
MR-LINAC-Guided Adaptive Radiotherapy for Gastric MALT: Two Case Reports and a Literature Review

Abstract
:Simple Summary
Abstract
1. Introduction
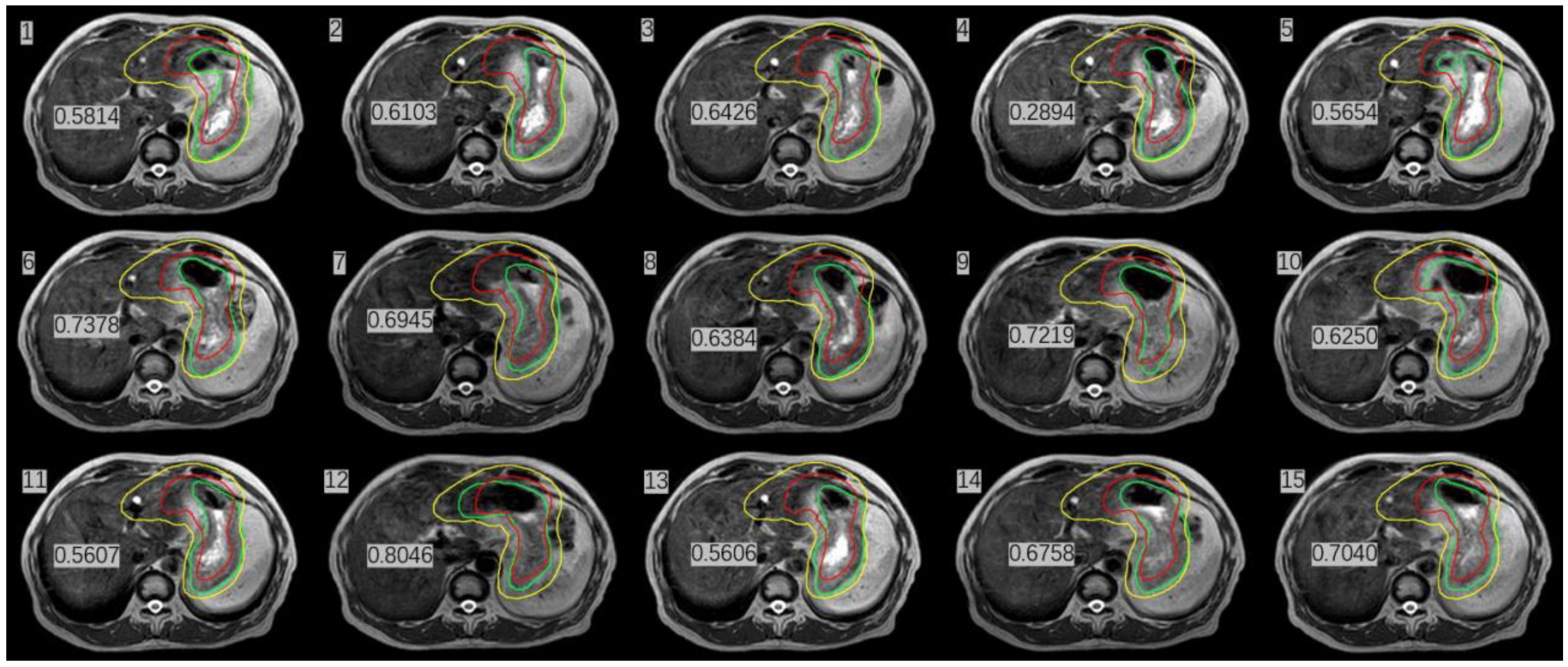
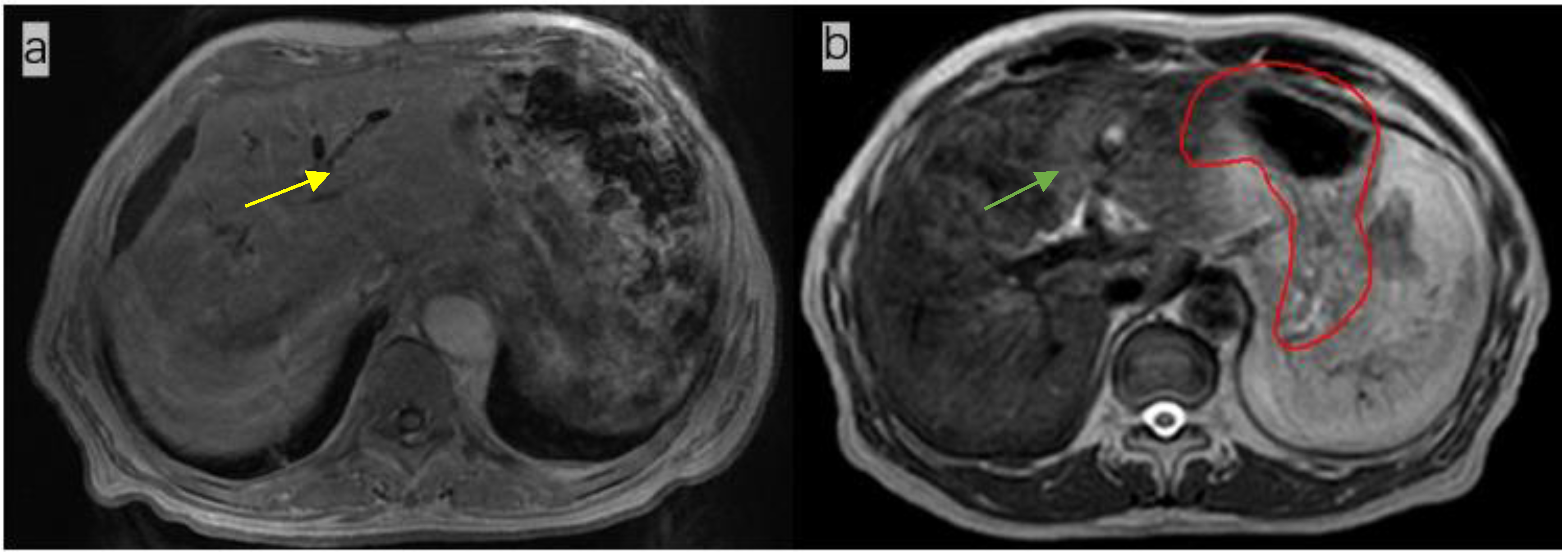
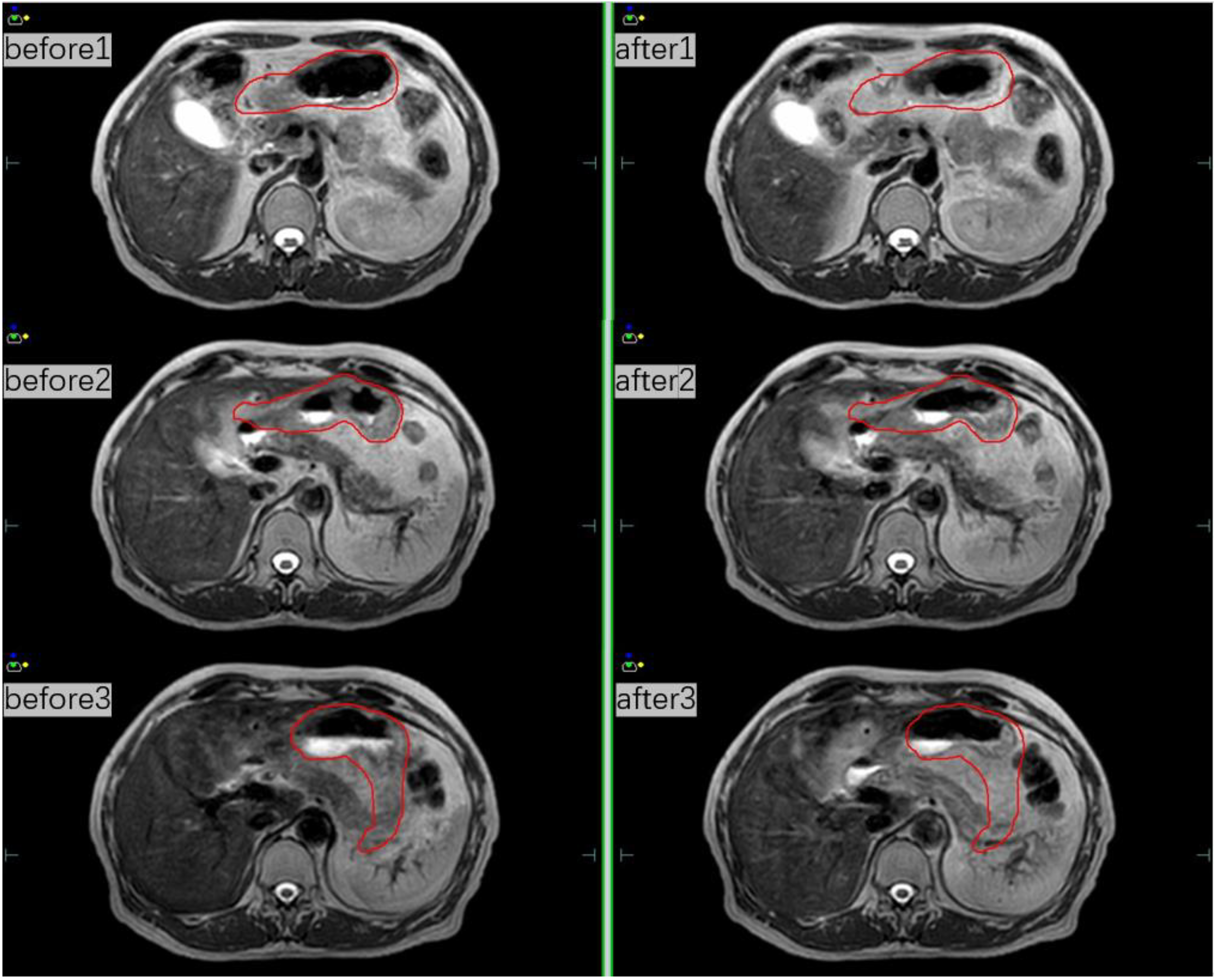
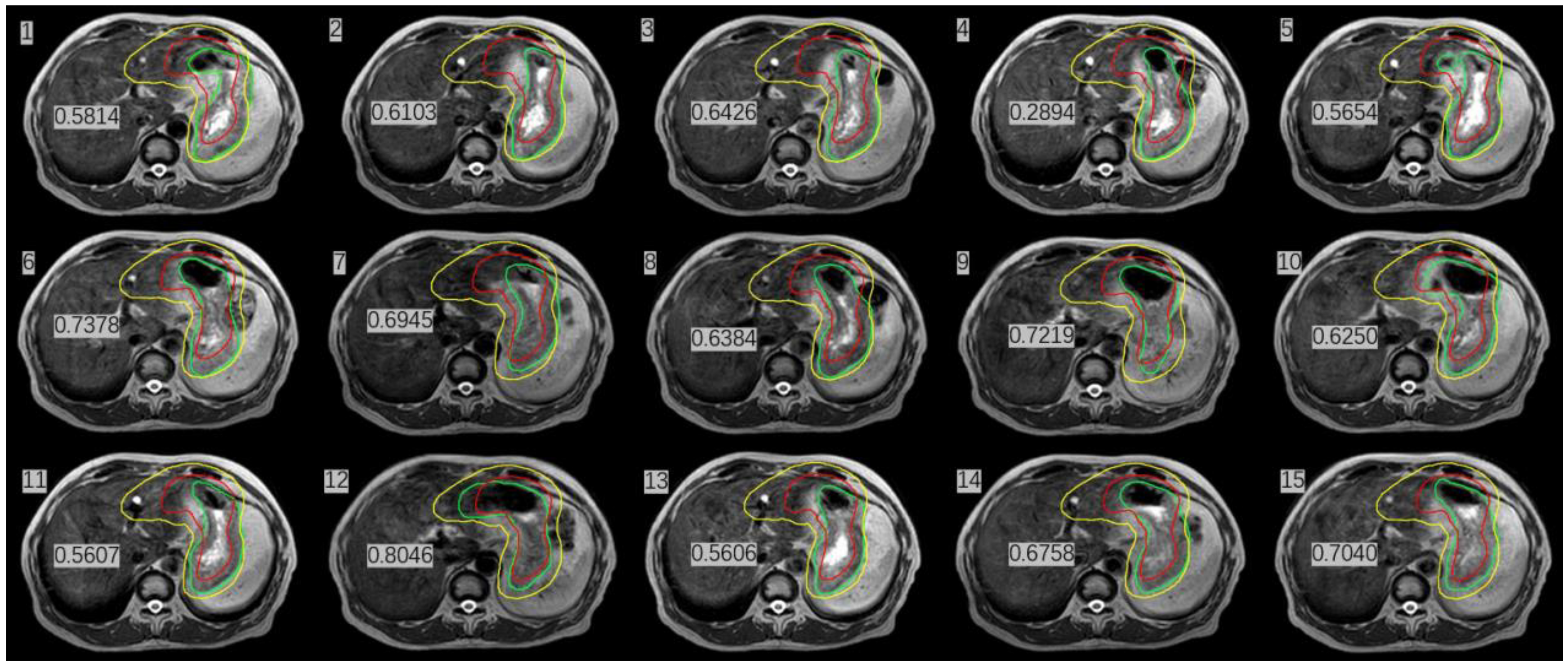
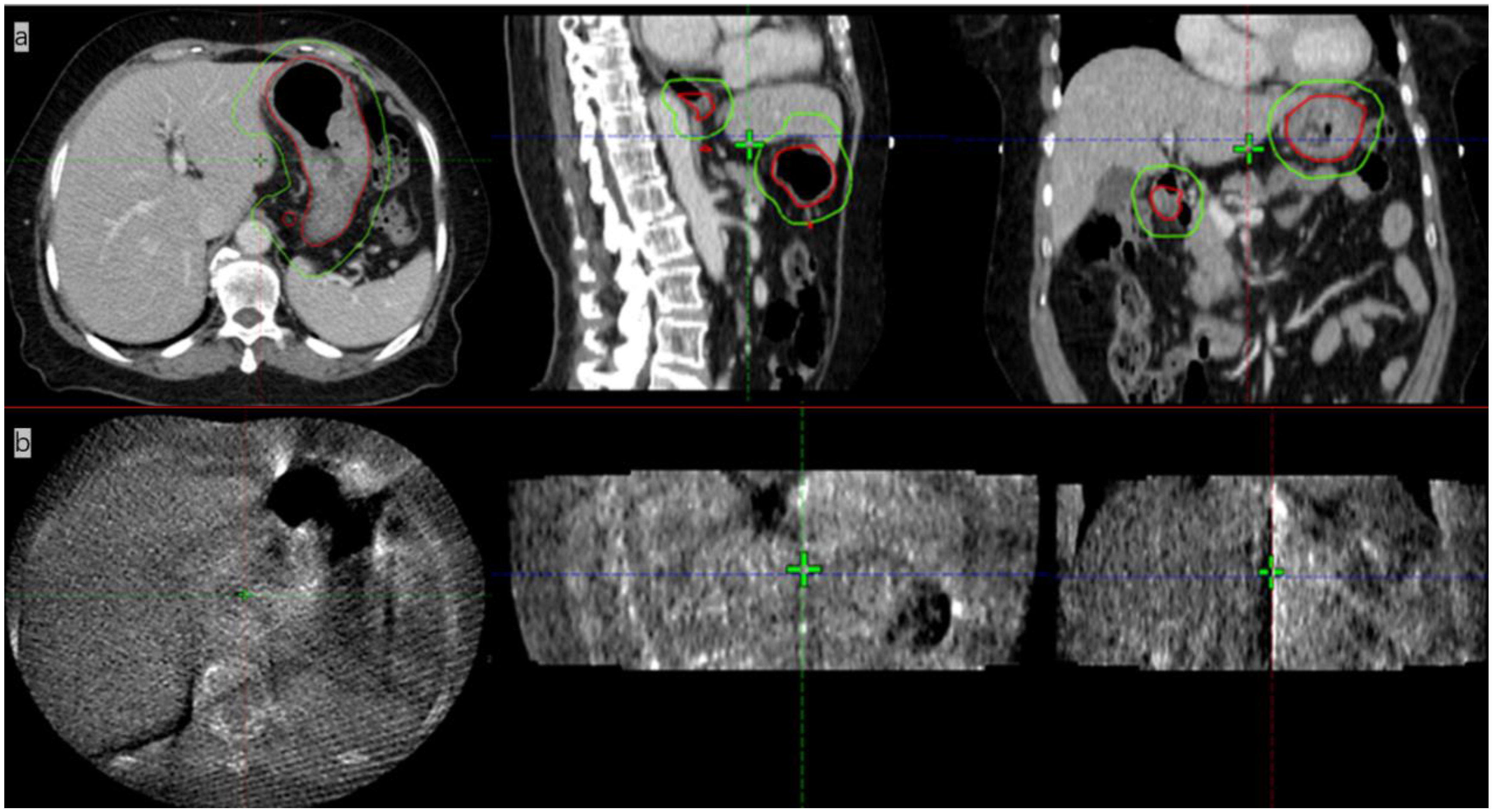
2. Presentation of Case #1
3. Presentation of Case #2
4. Discussion and Review of the Literature
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Connors, J.M.; Cozen, W.; Steidl, C.; Carbone, A.; Hoppe, R.T.; Flechtner, H.-H.; Bartlett, N.L. Hodgkin lymphoma. Nat. Rev. Dis. Primers 2020, 6, 61. [Google Scholar] [CrossRef] [PubMed]
- Bowzyk Al-Naeeb, A.; Ajithkumar, T.; Behan, S.; Hodson, D.J. Non-Hodgkin lymphoma. BMJ 2018, 362, k3204. [Google Scholar] [CrossRef] [PubMed]
- Daamen, L.A.; de Mol van Otterloo, S.R.; van Goor, I.W.J.M.; Eijkelenkamp, H.; Erickson, B.A.; Hall, W.A.; Heerkens, H.D.; Meijer, G.J.; Molenaar, I.Q.; van Santvoort, H.C.; et al. Online adaptive MR-guided stereotactic radiotherapy for unresectable malignancies in the upper abdomen using a 1.5T MR-linac. Acta Oncol. 2022, 61, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Kontaxis, C.; Bol, G.H.; Lagendijk, J.J.W.; Raaymakers, B.W. A new methodology for inter- and intrafraction plan adaptation for the MR-linac. Phys. Med. Biol. 2015, 60, 7485–7497. [Google Scholar] [CrossRef] [PubMed]
- Henke, L.; Kashani, R.; Robinson, C.; Curcuru, A.; DeWees, T.; Bradley, J.; Green, O.; Michalski, J.; Mutic, S.; Parikh, P.; et al. Phase I trial of stereotactic MR-guided online adaptive radiation therapy (SMART) for the treatment of oligometastatic or unresectable primary malignancies of the abdomen. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2018, 126, 519–526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raaymakers, B.W.; Lagendijk, J.J.W.; Overweg, J.; Kok, J.G.M.; Raaijmakers, A.J.E.; Kerkhof, E.M.; van der Put, R.W.; Meijsing, I.; Crijns, S.P.M.; Benedosso, F.; et al. Integrating a 1.5 T MRI scanner with a 6 MV accelerator: Proof of concept. Phys. Med. Biol. 2009, 54, N229–N237. [Google Scholar] [CrossRef] [PubMed]
- Lagendijk, J.J.W.; Raaymakers, B.W.; van Vulpen, M. The magnetic resonance imaging-linac system. Semin. Radiat. Oncol. 2014, 24, 207–209. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Tepper, J.E. Radiation therapy-associated toxicity: Etiology, management, and prevention. CA Cancer J. Clin. 2021, 71, 437–454. [Google Scholar] [CrossRef] [PubMed]
- Moore, K.L.; Kagadis, G.C.; McNutt, T.R.; Moiseenko, V.; Mutic, S. Vision 20/20: Automation and advanced computing in clinical radiation oncology. Med. Phys. 2014, 41, 010901. [Google Scholar] [CrossRef] [PubMed]
- Corradini, S.; Alongi, F.; Andratschke, N.; Belka, C.; Boldrini, L.; Cellini, F.; Debus, J.; Guckenberger, M.; Hörner-Rieber, J.; Lagerwaard, F.J.; et al. MR-guidance in clinical reality: Current treatment challenges and future perspectives. Radiat. Oncol. 2019, 14, 92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witt, J.S.; Rosenberg, S.A.; Bassetti, M.F. MRI-guided adaptive radiotherapy for liver tumours: Visualising the future. Lancet Oncol. 2020, 21, e74–e82. [Google Scholar] [CrossRef]
- Stephen, R.M.; Jha, A.K.; Roe, D.J.; Trouard, T.P.; Galons, J.-P.; Kupinski, M.A.; Frey, G.; Cui, H.; Squire, S.; Pagel, M.D.; et al. Diffusion MRI with Semi-Automated Segmentation Can Serve as a Restricted Predictive Biomarker of the Therapeutic Response of Liver Metastasis. Magn. Reson. Imaging 2015, 33, 1267–1273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaffray, D.A.; Siewerdsen, J.H.; Wong, J.W.; Martinez, A.A. Flat-panel cone-beam computed tomography for image-guided radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 2002, 53, 1337–1349. [Google Scholar] [CrossRef]
- Videtic, G.; Vassil, A.; Neil, W. Handbook of Treatment Planning in Radiation Oncology, 3rd ed.; Springer Publishing Company, LLC: New York, NY, USA, 2021; pp. 174–177. [Google Scholar]
- Winkel, D.; Werensteijn-Honingh, A.M.; Eppinga, W.S.C.; Intven, M.P.W.; Hes, J.; Snoeren, L.M.W.; Visser, S.A.; Bol, G.H.; Raaymakers, B.W.; Jürgenliemk-Schulz, I.M.; et al. Dosimetric feasibility of hypofractionation for SBRT treatment of lymph node oligometastases on the 1.5T MR-linac. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2021, 154, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Rudra, S.; Jiang, N.; Rosenberg, S.A.; Olsen, J.R.; Roach, M.C.; Wan, L.; Portelance, L.; Mellon, E.A.; Bruynzeel, A.; Lagerwaard, F.; et al. Using adaptive magnetic resonance image-guided radiation therapy for treatment of inoperable pancreatic cancer. Cancer Med. 2019, 8, 2123–2132. [Google Scholar] [CrossRef] [PubMed]
- Chun, S.-J.; Jeon, S.H.; Chie, E.K. A Case Report of Salvage Radiotherapy for a Patient with Recurrent Gastric Cancer and Multiple Comorbidities Using Real-time MRI-guided Adaptive Treatment System. Cureus 2018, 10, e2471. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Treatment Modality | Mean Dose (cGy) | |||
|---|---|---|---|---|
| Liver | Spinal Cord | Duodenum | Left Kidney | |
| CT simulation therapy | 929.1 | 470.8 | 1025.1 | 277.7 |
| MRI-guided therapy1 | 771.6 | 470.3 | 692.4 | 334.8 |
| MRI-guided therapy2 | 811.0 | 454.5 | 669.9 | 383.4 |
| MRI-guided therapy3 | 824.7 | 481.7 | 912.1 | 221.6 |
| MRI-guided therapy4 | 896.7 | 509.7 | 949.4 | 341.1 |
| MRI-guided therapy5 | 841.3 | 464.2 | 948.9 | 397.3 |
| MRI-guided therapy6 | 843.7 | 526.6 | 1038.7 | 255.8 |
| MRI-guided therapy7 | 845.0 | 437.2 | 952.5 | 282.1 |
| MRI-guided therapy8 | 913.2 | 405.1 | 704.4 | 188.2 |
| MRI-guided therapy9 | 856.0 | 564.0 | 994.7 | 170.8 |
| MRI-guided therapy10 | 778.7 | 462.2 | 787.0 | 508.6 |
| MRI-guided therapy11 | 899.0 | 541.7 | 838.1 | 322.4 |
| MRI-guided therapy12 | 882.0 | 534.5 | 1178.5 | 418.3 |
| MRI-guided therapy13 | 819.9 | 512.3 | 989.0 | 302.9 |
| MRI-guided therapy14 | 808.2 | 387.6 | 654.2 | 113.4 |
| MRI-guided therapy15 | 820.1 | 497.4 | 813.7 | 225.1 |
| MRI-guided therapy mean | 840.74 | 483.3 | 874.9 | 297.7 |
| Basic Information | Presentation of Case #1 | Presentation of Case #2 |
|---|---|---|
| Age (years) | 53 | 70 |
| Sex | Male | Female |
| Helicobacter pylori infection | negative | negative |
| immunohistochemistry | CD20+, CD43+, CD3+, BCL2+, CD5 minority+, CD23 minority-, CD38 minority+, CyclinD1 minority+, Lambda individual+, BCL-6-, Kappa-, Ki-67+10% | CD20+, CD79a+, CD3-, CD7-, CD5-, CD10-, BCL-6-small amount+, BCL-2 partial+, Mum-1-, C-Mum-1-, C-myc-, CyclinD1-, P53+ about 60% and Ki-67+ about 10%. |
| Ann Arbor staging | IIE | IIE |
| Anticancer drugs | 4 cycles of rituximab 600 mg (02/18–03/12/2022) | 4 cycles of rituximab 600 mg (11/23–12/15/2021) |
| Before the CT simulation | anisodamine (dose 10 mg) | anisodamine (dose 10 mg) |
| Radiation therapy | ISRT to 30 Gy with 15 fractions (Unity MR-LINAC) | ISRT to 30 Gy with 15 fractions (Halcyon LINAC) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Song, Y.; Li, Z.; Wang, H.; Zhang, Y.; Yue, J. MR-LINAC-Guided Adaptive Radiotherapy for Gastric MALT: Two Case Reports and a Literature Review. Radiation 2022, 2, 259-267. https://doi.org/10.3390/radiation2030019
Song Y, Li Z, Wang H, Zhang Y, Yue J. MR-LINAC-Guided Adaptive Radiotherapy for Gastric MALT: Two Case Reports and a Literature Review. Radiation. 2022; 2(3):259-267. https://doi.org/10.3390/radiation2030019
Chicago/Turabian StyleSong, Yajun, Zhenjiang Li, Huadong Wang, Yun Zhang, and Jinbo Yue. 2022. "MR-LINAC-Guided Adaptive Radiotherapy for Gastric MALT: Two Case Reports and a Literature Review" Radiation 2, no. 3: 259-267. https://doi.org/10.3390/radiation2030019
APA StyleSong, Y., Li, Z., Wang, H., Zhang, Y., & Yue, J. (2022). MR-LINAC-Guided Adaptive Radiotherapy for Gastric MALT: Two Case Reports and a Literature Review. Radiation, 2(3), 259-267. https://doi.org/10.3390/radiation2030019