1. Introduction
Coagulation is a factor activation cascade process that results in the formation of a blood clot. It takes place both during hemostasis, the natural cessation of blood loss after a vessel is damaged, as well as in pathological thrombosis, where a thrombus forms inside a vessel [
1,
2]. Pathological thrombosis can lead to several major acute and chronic conditions including venous thromboembolism, cerebral stroke, myocardial infarction, pulmonary embolism, and necrosis, among others [
3]. Different coagulation assays are commonly used to monitor and diagnose these conditions.
Assessing the coagulation status of blood is also critical for managing the blood condition during a variety of clinical procedures. These include cardiovascular surgeries requiring cardiopulmonary bypass (CPB), major surgeries in patients with coagulation disorders, extracorporeal life support (ECLS, ECMO), catheter-based interventional procedures, and hemodialysis, among others [
4]. In these situations, a fast assessment of the coagulation status of blood is highly desirable.
The current state of the art in coagulation monitoring relies on provocative, end-point, non-physiologic in vitro tests, where clot formation is induced using external stimuli such as kaolin, glass beads, or calcium [
5]. These clot-based tests can be performed on whole blood, e.g., activated clotting time (ACT) and thromboelastography (TEG) or on citrated plasma, e.g., prothrombin time (PT) and activated partial thromboplastin time (aPTT). In general, they are time-consuming because of the sample preparation requirements and the need for full coagulation to occur before global features of the coagulation process are determined. In some cases, chromogenic coagulation assays are also used to measure the activity of specific single factors [
6,
7]. Ultimately, the choice of a coagulation test is determined by both the level of detail desired and the other particular constraints of the measurement situation [
5,
8].
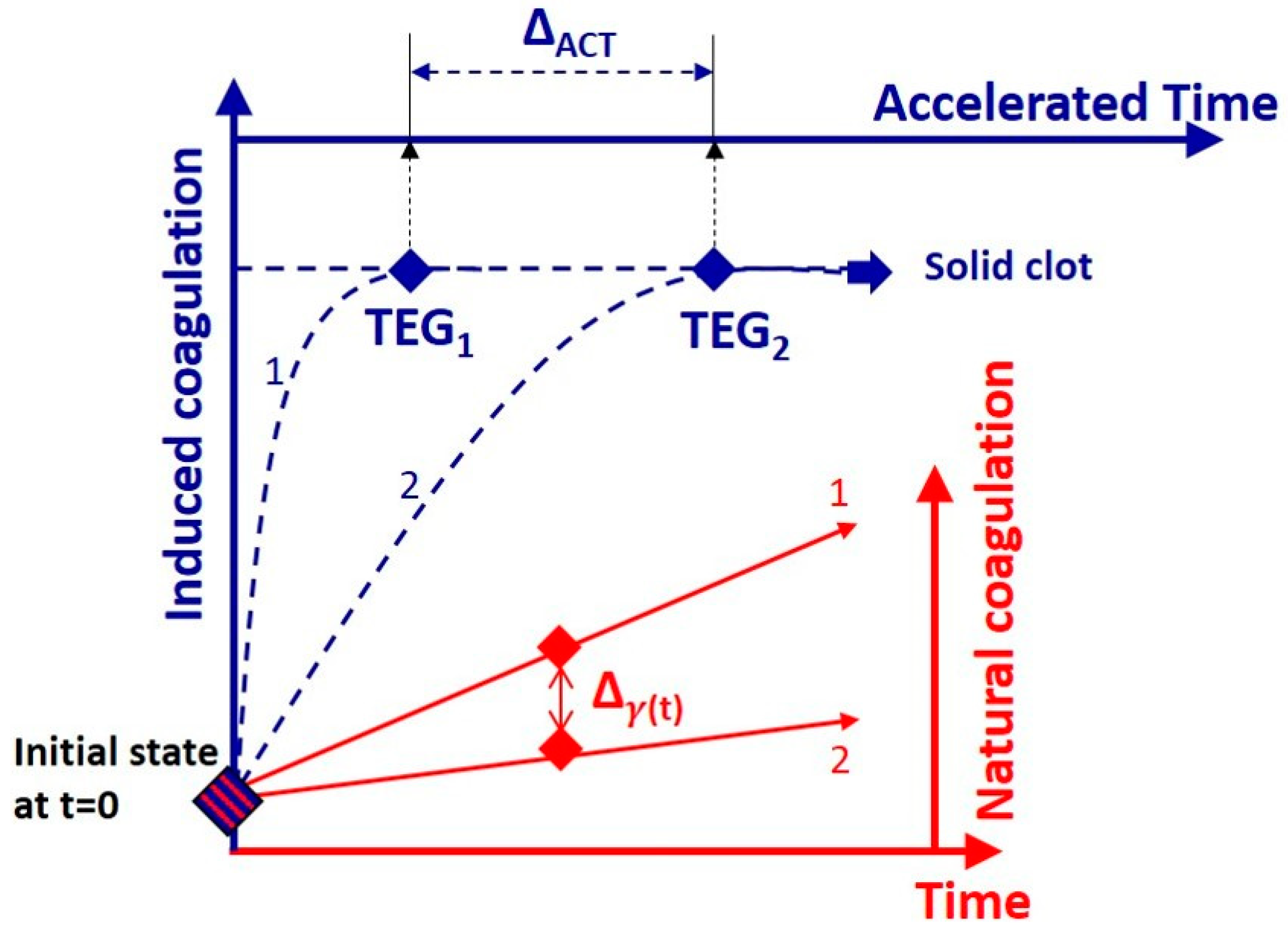
Due to its simplicity, ACT is one of the gold standards in point-of-care testing (POCT). The small volume of blood required and the minimal sample handling makes it useful in various clinical settings involving the administration of anticoagulants where the analytical range of other tests, such as aPTT and anti-Xa, is exceeded. The ACT test is an end-point measurement of the time it takes for whole blood to clot after an activator is administered, starting from a liquid state [
9]. During the assay, after an activator is introduced, the coagulation process evolves under “accelerated” conditions and the propensity of blood to coagulate in its initial state (coagulability) is then associated with the time necessary for the sample to clot.
Thromboelastrometry and thromboelastography provide a more detailed evaluation of the dynamic properties of whole blood during coagulation, and are used in POCT. TEG relies on the rotation of a pin submerged in an oscillating cup of blood to determine the global viscoelastic properties and the clot strength [
10]. Frequently, this measurement is also performed under “accelerated” conditions by using coagulation activators in order to reduce the duration of the measurement down to reasonable time frames [
11,
12,
13]. The process of clot formation is described by four parameters: the reaction time (
) for fibrin polymer generation (initiation stage), the coagulation time (
) taken to achieve a certain level of clot strength (amplification stage), the angle (
) which measures the speed at which fibrin builds up and cross-linking occurs (propagation phase), and the maximum amplitude (
) representing the ultimate clot strength (end of the coagulation stage). Using instrument-specific coefficients, these four parameters can also be linearly combined into a so-called coagulation index (
) [
10].
Recently, we demonstrated a new way to monitor the blood conditions without relying on induced coagulation. The Low-Coherence Dynamic Light Scattering (LC-DLS) technique provides real-time information about the blood status as determined by its microscopic viscoelastic properties. This is in contrast to ACT and TEG assays that rely on examining the coagulation process until a solid clot is formed. A pilot study on ten patients has indicated that (i) the LC-DLS technique has the necessary sensitivity to discriminate between different conditions of blood coagulability and (ii) the information retrieved significantly correlates with ACT [
14].
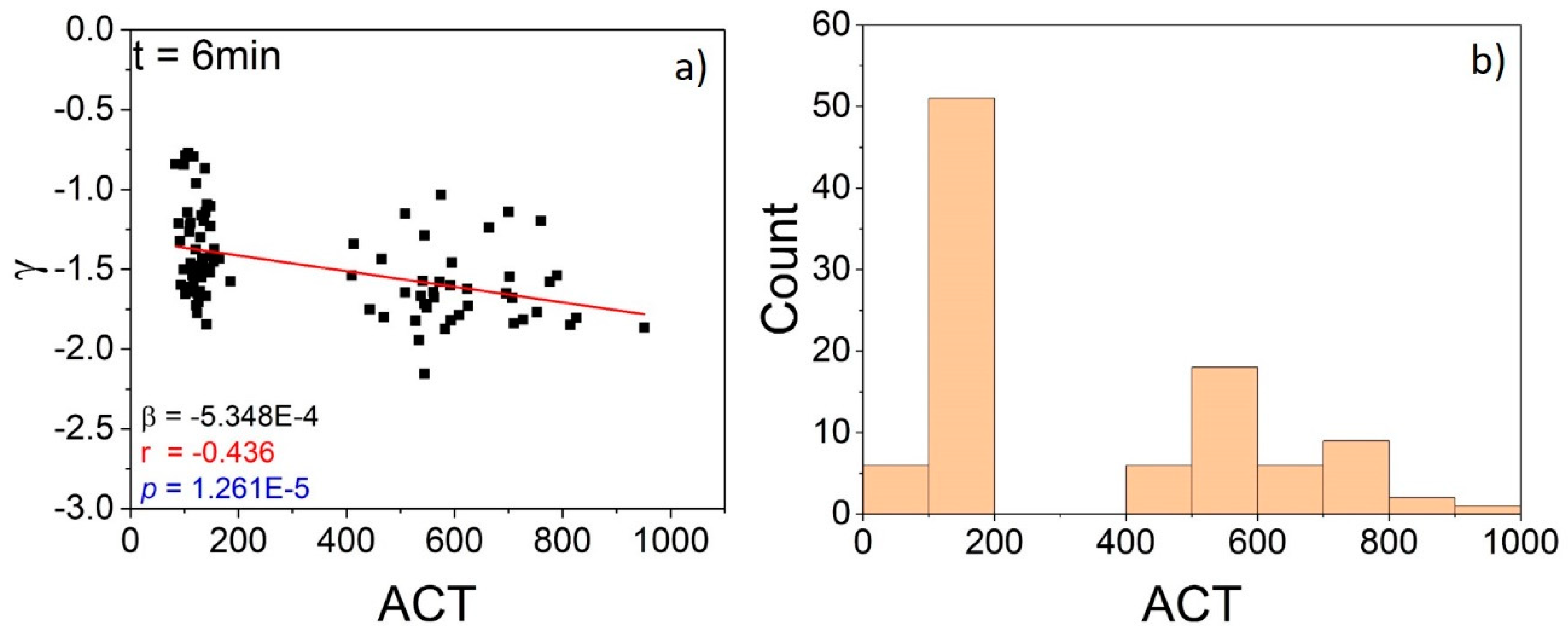
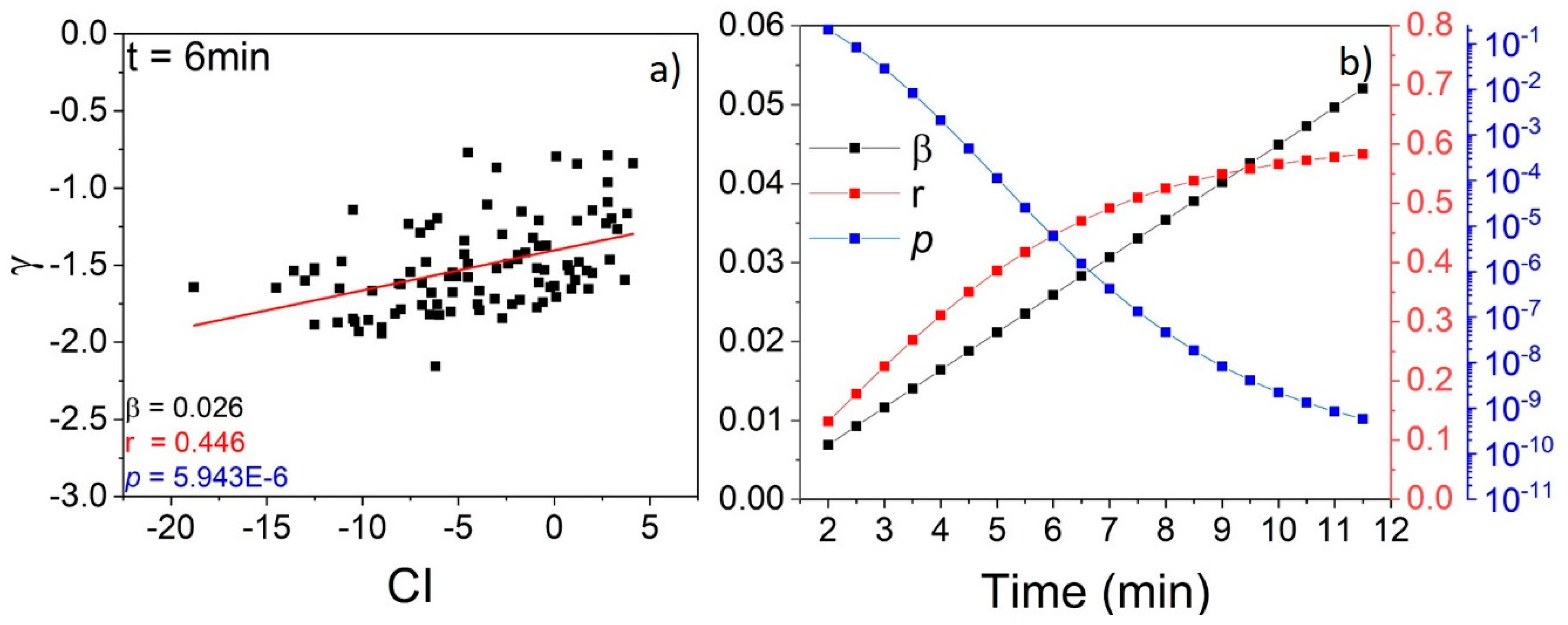
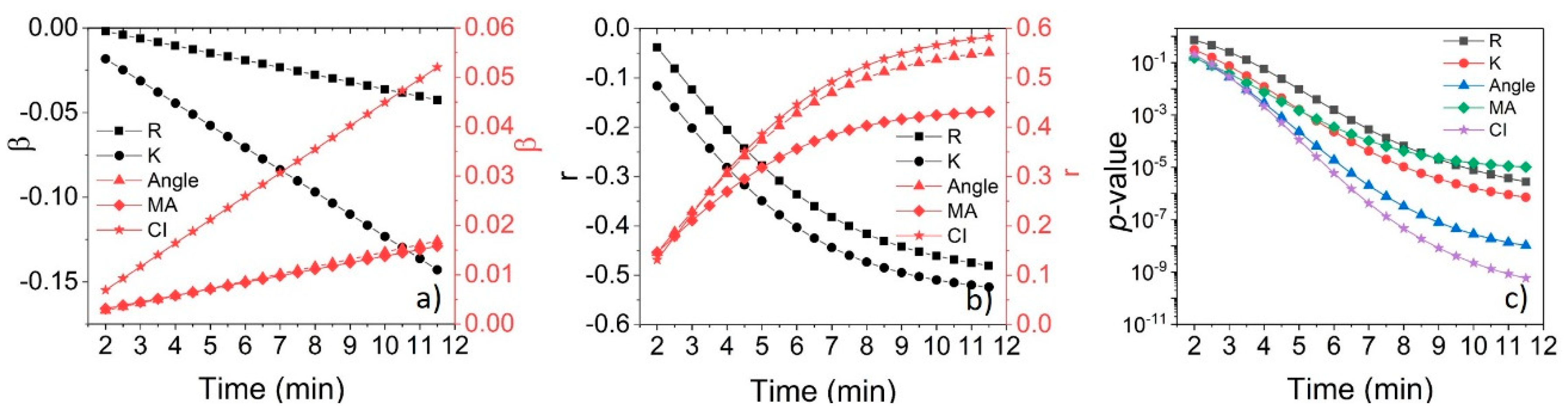
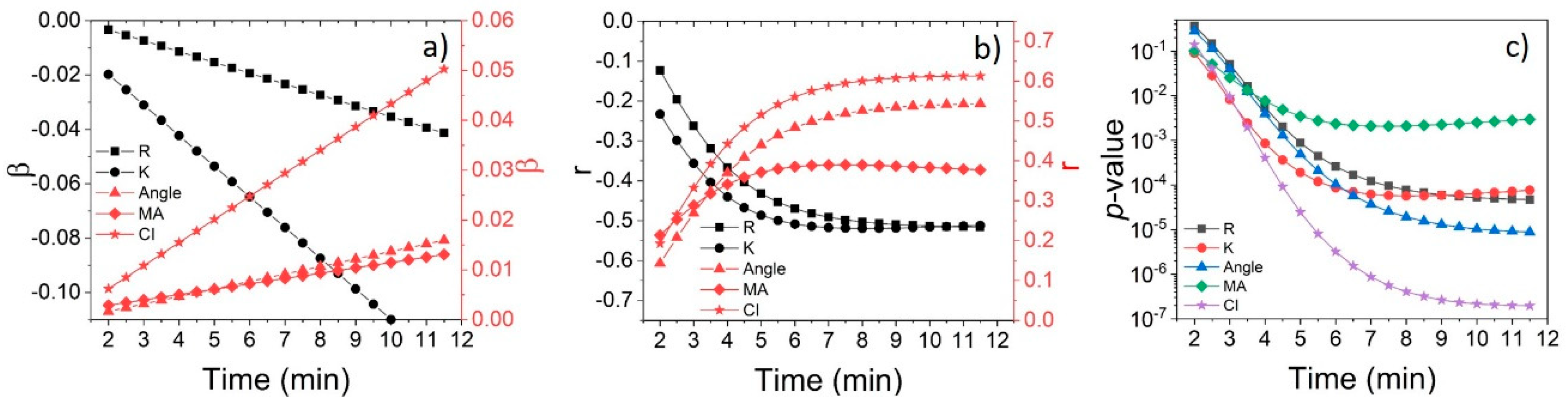
Here we extend the LC-DLS study to a larger cohort of 30 patients and provide a comprehensive correlation analysis with measurements of ACT and TEG. Aside from confirming a strong correlation with both ACT and TEG, we provide insights into the dynamics of incipient coagulation under natural conditions, and the relation to blood properties at advanced stages of the process. The developing correlation between the real-time information provided by LC-DLS and the end-point results of the externally triggered coagulation demonstrate the efficacy of this technique to monitor passively the early changes in the status of blood as required for efficient blood management during clinical procedures.
2. Materials and Method
LC-DLS Technique
The LC-DLS operation relies on the temporal fluctuations of the light intensity scattered from whole blood. In the time scales accessible in LC-DLS, these fluctuations are due to the movement of erythrocytes, which act as independent, rigid Brownian probes for the mechanical properties of the complex fluid surrounding them. This is in fact a micro-rheology measurement, where the scattered intensity fluctuations can be used to measure properties of complex fluids passively, in the presence of intrinsic thermal forces alone [
15,
16,
17].
It can be estimated that, at physiological conditions, the erythrocytes explore diffusively less than 1% of their own diameters during 1–10 ms. This means that in the frequency range 0.1 to 1 kHz, LC-DLS provides information about the viscoelasticity of medium in the immediate surroundings of an erythrocyte. The measurement is based on a robust setup where the light is sent out and detected through the same optical fiber element. More details can be found in the Supplementary Materials of Ref. [
14]. Practically, the dynamic information is recovered from the temporal autocorrelation of the fluctuations of light intensity scattered or, alternatively, from the corresponding power spectral density (PSD) of these intensity fluctuations.
At short time scales, the information about the microenvironment is encoded in the average mean-square displacement (MSD) of the probes (erythrocytes). In fact, MSD provides a close representation to the complex fluid’s response to an imposed shear strain [
18,
19]. In other words, the overall mechanical susceptibility of the fluid determines the way in which the probes diffuse. The process can be described as the MSD evolution
with a constant diffusion coefficient
and a viscoelasticity-dependent coefficient
. Depending on the value of this coefficient, the diffusion is classified as normal for
, and as sub- or super-diffusion for
and
, respectively [
20,
21]. Importantly, the effective parameter
determines the asymptotic PSD:
[
22,
23]. Thus, in the case of whole blood where the erythrocytes are the diffusing probes, the shape of
depends on the viscoelasticity of the complex fluid consisting of plasma and macromolecules. Due to the complex protein interactions, this viscoelasticity is expected to change during the process of coagulation.
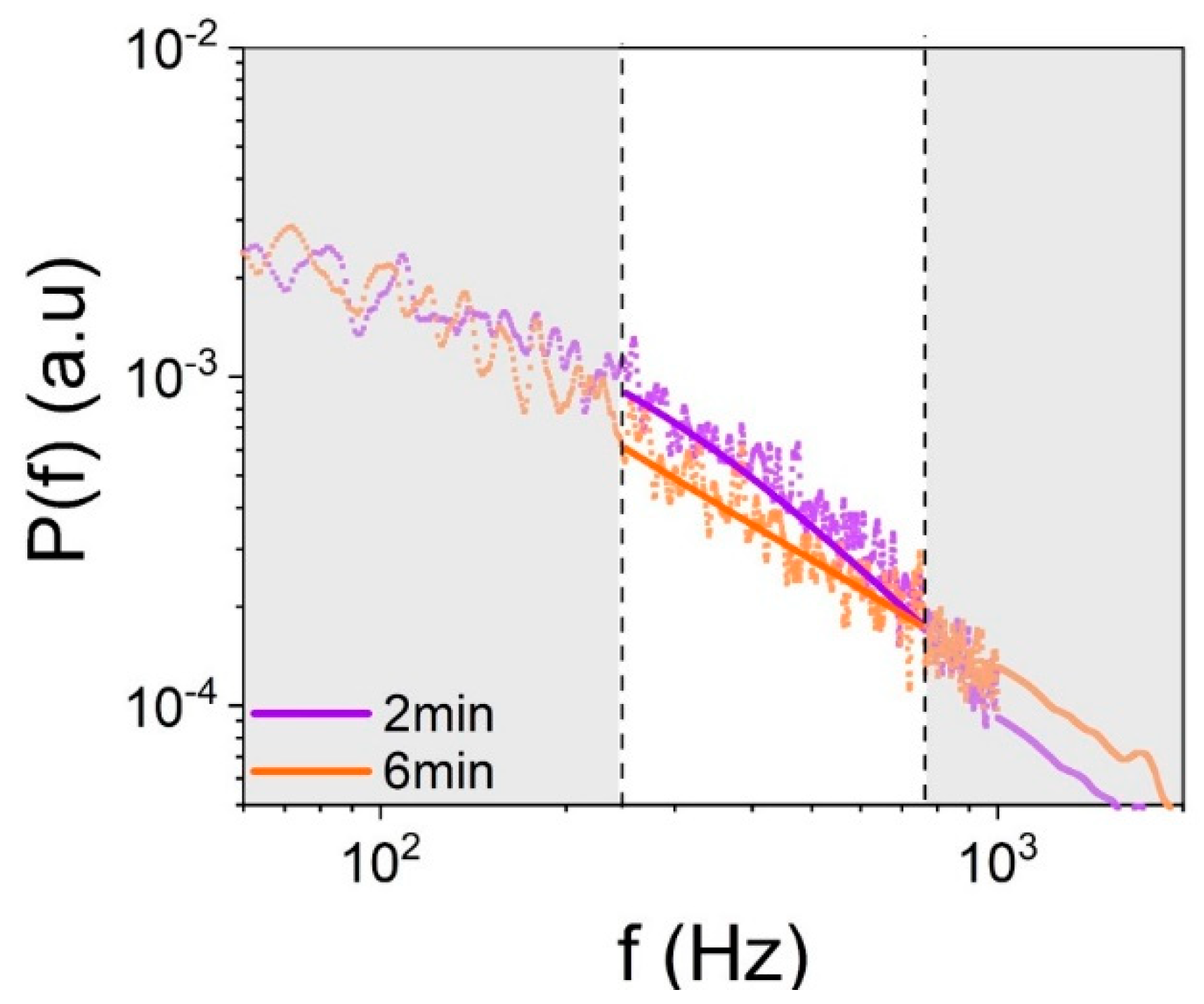
Typical LC-DLS measurements on whole blood taken at different times during the incipient, natural coagulation are illustrated in
Figure 1. As can be seen, the shape of
evolves indicating a reduction in the value of
, which relates to the slope of the PSD in the logarithmic representation as shown in
Figure 1. This means that, as blood starts to coagulate, the Red blood cells (RBCs) diffusion becomes more sub-diffusive, which can be associated to an increasing elasticity of the surrounding viscoelastic fluid. We emphasize that in these measurements no coagulation activators are used. Thus, the variations observed in
Figure 1 refer to minute changes in the mechanical properties of blood that take place during the incipient stages of natural coagulation, which is indicative of the high sensitivity of this optical measurement.
In the LC-DLS experiments,
is measured in the frequency range from 1 Hz to 10 kHz, with 1 Hz resolution and an integration time of 30 s. An averaged
was obtained from four consecutive measurements, which means that one power spectrum, as indicated by the dotted lines in
Figure 1, is obtained every 2 min. Then, the averaged
is fitted with a weighted superposition of Lorentzian functions,
with different relative amplitudes
and relaxation times
. This decomposition into Lorentzian modes relies on the rigorous single-scattering treatment for a monodisperse collection of particles whose diffusive motion is uncorrelated [
22,
24]. Besides its physical meaning, this fitting procedure provides means to generate a smoother PSD appropriate for data retrieval. We found that, for the entire set of measurements, five Lorentzians
is sufficient to follow the overall shape of
at all times over the frequency range (1 Hz to 10 kHz), while keeping the original 1 Hz resolution. The local logarithmic slope of
is then evaluated locally and an average value
is estimated in the frequency range from 250 Hz to 750 Hz, as shown in
Figure 1. The parameter
indicates the average decay of
within a frequency band, which is much narrower than the frequency range of the fit. As mentioned earlier,
quantifies practically the type of erythrocytes diffusion, which, in turn, is determined by the microscopic viscoelasticity of plasma. The range of
lies between the limits of viscous diffusion (
) and elastic confinement (
).
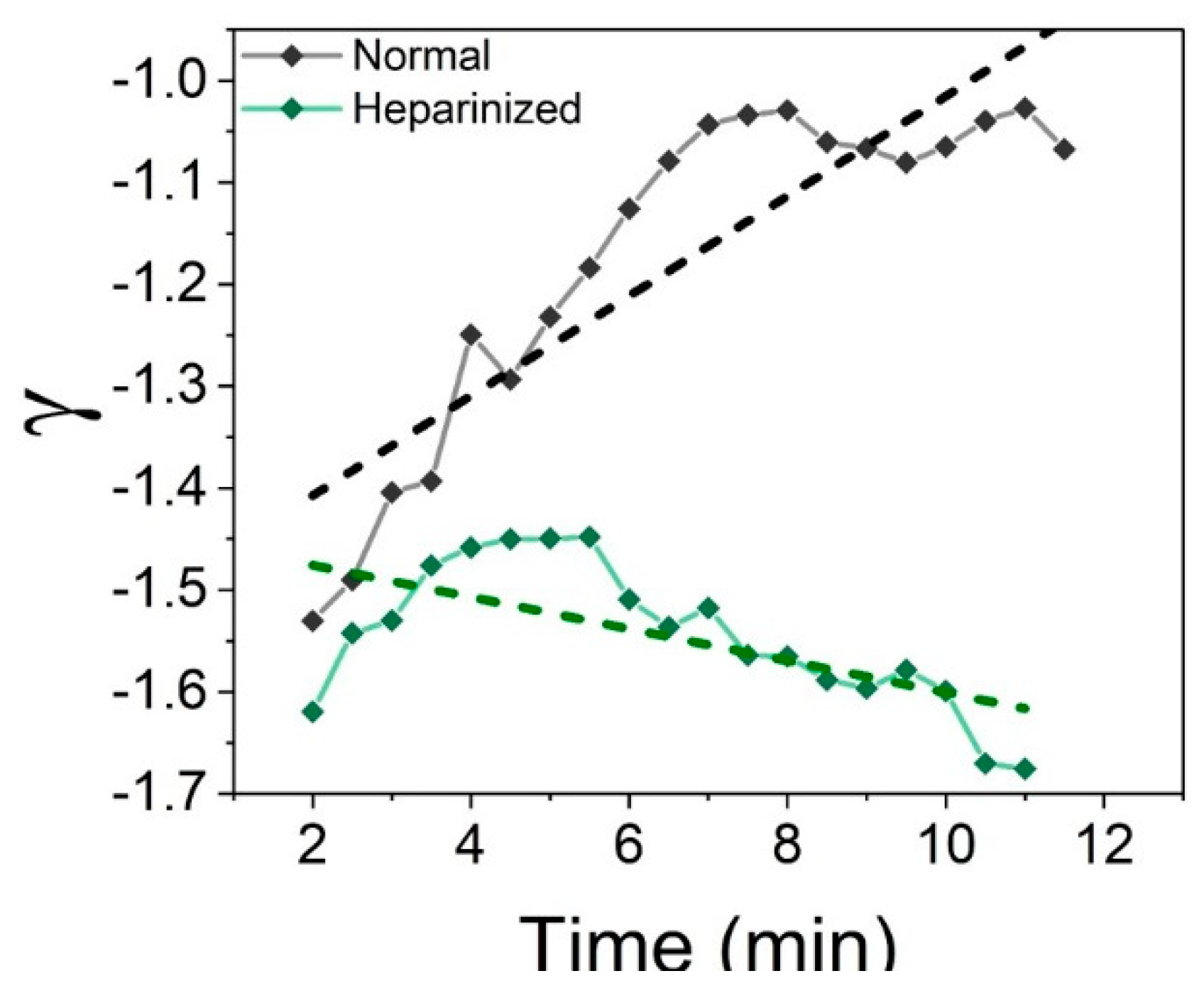
As an example of LC-DLS capabilities, let us now examine the initial stages of coagulation of blood with different coagulability.
Figure 2 illustrates how the measurement clearly captures the different evolution of
for untreated and heparinzed blood samples of the same origin (from the same patient). In the case of untreated blood, one can clearly see a progressive reduction of the absolute value of the log slope
, which indicates that the RBCs’ motion transitions gradually to a more sub-diffusive state characteristic to a more and more elastic environment. On the other hand, the thinning effect of heparin, administrated to the patient moments before the measurement, is to inhibit the creation of larger macromolecules responsible for the elastic behavior. The effect is evident: not only that coagulation is blocked but also there is still an ongoing action of heparin as apparent in the slight increase of |
|. Remember that a value of
closer to −2 indicates that the environment surrounding the erythrocytes is more fluid (
corresponds to a purely Newtonian fluid). We would like to emphasize that the differences illustrated in
Figure 2 were identified in the initial stages of blood evolution without the need of an external chemical trigger even from the beginning of the measurement.
4. Conclusions
The results of this study demonstrate that a continuous dynamic light scattering measurement is able to discriminate between subtle differences in the initial coagulation stages of blood in untreated and heparinized states without any coagulation stimulus. We demonstrated that the results of LC-DLS measurements at early times correlate with traditional ACT and TEG data. These correlations between the results of different types of measurements are significant for two reasons. First, they compare an instantaneous property of blood with characteristics derived from observing an entire process until it ends in a clot. Second, the processes examined evolve at different paces: one progresses naturally and the other is accelerated by external stimuli. Unsurprisingly, the correlation with traditional assays are non-stationary in nature: it grows in time. We would like to emphasize that the approximately six minutes needed to observe a significant correlation with the medical assay is due to both the different nature of the measurements (continuous vs. end-point) and the finite time necessary for the heparin effect to set in. This is not a limitation of the LC-DLS technique, which infers the blood status continuously and discriminates between different blood conditions even at early times.
The chosen figure of merit, the slope of the power spectrum of intensity fluctuations, is a just global parameter describing the viscoelastic properties of the fluid surrounding the erythrocytes. A more detailed model is necessary to relate the viscoelasticity to the microscopic composition of blood. In fact, LC-DLS provides the large-range frequency information necessary to describe fully the viscoelastic properties. Nevertheless, as our results demonstrate here, the slope captures well the propensity of blood to coagulate. Most importantly, this parameter is retrieved from a measurement that is fully passive.
Our results strongly suggest the LC-DLS is able to monitor continuously the status of blood, especially in situations where a sensitive fast measurement is needed. The figure of merit
used here can report small variations in the status of blood during full systemic anti-coagulation where ACT is mostly insensitive and in much shorter time compared to TEG [
27].


 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}







