scale, DAS-7, perceived self-disclosure questionnaire | Intervention group showed improved physical activity, functional capacity, QOL, vitality, social functioning, and mental health and dyadic trust. Control group improved body pain and functional capacity |
| Schmidt et al., 2018 [31] | Not reported | None | Daily reports of well-being | Well-being increased during class and returned to starting level during the next 6 days |
3.3. Study Specifics
3.3.1. Parkinson’s Disease
3.3.2. Multiple Sclerosis
3.3.3. Spinal Cord Injury
3.3.4. Stroke
3.3.5. Dementia
3.3.6. Cancer
3.3.7. Diabetes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carr, J.; Shepherd, R. Neurological Rehabilitation: Optimizing Motor Performance, 2nd ed.; Churchill Livingstone Elsevier: Amsterdam, The Netherlands, 2010. [Google Scholar]
- Batista, P.; Pereira, A. Quality of life in patient with neurodegenerative diseases. J. Neurol. Neurosci. 2016, 77, 1–7. [Google Scholar] [CrossRef]
- Farrell, J.; Merkas, J.; Pilutti, L. The effect of exercise training on gait, balance, and physical fitness asymmetries in persons with chronic neurological conditions: A systematic review of randomized controlled trials. J. Front. Physiol. 2020, 12, 1316. [Google Scholar]
- Rahal, M.; Alonso, A.; Andrusaitis, F.; Silva Rodrigues, T.; Souza Speciali, D.; D’Andrea Greve, J.; Eugenio Garcez Leme, L. Analysis of static and dynamic balance in healthy elderly practioners of Tai Chi Chuan versus ballroom dancing. Clinics 2015, 70, 157–161. [Google Scholar] [CrossRef]
- Merom, D.; Cumming, R.; Mathieu, E.; Anstey, K.; Rissel, C.; Simpson, J.; Morton, R.; Cerin, E.; Sherrington, C.; Lord, S. Can social dancing prevent falls in older adults? a protocol of the Dance, Aging, Cognition, Economics (DAnCE) fall prevention randomized controlled trial. BMC Public Health 2013, 13, 477. [Google Scholar] [CrossRef] [PubMed]
- Licher, S.; Darweesh, S.; Wolters, F.; Fani, L.; Heshmatollah, A.; Mutlu, U.; Koudstaal, P.; Heeringa, J.; Leening, M.; Ikram, M.; et al. Lifetime risk of common neurological diseases in the elderly population. J. Neurol. Neurosci. Psychiatry 2019, 90, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Mangeri, F.; Montesi, L.; Forlani, G.; Grave, R.; Marchesini, G. A standard ballroom and Latin dance program to improve fitness and adherence to physical activity in individuals with type 2 diabetes and in obesity. Diabetol. Metab. Syndr. 2014, 6, 74. [Google Scholar] [CrossRef] [PubMed]
- Pisu, M.; Demark-Wahnefried, W.; Kenzik, K.; Oster, R.; Lin, C.; Manne, S.; Alvarez, R.; Martin, M. A dance intervention for cancer survivors and their partners (RHYTHM). J. Cancer Surviv. 2017, 11, 350–359. [Google Scholar] [CrossRef]
- Chien-Hung, L.; Hung-Chou, C.; Tsan-Hon, L.; Wei, L.; Shih-Ching, C. Exercise interventions for individuals with neurological disorders: A systematic review of systematic reviews. Am. J. Phys. Med. Rehabil. 2019, 98, 921–930. [Google Scholar]
- Yang, F. Application of vibration training in people with common neurological disorders. In Manual of Vibration Exercise and Vibration Therapy; Rittweger, J., Ed.; Springer: Cham, Switzerland, 2020. [Google Scholar]
- Ng, A.; Bunyan, S.; Suh, J.; Huenink, P.; Gregory, T.; Gambon, S.; Miller, D. Ballroom dance for persons with multiple sclerosis: A pilot feasibility study. Disabil. Rehabil. 2019, 42, 1115–1121. [Google Scholar] [CrossRef]
- Mandelbaum, R.; Triche, E.; Fasoli, S.; Lo, A. A pilot study: Examining the effects and tolerability of structured dance intervention for individuals with multiple sclerosis. Disabil. Rehabil. 2016, 38, 218–222. [Google Scholar] [CrossRef]
- Lazarou, I.; Parastatidis, T.; Tsolaki, A.; Gkioka, M.; Karakostas, A.; Douka, S.; Tsolaki, M. International ballroom dancing against neurodegeneration: A randomized controlled trial in greek community-dwelling elders with mild cognitive impairment. Am. J. Alzheimer’s Dis. Other Dement. 2017, 32, 489–499. [Google Scholar] [CrossRef]
- Lakes, K.; Marvin, S.; Rowley, J.; Nicolas, M.S.; Arastoo, S.; Viray, L.; Orozco, A.; Jurnak, F. Dancers perceptions of the cognitive, social, emotional, and physical benefits of modern styles of partnered dancing. Complement. Ther. Med. 2016, 26, 117–122. [Google Scholar] [CrossRef]
- Kunkel, D.; Robison, J.; Fitton, C.; Hulbert, S.; Roberts, L.; Wiles, R.; Pickering, R.; Roberts, H.; Ashburn, A. It takes two: The influence of dance partners on the perceived enjoyment and benefits during participation in partnered ballroom dance classes for people with Parkinson’s. Disabil. Rehabil. 2017, 40, 1933–1942. [Google Scholar] [CrossRef]
- Hackney, M.; Earhart, G. Effects of dance on gait and balance in Parkinson disease: A comparison of partnered and non-partnered dance movement. Neurorehabilit. Neural Repair 2010, 24, 384–392. [Google Scholar] [CrossRef]
- Gomes da Cruz, C.; Molina, G.; Porto, L.; Junqueira, L. Resting bradycardia, enhanced postexercise heart rate recovery and cardiorespiratory fitness in recreational ballroom dancers. Res. Q. Exerc. Sport 2017, 88, 371–376. [Google Scholar] [CrossRef]
- Lankford, D.E.; Bennion, T.; King, J.; Hessing, N.; Lee, L.; Heil, D. The energy expenditure of recreational ballroom dance. Int. J. Exerc. Sci. 2014, 7, 228–235. [Google Scholar]
- Blanksby, B.A.; Reidy, P.W. Heart rate and estimated energy expenditure during ballroom dancing. Br. J. Sports Med. 1988, 22, 57–60. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Hogg, J.; Zandieh, S.; Bostwick, S. A ballroom dance classroom program promotes moderate to vigorous physical activity in elementary school children. Am. J. Health Promot. 2012, 26, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Liiv, H.; Jurimae, T.; Maestu, J.; Purge, P.; Hannus, A.; Jurimae, J. Physiological characteristics of elite dancers of different dance styles. Eur. J. Sport Sci. 2014, 14, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Maraz, A.; Kiraly, O.; Urban, R.; Griffiths, M.; Demetrovics, Z. Why do you dance? Development of the Dance Motivation Inventory (DMI). PLoS ONE 2015, 10, e0122866. [Google Scholar] [CrossRef]
- Merom, D.; Grunseit, A.; Eramudugolla, R.; Jefferis, B.; McNeill, J.; Anstey, K. Cognitive benefits of social dancing and walking in old age: The dancing mind randomized controlled trial. Front. Aging Neurosci. 2016, 8, 26. [Google Scholar] [CrossRef] [PubMed]
- Zajenkowski, M.; Jankowski, K.; Kolata, D. Let’s dance—Feel better! Mood changes following dancing in different situations. Eur. J. Sport Sci. 2015, 15, 640–646. [Google Scholar] [CrossRef] [PubMed]
- Sohn, J.; Park, S.-H.; Kim, S. Effects of DanceSport on walking balance and standing balance among the elderly. Technol. Health Care 2018, 26, S481–S490. [Google Scholar] [CrossRef] [PubMed]
- Kunkel, D.; Fitton, C.; Roberts, L.; Pickering, R.; Roberts, H.; Wiles, R.; Hulbert, S.; Robison, J.; Ashburn, A. A randomized controlled feasibility trial exploring partnered ballroom dancing for people with Parkinson’s disease. Clin. Rehabil. 2017, 31, 1340–1350. [Google Scholar] [CrossRef] [PubMed]
- Hulbert, S.; Ashburn, A.; Roberts, L.; Verheyden, G. Dance for Parkinson’s—The effects on whole body co-ordination during turning around. Complement. Ther. Med. 2017, 32, 91–97. [Google Scholar] [CrossRef]
- Blandy, L.; Beevers, W.; Fitzmaurice, K.; Morris, M. Therapeutic Argentine tango dancing for people with mild Parkinson’s disease: A feasibility study. Front. Aging Neurosci. 2015, 6, 122. [Google Scholar]
- Masters, B.; Kiratli, J.; Hong, M. Physical benefits in dancers with spinal cord injury participating in six week mixed ability Latin dance class. Phys. Med. Rehabil. 2013, 5, S236. [Google Scholar] [CrossRef]
- Hackney, M.; Hall, C.; Echt, K.; Wolf, S. Application of adapted Tango as therapeutic intervention for patients with chronic stroke. J. Geriatr. Phys. Ther. 2012, 35, 206–217. [Google Scholar] [CrossRef]
- Schmidt, T.; Rudolph, I.; Wozniak, T.; Ruetters, D.; Van Mackelenbergh, M.; Huebner, J. Effect of ballroom dancing on the well-being of cancer patients: Report of a pilot project. Mol. Clin. Oncol. 2018, 9, 342–346. [Google Scholar] [CrossRef]
- Wells, M.; Yang, F. A kinetic analysis of the triple step in recreational swing dancers. Sports Biomech. 2021, 1–14, (online ahead of print). [Google Scholar] [CrossRef]

| Number | Search Terms |
|---|---|
| 1 | Ballroom dance OR ballroom dancing |
| 2 | Partner dance |
| 3 | Movement disorders AND ballroom dance OR ballroom dancing |
| 4 | Cancer patients OR oncology patients OR patients with cancer AND ballroom dance OR ballroom dancing |
| 5 | Stroke OR CVA OR cerebrovascular accident AND ballroom dance OR ballroom dancing |
| 6 | Multiple sclerosis OR MS AND ballroom dance OR ballroom dancing |
| 7 | Parkinson’s disease OR PD AND ballroom dance OR ballroom dancing |
| 8 | Dementia OR Alzheimer’s OR cognitive impairment OR memory loss AND ballroom dance OR ballroom dancing |
| 9 | Spinal cord injury or SCI AND ballroom dance OR ballroom dancing |
| 10 | Diabetes OR obesity AND ballroom dance OR ballroom dancing |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wells, M.; Yang, F. Ballroom Dance as a Form of Rehabilitation: A Systematic Review. Biomechanics 2021, 1, 307-320. https://doi.org/10.3390/biomechanics1030026
Wells M, Yang F. Ballroom Dance as a Form of Rehabilitation: A Systematic Review. Biomechanics. 2021; 1(3):307-320. https://doi.org/10.3390/biomechanics1030026
Chicago/Turabian StyleWells, Meredith, and Feng Yang. 2021. "Ballroom Dance as a Form of Rehabilitation: A Systematic Review" Biomechanics 1, no. 3: 307-320. https://doi.org/10.3390/biomechanics1030026
APA StyleWells, M., & Yang, F. (2021). Ballroom Dance as a Form of Rehabilitation: A Systematic Review. Biomechanics, 1(3), 307-320. https://doi.org/10.3390/biomechanics1030026