1. Introduction
Malaria is responsible for approximately 219 million registered cases and 435,000 deaths per year [
1]. According to epidemiological analyses, Brazil has the largest number of cases on the American continent, with an estimated annual occurrence of over 300,000 cases [
2].
The highest prevalence of this disease is concentrated in the northern region of the country, with the main etiological agents being
Plasmodium vivax,
Plasmodium falciparum, and
Plasmodium malariae.
Plasmodium spp. is an intracellular protozoan of the order Haemosporida that has a heteroxenous life cycle, requiring vertebrate (mammal) or invertebrate hosts (
Anopheles spp.), and blood meal is the main form of parasite transmission [
3,
4].
The state of Espírito Santo (ES) has the highest occurrence of malaria in the southeast region, according to the epidemiological data from 1999 to 2006, due to its topographic and climatic characteristics, which favor the reproduction of pathogen vectors. Its endemic advance in recent decades is due to logging (an important economic activity until 1970), resulting in the migration of infected individuals from the Amazon to ES. Vector transmission of malaria in ES occurs in two main geographic regions, the central and metropolitan regions. The central region is predominantly hot (mean annual temperature varying from 21 to 23 °C), with low-lying areas to undulating relief, and carries the potential risk of introducing malaria due to high vector density and human migration from the Amazon and other malaria-endemic regions. The metropolitan region is characterized by a mountainous relief with the presence of the Atlantic Forest, where
Anopheles (
Kerteszia)
cruzii is predominant, and this species is responsible for the transmission of bromeliad malaria [
5,
6].
Diagnosis and treatment in the early phase are indispensable for preventing disease exacerbation and for reducing the risk of mortality. Knowledge about the epidemiology of malaria is still limited, and efforts by the scientific community to fill various knowledge gaps are necessary for the Espírito Santo population [
6]. The gold standards for diagnosing malaria are thick-smear and blood-smear microscopy. In some cases, other diagnostic methods, such as rapid diagnostic tests (RDT), may be used in resource-limited areas [
7]. The treatment of malaria depends on the type of parasite causing the illness and the severity of the symptoms. The specific type of medication and the duration of treatment vary depending on the country where malaria has been acquired and whether the acquired parasite is resistant to common medications. For uncomplicated malaria caused by
P. falciparum, artemether/lumefantrine (Coartem
®) combination therapy is often used [
8]. For other types of malaria, alternative antimalarial therapies may be used, including chloroquine, atovaquone/proguanil, mefloquine, and doxycycline [
9].
In this context, the main objective of this study was to evaluate reported cases of malaria in ES between 2007 and 2017.
2. Results
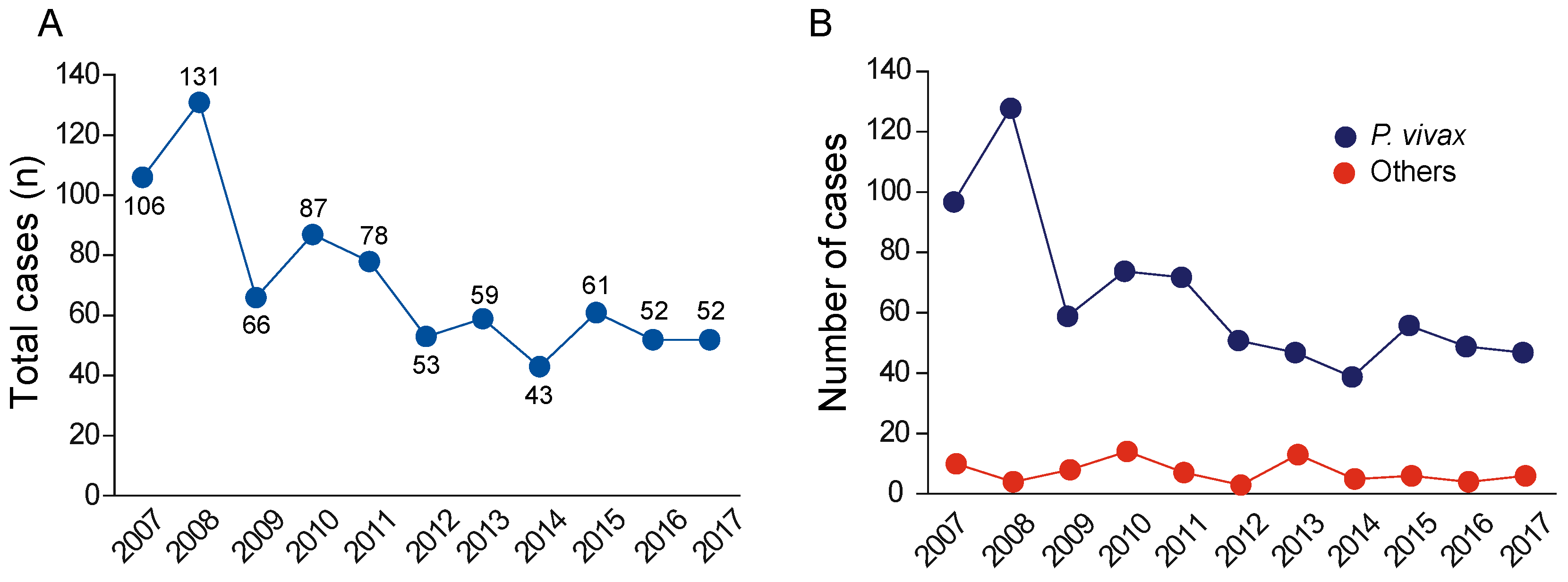
During the investigated period, from 2007 to 2017, a total of 4155 suspected cases were reported. However, only 788 cases were laboratory confirmed, so only these 788 cases were used in our analysis. It is important to note that 2004 was the period that registered the lowest number of malaria cases (43 notifications), while the highest number was registered in 2008 (131 notifications), showing an instability in the disease curve. On the other hand, 2015–2017, the period when most of the reports were made, was more stable in terms of the number of cases per year (
Figure 1A).
A total of 788 malaria cases were laboratory confirmed, and a higher occurrence of
P. vivax was presented in 708 cases (89.85%). In addition,
P. falciparum was the second most frequent cause, with 53 cases (6.73%), followed by co-infection of
P. vivax and
P. falciparum, with 11 cases (1.40%). Both
P. vivax and
P. falciparum gametocytes were observed in five cases (0.63%) as co-infection. At the same time, these analyses also showed co-infection of
P. falciparum and
P. falciparum gametocytes, which occurred in five cases (0.63%) based on the malaria notifications. In addition, we observed that co-infections happened with a combination of
P. falciparum and
P. malariae, albeit only in one malaria case (0.13%). Finally, single infection with the cepa from
P. malariae was presented in five cases, representing 0.63% of the total cases. Other
plasmodium species were not identified (
Figure 1B).
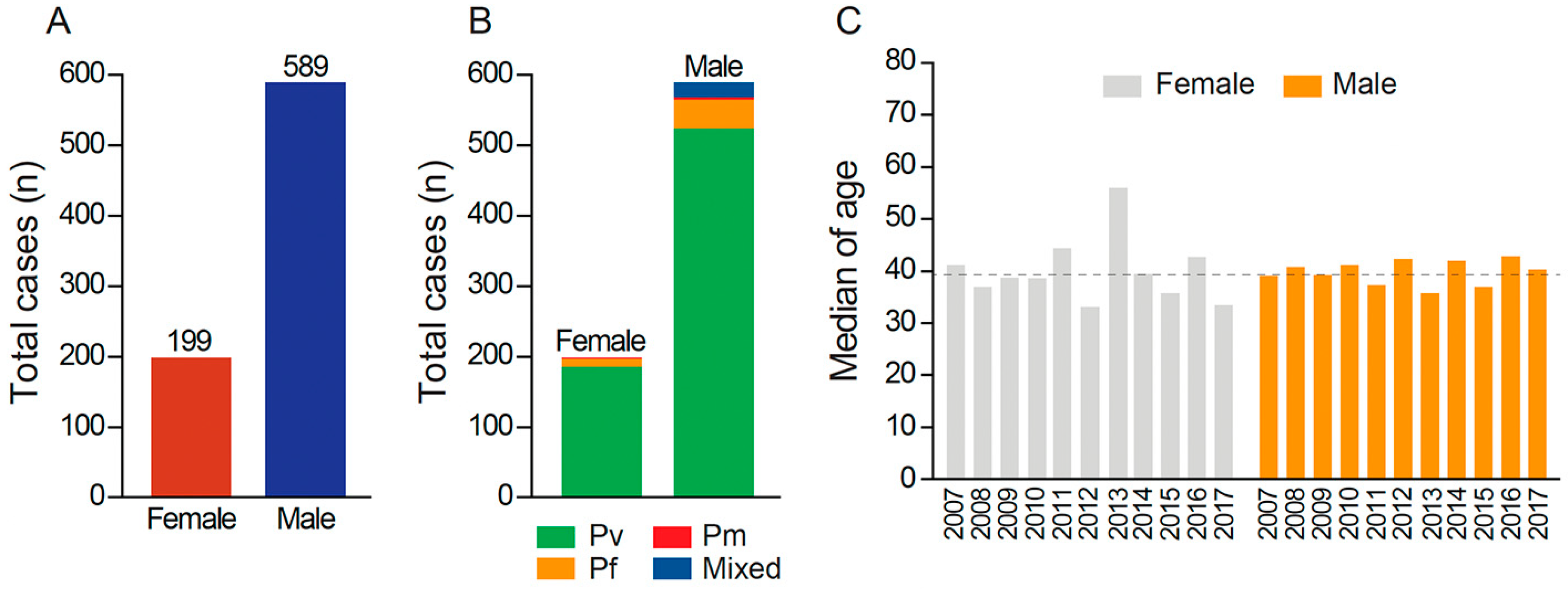
Cases were presented more frequently in men (589 patients) than in women (199 patients), as shown in
Figure 2A. Despite the discrepancy of cases between genders, an equally high incidence of
P. vivax was detected in both groups (
Figure 2B). The patients were on average 40 years old (
Figure 2C). In addition, the multivariate analysis showed that individual
P. falciparum infection or
P. vivax and
P. falciparum co-infection was preferentially allochthonous, occurred more frequently in individuals who had traveled in the previous 15 days, and occurred mainly in males (
Figure 2C).
P. vivax infection was mostly autochthonous and occurred in individuals who had practiced agriculture during the previous 15 days. Single infection with
P. vivax or
P. falciparum was related to occur in the group of 20–39 years of age and occurred more often in subjects with incomplete elementary school (
Figure 2B,C), while mixed infection mainly occurred in individuals between 40 and 59 years.
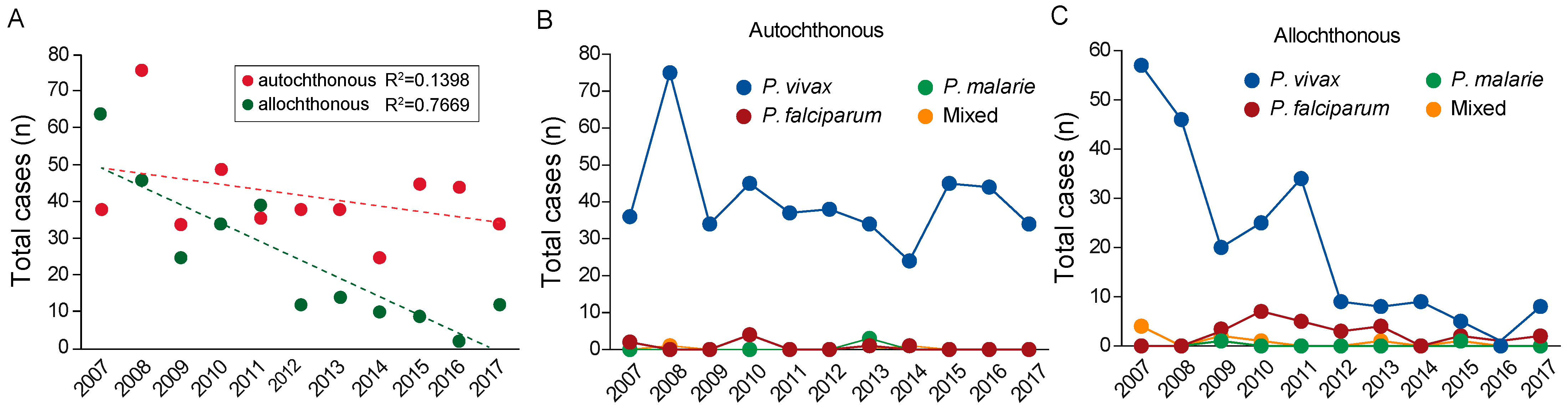
The distribution of both autochthonous and allochthonous cases is represented in
Figure 3. The total sample of 788 reported cases was categorized into 458 autochthonous cases (58.12%), 265 allochthonous cases (33.63%), and 65 unclassified cases (8.25%) (
Figure 3A). In all of these groups, there was a predominance of
P. vivax infection (
Figure 3B,C), and most confirmed cases of this species resulted from an infection of autochthonous origin, totaling 526 cases (66.77%).
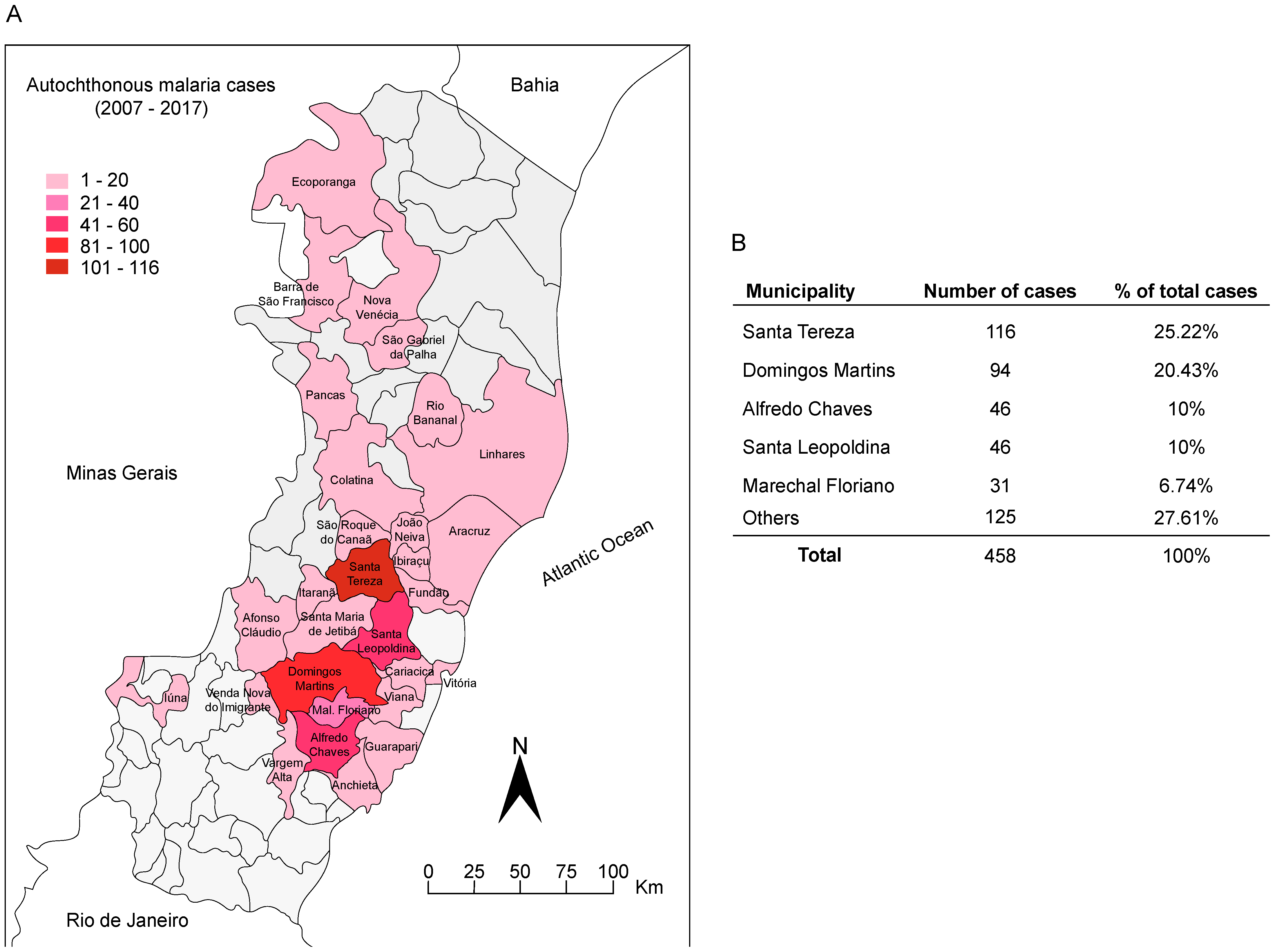
The analysis of the endemic cities of Espírito Santo state indicated that Santa Teresa had the highest number of reported cases for malaria that appear more highlighted in the map (
Figure 4A). Specifically, Santa Teresa presented 116 cases (25.22%) for malaria, followed by Domingos Martins (94 cases/20.43%), Alfredo Chaves and Santa Leopoldina (46 cases/10%), Marechal Floriano (31 cases/6.74%), and all other municipalities together (125/27.61%) (
Figure 4B).
The analysis of these numbers revealed the high incidence of infection in these municipalities, which together corresponded with an annual average of 29.51 cases per 100,000 inhabitants compared to 1.18 cases per 100,000 inhabitants for the entire state.
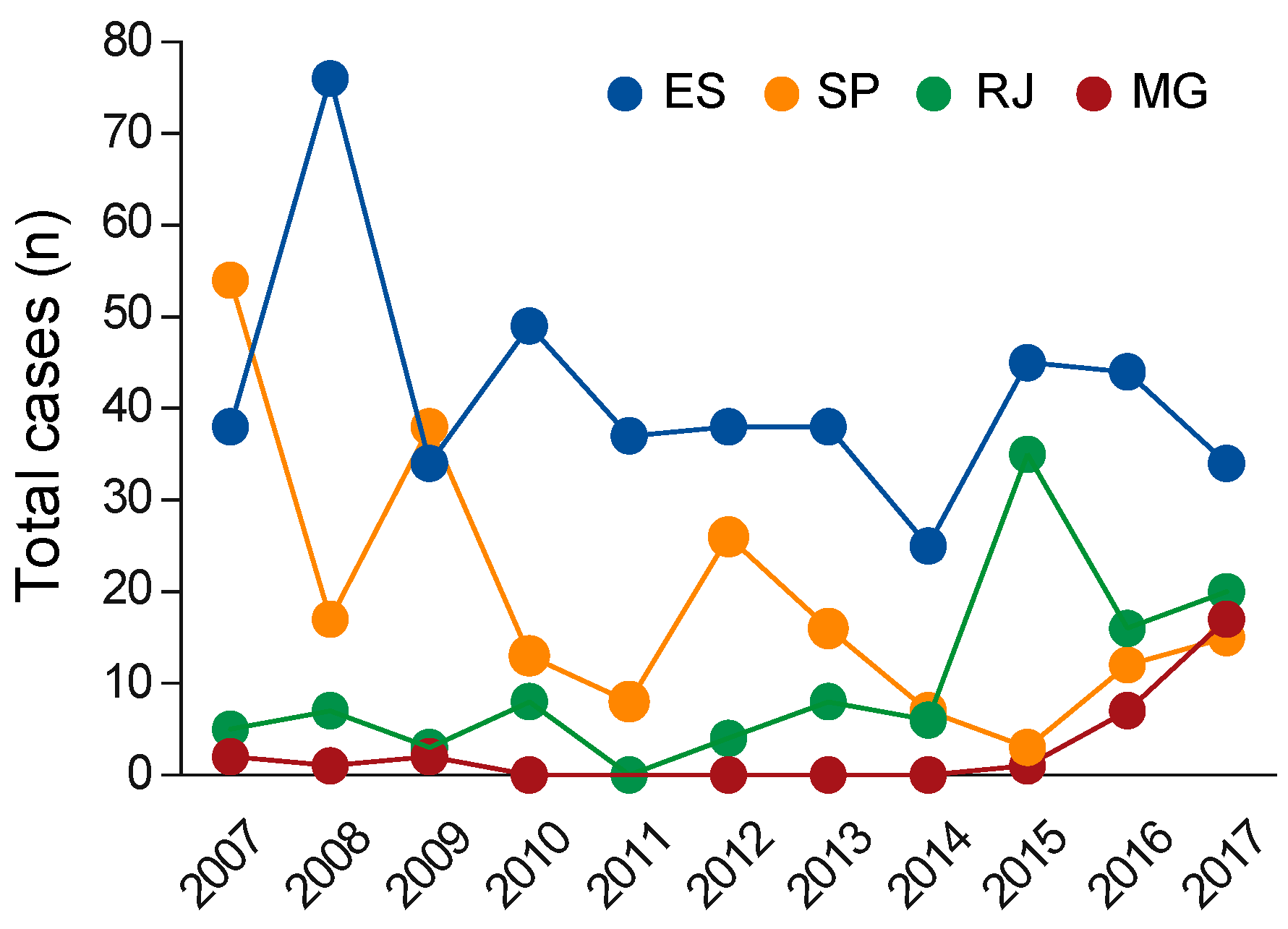
In a comparative analysis of reported cases in the southeast region of Brazil, Espírito Santo showed the highest incidence of infection [
3], although there was a significant decrease in the years 2015–2017, while nearby states (São Paulo, Minas Gerais, and Rio de Janeiro) showed a growing trend in the number of reported cases (
Figure 5).
3. Methods
3.1. Study Area
Espírito Santo state is located in the tropical zone of the southeastern region of Brazil, which also includes the states of Bahia, Minas Gerais, and Rio de Janeiro. The territory has 4,016,356 inhabitants, who are distributed over an area of 46,095 km² and divided among 78 municipalities [
10]. As for its natural aspects, Espírito Santo shows environmental and climatic diversity, with a predominance of the Atlantic Forest biome, and mild temperatures and frequent rainfall caused by air masses coming from the Atlantic Ocean. Regarding climate conditions, the local case is determined by humid tropical climate, with an average temperature of 25 °C and an annual rainfall of about 1400 mm. Thermal amplitude is low, and two well-defined seasons are present: dry and wet (or rainy). The main cities from ES present high numbers of reported cases of malaria, as Santa Tereza, Domingos Martins, Alfredo Chaves, Santa Leopoldina, and Marechal Floriano being the cities with the highest proportions of infection in the state, comprising 72.27% of autochthonous cases during the study period. The city of Santa Teresa stands out in relation to the number of malaria infections, presenting an average annual incidence of 49.90 cases per 100,000 inhabitants and an annual case density of 13.70 cases per 1000 km
2.
3.2. Data Sources
The data used in this study correspond to notifications that occurred during the 2007–2017 period and were obtained from the Special Center for Epidemiological Surveillance of Espírito Santo (NEVE-ES, Núcleo Especial de Vigilância Epidemiológica do Espírito Santo, in Portuguese). The information was obtained from the Individual Notification Forms organized by the Notification of Disease Information System (SINAN, in Portuguese), and these forms were collected indirectly through secondary data sources from those involved.
From the obtained data, we collected information corresponding to the variables of interest: population classification (autochthonous or allochthonous), parasitological laboratory results (P. vivax, P. falciparum, P. malariae, or mixed infection), parasitic density, date of notification and first symptoms, probable location of source of infection, gender, age, education, and activity within the past 15 days.
The data referring to cases from other states of the southeastern region (São Paulo, Minas Gerais, and Rio de Janeiro) were analyzed using DATA-SUS, and population density was obtained from the IBGE database.
3.3. Data Analysis
The data analysis consisted of 788 cases that were confirmed by laboratory tests. A total of 4155 cases were reported, and 3367 cases were notified as suspected cases only, without PCR confirmation. Thus, 788 malaria-confirmed cases were analyzed in this retrospective cross-sectional study, using Microsoft Excel to evaluate tables, graphs, and statistical calculations. The map presented in results was created using both Quantum GIS and Fitopac software.
3.4. Ethical Considerations
This study was approved by Multivix ethical committee that is an Institutional Review Board (IRB), CAAE: 94894718.9.0000.5066.
4. Discussion
Between 2007 and 2017, only 788 cases of malaria were confirmed from a total of 4155 suspected cases (
Figure 1). It is important to note that, it is possible that cases with mild symptoms could decrease the sensitivity of rapid diagnostic tests (RDTs), and then, this can interfere the average time of disease diagnosis in the state of ES, which is approximately 11 days. But, according to the National Program of Malaria Control (PNMC), the time of diagnosis from the appearance of first symptoms is estimated to be 24 h. Thus, perhaps it can explain because only 788 cases confirmed from a total 4155 suspected.
As for the confirmed cases, an analysis of diagnosed patients in the 20–39 age range revealed the predominance of males (74.7%) when compared to females (39.5%) (
Figure 2B,C). In fact, the reason why younger people are more prone to contract malaria needs to be investigated with possible new studies. Our efforts were focused on protozoan species to elucidate the principal species found here in ES and to compare it with the scenarios of other Brazilian states. We found indications in the reported malaria records that
P. vivax,
P. falciparum, and
P. malariae species, which are protozoans that cause malaria, were more frequently notified in the ES; thus, it is possible that these three species are the principal species found in local cases. In addition to this finding, it is worth noting that out of the 788 confirmed malaria cases, 458 cases were autochthonous and 265 cases were allochthonous. The statistical analysis of the evaluated period showed a significant decrease in the number of allochthonous cases compared to autochthonous cases (
Figure 3A). These results show that the ES state had mostly allochthonous cases in 2007, but after 2017, the most frequent notification was for autochthonous cases, which suggests that ES has some features that allow us to hypothesize that malaria is endemic to the area. More specifically, while there was a remarkable decrease in the rest of the country from 2006, which extended to 2008 with a considerable reduction in notifications of malaria [
11], there was a surprising rise in the number of cases in ES in 2008, with a 22% increase in total confirmed cases between 2007 and 2009, which was attributed to the high interregional migration of the time. According to the IBGE [
9], a growth in industrial activity led to the migration of individuals from many different states and countries (e.g., Angola) to ES during the study period. These included the state of Rondônia, where there was a higher annual parasite incidence in 2008, corresponding to 42.3 cases/1000 inhabitants. This was probably due to the presence of a high number of insect
Plasmodium vectors in that region. Thus, the state of Rondônia became the main source of disease migration, with 78.26% of allochthonous cases reported [
12], which corresponded with the high notification of ES allochthonous cases in that year. During the study period, the number of malaria cases decreased (
Figure 1A), and this reduction coincided with a decrease in case numbers in the Amazon region, reflecting the local program for malaria reduction [
11].
Despite preventive methods, urban regions containing the mosquito vector facilitate new outbreaks of autochthonous cases of malaria in the ES state. The main vector of
Plasmodium vivax reproduces in the verticals of the
Bromeliacea family plants, which are typical of the Atlantic Forest biome present in most of the territory of ES. As a result, in the municipalities with the largest numbers of cases (
Figure 4B), the disease is known as bromeliad malaria as there is a predominance of these plants in the tree canopies, especially in the city of Santa Tereza, and this would explain such a high incidence of this protozoan in ES. The large presence of Bromeliaceae in forested, mountainous terrains with an average temperature of 19 °C, such as Santa Teresa and Domingos Martins, another city with a higher prevalence of bromeliad malaria, seems to provide an appropriate environment for vector proliferation. This suggests that the transmission of RSMA by
Anopheles (K.) cruzii may be an indication of human occupation in previously preserved Atlantic Forest areas and that the spread of the disease is sustained by men entering the forest [
5]. Until 2007, malaria predominated in the allochthonous population, but from 2008 to 2017, the number of autochthonous cases increased (
Figure 3A). Thus, the incidence of autochthonous cases in ES increased, while in the other extra-Amazonian regions, allochthonous cases still prevailed [
13]. After 2007, this state had a higher number of combined cases (n = 458) when compared to the total number of malaria cases in the states of São Paulo, Rio de Janeiro, and Minas Gerais (n = 351) (
Figure 5).
Malaria involving the
P. vivax species is more prevalent in the Americas and, as also observed in this study, the majority of cases are of autochthonous origin, accounting for about 90% of confirmed cases (
Figure 1B). The increase in previously underreported cases of
P. vivax (data not shown) is believed to be due to the fact that this widely dispersed pathogen causes a milder type of malaria, which does not cause considerable damage to the host and has low lethality. Therefore, as
P. vivax infections are mostly asymptomatic or display signs and symptoms similar to other more frequent diseases, e.g., the flu, it is assumed that the number of infected individuals who do not seek medical attention is high. Individuals infected with the
P. falciparum parasite present the most severe form of the disease with alarming conditions, but its incidence in the state is not significant [
14]. Another important finding is the occurrence of mixed infection of both
P. vivax and
P. falciparum, the latter being the third most recurrent, surpassing infection by
P. malariae (
Figure 3B,C). The disease caused by
P. malariae has clinical conditions similar to
P. vivax infections, but with lower fevers with three days intervals.
P. malariae notifications in ES is not significant [
15], covering approximately 0.63% of the notified cases during the period evaluated.
Altogether, the analysis constructs a malaria disease scenario in the state of ES, which is one of the most important states for the economy in Brazil according to the IBGE [
16]. Currently, the public health agencies do not consider ES to be an endemic area for malaria, especially when compared to the Amazon region, which accounts for almost all cases of malaria. However, ES has a predominance of malaria cases when we compared it to the case–population ratio of other states in the southeast region (
Figure 5). This comparison supports the idea that ES is an endemic area, and it is important for public health agencies to lead the discussion in this direction upon the presentation of the results in this work [
13].

 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}




