Abstract
Globally, suicide mortality rates have decreased in this century; however, it has been reported that the decreasing trends of some subgroups were attenuated in the late 2010s. These tendencies are pronounced among adolescents. In this study, the temporal fluctuations of the age-standardized death rate of suicide (ASDR-suicide), crude mortality rate of suicide (CMR-suicide), and percentage of suicides per total deaths (PTD-suicide) among adolescents (10–24 years) in the global high-income and middle-income countries and in the Western Pacific Region (WPR) from 1990 to 2019, as well as the fixed effects of communication factors (penetration of cellular telephones and the Internet) on the ASDR-suicide/CMR-suicide/PTD-suicide of adolescents, were analyzed using the WHO Mortality Database. The male ASDR-suicide in global middle-income countries decreased, and those of males in global high-income countries and females in middle-income countries were unchanged, while the rate of other groups (males in the WPR and females in high-income countries and the WPR) increased. The ASDR-suicide of adolescent males in the WPR was almost equivalent to that of males in global high-income and middle-income countries in the 1990s but was higher than the rate in the 2010s. The ASDR-suicide of adolescent females in the WPR was consistently higher than that of females in global high-income and middle-income countries from 1990 to 2019, but the differences widened over time. The PTD-suicide of both males and females in middle-income countries was unchanged, whereas the PTD-suicide in global high-income countries and the WPR increased over time. The PTD-suicide in the WPR markedly increased by >40% in the late 2010s. The fixed effects of cellular telephone and Internet penetrations were negatively and positively related to adolescent suicide in the WPR, respectively. Therefore, these results suggest that, in this century, suicide prevention in adolescent health activities has been increasing in importance in the WPR compared with other regions.
1. Introduction
Adolescence (10–24 years of age) is the most stable generation in biological life prognosis; indeed, the crude mortality rate per 100,000 population (CMR) of all causes is the lowest among overall generations [1,2,3,4,5]. The leading causes of death drastically change with age, shifting from congenital abnormalities and infections in newborns/young children to road traffic accidents, interpersonal violence, and self-harm in adolescence [2,3,4,5].
It is well known that suicide displays age-dependent and geographic features. The suicide mortalities and the sex ratio (males/females) of suicide mortality in Asia countries have been higher than those in Western countries [6]. Previous epidemiologic findings suggested that complicated interactions among traditional cultural values, rapid economic transitions under market globalization, higher sensitivity to family conflicts, and financial security issues play important roles in these suicidal features in Asia [6,7,8]. It has been suggested that the relatively higher suicide mortality among females in Asia may be related to the higher prevalence of psychiatric disorders (mood disorders) and vulnerability to psychosocial stress [9], whereas other reports have emphasized that the role of mental deterioration in suicide in Asia was less important than in Western countries [6,10]. Suicide among younger children (younger than 10 years of age) is very rare; however, it begins to be detected in younger adolescents and drastically increases during adolescence [11]. Although the global age-standardized death rate of suicide per 100,000 population (ASDR-suicide) was 9.2 in 2019, the CMR of suicide (CMR-suicide) increased from 1.6 (10–14 years of age) to 5.9 (15–19 years of ages) in 2019 [12]. The CMR-suicide among adolescents was lower than that in adults, whereas from another perspective, suicide was the fifth leading cause of death globally in those aged 10–19 years [11,13,14,15]. Suicide was especially severe in Europe and the Western Pacific Region (WPR) and was the second leading cause of death among adolescents in those regions [12]. Therefore, suicide is one of the most severe adolescent health concerns globally, but it appears to be more serious in Europe and the WPR [11,13,14,15]. In other words, to discuss the seriousness of adolescent suicide, it is necessary to consider not only ASDR/CMR-suicide but also the proportion of suicides in the total number of deaths (PTD-suicide) among adolescents.
The Comprehensive Mental Health Action Plan of the World Health Organization (WHO) set a target of reducing global suicide mortality by 10% between 2012 and 2020 [16]. Temporal fluctuations of ASDR/CMR-suicide have usually been adopted to evaluate the Comprehensive Mental Health Action Plan [13]. Globally, ASDR-suicide has decreased in this century; however, the decreasing trends in some regions have attenuated or, conversely, increased after the late 2010s in countries such as Japan (attenuated decreasing trends) and the United States (increasing) [13,14,17,18,19]. These tendencies are particularly pronounced in adolescents [18,20,21,22]. Furthermore, recent studies using the “WHO Mortality Database” revealed that fluctuations in ASDR/CMR-suicide varied geographically [18,20,21,22]. In particular, although suicide was the second leading cause among all causes of death for adolescents in both the WPR and Europe, ASDR-suicide among adolescents consistently decreased in Europe [20] but increased in the WPR [18,21,23,24,25,26]. These previous findings suggest that evidence-based suicide prevention measures for adolescent health require not only knowledge of trends in suicide mortality rates (ASDR-suicide and CMR-suicide) but also the temporal fluctuations of the PTD-suicide of adolescents.
It is well known that various factors, such as socioeconomic and psychosocial factors, play important roles in suicide. Indeed, a number of studies have reported a plethora of findings regarding the causes and/or backgrounds of adolescent suicide [11,23,27,28,29,30]. Previously, the various risk factors for suicide among adolescents in the United States were reported to be diverse, depending on sex, ethnic group, and religion [31]. A longitudinal study of clinical cases integrating various risk factors and their interactions showed that health problems, including physical and psychiatric disabilities, were risk factors for suicide [32,33]. The majority of previous studies suggested that suicide risks across countries in the WPR may be consistent with those found in Western/European countries; however, countries in the WPR are composed of culturally, religiously, and economically diverse peoples. Indeed, diverse features related to suicide among the WPR countries have been revealed. In New Zealand, adolescents with the lowest socioeconomic status were reported to be over thirty times more likely to attempt suicide than individuals with a higher socioeconomic status [34]. However, in several Asian countries, school-related problems were common precipitants of adolescent suicide attempts [22,35], and the impacts of school-related problems also constituted over 40% of the causes of suicide among adolescents in Japan [18,21]. The populations in urban areas among WPR countries are larger compared with those among OECD member countries. In both the Republic of Korea (South Korea) and Japan, the CMR-suicide in the urban areas is lower than that in the rural areas, but the increasing trends of CMR-suicide in urban areas are greater than those in the rural areas [17,22,36]. Despite these efforts, cross-national causality analyses have been underestimated compared with time-series analyses, since valid international data on suicide risk factors for each country are limited and difficult to obtain. Thus, the majority of studies are limited to speculation due to the indirect comparisons of results between different cohort studies [18,20,21,22,37,38].
Adolescence represents a dramatic transition in psychosocial development, as a stage from dependence to independence [1]. Adolescents must strive for education, training, and physical strengthening for their future psychosocial and socioeconomic independence [1]. Therefore, the drastic psychosocial and socioeconomic transformation may affect adolescent individuals through education, training, and physical strengthening processes. In this century, the increasing penetrations of both the Internet and cellular telephones have been affecting adolescent lifestyles, including education, recreation, and communication with peers [39,40,41,42]. Although the Internet has become an important tool in the education of students, the adverse health consequences associated with inappropriate Internet use are a matter of concern [42,43,44,45,46]. The prevalence of Internet addiction is also increasing over time with increasing Internet penetration [44]. Notably, it is concerning that the increase in Internet usage has been related to an increase in health-risk behaviors, including suicide [42,43,45,46]. Thus, cross-national comparative analysis of the impact of the penetrations of the Internet and cellular telephones on adolescent suicide can provide important information for planning adolescent suicide prevention measures.
The WHO recommends dividing the 194 member countries into six regions (including the WPR) to promote its comprehensive health policies [47]. Based on these backgrounds, this study aimed to clarify the following three points: (1) the identification of the temporal fluctuations of adolescent suicides (ASDR/CMR-suicide) in the WPR in comparison with the global high-income and middle-income countries; (2) the determination of the proportion of suicides among causes of overall adolescents (PTD-suicide) in the WPR; and (3) the impacts of the penetration of the Internet and cellular telephones on adolescent suicide mortalities, using the “WHO Mortality Database” and the International Telecommunication Union (ITU) database [47,48]. Finally, through the findings of this study (temporal fluctuation of several values related to adolescent suicide, including ASDR-, CMR-, and PTD-suicide, as analyzed by time series analysis in the WPR and the impacts of the penetrations of the Internet and cellular telephones on adolescent suicide), we discuss how to improve suicide prevention measures for adolescents in the post-COVID-19 era.
2. Materials and Methods
This cross-sectional study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines [49]. The Medical Ethics Review Committee of Mie University waived the requirement for informed consent and ethical approval because these data were publicly available.
2.1. Data Source
Populations and the annual number of death caused by suicides (X60–X84, Y87.0 in ICD-10), infectious and parasitic diseases (A00–B99, G00–G04, G14, N70–N73, P37.3, P37.4 in ICD-10), respiratory infections (H65–H66, J00–J22, P23, U04, U07.1, U07.2, U09.9, U10.9 in ICD-10), malignant neoplasms (cancer: C00–C97 in ICD-10), road traffic accidents (V01–04, V06, V09, V10–79, V80–89, V99, Y85.0 in ICD-10) and violence (X85–Y09, Y871 in ICD-10) disaggregated by sex (male and female), age (5-year intervals: 10–14, 15–19, and 20–24 years), and overall age from 1990 to 2019 were obtained from the WHO Mortality Database [47]. Cellular telephone penetration (number of subscriptions per 100 people: mobile-sub) and Internet penetration (number of Internet users per 100 people: Internet users) were obtained from the International Telecommunication Union (ITU) [48].
The crude mortality rate per 100,000 population (CMR) of all-cause, suicide, infectious/parasitic disease, respiratory infection, cancer, traffic accidents, and violence, disaggregated by sex, age, and calendar year, was calculated by dividing the annual number of deaths by the 100,000 population of the corresponding group in the same calendar year. The age-standardized death rate per 100,000 suicides (ASDR-suicide) of overall ages and adolescents (10–25 years of age) was calculated using the WHO World Standard Population Model [50]. The proportion of suicides among all deaths (percentage of suicides per total deaths: PTD-suicide) was calculated by dividing the number of suicides by all deaths in the same groups. In the present study, the observation period was set to be from 1990 to 2019 to eliminate the impact of the COVID-19 pandemic and the incomplete suicide data in the WHO Mortality Database. According to the country income classification of the World Bank, the ASDR-suicide and PTD-suicide of global high-income and middle-income (upper-middle and lower-middle income) countries were calculated.
2.2. Statistical Analysis
Joinpoint regression was used to conduct a time-trend analysis of ASDR-suicide, CMR-suicide, and PTD-suicide from 1990 to 2019 using Joinpoint Regression Software (ver 5.0.2; National Cancer Institute). Joinpoint regression, which is well known for segmented regression analysis, simply fits the joinpoint model allowed by the trend data and identifies significant points where the trends change [18,22,26,51]. The estimated annual percent change (APC) and the corresponding 95% confidence interval (95%CI) were calculated for each identified segment by fitting a regression line to the natural logarithm of each value using the calendar year as a regressor variable [ln (rate) = a × (calendar year) + b; APC was estimated as 100 × (eb−1)]. The estimated average annual percent change from 1990 to 2019 (AAPC) was also calculated using the method that was used to estimate the APC [18,25,26,51,52]. Two-tailed p-values of <0.05 were considered to indicate statistical significance. The fixed effects of communication factors (mobile-sub and Internet-user) on adolescent ASDR-suicide and CMR-suicide at 10–14, 15–19, and 20–24 years of age were analyzed using hierarchical linear model with robust standard error (HLM) using Gretl v2023c [17,21,22]. Currently, the HLM is established as the most popular and useful statistical method for analyzing suicide causality at the national and international levels [53,54]. In particular, the HLM is considered to be a powerful statistical method for determining fixed effects on suicide mortality due to the elimination of “Simpson’s paradox” [55]. Two-tailed p-values of <0.05 were considered to indicate statistical significance. The time-dependent fluctuations of ASDR-suicide and PTD-suicide in the 1990s, 2000s, and 2010s were analyzed using two-way analysis of variance (ANOVA) with Scheffe’s post hoc test using BellCurve for Excel version 3.2 (Social Survey Research Information Co., Ltd., Tokyo, Japan). When the F-value of the ANOVA was significant (p < 0.05) and there was no significant variance inhomogeneity, the data were analyzed using Scheffe’s post hoc test [56].
The WHO Mortality Database published the mortality data in the WPR, including Australia, Brunei Darussalam, Hong Kong, Japan, the Republic of Korea (South Korea), Malaysia, New Zealand, the Philippines, Singapore, and Thailand. This study adopted the mortality data from Australia, Hong Kong, Japan, South Korea, New Zealand, and Singapore, which are high-income countries, while the data from Brunei Darussalam, Malaysia, the Philippines, and Thailand were incomplete and included many missing values, making an accurate statistical analysis impossible. Data were missing for Australia in 2005, Hong Kong in 2018–2019, and New Zealand in 2016–2019. No manipulation was performed for the missing values [47].
3. Results
The descriptive statistics, average populations, and total suicide numbers from 1990 to 2019 in the global high-income countries, global middle-income countries, and the WPR are summarized in Table 1.

Table 1.
Mean ± SD of population, total suicide numbers across overall ages and for the age ranges of 10–14, 15–19, and 20–24 years from 1990 to 2019.
3.1. ASDR-Suicide and PTD-Suicide of Overall Ages among Global High-Income and Middle-Income Countries and the WPR from 1990 to 2019
The ASDR-suicide of males of overall ages in global high-income and middle-income countries decreased from 1990 to 2019 (Figure 1, Table 2). Conversely, the ASDR-suicide of males of overall ages in the WPR did not change from 1990 to 2019, whereas that displayed the reversed U-shaped pattern (the joinpoint from increasing to decreasing was 2004) was observed in the WPR (Figure 1, Table 2). In the 1990s, the ASDR-suicides of males in the three groups (global high-income countries, middle-income countries, and the WPR) were almost equal, whereas the ASDR-suicide of males in the WPR was higher in comparison with that of the high-income and middle-income countries (Figure 2). The fluctuations of the ASDR-suicide of females were similar to those of males, indicating that the gaps among the three groups increased over time (Figure 1, Table 2). In the 1990s, the ASDR-suicide of females in the WPR was already higher in comparison with that of high-income and middle-income countries (Figure 2).
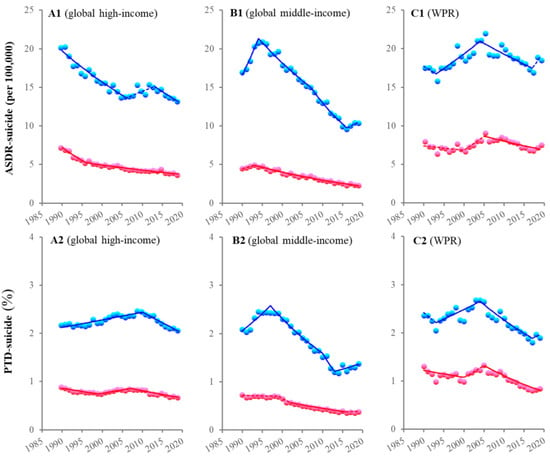
Figure 1.
Temporal fluctuations of ASDR-suicide and PTD-suicide of overall ages among global high-income, middle-income, and the WPR countries from 1990 to 2019. Temporal fluctuation of annual ASDR-suicide (upper side panels: (A1–C1)) and PTD-suicide (lower side panels: (A2–C2)) of overall ages among males (blue) and females (red) in high-income (A1,A2), middle-income (B1,B2), and the WPR (C1,C2) countries from 1990 to 2019 using joinpoint regression. Ordinates indicate the annual ASDR-suicide (per 100,000 population: (A1–C1)) or PTD-suicide (%: (A2–C2)). Abscissas indicate calendar years. Circles indicate the observed data. Solid and dotted lines indicate the significant and nonsignificant trends of ASDR-suicide and PTD-suicide detected by joinpoint regression, respectively.
Table 2.
Summary of AAPC values of ASDR-suicide and PTD-suicide of overall age from 1990 to 2019.
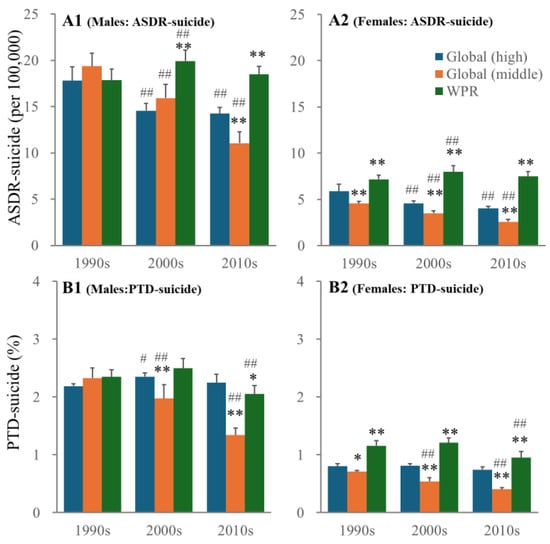
Figure 2.
ASDR-suicide and PTD-suicide of overall ages among males and females in global high-income, middle-income, and WPR countries from 1990 to 2019. Upper side panels indicate ASDR-suicide of males (A1) and females (A2). Lower side panels indicate PTD-suicide of males (B1) and females (B2). * p < 0.05, ** p < 0.01 relative to high-income countries, # p < 0.05, ## p < 0.01 relative to 1990s by two-way analysis of variance (ANOVA) with Scheffe’s post hoc test. F-values of ASDR-suicide of males and females were [Fregion(2,89) = 75.3 (p < 0.01), Fyear(2,89) = 75.7 (p < 0.01), Fregion*year(4,89) = 42.0 (p < 0.01)] and [Fregion(2,89) = 49.4 (p < 0.01), Fyear(2,89) = 59.9 (p < 0.01), Fregion*year(4,89) = 24.3 (p < 0.01)], respectively. F-values of ASDR-suicide of males and females were [Fregion(2,89) = 73.6 (p < 0.01), Fyear(2,89) = 74.0 (p < 0.01), Fregion*year(4,89) = 33.8 (p < 0.01)] and [Fregion(2,89) = 74.1 (p < 0.01), Fyear(2,89) = 53.3 (p < 0.01), Fregion*year(4,89) = 15.2 (p < 0.01)], respectively.
The fluctuations of the PTD-suicide of males and females in the global middle-income countries and the WPR were similar to the fluctuations of the ASDR-suicide (Figure 1, Table 2). However, the PTD-suicide in the global high-income countries showed different patterns from the ASDR-suicide. The PTD-suicide of males in the global high-income countries increased from 1990 to 2010, then decreased from 2010 to 2019, whereas the PTD-suicide of females increased from 1990 to 1999 and 2007 to 2019 but decreased from 1999 to 2007 (Figure 1).
3.2. ASDR-Suicide and PTD-Suicide among Adolescents in Global High-Income, Middle-Income, and WPR Countries from 1990 to 2019
In contrast to overall age, the ASDR-suicide of adolescent males in the global middle-income countries decreased; that of males in high-income countries and females in middle-income countries did not change, whereas the rate of other groups (males in the WPR and females in high-income countries and the WPR) increased (Figure 3, Table 3). The PTD-suicide of males and females in middle-income countries did not change, whereas the rates in global high-income countries and the WPR increased over time (Figure 3, Table 3). Notably, the PTD-suicide in the WPR markedly increased by approximately 40% in the late 2010s (Figure 4).
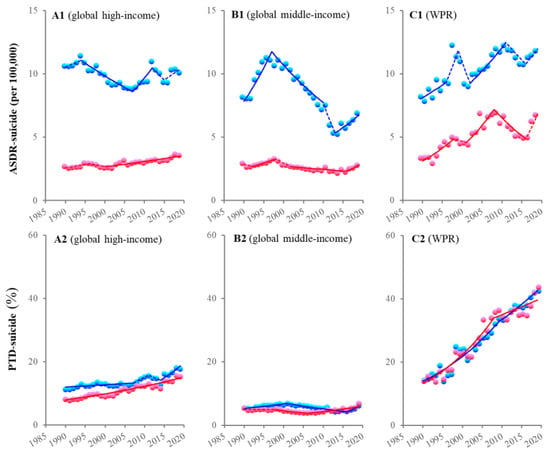
Figure 3.
Temporal fluctuations of ASDR-suicide and PTD-suicide among adolescents in global high-income, middle-income, and WPR countries from 1990 to 2019. Temporal fluctuation of annual ASDR-suicide (upper side panels: (A1–C1)) and PTD-suicide (lower side panels: (A2–C2)) among adolescent males (blue) and females (red) in high-income (A1,A2), middle-income (B1,B2), and WPR (C1,C2) countries from 1990 to 2019 using joinpoint regression. Ordinates indicate the annual ASDR-suicide (per 100,000 population: (A1–C1)) or PTD-suicide (%: (A2–C2)). Abscissas indicate calendar years. Circles indicate the observed data. Solid and dotted lines indicate the significant and nonsignificant trends of ASDR-suicide and PTD-suicide detected by joinpoint regression, respectively.
Table 3.
Summary of AAPC values of ASDR-suicide and PTD-suicide among adolescents in the global high-income, middle-income, and WPR countries from 1990 to 2019.
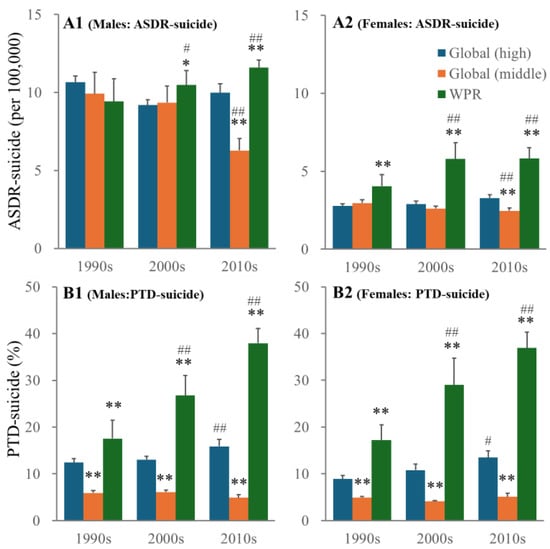
Figure 4.
ASDR-suicide and PTD-suicide among adolescent (10–24 years of age) males and females in global high-income, middle-income, and WPR countries from 1990 to 2019. Upper side panels indicate ASDR-suicide of males (A1) and females (A2). Lower side panels indicate PTD-suicide of males (B1) and females (B2). * p < 0.05, ** p < 0.01 relative to high-income countries, # p < 0.05, ## p < 0.01 relative to 1990s by two-way analysis of variance (ANOVA) with Scheffe’s post hoc test. F-values of ASDR-suicide of males and females were [Fregion(2,89) = 4.8 (p < 0.05), Fyear(2,89) = 38.4 (p < 0.01), Fregion*year(4,89) = 31.7 (p < 0.01)] and [Fregion(2,89) = 11.9 (p < 0.01), Fyear(2,89) = 22.4 (p < 0.01), Fregion*year(4,89) = 16.5 (p < 0.01)], respectively. F-values of ASDR-suicide of males and females were [Fregion(2,89) = 81.4 (p < 0.01), Fyear(2,89) = 64.7 (p < 0.01), Fregion*year(4,89) = 60.5 (p < 0.01)] and [Fregion(2,89) = 73.7 (p < 0.01), Fyear(2,89) = 62.6 (p < 0.01), Fregion*year(4,89) = 40.2 (p < 0.01)], respectively.
3.3. Adolescent ASDR-Suicide among Countries in the WPR from 1990 to 2019
The fluctuations in adolescent ASDR-suicide among countries in the WPR showed particularly complicated patterns. The ASDR-suicide of males in Australia (approximately 20) and New Zealand (approximately 30) in the 1990s was markedly higher than that in other countries (Figure 5). The ASDR-suicide of males in New Zealand consistently decreased, whereas that of males in Australia also decreased from 1990 to 2010, followed by an increase during the 2010s (U-shaped pattern) (Figure 5). Notably, the ASDR-suicide of males and females in Japan increased, but the rates in South Korea, Hong Kong, and Singapore did not change from 1990 to 2019 (Figure 5, Table 4).
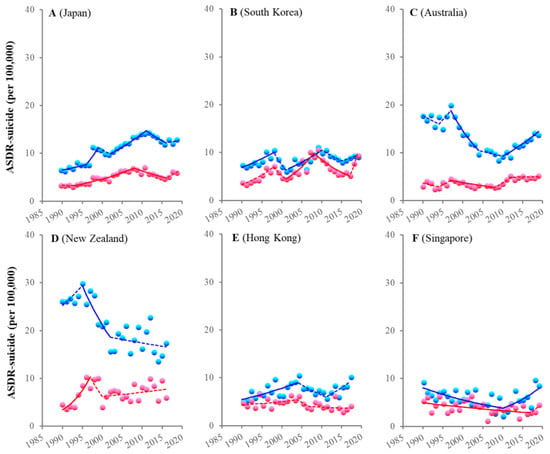
Figure 5.
Temporal fluctuations of adolescent ASDR-suicide in the WPR countries from 1990 to 2019. Temporal fluctuation of annual ASDR-suicide among adolescent males (blue) and females (red) in six countries in the WPR, including Japan (A), South Korea (B), Australia (C), New Zealand (D), Hong Kong (E), and Singapore (F), from 1990 to 2019 using joinpoint regression. Ordinates indicate the annual ASDR-suicide (per 100,000 population). Abscissas indicate calendar years. Circles indicate the observed data. Solid and dotted lines indicate the significant and nonsignificant trends of ASDR-suicide detected by joinpoint regression, respectively.
Table 4.
Summary of AAPC values of adolescent ASDR-suicide in the WPR countries from 1990 to 2019.
3.4. Adolescent PTD-Suicide among Countries in the WPR from 1990 to 2019
In contrast to the ASDR-suicide, the PTD-suicide in all the countries in the WPR increased consistently from 1990 to 2019 (Figure 6, Table 5). The PTD-suicide in all the countries in the WPR was approximately ≤20% in the 1990s; however, it then increased to over 40% (except for Singapore) (Figure 6, Table 5).
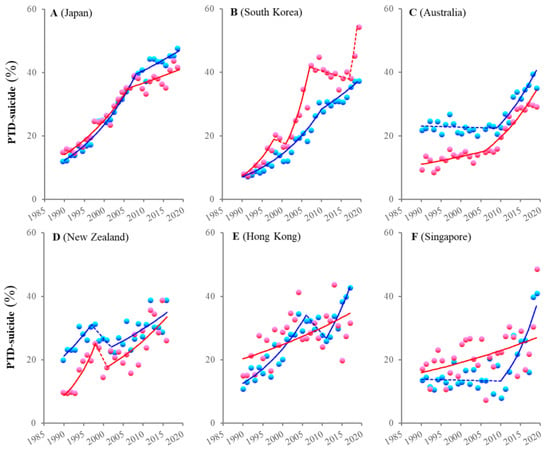
Figure 6.
Temporal fluctuations of adolescent PTD-suicide in the WPR countries from 1990 to 2019. Temporal fluctuation of annual PTD-suicide among adolescent males (blue) and females (red) in six countries in the WPR, including Japan (A), South Korea (B), Australia (C), New Zealand (D), Hong Kong (E) and Singapore (F), from 1990 to 2019 using joinpoint regression. Ordinates indicate the annual PTD-suicide (%). Abscissas indicate calendar years. Circles indicate the observed data. Solid and dotted lines indicate the significant and nonsignificant trends of PTD-suicide detected by joinpoint regression, respectively.
Table 5.
Summary of AAPC values of PTD-suicide among adolescents in the WPR countries from 1990 to 2019.
3.5. Age-Dependent Fluctuation of PTD among Global High-Income, Middle-Income, and WPR Countries from 1990 to 2019
The discrepancy in temporal fluctuation patterns between the ASDR-suicide and PTD-suicide in adolescents in the WPR probably involved a combination of a relative increase in ASDR-suicide and a decrease in the ASDR of other causes. In global high-income countries and the WPR, the leading causes of death at 10–14 and 15–24 years of age in the 1990s were cancer and traffic accidents, respectively (Figure 7 and Figure 8). The impact of cancer was consistent, whereas that of traffic accidents decreased from the 1990s to the 2010s. In contrast to traffic accidents, PTD-suicide increased, resulting in suicide becoming the leading cause of death among adolescents in global high-income countries and in the WPR (Figure 4 and Figure 5). These relations between traffic accidents and suicides were much more pronounced in the WPR in comparison with the global high-income countries (Figure 7 and Figure 8).
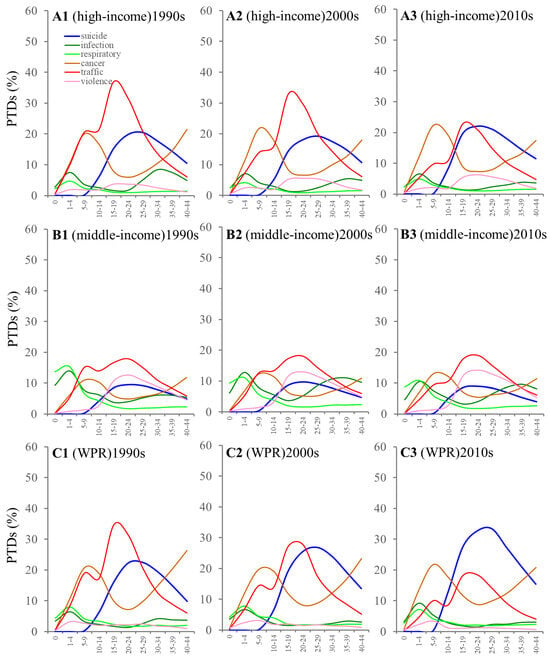
Figure 7.
Age-dependent fluctuation of PTD of major causes of death among males in global high-income, middle-income, and WPR countries from 1990 to 2019. Age-dependent fluctuation of PTD of major causes of death, such as suicide (blue), infectious and parasitic diseases (green), respiratory infections (light green), malignant neoplasms (cancer: blown), road traffic accidents (red), and violence (pink) among males in high-income (A1–A3), middle-income (B1–B3), and WPR (C1–C3) countries in the 1990s ((A1,B1,C1): 1990–1999), 2000s ((A2,B2,C2): 2000–2009), and 2010s ((A3,B3,C3): 2010–2019). Ordinates and abscissas indicate PTD (%) and 5 interval ages, respectively.
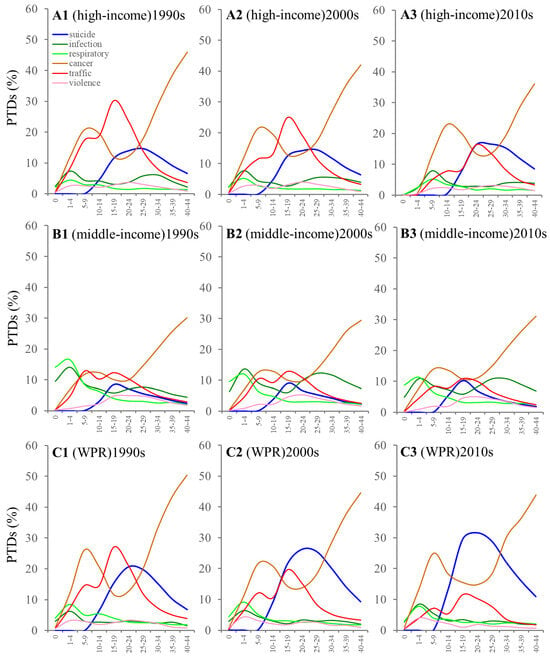
Figure 8.
Age-dependent fluctuation of PTD of major causes of death among females in global high-income, middle-income, and WPR countries from 1990 to 2019. Age-dependent fluctuation of PTD of major causes of death, such as suicide (blue), infectious and parasitic diseases (green), respiratory infections (light green), malignant neoplasms (cancer: blown), road traffic accidents (red), and violence (pink) among females in high-income (A1–A3), middle-income (B1–B3), and WPR (C1–C3) countries in the 1990s ((A1,B1,C1): 1990–1999), 2000s ((A2,B2,C2): 2000–2009), and 2010s ((A3,B3,C3): 2010–2019). Ordinates and abscissas indicate PTD (%) and 5 interval ages, respectively.
3.6. Causality Analyses for Increasing Adolescent Suicides in the WPR from 1990 to 2019
The fixed effects of the PTD caused by traffic accidents were negatively related to PTD-suicide in all male and female adolescent groups in the WPR. The fixed effects of the PTD caused by cancer were negatively related to PTD-suicide in all adolescent female groups, whereas the negative impact of cancer was only observed in males under 15 years of age (the PTD-suicide of males > 15 years of age was not related to the PTD caused by cancer) (Table 6). In the population over 20 years of age, PTD-suicide in males was negatively related to infectious and parasitic diseases, respiratory infections, traffic accidents, and violence, while PTD-suicide in males was negatively related to cancer, respiratory infections, traffic accidents, and violence. In contrast to the PTD, CMR-suicide was not related to any CMR other than suicide in any of the adolescent groups (Table 6). The increase in PTD-suicide in the WPR is assumed to be relatively attributable to deaths from causes other than suicide. However, the increase in CMR-suicide among adolescents in the WPR was not related to the CMR of other causes of death.
Table 6.
Fixed effects of other causes of death on CMR-suicide and PTD-suicide among adolescent males and females in the WPR from 1990 to 2019.
In contrast to the cause of death, the fixed effects of communication factors (penetrations of cellular telephone and Internet) on CMR-suicide and PTD-suicide showed similar relations. The penetration of cellular telephones (mobile-sub) was negatively related to CMR-suicide in males > 15 years and in females > 20 years of age and to PTD-suicide in all groups other than males < 15 years of age (Table 7). In contrast, Internet penetration (Internet-user) was positively related to PTD-suicide in males > 15 years of age and all female groups. In females, the positive impacts of Internet penetration on CMR-suicide were only detected at >20 years of age (Table 7).
Table 7.
Fixed effects of communication factors on ASDR-suicide, CMR-suicide, and PTD-suicide among adolescent males and females in the WPR from 1990 to 2019.
4. Discussion
This study revealed the common temporal fluctuations in adolescent suicide mortality underlying the recent increase in ASDR-suicide/CMR-suicide/PTD-suicide from 1990 to 2019 in the WPR. The ASDR-suicide of adolescent males in global high-income, global middle-income, and WPR countries (Australia, Hong Kong, Japan, South Korea, New Zealand, and Singapore) remained unchanged, decreased, and increased from 1990 to 2019, respectively. Conversely, in adolescent females, ASDR-suicide in global middle-income countries remained unchanged, while the rate in both the WPR and global high-income countries increased from 1990 to 2019. PTD-suicide in global middle-income countries remained unchanged from 1990 to 2019, while that in both the WPR and global high-income countries increased. These findings indicate the possibility that adolescent suicide in the WPR has emerged as a major public health issue compared with other regions from 1990 to 2019 (before the COVID-19 pandemic outbreak). This possibility is supported by the fact that in the 1990s, PTD-suicide in the WPR and global high-income countries was almost equal (approximately 15%), while in the 2010s, PTD-suicide increased to approximately 20% in the global high-income countries and 40% in the WPR. The fixed effects of cellular telephone penetration contributed to a decrease in adolescent suicide, while Internet penetration contributed to an increase in adolescent suicide. The findings of this study suggest that medical and public health measures in the WPR have promoted adolescent health; however, some challenges related to communication factors, such as excessive use of the Internet, might, at least partially, have had serious negative impacts and act as risk factors for adolescent suicide in the WPR from 1990 to 2019 (before the COVID-19 pandemic outbreak).
4.1. Characteristics of Fluctuation of Adolescent Suicide in the WPR
The increasing fluctuation pattern of adolescent ASDR-suicide in the WPR was greater than that observed in the global high-income countries, but the patterns of fluctuation were not identical in each country in the WPR. In the 1990s, the ASDR-suicide of adolescent males in both Australia (approximately 20) and New Zealand (approximately 30) was markedly higher in comparison with the other WPR countries and then decreased from the 1990s to the early 2010s. It is well known that the ASDR-suicide/CMR-suicide of overall age in Asian countries sharply increased after the Asian financial crisis in 1997 [6,57,58,59,60]. A nonsignificant increase in adolescent ASDR-suicide, which synchronized with the Asian financial crisis, was observed in both Japan and South Korea. National/government suicide prevention programs were implemented in Australia, New Zealand, South Korea, and Japan in 1992, 1996, 2004, and 2007, respectively [21,34,61,62,63]. For several years after the implementation of the national/governmental suicide prevention programs, adolescent ASDR-suicide decreased; this decreasing trend continued for approximately 10 years, followed by an attenuation of the decreasing trend or a transformation to an increasing trend. In contrast, the fluctuation pattern of PTD-suicide shows a consistent increase in the WPR countries. Furthermore, in the 2010s, PTD-suicide among adolescent males and females consistently increased in all the WPR countries. It is well known that the sex ratio (males/females) of suicide mortality in Asia is consistently lower than that in Western countries [6,13,64,65,66]. In South Korea, surprisingly, the PTD-suicide of female adolescents was higher in comparison with that of males, with the male-to-female sex ratio of ASDR-suicide in South Korea being lower than that in other countries in the WPR, indicating that adolescent female suicide in South Korea is dominant in comparison with other countries.
Considering the findings obtained from the causality analyses, the drastic increase in adolescent PTD-suicide in the WPR is considered to be the result of the interaction between decreasing death from other causes and increasing adolescent suicide, but the increase in adolescent ASDR-suicide itself is not affected by the decrease in other causes of death. Therefore, the measures promoting adolescent public health have successfully contributed to a decrease in overall adolescent deaths from causes other than suicide but may have made relatively little progress in reducing suicide compared with other targets.
4.2. Impacts of Communication Tool Factors on Adolescent Suicide in the WPR
In this century, communication methods have drastically transformed with the advent of the cellular telephone and the Internet. During the COVID-19 pandemic, social restrictions to suppress the pandemic made digital communication tools even more important, resulting in both cellular telephones and the Internet becoming essential social infrastructures for education, recreation, and communication with peers [39,40,41]. However, it is concerning that increased Internet usage has been related to increased health-risk behaviors, including suicide [42,43,45,46]. In this study, cellular telephone penetration consistently suppressed suicide among adolescents, whereas increasing opportunities for Internet usage possibly contributed to the increase in adolescent suicides. Considering that the cellular telephone is a major terminal of Internet access, this discrepancy suggests that the cellular telephone is an essential and useful communication tool for the majority of adolescents but that Internet use may be a risk factor for suicide for some vulnerable adolescents. The adverse health consequences associated with inappropriate Internet use, especially among students, are a matter of concern [43,44]. The prevalence of Internet addiction is increasing over time, with increasing Internet penetration [44]. In the relevant literature, the major discourse regarding social media use and the risk factors for adolescent health has focused on the frequency of Internet use, such as screen time; currently, however, Internet use patterns are being evaluated to better understand the adverse health consequences, including suicide among adolescents [43,44,67].
Although this study did not analyze the impacts of Internet use patterns on suicide mortality, the fixed effects of Internet penetration on national-level adolescent suicides in the WPR indicated that there was a positive relationship. The fixed-effects model can control for unobserved time-invariant factors, such as culture, climate, and economic and educational situation (as well as sleep, diet, exercise, and social rhythms), which may affect the incidence or mortality induced by Internet use, resulting in an effect on regional suicide mortality rates each period [68,69,70]. The present study adopted robust standard errors, clustered according to the countries in the WPR, to prevent heteroscedasticity and autocorrelation. Given the advantages of fixed-effect analysis using the hierarchical linear regression model with robust standard errors, the positive impacts of increasing Internet penetration on adolescent suicides in the WPR, as demonstrated in this study, cannot be ignored.
This study detected interesting findings regarding the impacts of Internet penetration on adolescent suicide mortality. Internet penetration was positively related to the female adolescent PTD-suicide of those aged 10–24 and the male PTD-suicide of those aged 15–24, but it was not related to the PTD-suicide of those aged 10–15. Additionally, the β-values (coefficients) of the HLM of the female PTD-suicide were larger than those of the males among all the age groups. These results suggest the possibility that the increasing Internet penetration was probably involved, at least partially, in drastically increasing the female adolescent PTD-suicide in the WPR in the 2010s. Various studies conducted after 2010 support the possibility that females are more likely to suffer from the health hazards caused by the Internet than males. The Internet or social media exposure times of female adolescents are greater than those of male adolescents, and female adolescents use the Internet more actively than males [43]. Female adolescents are also more likely to be victims of cyberbullying compared with males [71]. There have even been reported findings showing that the association between Internet-based behavior and mental health deterioration, such as depression and suicide risks, was predominant in female adolescents in comparison with males [72,73,74]. Considering these previous findings, the results in this study emphasize the importance of exploring the impacts of the penetration of the Internet on female adolescent suicides compared with male suicides.
The sex ratio of PTD-suicide was particularly low in South Korea and Japan, among the WPR countries. Traditionally, it is well known that in both countries, hanging has been the leading method of suicide compared with the methods used in the United States and Australia [64]. In 2024, a very shocking finding regarding the sex differences in suicides in Japan was reported [75]. The association between suicides and mosaic chromosomal alterations, including mosaic loss of the X and Y chromosomes, revealed that mosaic losses of the X chromosome were significantly increased in female suicide [75]. This finding is preliminary, but it may indicate the impacts of genetic backgrounds on suicide mortality and the sex differences in suicides in Japan.
4.3. Limitation
The present study was associated with several limitations. To identify the regional features of adolescent suicide mortality in the WPR, this study determined the temporal fluctuations of various suicide values (ASDR-suicide, CMR-suicide, and PTD-suicide) in the WPR, including Australia, Hong Kong, Japan, South Korea, New Zealand, and Singapore, using the WHO Mortality Database. However, all six countries are high-income countries. The WHO Mortality Database published suicide statistics for middle-income countries in the WPR, including Malaysia, the Philippines, and Thailand. The suicide statistics of these three middle-income countries in the WPR were incomplete and had numerous missing values, which made it impossible to perform an accurate statistical analysis. The data from China, which has the largest population and number of suicides in the WPR [76,77,78], were also not published in the WHO Mortality Database. To clarify the actual features of adolescent suicides in the WPR, it is necessary to conduct analyses that include suicide mortality in middle-income countries in the WPR.
This was a cross-sectional observational study that may have been subject to an ecological fallacy [79,80]. Comparisons of suicide mortality across different populations over the same period or within the same population over time are subject to confounding. Considering the ecological fallacy, the positive impact of Internet penetration on suicide mortality among adolescents in the WPR should be clarified through more detailed analyses.
In order to identify the actual circumstances of suicide, it is necessary to determine the suicidal behavior, which is composed of completed suicide, the suicide attempt, and suicidal ideation [81]. However, this study could not conduct a survey that included suicidal ideation and suicide attempts, since this study analyzed the data from the WHO Mortality Database.
5. Conclusions
This cross-sectional study revealed the existence of specific patterns of fluctuation in adolescent ASDR-suicide/CMR-suicide among six high-income countries in the WPR in comparison with global high- and middle-income countries. In the 1990s, male ASDR-suicide in Oceanian countries (Australia and New Zealand) was markedly higher than in other countries, whereas, after the implementation of national/government suicide prevention programs, ASDR-suicide in these countries decreased. ASDR-suicide in Japan and South Korea also decreased after the implementation of national/government suicide prevention programs in the 2000s. Surprisingly, despite these efforts, in the late 2010s, ASDR-suicide among adolescents in the WPR increased. The increasing penetration of cellular telephones is a protective factor for adolescent suicide, while the increasing penetration of the Internet is a risk factor. In contrast to ASDR-suicide, PTD-suicide consistently increased in all countries in the WPR from 1990 to 2019. Therefore, among adolescent health activities, the importance of suicide prevention in the WPR has been increasing in comparison with other regions in the current century. Considering the discrepancy between the effects of the penetrations of cellular telephones and the Internet on adolescent suicide mortality, analyses of both the actual state of Internet usage in adolescents and the impact of Internet usage patterns on adolescent suicide mortality should be required in the development of guidelines for appropriate Internet use for vulnerable adolescents. An examination of the temporal fluctuations of adolescent suicide mortalities in the WPR before the COVID-19 pandemic outbreak, from 1990 to 2019 (for 30 years), using the WHO Mortality Database, could strengthen the validity of the findings from this study. When the annual numbers of suicides during and after the COVID-19 pandemic are published in the WHO Mortality Database, the findings from this study could contribute to a more detailed understanding of the impact of COVID-19 and its side effects on suicide mortality through analyses with an extended observation period.
Author Contributions
M.O. had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. R.O. and R.M., concept and design, acquisition, analysis, or interpretation of data, drafting of the manuscript, critical review of the manuscript for important intellectual content, statistical analysis, obtained funding; E.M., acquisition, analysis, or interpretation of data, drafting of the manuscript and statistical analysis; M.O., concept and design, acquisition, analysis, or interpretation of data, drafting of the manuscript, critical review of the manuscript for important intellectual content, statistical analysis, obtained funding, administrative, technical, or material support, and supervision. All authors have read and agreed to the published version of the manuscript.
Funding
This study is supported by the Japan Society for the Promotion of Science (23K06987) and the Regional Suicide Countermeasures Emergency Enhancement Fund of Mie Prefecture (2024-40). The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the JSPS or Mie Prefecture. The funder played no role in the study design, in the collection, analysis, or interpretation of the data, in the writing of the paper, or in the decision to submit the article for publication. All authors were independent from the funders.
Institutional Review Board Statement
The Medical Ethics Review Committee of Mie University waived the need for ethical approval due to the use of publicly available governmental data.
Informed Consent Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
Data Availability Statement
All raw data are publicly available to any persons via the databases in WHO (https://www.who.int/data/data-collection-tools/who-mortality-database), World Bank (https://data.worldbank.org/indicator) (accessed on 11 September 2024), and ITU (https://datahub.itu.int/data/) (accessed on 11 September 2024). Participant consent for data sharing was not obtained, but the presented data are anonymized by WHO and all governments, and the risk of identification is none.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Sawyer, S.M.; Azzopardi, P.S.; Wickremarathne, D.; Patton, G.C. The age of adolescence. Lancet Child Adolesc. Health 2018, 2, 223–228. [Google Scholar] [CrossRef] [PubMed]
- WHO. Adolescent and Young Adult Health. Available online: https://www.who.int/news-room/fact-sheets/detail/adolescents-health-risks-and-solutions (accessed on 4 January 2024).
- Azevedo, J.P.; Banerjee, A.; Wilmoth, J.; Fu, H.; You, D. Hard truths about under-5 mortality: Call for urgent global action. Lancet 2024, 404, 506–508. [Google Scholar] [CrossRef] [PubMed]
- Collaborators, G.B.D.A.M. Global, regional, and national mortality among young people aged 10–24 years, 1950–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2021, 398, 1593–1618. [Google Scholar] [CrossRef]
- Collaborators, G.B.D.C.o.D. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990–2021: A systematic analysis for the Global Burden of Disease Study 2021. Lancet 2024, 403, 2100–2132. [Google Scholar] [CrossRef]
- Chen, Y.Y.; Wu, K.C.; Yousuf, S.; Yip, P.S. Suicide in Asia: Opportunities and challenges. Epidemiol. Rev. 2012, 34, 129–144. [Google Scholar] [CrossRef] [PubMed]
- Han, C.S.; Ogrodniczuk, J.S.; Oliffe, J.L. Qualitative research on suicide in East Asia: A scoping review. J. Ment. Health 2013, 22, 372–383. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.A.; Courtwright, A.; Wu, K.C. The Role of Stigma and Denormalization in Suicide-Prevention Laws in East Asia: A Sociocultural, Historical, and Ethical Perspective. Harv. Rev. Psychiatry 2017, 25, 229–240. [Google Scholar] [CrossRef]
- Vijayakumar, L. Suicide in women. Indian J. Psychiatry 2015, 57, S233–S238. [Google Scholar] [CrossRef]
- Phillips, M.R. Rethinking the role of mental illness in suicide. Am. J. Psychiatry 2010, 167, 731–733. [Google Scholar] [CrossRef]
- Hughes, J.L.; Horowitz, L.M.; Ackerman, J.P.; Adrian, M.C.; Campo, J.V.; Bridge, J.A. Suicide in young people: Screening, risk assessment, and intervention. BMJ 2023, 381, e070630. [Google Scholar] [CrossRef]
- WHO. Suicide. Available online: https://www.who.int/news-room/fact-sheets/detail/suicide (accessed on 28 August 2023).
- Naghavi, M.; Global Burden of Disease Self-Harm, C. Global, regional, and national burden of suicide mortality 1990 to 2016: Systematic analysis for the Global Burden of Disease Study 2016. BMJ 2019, 364, l94. [Google Scholar] [CrossRef] [PubMed]
- Parry, J. Falling suicide rates in China mask emerging upward trends. BMJ 2014, 348, g4486. [Google Scholar] [CrossRef] [PubMed]
- Turecki, G.; Brent, D.A.; Gunnell, D.; O’Connor, R.C.; Oquendo, M.A.; Pirkis, J.; Stanley, B.H. Suicide and suicide risk. Nat. Rev. Dis. Primers 2019, 5, 74. [Google Scholar] [CrossRef] [PubMed]
- Saxena, S.; Setoya, Y. World Health Organization’s Comprehensive Mental Health Action Plan 2013–2020. Psychiatry Clin. Neurosci. 2014, 68, 585–586. [Google Scholar] [CrossRef] [PubMed]
- Okada, M.; Matsumoto, R.; Motomura, E.; Shiroyama, T.; Murata, M. Exploring characteristics of increased suicide during the COVID-19 pandemic in Japan using provisional governmental data. Lancet Reg. Health–West. Pac. 2022, 24, 100481. [Google Scholar] [CrossRef]
- Okada, M.; Matsumoto, R.; Shiroyama, T.; Motomura, E. Suicidal Mortality and Motives among Middle-School, High-School and University Students. JAMA Netw. Open 2023, 6, e2328144. [Google Scholar] [CrossRef]
- Lange, S.; Cayetano, C.; Jiang, H.; Tausch, A.; Oliveira, E.S.R. Contextual factors associated with country-level suicide mortality in the Americas, 2000–2019: A cross-sectional ecological study. Lancet Reg. Health–Am. 2023, 20, 100450. [Google Scholar] [CrossRef]
- Bertuccio, P.; Amerio, A.; Grande, E.; La Vecchia, C.; Costanza, A.; Aguglia, A.; Berardelli, I.; Serafini, G.; Amore, M.; Pompili, M.; et al. Global trends in youth suicide from 1990 to 2020: An analysis of data from the WHO mortality database. EClinicalMedicine 2024, 70, 102506. [Google Scholar] [CrossRef]
- Matsumoto, R.; Motomura, E.; Shiroyama, T.; Okada, M. Impact of the Japanese government’s “general policies for comprehensive measures against suicide” on youth suicide from 2007–2022. BJPsy Open 2023, 10, e16. [Google Scholar] [CrossRef]
- Okada, M. Suicide mortality rates in Japan before and beyond the COVID-19 pandemic era. Psychiatry Clin. Neurosci. Rep. 2024, 3, e188. [Google Scholar] [CrossRef]
- Mahase, E. US suicide rates in young people are highest since 2000. BMJ 2019, 365, l4289. [Google Scholar] [CrossRef] [PubMed]
- Kolves, K.; De Leo, D. Adolescent Suicide Rates between 1990 and 2009: Analysis of Age Group 15–19 Years Worldwide. J. Adolesc. Health 2016, 58, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Okada, M. Is an increase in Japan’s suicides caused by COVID-19 alone? Asian J. Psychiatry 2022, 78, 103320. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, R.; Motomura, E.; Okada, M. Fluctuation of suicide mortality and temporal causality from unemployment duration to suicide mortality in Japan during 2009–2022. Asian J. Psychiatry 2023, 84, 103574. [Google Scholar] [CrossRef]
- Stuckler, D.; Basu, S.; Suhrcke, M.; Coutts, A.; McKee, M. The public health effect of economic crises and alternative policy responses in Europe: An empirical analysis. Lancet 2009, 374, 315–323. [Google Scholar] [CrossRef]
- Kieling, C.; Baker-Henningham, H.; Belfer, M.; Conti, G.; Ertem, I.; Omigbodun, O.; Rohde, L.A.; Srinath, S.; Ulkuer, N.; Rahman, A. Child and adolescent mental health worldwide: Evidence for action. Lancet 2011, 378, 1515–1525. [Google Scholar] [CrossRef]
- Karanikolos, M.; Mladovsky, P.; Cylus, J.; Thomson, S.; Basu, S.; Stuckler, D.; Mackenbach, J.P.; McKee, M. Financial crisis, austerity, and health in Europe. Lancet 2013, 381, 1323–1331. [Google Scholar] [CrossRef]
- Collaborators, G.B.D.D. Global age-sex-specific fertility, mortality, healthy life expectancy (HALE), and population estimates in 204 countries and territories, 1950–2019: A comprehensive demographic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1160–1203. [Google Scholar] [CrossRef]
- Borowsky, I.W.; Ireland, M.; Resnick, M.D. Adolescent suicide attempts: Risks and protectors. Pediatrics 2001, 107, 485–493. [Google Scholar] [CrossRef]
- Mann, J.J.; Waternaux, C.; Haas, G.L.; Malone, K.M. Toward a clinical model of suicidal behavior in psychiatric patients. Am. J. Psychiatry 1999, 156, 181–189. [Google Scholar] [CrossRef]
- Hawton, K.; Harriss, L. Deliberate self-harm in people aged 60 years and over: Characteristics and outcome of a 20-year cohort. Int. J. Geriatr. Psychiatry 2006, 21, 572–581. [Google Scholar] [CrossRef] [PubMed]
- Beautrais, A.; Fergusson, D.; Coggan, C.; Collings, C.; Doughty, C.; Ellis, P.; Hatcher, S.; Horwood, J.; Merry, S.; Mulder, R.; et al. Effective strategies for suicide prevention in New Zealand: A review of the evidence. N. Z. Med. J. 2007, 120, U2459. [Google Scholar] [PubMed]
- Choo, C.C.; Chew, P.K.H.; Ho, R.C. Suicide Precipitants Differ Across the Lifespan but Are Not Significant in Predicting Medically Severe Attempts. Int. J. Environ. Res. Public Health 2018, 15, 691. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.H.; Kim, D.H. Trend of Suicide Rates According to Urbanity among Adolescents by Gender and Suicide Method in Korea, 1997–2012. Int. J. Environ. Res. Public Health 2015, 12, 5129–5142. [Google Scholar] [CrossRef] [PubMed]
- Pompili, M.; Vichi, M.; De Leo, D.; Pfeffer, C.; Girardi, P. A longitudinal epidemiological comparison of suicide and other causes of death in Italian children and adolescents. Eur. Child Adolesc. Psychiatry 2012, 21, 111–121. [Google Scholar] [CrossRef]
- Bilsen, J. Suicide and Youth: Risk Factors. Front. Psychiatry 2018, 9, 540. [Google Scholar] [CrossRef]
- Exner-Cortens, D.; Baker, E.; Gray, S.; Fernandez Conde, C.; Rivera, R.R.; Van Bavel, M.; Vezina, E.; Ambrose, A.; Pawluk, C.; Schwartz, K.D.; et al. School-Based Suicide Risk Assessment Using eHealth for Youth: Systematic Scoping Review. JMIR Ment. Health 2021, 8, e29454. [Google Scholar] [CrossRef]
- Gunasekeran, D.V.; Chew, A.; Chandrasekar, E.K.; Rajendram, P.; Kandarpa, V.; Rajendram, M.; Chia, A.; Smith, H.; Leong, C.K. The Impact and Applications of Social Media Platforms for Public Health Responses before and during the COVID-19 Pandemic: Systematic Literature Review. J. Med. Internet Res. 2022, 24, e33680. [Google Scholar] [CrossRef]
- Salas-Pilco, S.Z.; Yang, Y.; Zhang, Z. Student engagement in online learning in Latin American higher education during the COVID-19 pandemic: A systematic review. Br. J. Educ. Technol. 2022, 53, 593–619. [Google Scholar] [CrossRef]
- Matsumoto, R.; Kawano, Y.; Motomura, E.; Shiroyama, T.; Okada, M. Analyzing the Changing Relationship between Personal Consumption and Suicide Mortality during COVID-19 Pandemic in Japan, using governmental and personal consumption transaction databases. Front. Public Health 2022, 10, 982341. [Google Scholar] [CrossRef]
- Nesi, J.; Burke, T.A.; Bettis, A.H.; Kudinova, A.Y.; Thompson, E.C.; MacPherson, H.A.; Fox, K.A.; Lawrence, H.R.; Thomas, S.A.; Wolff, J.C.; et al. Social media use and self-injurious thoughts and behaviors: A systematic review and meta-analysis. Clin. Psychol. Rev. 2021, 87, 102038. [Google Scholar] [CrossRef] [PubMed]
- Chung, T.W.H.; Sum, S.M.Y.; Chan, M.W.L. Adolescent Internet Addiction in Hong Kong: Prevalence, Psychosocial Correlates, and Prevention. J. Adolesc. Health 2019, 64, S34–S43. [Google Scholar] [CrossRef]
- Wang, J.; Hao, Q.H.; Tu, Y.; Peng, W.; Wang, Y.; Li, H.; Zhu, T.M. Assessing the Association Between Internet Addiction Disorder and Health Risk Behaviors among Adolescents and Young Adults: A Systematic Review and Meta-Analysis. Front. Public Health 2022, 10, 809232. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.S.; Tseng, P.T.; Lin, P.Y.; Chen, T.Y.; Stubbs, B.; Carvalho, A.F.; Wu, C.K.; Chen, Y.W.; Wu, M.K. Internet Addiction and Its Relationship with Suicidal Behaviors: A Meta-Analysis of Multinational Observational Studies. J. Clin. Psychiatry 2018, 79, 9291. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Mortality Database. Available online: https://www.who.int/data/data-collection-tools/who-mortality-database (accessed on 6 January 2024).
- ITU. International Telecommunication Union. Available online: https://datahub.itu.int/data/ (accessed on 6 January 2024).
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gotzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; Initiative, S. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. PLoS Med. 2007, 4, e297. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, O.B.; Boschi-Pinto, C.; Lopez, A.D.; Murray, C.J.; Lozano, R.; Inoue, M. Age standardization of rates: A new WHO standard. In GPE Discussion Paper Series: No.31; World Health Organization: Geneva, Switzerland, 2001; Volume 9. [Google Scholar]
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- NCI. Joinpoint Regression Program ver4.9.1.0. Available online: https://surveillance.cancer.gov/joinpoint/ (accessed on 8 January 2022).
- Raudenbush, S.W.; Bryk, A.S. Hierarchical Linear Models: Applications and Data Analysis Methods; Sage: Newcastle upon Tyne, UK, 2002; Volume 1. [Google Scholar]
- Kashimoto, K.; Okada, M. Analysing the Impacts of Financial Expenditure of Prefectures on Methods of Suicide Completion in Japan. Psychiatry Int. 2021, 3, 1–16. [Google Scholar] [CrossRef]
- Mangalam, M.; Kelty-Stephen, D.G. Point estimates, Simpson’s paradox, and nonergodicity in biological sciences. Neurosci. Biobehav. Rev. 2021, 125, 98–107. [Google Scholar] [CrossRef]
- Okada, M.; Fukuyama, K.; Motomura, E. Impacts of exposure to and subsequent discontinuation of clozapine on tripartite synaptic transmission. Br. J. Pharmacol. 2024. [Google Scholar] [CrossRef]
- Huikari, S.; Miettunen, J.; Korhonen, M. Economic crises and suicides between 1970 and 2011: Time trend study in 21 developed countries. J. Epidemiol. Community Health 2019, 73, 311–316. [Google Scholar] [CrossRef]
- Jeon, S.Y.; Reither, E.N.; Masters, R.K. A population-based analysis of increasing rates of suicide mortality in Japan and South Korea, 1985–2010. BMC Public Health 2016, 16, 356. [Google Scholar] [CrossRef] [PubMed]
- Soleymani, M.; Yip, P.S.F. Assessing the impact of the economic crises in 1997 and 2008 on suicides in Hong Kong, Taiwan and South Korea using a strata-bootstrap algorithm. J. Appl. Stat. 2020, 47, 666–684. [Google Scholar] [CrossRef] [PubMed]
- Uutela, A. Economic crisis and mental health. Curr. Opin. Psychiatry 2010, 23, 127–130. [Google Scholar] [CrossRef]
- Wang, S.S.; Eapen, V.; Lin, P.I. The relationship between mental health reforms and general population suicide rates in Australia over the past three and a half decades: 1987–2021. Psychiatry Res. 2024, 335, 115884. [Google Scholar] [CrossRef]
- Gong, A.K.; Yun, J.H.; Kim, I.S.; Yuh, M.A.; Woo, S.H.; Kim, J.; Hong, S. Factors Affecting Emergency Medical Utilization after Self-harm and Effectiveness of Community-Based Suicide Prevention Provisions in Preventing Self-harm: A Nationwide Registry-Based Study in Korea. Community Ment. Health J. 2023, 59, 942–953. [Google Scholar] [CrossRef] [PubMed]
- Kato, R.; Okada, M. Can Financial Support Reduce Suicide Mortality Rates? Int. J. Environ. Res. Public Health 2019, 16, 4797. [Google Scholar] [CrossRef]
- Hee Ahn, M.; Park, S.; Ha, K.; Choi, S.H.; Hong, J.P. Gender ratio comparisons of the suicide rates and methods in Korea, Japan, Australia, and the United States. J. Affect. Disord. 2012, 142, 161–165. [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, Y.; Cho, Y.T.; Obayashi, Y.; Arai, A.; Tamashiro, H. Gender differences of suicide in Japan, 1947–2010. J. Affect. Disord. 2013, 151, 325–330. [Google Scholar] [CrossRef]
- Chang, Y.H.; Gunnell, D.; Hsu, C.Y.; Chang, S.S.; Cheng, A.T. Gender difference in suicide in Taiwan over a century: A time trend analysis in 1905–1940 and 1959–2012. J. Epidemiol. Community Health 2020, 74, 898–906. [Google Scholar] [CrossRef]
- Odgers, C.L.; Jensen, M.R. Annual Research Review: Adolescent mental health in the digital age: Facts, fears, and future directions. J. Child Psychol. Psychiatry 2020, 61, 336–348. [Google Scholar] [CrossRef]
- Kerr, W.C.; Kaplan, M.S.; Huguet, N.; Caetano, R.; Giesbrecht, N.; McFarland, B.H. Economic Recession, Alcohol, and Suicide Rates: Comparative Effects of Poverty, Foreclosure, and Job Loss. Am. J. Prev. Med. 2017, 52, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Goto, H.; Kawachi, I.; Vandoros, S. The association between economic uncertainty and suicide in Japan by age, sex, employment status, and population density: An observational study. Lancet Reg. Health–West. Pac. 2024, 46, 101069. [Google Scholar] [CrossRef] [PubMed]
- Matsubayashi, T.; Ueda, M. The effect of national suicide prevention programs on suicide rates in 21 OECD nations. Soc. Sci. Med. 2011, 73, 1395–1400. [Google Scholar] [CrossRef] [PubMed]
- Hamm, M.P.; Newton, A.S.; Chisholm, A.; Shulhan, J.; Milne, A.; Sundar, P.; Ennis, H.; Scott, S.D.; Hartling, L. Prevalence and Effect of Cyberbullying on Children and Young People: A Scoping Review of Social Media Studies. JAMA Pediatr. 2015, 169, 770–777. [Google Scholar] [CrossRef] [PubMed]
- Booker, C.L.; Kelly, Y.J.; Sacker, A. Gender differences in the associations between age trends of social media interaction and well-being among 10–15 year olds in the UK. BMC Public Health 2018, 18, 321. [Google Scholar] [CrossRef]
- Nesi, J.; Prinstein, M.J. Using Social Media for Social Comparison and Feedback-Seeking: Gender and Popularity Moderate Associations with Depressive Symptoms. J. Abnorm. Child Psychol. 2015, 43, 1427–1438. [Google Scholar] [CrossRef]
- Twenge, J.M.; Martin, G.N. Gender differences in associations between digital media use and psychological well-being: Evidence from three large datasets. J. Adolesc. 2020, 79, 91–102. [Google Scholar] [CrossRef]
- Otsuka, I.; Uchiyama, S.; Shirai, T.; Liu, X.; Takahashi, M.; Kamatani, Y.; Terao, C.; Hishimoto, A. Increased somatic mosaicism in autosomal and X chromosomes for suicide death. Mol. Psychiatry 2024. [Google Scholar] [CrossRef]
- Wu, Y.; Su, B.; Zhong, P.; Wang, Y.; Huang, Y.; Zheng, X. The long-term changing patterns of suicide mortality in China from 1987 to 2020: Continuing urban-rural disparity. BMC Public Health 2024, 24, 1269. [Google Scholar] [CrossRef]
- Tian, Y.; Luan, M.; Chen, H.; Zhang, J. Temporal Trend in Suicide Mortality for Chinese Adolescents, 2008 to 2021. JAMA Pediatr. 2023, 177, 1224–1226. [Google Scholar] [CrossRef]
- Ji, Z.; Wu, H.; Zhu, R.; Wang, L.; Wang, Y.; Zhang, L. Trends in Cause-Specific Injury Mortality in China in 2005–2019: Longitudinal Observational Study. JMIR Public Health Surveill. 2023, 9, e47902. [Google Scholar] [CrossRef] [PubMed]
- Silva Junior, F.; Miranda, P.I.G.; Sales, J.; Parente, A.; Monteiro, C.F.S.; Costa, A.P.C.; Campos, L.R.B.; Lima, L.A.A.; Ibiapina, A.R.S.; Pillon, S.C.; et al. Suicidal behaviour in adults during the COVID-19 pandemic: Protocol for systematic review of observational studies. BMJ Open 2021, 11, e045313. [Google Scholar] [CrossRef] [PubMed]
- Favril, L.; Yu, R.; Geddes, J.R.; Fazel, S. Individual-level risk factors for suicide mortality in the general population: An umbrella review. Lancet Public Health 2023, 8, e868–e877. [Google Scholar] [CrossRef] [PubMed]
- Cocchio, S.; Tremolada, G.; Cogo, N.; Cozzolino, C.; Saia, M.; Tonon, M.; Russo, F.; Furlan, P.; Fonzo, M.; Baldo, V. Hospitalizations for Suicidal Events: Reiteration Risk—The Experience in the Veneto Region, Italy. Psychiatry Int. 2024, 5, 434–446. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).