1. Introduction
Physical inactivity in children and adolescents is a major public health challenge. Recent studies have associated more time in children’s sedentary behavior with lower health-related quality of life [
1] and poorer mental health outcomes [
2]. Furthermore, the recent COVID-19 outbreak forced children around the globe to change their lifestyle, due to social distancing measures, and caused an increase in physical inactivity [
3,
4]. It is known that regular physical activity may increase life expectancy and play an important role towards the prevention of chronic conditions such as obesity, cardiovascular diseases, and metabolic syndrome [
5], and it has unarguable benefits for the health of children [
6]. In this context, interventions and policies to promote physical activity in children are required, which have to rely on valid tools and methods for the physical activity assessment of young populations.
During the last years, the development of wearable devices, such as pedometers and wristband activity trackers based on accelerometer recordings, has enabled the reliable assessment of the duration and level of physical activity [
7,
8]. Those tools can be an important component of interventions for physical activity enhancement. However, the cost of wearable devices, factors such as comfort and usability, and issues related to data extraction, processing, and protection may impose significant barriers for their wide adoption by children and their carers [
9,
10].
Self-reporting tools provide a cheap and convenient way to assess or estimate physical activity in large populations. The Physical Activity Questionnaire for Children (PAQ-C) constitutes one of the most widely used self-reporting instruments in sport epidemiology studies for school populations [
11,
12]. The PAQ-C is a simple self-administered questionnaire based on nine items to estimate the general level of physical activity during the last 7 days, aimed for children between 8 and 14 years of age. The total score in the PAQ-C provides a summary physical activity score derived from the nine items, each scored on a 5-point scale. The first item is an activity checklist consisting of common sports, leisure activities and games, plus room for other activities. Six items assess activity in physical education classes, recess, lunch, right after school, in the evenings, and on the weekend. One item asks which statement “describes you best for the last 7 days”, with five statements describing low activity to very high activity levels. Finally, one question asks the child to indicate how often he or she did physical activity for each day of the week. A limitation of the PAQ-C is that, in contrast with wearable activity trackers, it cannot provide exact day-to-day frequency, intensity, and time information about physical activity levels [
13].
The validity of the PAQ-C in comparison with accelerometer-based devices for assessing physical activity in children has been explored in several studies, with some demonstrating moderate correlation [
11,
12,
13] and others weaker correlation outcomes [
14,
15,
16]. Furthermore, a recent meta-analysis of studies has shown moderate relationship between the PAQ-C and accelerometer measures [
17]. However, the studies conducted to assess the reliability and validity of the PAQ-C so far have mostly relied on samples of wide age ranges and have not considered a child’s age as a possible affecting factor. It is well-known that the accuracy of recall is critical for the validity of self-reporting tools [
18], and younger children in particular may face challenges in recalling the duration, frequency, and level of their physical activity.
Although several studies have shown the reliability and validity of the PAQ-C for children, there has been a scarcity in studies comparing PAQ-C agreement with wearable accelerometer-based devices in young versus older children. To this end, this study aims to improve our knowledge on whether the age of children is a crucial factor which care practitioners and researchers should take into account when assessing physical activity through self-reporting tools.
2. Materials and Methods
2.1. Participants
This was a cross-sectional study. Data collection was conducted in two rounds with independent samples. An invitation was sent to a convenient sample of parents whose children attended the 3rd or 7th grade. During the first round, 99 9-year-old children attending the 3rd grade were recruited, while during the second round, 62 12-year-olds attending the 7th grade agreed to participate in the study with their parents’ approval. The study took place in a private school in Athens (primary and secondary school), Greece, between January and April 2019. Consent forms were signed by parents prior to their children’s participation, providing detailed information about the aims and procedures of the study. The study was approved by the Ethics Committee of the Democritus University of Thrace (approval number 4/33/2018).
2.2. Instruments and Procedure
Objective measures of physical activity were obtained through the Fitbit Flex 2 (FF-2) wearable physical activity tracker (Fitbit Inc, San Francisco, CA, USA), which is based on accelerometer recordings and worn on the wrist. Data obtained through the FF-2 for this study included daily steps and active minutes in terms of moderate-to-vigorous physical activity (MVPA), which are considered to be common measures to assess the level and intensity of physical activity according to guidelines [
5]. The validity of the FF-2 device in those physical activity measures has been shown in previous studies [
19,
20]. The FF-2 provided additional data such as sleep duration, sedentary minutes, and calories burned, which were not used in the study.
Children were instructed to wear the physical activity tracker on their dominant arm for 7 consecutive days on a 24-h basis. This had been a methodological strength of this study, since in most previous studies, children were advised to remove the device when sleeping or engaging in water-based activities (whereas there was not such a need for the FF-2 which is waterproof) [
14,
21]. Children were instructed to charge their devices overnight in case the battery was close to running out.
Physical activity was assessed through the PAQ-C tool after the 7-day period wearing the physical activity tracker. In the school environment, members of the research team asked children to recall as accurately as they could the duration, type, and frequency of physical activities performed during the last 7 days, and their answers were filled on hard copies of the translated PAQ-C questionnaire.
Anonymous collected data was analysed using Python ver. 3.6 scripts (Python Software Foundation, Wilmington, DE, USA) and the Statsmodels package, as well as other scientific toolkits (NumPy, Pandas, SciPy). We performed a reliability analysis of the PAQ-C questionnaire through exploring its internal consistency by the Cronbach’s α coefficient. The Spearman’s rank correlation coefficient was used for correlation analysis in self-reported items and steps, MVPA, or total Physical Activity (PA) derived from the FF-2. Level of significance was set at
p < 0.05. Bland–Altman plots were also used to identify the agreement between FF-2 recordings and PAQ-C answers, by calculating the mean and the standard deviation (SD) of the differences between the two measurements. In terms of preprocessing, we removed from the datasets all recordings in which a step count (as recorded by the FF-2) of below 500 steps/day was present, along with zero and NA values. We considered such recordings of having no significant value (e.g., the child might have not worn the FF-2 device the whole day or the device malfunctioned), in accordance with other studies [
22]. In case a participant had two or more days with less than 500 steps, he/she was removed from the analysis. Participants who did not complete one or more items of the PAQ-C questionnaire were also not included in the analysis.
3. Results
Characteristics of the included participants in the analysis, after removal of subjects with missing data in the PAQ-C questionnaire or lack of FF-2 recordings (as explained above), are shown in
Table 1. In total, 131 children, 79 9-year-old children (3rd graders) and 52 12-year-old children (7th graders) were included. A total of 43 3rd graders were girls (54%) and 36 were boys (46%), whereas 31 7th graders were girls (60%), and 21 children (40%) were boys. Eight 3rd graders and 14 7th graders were overweight or obese, in terms of body mass index (BMI) exceeding the 85th percentile adjusted for age and sex. Significant differences for total PAQ-C score between the two age groups (3rd graders vs. 7th graders) were not found (boys: 2.40 ± 0.41 vs. 2.46 ± 0.28, girls: 2.28 ± 0.46 vs. 2.18 ± 0.39). There were also no significant differences in MVPA as measured by accelerometer between the two age groups (boys: 61.51 ± 30.98 vs. 61.61 ± 29.48, girls: 23.31 ± 13.14 vs. 22.74 ± 14.64), however boys were found to be much more active than girls of the same age group (both in terms of MVPA and steps/day).
In
Table 2, the internal consistency coefficients of the PAQ-C questionnaire are shown. A total consistency of 0.74 in terms of Cronbach’s α coefficient was obtained. After removing each item of the questionnaire, the consistency was reduced, except for the case of item 3, related to activity at recess (In the last 7 days, what did you do most of the time at recess?). Internal consistency of the PAQ-C was higher for the 9-year-old children compared to the 12-year-old children (0.79 vs. 0.64).
Table 3 shows the Spearman’s rank correlation coefficient between the answers to the PAQ-C questionnaire and physical activity measures obtained from the accelerometer. The highest correlation coefficient in the total population with statistical significance set at
p < 0.01 was detected for item 3 of the PAQ-C (rho = 0.34 for total physical activity (PA), rho = 0.30 for MVPA, rho = 0.44 for steps) and the total PAQ-C score (rho = 0.23 for total PA, rho = 0.30 for MVPA, rho = 0.30 for steps).
A subgroup correlation analysis for the 9-year-old and the 12-year-old children showed that the total PAQ-C score was highly correlated with the physical activity measures of the 12-year-old children (rho = 0.47 for total PA, rho = 0.43 for MVPA, rho = 0.41 for steps, all p < 0.01), but not those of the 9-year-old children (rho = 0.08 for total PA, rho = 0.21 for MVPA, rho = 0.19 for steps, all p > 0.05). The highest correlation coefficient between PAQ-C items and physical activity measures in 9-year-old children was detected for item 3 (rho = 0.25 for MVPA, rho = 0.26 for steps, all p < 0.05), followed by item 7 (rho = 0.24 for MVPA, p < 0.05), whereas in 12-year-old children, items showing the highest correlation were item 9 (rho = 0.46 for total PA, rho = 0.36 for MVPA, rho = 0.39 for steps, all p < 0.01), item 8 (rho = 0.37 for total PA, rho = 0.47 for MVPA, rho = 0.41 for steps, all p < 0.01), item 3 (rho = 0.31, p < 0.05 for total PA, rho = 0.48, p < 0.01 for MVPA, rho = 0.38, p < 0.01 for steps), and item 7 (rho = 0.34, p < 0.05 for total PA, and rho = 0.39, p < 0.01 for MVPA).
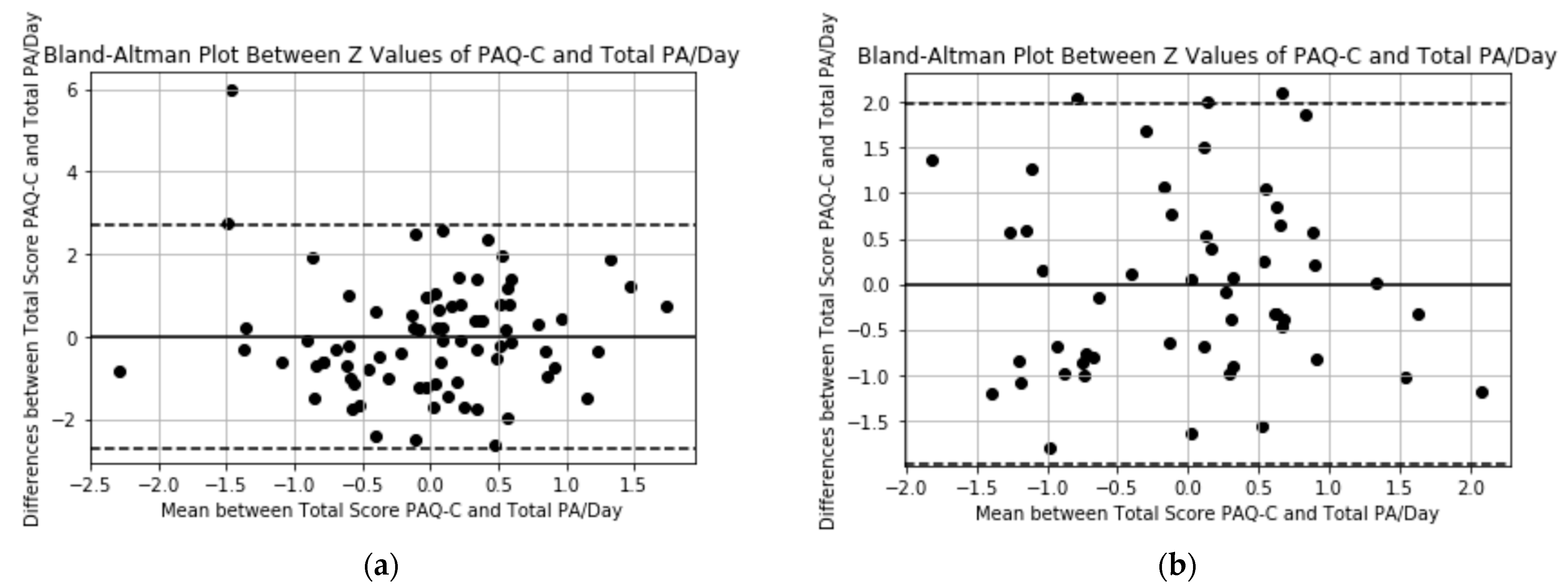
Visual data inspection with Bland–Altman plots in
Figure 1 shows that although the line for mean difference between Z values of total PAQ-C score and total PA is close to zero for both 9-year-old and 12-year-old children, the limits of agreement (mean ± 1.96 × SD) are wider for 9-year-old children (±2.695 vs. ± 1.972).
4. Discussion
A study was conducted to compare self-reported with accelerometer-measured physical activity in young (9 year old) versus older (12 year old) children, thereby taking a different angle from previous studies which did not consider differentiating age as possible affecting factor in such a comparison. Overall reliability of the PAQ-C questionnaire for physical activity assessment in children was found to be satisfactory (Cronbach α score for total target population > 0.7). Our main finding is that the total PAQ-C score was not in agreement with any of the physical activity measures derived from a worn accelerometer (total PA, MVPA, steps) in 9-year-old children, as opposed to 12-year-old children. Further studies with larger sample sizes would be needed to confirm this finding, given the wide adoption of the PAQ-C for assessing physical activity.
The results of this study suggest that when the PAQ-C is administered to younger children, the outcomes of their physical activity assessment should be treated with caution. Recalling physical activity during the past 7 days is indeed a complex cognitive task which requires abstract thinking and detailed recall [
18], and younger children might overestimate or underestimate their physical activity, which might explain the lack of correlation between the measures from the questionnaire and the wearable device. Further longer-term studies with more participants, as well as qualitative studies exploring the recall, reading, and questionnaire-understanding abilities of younger populations are needed to confirm those findings.
Administering physical activity questionnaires is easy, inexpensive, and may be the only available data collection method for assessing physical activity in young populations. The PAQ-C questionnaire has been widely adopted for such a purpose and used even by children being younger than 9 years old [
23,
24]. Nevertheless, our findings concerning the use of the PAQ-C in comparison with accelerometer-based measurements by 9-year-olds suggest that health practitioners should pay attention when interpreting such subjective self-reporting information based on a child’s recall. Instead, wearable devices and objective physical activity measures derived from them should be preferred by researchers and health practitioners, especially in younger populations, due to their more accurate physical activity assessment.
With the above in mind, the employment of wearable devices would enable to realize the development of reliable and unobtrusive computerized systems and digital health interventions for children and their carers, and overcome the potential inaccuracy of children’s self-reports. Such an approach can be a step towards acquiring optimal physical activity outcomes through longitudinal physical activity monitoring, assessment, and coaching [
25].
Limitations
A commercial consumer accelerometer-based device, i.e., the FF-2, which has been largely used in several physical activity studies [
26,
27], was adopted. There have been studies showing that the FF-2 is accurate and reliable in assessing physical activity [
19], demonstrating high agreement in steps with a research grade accelerometer such as Actigraph [
28]. However, other studies have shown that the FF-2 has moderate validity [
29,
30]. Test–retest reliability was not explored in this study due to constraints in providing the PAQ-C twice to students within the school environment. The results of this research refer to 9 and 12-year-old students of one school, and therefore the generalizability of our findings is limited.
5. Conclusions
Physical activity assessment through valid and reliable tools is first and foremost required towards the development of interventions for physical activity enhancement in children. The scarcity of studies exploring the agreement between questionnaire-based measures and wearable accelerometer-based devices for the physical activity assessment of young versus older children was the main motivation for the conduction of the current study. The study showed that a well-known self-reporting tool for physical activity assessment, i.e., the PAQ-C, was not in agreement with accelerometer recordings for 9-year-old children. On the contrary, the PAQ-C score of 12-year-old children in the same study showed high correlation with physical activity measures obtained from the accelerometer. In this context, outcomes of physical activity assessment in young populations through the use of the PAQ-C should be treated with caution. Rigorous studies with larger samples should further investigate this finding, and provide more robust evidence.
Author Contributions
Conceptualization, A.T.; methodology, A.T., A.A., K.S. and T.F.; software, A.A.; validation, A.T. and A.A.; formal analysis, A.T. and A.A.; investigation, A.T.; resources, K.S. and T.F.; data curation, K.S. and T.F.; writing—original draft preparation, A.T.; writing—review and editing, A.T., A.A., K.S., T.F., K.V. and D.T.; visualization, A.T.; supervision, K.V.; project administration, K.V. and D.T.; funding acquisition, K.V. and D.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the European Union‘s HORIZON 2020 Programme (2014–2020), under ID n° 777082, and from the Brazilian Ministry of Science, Technology and Innovation through Rede Nacional de Ensino e Pesquisa (RNP) under Ocariot.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Department of Physical Education & Sport Sciences, Democritus University of Thrace (approval number 4/33/2018).
Informed Consent Statement
All subjects and their parents gave their informed consent for inclusion before they participated in the study.
Data Availability Statement
The data presented in this study are available upon reasonable request to the authors, with the permission of Democritus University of Thrace.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- Wu, X.Y.; Han, L.H.; Zhang, J.H.; Luo, S.; Hu, J.W.; Sun, K. The influence of physical activity, sedentary behavior on health-related quality of life among the general population of children and adolescents: A systematic review. PLoS ONE 2017, 12, e0187668. [Google Scholar] [CrossRef]
- Rodriguez-Ayllon, M.; Cadenas-Sánchez, C.; Estévez-López, F.; Muñoz, N.E.; Mora-Gonzalez, J.; Migueles, J.H.; Molina-García, P.; Henriksson, H.; Mena-Molina, A.; Martínez-Vizcaíno, V.; et al. Role of physical activity and sedentary behavior in the mental health of preschoolers, children and adolescents: A systematic review and meta-analysis. Sports Med. 2019, 49, 1383–1410. [Google Scholar] [CrossRef]
- Bates, L.; Zieff, G.; Stanford, K.; Moore, J.; Kerr, Z.; Hanson, E.; Gibbs, B.B.; Kline, C.; Stoner, L. COVID-19 impact on behaviors across the 24-hour day in children and adolescents: Physical activity, sedentary behavior, and sleep. Children 2020, 7, 138. [Google Scholar] [CrossRef]
- López-Gil, J.; Tremblay, M.; Brazo-Sayavera, J. Changes in healthy behaviors and meeting 24-h movement guidelines in Spanish and Brazilian preschoolers, children and adolescents during the COVID-19 lockdown. Children 2021, 8, 83. [Google Scholar] [CrossRef]
- Physical Activity Guidelines Advisory Committee. Physical Activity Guidelines Advisory Committee Report; US Department of Health and Human Services: Washington, DC, USA, 2008.
- Tudor-Locke, C.; Craig, C.L.; Beets, M.W.; Belton, S.; Cardon, G.M.; Duncan, S.; Hatano, Y.; Lubans, D.R.; Olds, T.S.; Raustorp, A.; et al. How many steps/day are enough? For children and adolescents. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 78. [Google Scholar] [CrossRef]
- Poitras, V.J.; Gray, C.E.; Borghese, M.M.; Carson, V.; Chaput, J.-P.; Janssen, I.; Katzmarzyk, P.T.; Pate, R.R.; Gorber, S.C.; Kho, M.E.; et al. Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Appl. Physiol. Nutr. Metab. 2016, 41, S197–S239. [Google Scholar] [CrossRef]
- Colley, R.C.; Garriguet, D.; Janssen, I.; Craig, C.L.; Clarke, J.; Tremblay, M.S. Physical activity of Canadian children and youth: Accelerometer results from the 2007 to 2009 Canadian Health Measures Survey. Health Rep. 2011, 22, 1. [Google Scholar]
- Harrison, D.; Marshall, P.; Bianchi-Berthouze, N.; Bird, J. Activity tracking: Barriers, workarounds and customisation. In Proceedings of the UbiComp 2015—Proceedings of the 2015 ACM International Joint Conference on Pervasive and Ubiquitous Computing, Osaka, Japan, 7–11 September 2015; pp. 617–621. [Google Scholar] [CrossRef]
- Meyer, J.; Fortmann, J.; Wasmann, M.; Heuten, W. Making Lifelogging Usable: Design Guidelines for Activity Trackers; Springer: Berlin/Heidelberg, Germany, 2015; pp. 323–334. [Google Scholar] [CrossRef]
- Voss, C.; Dean, P.H.; Gardner, R.F.; Duncombe, S.L.; Harris, K.C. Validity and reliability of the Physical Activity Questionnaire for Children (PAQ-C) and Adolescents (PAQ-A) in individuals with congenital heart disease. PLoS ONE 2017, 12, e0175806. [Google Scholar] [CrossRef]
- Wang, J.J.; Baranowski, T.; Lau, W.P.; Chen, T.A.; Pitkethly, A.J. Validation of the Physical Activity Questionnaire for Older Children (PAQ-C) among Chinese children. Biomed. Environ. Sci. 2016, 29, 177–186. [Google Scholar]
- Kowalski, K.C.; Crocker, P.R.; Faulkner, R.A. Validation of the Physical Activity Questionnaire for Older Children. Pediatr. Exerc. Sci. 1997, 9, 174–186. [Google Scholar] [CrossRef]
- Benítez-Porres, J.; López-Fernández, I.; Raya, J.F.; Carnero, S.Á.; Alvero-Cruz, J.R.; Carnero, Á.E. Reliability and validity of the PAQ-C Questionnaire to assess physical activity in children. J. Sch. Health 2016, 86, 677–685. [Google Scholar] [CrossRef]
- Cuberek, R.; Janíková, M.; Dygrýn, J. Adaptation and validation of the Physical Activity Questionnaire for older children (PAQ-C) among Czech children. PLoS ONE 2021, 16, e0245256. [Google Scholar] [CrossRef] [PubMed]
- Ben Jemaa, H.; Mankaï, A.; Mahjoub, F.; Kortobi, B.; Khlifi, S.; Draoui, J.; Minaoui, R.; Karmous, I.; Ben Hmad, H.; Ben Slama, F.; et al. Physical activity level assessed by accelerometer and PAQ-C in Tunisian Children. Ann. Nutr. Metab. 2018, 73, 234–240. [Google Scholar] [CrossRef] [PubMed]
- Marasso, D.; Lupo, C.; Collura, S.; Rainoldi, A.; Brustio, P. Subjective versus Objective measure of physical activity: A systematic review and meta-analysis of the convergent validity of the Physical Activity Questionnaire for Children (PAQ-C). Int. J. Environ. Res. Public Health 2021, 18, 3413. [Google Scholar] [CrossRef] [PubMed]
- Chinapaw, M.J.M.; Mokkink, L.B.; Van Poppel, M.N.M.; Van Mechelen, W.; Terwee, C.B. Physical activity questionnaires for youth: A systematic review of measurement properties. Sport Med. 2010, 40, 539–563. [Google Scholar] [CrossRef]
- Diaz, K.M.; Krupka, D.J.; Chang, M.J.; Peacock, J.; Ma, Y.; Goldsmith, J.; Schwartz, J.E.; Davidson, K.W. Fitbit®: An accurate and reliable device for wireless physical activity tracking. Int. J. Cardiol. 2015, 185, 138–140. [Google Scholar] [CrossRef]
- Imboden, M.T.; Nelson, M.B.; Kaminsky, L.A.; Montoye, A.H. Comparison of four Fitbit and Jawbone activity monitors with a research-grade ActiGraph accelerometer for estimating physical activity and energy expenditure. Br. J. Sports Med. 2018, 52, 844–850. [Google Scholar] [CrossRef]
- Manios, Y.; Androutsos, O.; Moschonis, G.; Birbilis, M.; Maragkopoulou, K.; Giannopoulou, A.; Argyri, E.; Kourlaba, G. Criterion validity of the Physical Activity Questionnaire for Schoolchildren (PAQ-S) in assessing physical activity levels: The Healthy Growth Study. J. Sports Med. Phys. Fit. 2013, 53, 502–508. [Google Scholar]
- Wood, E.; Yang, Q.; Steinberg, D.; Barnes, A.; Vaughn, J.; Vorderstrasse, A.; Crowley, M.; Henriquez, C.; Streicher, M.; Blue, D.B.; et al. Diabetes mobile care: Aggregating and visualizing data from multiple mobile health technologies. AMIA Jt. Summits Transl. Sci. 2019, 2019, 202–211. [Google Scholar]
- Karppanen, A.-K.; Ahonen, S.-M.; Tammelin, T.; Vanhala, M.; Korpelainen, R. Physical activity and fitness in 8-year-old overweight and normal weight children and their parents. Int. J. Circ. Health 2012, 71, 17621. [Google Scholar] [CrossRef][Green Version]
- Dutra, G.F.; Kaufmann, C.C.; Pretto, A.D.B.; Albernaz, E.P. Television viewing habits and their influence on physical activity and childhood overweight. J. Pediatr. 2015, 91, 346–351. [Google Scholar] [CrossRef] [PubMed]
- Triantafyllidis, A.; Filos, D.; Claes, J.; Buys, R.; Cornelissen, V.; Kouidi, E.; Chouvarda, I.; Maglaveras, N. Computerised decision support in physical activity interventions: A systematic literature review. Int. J. Med. Inform. 2018, 111, 7–16. [Google Scholar] [CrossRef]
- Yoon, S.; Schwartz, J.E.; Burg, M.M.; Kronish, I.M.; Alcantara, C.; Julian, J.; Parsons, F.; Davidson, K.W.; Diaz, K.M. Using behavioral analytics to increase exercise: A randomized N-of-1 study. Am. J. Prev. Med. 2018, 54, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Mendoza, J.A.; Baker, K.S.; Moreno, M.A.; Whitlock, K.; Abbey-Lambertz, M.; Waite, A.; Colburn, T.; Chow, E.J. A Fitbit and Facebook mHealth intervention for promoting physical activity among adolescent and young adult childhood cancer survivors: A pilot study. Pediatr. Blood Cancer 2017, 64, e26660. [Google Scholar] [CrossRef] [PubMed]
- Chu, A.H.Y.; Ng, S.H.X.; Paknezhad, M.; Gauterin, A.; Koh, D.; Brown, M.S.; Müller-Riemenschneider, F. Comparison of wrist-worn Fitbit Flex and waist-worn ActiGraph for measuring steps in free-living adults. PLoS ONE 2017, 12, e0172535. [Google Scholar] [CrossRef] [PubMed]
- Sushames, A.; Edwards, A.; Thompson, F.; McDermott, R.; Gebel, K. Validity and reliability of Fitbit Flex for step count, moderate to vigorous physical activity and activity energy expenditure. PLoS ONE 2016, 11, e0161224. [Google Scholar] [CrossRef]
- Reid, R.E.; Insogna, J.A.; Carver, T.E.; Comptour, A.M.; Bewski, N.A.; Sciortino, C.; Andersen, R.E. Validity and reliability of Fitbit activity monitors compared to ActiGraph GT3X+ with female adults in a free-living environment. J. Sci. Med. Sport 2017, 20, 578–582. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).



 and
and 

{kind=link}