Abstract
Thyroid disorders (TDs) and diabetes mellitus (DM) represent significant metabolic pathologies with an important global burden. Diabetes, characterized by chronic hyperglycemia, induces widespread dysregulation of lipid, protein, and carbohydrate metabolism. The thyroid gland, a central regulator of endocrine homeostasis, modulates metabolic processes through the secretion of thyroid hormones (THs). A complex bidirectional relationship exists between type 2 diabetes mellitus (T2DM) and thyroid dysfunction, wherein each condition may exacerbate the pathophysiological consequences of the other. At the core of this interplay lies insulin resistance (IR), a fundamental mechanism underlying their coexistence and mutual aggravation. A thorough investigation into the underlying mechanisms of thyroid function could reveal new insights into the development and progression of T2DM. Grasping the clinical correlation between these widespread endocrine disorders is crucial for customizing treatments for individuals confronting both conditions. This narrative review seeks to offer an understanding of the epidemiological, pathophysiological, and clinical dimensions of the relationship between TD and T2DM. Considering the substantial clinical ramifications of concurrent T2DM and TD, it is imperative to institute suitable screening and management approaches for both endocrine disorders to guarantee optimal care for patients.
1. Introduction
Diabetes mellitus (DM) ranks among the most common chronic pathological conditions, primarily attributable to impaired pancreatic β-cell function, frequently developing in the setting of IR. With swift economic progress, profound shifts in lifestyles, and an aging demographic, T2DM has emerged as a prominent public health challenge worldwide, particularly in developing nations. As per the most recent data from the International Diabetes Federation (IDF), the global prevalence of T2DM among adults reached 536.6 million individuals (10.5%) in 2021. Projections indicate that, by 2045, there will be 783.2 million people (12.2%) living with diabetes globally [1,2].
Thyroid conditions are frequently encountered within the broader population, with a notable prevalence across diverse demographic groups. Overt hypothyroidism affects approximately 0.2% to 5.3% of the European population and 0.3% to 3.7% of individuals in the USA, depending on the diagnosis criteria and studied demographics. Large-scale longitudinal studies in the UK revealed an incidence rate of 3.5–5.0 per 1000 for women and 0.6–1.0 per 1000 for men in spontaneous hypothyroidism [3,4].
Conversely, the prevalence of overt hyperthyroidism ranges from 0.2% to 1.3% in iodine-sufficient regions globally. In the United States National Health and Nutrition Examination Survey (NHANES III), overt hyperthyroidism was identified in 0.5% of the population, with an additional 0.7% having subclinical hyperthyroidism, leading to an overall prevalence of 1.3%. Similar rates have been reported in studies from various countries such as Sweden, Denmark, Norway, and Japan. A meta-analysis of European studies estimated a mean prevalence rate of 0.75% and an incidence rate of 51 per 100,000 per year [3,5].
The interplay between diabetes and thyroid dysfunction has been a subject of research for decades [6]. Researchers have predominantly delved into the prevalence of thyroid disease among individuals with type 1 diabetes, considering its autoimmune origin. In contrast, the association between T2DM and TD has remained relatively understudied.
2. Materials and Methods
A comprehensive and systematic literature search was conducted to explore the relationship between TD and T2DM. The search was performed across three major databases—PubMed, Google Scholar, and the Cochrane Library—covering studies published from January 2004 to February 2024. Searches were restricted to publications in English and to studies involving adult human subjects (≥18 years).
We used a combination of keywords and Medical Subject Headings to capture relevant studies. The search terms included “thyroid dysfunction” AND “type 2 diabetes mellitus”, “hypothyroidism” AND “type 2 diabetes mellitus”, “hyperthyroidism” AND “type 2 diabetes mellitus”, “subclinical hypothyroidism” OR “thyroid function” AND “insulin resistance”, “thyroid disorders” AND “type 2 diabetes” AND “guidelines”. Boolean operators “AND” and “OR” were used to combine the search terms, and additional manual screening of reference lists from related articles and recent reviews was conducted to identify further eligible studies.
Inclusion Criteria:
- Peer-reviewed articles published between January 2004 and February 2024;
- Adult populations aged 18 years or above;
- Studies investigating the association between thyroid function (hypothyroidism, hyperthyroidism, and subclinical dysfunction) and T2DM;
- Observational studies (cohort, case–control, and cross-sectional) and interventional studies;
- Clinical guidelines from internationally recognized endocrinology and diabetes organizations.
Exclusion Criteria:
- Non-English language publications;
- Pediatric or adolescent populations (<18 years);
- Studies focused exclusively on type 1 diabetes or gestational diabetes;
- Animal experiments or in vitro research;
- Case reports, editorials, letters to the editor, or opinion pieces without original research data;
- Articles lacking a clear diagnostic definition of thyroid dysfunction.
A total of 1387 records were identified from the database searches. After removing 382 duplicates, 1005 titles and abstracts were screened. Of these, 142 full-text articles were assessed for eligibility. Based on the inclusion and exclusion criteria, 21 studies were included in the final synthesis (Figure 1).
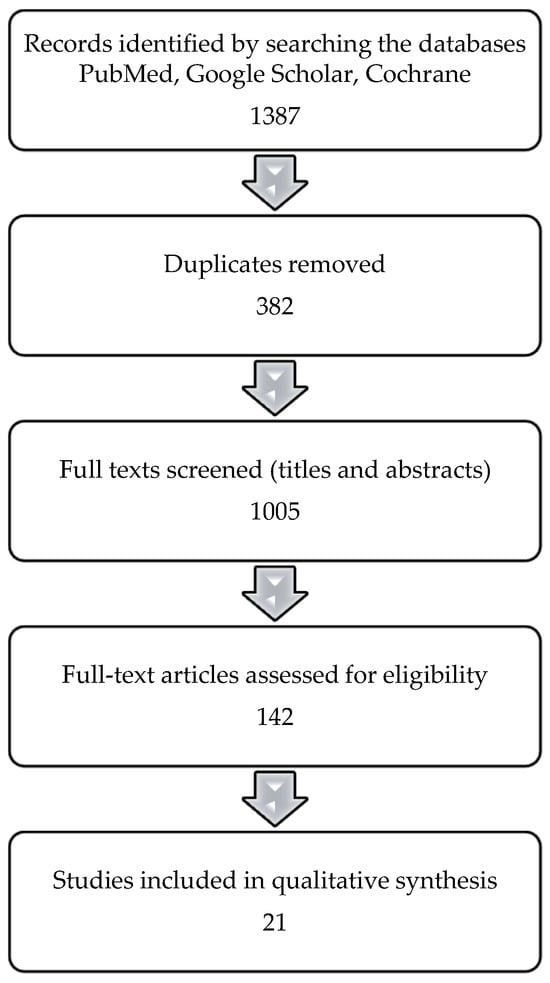
Figure 1.
Flow diagram of the article inclusion process.
Additionally, we examined the current screening guidelines for TD in patients with T2DM, as issued by the American Diabetes Association (ADA), American Thyroid Association (ATA), and European Thyroid Association (ETA). These recommendations were reviewed to identify potential gaps in practice and to inform evidence-based clinical suggestions.
3. Results
3.1. Unravelling the Prevalence of Thyroid Dysfunction in T2DM
Certain investigations have proposed a reciprocal impact of diabetes and TD on each other. The Third National Health and Nutrition Examination Survey (NHANES III), a substantial cross-sectional survey comprising 17,353 participants in the USA, found that hypothyroidism affected 4.6% of the study cohort, while hyperthyroidism affected 1.3% of participants. Furthermore, NHANES III noted an increased prevalence of thyroid dysfunction in individuals with diabetes in comparison to those without diabetes [7].
Certain studies have indicated a greater prevalence of thyroid dysfunction in patients with T2DM than in the general population, with varying estimates across studies. The data from selected studies regarding the prevalence of hypo/hyperthyroidism in T2DM subjects are presented in Table 1 [8,9,10,11,12,13,14,15,16,17].

Table 1.
Comparison of studies introduced in the current research containing information on the relationship between thyroid dysfunction and type 2 diabetes mellitus.
3.2. Thyroid Hormones and Glucose Metabolism: Insights into T2DM Pathogenesis
The immediate regulation of cellular metabolic processes relies heavily on the interplay between insulin and glucagon, two hormones released by the beta- and alpha-cells located in the pancreatic islets. However, a substantial body of evidence indicates a significant impact of THs on the maintenance of glucose levels in the body, with their collective effects, alongside insulin, determining the specific metabolic pathways for glucose and lipids. For instance, both triiodothyronine (T3) and insulin seem to modulate the activities of key regulatory proteins responsible for glucose uptake into cells, as well as those crucial for the metabolic cascades of glucose and lipids [19].
Previous literature reviews have detailed the effects of insulin and THs on various tissues of the body. THs demonstrate both insulin-like actions and actions that oppose insulin in multiple organs. These actions are usually finely balanced, and any deficiency or excess of THs can disrupt this balance, leading to disturbances in carbohydrate metabolism [20,21].
Conversely, diabetes can affect thyroid function in various ways. In diabetes, the response of thyroid-stimulating hormone (TSH) to thyrotropin-releasing hormone can become impaired, leading to hypothyroidism and, subsequently, lower levels of T3. This decrease in T3 levels might also be due to the reduced conversion of T3 from T4 in diabetes, as evidenced by studies showing a reversible decrease in deiodinase activity and hepatic thyroxine concentration induced by hyperglycemia [22,23]. However, there are studies suggesting that a short-term excess of T3 could induce IR, potentially contributing to the development of T2DM [24].
The association between TH levels and the risk of developing T2DM remains a subject of considerable debate within the scientific community. Findings from human studies have been inconsistent: some investigations suggest that elevated TSH levels and reduced free thyroxine (FT4) concentrations are linked to hyperglycemia and IR, while others report no significant association [13,25,26,27]. These discrepancies highlight the need for a more comprehensive assessment of the relationship between TSH, FT4, and T2DM.
Additionally, most existing research has predominantly focused on evaluating the impact of baseline TSH and FT4 levels on the future risk of T2DM [22,28,29,30,31].
3.3. Thyroid Dysfunction and Insulin Resistance: Partners in T2DM Pathogenesis?
IR denotes a state wherein the responsiveness of target cells to regular levels of insulin is diminished. This state often coexists with an array of metabolic and cardiovascular abnormalities, collectively termed “insulin resistance syndrome” [32].
The prevalent forms of human IR typically align with obesity and physical inactivity, yet pinpointing a singular cellular basis for these conditions continues to elude researchers. T2DM results from pancreatic β-cell dysfunction, frequently on the background of IR, and is explained by genetic, environmental, and metabolic factors. Persistent overnutrition drives hyperinsulinemia, β-cell failure, and disease progression, with obesity—particularly visceral and hepatic fat—being a key contributor [33,34,35,36]. IR impairs β-cell insulin secretion, increases lipolysis, and elevates serum levels of non-esterified fatty acids (NEFA), further disrupting the metabolic balance. Beyond glycemic control, IR is independently linked to macrovascular and microvascular complications, including diabetic cardiomyopathy and chronic kidney disease [32,37].
Alterations in thyroid function, including both hypothyroidism and hyperthyroidism, have been implicated in the development of IR, mirroring the disturbances in glucose metabolism typically observed in T2DM [38,39].
THs are integral to glucose metabolism and insulin sensitivity, with their dysregulation contributing to IR in both hypo- and hyper-thyroid states. In hyperthyroidism, elevated TH levels enhance hepatic glucose production and turnover, leading to hepatic IR and impaired glucose tolerance. Conversely, hypothyroidism is associated with IR predominantly in peripheral tissues, such as skeletal muscle and adipose tissue, resulting in decreased glucose uptake and utilization. These alterations in insulin sensitivity underscore the critical role of thyroid function in maintaining metabolic homeostasis and highlight the importance of monitoring and managing IR in patients with TD to prevent the progression of metabolic complications [39].
THs significantly influence the expression and function of glucose transporters, notably GLUT2, GLUT3, and GLUT4, across various tissues. In a clinical study, Maratou et al. (2009) demonstrated that patients with overt and subclinical hypothyroidism exhibited decreased insulin-stimulated glucose uptake in monocytes, attributed to the impaired translocation of GLUT4 transporters to the plasma membrane, indicating peripheral IR [40]. Conversely, the same study observed an increased baseline expression of GLUT3 and GLUT4 transporters in monocytes from patients with overt and subclinical hyperthyroidism, suggesting an adaptive response to heightened metabolic demands [40,41].
In preclinical models, perinatal hypothyroidism in rats was shown to impair the normal transition of GLUT4 and GLUT1 expression in heart and brown adipose tissue, highlighting the tissue-specific regulation of GLUT4 by THs. Furthermore, the administration of T3 in hypothyroid rats increased GLUT4 mRNA and protein expression in skeletal muscle, enhancing both basal and insulin-stimulated glucose uptake [42,43,44,45]. Regarding GLUT2, THs have been found to regulate its expression in the liver. Specifically, T3 administration in hypothyroid rats led to a significant upregulation of hepatic GLUT2 mRNA and protein levels, facilitating increased hepatic glucose output [44,46].
These findings collectively underscore the pivotal role of THs in modulating glucose transporter expression and function, contributing to alterations in glucose metabolism observed in thyroid dysfunctions.
Another potential pathogenetic mechanism for the development of IR in hypothyroidism is associated with decreased blood flow in peripheral tissues [47].
Independently on their etiology, both hypo- and hyperthyroidism may affect glucose regulation in diabetic patients, as well as in non-diabetic subjects [48].
3.4. Hypothyroidism and T2DM: Is There a Link Between T2DM and Hypothyroidism?
Hypothyroidism is the most prevalent thyroid disorder in the adult population. Some studies suggest a higher prevalence of overt hypothyroidism in individuals with T2DM than in the general population, although the link between subclinical hypothyroidism and T2DM remains contentious. The coexistence of T2DM and hypothyroidism is becoming increasingly recognized in clinical settings. While the individual metabolic impacts of T2DM and hypothyroidism are well documented, there is a notable scarcity of research examining the combined metabolic consequences when both conditions are present [4,40,49,50,51,52,53,54].
THs have an influence on the regulation of insulin secretion. In the case of hypothyroidism, a reduction in insulin production by pancreatic beta-cells has been observed, while hyperthyroidism tends to enhance beta-cell sensitivity to catecholamines or glucose, likely due to an increase in beta-cell mass. Additionally, thyrotoxicosis is associated with enhanced insulin clearance. These thyroid hormone-related alterations are thought to elevate the risk of developing T2DM and may contribute to the progression of diabetic complications or exacerbate existing diabetic symptoms [23,55,56,57].
Hypothyroidism is associated with several metabolic alterations, including reduced glucose absorption from the gastrointestinal tract, prolonged peripheral glucose accumulation, diminished gluconeogenesis, decreased hepatic glucose production, and impaired glucose disposal [58]. In association with T2DM, hypothyroidism can influence glucose metabolism through various mechanisms. For instance, subclinical hypothyroidism may contribute to IR by reducing the rate of insulin-stimulated glucose transport, potentially due to alterations in the GLUT2 gene translocation. Recent studies have also suggested that hypothyroidism reduces renal insulin clearance, thereby lowering the physiological demand for insulin [56].
IR has been consistently linked to hypothyroidism in multiple preclinical and in vitro studies, which have shown diminished insulin sensitivity in peripheral muscle tissues under hypothyroid states [59]. Dysregulated leptin metabolism has also been proposed as a possible contributing factor to this pathological process. Although several studies have highlighted a correlation between hypothyroidism and IR, the discrepancies in some findings point to the need for further exploration of this relationship [56].
The variability in the prevalence of hypothyroidism across different diabetic populations can be attributed to several factors, including the adequacy of iodine intake, which influences the baseline thyroid function of the population, as well as the presence of goiter. Other metabolic factors, such as the prevalence of glycemic disturbances, metabolic syndrome, and comorbidities associated with thyroid dysfunction, also play a role. From an epidemiological standpoint, the overall prevalence of diabetes within the population further contributes to this variability. In essence, studies examining the comorbidities of diabetes and TD are often population-specific [17].
3.5. Effects of Hyperthyroidism on Glucose Metabolism
The incidence of clinically manifest T2DM has increased in the context of thyrotoxicosis since Rohdenburg first showed that elevated TH levels cause disruptions in carbohydrate metabolism and established a mechanistic link between modified serum levels of thyroid hormones and diabetes mellitus [60]. IR and the poor regulation of glucose are commonly linked to hyperthyroidism, with overt diabetes identified in 2–3% of cases and glucose intolerance described in around 50% of hyperthyroid patients. Numerous studies have been conducted to determine the underlying mechanism of how hyperthyroidism affects the decline in glycemic control [20,40,61,62,63,64,65].
Hyperthyroidism can create IR through some of the following potential mechanisms: it increases intestinal glucose absorption, induces postprandial hyperglycemia, increases hepatic glucose output, increases serum levels of free fatty acids (FFAs), reduces insulin secretion, and decreases sensitivity to insulin in peripheral tissues [39,40,65,66].
Hyperthyroidism increases glucose demand, primarily met by enhanced hepatic gluconeogenesis (fasting state) and Cori cycle activity (postprandial and fasting states). Fasting-state lipolysis elevates serum levels of glycerol and non-esterified fatty acids (NEFAs), with glycerol and amino acids from proteolysis serving as gluconeogenic substrates. NEFAs stimulate gluconeogenesis and fuel oxidation in peripheral tissues. Postprandially, insulin-stimulated glucose uptake in skeletal muscle is normal or elevated due to increased perfusion, but glycogen synthesis is impaired, favoring lactate production and Cori cycle activation. This cycle acts as a glucose–lactate buffer for metabolic flexibility. Postprandial lipolysis suppression facilitates glucose utilization by insulin-resistant muscle, preserving fat stores [63,67,68,69].
Excessive hepatic glucose production is a critical factor in peripheral IR, glucose intolerance, and hyperinsulinemia. In thyrotoxicosis, increased glycogenolysis and hepatic glucose output contribute to impaired glucose tolerance, promoting progression from prediabetes to diabetes and exacerbating hyperglycemia in T2DM.
Both T2DM and hyperthyroidism share pathophysiological mechanisms, including β-cell dysfunction, IR, altered glucagon secretion, increased intestinal glucose absorption, and elevated catecholamine levels [3,19,23,70,71].
Among these, IR represents the primary link between thyroid dysfunction and T2DM. Hepatic IR is driven by excessive glucose output rather than fasting hyperinsulinemia, and elevated hepatic glucose production is a major determinant of increased fasting plasma glucose in T2DM [40,56]. Skeletal muscle IR further disrupts glucose homeostasis, contributing to metabolic deterioration [37,63]. Additionally, IR influences lipid metabolism, reinforcing the link between thyroid dysfunction and T2DM [56,71,72].
3.6. Genetic Influences on Thyroid Function and Glucose Metabolism
THs significantly influence glucose metabolism through the genetic regulation of various metabolic pathways. The key genes involved include mitochondrial uncoupling proteins (UCP-3), glucose transporters (GLUT-4 and GLUT-1), and PGC-1α. T3 enhances GLUT-4-mediated glucose transport, while UCP-3 affects fatty acid oxidation and glucose metabolism. TH receptors (TRα1, TRβ1, and TRβ2) modulate metabolic processes, with TRβ isoforms maintaining hypothalamic–pituitary–thyroid axis homeostasis [56,73].
Genetic factors substantially determine thyroid function and glucose metabolism. Studies indicate that up to 67% of circulating TH and TSH concentrations are genetically determined, suggesting a genetic "set point" for individual thyroid function [73]. Genetic factors are recognized as major contributors to the inter-individual variability in circulating levels of TSH and FT4, accounting for an estimated 58–71% of this variation [74].
Deiodinases (D1, D2, and D3) regulate T3 bioavailability, impacting insulin responsiveness. Variants such as Thr92Ala in D2 are associated with IR and altered glucose turnover in skeletal muscle and adipose tissue [19,23,75]. Furthermore, hyperthyroidism enhances GLUT-2 expression, lipid peroxidation, and catecholamine-mediated lipolysis, disrupting lipid metabolism and reinforcing IR.
In summary, genetic influences on thyroid function significantly impact glucose metabolism through the regulation of key metabolic genes and pathways. Understanding these genetic interactions is crucial for developing targeted therapeutic strategies for metabolic disorders involving TD and impaired glucose metabolism.
Table 2 highlights studies from the literature that substantiate the bidirectional influence between TD and T2DM, reinforcing the complex interplay between these conditions.
Table 2.
Bidirectional relationship between thyroid dysfunction and type 2 diabetes: a review of key studies.
4. Conclusions
Due to the complex interplay between thyroid function and diabetes, it is recommended to adopt a systematic and comprehensive strategy for thyroid assessment in individuals with T2DM, especially those with challenging comorbidities. The management of hypo/hyperthyroidism plays a pivotal role in achieving improved control over concurrent conditions.
Identifying and addressing latent hypothyroidism in these patients stand to augment their overall quality of life. Consequently, it is imperative to identify instances where hypothyroidism contributes to morbidity and specifically where it underlies suboptimal management of concurrent medical conditions.
Moreover, the existing literature supports the notion that TD, particularly hypothyroidism, frequently coexists with DM, potentially exacerbating metabolic derangements and complicating therapeutic regimens. As such, routine screening for TD in diabetic populations, especially in those exhibiting challenging clinical profiles, is a prudent clinical approach.
Accumulating evidence points to a bidirectional relationship between TD and T2DM, wherein each condition may exacerbate the development, progression, and management of the other. These findings underscore the necessity of the early identification and appropriate management of TD in individuals with diabetes, with the aim of optimizing clinical outcomes and minimizing the risk of complications.
Author Contributions
Conceptualization, D.-M.T. and A.M.A.; methodology, D.-M.T.; software, D.-M.T.; validation, A.M., M.C. and D.L.P.; formal analysis, D.L.P.; investigation, A.M.A.; resources, C.G.; data curation, C.D.; writing—original draft preparation, D.-M.T. and A.M.A.; writing—review and editing, C.G.; visualization, C.G.; supervision, C.G.; project administration, D.L.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| NHANES III | Third United States National Health and Nutrition Examination Survey |
| NHIRD | National Health Insurance Research Database |
| UCP-3 | uncoupling protein |
| GLUT | glucose transporter in the plasma membrane |
| NEFA | non-esterified fatty acid |
| T2DM | type 2 diabetes mellitus |
| TSH | thyroid-stimulating hormone |
| TH | thyroid hormone |
| SHR | subclinical hyperthyroidism |
| FT4 | free thyroxine |
| CVD | cardiovascular disease |
| TD | thyroid disorder |
| DM | diabetes mellitus |
| T3 | triiodothyronine |
| IR | insulin resistance |
| HR | hyperthyroidism |
References
- American Diabetes Association Professional Practice Committee; ElSayed, N.A.; Aleppo, G.; Bannuru, R.R.; Beverly, E.A.; Bruemmer, D. Summary of Revisions: Standards of Care in Diabetes—2024. Diabetes Care 2024, 47, S5–S10. [Google Scholar] [CrossRef]
- Magliano, D.J.; Boyko, E.J.; IDF Diabetes Atlas 10th Edition Scientific Committee. IDF DIABETES ATLAS, 10th ed.; International Diabetes Federation: Brussels, Belgium, 2021. Available online: https://www.ncbi.nlm.nih.gov/books/NBK581934/ (accessed on 26 April 2025).
- Taylor, P.N.; Albrecht, D.; Scholz, A.; Gutierrez-Buey, G.; Lazarus, J.H.; Dayan, C.M.; Okosieme, O.E. Global epidemiology of hyperthyroidism and hypothyroidism. Nat. Rev. Endocrinol. 2018, 14, 301–316. [Google Scholar] [CrossRef]
- Chiovato, L.; Magri, F.; Carlé, A. Hypothyroidism in Context: Where We’ve Been and Where We’re Going. Adv. Ther. 2019, 36, 47–58. [Google Scholar] [CrossRef] [PubMed]
- Han, C.; He, X.; Xia, X.; Li, Y.; Shi, X.; Shan, Z.; Teng, W. Subclinical hypothyroidism and type 2 diabetes: A systematic review and meta-analysis. PLoS ONE 2015, 10, e0135233. [Google Scholar] [CrossRef] [PubMed]
- Roa Dueñas, O.H.; Van der Burgh, A.C.; Ittermann, T.; Ligthart, S.; Ikram, M.A.; Peeters, R.; Chaker, L. Thyroid Function and the Risk of Prediabetes and Type 2 Diabetes. J. Clin. Endocrinol. Metab. 2022, 107, 1789–1798. [Google Scholar] [CrossRef]
- Hollowell, J.G.; Staehling, N.W.; Flanders, W.D.; Hannon, W.H.; Gunter, E.W.; Spencer, C.A.; Braverman, L.E. Serum TSH, T4, and Thyroid Antibodies in the United States Population (1988 to 1994): National Health and Nutrition Examination Survey (NHANES III). J. Clin. Endocrinol. Metab. 2002, 87, 489–499. [Google Scholar] [CrossRef]
- Khassawneh, A.H.; Al-Mistarehi, A.H.; Zein Alaabdin, A.M.; Khasawneh, L.; AlQuran, T.M.; Kheirallah, K.A.; Saadeh, N.A.; Beni yonis, O.; Shawkat, M.; Obeidat, N. Prevalence and predictors of thyroid dysfunction among type 2 diabetic patients: A case–control study. Int. J. Gen. Med. 2020, 13, 803–816. [Google Scholar] [CrossRef]
- Bukhari, S.I.; Ali, G.; Memom, M.Y.; Sandeelo, N.; Alvi, H.; Talib, A.; Ahmed, I.; Lal, H.; Asghar, M.S.; Naseer, U. Prevalence and predictors of thyroid dysfunction amongst patients with Type 2 diabetes mellitus in Pakistan. J. Family Med. Prim. Care 2022, 11, 2739. [Google Scholar] [CrossRef]
- Ogbonna, S.U.; Ezeani, I.U.; Okafor, C.I.; Chinenye, S. Association between glycemic status and thyroid dysfunction in patients with type 2 diabetes mellitus. Diabetes Metab. Syndr. Obes. 2019, 12, 1113–1122. [Google Scholar] [CrossRef]
- Shrestha, B.; Rai, C.K. Hypothyroidism among Type 2 Diabetic Patients Visiting Outpatient Department of Internal Medicine of a Tertiary Care Centre: A Descriptive Cross-sectional Study. J. Nepal. Med. Assoc. 2023, 61, 325–328. [Google Scholar] [CrossRef]
- Ishay, A.; Chertok-Shaham, I.; Lavi, I.; Luboshitzky, R. Prevalence of subclinical hypothyroidism in women with type 2 diabetes. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2009, 15, CR151-5. [Google Scholar]
- Raghuwanshi, P.K.; Rajput, D.P.S.; Ratre, B.K.; Jain, R.; Patel, N.; Jain, S. Evaluation of thyroid dysfunction among type 2 diabetic patients. Asian J. Med. Sci. 2014, 6, 33–37. [Google Scholar] [CrossRef]
- Mehalingam, V.; Sahoo, J.; Bobby, Z.; Vinod, K. Thyroid dysfunction in patients with type 2 diabetes mellitus and its association with diabetic complications. J. Family Med. Prim. Care 2020, 9, 4277. [Google Scholar] [CrossRef] [PubMed]
- Elgazar, E.H.; Esheba, N.E.; Shalaby, S.A.; Mohamed, W.F. Thyroid dysfunction prevalence and relation to glycemic control in patients with type 2 diabetes mellitus. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 2513–2517. [Google Scholar] [CrossRef]
- Chubb, S.A.P.; Peters, K.E.; Bruce, D.G.; Davis, W.A.; Davis, T.M.E. The relationship between thyroid dysfunction, cardiovascular morbidity and mortality in type 2 diabetes: The Fremantle Diabetes Study Phase II. Acta Diabetol. 2022, 59, 1615–1624. [Google Scholar] [CrossRef]
- Subekti, I.; Pramono, L.A.; Dewiasty, E.; Harbuwono, D.S. Thyroid Dysfunction in Type 2 Diabetes Mellitus Patients. Acta Medica Indones. 2017, 49, 314. [Google Scholar]
- Pramanik, S.; Ghosh, S.; Mukhopadhyay, P.; Bhattacharjee, R.; Mukherjee, B.; Mondal, S.A.; Ghosh, I.; Bari, R.; Chowdhury, S. Thyroid status in patients with Type 2 diabetes attending a Tertiary Care Hospital in Eastern India. Indian. J. Endocrinol. Metab. 2018, 22, 112–115. [Google Scholar] [CrossRef]
- Eom, Y.S.; Wilson, J.R.; Bernet, V.J. Links between Thyroid Disorders and Glucose Homeostasis. Diabetes Metab. J. 2022, 46, 239–256. [Google Scholar] [CrossRef]
- Venditti, P.; Reed, T.T.; Victor, V.M.; Di Meo, S. Insulin resistance and diabetes in hyperthyroidism: A possible role for oxygen and nitrogen reactive species. Free Radic. Res. 2019, 53, 248–268. [Google Scholar] [CrossRef]
- Mullur, R.; Liu, Y.Y.; Brent, G.A. Thyroid Hormone Regulation of Metabolism. Physiol. Rev. 2014, 94, 355. [Google Scholar] [CrossRef]
- Rong, F.; Dai, H.; Wu, Y.; Li, J.; Liu, G.; Chen, H.; Zhang, X. Association between thyroid dysfunction and type 2 diabetes: A meta-analysis of prospective observational studies. BMC Med. 2021, 19, 257. [Google Scholar] [CrossRef] [PubMed]
- Biondi, B.; Kahaly, G.J.; Robertson, R.P. Thyroid Dysfunction and Diabetes Mellitus: Two Closely Associated Disorders. Endocr. Rev. 2019, 40, 789–824. [Google Scholar] [CrossRef] [PubMed]
- Solá, E.; Morillas, C.; Garzón, S.; Gómez-Balaguer, M.; Hernández-Mijares, A. Association between diabetic ketoacidosis and thyrotoxicosis. Acta Diabetol. 2002, 39, 235–237. [Google Scholar] [CrossRef] [PubMed]
- Hage, M.; Zantout, M.S.; Azar, S.T. Thyroid disorders and diabetes mellitus. J. Thyroid Res. 2011, 2011, 439463. [Google Scholar] [CrossRef]
- Jali, M.V.; Kambar, S.; Jali, S.M.; Pawar, N.; Nalawade, P. Prevalence of thyroid dysfunction among type 2 diabetes mellitus patients. Diabetes Metab. Syndr. Clin. Res. Rev. 2017, 11, S105–S108. [Google Scholar] [CrossRef]
- Demitrost, L.; Ranabir, S. Thyroid dysfunction in type 2 diabetes mellitus: A retrospective study. Indian. J. Endocrinol. Metab. 2012, 16, 334. [Google Scholar] [CrossRef]
- Jun, J.E.; Jee, J.H.; Bae, J.C.; Jin, S.M.; Hur, K.Y.; Lee, M.K.; Kim, T.H.; Kim, S.W.; Kim, J.H. Association Between Changes in Thyroid Hormones and Incident Type 2 Diabetes: A Seven-Year Longitudinal Study. Thyroid 2017, 27, 29–38. [Google Scholar] [CrossRef]
- de Vries, T.I.; Kappelle, L.J.; van der Graaf, Y.; de Valk, H.W.; de Borst, G.J.; Nathoe, H.M.; Visseren, F.L.; Westerink, J.; SMART Study Group. Thyroid-stimulating hormone levels in the normal range and incident type 2 diabetes mellitus. Acta Diabetol. 2019, 56, 431–440. [Google Scholar] [CrossRef]
- Chang, C.H.; Yeh, Y.C.; Shih, S.R.; Lin, J.W.; Chuang, L.M.; Caffrey, J.L.; Tu, Y.K. Association between thyroid dysfunction and dysglycaemia: A prospective cohort study. Diabet. Med. 2017, 34, 1584–1590. [Google Scholar] [CrossRef]
- Al-Geffari, M.; Ahmad, N.A.; Al-Sharqawi, A.H.; Youssef, A.M.; Alnaqeb, D.; Al-Rubeaan, K. Risk factors for thyroid dysfunction among type 2 diabetic patients in a highly diabetes mellitus prevalent society. Int. J. Endocrinol. 2013, 2013, 417920. [Google Scholar] [CrossRef]
- Lee, S.H.; Park, S.Y.; Choi, C.S. Insulin Resistance: From Mechanisms to Therapeutic Strategies. Diabetes Metab. J. 2021, 46, 15. [Google Scholar] [CrossRef]
- Ahmed, A.; Atkinson, R.L. Obesity|Complications. In Encyclopedia of Human Nutrition; Elsevier: Amsterdam, The Netherlands, 2005; pp. 406–413. [Google Scholar] [CrossRef]
- Gupta, A. Etiopathogenesis of insulin resistance. In Understanding Insulin and Insulin Resistance; Elsevier: Amsterdam, The Netherlands, 2022; pp. 231–273. [Google Scholar] [CrossRef]
- Insulin Resistance—An Overview|ScienceDirect Topics n.d. Available online: https://www.sciencedirect.com/topics/medicine-and-dentistry/insulin-resistance (accessed on 26 April 2025).
- Courtney, C.H.; Olefsky, J.M. Insulin Resistance. In Mechanisms of Insulin Action: Medical Intelligence Unit; Springer: New York, NY, USA, 2023; pp. 185–209. [Google Scholar] [CrossRef]
- Zhao, X.; An, X.; Yang, C.; Sun, W.; Ji, H.; Lian, F. The crucial role and mechanism of insulin resistance in metabolic disease. Front. Endocrinol. 2023, 14, 1149239. [Google Scholar] [CrossRef] [PubMed]
- Kocatürk, E.; Kar, E.; Küskü Kiraz, Z.; Alataş, Ö. Insulin resistance and pancreatic β cell dysfunction are associated with thyroid hormone functions: A cross-sectional hospital-based study in Turkey. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 2147–2151. [Google Scholar] [CrossRef]
- Gierach, M.; Gierach, J.; Junik, R. Insulin resistance and thyroid disorders. Endokrynol. Pol. 2014, 65, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Maratou, E.; Hadjidakis, D.J.; Kollias, A.; Tsegka, K.; Peppa, M.; Alevizaki, M.; Mitrou, P.; Lambadiari, V.; Boutati, E.; Nikzas, D.; et al. Studies of insulin resistance in patients with clinical and subclinical hypothyroidism. Eur. J. Endocrinol. 2009, 160, 785–790. [Google Scholar] [CrossRef]
- Matsuzu, K.; Segade, F.; Wong, M.; Clark, O.H.; Perrier, N.D.; Bowden, D.W. Glucose transporters in the thyroid. Thyroid 2005, 15, 545–550. [Google Scholar] [CrossRef]
- Weinstein, S.P.; Haber, R.S. Differential regulation of glucose transporter isoforms by thyroid hormone in rat heart. BBA—Mol. Cell Res. 1992, 1136, 302–308. [Google Scholar] [CrossRef]
- Matthaei, S.; Trost, B.; Hamann, A.; Kausch, C.; Benecke, H.; Greten, H.; Höppner, W.; Klein, H.H. Effect of in vivo thyroid hormone status on insulin signalling and GLUT1 and GLUT4 glucose transport systems in rat adipocytes. J. Endocrinol. 1995, 144, 347–357. [Google Scholar] [CrossRef]
- Santalucía, T.; Palacín, M.; Zorzano, A. T3 strongly regulates GLUT1 and GLUT3 mRNA in cerebral cortex of hypothyroid rat neonates. Mol. Cell Endocrinol. 2006, 251, 9–16. [Google Scholar] [CrossRef]
- Torrance, C.J.; Devente, J.E.; Jones, J.P.; Dohm, G.L. Effects of Thyroid Hormone on GLUT4 Glucose Transporter Gene Expression and NIDDM in Rats. Endocrinology 1997, 138, 1204–1214. [Google Scholar] [CrossRef]
- Lyu, J.; Imachi, H.; Yoshimoto, T.; Fukunaga, K.; Sato, S.; Ibata, T.; Kobayashi, T.; Dong, T.; Yonezaki, K.; Yamaji, N.; et al. Thyroid stimulating hormone stimulates the expression of glucose transporter 2 via its receptor in pancreatic β cell line, INS-1 cells. Sci. Rep. 2018, 8, 1–10. [Google Scholar] [CrossRef]
- Dimitriadis, G.; Mitrou, P.; Lambadiari, V.; Boutati, E.; Maratou, E.; Panagiotakos, D.B.; Koukkou, E.; Tzanela, M.; Thalassinos, N.; Raptis, S.A. Insulin Action in Adipose Tissue and Muscle in Hypothyroidism. J. Clin. Endocrinol. Metab. 2006, 91, 4930–4937. [Google Scholar] [CrossRef] [PubMed]
- Sotak, S.; Felsoci, M.; Lazurova, I. Type 2 diabetes mellitus and thyroid disease: A two-sided analysis. Bratisl. Med. J. 2018, 119, 361–365. [Google Scholar] [CrossRef]
- Bermúdez, V.; Salazar, J.; Añez, R.; Rojas, M.; Estrella, V.; Ordoñez, M.; Chacín, M.; Hernández, J.D.; Arias, V.; Cabrera, M.; et al. Metabolic Syndrome and Subclinical Hypothyroidism: A Type 2 Diabetes-Dependent Association. J. Thyroid Res. 2018, 2018, 8251076. [Google Scholar] [CrossRef] [PubMed]
- Alsolami, A.A.; Alshali, K.Z.; Albeshri, M.A.; Alhassan, S.H.; Qazli, A.M.; Almalki, A.S.; Bakarman, M.A.; Mukhtar, A.M. Association between type 2 diabetes mellitus and hypothyroidism: A case–control study. Int. J. Gen. Med. 2018, 11, 457–461. [Google Scholar] [CrossRef] [PubMed]
- Nair, A.; Jayakumari, C.; Jabbar, P.K.; Jayakumar, R.V.; Raizada, N.; Gopi, A.; George, G.S.; Seena, T.P. Prevalence and Associations of Hypothyroidism in Indian Patients with Type 2 Diabetes Mellitus. J. Thyroid Res. 2018, 2018, 5386129. [Google Scholar] [CrossRef]
- Fang, T.; Deng, X.; Wang, J.; Han, F.; Liu, X.; Liu, Y.; Sun, B.; Chen, L. The effect of hypothyroidism on the risk of diabetes and its microvascular complications: A Mendelian randomization study. Front. Endocrinol. 2023, 14, 1288284. [Google Scholar] [CrossRef]
- Talwalkar, P.; Deshmukh, V.; Bhole, M. Prevalence of hypothyroidism in patients with type 2 diabetes mellitus and hypertension in india: A cross-sectional observational study. Diabetes Metab. Syndr. Obes. 2019, 12, 369–376. [Google Scholar] [CrossRef]
- Brenta, G.; Caballero, A.S.; Nunes, M.T. Case finding for hypothyroidism should include type 2 diabetes and metabolic syndrome patients: A Latin American Thyroid Society (LATS) position statement. Endocr. Pract. 2019, 25, 101–105. [Google Scholar] [CrossRef]
- Martinez, B.; Ortiz, R.M. Thyroid hormone regulation and insulin resistance: Insights from animals naturally adapted to fasting. Physiology 2017, 32, 141–151. [Google Scholar] [CrossRef]
- Majeed, S.; Hussein, M.; Abdelmageed, R.M. The Relationship Between Type 2 Diabetes Mellitus and Related Thyroid Diseases. Cureus 2021, 13, e20697. [Google Scholar] [CrossRef]
- Bar-Tana, J. Insulin Resistance, Secretion and Clearance –Taming the Three Effector Encounter of Type 2 Diabetes. Front. Endocrinol. 2021, 12, 741114. [Google Scholar] [CrossRef] [PubMed]
- Althausen, T.L.; Stockholm, M. Influence of the thyroid gland on absorption in the digestive tract. Am. J. Physiol.-Leg. Content 1938, 123, 577–588. [Google Scholar] [CrossRef]
- Dimitriadis, G.; Parry-Billings, M.; Bevan, S.; Leighton, B.; Krause, U.; Piva, T.; Tegos, K.; Challiss, R.A.J.; Wegener, G.; Newsholme, E.A. The effects of insulin on transport and metabolism of glucose in skeletal muscle from hyperthyroid and hypothyroid rats. Eur. J. Clin. Investig. 1997, 27, 475–483. [Google Scholar] [CrossRef]
- Rohdenburg, G.L. Thyroid diabetes. Endocrinology 1920, 4, 63–70. [Google Scholar] [CrossRef]
- Singh, I.; Srivastava, M.C. Hyperglycemia, keto-acidosis and coma in a nondiabetic hyperthyroid patient. Metabolism 1968, 17, 893–895. [Google Scholar] [CrossRef]
- Chambers, T.L. Coexistent coeliac disease, diabetes mellitus, and hyperthyroidism. Arch. Dis. Child. 1975, 50, 162–164. [Google Scholar] [CrossRef][Green Version]
- Mitrou, P.; Raptis, S.A.; Dimitriadis, G. Insulin action in hyperthyroidism: A focus on muscle and adipose tissue. Endocr. Rev. 2010, 31, 663–679. [Google Scholar] [CrossRef]
- Butterfield, W.J.H.; Whichelow, M.J. Are thyroid hormones diabetogenic? A study of peripheral glucose metabolism during glucose infusions in normal subjects and hyperthyroid patients before and after treatment. Metabolism 1964, 13, 620–628. [Google Scholar] [CrossRef]
- Orsetti, A.; Collard, F.; Jaffiol, C. Abnormalities of carbohydrate metabolism in experimental and clinical hyperthyroidism: Studies on plasma insulin and on the A- and B-chains of insulin. Acta Diabetol. Lat. 1974, 11, 486–492. [Google Scholar] [CrossRef]
- Seino, Y.; Taminato, T.; Kurahachi, H.; Ikeda, M.; Goto, Y.; Imura, H. Comparative insulinogenic effects of glucose, arginine and glucagon in patients with diabetes mellitus, endocrine disorders and liver disease. Acta Diabetol. Lat. 1975, 12, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Dimitriadis, G.D.; Raptis, S.A. Thyroid hormone excess and glucose intolerance. Exp. Clin. Endocrinol. Diabetes 2001, 109 (Suppl. S2), S225–S239. [Google Scholar] [CrossRef] [PubMed]
- Mendez, D.A.; Ortiz, R.M. Thyroid hormones and the potential for regulating glucose metabolism in cardiomyocytes during insulin resistance and T2DM. Physiol. Rep. 2021, 9, e14858. [Google Scholar] [CrossRef] [PubMed]
- Salleh, M.; Ardawi, M.; Khoja, S.M. Effects of hyperthyroidism on glucose, glutamine and ketone-body metabolism in the gut of the rat. Int. J. Biochem. 1993, 25, 619–624. [Google Scholar] [CrossRef]
- Wang, C. The Relationship between Type 2 Diabetes Mellitus and Related Thyroid Diseases. J. Diabetes Res. 2013, 2013, 390534. [Google Scholar] [CrossRef]
- Grigoriadis, G.; Koufakis, T.; Kotsa, K. Epidemiological, Pathophysiological, and Clinical Considerations on the Interplay between Thyroid Disorders and Type 2 Diabetes Mellitus. Medicina 2023, 59, 2013. [Google Scholar] [CrossRef]
- Duntas, L.H.; Orgiazzi, J.; Brabant, G. The interface between thyroid and diabetes mellitus. Clin. Endocrinol. 2011, 75, 1–9. [Google Scholar] [CrossRef]
- Panicker, V. Genetics of Thyroid Function and Disease. Clin. Biochem. Rev. 2011, 32, 165. [Google Scholar]
- Sterenborg, R.B.; Steinbrenner, I.; Li, Y.; Bujnis, M.N.; Naito, T.; Marouli, E.; Galesloot, T.E.; Babajide, O.; Andreasen, L.; Astrup, A.; et al. Multi-trait analysis characterizes the genetics of thyroid function and identifies causal associations with clinical implications. Nat. Commun. 2024, 15, 888. [Google Scholar] [CrossRef]
- Medici, M.; Visser, T.J.; Peeters, R.P. Genetics of thyroid function. Best. Pract. Res. Clin. Endocrinol. Metab. 2017, 31, 129–142. [Google Scholar] [CrossRef]
- Zuanna, T.D.; Pitter, G.; Canova, C.; Simonato, L.; Gnavi, R. A systematic review of case-identification algorithms based on italian healthcare administrative databases for two relevant diseases of the endocrine system: Diabetes mellitus and thyroid disorders. Epidemiol. Prev. 2019, 43, 17–36. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.A.; Choi, D.W.; Kwon, J.; Lee, D.W.; Park, E.C. Association between continuity of care and type 2 diabetes development among patients with thyroid disorder. Medicine 2019, 98, e18537. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.H.; Chen, H.Y.; Man, K.M.; Chen, S.J.; Chen, W.; Liu, P.L.; Chen, Y.H.; Chen, W.C. Thyroid diseases increased the risk of type 2 diabetes mellitus: A nation-wide cohort study. Medicine 2019, 98, e15631. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).