1. Introduction
The International Diabetes Foundation estimates that there are 537 million people globally who have diabetes and up to 1/3 will develop a diabetic foot ulcer (DFU) over their lifetime [
1]. Recurrence rates are high with 40% of DFUs recurring within one year, and 65% recur within 5 years [
2].
Those who develop a DFU have a 5-year mortality rate of nearly 50% [
3]. DFU is the leading cause of lower limb amputations and more than half of the people who have a lower extremity amputation die within five years [
4].
DFU contributing factors include neuropathy, poor blood flow, minor repetitive trauma (e.g., poor-fitting footwear), and infection following an injury. Diabetic neuropathy causes a lack of sensation in the feet, making the person vulnerable to undetected injury. Neural autonomic dysfunction associated with diabetes causes impaired sweat production, resulting in susceptibility to dryness and the cracking of the foot. In addition, motor neuron dysfunction associated with diabetes causes muscle wasting and structural deformities (such as Charcot foot), resulting in pressure points for ulcer development [
5]. Once wounds occur, they would normally go through the stages of healing: hemostasis, inflammation, proliferation, and remodeling in a linear fashion. However, DFUs stall in one or more of these phases. Wounds that are chronic are thought to stagnate between the inflammatory and proliferative stage, leading to increased inflammation and a lack of tissue rebuilding. Increasing bacterial bioburden contributes to the development of biofilms, which are hard to remove during routine wound care. These biofilms form in about 60% of all chronic wounds and may be present as early as 10 h after wound formation [
4]. In persons with diabetes, hyperglycemia causes a proinflammatory environment, leading to a complex molecular cascade of events that inhibit wound healing. Because of the pathologic complexity of DFUs, many wounds go unrecognized until severe symptoms have developed [
3].
Poor blood flow to a DFU is usually related to peripheral artery disease (PAD) causing restricted peripheral blood supply, resulting in a poor response to injury. Critical limb ischemia (CLI) is the advanced stage of PAD where there is an occlusion of the arteries in the extremity. CLI causes ischemic pain and leads to DFU development and gangrene [
6]. The mortality rate for people with CLI can be 24% in the first year after diagnosis and 60% over 5 years [
4]. PAD is associated with higher rates of amputation in persons with DFUs and can contribute to increased minor (toe/forefoot) as well as major amputations. Major amputations include Below-Knee Amputation (BKA), also referred to as Transtibial Amputation (TTA), or Above-Knee Amputation (AKA), also referred to as Transfemoral Amputation (TFA).
The only effective preventive measure for DFU is regular diabetic foot screening [
3]. Those who develop a DFU have a 5-year mortality rate of nearly 50% [
3]. DFU is the leading cause of lower limb amputations and more than half of the people who have a lower extremity amputation die within five years [
4]. In a systematic review of 67 studies by Zhang et al., in 2017, the highest prevalence of DFU was in North America with 13% [
5].
Currently, DFU treatment is not standardized and often very challenging. Although comprehensive wound care, provided by a multidisciplinary team, is the key to optimal outcomes, the mortality rate for diabetic patients with DFUs is still very high. However, a multidisciplinary team can reduce lower limb amputations related to diabetes. The composition of the team may vary but usually includes a specialty provider (infectious disease, endocrinologist, wound specialist) and two or more surgical specialty providers (vascular, podiatric, orthopedic, and wound care or plastic surgeon). The implementation of a multidisciplinary team approach reduces the pooled OR for amputation by 0.40 [
7].
The mainstays of DFU treatment are debridement, off-loading, early recognition, and the appropriate management of infection and selection of a wound dressing that optimizes the wound environment and ensures patient/family compliance. Even with adequate care, 20% of foot infections will progress to osteomyelitis.
Debridement is a standard treatment for DFUs and practice guidelines recommend debridement weekly or bi-weekly. Weekly debridement has shown a significant increase in healing of DFUs when compared to less frequent debridement [
2].
Off-loading is an important part of treatment as well. Off-loading spreads the weight and force of the foot over a larger area, allowing healing to take place. Off-loading is best accomplished by a total contact cast or a knee-high walker, which reduces pressure at the ulcer site by up to 80–90% when compared to a standard shoe [
2].
Wound dressings need to consider the wound characteristics, including inflammation. Generally, the dressing should provide a moist environment, promoting tissue growth and epithelial cells from around the wound to migrate, providing a sheet to cover the open wound. Several new topical agents have been trialed to support these wound healing activities, such as topical fibrin and placenta products [
2].
Other therapies, such as hyperbaric oxygen therapy, have been evaluated as adjunct treatment in DFU patients who have failed standard treatment. Negative-pressure wound therapy has been used in patients with complications or post-operative DFU wounds. It seems most effective in decreasing wound depth and developing a bed of granulation tissue for healing with skin grafts [
2]. NPWT placed on plantar ulcers is challenging given that even with minimal weight bearing, the potential to break the seal is increased, thus disrupting the therapy.
In patients with critical limb ischemia from PAD, revascularization is imperative. One retrospective study found that patients waiting more than 14 days for revascularization had a higher rate of major amputations (OR 3.1) than those who had early revascularization [
8]. There are, however, many patients for whom surgical revascularization is not an option either due to co-morbidities and risk or the lack of viable surgical options.
When infection is involved, delivering antibiotics to the site of the infection is critical in decreasing the risk of hospitalization and amputation. However, other conditions such as ischemia or peripheral arterial disease (PAD) hamper antibiotic delivery [
9]. DFUs caused by neuropathy are most common, but ischemic ulcers have the poorest healing rates. The lifetime mortality rates for neuropathic and ischemic ulcers are 45% and 55%, respectively [
10].
Human skin equivalents have been compared with saline gauze in promoting healing and reducing infection leading to amputation. A randomized control trial of a human skin equivalent in noninfected, nonischemic wounds found an 18% increase in healing compared with the control group [
11].
Studies on advanced biologics have been limited to small wounds in patients with no additional risk factors, which has yielded a homogenous sample but not a “real world” representation. To examine chronic wound healing in a real-world setting, 15 centers collected data on the treatment of 179 chronic wounds in 165 patients. Venous leg ulcers were the most common wounds (
n = 98, 49.7%), and DFUs were second (
n = 47, 26.3%), followed by pressure ulcers (
n = 20, 11.2%), arterial ulcers (
n = 15, 8.4%), and collagen disease wounds (
n = 8, 4.5%). Wounds with infection were the only exclusion criteria. In this study, 60 (49.6%) patients achieved wound closure, despite the inclusion of complex wounds and co-morbidities, in an average of 8 weeks [
12].
Studies on complex wounds and those at moderate-to-high risk for amputation are limited often because these treatments are withheld until a failure to heal has been demonstrated. Therefore, persons with PAD, osteomyelitis, and poor glucose management are typically excluded; yet, they represent the highest risk for amputation.
A small prospective cohort study was conducted at the Boise VAMC to examine the use of dehydrated amniotic (DAMA) tissue as early DFU treatment in veterans with a moderate-to-high risk of amputation based on the WiFI classification system [
13]. This is a five-year follow-up report of that study [
14].
2. Materials and Methods
This retrospective chart review was conducted as a 5-year follow-up on veterans who participated in a prospective, open-label, cohort study (ClinicalTrials.gov Identifier NCT02632929) at the Boise VA Medical Center between July 2015 and November 2017 [
14]. The inclusion criteria were very broad, allowing for the presence of infection and osteomyelitis (if treated), arterial disease, end-stage renal-disease (ESRD), mental health conditions, and socioeconomic challenges. Veterans who could not travel to Boise, were enrolled in hospice, had or were suspected of having a malignancy, were pregnant, or had signs of progressive gangrene were excluded from the study. This pilot study included 24 wounds in 20 veterans. Twelve wounds were classified as moderate risk for amputation and 12 wounds were at high risk for amputation, according to the WiFI classification system [
13]. The enrolled veterans ranged in age from 56 to 82 with a mean age of 67.2 years. For this group, the wound had been present for 1 to 26 weeks prior to the study. Fifteen of the 20 veterans had a prior DFU and 50% of the wounds were recurrences of prior wounds. Nine veterans had experienced a prior amputation, with six having had minor, one having had major (BKA), and two having had both major and minor amputations. One veteran was homeless and five had mental health disorders that interfered with their ability to care for themselves. In addition, forty-five percent of the veterans smoked [
14].
Prevention of amputation was the primary endpoint of the initial study, and wound closure was the secondary endpoint with a follow-up of 4 months. The treatment intervention involved an advanced biologic dehydrated amniotic (DAMA) tissue. DAMA treatment was applied weekly until the wounds healed. In addition, veterans received comprehensive care from a multidisciplinary team that included appropriate wound dressing, debridement, off-loading, and antibiotics as needed for infection. Risk factors for this group included neuropathy (20 veterans), peripheral arterial disease (10 veterans), and Charcot deformity (5 veterans). Risk factors associated with the wounds included osteomyelitis (16 wounds) and exposed tendons/ligaments/bones (19 wounds) [
14].
All wounds healed within 4–33 weeks (mean: 13.2 weeks) and no veterans experienced amputation of the limb during the study. This pilot study indicated that early and frequent application of advanced biologics along with comprehensive, multidisciplinary care may prevent amputation in patients at moderate-to-high risk [
14].
This follow-up chart review was approved as a project amendment (1587628-7) of the initial cohort study. The 20 veterans from the initial study were notified by certified letter of the chart review and given the opportunity to respond within 14 days to opt out. One returned the letter without a signature indicating opting out and one had moved out of the area; therefore, 18 of the 20 veterans were included in the follow-up.
A member of the research team collected the data from each veteran’s electronic medical record. Specific data included re-ulceration, amputation (minor and major) of either the treated limb or the contralateral limb, additional ulceration, stroke, end-stage renal disease with dialysis dependence, hospitalization, limb threatening ischemia, and cause of death (if applicable). In addition, housing status information was collected.
The data were de-identified and entered in an Excel spreadsheet. Descriptive statistics were calculated for all data elements captured (either by count and percent or mean and standard deviation).
3. Results
Veterans with a moderate-to-high risk for amputation according to each wound, ischemia, and foot infection (WiFI) classification system were enrolled in the initial study. These veterans received weekly applications of dehydrated human amniotic tissue (AMNIOEXCEL
®, Derma Science, Princeton, NJ, USA) along with comprehensive care until their diabetic foot ulcers healed.
Table 1 compares the personal characteristics and risk factors of the 20 veterans in the original study with the 18 participants included in this 5-year follow-up.
The mean ages of the veterans in the initial study and the follow-up were 67.2 and 76.1, respectively.
Three types of conditions have been attributed as causes of DFUs: neuropathic (35%), purely ischemic (15%), and mixed neuroischemic (50%) conditions [
15]. In the initial study, 20 veterans had peripheral neuropathy (100%) and 10 veterans had peripheral arterial disease (50%). The follow-up study had similar findings, with all 18 (100%) veterans having neuropathy and 10 (55%) having PAD.
Renal disease (ESRD) on dialysis was present in five or 25% of the veterans at the beginning of the initial study. An additional veteran began dialysis during the 5-year follow-up. Nine veterans had experienced both minor (six veterans) and major (one veteran) amputations before the initial study. In addition, 15 of the 20 (75%) veterans had experienced a prior DFU and ½ of the study wounds were recurrent wounds.
None of the veterans underwent minor or major amputations during the initial study. All 24 wounds healed within 4 to 32.7 weeks. However, during the 4-month monitoring period, 12 recurrent wounds developed at the study ulcer site, and 10 new ulcer sites developed, despite the implementation of protective footwear, orthotics, and routine visits with close monitoring. Other non-DFU-related significant events occurred during the immediate monitoring period including the initiation of dialysis associated with renal failure (two veterans), elective discontinuation of dialysis due to recurrent peritonitis resulting in death (one veteran), sequential bilateral major amputations (one veteran) and amputation of a non-study limb (one veteran).
Homelessness and mental health issues were present in one and five veterans, respectively.
In 2022, Chen et al. conducted a systematic review and meta-analysis of observational studies from 16 countries (America, South-East Asia, Europe, Eastern Mediterranean, and Western Pacific) [
3]. A total of 124,376 patients were included in the analysis to estimate the long-term risk factors for mortality in diabetic foot ulcer patients. Of those, 51,386 (41%) died within 5 years. Most patients were male (58%), with an average age ranging from 57 to 71 years. The highest mortality was associated with an older age, PAD, chronic kidney disease (CKD, particularly ESRD), amputation, and history of cardiovascular disease [
16]. The findings from this systematic review and meta-analysis will be used to compare the findings from this 5-year follow-up.
3.1. 5-Year Mortality
A study in Thailand of patients with DFUs found that chronic kidney disease (CKD) and PAD, especially advanced PAD (chronic limb ischemia), are strong risk factors for major cardiovascular events (heart attack, heart failure, and stroke). The mean eGFR for the 246 patients in the study was 54.4 ± 28.9 mL/min/1.73 m
2. Patients were stratified into four groups: normal eGFR (≥90 mL/min/1.73 m
2), which consisted of 79 patients; mildly decreased eGFR (60–89 mL/min/1.73 m
2), which consisted of 91 patients; moderately decreased eGFR (30–59 mL/min/1.73 m
2), which consisted of 60 patients; and severely decreased eGFR (<30 mL/min/1.73 m
2), which consisted of 16 patients. Thirteen of the patients in the severely decreased eGFR group started hemodialysis at enrollment. Over the 7-year follow-up, more than 1/3 (86 or 35%) of the patients died. There was a significant difference between the survival rates of patients with normal eGFR and moderate eGFR and between those with normal and severe eGFR. The researchers found that a severe reduction in the glomerular filtration rate (eGFR) in Type 2 diabetes patients with PAD was an independent risk factor for major cardiovascular events. They found that death occurred within 7 years for 53.5% of the patients with CKD and PAD [
17].
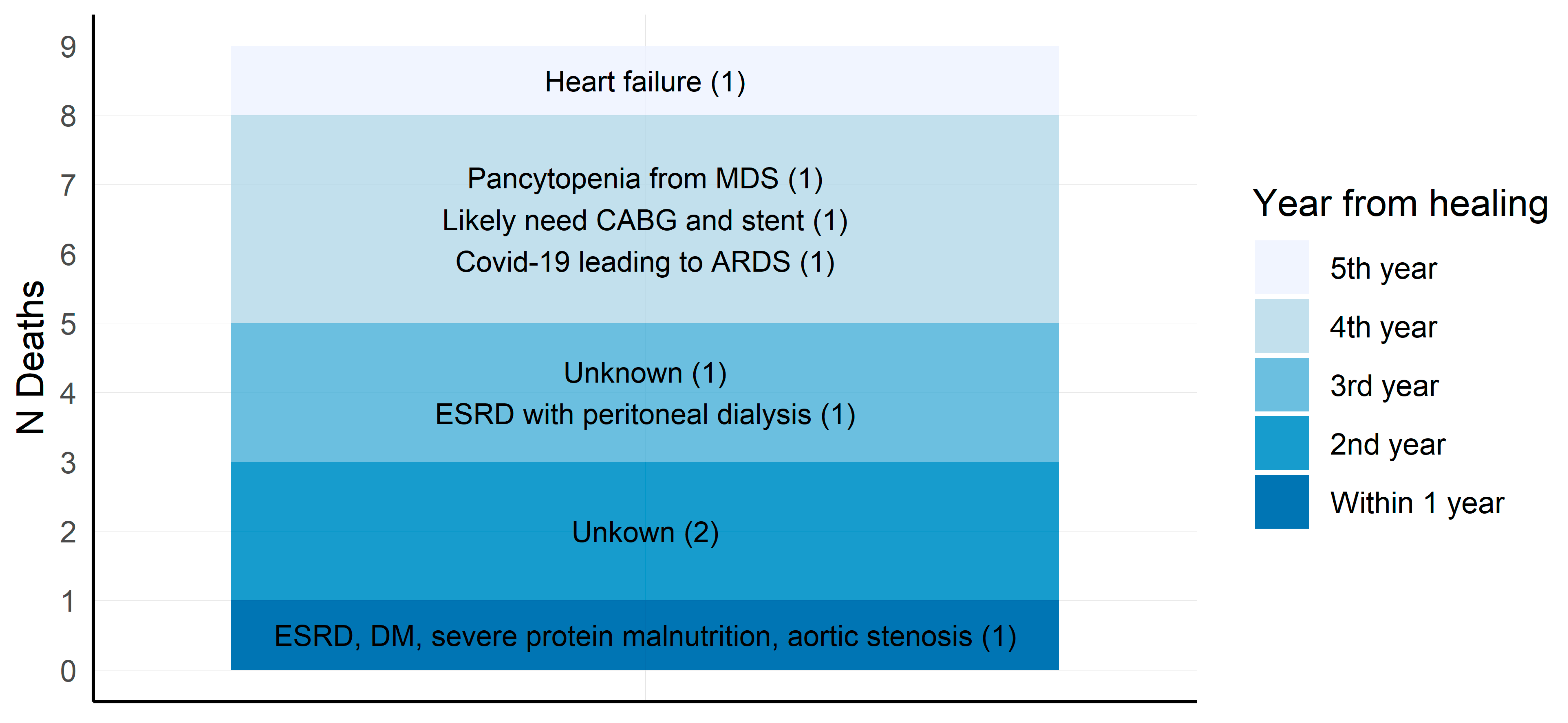
The 5-year mortality rate (from time of study wound healing) for the 18 participants in the 5-year follow-up was 50% (9/18 deceased) (
Figure 1). This was in line with other current studies, which cite that the 5-year mortality of diabetic patients with DFUs is about 40% with the major risk factors for death being age, the male gender, peripheral vascular disease (PVD), and renal disease. A meta-analysis of 21,171 patients found the 1-, 3-, 5-, 10-year survival rates to be 86.9%, 66.9%, 50.9%, and 23.1%, respectively [
16].
The atherosclerosis of the cardiovascular system is the cause of many deaths in diabetic patients who have PAD. A prospective study of 500 diabetic patients with PAD found that CKD, gangrene/chronic ulcers, having had aortic surgery, and histories of treatment with warfarin were associated with major adverse cardiac events, with hazard ratios of 2.32, 3.03, 24.07, 2.16, and 3.24, respectively [
6]. The death rate for patients with CLI and a history of cardiac disease is 26% and as high as 75% within 10 years [
18].
The two leading causes of death in this 5-year cohort were cardiovascular disease and infections. The cause of death for three of the eighteen participants was not recorded in the medical record. Heart-related conditions were associated with two deaths, and end-stage renal disease (ESRD) and diabetes were noted to be related to two deaths. COVID-19 resulting in acute respiratory distress syndrome (ARDS) was associated with one death and pancytopenia from myelodysplastic syndrome (MDS) was noted as the cause of one death. These findings were like those of the study on 513 DFU patients in the Northern Territory of Australia, with the most common causes of death being CKD (24.6%), cardiovascular events (19.6%), sepsis (15.6%), respiratory failure (10.0%), malignancy (9.5%), and multi-organ failure (5.0%). However, the Northern Australia group was younger and had a shorter diabetes duration [
19].
3.2. Re-Ulceration/Recurrence
The strongest predictor of developing a DFU is having had a previous DFU or an amputation. According to the Internation Diabetes Federation, the recurrence of DFUs in the U.S. in 2018 was 52%, which was much higher than the DFU recurrence in 2013 of 8% [
7].
While having had a previous DFU is a strong predictor for developing additional DFUs, the pattern and locations of subsequent ulcerations are less predictable. Petersen et al. conducted a secondary analysis of 129 patients with DFUs prior to and during a 34-week trial. They found that 37 patients had a total of 53 recurrent DFUs (0.63 DFU/patient year) to both limbs. On average patients had 2.2 DFUs by the end of the study. In addition, more than 60% had DFUs in more than one location, and one patient had a history of DFUs in nine different locations on their feet. In the patients experiencing a recurrence during the trial (28.7%), 48% of the DFUs were on the contralateral foot, 35% were in a different location on the same foot, and 17% at the same location [
20].
In this follow-up study, 94% (17 out of 18) of the participants developed the re-ulceration of the study site or additional ulcerations within 5 years.
Table 1 shows the prevalence of re-ulceration in the study site and the occurrence of DFU at other sites within the 5 years.
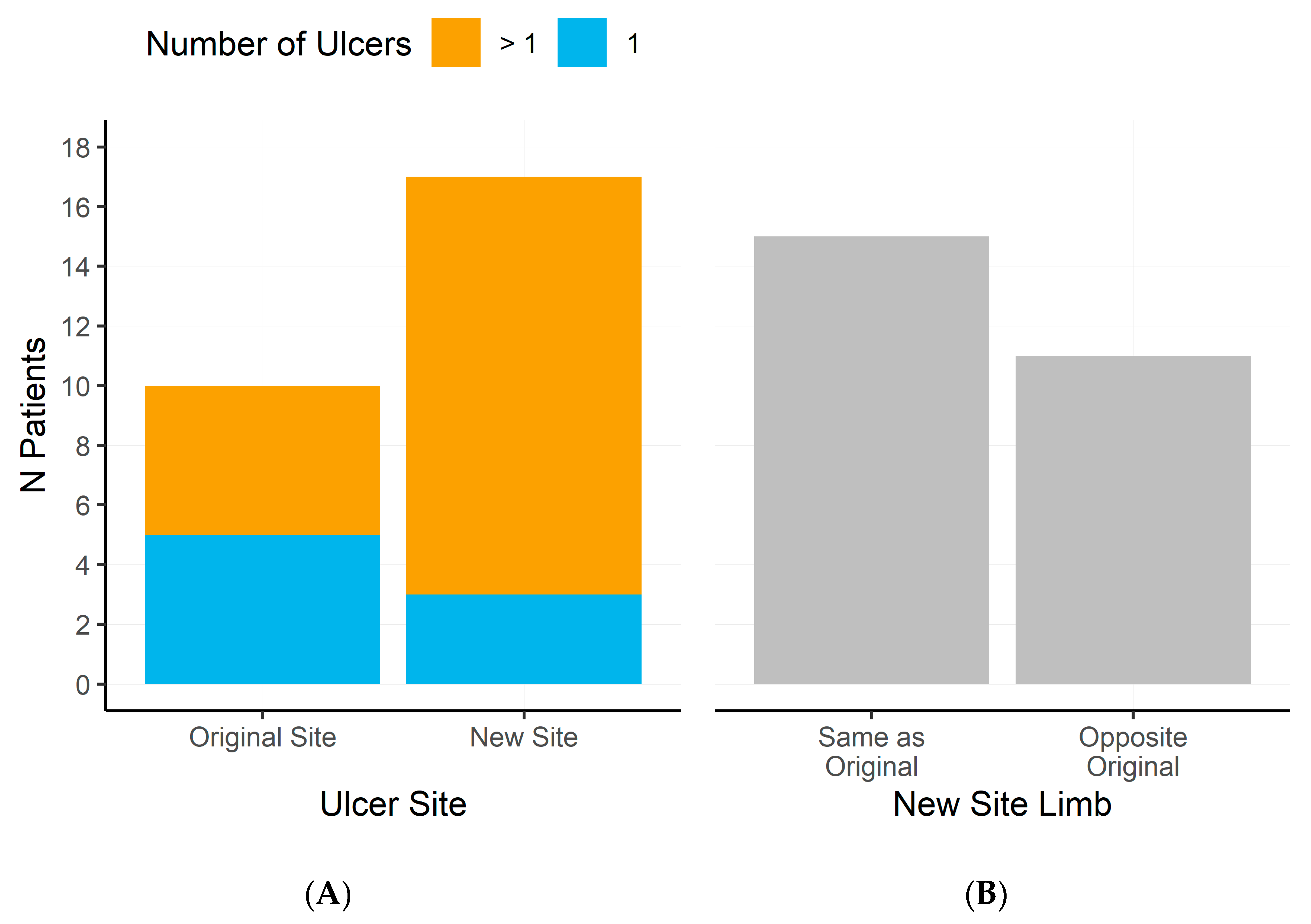
Over fifty percent (55.5% or 10 out of 18) of the participants in this follow-up study experienced the re-ulceration of the original study ulcer. (
Figure 2) Out of the ten who experienced re-ulcerations, five had more than one re-occurrence over the years. These findings are within the range noted in prospective cohort studies of a 50–65% recurrence rate at five years [
2].
Almost all (17 of 18) participants developed a new ulceration site within the five years and 82% (14 out of 17) developed more than one additional ulceration. New site ulcerations were further analyzed to distinguish the limb sides of the original ulcers. Of the 17 that experienced an additional ulcer, 88% (15 out of 17) of participants developed at least one additional ulcer on the same limb as the original ulcer; 64% (11 out of 17) of additional ulcers developed on the opposite limb.
3.3. Amputation
The number of nontraumatic lower extremity amputations in the United States decreased by half from 2000 to 2009, but since then, the rate has risen, with rates highest in the older age group [
21]. Studies typically differentiate between major amputations and minor amputations. The current literature indicates that the lifetime risk of lower extremity amputation among people with DFUs is at least 19% [
15]. A study found that after an amputation, up to 50% of the people die within 2 years [
9].
Amputations, particularly Below-Knee Amputations (BKAs), also referred to as Transtibial Amputations (TTAs), are associated with high risks for death: 27.3% within the first year and 63.2% within 5 years. They are also at risk for re-amputations because of wound complications such as infection or wound necrosis. In a retrospective study on patients who received major amputations between 2009 and 2012, 167 patients had 180 major lower extremity amputations. The 90-day re-amputation TTA rate was 30%, the through-the-knee (TKA) rate was 34%, and the Above-Knee Amputation (AKA) (also known as Transfemoral Amputation (TFA)) rate was 9%. Beginning in 2014, TKA amputations were not performed at the study facility and the 90-day re-amputation rates for the 108 patients with 116 procedures were 19% for BKA and 5% for AKA [
22].
Amputations also have other complications, largely related to poor blood flow to the surgical site, that can lead to other procedures. Those factors that affect blood flow include diabetes complications such as renal failure, PAD, hemoglobin levels, blood transfusions, and taking anticoagulant or antithrombotic drugs, along with procedures such as percutaneous transluminal angioplasty (PTA) and bypass surgery. Lee, Lee, and Byun examined the medical records of 181 patients who had had BKAs. The sample was divided into groups in which group 1 consisted of patients with diabetes (59 or 32.6%), group 2 consisted of patients with diabetes and chronic kidney disease (12 or 6.6%), group 3 consisted of patients with diabetes and occlusive arteriosclerosis (85 or 47%), and group 4 consisted of patients with diabetes and all three underlying conditions (25 or 13.8%). In this study, 40 (22.1%) of the patients experienced complications (dehiscence, hematoma, necrosis, and infection), with group 1 and 3 patients having the largest numbers of complications: 16 (40%) and 13 (32.5%), respectively [
23].
One school of thought says that because of the high rate of complications and mortality, amputation should be prevented whenever possible and limb salvage should be the primary goal of DFU treatment [
9]. An additional consideration is regarding whether the prevention of amputation can truly alter the underlying disease process involving the morbidity and mortality associated with diabetes.
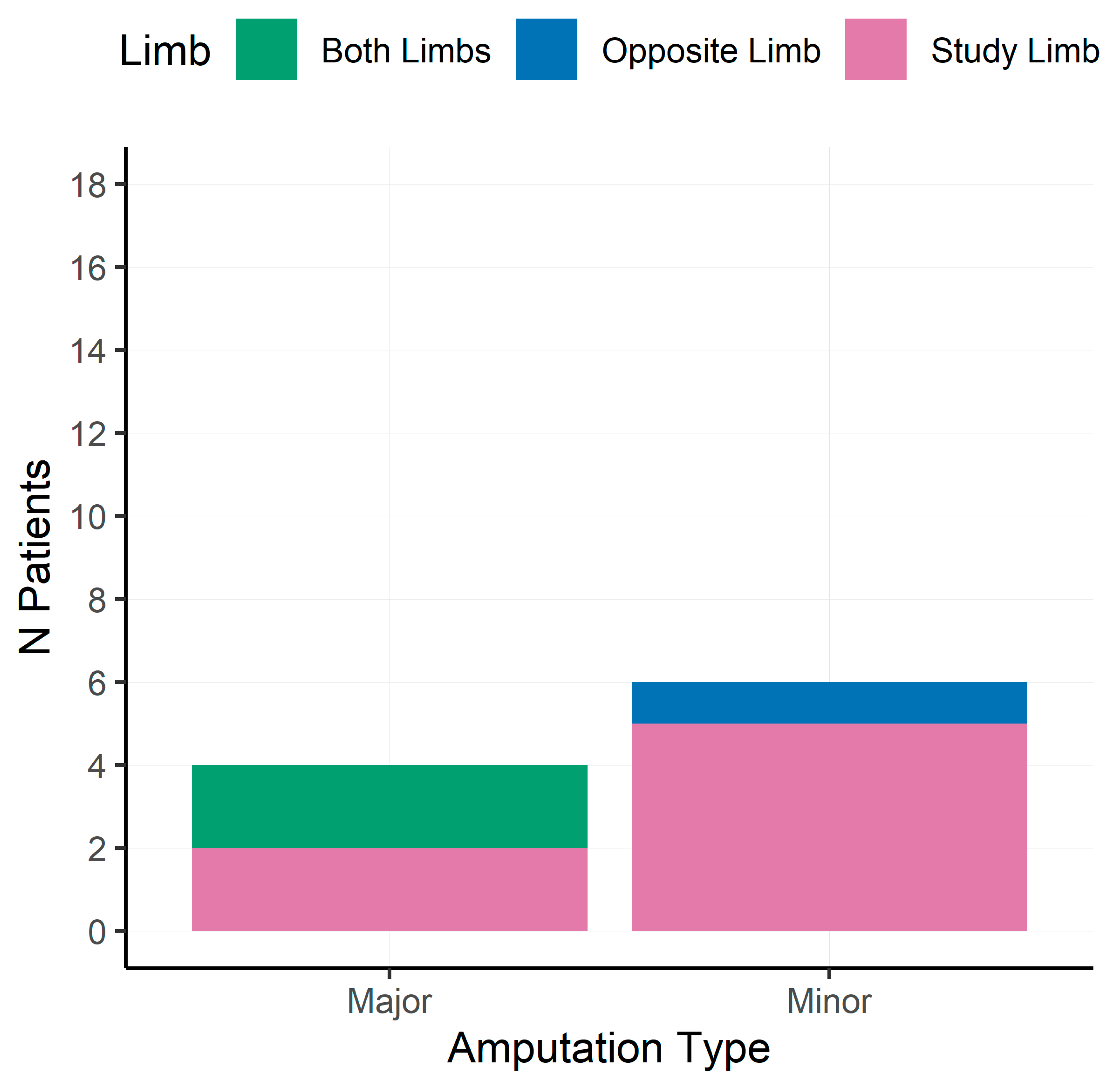
In this 5-year follow-up, four of the eighteen participants (22.2%) underwent major amputation within 5 years of study completion; two of these were on the same side as the ulcer and the other two were contralateral limb amputations. Regarding the two participants with contralateral limb amputations, one resulted from significant deep vein thrombosis and one resulted from a non-healing DFU. Two of the four participants had major amputation to both limbs (right below-knee/transtibial and left above-knee/transfemoral amputations) and bilateral above-knee/transfemoral amputations. Fifty percent (2/4) of the participants that underwent major amputation died within 5 years after the initial study wounds healed.
Figure 3 shows the minor and major amputations among this cohort.
3.4. Hospitalizations
About 20% of diabetic hospitalizations are related to foot problems [
24]. The hospital readmission rate for DFUs is as high as 30%, with about 17.6% occurring in the first 30 days. Average hospital stays are in the range of 8.6–9.1 days and 67% of the readmissions are related to non-healing wounds [
9].
Of the 18 veterans in our 5-year follow-up study, all experienced one hospitalization. The length of stay for this first hospitalization ranged from 1 to 7 days, with an average inpatient stay of 2.59 days.
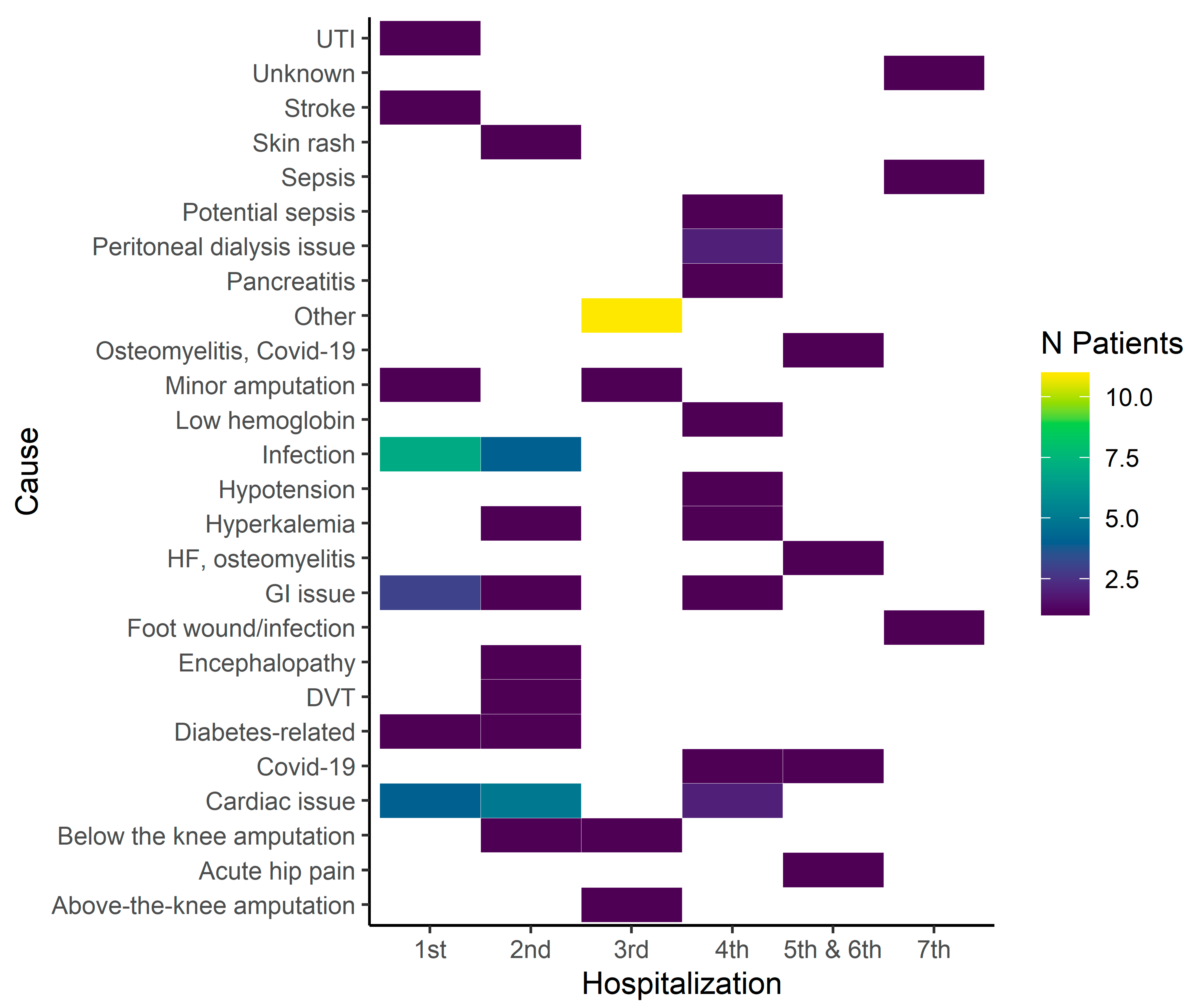
The causes associated with the hospitalizations are listed in
Figure 4. For the first hospitalization, the most common cause was infection, five were wounds, and two were respiratory issues. Cardiac issues were the second leading cause for hospitalization in this group and accounted for 22% of the admissions.
As far as the time from healing from the study wound was concerned, no one in the follow-up group was admitted within 30 days. The earliest admission from study wound healing was 43 days, and that veteran was admitted for a stroke.
Sixteen veterans experienced a second hospital admission. The length of stay for the second hospitalization ranged from 1 to 11 days, with an average stay of 4.3 days. One veteran was admitted 8 days from the first hospitalization for a UTI. Two were admitted 12 days after the first admission: one for the osteomyelitis of a wound and the other for a suspicion of a heart attack (HA).
It is interesting to note that the first major amputation among the 18 veterans in this follow-up study occurred in the veteran’s second hospitalization, which was almost 2 years (1.81) since the study wound healed. Fourteen veterans experienced a third hospitalization. During this hospitalization, one veteran had bilateral Above-Knee Amputations (2.81 years after healing) and one had a Below-Knee Amputation (1.87 years after healing). All amputations were related to non-healing wounds. An additional veteran had a minor amputation because of osteomyelitis (4.79 years after healing).
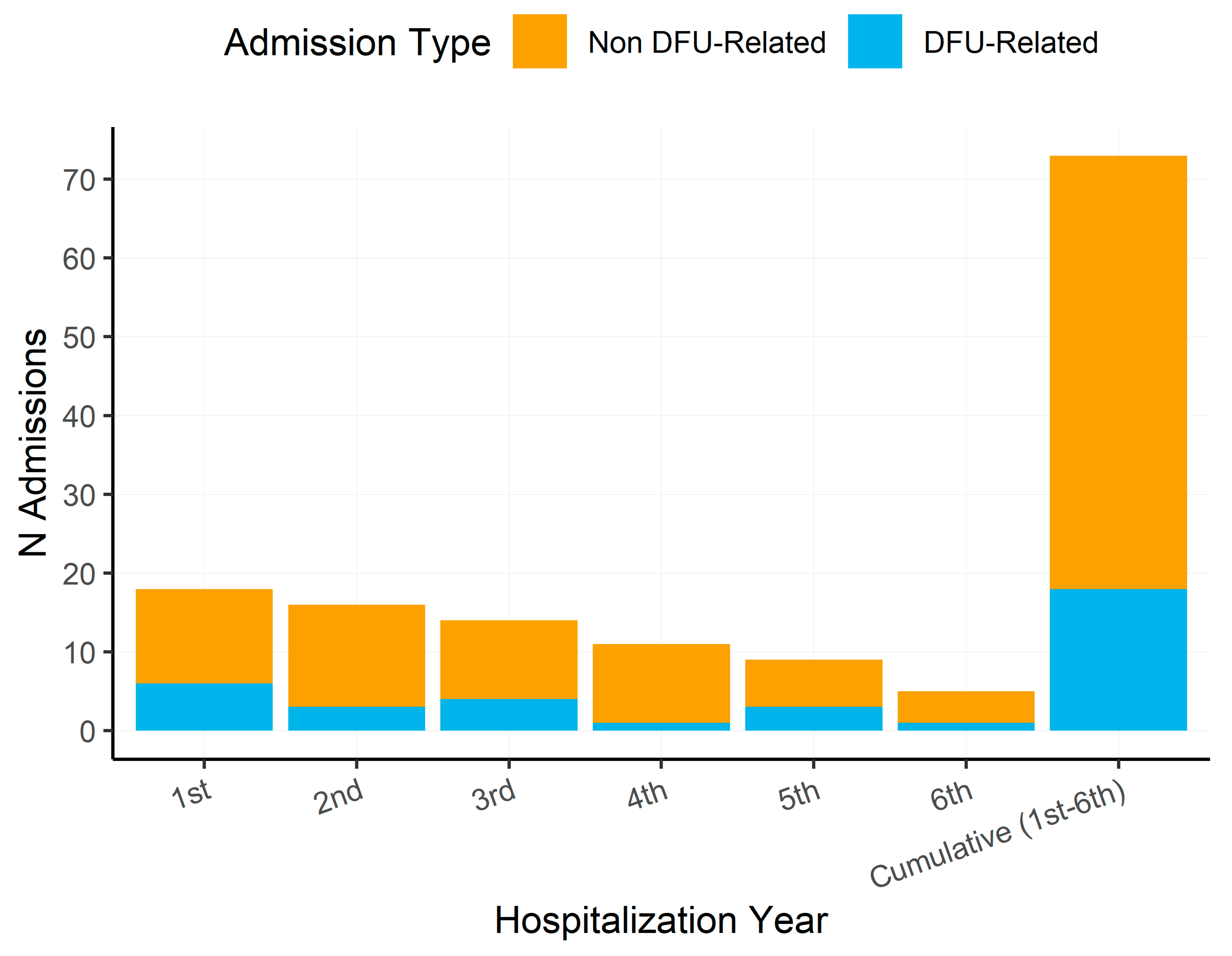
Eleven of the eighteen veterans experienced a fourth hospitalization within the 5-year follow-up. Nine veterans in this cohort experienced a fifth hospitalization. It is interesting to note that one veteran had a minor amputation during this hospitalization. Four veterans experienced a sixth hospitalization within the 5-year follow-up. Three of the four veterans experienced a seventh hospitalization.
Over the 5 years, hospital admissions for DFU-related issues (infection, sepsis, osteomyelitis, minor amputation, and PAD) ranged from 9 to 33% with the 5 year average of 24.7%, which was slightly above the national average of 20% (26).
Figure 5 demonstrates the information by admission.
3.5. End-Stage Renal Disease (ESRD) with Dialysis Dependence
In patients with renal disease, neuropathy, PAD, susceptibility to infection (due to compromised immunity from uremia), and dialysis are risk factors for the development of DFUs. For those patients on dialysis, the prevalence of foot complications is 250% higher. In addition, dialysis has been linked with a 2-fold higher risk for amputation [
6].
At the conclusion of the original study, 5/18 of the veterans had end-stage renal disease (ESRD), three of whom were on dialysis. In the 5-year follow-up, one additional veteran developed ESRD and started hemodialysis.
3.6. Limb-Threatening Ischemia
A DFU is often accompanied by peripheral artery disease (PAD). In 2019, Paisey et al. conducted an 18-year study on 83 patients with a DFU and found that those patients with peripheral vascular disease had a 5-year survival rate of 35% [
11]. In 2022, Rodrigues et al. conducted a systematic review and found that ischemic ulcers were significantly associated with amputation and mortality rates, likely due to poor perfusion and healing along with peripheral vascular disease [
10].
In 2018, Mustapha et al. investigated the long-term outcomes of over 72,000 Medicare beneficiaries after initial diagnosis of chronic limb ischemia (CLI). During the 4 years, seventy-one percent of the patients had at least one revascularization or amputation procedure. The claims review found that over the 4-year follow-up, 54% died and 3% had major amputations [
25].
Over time, PAD progresses to critical limb ischemia (CLI), characterized by pain when at rest, non-healing ulcers, tissue loss, and possible gangrene. Twenty studies of patients with ischemic limb were included in an analysis by Wolfe and Wyatt [
18]. All patients were treated conservatively with reconstructive surgery or angioplasty or amputation. The one-, three-, and five-year mortality rates for the total sample were 26%, 44%, and 56%, respectively. The researchers separated the sample into a low-risk group (rest pain with normal ankle pressure) and a high-risk group (tissue loss and low ankle pressure). At one year, both the low-risk and high-risk groups had experienced amputation, with 73% and 95%, respectively. However, only 25% of high-risk patients who had reconstructive surgery required a major amputation within the first year. Their findings indicate that 26% of a high-risk group will die within one year no matter what treatment is provided, 5% who are treated conservatively will not have an amputation, and 69% may improve with treatment. These findings indicate that there is a group of patients with high-risk ischemia in which surgery is the only intervention that will save a limb [
18].
A systematic review of PAD assessment methods, including ABI, ankle pressure, TBI, toe pressure, TcP02, skin perfusion pressure, continuous wave Doppler, the palpation of pedal pulses, and ankle peak systolic velocity, was conducted by Chuter et al. in 2023 [
26]. The findings indicated that no test was superior for testing PAD. In the prediction of major amputation in diabetic patients with DFUs, only an ABI of 0.9 was associated with a 45% increase in the probability of not having a major amputation.
4. Discussion
This cohort with DFUs was characteristic of samples in other studies in that about ½ of the patients had PAD. Invasive revascularization is often used to improve peripheral circulation by restoring blood flow to the occluded tissues. According to a retrospective chart review, revascularization resulted in a wound cure rate of 78.3% when compared with a 26.1% cure rate for those without revascularization. Patients who had revascularization had a 14.944 (1.102–202.692)-times higher likelihood of healing. In patients with a WiFI classification of stage 2–3, it was 11.926 (1.438–98.883) times more likely for the wounds to heal than in patients with a WiFI classification of 4 [
27].
The veterans in this study were classified as having moderate-to-high risks for amputation using the WiFI classification system and ten of these patients had PAD. These patients had undergone vascular review and were determined to not be surgical candidates at the time of enrollment either due to co-morbidities or a lack of surgical options. Revascularization procedures were not collected in this follow-up, but hospitalizations reflect admissions for infections, amputations, and cardiac issues that may have resulted from the combination of severe wounds associated with PAD.
The mortality rate for this veteran cohort was 50%, which was in line with a 5-year survival rate of 50.9% [
3]. Causes of death included heart-related conditions, ESRD and diabetes, COVID-19 resulting in ARDS, and pancytopenia from MDS. These findings are like those of the Northern Territory of Australia study, with the most common cause of deaths being CKD (24.6%), cardiovascular events (19.6%), sepsis (15.6%), respiratory failure (10.0%), malignancy (9.5%), and multi-organ failure (5.0%). However, the Northern Australia group was younger and had a shorter diabetes duration than this veteran group. One interesting point to note is that these 18 veterans had the same 5-year outcomes as in studies on people with first-time DFUs with lower risks for amputation.
The lifetime risk of lower extremity amputation among people with DFUs is at least 19% [
2]. Four veteran (22.2%) in this cohort underwent major amputations within 5 years and two had major amputations of both limbs. The current literature cites that up to 50% of people die within 2 years after a major amputation. In this cohort, fifty percent of those who experienced major amputation died within 5 years.
All the veterans in this cohort experienced one hospitalization within the 5-year follow-up and three experienced seven hospitalizations. Most hospitalizations were related to infection, cardiac issues, stroke, or ESRD.
Overall, this was a small sample with no control group, which certainly limits the generalization of the findings. Further analysis would be warranted, looking at the cost/benefit ratio and quality of life survey (which was part of the original study). A review of existing guidelines for the utilization of advanced biologics in a population such as this would be beneficial to efforts of limb salvage programs. One interesting point to note is that these 18 veterans had the same 5-year outcomes as in studies on people with first-time DFUs with lower risks for amputation. This finding suggests that further investigations into the utilization of advanced therapies for the early treatment of diabetic foot ulcers in patients with moderate-to-high risks of amputation would be warranted.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}