Abstract
Cystic Echinococcosis (CE) is an endemo-epidemic disease in the Rio Negro Province, República Argentina. Due to the number of cases, the length of hospital stays after surgery and its associated mortality, it is a serious public health problem that generates high costs for the health system. Oriented towards its control, primary prevention activities have been carried out since 1980, based on the deworming of dogs and the vaccination of lambs; secondary prevention has consisted in the actively search for cases through serological or ultrasonographic screening; and tertiary prevention has been based on timely treatment, either by surgery or by medical treatment with albendazole. All these prevention activities have been carried out under the concept and strategies of the “One Health” model, through both inter-institutional and interdisciplinary work, as well as with the support, commitment and critical participation of the community. As a result, an important drop has been observed in the prevalence of CE in humans and in its lethality (0.5% in 1997–2020, no deaths in the last two years); moreover, an important decrease has been observed in costs to the health system, due to the reduction of hospitalizations and the number of surgeries.
1. Introduction
Cystic Echinococcosis (CE) is a zoonosis that has an impact on the health systems of endemic areas, due to the high number of medical consultations and the high costs generated by the treatment of patients (many of it surgical), together with the need to keep control programs that need to be sustained for many years to be truly effective. CE mostly affects rural populations, and for the study and treatment of their condition they must be sent to tertiary referral hospitals with surgical devices, hundreds of kilometers away, with consequent uprooting, loss of workdays and family breakdown. In addition, the treatment of CE should be considered together with morbidity and mortality. On the other hand, CE generates production losses linked to affected sheep and goats [1,2].
The cestode Echinococcus granulosus (EG), an etiological agent of CE, resides, in its adult form, in the intestines of dogs and other canids, which periodically eliminate eggs through their feces. These eggs contaminate the environment and can be accidentally ingested by intermediate hosts (usually sheep and goats) and, eventually, by humans. The eggs hatch in the stomach, releasing the embryos into the small intestine of the definitive host; the embryos pass through the intestinal villi into the bloodstream and grow in different organs, where they develop their cystic form; the liver and lungs are the most frequently affected organs [3,4]. The rate of growth in humans varies, depending on the organs affected: the lungs and peritoneum are less resistant to cystic growth than the liver, and this is closely related to the onset of symptoms [3,4].
Patients can either remain asymptomatic for many years, or develop symptoms, depending on the affected organ and/or cystic complications. In other words, a human being can either remain asymptomatic throughout their life, or develop symptoms with varying degrees of severity; in some cases, a CE cyst can lead to death [3].
In sheep, CE cysts become fertile between the first and second years of life and live until the animal is slaughtered, thus securing the survival of EG in the territory during the sheep’s seven to nine years of life. Even though animals do not present any morbimortality, their production, on the other hand, could be affected.
Primary endemic foci occur in marginal rural areas, which are often (although not exclusively) linked to both low social and economic conditions and sheep and goat production; thus, producers and their families (native communities very often included) who raise sheep and goats as their main means of subsistence, are more commonly affected by CE. Secondary endemic foci occur in the periphery of cities (suburban neighborhoods) close to endemic areas, in relation to migratory flows from the countryside to the city, with the subsequent transfer of habits and customs that lead to the appearance of cases in marginal, peri-urban populations [4,5,6].
The study, diagnosis, treatment, surveillance and control of CE is a perfect example of the strategies that have been developed on the basis of the “One Health” approach, an holistic method that contributes to the prevention of endemic and epizootic diseases, with due respect for the integrity of ecosystems and for the benefit of humans, domestic animals and biodiversity; among its priorities, this method includes zoonoses, vectors, food security, antimicrobial resistance, the effects of climate change and the emergence and reemergence of diseases [7,8]. “One Health” is promoted jointly by the World Health Organization (WHO), the World Organization for Animal Health (OIE) and the Food and Agriculture Organization of United Nations (FAO). It emphasizes the need for a paradigm shift from disease-specific interventions to holistic cross-cutting approaches, coordinating with adjacent disciplines [8,9].
Naturally, the concept “One World, One Health” arises from diverse experiences in disease control, and from previous experiences with inter-institutional or interdisciplinary articulation; such is the case of the scheme carried out in the Province of Rio Negro, Argentina, where CE is endemic.
In 1980, the Ministry of Health of the Province of Rio Negro launched a Control Program against CE, with activities related to its diagnosis, treatment, surveillance and control [6,10,11,12].
The aim of this paper is to summarize the strategies developed and their results, according to the approach now called “One Health”, on a multi-disciplinary basis and at different levels of health prevention.
2. Materials and Methods
Primary prevention includes all the actions that are aimed at the prevention of the disease and all the activities that are oriented towards health education and the fostering of health habits; secondary prevention consists of early diagnosis in order to reduce impact of the disease, including the actions undertaken to detect it in the asymptomatic period. Finally, tertiary prevention is performed in the pathogenic period of the disease, and treatment is approached with a view to the recovery of health with minimum morbidity and mortality (Table 1) [13,14].

Table 1.
The levels of prevention and the “One Health” strategy for the care of cystic echinococcosis in the Province of Rio Negro, Argentina.
2.1. Work Area
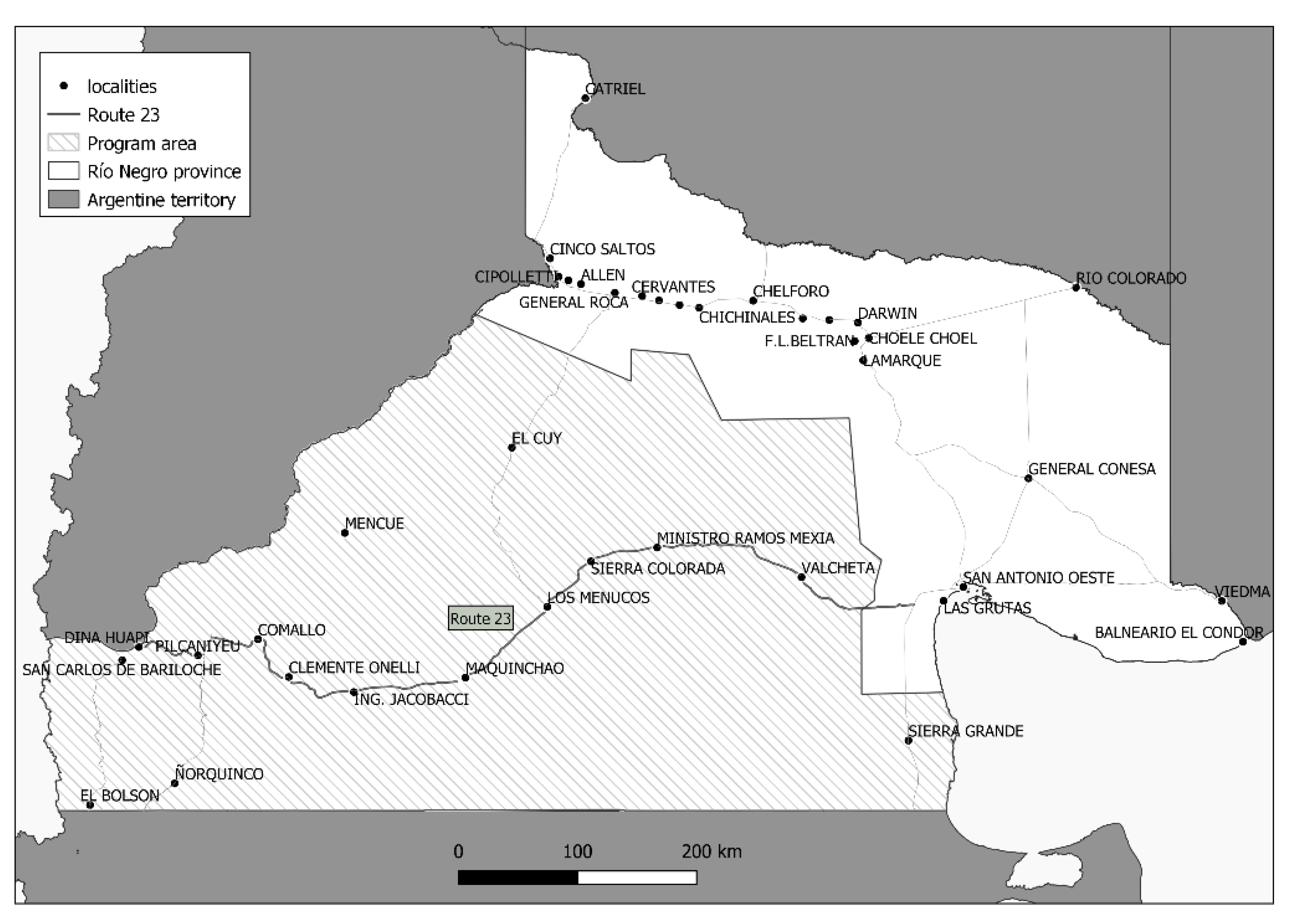
The control activities are centered in the south and west of the Province of Rio Negro, in the Patagonian region of Argentina, in the Departments of Bariloche, Ñorquinco, Pilcaniyeu, 25 de Mayo, 9 de Julio and Valcheta, ranging from the mountain towns of El Bolsón and San Carlos de Bariloche on the border with Chile in the east, to the rural zones of the Patagonian plateau areas of Cona Niyeu (Sierra Grande) and Aguada Cecilio (Valcheta) in the west (120,013 km2, with only 0.88 inhabitants per km2, Figure 1), across geographical coordinates ranging from −41.965530/−71.5341200 to −41.3308100/−69.5457600.
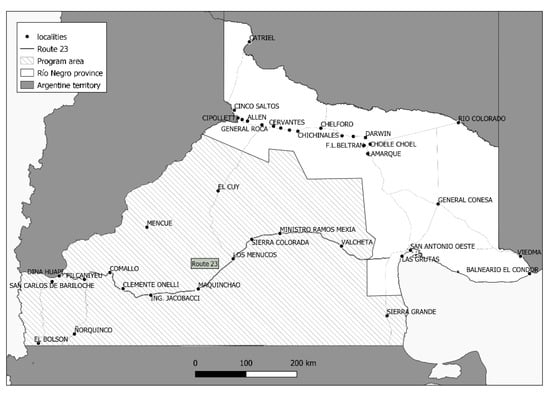
Figure 1.
Endemic area with a cystic echinococcosis control program, Rio Negro Province, Argentina.
In this region, which the highest number of cases in the province, sheep and goat farming are the main production activities, thus providing ideal epidemiological conditions due to the lasting habits of slaughtering adult sheep, followed by delivery of viscera to dogs; other important factors include an excessive number of dogs, a lack of drinking water, and weather conditions, all of which favor the survival of Echinococcus granulosus eggs in the environment [6,10,11,12].
2.2. Primary Prevention
Since the beginning of the program, the Veterinary Public Health (VPH) team, together with 65 health workers from 13 rural hospitals and general practitioners from primary care, have carryied out policies oriented towards health education at various levels and on different population groups, thus complementing the task of schoolteachers in the aim of both fostering adoption of healthy practices against CE and encouraging the active participation of the community in surveillance and control activities.
Since 1980, the treatment of dogs, which is aimed at breaking the cycle of transmission, has been carried out with PZQ at a dose of 5 mg/kg, in home visits by sanitary agents four times a year; the continuity of this treatment is dependent on the accessibility of rural areas (depending on weather and road conditions), as well as on the political and economic changes that have taken place over time. The tablets (coated in pâté for better acceptance by the dog) were delivered to the owners or provided by sanitary agents for the owners to deworm their dogs under their own responsibility. This was complemented by the VPH team during surveillance and vaccination activities [10,12,15]. The number of rural dogs in the program area registered by health workers on house-to-house visits ranged from 11,000 to 14,000 at the beginning of the program.
In 2006, the annual vaccination of lambs with the EG 95 vaccine was incorporated as a control strategy by the VPH team in some risk zones, where the prevalence of sheep remained high, especially in those areas with a predominant native population (mainly the Mapuche community). A maximum of three doses were applied to lambs at 30 and 60 days of age, as well as one booster per year [15]. Goats were not included in the vaccination program, given that the most important strain acting in the region was G1 sheep (unpublished data) and because, from the initial point of view of the author, goats play a secondary epidemiological role in the work area.
The surveillance of the animals by VPH was carried out initially through the oral administration of taeniafuge arecoline hydrobromide (arecoline) tests to dogs, with the subsequent identification of adult E. granulosus in the dogs’ eliminated feces. The drug was optionally applied at a canine concentration of 1% at the dose of 4 mg/kg, with prior agreement from the owners.
In 2003, the arecoline test was replaced by the copro Elisa/PCR test, which was used to confirm the identification of parasitic antigens by “in- house” tests on samples of canine fecal matter collected from the environment. The test was applied in randomized cross-sectional sampling in the periods 2003–2005, 2009–2010 and 2017–2018. According to the results, the surveillance system was based on the identification of both sheepfarms and/or the owners of dogs with current transmission; those with at least one positive result obtained from the animals’ fecal matter and confirmed by PCR, in were considered at risk [10,12,16].
2.3. Secondary Prevention
Since 1980, human screening activities have been included in the area under the Control Program against CE. During the period 1980–1996, serological screening was carried out using the double diffusion test (DD5) and, later, enzyme-linked immunosorbent assays (ELISAs), depending on the technology available; in some positive cases, serology imaging, such as ultrasound and chest X-ray, was required for the diagnosis of localization of CE, as well as for immediate surgical treatment [10,11]. In 1997, abdominopelvic ultrasound (US) imaging replaced the serological test for screening, and it is now the technique of choice, owing to both its higher sensitivity and specificity and its low operating cost; another advantage is that moving to remote rural areas is made easier by portable US equipment [11,17,18]. The program has invested in this portable ultrasound equipment and has trained general practitioners at rural hospitals in screening populations, through a FASE (Focused Assessment with Sonography for Echinococcosis) training course delivered by a medical committee of imaging-diagnosis specialists and surgeons [19].The US abdominal scans during surveys are performed with the consent of the parents by signing the informed consent form [11].
In all cases, the main subjects are schoolchildren (aged 6 to 14 years old), although spot screenings are also carried out in all age groups [6,17]. Surveys of schoolchildren in rural areas are conducted on an annual basis, thus ensuring early diagnosis and a system of surveillance of CE disease among the population.
2.4. Tertiary Prevention
At the beginning of the program, surgery was the only treatment for CE [20,21]. New therapeutic options [22] were included early in the program, especially antiparasitics, such as albendazole, (ABZ) and occasional percutaneous treatment, when indicated [18].
Thus, even in simple rural hospitals, advances in knowledge about the natural history of C and, new treatment options associated with the availability of imaging techniques. such as US, have allowed the incorporation of new strategies within the program, depending on the type of cyst, its location, and the opportunities for follow-up in rural areas; such strategies include both treatment with antiparasitics and the longitudinal monitoring of patients, in order to determine the cysts’ evolution and to accordingly decide on the best and most convenient treatments [11,18].The mandatory notification, registration and follow-up of new cases has also made it possible to maintain a comprehensive and integrated surveillance of the population.
Finally, Table 2 presents a timeline summary of the techniques used by the program from the first diagnosis of the situation to the present.
Table 2.
Summary of the techniques and activities performed within the program from the first diagnosis of the situation to the present.
2.5. Statistical Analysis
The medical and US detection records, dog epidemiological surveillance and sheep vaccination records were built in databases created with Microsoft Excel® 2.0 (Raymond, WA, USA). The statistical analyses were performed using EpiDat® 3.1 (Xunta de Galicia, Spain), including estimates of proportions and their confidence intervals (95% CI), x2 of the association, with a significant level of p < 0.05, and sample size estimates.
The geographical analyses and mappings were carried out with QGIS® 3.4 (Free Software Formation Inc., Boston, MA, USA).
3. Results
Between 1980 and 1997, 185,000 PZQ tablets were delivered, at an average of 2.2 tablets per dog, with coverage estimated at 65% [10]. In subsequent years, the provision of PZQ was continuous with a distribution to rural hospitals of 100,000 tablets per year.
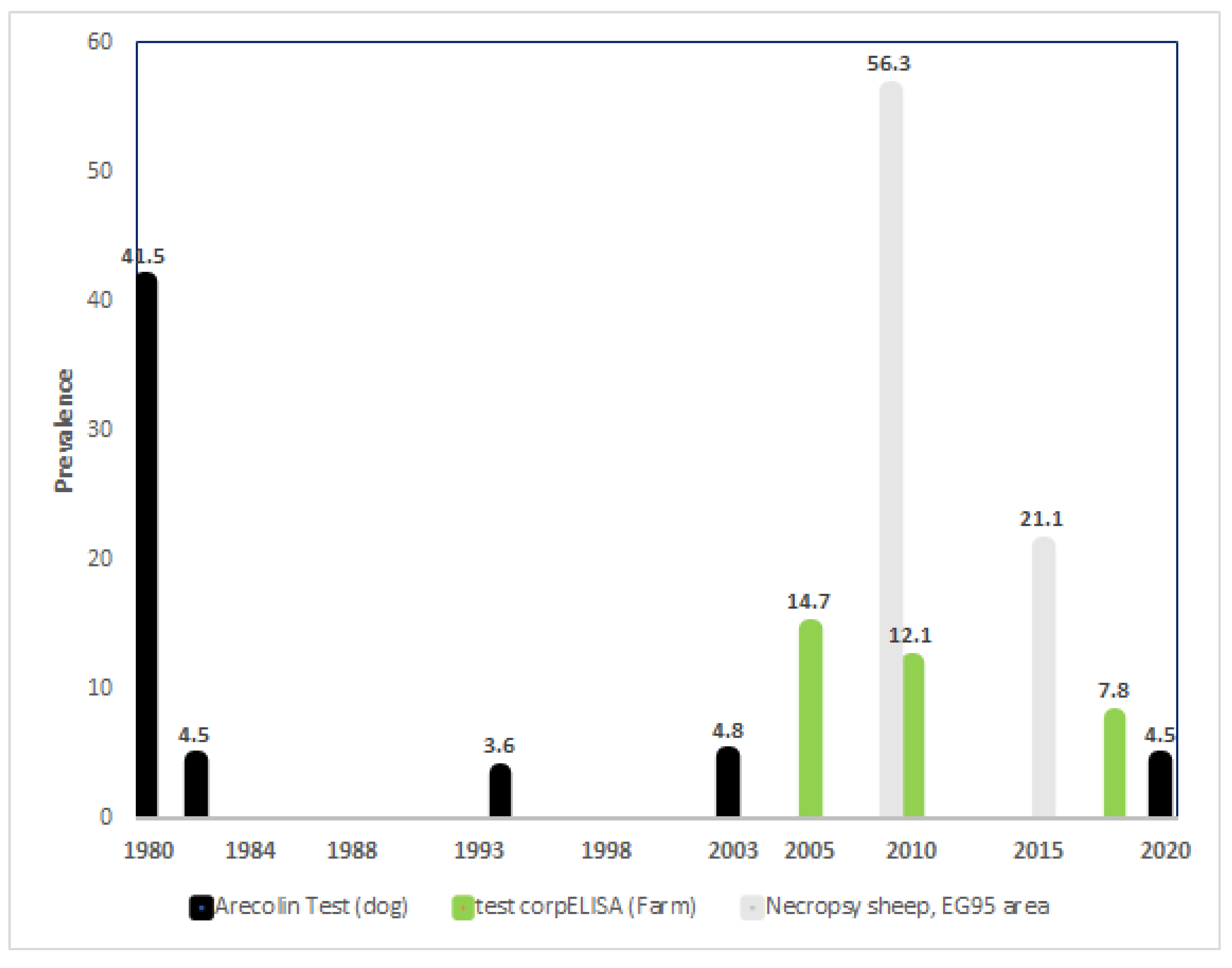
For surveillance purposes, the arecoline test was performed on 23,895 dogs in the period 1980–2003. The initial prevalence was 41.5% ((95% CI 38.4–43.5), dropping to 6.1% (95% CI 4.8–7.6)) in the first year of work, and to 4.5 (95% CI 3.0–6.5) in 1982. Since then, it has remained at the same level, with small annual variations (ranging from 2.3% to 9.5%) The last global evaluation with the arecoline test was in 2003, with a canine prevalence of 4.8% (95% CI 2.8–7.2) (Figure 2) [10,16].
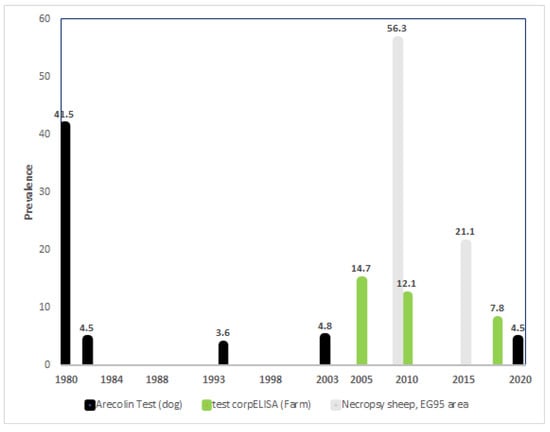
Figure 2.
Primary prevention: main indicators of the evolution of prevalence rates in animals and the environment, related to control actions between 1980 and 2020. Note: arecoline 2020 of EG95 area.
The copro ELISA/PCR test was carried out on 1780 samples of canine feces from 780 randomly selected farms, in three cross-sectional studies in 2003–2005, 2009–2010 and 2017–2018. A total of 17.0%, 18.2% and 8.2% of samples of fecal matter tested positive, respectively, which indicated the presence of at least one infected dog in 14.7% (95%CI 10.7–19.5), 12.1% (95% CI 12.1–16.6) and 7.8% (95% CI 4.7–11.9) of the establishments studied, the difference being statistically significant (p < 0.001) (Figure 2) [12,16].
The vaccination strategy, which began in 2009, was applied only on indigenous reservations inhabited by the Mapuche population, a limited part of the endemic area where the control of the disease presented special geographical and socio-cultural difficulties.
In this area, 3146 lambs from 79 producers were included in the vaccination program. Between 2009 and 2020, 43,953 doses of vaccine were applied with a coverage of 80.1% to 85.75% [14]. The lambs’ humoral response to vaccination reached its maximum value after reinforcement at one year of life (optical density 405, 0.828).
As a result of the activities described, the prevalence of infection in adult sheep in these indigenous reservations dropped in the first five years, from 56.3% to 21.1%. Likewise, the number of hydatid cysts per sheep (the total number of cysts detected at necropsy/number of necropsied sheep) decreased from 94.7% to 23.5% (Figure 2) [15].
Research conducted in 2020/2021 showed an absence of positives on autopsy in adult goats (unpublished date).
With regards to dogs, after 8 years, the number of producers whose dogs tested positive on the copro ELISA/PCR test dropped from 45.8% to 23.4%, whereas, with arecoline tests, no significant differences were observed [15].
During the period 2006–2016, eight cases were identified in children under 16 years of age; in 2017 there was only one such case, and there were zero cases between 2018 and 2020.
With reference to secondary prevention, between 1980 and 1997, the active search for cases was carried out by 48,826 serological studies among the asymptomatic population; positive cases were studied for organ localization and early surgical treatment [10,18].
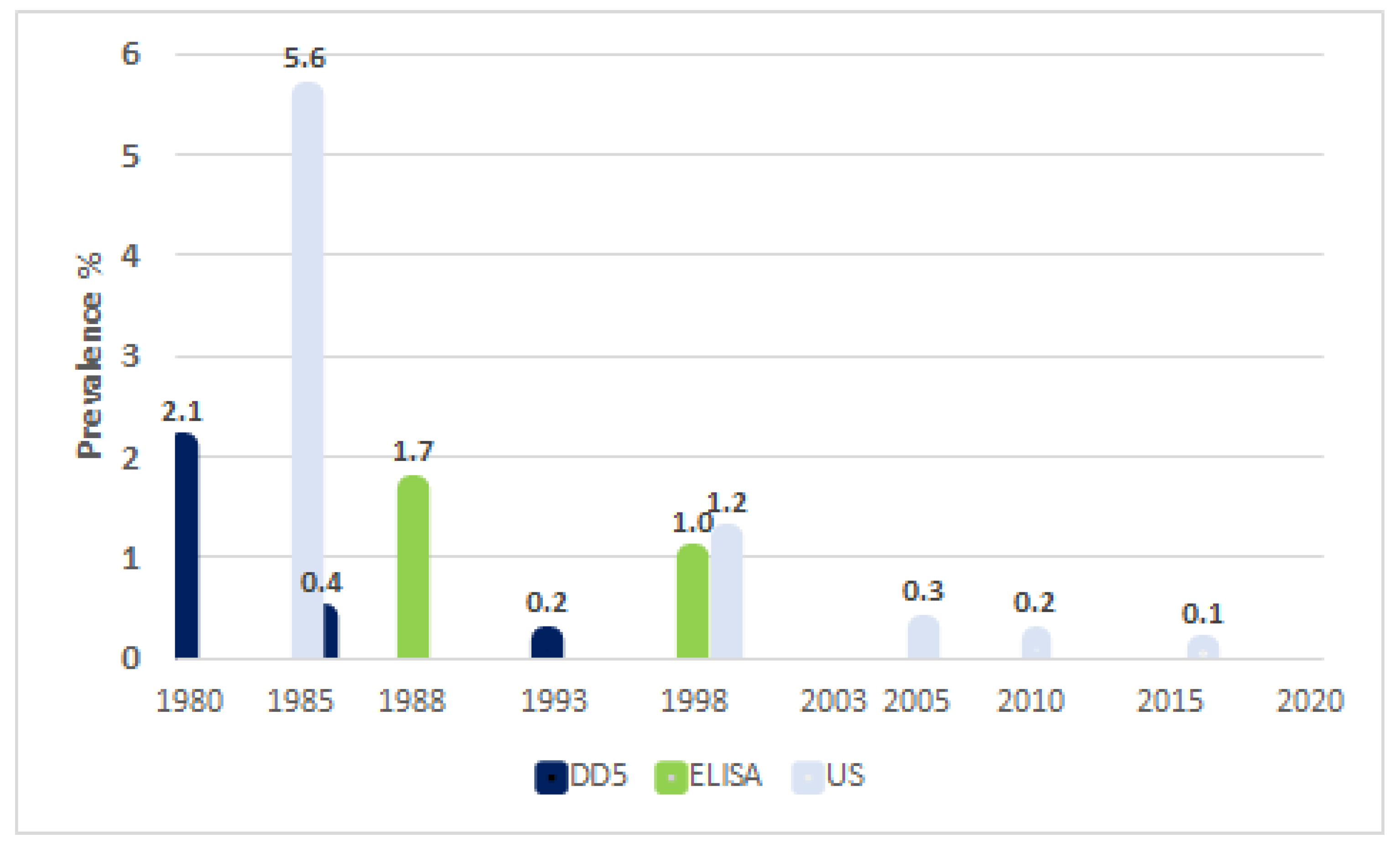
The initial prevalence rate in schoolchildren was 2.05% (CI 95%, 1.9–2.2), which then showed a descending curve, reaching 0.41% in 1984, and a rate of 0.20% (CI 0.1–0.3) positive DD5s was observed in 1993. With ELISA, the first study in 1988 showed a positive rate of 1.70% (95% CI 0.8–3.1), while the last screening showed a positive rate of 1.00% (0.7–2.2) [11,18].
The first screening with US was carried out in schoolchildren between 1984 and 1986, detecting a prevalence of CE cyst carriers of 5.60% (95% CI 3.2–9.9). Its systematic use for surveillance purposes began in 1999, with a prevalence of 1.20% (CI 95% 0.04–2.7), gradually decreasing to reach a prevalence of 0.30% in 2005 and 0.20% (95% CI 0.1–0.3) in 2018, for a total of 47,233 studies conducted between 1997 and 2018 (Figure 3) [11,18,23].
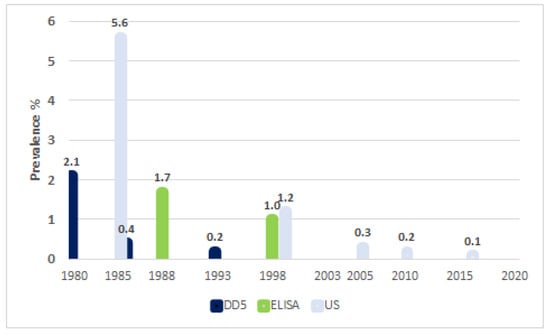
Figure 3.
Secondary prevention: main indicators of the evolution of prevalence rates in children aged 6 to 14 years, related to control actions.
With respect to tertiary prevention, the treatment approach to CE was exclusively surgical until 2000 [20,21]. For instance, in the surgery service of Artémides Zatti Hospital in Viedma, from January 1974 to July 1992, a total of 317 surgeries were performed on 294 patients; postoperative mortality was 8.3%, with an average hospital stay of 34.3 days, and of 55.6 for those surgeries with multiple CE cysts. A total of 13.3% of surgical bed days and 8% of intensive care discharges were linked to CE patients [20,21,24].
The annual cost to the health system incurred by the care of patients with CE was extensively studied in 2010, amounting to US$ 256,000 (CI 5% 84,000–764,000) for surgical cases and US$ 15,900 (5800–46,900) for non-surgical cases. The total cost of human CE for the province of Rio Negro, involving direct costs to the health system and indirect costs (loss of workdays included) was estimated at US$ 1,194,000 (CI 95% 218,000–2813,000) [25].
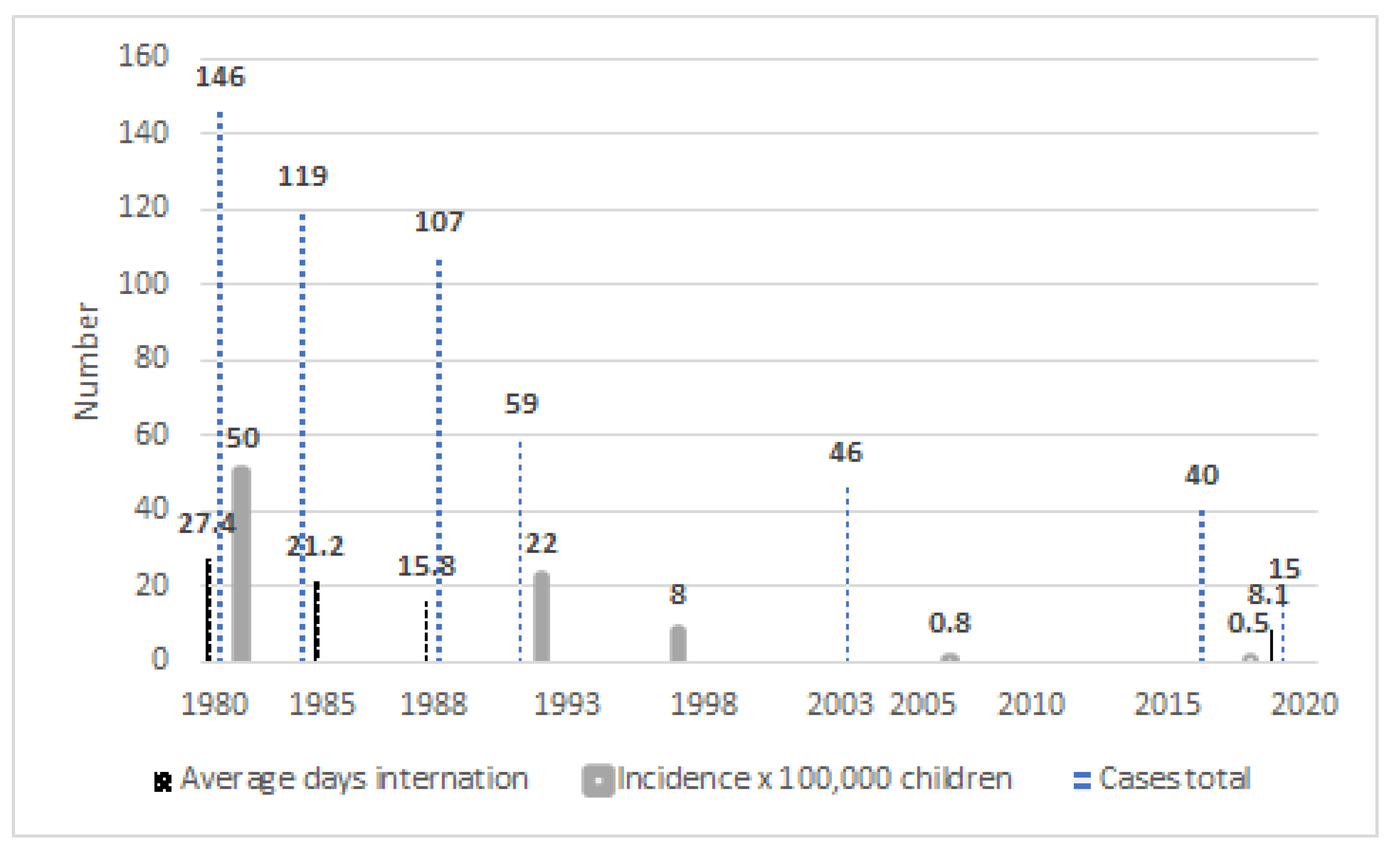
After the implementation of primary prevention measures, in the period 1980–1996 1720 new cases were diagnosed (101 cases on average per year, with initial incidence rates between 76 and 120 × 100,000, decreasing to 29 × 100,000 in 1997), while in the period 2006–2016 there were 478 cases (43 cases on average per year, with incidence rates of 6 × 100,000) [9,13]. In 2019, the number of reported cases was 15 (2.3 × 100,000). For children under 16 years old, in 1980, the incidence rate was 50 × 100,000; in 1990, it was 22 × 100,000; in 1997, it was 8 × 100,000; in 2006, it was 0.8 × 100,000; and it was 0.5 × 100,000 in 2016 [11,18].
It should be pointed out that after the incorporation of secondary prevention programs, with their components of active case search and early surgery, mortality decreased: in the period 1982–1992, it was 0.96% [20,21]. Hospital stays also dropped from 27.4 days in 1980, to 15.8 days in 1988 and 8.1 days in 2019–2020.
In 1997, the Control Program protocolized and standardized the use of albendazole (ABZ) in the treatment of asymptomatic carriers; the protocol, with periodic updates, is still in use [9,18,21]. Thus, in the period 1997–2016, out of all asymptomatic children from 6 to 14 years old with CE cysts, 43.3% were treated with ABZ, 43.3% entered the follow-up-only protocol and 8.8% were submitted to surgery (Figure 4) [11,18].
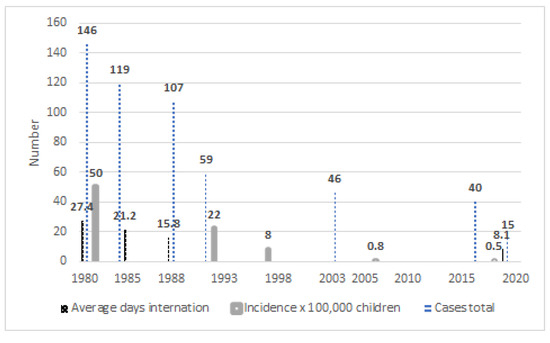
Figure 4.
Tertiary prevention: main indicators of the evolution of treatments and their relationship with control measures.
In the period 1997–2020, the Ramon Carrillo Hospital in Bariloche reported a lethality of 0.5% in surgical patients. Finally, 83.3% of the cases detected by screening performed in 2020 were born before start of Control Program.
4. Discussion
CE is included within the World Health Organization’s list of “Neglected Tropical Diseases”, based on the damage it causes to both the health system and the economy [5]. “One Health” is acknowledged as one of the primary strategies for the control and prevention of diseases, especially those of zoonotic origin, both emerging and reemerging, as well as those linked to the environment; this model involves both interdisciplinary and multidisciplinary handling to minimize damage and maximize the benefits of joint management of the health of humans, animals and ecosystems [7,8,9].
Given that the “One-Health” approach seeks to develop more effective and suitable strategies to address health problems at the human–animal–environment interface, CE presents ideal conditions for its application, since it involves all three of the strategy’s components. In this paper, therefore, we report our experience as an example of what is now called “One Health”, which encompasses the effects of actions on humans, animals and the environment, on an interdisciplinary basis and with an integrative approach to prevention.
It has been pointed out that the optimization of available resources such as individual skills, professional roles and institutions already working on different aspects of the same problems, are usually not coordinated toward specific goals, especially when dealing with neglected zoonoses like CE. Likewise, the need for health education for populations at risk of becoming ill from CE has been identified as a necessary part of any comprehensive control strategy [26,27].
From the outset, in the Rio Negro province, we have worked simultaneously on early detection and treatment in the population, updating technology when it has been accessible to the health system, and consistently performing control actions for the different hosts, with the support of a robust surveillance system and a comprehensive health education program [6,10,11,12,13,14,15,16,17,18,19,20,21].
The strategy contributed to a strong decrease in the prevalence of the disease in the community, even in an inhospitable environment with a highly dispersed rural population and with accessibility to health teams limited by local geographical conditions; in fact, CE was practically eliminated as a cause of death, and its costs to the health system were clearly reduced by the decrease in both hospital stays and the number of surgeries. One particularly important factor in the control of CE is has been support from the community, which has manifested itself in various ways over time: the permission from owners to the administration of arecoline to their dogs, and their deworming of canines with the PZQ delivered by health teams; and the agreement by owners of farms to the vaccination of their flocks, as well as their participation in serological and US screenings.
Cystic Echinococcosis has shown a wide global geographical distribution, and its control has proven difficult for long periods of time, owing to the limitations imposed by geography and health infrastructure on the achievement of widespread deworming with PZQ and vaccination with EG95 [4,5,28]. Island communities, such as New Zealand and Tasmania, are examples of first-generation control programs that were very successful in the eventual elimination of CE as a public health problem and even in the elimination of the parasite in dogs and sheep [4,5,28].
In continental territories, where geographical and infrastructural limitations are greater in relation to those on the islands where first-generation control programs were so successful, achievements have been short-lived (as was the case with Chile and Peru). Over long intervals, political and economic changes tend to occur (especially in developing countries), which hinder the continuity of control programs and the chance to cut transmission of CE to humans in the long term. In this sense, the program carried out in Rio Negro has been one of the few successful control experiences in continental areas [4,28].
5. Conclusions
Coordinated inter-institutional and interdisciplinary actions following the strategic guidelines from Primary Health Care (PHC) and “One Health” have succeeded in reducing the prevalence of CE in the Province of Rio Negro so that, despite the current occurrence of some cases, CE has ceased to be one of the main health problems affecting the Rio Negro population.
Author Contributions
Conceptualization, E.L.; formal analysis, M.A.; investigation, G.M., L.U., D.A., J.C.S., J.L.L., M.S. (Mariano Sobrino), E.H., O.P., G.T., H.T., C.G. and C.H.M.; methodology, P.B. and E.L.; project administration, M.S. (Marcos Seleiman); drafting the manuscript, E.L., G.M., J.C.S., P.B., G.T. and L.U.; critical reading and revision, D.A., J.L.L., M.S. (Mariano Sobrino), M.A., M.S. (Marcos Seleiman), E.H., O.P., H.T. and C.H.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgments
Thanks to Martin Odriozola, Bernardo Frider and Mario del Carpio, to the veterinaries Jorge Alvarez, Amar Thakur, María Teresa Costa, Gustavo Cantoni and to the biochemists Alicia Perez and Frida Vargas for their invaluable contributions during their time with the Control Program and the new generation of general practitioners, surgeons and veterinarians who keep the program going today.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Larrieu, E.; Gavidia, C.M.; Lightowlers, M.W. Control of cystic echinococcosis: Background and prospects. Zoonoses Public Health 2019, 66, 889–899. [Google Scholar] [CrossRef] [PubMed]
- Budke, C.M.; Deplazes, P.; Torgerson, P.R. Global socioeconomic impact of cystic echinococcosis. Emerg. Infect. Dis. 2006, 2, 296–303. [Google Scholar] [CrossRef] [PubMed]
- Eckert, J.; Gemmel, M.A.; Meslin, F.X.; Pawlowski, Z.S. WHO/OIE Manual on Echinococcosis in Humans and Animals: A Public Health Problem of Global Concern; WHO/FAO: Paris, France, 2001; p. 265. [Google Scholar]
- Craig, P.S.; Hegglin, D.; Lightowlers, M.W.; Torgerson, P.R.; Wang, Q. Echinococcosis: Control and Prevention. Adv. Parasitol. 2017, 96, 55–158. [Google Scholar]
- Pavletic, C.F.; Larrieu, E.; Guarnera, E.A.; Casas, N.; Irabedra, P.; Ferreira, C.; Sayes, J.; Gavidia, C.M.; Caldas, E.; Zini Lise, M.; et al. Cystic echinococcosis in America: A call for action. Rev. Panam. Salud Publica 2017, 21, 41–42. [Google Scholar]
- Uchiumi, L.; Mujica, G.; Araya, D.; Salvitti, J.C.; Sobrino, M.; Moguillansky, S.; Solari, A.; Blanco, P.; Barrera, F.; Lamunier, J.; et al. Prevalence of human cystic echinococcosis in the towns of Ñorquinco and Ramos Mexia in Rio Negro Province, Argentina, and direct risk factors for infection. Parasit. Vectors 2021, 19, 262. [Google Scholar] [CrossRef]
- Marcos, E. The One Health Concept as Integrator of the Interface Human-Animal-Environmental, Against Diseases Emerging, Reemerging and Cross-Border. Epidemiol. Salud. 2013, 1, 16–20. [Google Scholar]
- FAO; OIE; OMS. A Tripartite Guide to Addressing Zoonotic Diseases in Countries. 2019. Available online: https://www.oie.int/fileadmin/Home/eng/Media_Center/docs/EN_TripartiteZoonosesGuide_webversion.pdf (accessed on 18 July 2021).
- Laing, G.; Vigilato, M.A.N.; Cleaveland, S.; Thumbi, S.M.; Blumberg, L.; Salahuddin, N.; Abdela-Ridder, B.; Harrison, W. One Health for neglected tropical diseases. Trans. R. Soc. Trop. Med. Hyg. 2021, 28, 182–184. [Google Scholar] [CrossRef]
- Larrieu, E.; Costa, M.T.; Cantoni, G.; Labanchi, J.L.; Bigatti, R.; Pérez, A.; Araya, D.; Mancini, S.; Herrero, M.E.; Talmon, G.; et al. Control program of hydatid disease in the province of Río Negro Argentina 1980–1997. Bol. Chil. Parasitol. 2000, 55, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Larrieu, E.; Uchiumi, L.; Salvitti, J.C.; Sobrino, M.; Panomarenko, O.; Tissot, H.; Mercapide, C.H.; Sustercic, J.; Arezo, M.; Mujica, G.; et al. Epidemiology, diagnosis, treatment and follow up of cystic echinococcosis in asymptomatic carriers. Trans. R. Soc. Trop. Med. Hyg. 2019, 113, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Arezo, M.; Mujica, G.; Uchiumi, L.; Santillán, G.; Herrero, E.; Labanchi, J.L.; Araya, D.; Salvitti, J.C.; Cabrera, M.; Grizmado, C.; et al. Identification of potential ′hot spots′ of cystic echinococcosis transmission in the province of Río Negro, Argentina. Acta Trop. 2020, 204, 105341. [Google Scholar] [CrossRef]
- Vignolo, J.; Vacarezza, M.; Alvarez, C.; Sosa, A. Levels of care, prevention and primary health care. Arch. Med. 2011, 33, 1. [Google Scholar]
- Leavell, H.R.; Clark, E.G. Preventive Medicine for the Doctor in His Community; McGraw-Hill Book Company: New York, NY, USA, 1965. [Google Scholar]
- Larrieu, E.; Mujica, G.; Araya, D.; Labanchi, J.L.; Arezo, M.; Herrero, E.; Santillán, G.; Vizcaychipi, K.; Uchiumi, L.; Salvitti, J.C.; et al. Pilot field trial of the EG95 vaccine against ovine cystic echinococcosis in Rio Negro, Argentina: 8 years of work. Acta Trop. 2019, 191, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Pérez, A.; Costa, M.T.; Cantoni, G.; Mancini, S.; Mercapide, C.; Herrero, E.; Volpe, M.; Araya, D.; Talmon, G.; Chiosso, C.; et al. Epidemiological surveillance of cystic echinococcosis in dogs, sheep farms and humans in the Rio Negro Province. Medicina 2006, 66, 193–200. [Google Scholar] [PubMed]
- Salvitti, J.C.; Sobrino, M.; Del Carpio, M.; Mercapide, C.; Uchiumi, L.; Moguilensky, J.; Moguilansky, S.; Frider, B.; Larrieu, E. Hydatidosis: Ultrasonographyc screening in the Río Negro Province 25 years after the first screening. Acta Gastroenterol. Latamer. 2014, 44, 311–315. [Google Scholar]
- Larrieu, E.; Del Carpio, M.; Mercapide, C.H.; Salvitti, J.C.; Sustercic, J.; Moguilensky, J.; Panomarenko, H.; Uchiumi, L.; Herrero, E.; Talmon, G.; et al. Programme for ultrasound diagnoses and treatment with albendazole of cystic echinococcosis in asymptomatic carriers: 10 years of follow-up of cases. Acta Trop. 2011, 117, 1–5. [Google Scholar] [CrossRef]
- Del Carpio, M.; Mercapide, C.H.; Salvitti, J.C.; Uchiumi, L.; Sustercic, J.; Panomarenko, H.; Moguilensky, J.; Herrero, E.; Talmon, G.; Volpe, M.; et al. Early diagnosis, treatment and follow-up of cystic echinococcosis in remote rural areas in Patagonia: Impact of ultrasound training of non-specialists with a focused approach on CE. PLoS. Neg. Trop. Dis. 2011, 6, e1444. [Google Scholar] [CrossRef]
- Mercapide, C.H.; Pereyra, R.; Giménez, R.; Pérez, C.; Michelena, F. Tránsitos hidatídicos abdomino torácicos. Prensa Med. Argent. 1993, 80, 300–306. [Google Scholar]
- Mercapide, C.H.; Gimenez, R.; Pereyra, R.; Perez, C.; Michelena, F. Tratamiento de la hidatidosis hepática. Prensa Med. Argent. 1994, 81, 275–281. [Google Scholar]
- Brunett, E.; Garcia, H.H.; Junghanss, T. Cystic echinococcosis: Chronic, complex, and still neglected. PLoS. Negl. Trop. Dis. 2011, 5, e1146. [Google Scholar] [CrossRef] [Green Version]
- Larrieu, E.; Frider, B.; del Carpio, M.; Salvitti, J.C.; Mercapide, C.; Pereyra, R.; Costa, M.; Odriozola, M.; Pérez, A.; Cantoni, G.; et al. Asymptomatic carriers of hydatidosis: Epidemiology, diagnosis, and treatment. Rev. Panam. Salud Publ. 2000, 8, 250–256. [Google Scholar] [CrossRef] [Green Version]
- Larrieu, E.; Costa, M.T.; Cantoni, G.; Alvarez, J.; Pérez, A.; Giménez, N.; Giménez, R.; Odriozzola, M. Control of hydatidosis in the Province of Rio Negro, Argentina: Epidemiology. Bol. Chil. Parasitol. 1991, 46, 3–7. [Google Scholar]
- Bingham, G.M.; Larrieu, E.; Uchiumi, L.; Mercapide, C.H.; Mujica, G.; Del Carpio, M.; Hererro, E.; Salvitti, J.C.; Norby, B.; Budke, C.M. The Economic Impact of Cystic Echinococcosis in Rio Negro Province, Argentina. Am. J. Trop. Med. Hyg. 2016, 94, 615–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canali, M.; Aragrande, M.; Angheben, A.M.; Capelli, G.; Drigo, M.; Gobbi, F.; Tamarozzi, F.; Cassini, R. Epidemiologic-economic models and the One Health paradigm: Echinococcosis and leishmaniasis, case studies in Veneto region, Northeastern Italy. One Health 2019, 27, 100115. [Google Scholar] [CrossRef] [PubMed]
- Abdulhameed, M.F.; Robertson, I.D.; Al-Azizz, S.A.; Habib, I. Neglected Zoonoses and the Missing Opportunities for One Health Education: The Case of Cystic Echinococcosis among Surgically Operated Patients in Basrah, Southern Iraq. Diseases 2019, 7, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larrieu, E.; Zanini, F. Critical analysis of the strategies to control cystic echinococcosis and the use of praziquantel in South America: 1980–2009. Rev. Panam. Salud Publica 2012, 31, 73–81. [Google Scholar]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).