Abstract
Bladder cancer (BC) remains a clinical challenge due to its complex etiology and high incidence, especially in developed populations. This article presents a broad analysis of the latest advances in BC treatment, offering a new perspective on the growing role of innovative therapies that are effectively changing the standards of oncological care. Focusing on targeted therapy, immunotherapy, antibody–drug conjugates, and breakthrough gene therapies, the paper shows how modern approaches can counteract resistance mechanisms and improve treatment efficacy while limiting toxicity for patients. Progress in the field of immune therapies, including checkpoint inhibitors, offers hope for significant improvement in the outcomes of patients with advanced forms of cancer, and the concept of targeted therapy tailored to the molecular characteristics of the tumor indicates the potential of personalized oncology. Gene and photodynamic therapies, in turn, offer new possibilities for precise action on cancer cells, minimizing the side effects of traditional methods. The article presents innovative therapeutic strategies and results of the latest clinical trials, showing the prospects for the development of BC treatment and highlighting the key challenges facing oncology.
1. Introduction
Bladder cancer (BC) is a common malignancy of the genitourinary system, especially in Western countries, where it accounts for 5–10% of cancers in men, with peak incidence in those over 70 years of age [1]. In 2022, BC ranked ninth globally, with 613,799 new cases—76.7% in men and 23.3% in women [2]. The highest incidence rates occur in Southern and Northern Europe, with Spain and the Netherlands leading among men and women, respectively [3]. Europe reported the highest 5-year prevalence (154.4%), followed by Asia and North America [4]. Rising incidence in high-income countries is offset by declining mortality due to earlier detection and improved treatment [5]. Key risk factors include smoking, occupational carcinogen exposure, and arsenic in drinking water [6]. Although the COVID-19 pandemic caused temporary disruptions in cancer care, its long-term impact remains uncertain [3]. Mortality is falling in high-HDI countries but rising in some regions, possibly due to disparities in prevention and healthcare access [7,8].
1.1. Major Risk Factors for Developing Bladder Cancer
1.1.1. Sex
Bladder cancer is diagnosed about four times more often in men than in women, with higher male mortality largely attributed to smoking. Male smokers have a greater relative risk of death than female smokers (3.0 vs. 2.4). In countries with high female smoking rates, such as Lebanon, incidence in women is also elevated. Other male-specific risk factors include occupational exposure, alcohol, and red meat. Smoking accelerates onset in both sexes by about six years [9,10].
1.1.2. Age
Bladder cancer mainly affects older adults—about 90% of U.S. cases occur in those over 55, and 80% in those over 65. The average age at diagnosis is 73, higher than for most cancers (65–70), indicating a need for prolonged exposure to mutagens for carcinogenesis [11,12].
1.1.3. Smoking Tobacco Products
Smoking is the main risk factor for bladder cancer, causing 50–65% of cases and increasing risk 3–4 times. Tobacco carcinogens induce genetic mutations via DNA adducts, often leading to cancer after a latency of ~30 years. Quitting smoking reduces the risk by ~40% within 1–4 years, with near-baseline risk after 20 years. Cigarette smokers face the highest risk due to deeper inhalation and higher combustion temperatures [13,14].
1.1.4. Obesity
Obesity and pre-obesity are notable risk factors for bladder cancer. A meta-analysis of 15 cohort studies found a 7% increased risk with pre-obesity and 10% with obesity. Each 5 kg/m2 rise in BMI raises the risk by 4.2%, regardless of other factors like smoking or diet. While the exact mechanism is unclear, obesity may promote tumorigenesis through increased insulin and IGF-I levels, influencing cell growth and survival [15,16].
1.1.5. Pathogens
In parts of Sub-Saharan Africa, Schistosoma haematobium infection causes over half of bladder cancer cases. Schistosomiasis, the second most serious tropical disease after malaria, raises cancer risk significantly. In endemic areas, squamous cell carcinoma predominates, with diagnosis often between ages 40–49. Men are affected 4–5 times more often, likely due to occupational exposure [17,18,19].
1.1.6. Genetics
Many authors indicate a correlation between the occurrence of bladder cancer in a family and increased risk of developing this cancer in subsequent family members. Selected genetic mutations associated with this risk are presented in Table 1, along with their brief characteristics.

Table 1.
Genetic mutations associated with bladder cancer risk and their brief description.
1.1.7. Occupational Diseases
Around 20% of bladder cancer cases are linked to occupational exposure to chemicals, especially in industries like dye, paint, petrochemical, and metal processing. Male printing machine operators show significantly higher risk, independent of smoking. In women, no significant link was found after adjusting for exposure and smoking [27].
1.1.8. Genetics–Environment Interaction
Genetic–environmental interactions, particularly involving carcinogens like tobacco smoke or arsenic, significantly influence bladder cancer risk. Slow acetylators (NAT2 polymorphism) show higher susceptibility, especially heavy smokers (up to 3× risk) [28,29]. Similar risks apply to occupational exposure and use of hair dyes in women with slow NAT2 variants [30,31]. The absence of GSTM1, key in detoxification, also raises the risk, notably with high environmental exposure [32,33]. Lesseur et al. found increased bladder cancer risk in those with specific genotypes (e.g., AQP3, GST) and high arsenic exposure [34]. Variants in the MnSOD, COMT, and NQO1 genes combined with smoking or PAH exposure further elevated risk, particularly with the MnSOD Val/Ala genotype [35,36].
1.1.9. Eating Habits and Physical Activity
Diet and physical activity also influence bladder cancer risk. A diet rich in fruits and vegetables, especially citrus and cruciferous types like broccoli, has a protective effect (RR 0.84; 95% CI 0.77–0.91) [37,38]. Regular black tea consumption was also linked to reduced risk (RR 0.79; 95% CI 0.59–0.99) [39]. Dairy intake, particularly skimmed and fermented milk, was associated with lower risk (RR 0.84; 95% CI 0.72–0.97), whereas whole milk increased it (RR 2.23; 95% CI 1.45–3.00) [40]. While red meat showed no strong link, processed meats raised the risk (RR 1.22; 95% CI 1.04–1.43) [41]. Supplementation with vitamins A, E, and D correlated with reduced risk (RR 0.82 for A and E; RR 0.75; 95% CI 0.65–0.87 for D) [42,43,44], and selenium also showed protective effects (RR 0.61; 95% CI 0.42–0.87) [45]. Surprisingly, antioxidant supplements increased bladder cancer risk by 52% (RR 1.52; 95% CI 1.06–2.17) [46].
Higher levels of physical activity are linked to a significantly reduced risk of bladder cancer (RR 0.86; 95% CI 0.77–0.95), independent of BMI or smoking status [47]. On a cellular level, physical activity supports defense mechanisms by modifying carcinogen activity, enhancing DNA repair, and boosting antioxidant defenses [48,49].
1.1.10. The Role of the Microbiome
The urinary tract microbiome, once thought sterile, influences immune responses and may contribute to bladder cancer via chronic inflammation and the activation of pathways like TLRs, JAK-STAT3, NF-κB, and PI3K-Akt-mTOR [50,51]. E. coli infections may promote carcinogenesis by activating NF-κB and inhibiting apoptosis [52]. Age-related microbiome shifts may increase infection risk and cancer susceptibility [53,54].
1.2. Types and Subtypes of Bladder Cancer
Below is Figure 1 showing the frequency of the types of bladder cancer worldwide in a bar chart.
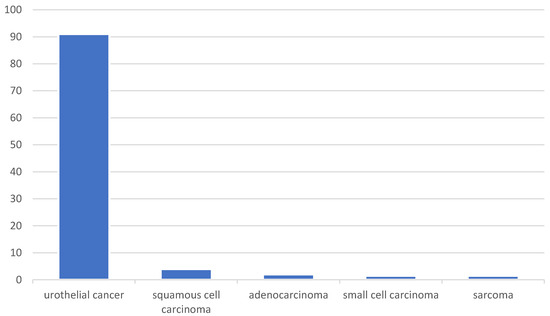
Figure 1.
The incidence of different types of bladder cancer. Urothelial cancer accounts for the majority of cases (91%), while the other types occur much less frequently: squamous cell carcinoma (4%), adenocarcinoma (2%), sarcoma (1.5%), and small cell carcinoma (<1.5%).
Bladder cancer includes several histological types, with urothelial carcinoma being the most common (~91%). It is classified into invasive (MIBCa) and non-invasive (NMIBCa) forms, with the former carrying higher metastatic risk. Squamous cell carcinoma (~4%) is linked to Schistosoma haematobium and is highly aggressive. Adenocarcinoma (~2%) is associated with congenital anomalies. Rare types include sarcomas (~1.5%), typically in younger patients, and small cell carcinoma (<1.5%), which is aggressive and requires intensive treatment [54].
2. Materials and Methods
The aim of this review was to present the dynamically evolving directions in the treatment of bladder cancer, which in recent years have significantly expanded therapeutic options in oncology. Particular attention was given to modern methods that go beyond traditional approaches, offering new perspectives for more effective and targeted therapies.
This article provides a comprehensive synthesis of recent innovations in bladder cancer treatment, with a special emphasis on emerging therapeutic strategies that have the potential to transform clinical practice. By integrating findings from the past several years, this review contributes a current and forward-looking perspective on bladder cancer management—highlighting both clinical advances and promising directions in translational research.
The analysis included studies on innovative methods of bladder cancer treatment published over the past seven years, starting from 2018, with the exception of works describing standard approaches, where articles published as early as 2000 were considered. The review focused on modern therapeutic approaches such as immunotherapy, targeted therapies, antibody–drug conjugates, gene therapies, and photodynamic therapies. Given the rapid development of novel oncological treatments, particular emphasis was placed on clinical trials in advanced phases (II–IV) as well as meta-analyses and systematic reviews that reliably discussed innovations in bladder cancer therapy. In the case of preclinical studies, only those that significantly contributed to the development of future therapeutic strategies were included.
The exclusion criteria comprised studies that did not directly relate to bladder cancer or focused exclusively on traditional surgical techniques and chemotherapy without offering novel perspectives. Also excluded were studies with a narrow scope, those focusing solely on palliative or long-term care, as well as speculative articles lacking empirical support. The time-based criterion also led to the exclusion of articles published before 2018, except for those addressing the foundations of standard treatment modalities.
The literature search was conducted using three major databases: PubMed, Scopus, and Web of Science. PubMed, as one of the most widely used sources for biomedical literature and clinical studies, was utilized to identify up-to-date systematic reviews and primary research. Scopus provided access to a broad array of publications describing innovative therapies and experimental treatment strategies, while Web of Science was used to identify cutting-edge studies in oncology and biomedicine.
The search was based on a set of precisely selected keywords, including “Bladder cancer”, “Innovative treatment”, “Immunotherapy”, “Targeted therapy”, “Gene therapy”, “Antibody-drug conjugates”, “Photodynamic therapy”, “Microbiome and bladder cancer”, and “Side effects in bladder cancer treatment”. The selection of keywords aimed to capture the most relevant and recent studies on modern treatment methods for bladder cancer. Throughout the review process, particular care was taken to ensure that the analysis reflected the latest clinical research findings and the current state of scientific knowledge.
In the course of the literature analysis, the effectiveness and limitations of the studied methods were evaluated, with a focus on their potential benefits for patients and their applicability in setting new treatment standards. This article adds value by integrating recent advances and identifying therapeutic trends that go beyond traditional treatment, thus offering a comprehensive overview of cutting-edge strategies that are shaping the future of bladder cancer care.
3. Results
3.1. Current Treatment Standards
3.1.1. Localized Immunotherapeutic and Chemotherapeutic Approaches
Bacillus Calmette–Guérin (BCG) immunotherapy is the standard treatment for patients with intermediate- to high-risk non-muscle-invasive bladder cancer (NMIBC). Originally developed as a vaccine against tuberculosis, BCG has potent immunostimulatory effects against cancer. When administered intravesically, BCG activates a complex immune response, including dendritic cells, macrophages, NK cells, and T lymphocytes, triggering the production of cytokines that support the fight against the tumor. Treatment usually begins with a six-week induction course, followed by maintenance therapy for up to three years, which significantly reduces the risk of relapse and disease progression. BCG is also preferred for cancers containing carcinoma in situ (CIS), where it effectively delays the need for more invasive methods. Despite potential side effects such as irritant symptoms and mycobacterial infections, BCG remains the gold standard treatment for NMIBC, with promising studies to further improve this immunotherapy [55].
On 16 December 2022, the FDA authorized the use of nadofaragene firadenovec-vncg (Adstiladrin), marking it as the first gene therapy utilizing adenoviral vectors approved for adults with high-risk NMIBC and carcinoma in situ who did not respond to BCG treatment. The treatment’s effectiveness was confirmed in the CS-003 clinical trial, which included 98 participants receiving intravesical administration every three months. A complete response was observed in 51% of patients after three months (95% CI: 40.7–61.3%), with 46% of those maintaining this response for at least a year. The median duration of response was 9.7 months, ranging from 3 to over 52 months [56].
Nogapendekin alfa inbakicept-pmln (NAI) is an immunotherapy for patients with NMIBC who do not respond to BCG treatment. Due to the limited effectiveness and side effects of BCG, alternative therapies are urgently needed. NAI is a recombinant fusion protein that combines a targeting domain binding to tumor cells with a modified cytokine that stimulates a local immune response. This dual mechanism enables both precision targeting and immune activation. In a phase II clinical trial, NAI achieved a 45% complete response rate in patients with carcinoma in situ unresponsive to BCG, outperforming other second-line therapies. It was well tolerated, with mostly mild side effects. NAI, alone or in combination with BCG, represents a promising bladder-sparing option, particularly for patients ineligible for radical cystectomy [57].
Intravesical gemcitabine and docetaxel (Gem/Doce) is a promising bladder-sparing option for high-risk NMIBC, particularly amid BCG shortages. In a study of 138 patients, including 9 with focal micropapillary urothelial carcinoma (MPUC), 24-month high-grade recurrence-free survival was 89% for MPUC and 80% for conventional urothelial carcinoma, with no significant difference. None of the MPUC patients progressed, required cystectomy, or died. Recurrent cases responded well to salvage valrubicin and docetaxel (Val/Doce), suggesting that sequential therapy may be effective in select patients. These results support Gem/Doce as a viable option, though further prospective studies are needed [58].
Given the limitations of systemic pembrolizumab, particularly its toxicity profile and limited durable responses in BCG-unresponsive, this phase I study (NCT02808143) explored an alternative delivery method via the bladder. Nine patients received intravesical pembrolizumab at doses of 1 or 2 mg/kg alongside standard BCG instillations. The median recurrence-free survival reached 6.2 months, with only 22% of participants free from recurrence at one year. Most treatment-related adverse events were low grade and localized to the urinary tract, with only one immune-mediated fatal event (myasthenia gravis) observed at the higher dose. Notably, pembrolizumab was undetectable in systemic circulation, indicating localized drug activity. Immune monitoring via urine and spatial transcriptomic analysis of tumor tissue revealed enhanced immune engagement within the bladder microenvironment in patients with delayed recurrence. These preliminary findings support the feasibility and potential benefit of bladder-directed checkpoint inhibition, meriting further clinical investigation [59].
3.1.2. Surgical Approach
Transurethral resection of bladder tumor (TURBT) is the fundamental diagnostic and therapeutic approach for non-muscle-invasive bladder cancer (stages Ta, T1). Its quality significantly affects oncological outcomes, as incomplete tumor removal increases the risk of recurrence and progression. A key quality marker is the presence of detrusor muscle in the resected specimen, ensuring accurate staging. Its absence is linked to worse five-year survival, while its presence reduces recurrence rates. For high-grade T1 tumors, repeat resection (reTURBT) is recommended to confirm staging and remove residual disease. Urological guidelines (EAU, NICE, NCCN, AUA) underline the importance of complete resection and reTURBT in high-grade cases to improve outcomes [60].
In advanced bladder cancer, radical cystectomy (RC) and robot-assisted radical cystectomy (RARC) are the main treatment options. While RC remains the standard, RARC offers benefits like reduced blood loss and fewer transfusions. Both techniques yield comparable oncological results, including overall and recurrence-free survival. Despite longer operative time, RARC provides better surgical visualization and hemostasis. However, complication rates and health-related quality of life (HRQOL) at 30 and 90 days post-op are similar, indicating a comparable safety and quality of life profile [61].
Partial cystectomy (PC) is an operation that involves removing the tumor along with a margin of healthy tissue, leaving the remaining part of the bladder intact. This procedure is used in selected patients with bladder cancer, especially when the tumor is single, well located, and confined to one part of the bladder. The goal of PC is to preserve bladder function and avoid more radical procedures, which can significantly affect the quality of life of patients, especially younger ones, for whom complete removal of the bladder (radical cystectomy) would involve significant changes in daily functioning. However, PC is more invasive than endoscopic methods because it requires opening the abdomen. This prolongs the operation, increases the risk of complications such as infections, and prolongs hospitalization and recovery. Although the procedure aims to remove all cancer cells, there is a risk of recurrence or progression of the cancer, which means that patients require regular and long-term follow-up after surgery. Despite the greater surgical challenges, PC can be an effective option for patients who wish to preserve bladder function and have a good prognosis for complete recovery. Regular follow-up examinations, such as cystoscopy and imaging studies, are essential to monitor disease recurrence and enable prompt intervention if needed. It is important to note that a rigorous follow-up protocol is equally crucial after radical cystectomy, not only in bladder-preserving approaches [62].
3.1.3. Chemotherapeutic Approach
Neoadjuvant chemotherapy (NAC) is the standard approach for patients with muscle-invasive bladder cancer (MIBC) who are eligible for cisplatin-based treatment. Administered before radical cystectomy, NAC—most commonly in the form of gemcitabine and cisplatin over four cycles—reduces tumor size, facilitates surgical resection, and targets micrometastases. This strategy significantly improves both overall survival and event-free survival, decreasing the risk of recurrence and progression [63].
Adjuvant chemotherapy (AC), provided after cystectomy, is recommended for patients with high-risk features such as lymph node involvement (pN+). Its goal is to eliminate residual microscopic disease and prevent relapse. While AC improves survival compared to no chemotherapy (5-year OS: 42.6% vs. 37.8%), its efficacy appears slightly lower than NAC (5-year OS: 48.3%). Despite its benefits, AC is used less frequently, which may stem from fewer supporting studies, lack of consensus on indications, and limited eligibility among older or comorbid patients [64].
The VESPER (GETUG-AFU V05) trial was a randomized phase III study comparing two perioperative chemotherapy regimens—dose-dense MVAC (dd-MVAC) and gemcitabine–cisplatin (GC)—in patients with MIBC. Among 493 enrolled patients, most (88%) received neoadjuvant chemotherapy. While the trial did not meet its primary endpoint in the entire cohort (3-year PFS: 64% for dd-MVAC vs. 56% for GC; p = 0.066), dd-MVAC significantly improved 3-year PFS in the neoadjuvant group (66% vs. 56%; HR = 0.70; p = 0.025). dd-MVAC also led to better local tumor control and longer time to progression, despite comparable complete response rates. Although dd-MVAC was associated with higher rates of hematologic and gastrointestinal toxicity, it did not increase postoperative complications. The study suggests that dd-MVAC is a feasible and more effective neoadjuvant option for fit patients with MIBC, and it may become the preferred regimen pending overall survival data [65].
The NIAGARA trial (NCT03732677), a phase III randomized study, assessed the efficacy of adding durvalumab to standard neoadjuvant gemcitabine–cisplatin chemotherapy in cisplatin-eligible patients with MIBC. Patients received either chemotherapy alone followed by radical cystectomy or perioperative durvalumab—administered during neoadjuvant treatment and continued postoperatively for eight cycles. At 24 months, event-free survival was significantly improved in the durvalumab group (67.8% vs. 59.8%; HR = 0.68; p < 0.001), as was overall survival (82.2% vs. 75.2%; HR = 0.75; p = 0.01). Grade 3–4 adverse events occurred at similar rates in both groups (~41%), and radical cystectomy completion rates remained high (88.0% vs. 83.2%). These results support perioperative durvalumab as a new standard approach in MIBC treatment [66].
The CheckMate 274 trial (NCT02632409) was a phase III, randomized, double-blind study assessing the efficacy of adjuvant nivolumab in patients with high-risk MIBC after radical surgery. Participants were randomized to receive either nivolumab (240 mg every two weeks for up to one year) or placebo. Prior neoadjuvant cisplatin-based chemotherapy was allowed. The results showed a notable extension of disease-free survival (DFS) in the nivolumab group compared to placebo—20.8 vs. 10.8 months in the overall population (HR = 0.70; p < 0.001). Among patients with PD-L1 expression ≥1%, the benefit was even more significant (HR = 0.55; p < 0.001). Nivolumab also improved distant recurrence-free survival (22.9 vs. 13.7 months; HR = 0.72). Grade ≥3 treatment-related adverse events occurred in 17.9% of the nivolumab group versus 7.2% in the placebo group, with two fatal cases of pneumonitis. These findings suggest that adjuvant nivolumab provides a clinically meaningful benefit in reducing recurrence risk after surgery, especially in PD-L1 positive patients [67].
The AMBASSADOR (A031501) study was a phase III randomized clinical trial assessing adjuvant pembrolizumab in patients with high-risk MIBC after radical surgery. Participants were randomized to receive pembrolizumab (200 mg every 3 weeks for up to one year) or observation. The primary outcomes were disease-free survival (DFS) and overall survival (OS). At a median follow-up of nearly 45 months, pembrolizumab significantly improved DFS compared to observation (29.6 vs. 14.2 months; HR = 0.73; 95% CI, 0.59–0.90; p = 0.0027). The benefit was observed regardless of PD-L1 expression, prior neoadjuvant chemotherapy, or disease location. Interim analysis of OS showed no significant difference (HR = 0.98; 95% CI, 0.76–1.26), possibly due to crossover to immunotherapy in the observation group. Grade ≥ 3 adverse events were more frequent with pembrolizumab (50.7% vs. 31.6%), though no unexpected safety concerns emerged. These findings support the use of adjuvant checkpoint inhibition in improving DFS for select patients with high-risk MIBC, which is consistent with the results from previous studies using similar immunotherapies [68].
3.1.4. Radiotherapy Approach
Radiotherapy (RT) is an important alternative in the treatment of bladder cancer and is gaining importance as an option for patients eligible for radical treatment, in addition to RC. In patients with clinically positive lymph nodes (cN+ M0), radiotherapy can be used in a radical form (RadRT) as an option that allows for bladder preservation. Studies have shown that patients undergoing RadRT have comparable overall survival (OS) and progression-free survival (PFS) to those who underwent cystectomy. Radiotherapy regimens used in patients with advanced disease may include irradiation of both the bladder itself and the surrounding lymph nodes, which allows for tailoring the treatment to the individual patient’s situation. Radiotherapy also offers the possibility of using radiosensitizers such as gemcitabine or mitomycin, which increase the effectiveness of the therapy by enhancing the tumor response. Current data suggest that in selected cases, RadRT may be an effective treatment option in patients for whom bladder preservation is a priority [69].
3.1.5. Trimodal Therapy
Trimodal therapy (TMT) is an effective bladder-preserving treatment option for selected patients with muscle-invasive bladder cancer (MIBC). It combines three components: radical transurethral resection of the bladder tumor (TURB), radiotherapy, and radiosensitizing chemotherapy (e.g., cisplatin or mitomycin C with 5-fluorouracil). TMT is considered an alternative to radical cystectomy, especially for older patients or those with comorbidities. Two treatment schedules are used: split-course (with interim evaluation) and continuous-course (with post-treatment evaluation). When properly selected—patients with good bladder function, cT2 tumors, no hydronephrosis—TMT shows outcomes comparable to cystectomy, with complete response rates of 60–80% and 5-year disease-specific survival of 60–70%. Importantly, TMT helps preserve bladder function and quality of life, with about 75% of patients maintaining normal bladder control. In the case of recurrence, salvage cystectomy remains an option. Current research explores combining TMT with immunotherapy (e.g., PD-1/PD-L1 inhibitors), which may further improve outcomes. For carefully selected patients, TMT is becoming an increasingly viable treatment alternative [70].
3.1.6. Mitomycin C (MMC) Approach
Mitomycin C (MMC) is a widely used intravesical chemotherapeutic agent for non-muscle-invasive bladder cancer (NMIBC), with a well-established mechanism of DNA crosslinking and limited systemic absorption. Despite its effectiveness, recurrence rates remain high, prompting strategies to optimize its delivery. These include increasing the dose to 40 mg, alkalizing urine, restricting fluids, and extending dwell time—measures that significantly improve recurrence-free survival. Advanced delivery methods such as chemohyperthermia (C-HT) and electromotive drug administration (EMDA) further enhance MMC penetration and efficacy, especially in high-risk patients. Maintenance therapy with MMC may also reduce recurrence, though data are mixed. Combination regimens—particularly with gemcitabine—show promise, while combinations with BCG have not proven superior, except when EMDA is used. Emerging research into drug resistance mechanisms (e.g., MDR1 expression, β1-integrin activity, HSPs) aims to enable more personalized treatment. When applied in optimized or combination protocols, MMC remains a key tool in the effective management of NMIBC [71].
3.2. The Distinction Between Non–Muscle-Invasive and Muscle-Invasive Bladder Cancer Treatments
Treatment strategies for bladder cancer differ significantly depending on whether the disease is classified as non–muscle-invasive (NMIBC) or muscle-invasive (MIBC).
NMIBC is typically managed with organ-sparing, localized therapies, including intravesical treatments such as Bacillus Calmette–Guérin (BCG) and chemotherapy agents like mitomycin C, gemcitabine, and docetaxel. Gene therapy (e.g., nadofaragene firadenovec) and novel immunotherapeutics like nogapendekin alfa inbakicept are emerging options for BCG-unresponsive cases. Surgery is limited to transurethral resection of bladder tumor (TURBT), often followed by re-TURBT for staging and complete resection.
In contrast, MIBC requires more aggressive, systemic treatment. The standard of care includes neoadjuvant cisplatin-based chemotherapy followed by radical cystectomy or trimodal therapy (TURBT + chemoradiation) for bladder preservation. Adjuvant immunotherapies, such as nivolumab or pembrolizumab, improve disease-free survival post-cystectomy in high-risk patients. Radiotherapy, sometimes combined with radiosensitizers, offers a bladder-preserving alternative in select cases.
In summary, NMIBC focuses on bladder preservation through localized treatment, while MIBC management involves multimodal systemic therapies and radical surgery, reflecting the more aggressive nature of invasive disease [55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71].
3.3. Potential Side Effects of Traditional Treatments
For non–muscle-invasive bladder cancer (NMIBC), intravesical BCG remains the gold standard but can cause local irritative symptoms (e.g., dysuria, frequency) and, less commonly, systemic complications such as mycobacterial infections. Newer agents like nadofaragene firadenovec have shown a favorable safety profile, with most adverse effects being mild and localized. Nogapendekin alfa inbakicept was also well tolerated, with low-grade immune-related effects. Intravesical gemcitabine/docetaxel and mitomycin C (MMC) are generally well tolerated, though MMC can cause chemical cystitis, and advanced delivery methods (e.g., chemohyperthermia, EMDA) may increase local irritation. Systemic toxicity is rare due to limited drug absorption.
For muscle-invasive bladder cancer (MIBC), treatment-related toxicity is more significant. Neoadjuvant and adjuvant cisplatin-based chemotherapy frequently causes hematologic (anemia, neutropenia) and gastrointestinal toxicities (nausea, vomiting, mucositis). In the VESPER trial, dd-MVAC led to higher toxicity compared to gemcitabine–cisplatin, though without increased postoperative complications. Immune checkpoint inhibitors (e.g., nivolumab, pembrolizumab) used in the adjuvant setting may induce immune-related adverse events, including pneumonitis, fatigue, and endocrinopathies. In AMBASSADOR, grade ≥ 3 AEs occurred in over 50% of patients receiving pembrolizumab.
Radiotherapy, particularly in trimodal therapy (TMT), can cause local side effects such as cystitis, proctitis, and fatigue, while combining with radiosensitizing chemotherapy increases the risk of hematologic and gastrointestinal toxicity. However, modern techniques have improved tolerability.
Overall, localized treatments for NMIBC have mostly manageable local toxicities, while systemic therapies for MIBC pose higher risks of serious adverse events, requiring careful patient selection and monitoring [55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71].
3.4. Types of Innovative Therapies and Latest Research in BC Treatment
In recent years, there has been significant progress in the field of BC treatment, focusing on the development of innovative therapies that can increase the effectiveness of treatment and improve patient prognosis. New approaches include targeted therapies, immunotherapy, and gene therapies, which aim not only to destroy cancer cells but also to inhibit the mechanisms that promote their growth and metastasis. In the following section, we will discuss the most important innovative therapies and the results of the latest research that shape the future of BC treatment and may be a significant step towards more personalized and effective cancer care.
3.4.1. Immunotherapy
New Prognostic or Predictive Biomarkers and Immune Checkpoint Inhibitors (ICIs)
Programmed death-ligand 1 (PD-L1) is a transmembrane protein belonging to the immunoglobulin superfamily, playing a central role in the regulation of immune responses. Its expression on cancer cells allows them to evade immune surveillance by binding to the PD-1 receptor on T lymphocytes, thereby inhibiting their activity and enabling tumor immune escape, which facilitates cancer progression. In recent years, PD-L1 has become a crucial therapeutic target in oncology, particularly with the emergence of immune checkpoint inhibitors (ICIs), such as monoclonal antibodies targeting PD-1/PD-L1. These therapies have revolutionized the treatment of advanced bladder cancer, particularly in patients ineligible for cisplatin-based chemotherapy. In 2017, the FDA approved atezolizumab and pembrolizumab for patients with locally advanced or metastatic urothelial carcinoma, based on studies showing moderate objective response rates and durable clinical benefit, regardless of PD-L1 expression, although responses were more frequent in PD-L1 high-expressing tumors [72].
The development of immunotherapy has also expanded the search for predictive biomarkers. Circulating tumor DNA (ctDNA) has emerged as a promising non-invasive tool. One study demonstrated that changes in variant allele frequency (VAF) in ctDNA after six weeks of anti-PD-L1 therapy correlated with clinical outcomes—patients with reduced VAF had longer progression-free survival (PFS) and overall survival (OS), suggesting that ctDNA dynamics could help identify non-responders and inform early treatment adjustments [73].
Equally critical is the precise assessment of PD-L1 expression in tumor tissues. The Ventana PD-L1 (SP263) assay has been validated for this purpose, demonstrating high analytical precision and reproducibility. In the CD-ON-MEDI4736-1108 trial, durvalumab showed durable responses across both PD-L1 high and low expressers, with greater efficacy in the former, underlining the assay’s value in treatment selection [74]. Further evidence comes from the PURE-01 study, where neoadjuvant pembrolizumab significantly improved event-free survival (EFS) in muscle-invasive bladder cancer (MIBC) patients with high PD-L1 expression—89.8% in those with high combined positive score (CPS) versus 59.7% in those with low CPS (p = 0.0013) [75].
Additionally, the phase III KEYNOTE-361 trial reinforced the role of PD-L1 CPS and tumor mutational burden (TMB) as predictive biomarkers. Patients with high TMB (≥175 mutations/exome) and high CPS (≥10) experienced better PFS, OS, and objective response rates (ORRs) with pembrolizumab, either alone or with chemotherapy. These findings underscore the value of combining PD-L1 and TMB in stratifying patients for immunotherapy and enhancing treatment personalization [76].
Among ICIs, those targeting PD-1, PD-L1, and CTLA-4 have become pivotal in MIBC treatment, particularly in advanced or metastatic stages. Pembrolizumab and atezolizumab are now standard options in this setting. Another promising checkpoint target is lymphocyte-activation gene 3 (LAG-3). The elevated expression of LAG-3 on stromal immune cells has been associated with reduced OS and disease-free survival in MIBC, as well as poor response to adjuvant chemotherapy. Tumors with high LAG-3+ cell infiltration exhibit an immunosuppressive microenvironment enriched with cytokines and other checkpoints and are linked to CD8+ T cell dysfunction. LAG-3 expression correlates with luminal and basal molecular subtypes, reduced frequency of FGFR3 mutations, and enhanced EGFR pathway activation. Thus, LAG-3 may serve both as a prognostic biomarker and a potential therapeutic target, although further prospective studies are required to confirm its clinical relevance [77].
The efficacy of checkpoint inhibition was further demonstrated in the phase III JAVELIN Bladder 100 trial, where maintenance therapy with avelumab after platinum-based chemotherapy significantly improved OS and PFS compared to best supportive care (BSC) alone (HR for OS: 0.63–0.79). In this study involving 700 patients with advanced urothelial cancer (UC), avelumab was generally well tolerated, though grade ≥ 3 adverse events were reported in 43–62% of cases. These results established avelumab maintenance as a new standard of care in advanced UC and emphasized the growing impact of ICIs in modern uro-oncology [78].
New Bladder Cancer-Specific Antigens
Sialylated tumor-derived IgG (SIA-CIgG) has been identified as a promising bladder cancer-specific antigen with minimal expression in healthy tissues. Studies have shown that CAR-T cells targeting SIA-CIgG effectively kill bladder cancer cells, and their cytotoxicity is dependent on the expression level of this antigen. Compared to HER2-targeted CAR-Ts, SIA-CIgG CAR-Ts demonstrate milder tumor cell lysis and improved functional durability, making them a potentially safer therapeutic option. Furthermore, the combination of SIA-CIgG CAR-Ts with the histone deacetylase inhibitor (HDACi), vorinostat, significantly increases the ability of CAR-Ts to kill tumor cells, suggesting the benefits of combination therapy [79]. Nectin-4, a protein widely expressed in conventional urothelial cancer (UC), is a promising therapeutic target for the antibody–drug conjugate enfortumab-vedotin (EV). Studies have shown that 87% of non-muscle-invasive and 58% of musculoskeletal cancer samples expressed nectin-4. The highest expression was observed in non-muscle-invasive papillary carcinomas (97%) and in situ carcinomas (87.5%). However, nectin-4 expression is variable in other morphological variants of bladder cancer. Low or absent expression occurs in small cell carcinomas (0%) and sarcomatoid carcinomas (10%). RNA analyses have shown that these tumor variants often express other molecular targets, such as trop2, the target of sacituzumab-govitecan, and HER2/ERBB2, the target of trastuzumab-deruxtecan. Nectin-4 remains a key specific antigen for many types of bladder cancer, but testing its expression in less common UC variants may help personalize therapy. In cases of low nectin-4 expression, alternative molecular targets should be considered and treatment should be adjusted accordingly. These results underscore the importance of nectin-4 in developing new therapies for bladder cancer and indicate the need for further studies on antigens specific to this tumor [80].
Personalization of Immune Therapy- New Immunological Strategies
The tumor mutational profile, including parameters such as dMMR (deficient Mismatch Repair) and MSI-H (Microsatellite Instability-High), provides key prognostic and predictive information in bladder cancer immunotherapy. A 2024 systematic review examined the prevalence of dMMR and MSI-H in bladder cancer (BC) and upper urinary tract cancer (UTUC). The results showed that dMMR occurred in 2.3% of BC patients and 8.95% of UTUC patients, whereas MSI-H was detected in 2.11% of BC patients and 8.36% of UTUC patients. The prevalence of MSI-H was higher in localized tumors (5.26% in BC and 18.04% in UTUC) than in metastatic tumors (0.86% in BC and 4.96% in UTUC). In metastatic UC, dMMR/MSI-H patients treated with checkpoint inhibitors (ICIs) had a response rate of 64.7%, compared with 11.1% in patients treated with chemotherapy. These results suggest that dMMR and MSI-H may play a key role in predicting the efficacy of immunotherapy and supporting the personalization of treatment. Particularly in metastatic bladder cancer, these biomarkers may also indicate resistance to cisplatin-based chemotherapy, highlighting their importance in individualizing therapy [81]. In another study, long non-coding RNAs (lncRNAs) associated with necroptosis were identified as prognostic biomarkers supporting the personalization of immunotherapy in urothelial bladder cancer (BLCA). The developed lncRNA model showed high performance in predicting patient prognosis, with accuracy for 1-, 3-, and 5-year survival (AUC 0.707, 0.679, and 0.675, respectively). Analyses revealed differences in the tumor microenvironment, allowing for the division into “cold” and “hot” tumors. “Hot” tumors, characterized by higher immune activity, were more sensitive to immunotherapy, which increased their chances of effective response to immunological drugs. On the other hand, “cold” tumors, with lower immune activity, required the use of alternative therapeutic strategies. These results emphasize the importance of lncRNAs in identifying tumor characteristics and tailoring treatment to specific patient needs. Personalization of therapy based on these biomarkers can significantly improve the efficacy of bladder cancer treatment [82].
Cancer vaccines are a promising strategy for treating bladder cancer, which aim to stimulate the immune system to recognize and destroy cancer cells. Among the different approaches used to develop such vaccines are peptide vaccines, which use specific peptides derived from tumor antigens, such as MAGE-A3 or NY-ESO-1, which induce a T cell response against cancer cells. Another solution is dendritic cell-based vaccines, which load these cells with tumor antigens, which allows them to present these antigens to T cells and lead to their activation. DNA and RNA vaccines are gaining particular attention because they introduce genetic material encoding tumor antigens directly into the patient’s cells. This leads to the expression of antigens that stimulate the immune system. Viral vaccines, which use modified viruses as vectors to deliver genes encoding tumor antigens, work in a similar way. These methods are attractive because of their ability to quickly induce an immune response and their ease of production. mRNA-based vaccines are particularly promising and have gained increasing interest in recent years due to their successful use in other types of cancer. Despite promising results, challenges in the development of cancer vaccines include identifying appropriate tumor antigens, developing effective delivery methods, and overcoming immunosuppression mechanisms in the tumor microenvironment. Additionally, combining cancer vaccines with other forms of immunotherapy, such as checkpoint inhibitors, opens new possibilities to increase treatment efficacy and improve clinical outcomes in patients with bladder cancer. The development of this technology and clinical trials conducted in this field hold promise for more effective therapies for patients with this tumor [83].
CAR-T Therapy
CAR-T therapy (Chimeric Antigen Receptor T cell therapy) is one of the most advanced approaches in cancer immunotherapy, offering a unique opportunity to precisely destroy cancer cells. The basis of this method is the genetic modification of the patient’s T lymphocytes to express a chimeric antigen receptor (CAR), which allows them to recognize specific antigens on the surface of cancer cells. Once introduced into the patient’s body, CAR-T cells not only identify and destroy cancer cells, but can also create immunological memory, making this therapy a potential tool for preventing relapses. One of the breakthroughs in the development of CAR-T therapy in the treatment of bladder cancer is targeting the specific antigens mentioned in the previous subsections, such as Nectin-4 and SIA-CIgG. These antigens, due to their high expression in cancer cells and low presence in healthy tissues, are ideal targets for this therapy. Studies indicate that targeting these antigens can significantly increase the effectiveness of treatment and reduce the risk of relapses due to the ability of CAR-T cells to maintain immunological memory. This ability of the immune system to “remember” allows for long-term protection against disease progression, which is one of the main goals in the therapy of solid tumors. A novel approach in CAR-T therapy in the treatment of bladder cancer is the use of a mutated TIGIT co-receptor, targeting prostate stem cell antigen (PSCA). TIGIT has been modified to increase its affinity for the CD155 protein, which allows CAR-T cells to function more effectively in the immunosuppressive tumor microenvironment. Additionally, the use of CD28 activation signals in the CAR-T construct further enhances their effectiveness. Preclinical studies have shown that CAR-T cells targeting PSCA demonstrate higher production of cytokines, such as IFN-γ, and greater cytotoxic efficiency compared to traditional CAR-T constructs. In in vivo models, these cells were more effective in reducing the bioluminescent tumor signal, confirming their potential in the treatment of bladder cancer [84].
Despite promising results, CAR-T therapy in bladder cancer faces significant challenges. One of the main limitations is the immunosuppressive tumor microenvironment, which impairs the efficacy of T lymphocytes. Factors such as TGF-β cytokines inhibit the immune response, while others, such as IL-2 and IL-12, can support CAR-T activity, opening new therapeutic possibilities. Additionally, CAR-T therapy is associated with the risk of serious adverse events, such as cytokine release syndrome (CRS) or neurotoxicity (ICANS), which requires further research to develop strategies to minimize these complications [85].
3.4.2. Innovations in Targeted Therapies
Innovations in Targeted Therapies
FGFR3 (fibroblast growth factor receptor 3) is a key predictive biomarker for targeted therapy in bladder cancer, especially in advanced urothelial cancer (UC). The most common FGFR3 alterations are activating mutations, such as S249C and R248C, and gene fusions, including FGFR3-TACC3, which lead to constitutive activation of the receptors, driving tumor cell proliferation and disease progression [86,87,88]. FGFR3 alterations are more common in the luminal-papillary subtype of UC, which allows for the selection of patients for targeted therapy [89,90]. PD-L1 expression is found in approximately 20–30% of bladder cancer cases. Higher levels of PD-L1 expression are associated with more advanced disease stages and higher mortality, suggesting that PD-L1 has prognostic value and may be used as a biomarker in targeted therapies [91].
HER2, also known as ErbB2, is one of the human epidermal growth factor receptor (HER/ErbB) family members that plays a key role in regulating cell proliferation, tumor growth, and therapy resistance [92,93]. HER2 is distinguished by its ability to signal in a ligand-independent manner. Studies have shown that HER2 amplification, mutations, and overexpression occur in approximately 20–30% of patients with bladder cancer, making this receptor a significant therapeutic target [94].
Mutations in the TERT promoter (mainly C228T and C250T) are the most common somatic abnormalities in bladder cancer, occurring in 60–80% of cases, regardless of the stage of disease. The high sensitivity and specificity of TERT promoter mutations in urine samples make them promising markers for monitoring bladder cancer recurrence and early detection of cancer [95].
RB1 (Retinoblastoma 1) is a tumor suppressor gene that plays a key role as a negative regulator of the cell cycle. Its inactivation is associated with the carcinogenesis process in many cancers, including bladder cancer. Loss of RB1 expression has been independently associated with poor prognosis in muscle-invasive bladder cancer, including lower overall survival rates and a higher risk of recurrence after cystectomy [96,97]. TP53, a key tumor suppressor gene, is one of the most frequently mutated genes in bladder cancer (BLCA). Mutations in TP53 occur in nearly 50% of patients with BLCA, and functional inactivation of the gene occurs in as many as 76% of samples. TP53 is particularly associated with advanced stages of the disease, such as muscle-invasive bladder cancer (MIBC) and metastatic bladder cancer, and with poor prognosis in these cases [98].
MIB-1 is a monoclonal antibody directed against the Ki-67 protein, which is expressed in the active cell cycle phases (G1, S, G2, M), but not in the G0 (resting) phase. This makes it a sensitive indicator of tumor proliferative activity. High MIB-1 values are associated with a more aggressive phenotype of bladder cancer. Studies indicate that its expression is correlated with a higher risk of relapse and progression of the disease [99].
VEGF (vascular endothelial growth factor) plays a key role in the process of angiogenesis. It is essential for the growth and metastasis of tumors, including BC. Angiogenesis enables the delivery of nutrients and oxygen to rapidly growing tumors through a network of new blood vessels. In BC, increased VEGF expression is associated with an aggressive course of the disease, a higher risk of relapse, and metastasis [100,101].
MUTYH encodes the enzyme DNA glycosylase involved in the repair of oxidative DNA damage. It is a key enzyme responsible for the excision of adenines in aberrant pairs with 8-oxo-7,8-dihydroguanine, which helps maintain genome integrity. Oxidative DNA damage is common in cancers with high levels of oxidative stress, such as bladder cancer [102].
Personalization of Therapy Based on Tumor Molecular Profile
Targeted therapies represent a promising advance in bladder cancer treatment, emphasizing the importance of personalized approaches tailored to the molecular profile of individual tumors. Recent studies have identified distinct molecular subtypes of bladder cancer, characterized by unique genomic, transcriptomic, and proteomic alterations that influence disease progression and response to treatment. The integration of validated biomarker panels with clinical and epidemiologic data enables precise risk stratification and identification of patients who may benefit from targeted therapies. By interfering with key molecular pathways, such as FGFR3, p53, or angiogenesis regulators, targeted therapies allow for the inhibition of cancer progression at critical points. This approach personalizes the treatment, increasing its effectiveness and adapting it to specific biological features of the tumor [103].
Inhibitors of Specific Signaling Pathways
In a phase II cohort study, erdafitinib, an oral FGFR kinase inhibitor, was evaluated in patients with intermediate-risk non-invasive bladder cancer (IR NMIBC) with FGFR3/2 alterations. The study included 18 patients who had all tumors removed except for a marker tumor. Patients received erdafitinib at 6 mg daily for 28-day cycles, with follow-up cystoscopy after 3 months. Interestingly, after a median follow-up of 10 months, the complete response (CR) rate was 83.3%, and 11.1% of patients had a partial response (PR). The median time to response was 1.15 months, and the median duration of response (DOR) was 12.8 months. The most common side effects were hyperphosphatemia (100%), diarrhea (83.3%), and dry skin (50%). Importantly, there were no deaths in the study. Erdafitinib demonstrated high efficacy and safety profile in patients with IR NMIBC with FGFR mutations, representing a breakthrough in the treatment of patients with this mutation [104].
Rogaratinib, an oral FGFR1-4 inhibitor, has demonstrated promising efficacy and safety profile in the treatment of locally advanced or metastatic urothelial cancer (UC) with the overexpression of FGFR1/3 mRNA. In the phase II FORT-1 study (NCT03410693), its efficacy was compared with chemotherapy in patients previously treated with platinum-based chemotherapy. Rogaratinib achieved an objective response rate (ORR) of 20.7%, with a median overall survival (OS) of 8.3 months, which was comparable to chemotherapy (ORR 19.3%, OS 9.8 months). Exploratory analysis suggests that patients with FGFR3 DNA mutations and FGFR1/3 mRNA overexpression may have a better response to rogaratinib (ORR 52.4% vs. 26.7% for chemotherapy). Rogaratinib was well tolerated, with the most common adverse events including diarrhea, hyperphosphatemia, and fatigue. Grade 3 or higher events occurred in 43% of patients but were mostly manageable. There were no rogaratinib-related deaths. Although phase II results did not support progression to phase III in the population selected solely based on FGFR1/3 mRNA overexpression, the analysis suggests that combining FGFR3 mutation and mRNA expression analysis may better identify patients who would benefit most from therapy. Rogaratinib represents a potential alternative for patients with chemotherapy-refractory UC, which requires further study in well-defined subgroups [105].
Pemigatinib, a selective oral FGFR1-3 inhibitor, has antitumor activity in urothelial cancer (UC) with FGFR3 mutations or rearrangements. In the phase II FIGHT-201 study, it achieved an objective response rate (ORR) of 17.8% with the continuous regimen and 23.3% with the intermittent regimen, with a median duration of response (DOR) of 6.2 months and a median progression-free survival (PFS) of 4.0–4.3 months. The best results were achieved in patients with S249C, R248C, and G370C mutations (ORR up to 29%), whereas efficacy was lower with FGFR3 fusions (17%). Pemigatinib was generally well tolerated; the most common adverse events were diarrhea (44.6%), alopecia, stomatitis, and hyperphosphatemia (42.7% each), and more severe events such as stomatitis (8.8%) and anemia (8.1%) were rare. Resistance mechanisms included secondary FGFR3 mutations (e.g., V555M/L and N540K/S), and concomitant alterations in PI3K pathway genes (e.g., TSC1) correlated with poorer treatment response. Pemigatinib represents an important therapeutic option for previously treated patients with FGFR3-altered UC, especially in the context of molecular profiling, which highlights the importance of further studies on combination therapies and the optimization of predictive biomarkers [106].
Everolimus and Temsirolimus, first-generation mTOR inhibitors, are being studied for the treatment of bladder cancer. They act by inhibiting mTORC1, which leads to the inhibition of cell proliferation and angiogenesis. Everolimus shows moderate efficacy, especially in patients with mutations in the TSC1 or PIK3CA genes, but is accompanied by significant toxicity, including insulin resistance, pneumonia, and hyperlipidemia. Studies have shown that genetic analysis can help identify patients most responsive to therapy. Temsirolimus shows similar efficacy, with favorable outcomes in 48.9% of patients in clinical trials. However, as many as 94% of patients experienced adverse events, 53% of which were severe. Efficacy was higher in patients with TSC1 mutations. As can be seen, both drugs have encountered limitations related to toxicity and efficacy in monotherapy. Currently, studies are focusing on combination therapy with other signaling pathway inhibitors, which may improve treatment efficacy [107].
The PI3K/Akt/mTOR pathway, which is implicated in UC cell proliferation and invasion, represents a promising therapeutic target. Alterations in the PIK3CA gene occur in 25% of UC cases, but studies of mTOR and PI3K inhibitors to date have shown modest efficacy, suggesting a need to identify specific molecular changes that may sensitize tumors to these therapies. Buparlisib (BKM120) is an oral PI3K inhibitor that is being tested in a phase II trial in patients with metastatic UC refractory to platinum chemotherapy. Although the trial did not meet its primary endpoint (8-week progression-free survival (PFS) of 54%), one patient with a TSC1 mutation achieved a durable partial response (PR) at 15.9 months. Retrospective analyses have shown that buparlisib inhibits mTOR signaling in TSC1-mutated tumors, which may explain its efficacy in some patients. Toxicity was significant, with common adverse events including hyperglycemia, fatigue, and mood disorders. The results suggest that mutations in TSC1 may be associated with sensitivity to buparlisib, although the lack of clear predictive evidence limits its use. Buparlisib has shown limited efficacy in UC, but the results suggest the potential value of selective therapy in molecularly defined patient subgroups. Future studies of more specific PI3K inhibitors and combination therapies are needed to improve treatment efficacy in this clinically challenging patient population [108].
Bevacizumab, a humanized monoclonal antibody against VEGF-A, inhibits angiogenesis, a key process in tumor growth and progression. In bladder cancer, blocking VEGF-A has been used to reduce tumor perfusion, inhibit tumor growth, and improve the efficacy of chemotherapy. However, in a phase III trial (CALGB 90601), the addition of bevacizumab to standard chemotherapy with gemcitabine and cisplatin did not improve overall survival, although it did slightly prolong progression-free survival (by 1.3 months), which was considered clinically insignificant. Bevacizumab was also associated with adverse events, including hypertension and proteinuria. Despite previous promising results, bevacizumab has not changed the standard of care for bladder cancer, and its use requires further investigation of biomarkers that identify patients who are most likely to benefit from this therapy [109].
The JAVELIN Medley VEGF trial evaluated avelumab (PD-L1 inhibitor) and axitinib (VEGFR inhibitor) in patients with advanced urothelial cancer who were ineligible for cisplatin-based chemotherapy. The objective response rate (ORR) was 10%, with partial responses in two patients. The median progression-free survival (PFS) was 2.3 months and overall survival (OS) was 21.2 months. A higher percentage of CD8+ tumor cells was associated with better outcomes, suggesting a potential role for immunomodulation. The safety profile was consistent with previous studies, although 50% of patients experienced serious adverse events, including hypertension and fatigue, and the therapy was associated with two deaths. The therapy showed limited efficacy in this group of patients but may be an option for cisplatin-ineligible patients, requiring further study to optimize its use [110].
A study published in 2024 presented the role of the HER2 receptor (erbB2) and its ERBB2 signaling pathway in cancer treatment and HER2-targeted therapy, which has revolutionized the treatment of breast cancer and is used in other types of cancers—including BC. HER2 plays a key role in cancer progression, and its overexpression and amplification are associated with an aggressive course of the disease. Depending on the type of cancer, HER2 changes affect prognosis differently, justifying the use of different targeted therapies. HER2 is currently a therapeutic target in several types of cancer, and tyrosine kinase inhibitors such as lapatinib and tucatinib and ADCs such as trastuzumab emtansine (T-DM1) and trastuzumab deruxtecan (T-DXd) have shown clinical efficacy. However, different cancers require different approaches due to different patterns of HER2 expression. The challenge in this therapy is treatment resistance—acquired and primary resistance to anti-HER2 drugs, which is the result of mechanisms such as the activation of alternative signaling pathways, the aberrant expression of HER ligands, and changes in the tumor microenvironment [111].
Development of Technologies Related to Targeted Therapy
Bladder cancer, especially non-muscle-invasive bladder cancer (NMIBC), remains a therapeutic challenge due to its high rates of recurrence and progression. CRISPR/Cas9 technology, which allows for precise genome editing, offers new treatment options by targeting the DAD1 gene, which is responsible for anti-apoptotic regulation and is overexpressed in bladder cancer cells. Preclinical studies have shown that silencing DAD1 with CRISPR/Cas9 leads to apoptosis of cancer cells, reducing tumor growth in in vitro and in vivo models. By using innovative carriers such as fluorinated polymers PLLF, it is possible to effectively deliver the CRISPR/Cas9 system via intravesical instillation, which ensures better penetration of the bladder mucosa and reduces side effects. Preclinical results demonstrate the high efficacy and biocompatibility of this technology, which opens new possibilities for the treatment of bladder cancer, although it requires further clinical validation. CRISPR/Cas9 offers a highly precise and flexible gene editing approach that may contribute to future therapeutic strategies for treatment-resistant bladder cancer [112].
The multi-omics system, including technologies such as genomics, transcriptomics and proteomics, significantly supports the development of targeted therapies in BC. It enables the identification of biomarkers, such as the multidimensional PD-L1 regulatory index (PMRI), which allows for the prediction of the response to immunotherapy and the selection of personalized treatment. Multi-omics also allows for the understanding of molecular mechanisms of cancer, including the regulation of PD-L1 by signaling pathways and epigenetic modifications, which opens the way to new targeted therapies, e.g., using valrubicin or cobicistat. The integration of different data layers supports more accurate classification of tumors and real-time monitoring of treatment, improving patient prognosis. Thus, multi-omics becomes a key tool in the personalization of BC therapy [113].
Artificial intelligence (AI) plays a key role in BC treatment by using advanced machine learning algorithms to analyze molecular and clinical data. The AIGS (Artificial Intelligence-Derived Gene Signature) consensus gene signature (AIGS) was developed using 10 machine learning algorithms and 76 models that accurately predicted prognosis, relapse, and response to immunotherapy and chemotherapy in eight independent patient cohorts. AIGS proved to be more effective and stable compared to traditional clinical features and other published models. Patients with low AIGS scores responded better to immunotherapy, while patients with high AIGS scores could be candidates for new molecular therapies. AI multi-omics analysis also identified gene mutations and copy number changes associated with AIGS, contributing to a better understanding of tumor biology and further development of precision therapies [114].
3.4.3. Antibody–Drug Conjugates (ADCs)
ADC Mechanism of Action
Antibody–drug conjugates (ADCs) are a new therapeutic option that combines a tumor antigen-specific antibody with an anticancer drug via an appropriate linker [115]. The mechanism of action of ADCs begins with the recognition of the target antigen, which should be highly expressed only in tumor cells, minimizing toxicity in normal tissues [116]. The ADC–antigen complex is then internalized by the tumor cell via endocytosis [117].
Inside the cell, in the lysosomal environment characterized by low pH and the presence of proteases, the linker is cleaved. Cleavable linkers, such as those unstable at low pH, release the cytotoxic drug under appropriate conditions, allowing its activity. In contrast, non-cleavable linkers require lysosomal degradation to release their cargo [116].
The released cytotoxic drug exerts its antitumor effects through various mechanisms. For example, auristatins block tubulin assembly, causing cell cycle arrest in the G2/M phase. Maytansinoids, such as trastuzumab emtansine (T-DM1), also act by disrupting tubulin function. DNA-damaging agents, such as calicheamicin and duocarmycin, bind to the minor groove of DNA, leading to the disruption of replication and transcription. Modern ADCs use human monoclonal antibodies, which minimize immune responses, as well as more advanced linkers and highly potent cytotoxic drugs [118]. As a result, ADCs have become a promising tool in cancer treatment, offering new therapeutic options, especially in cases where traditional methods have failed [115].
Examples of ADC Use in Bladder Cancer
Enfortumab vedotin (EV) is an innovative antibody–drug conjugate (ADC) that consists of an antibody targeting Nectin-4 and a microtubule inhibitor. It is the first ADC approved by the FDA for the treatment of patients with advanced urothelial cancer (mUC), based on the results of a phase II clinical trial [119]. Nectin-4, a type 1 transmembrane protein, is a member of the immunoglobulin-related adhesion molecule family, which plays a key role in cell–cell adhesion processes [120]. Nectin-4 is exceptionally highly expressed in urothelial cancers, distinguishing it from other cancers and healthy tissues, while contributing to cancer cell growth and proliferation. Enfortumab vedotin is designed to bind to Nectin-4 with exceptionally high affinity. Once bound, the ADC is internalized by the tumor cells and the cytotoxic payload, monomethyl auristatin E (MMAE), is released. MMAE acts as a microtubule inhibitor, disrupting their function, leading to the inhibition of cell division and ultimately to tumor cell death [121]. On 18 December 2019, the FDA granted accelerated approval for enfortumab vedotin-ejfv (EV, trade name: PADCEV) for the treatment of patients with locally advanced or metastatic urothelial cancer who have previously received a PD-1 or PD-L1 inhibitor and platinum-based chemotherapy. The decision was based on the results of the EV-201 study, which showed a 44% response rate at a dose of 1.25 mg/kg in 28-day cycles, with a median duration of response of 7.6 months. The most commonly reported grade 3–4 adverse events included fatigue, peripheral neuropathy, and rash, and 73% of patients experienced high-grade adverse events. EV is an antibody–drug conjugate (ADC) targeting Nectin-4. It uses an antibody to transport the toxic compound MMAE into Nectin-4-expressing cancer cells, causing them to die. Importantly, the FDA does not recommend EV in patients with severe hepatic impairment. Preliminary studies have shown that EV has significant efficacy and an acceptable risk profile [122].
It is worth noting that on 15 December 2023, the FDA granted traditional approval for the combination of enfortumab vedotin-ejfv (EV) in combination with pembrolizumab (Pembro) for the treatment of locally advanced or metastatic urothelial cancer (la/mUC). The decision was based on the results of the EV-302/KEYNOTE-A39 trial, which compared the efficacy and safety of EV + Pembro with cisplatin or carboplatin plus gemcitabine (Plat + Gem) in 886 patients with previously untreated la/mUC. The trial results showed a significant advantage of EV + Pembro over Plat + Gem in terms of OS and PFS. The median PFS was 12.5 months for EV + Pembro versus 6.3 months for Plat + Gem (HR = 0.450; p < 0.0001). The median OS was also significantly longer for EV + Pembro at 31.5 months versus 16.1 months for Plat + Gem (HR = 0.468; p < 0.0001). The safety profile of EV + Pembro was consistent with previous observations from the EV-103/KEYNOTE-869 study, which evaluated the combination in cisplatin-ineligible patients with la/mUC. Traditional approval was based on clear PFS and OS benefits and an acceptable safety profile of EV + Pembro, which represents a new option for patients with advanced urothelial cancer [123].
Sacituzumab govitecan (SG) was an innovative ADC therapy directed against the TROP2 antigen, which is highly expressed in many epithelial malignancies, including urothelial carcinoma (UC) [124]. SG combines the antibody with SN-38, an active metabolite of irinotecan, which acts as a potent cytotoxic drug [125]. In the TROPHY-U-01 study, SG achieved an objective response rate (ORR) of 27% and a median progression-free survival (PFS) of 5.4 months, with a median overall survival (OS) of 10.5 months. The most common adverse events included neutropenia, leukopenia, and anemia, with an acceptable toxicity profile [126]. The TROPiCS-04 trial evaluated the efficacy of sacituzumab govitecan (SG) in patients with advanced urothelial carcinoma after failure of platinum-based chemotherapy and immune checkpoint inhibitor therapy. In this randomized phase III study, SG was compared with the physician’s choice of chemotherapy (TPC: paclitaxel, docetaxel, or vinflunine). SG demonstrated a higher objective response rate (ORR: 23% vs. 14%); it did not result in a significant improvement in overall survival (OS: 10.3 vs. 9.0 months; p = 0.087) or progression-free survival (PFS: 4.2 vs. 3.6 months). Additionally, there was a higher incidence of severe adverse events, particularly neutropenia and fatal infections, especially among patients who did not receive G-CSF prophylaxis. Due to the lack of therapeutic superiority and the unfavorable safety profile, sacituzumab govitecan was withdrawn from use in the treatment of bladder cancer [127,128].
The CheckMate 901 trial was a phase III, randomized, open-label study evaluating the addition of nivolumab to standard cisplatin–gemcitabine chemotherapy in the first-line treatment of patients with unresectable or metastatic urothelial carcinoma who were eligible for cisplatin. The combination significantly improved overall survival compared to chemotherapy alone (median OS: 21.7 vs. 18.9 months; HR 0.75; p = 0.017) and yielded higher overall (58% vs. 43%) and complete response rates (22% vs. 12%). While antibody–drug conjugates (ADCs), such as enfortumab vedotin, have shown even more pronounced efficacy in other studies, CheckMate 901 remains a relevant option, particularly in settings where access to ADCs is limited or cost-prohibitive. The manageable toxicity profile and fixed treatment duration of the chemoimmunotherapy regimen further support its clinical utility in a globally diverse patient population [129].
Trastuzumab emtansine (T-DM1) is an advanced ADC therapy that combines the HER2-targeting antibody trastuzumab with emtansine (DM1), a potent microtubule inhibitor. The overexpression of HER2, usually resulting from gene amplification, is an important therapeutic target in urothelial cancer (UC), particularly because it is low in normal urothelium and increases with disease progression [130,131]. In preclinical studies, T-DM1 has shown superior efficacy in inhibiting the growth of UC cells with high HER2 expression compared with trastuzumab alone [132]. Two phase II clinical trials (NCT02999672, NCT02675829) are currently evaluating the efficacy of T-DM1 in patients with HER2-positive UC. In one study, T-DM1 doses ranged from 2.4 mg/kg every week to 3.6 mg/kg every three weeks, with treatment continuing until disease progression or toxicity. Although data in UC are limited, these studies are designed to confirm the potential of T-DM1 in treating UC, based on its promising results in other HER2-positive tumors [114]. Vicinium (Oportuzumab monatox, OM) is a recombinant fusion protein that combines a humanized single-chain antibody against EpCAM with Pseudomonas exotoxin A. EpCAM, highly expressed in epithelial tumors, including urothelial carcinoma (UC), allows Vicinium to block protein synthesis and induce tumor cell death [133,134]. In phase I studies, Vicinium demonstrated good tolerability and antitumor activity, warranting further study [135]. In phase II studies, 46 patients with BCG-refractory non-muscle-muscle-invasive bladder cancer (NMIBC) had a complete response of 39–41% at 3 months, and 16% remained disease-free [136]. These studies confirmed the efficacy and safety of Vicinium in second-line treatment of NMIBC, with mild side effects, mainly bladder irritation. Despite promising results, Vicinium was not approved by the FDA due to insufficient data. The phase III VISTA study (NCT02449239) investigated efficacy in BCG-refractory NMIBC, achieving a 3-month response rate of 40% and a median duration of response of 9.4 months. The 2-year OS was 96% [95% CI] for the study group. Combination therapy studies, such as Vicinium with durvalumab (NCT03258593), are also ongoing to assess the safety and efficacy of therapy in UC without muscle invasion [118].
Tisotumab vedotin (TV) is the first ADC directed against tissue factor (TF), expressed on the surface of cancer cells [137]. TV consists of a human monoclonal antibody specific for TF linked to the microtubule inhibitor MMAE via a protease-cleavable valine-citrulline linker. TF, a transmembrane glycoprotein, plays a key role in tumor growth, metastasis, and angiogenesis, and its expression in urothelial cancer (UC) reaches 77.6%. High levels of TF are associated with disease-specific survival, risk of progression, and efficacy of adjuvant chemotherapy [138]. In 2019, de Bono et al. conducted a phase I/II clinical trial involving 174 patients, including 17 with bladder cancer. The safety and tolerability of TV were assessed in the dose escalation phase (0.3 mg/kg and 1.5 mg/kg) and dose expansion phase (2.0 mg/kg). Observations included the frequency of adverse events, including serious and infusion-related adverse events. In the dose expansion phase, 26.7% of bladder cancer patients achieved an objective response to treatment according to RECIST 1.1 criteria. Although the study was not focused on the assessment of the therapeutic effect, TV showed promising antitumor activity in a broad spectrum of solid tumors, including UC, which justifies further clinical studies [139].
3.4.4. Gene Therapies
Examples of Innovative Gene Therapies
Nadofaragene firadenovec-vncg (Adstiladrin) is a novel, non-replicating adenoviral vector-based gene therapy for the treatment of adult patients with high-risk NMIBC who do not respond to BCG. It is used in cases of CIS with or without papillary tumors. The therapy works by delivering the gene encoding interferon alpha-2b (IFNα-2b) directly to bladder epithelial cells, resulting in the secretion of IFNα-2b. The therapeutic effects include cytotoxic, antiangiogenic, and immunomodulatory effects, which enhance the immune response and increase the immunogenicity of tumor cells. Phase III clinical trials have shown that more than half of patients achieved a complete response after three months of therapy, and efficacy was maintained in some of them for a year or more. The safety profile of the drug is also extremely favorable, with few adverse events, mainly local and mild, and a low risk of systemic toxicity. The introduction of this therapy gives patients the opportunity to avoid radical cystectomy, which contributes to the improvement of the quality of life, while maintaining full bladder function [140,141]. In the study presented by Chinese researchers, a novel approach to BC therapy was presented by creating artificial circular RNA (acircRNA), which uses aptamers to specifically silence signaling pathways associated with oncogenic transcription factors, such as β-catenin and NF-κB—transcription factors crucial for the development and progression of BC. Unlike traditional RNA-based methods, circular RNA is more stable and effective in inhibiting carcinogens. In the study, acircRNA consisting of three functional units (aptamers) was created, which specifically bind and inhibit β-catenin and NF-κB. The effectiveness of acircRNA was tested on bladder cancer cell lines (T24 and 5637). The results showed that acircRNA effectively reduced the expression of oncogenic genes such as c-myc and cyclin D1 (related to β-catenin) and Bcl-XL and TRAF1 (related to NF-κB). In vitro studies showed that acircRNA reduced cancer cell proliferation, increased apoptosis, and inhibited cancer cell migration. To deliver acircRNA to target cells, the researchers used exosomes with the fusion protein CD63-HuR, which facilitated the loading of acircRNA into exosomes and their delivery to cancer cells. Exosomes containing acircRNA were more effective in inhibiting β-catenin and NF-κB than the traditional CRISPR-dCas9-KRAB system, making them a potentially more effective therapeutic tool. The findings suggest that acircRNA may be a promising, innovative treatment strategy for bladder cancer [142].
Polyethyleneimine (PEI) is a promising cationic polymer used in the delivery of nucleic acids to cancer cells, making it an important tool in the development of gene therapy for the treatment of bladder cancer. Due to its ability to form polyplex complexes, PEI facilitates the transport of genetic material across cell membranes, offering a potential alternative to viral therapies. In the treatment of cancers such as BC, PEI has demonstrated the ability to effectively deliver therapeutic genes that can induce cytotoxic responses, e.g., by expressing tumor suppressor genes (e.g., p53) or antiangiogenic genes (e.g., sFLT-1) that inhibit tumor growth. However, PEI is associated with certain clinical limitations, such as toxicity resulting from its high cationic charge and limited biodegradability. In order to improve biocompatibility and increase clinical efficacy, innovative formulations of PEI are being developed, including combinations with biodegradable links or modifications to the polymer structure. Studies of PEI delivery by direct injection into the bladder tumor suggest that local administration may reduce systemic toxicity while increasing antitumor efficacy. With these advances, PEI has the potential to become a versatile tool in gene therapy for bladder cancer, with the potential to significantly improve treatment outcomes while reducing adverse events [143]. CG0070 is an oncolytic adenovirus designed to selectively replicate and kill Rb pathway-defective tumor cells (retinoblastoma). It acts by directly killing tumor cells and stimulating the immune system. It has been used intravesically to treat non-muscle-invasive bladder cancer (NMIBC), particularly in patients who are unresponsive to Bacillus Calmette–Guérin (BCG). In the BOND003 (phase III) study, CG0070 achieved an overall response rate of 76%, with 74% of patients maintaining a response for at least 6 months. The therapy was well tolerated, with mild adverse events such as bladder spasms (20%) and urinary frequency (16%). When combined with pembrolizumab in the CORE001 (phase II) trial, the overall response rate was 85%. CG0070 offers an effective alternative for patients who do not respond to standard therapies, with low toxicity and bladder-sparing potential. Due to promising results, it has been granted Breakthrough Therapy Designation by the FDA [144]. EG-70 (detalimogen voraplasmid) is an investigational, nonviral gene therapy designed to locally stimulate an antitumor immune response in high-risk non-muscle-invasive bladder cancer (NMIBC) that is unresponsive to Bacillus Calmette–Guérin (BCG). The therapy aims to provide durable efficacy while limiting the risk of systemic toxicity resulting from immunostimulation. In preclinical studies, EG-70 has demonstrated the ability to significantly remodel the tumor microenvironment from an immunosuppressive to a proinflammatory one. In a murine bladder cancer model, EG-70 administration reduced myeloid cell counts and IL-4 levels, while increasing NK and T cell counts and proinflammatory cytokines. This led to effective tumor clearance and improved survival, with durable protection against tumor recurrence. T cells played a key role in the mechanism of action. In the phase 1/2 LEGEND clinical trial (NCT04752722), EG-70 was administered intravesically to patients with high-risk NMIBC and carcinoma in situ (CIS). The therapy was well tolerated at all dose levels, with a complete response rate of 73%. These results support the efficacy of EG-70 in stimulating a local immune response, enabling effective treatment of NMIBC with minimal side effects. EG-70 is a promising treatment for bladder cancer that is unresponsive to standard therapies [145].
BC-819 is an innovative gene therapy based on a double-stranded DNA plasmid that contains the A subunit of diphtheria toxin (dtA) under the control of the H19 promoter. The mechanism of action of BC-819 is based on the selective activation of dtA toxin synthesis in cancer cells that express high H19 gene activity. The H19 gene, a key factor in this process, is highly active in many human cancers, including bladder cancer, while its expression is virtually undetectable in healthy tissues. As a result, BC-819 targets cancer cells, selectively inhibiting protein synthesis and causing their death, while minimizing the impact on healthy tissues. The safety and efficacy of BC-819 were assessed in a phase I/II study in patients with non-muscle-invasive bladder cancer (NMIBC) who were unresponsive to standard BCG therapy. The results showed promising results: 22% of patients (4 out of 18) showed tumor marker ablation, and five out of nine patients who received a month of maintenance therapy had a DFS (disease-free survival) exceeding 35 weeks. Importantly, no serious treatment-related adverse events (DLT) were reported. Although the results of the initial studies are encouraging, further studies are needed to confirm the efficacy and safety of BC-819 in this group of patients and to introduce the therapy as a potential treatment option for H19-expressing NMIBC [146].
Potential Limitations and Side Effects of Gene Therapies
We still have to deal with many limitations or side effects in the aspect of gene therapies. In the case of acircRNA, in vivo studies are necessary to confirm the efficacy also in this field [142]. In turn, when it comes to PEI, a major obstacle is toxicity resulting from the high cationic charge and limited biodegradability, which may play a major role in the era of climate change [144]. In the case of CG0070, further studies are needed to investigate the long-term efficacy of this therapy [144]. EG-70 faces a similar problem as, in this case, it is also necessary to collect data that will include aspects of long-term efficacy [145]. The least studied therapy of all mentioned is undoubtedly BC-819, which requires further work in terms of both confirmation of efficacy and safety [146].
3.4.5. Photodynamic Therapy
Photodynamic therapy (PDT) is a promising treatment method for BC, based on the use of a photosensitizer that selectively accumulates in cancer cells. Activated by light of an appropriate wavelength, the photosensitizer generates reactive oxygen species (ROS), which leads to cancer cell damage and death. PDT has the potential to be used in neoadjuvant and adjuvant treatment of bladder cancer, potentially reducing recurrence and increasing the effectiveness of local control. Photosensitizers used in PDT, such as 5-ALA, hypericin, and chlorophyllin, differ in their mechanism of action and selectivity for cancer cells, which allows for more precise treatment. Animal models and in vitro studies indicate that combining PDT with other therapies, such as intravesical chemotherapy or targeted therapy, can improve treatment outcomes. Clinical studies suggest that PDT may be an effective option for treating recurrent BC, but further technological refinement is needed to reduce side effects and optimize therapeutic regimens for wider clinical use [147]. Particularly great interest is observed in the area of photodynamic diagnostics (PDD) and PDT with 5-aminolevulinic acid (5-ALA). These are advanced methods of BC treatment and detection, especially useful for detecting superficial and flat tumors such as CIS, which are difficult to see with conventional cystoscopy. In PDT, 5-ALA combined with an appropriate wavelength of light generates ROS, which destroys tumor cells by damaging mitochondria and inducing apoptosis. For better light penetration, red light is most often used in PDT. This procedure is minimally invasive and can be performed repeatedly without damaging the bladder, making it a safe adjunct to BC treatment, especially in patients at high risk of relapse. Clinical use of 5-ALA-PDT may replace aggressive treatments such as chemotherapy or BCG therapy, which are associated with a higher risk of complications. 5-ALA-PDT is able to effectively control CIS and other flat lesions without causing systemic side effects. Studies are ongoing to improve the formulation of 5-ALA, which may further increase its efficacy. The future of 5-ALA-PDT in NMIBC therapy seems promising, offering a safer and more effective alternative in the diagnosis, treatment, and monitoring of bladder cancer [148].
3.5. Nanomedicine
3.5.1. Nanomedicine in Photodynamic Therapy
Nanotechnology-assisted photodynamic therapy (PDT) is a promising method for treating bladder cancer, combining the use of a photosensitizer, light of an appropriate wavelength, and oxygen to generate reactive oxygen species that destroy cancer cells. The innovative use of nanoparticles such as MnO2 significantly increases the efficacy of this therapy, overcoming the problem of tumor hypoxia by providing additional oxygen to their environment. Nanotechnology also allows for precise delivery of photosensitizers to tumor tissue, minimizing damage to healthy tissues and reducing systemic toxicity thanks to the controlled release of active substances. Moreover, the synergistic action of ROS supported by advanced light targeting systems improves the therapeutic efficacy of PDT, making it more effective compared to traditional treatment methods [149].
Numerous studies have been conducted to overcome the limitations of PDT in the treatment of BC. In one such study, Yan et al. created nanoparticles containing 5-ALA and evaluated their phototoxic potential against T24 bladder cancer cells in laboratory studies. The nanoparticle base was a copolymer of caprolactone, polyethylene glycol, and lactide, prepared by ring-opening copolymerization. The process of loading 5-aminolevulinic acid into the nanoparticles was carried out using the nanoprecipitation technique. MTT cytotoxicity assay showed that nanoparticles with 5-ALA had a higher level of toxicity towards cancer cells compared to free 5-ALA alone. Moreover, the inhibition effect of cancer cell growth was more than twice as high using 5-ALA nanoformulation compared to the drug alone. These results suggest that the modification of 5-aminolevulinic acid using nanotechnology enhances the efficacy of PDT [150]. Current photosensitizers have limitations, such as low selectivity, poor absorption bandwidth, limited bioavailability, and insufficient efficiency. They also lack the ability to co-deliver chemotherapeutic drugs and induce photothermal effects. In response to these challenges, Lin et al. developed a multifunctional nanoporphyrin (PNP) platform encapsulated with the ligand PLZ4, which enables simultaneous photodynamic, photothermal, and targeted chemotherapy diagnostics and therapy. PLZ4 specifically binds to integrin αvβ3, which is expressed on invasive transitional cell bladder cancer cells. The PNP platform with doxorubicin (DOX) showed high cytotoxicity against bladder cancer cells after irradiation, increasing cell damage such as edema and membrane degradation. In mouse models of bladder cancer, the intravesical application of PNP-DOX effectively delivered the drug to cancer cells and inhibited tumor growth, with minimal side effects. The study showed that PNP therapy was more effective than 5-ALA alone, offering better selectivity, slower drug release, and longer systemic duration of action [151,152]. A study published in September 2024 developed an innovative approach to PDT of bladder cancer using X-ray activated nanotransducers that combines diagnostics and therapy. The main technology is based on lanthanide nanomaterials that emit light simultaneously in the visible and near-infrared (NIR-II) range, which allows real-time monitoring and imaging. Nanotransducers, enriched with a peptide targeting cancer cells, were administered to the bladder of mice with cancer. X-ray radiation excites photosensitizers in the nanomaterials, which generates ROS that destroy cancer cells and stimulates an immune response. Studies have shown that the use of fractionated PDT with nanotransducers leads to the inhibition of tumor growth, reduced recurrence, and improved survival rates. With NIR-II imaging, it is possible to track therapy and adjust radiation doses in response to tumor status. This nanotechnology-based strategy offers a promising, non-invasive solution that may support the diagnosis and monitoring of bladder cancer, while eliminating the need for biopsy and increasing treatment efficacy [153].
3.5.2. Nanomedicine in Gene Therapies
In bladder cancer therapy, one approach to reducing gene expression is the use of RNA interference (RNAi), where siRNA and shRNA have been particularly effective in limiting cancer cell proliferation and invasion and reversing their drug resistance. In response to these challenges [154]. Liang et al. in 2021 [155] attempted to design a chitosan–hyaluronic acid dialdehyde nanoparticle (NP) (CS-HAD NP) as a carrier for siRNA targeting the BCL-2 gene, which is a gene responsible for tumor development. Hyaluronic acid (HAD) was prepared using a mixture of water and ethanol and then conjugated with chitosan amino groups to form nanoparticles of 100–120 nm in size. These CS-HAD NPs are capable of selectively transporting siRNA to cancer cells overexpressing the CD44 protein. The siRNA was placed in the nanoparticle core with an efficiency of 95%, which ensures its delivery efficiency. Studies conducted both at the cellular level (in vitro) and in mice (in vivo) showed that siRNA@CS-HAD NPs significantly reduced the viability of T24 cancer cells and increased the levels of cleaved PARP, suggesting that the system effectively silences cancer genes. The nanoparticles also showed compatibility with blood, without affecting red blood cells. When administered to mice with T24 tumors, they inhibited their growth significantly more than the use of naked siRNA or nanoparticles without hyaluronic acid. Thanks to this innovative approach, the siRNA@CS-HAD NP system has the potential to treat breast cancer with high expression of the CD44 protein [155]. ncRNAs, or non-coding RNAs, play important regulatory roles in organisms, controlling processes such as cell differentiation, proliferation, and migration. MicroRNAs (miRs), which are short ncRNA segments, silence genes by binding to specific regions of mRNA (3′-UTR), which results in the inhibition of their translation. There are two main groups of miRs: tumor suppressors (inhibiting tumor development) and oncogenic miRs, so-called oncomiRs, promoting its growth. The abnormal expression of miRs is associated with various solid tumors. For example, miR-34a acts as a tumor suppressor, limiting the proliferation, migration, and metastasis of cancer cells. It has been shown that miR-34a reduces the expression of CD44 on the surface of cancer cells and increases their susceptibility to drugs. Shahidi et al. created silica nanoparticles (c(RGDfK)-MSN NPs) that can deliver miR-34a and siRNA (siPD-L1) to bladder cancer cells. PD-L1 is a protein that helps cancer avoid T cell attack. The use of a PD-1/PD-L1 inhibitor increases the effectiveness of treatment, and the delivery of miR-34a and siPD-L1 to cells reduces the expression of PD-L1 and CD44, which results in higher apoptosis of cancer cells. In vitro and in vivo studies have shown that c(RGDfK)-MSN NPs were stable in blood and effectively delivered cargo to cells. In an acidic environment (pH 5.4), miR-34a and siPD-L1 were released, and the nanoparticles showed high selectivity for T24 cancer cells, reducing their migration and invasion by 55% and 45%, respectively. Tests on mice have shown that these nanoparticles effectively inhibit tumor growth, making them a promising tool in cancer therapy [154,156]. KDM6A is a key regulator of bladder cancer progression, and its mutation promotes immune escape of tumor cells and reduces immune cell infiltration. KDM6A promotes ARHGDIB expression, which inhibits Rac1 and limits tumor metastasis. The described study involved the delivery of KDM6A-mRNA using mucoadhesive nanostructures, which increased the exposure of mRNA to the tumor site and prolonged its delivery. Higher expression of KDM6A significantly reduced metastasis, and nanostructures with mRNA showed synergistic effects with other clinically used drugs [157,158,159].
3.5.3. Nanomedicine in Immunotherapy
Terán-Navarro and colleagues created the GNP-LLO91–99 nano-vaccine by combining gold glycoside (GNP) molecules with peptides 91–99 of the bacterial toxin listeriolysin O (LLO). The nano-vaccine effectively counteracted the immunosuppression characteristic of bladder cancer by stimulating the immune system. It increased the number of cytotoxic T lymphocytes and dendritic cells (DCs) present in the tumor, while reducing the number of regulatory T cells (T reg) and myeloid-derived suppressor cells (MDSC), which are responsible for inhibiting the immune response [160]. The main advantage of nanoparticles is their extremely small size, which, with their outstanding transport efficiency, allows for precise targeting of selected sites or cells, enhancing the immune response and limiting adverse effects (irAEs) [161]. It is also important to note that nanoparticles can be targeted not only to cancer cells, but also to matrix metalloproteinases (MMPs) or lysoxidase (LOX) present in the tumor microenvironment (TME), which allows for dual recognition. In addition, nanoparticles can induce immunogenic cell death (ICD) and trigger threat-associated molecular patterns (DAMPs), which support the maturation of dendritic cells (DCs) and enable the conversion of M2 macrophages to M1 macrophages in the TME. Combining nanoparticles with immunotherapeutic drugs allows for faster delivery to tumors and simultaneous acceleration of their elimination from the bloodstream, which reduces systemic exposure while maintaining adequate stimulation in the TME [162]. BCG nanoformulations, or Bacillus Calmette–Guérin vaccines on a nanoscale, offer a modern approach to bladder cancer immunotherapy. By using lipid, polymer and magnetic nanocarriers, nano-BCG enables precise delivery of the vaccine to cancer cells, increasing its effectiveness and minimizing side effects. These advanced carriers improve bioavailability and allow for prolonged release of the substance, which enhances the immune response. When combined with chemotherapeutics, nano-BCG shows synergistic effects—not only intensifying the destruction of cancer cells but also reducing the systemic toxicity of the therapy. Although the research remains at the experimental stage, nano-BCG has enormous clinical potential, offering more effective and more tolerable treatment for bladder cancer [163]. In 2021, Zhou et al. designed a novel system for the simultaneous delivery of different drugs to cancer tissues in breast cancer therapy. The main goal of this approach was to weaken the influence of the tumor microenvironment, which inhibits the activity of immune system cells, and to enhance the effect of checkpoint inhibitors. To this end, scientists created macrophage-derived exosome-mimicking nanovesicles (EMVs) that precisely deliver a CD73 inhibitor (AB680) and a monoclonal antibody (aPDL1). Both in vitro and in vivo studies confirmed the high stability and biological safety of this therapy, as well as the effective targeting of delivery to breast cancer cells. The blockade of CD73 reduced the production of extracellular adenosine, while the inhibition of PD-L1 expression prevented cancer cells from evading the immune response. The combined therapy increased the activation and infiltration of cytotoxic T lymphocytes, resulting in the inhibition of tumor growth and prolonged survival in mouse models [164]. In 2024, Chinese scientists developed a novel theranostic nanotransformer (CTMF NP) designed specifically for bladder cancer therapy. Due to the dynamic metal–polyphenol coating activated by the tumor microenvironment (TME), this nanotransformer exhibits high bioadhesiveness, which enables precise, local, and long-lasting anticancer effects. This nanotransformer uses zero-background 19 F-MRI technology and photoacoustic imaging, which enables precise monitoring and control of the therapy. Additionally, the coating enhances oxidative stress in cancer cells by depleting glutathione (GSH) and generating ROS, which leads to structural damage and mitochondrial dysfunction of cancer cells. This technology also enables the induction of ICD, which increases the body’s immune response. CTMF NP offers a promising strategy for synergistic anticancer therapy by combining photothermal, chemical, and immunological effects in one system [165].
As a new approach to bladder cancer treatment, urease-powered nanobots have been developed, which demonstrate greater therapeutic efficacy compared to traditional intravesical drug delivery methods. Due to their self-propulsion, these nanobots move better in urine, which facilitates their diffusion and increases their accumulation at the tumor site. In a mouse model, it was shown that silica-based nanobots, radioactively labeled (131 I), effectively reached the tumor, which enabled precise radionuclide therapy (RNT) and reduced tumor size by about 90%. The nanobots showed the ability to penetrate the tumor and to be retained in the tumor tissue, as demonstrated by PET-CT imaging and scattered light microscopy. It was also found that nanobots, acting at low doses, achieve high therapeutic efficacy, making them a promising tool in the treatment of bladder cancer in clinical settings [166].
3.5.4. Nanomedicine in Targeted Therapy
iRNA delivery systems such as lipid and viral carriers are widely used, but their limitation is the frequent cytotoxicity in humans. In response to this problem, Chen et al. designed an innovative system based on Mg(II)-catechin nanogenes, which enables precise delivery of EIF5A2 siRNA. In the conducted studies, both on T24 cell lines and in xenogeneic models, the Mg(II)-catechin/siEIF5A2 complex significantly inhibited the growth of bladder cancer. These self-assembled nanoparticles, distinguished by high biocompatibility, showed selective activity against bladder cancer cells and strong synergistic anticancer properties. The results of the study introduce a novel way of designing nanoparticles, using natural anticancer substances to increase the effectiveness of therapy [167]. Maria et al. used a patented poly(beta-aminoester) polymer as a siRNA carrier and tested it on two bladder cancer cell lines. This nanoparticle contained a C32 pBAE backbone, in which the final oligopeptides were 50% arginine and 50% lysine, and a bromelain protein shell, which enabled efficient crossing of mucus barriers. After the application of siRNA encapsulated in these nanoparticles, a significant decrease in the viability of bladder cancer cells was observed. However, the efficacy of paclitaxel (PTX) was significantly higher than that of siRNA NPs. Additionally, the simultaneous use of both anticancer drugs did not show a synergistic effect, suggesting that these siRNA NPs are not able to improve the resistance of bladder cancer cells to PTX [168]. AIB1 was initially identified as a gene overexpressed in many cancers. Later studies showed its expression in urothelial bladder cancers, making it a new, independent prognostic marker for patient survival. Wei et al. developed ACC/CaIP6 nanoparticles (NPACC/CaI--P6) to deliver siRNA directed against AIB1. The new nanoparticle was characterized by the absence of cytotoxicity. In both in vitro and in vivo studies, the ACC/CaIP6/siRNA complex effectively inhibited cell proliferation, induced apoptosis, and downregulated the expression of PI3K/Akt pathway [169]. Table 2 below presents a comparison between innovative therapies and existing standard treatments (e.g., chemotherapy, immunotherapy, targeted therapy), clarifying their impact on clinical practice and patient outcomes.
Table 2.
Summary of differences between recent methodologies in bladder cancer.
3.6. Parameters or Indices That May Impact Prognosis and Patient Eligibility for Various Treatment Options
A growing body of evidence emphasizes the importance of individual patient characteristics—beyond tumor type and stage—in determining prognosis and selecting optimal treatment strategies for bladder cancer (BC). A recent systematic review and meta-analysis assessed risk factors for chronic kidney disease (CKD) in patients undergoing radical cystectomy (RC) and their impact on survival outcomes. The analysis identified several clinical parameters significantly associated with long-term decline in renal function following RC, including advanced age, low baseline renal function, high Charlson Comorbidity Index (CCI), diabetes, hypertension, postoperative hydronephrosis, ureteroenteric and bowel strictures, and locally advanced disease. Notably, preoperative hydronephrosis, perioperative chemotherapy, and type of urinary diversion did not significantly affect renal function. Moreover, a higher stage of CKD was independently associated with worse metastasis-free survival, cancer-specific survival, and overall survival after RC. These findings highlight that renal function, comorbidities, and overall health status are crucial factors in both risk stratification and therapeutic decision-making in BC patients. Given the high costs and strict qualification criteria of modern therapies, including immunotherapy and targeted treatments, integrating these clinical parameters into patient assessment is essential for tailoring treatment and optimizing outcomes [170].
The study published in 2023 emphasizes the prognostic value of functional status, as assessed by the Barthel Index (BI), in patients undergoing radical cystectomy (RC) for bladder cancer (BCa). Patients with impaired ability to perform activities of daily living (BI ≤ 90) demonstrated significantly worse oncologic outcomes—including higher rates of disease recurrence, cancer-specific mortality, and overall mortality—compared to those with higher functional independence (BI 95–100). Furthermore, individuals with lower BI were less likely to receive intravesical adjuvant therapy and more likely to undergo simpler urinary diversion procedures. Given that many modern and costly treatment options for BCa have strict eligibility criteria, these findings highlight that treatment decisions should not be based solely on tumor aggressiveness or histological type. The overall health status and comorbidities of the patient play a critical role in determining therapeutic suitability. Incorporating functional assessment tools such as the BI into clinical practice may improve patient risk stratification and guide more personalized treatment planning [171].
The study published by R Ben-David assessed the prognostic value of circulating tumor DNA (ctDNA) in patients with bladder cancer (BC) undergoing radical cystectomy (RC). Detectable ctDNA before surgery was associated with a higher risk of lymph node involvement, locally advanced disease, and significantly worse recurrence-free survival (RFS), regardless of clinical stage or use of neoadjuvant therapy. Furthermore, the presence of ctDNA in the minimal residual disease window after RC emerged as a strong predictor of disease recurrence. These findings highlight the growing importance of precise biological markers in selecting candidates for complex and high-cost therapies such as neoadjuvant, adjuvant, or immunotherapy. Given the resource-intensive nature of these treatments, decision-making should go beyond tumor characteristics like type or aggressiveness. Instead, a comprehensive assessment including the patient’s general condition, comorbidities, and molecular indicators such as ctDNA status is essential. Incorporating such parameters into clinical practice may improve treatment stratification and enable more personalized, effective management of bladder cancer [172].
3.7. Limitations, Clinical Challenges, and Future Perspectives Regarding Innovative Therapies for BC Treatment
The systemic immune-inflammation index (SII) shows promise as a prognostic biomarker in BC, but its clinical application remains limited. Elevated preoperative SII is associated with more advanced disease and poorer survival outcomes; however, the lack of standardized cut-off values, potential influence of unrelated inflammatory conditions, and insufficient external validation restrict its current utility. In light of the high costs and strict eligibility criteria of innovative therapies, there is a growing need for reliable and accessible indicators to guide treatment selection. While SII alone may lack specificity, it could complement existing risk models and help identify high-risk patients more accurately—particularly those who may benefit from targeted therapies such as immune checkpoint inhibitors [173].
Although research into the urinary microbiome (urobiome) in BCa has identified potential diagnostic markers—particularly Porphyromonas and P. somerae in men over 50—the clinical application of these findings remains limited. Key challenges include the lack of standardized urine collection methods, low microbial biomass, and a high risk of contamination, all of which can compromise data reliability. Clinically, while the urobiome shows promise as a non-invasive biomarker for risk stratification, its utility has yet to be validated in large, independent cohorts. This is especially important given the strict eligibility criteria and high costs of advanced therapies like immunotherapy. Looking ahead, the urobiome may support personalized treatment strategies in BC by helping to identify high-risk patients or predict treatment response. However, its role is currently experimental and further research is essential before integration into routine clinical practice [174].
Modern therapies for bladder cancer—such as nanomedicine, immunotherapy, gene therapies—offer promising potential but still face significant limitations. Key challenges include tumor heterogeneity, treatment resistance, low drug bioavailability, and the lack of standardized diagnostic methods (e.g., in urobiome analysis, exosome profiling, and radiomics). Nanocarriers and RNA-based therapies require further optimization in terms of safety, stability, and selectivity. While immunotherapies are effective, they may provoke strong immune reactions. Physical approaches like hyperthermia remain limited to localized lesions. The development of personalized therapies based on molecular and imaging data also demands harmonized procedures and clinical validation. To integrate these innovative strategies into routine clinical practice, further research, larger patient cohorts, and effective combination with existing treatment protocols are essential [175].
4. Conclusions
Recent advancements in bladder cancer treatment have led to significant changes in therapeutic standards, particularly regarding targeted therapies and immunotherapy. The emergence of new agents such as nadofaragene firadenovec, nogapendekin alfa inbakicept, and both systemic and intravesical immunotherapies (e.g., pembrolizumab, durvalumab, nivolumab) has substantially expanded the range of treatment options, especially for patients unresponsive to conventional BCG therapy.
Current clinical data support the effectiveness of combination strategies such as chemoimmunotherapy (CheckMate 901), adjuvant immunotherapy (CheckMate 274, AMBASSADOR), and perioperative checkpoint inhibitor use (NIAGARA). Simultaneously, molecular research and the development of predictive biomarkers—including PD-L1 expression, FGFR3 mutations, and MSI-H/dMMR status—are enabling increasingly personalized treatment selection based on individual tumor characteristics.
Targeted therapies, such as FGFR inhibitors (erdafitinib, rogaratinib, pemigatinib), next-generation agents (e.g., CAR-T cells directed at SIA-CIgG and Nectin-4), and experimental applications of CRISPR/Cas9, represent a dynamic direction in oncological innovation.
Despite significant progress, numerous challenges remain, including therapy accessibility, treatment costs, immune-related adverse effects, and the need for further biomarker validation. Therefore, ongoing translational research and large-scale, randomized clinical trials are essential to solidify the role of these novel therapeutic approaches.
In light of current evidence, bladder cancer treatment is moving toward an increasingly individualized model, grounded in molecular diagnostics and the integration of targeted and immune-based therapies. This approach holds great promise for improving prognosis and quality of life for patients affected by this difficult-to-treat malignancy.
Author Contributions
Conceptualization, D.G., S.C., J.S., D.B.-A. and D.A.; methodology, D.G., S.C., J.S., D.B.-A. and D.A.; validation, D.G., S.C., J.S., D.B.-A. and D.A.; formal analysis, D.G., S.C., J.S., D.B.-A., D.A.; resources, D.G., S.C., J.S., D.B.-A. and D.A.; writing—original draft preparation, D.G., S.C., J.S., D.B.-A. and D.A.; writing—review and editing D.G., S.C., J.S., D.B.-A. and D.A.; visualization, D.G., S.C., J.S., D.B.-A. and D.A.; supervision, D.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Alouini, S. Risk Factors Associated with Urothelial Bladder Cancer. Int. J. Environ. Res. Public Health 2024, 21, 954. [Google Scholar] [CrossRef] [PubMed]
- International Agency for Research on Cancer. World Fact Sheet. GLOBOCAN. 2022. Available online: https://gco.iarc.who.int/media/globocan/factsheets/populations/900-world-fact-sheet.pdf (accessed on 6 February 2023).
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global Cancer Statistics 2022: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Ervik, M.; Lam, F.; Laversanne, M.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today; International Agency for Research on Cancer: Lyon, France, 2024; Available online: https://gco.iarc.who.int/today (accessed on 6 February 2023).
- Teoh, J.Y.; Huang, J.; Ko, W.Y.; Lok, V.; Choi, P.; Ng, C.F.; Sengupta, S.; Mostafid, H.; Kamat, A.M.; Black, P.C.; et al. Global Trends of Bladder Cancer Incidence and Mortality, and Their Associations with Tobacco Use and Gross Domestic Product Per Capita. Eur. Urol. 2020, 78, 893–906. [Google Scholar] [CrossRef] [PubMed]
- Silverman, D.T.; Koutros, S.; Figueroa, J.D.; Prokunina-Olsson, L.; Rothman, N. Bladder Cancer. In Schottenfeld and Fraumeni Cancer Epidemiology and Prevention, 4th ed.; Oxford University Press: New York, NY, USA, 2017; pp. 977–996. [Google Scholar]
- Babjuk, M.; Burger, M.; Zigeuner, R.; Shariat, S.F.; van Rhijn, B.W.; Compérat, E.; Sylvester, R.J.; Kaasinen, E.; Böhle, A.; Palou Redorta, J.; et al. EAU Guidelines on Non-Muscle-Invasive Urothelial Carcinoma of the Bladder: Update 2013. Eur. Urol. 2013, 64, 639–653. [Google Scholar] [CrossRef]
- Antoni, S.; Ferlay, J.; Soerjomataram, I.; Znaor, A.; Jemal, A.; Bray, F. Bladder Cancer Incidence and Mortality: A Global Overview and Recent Trends. Eur. Urol. 2017, 71, 96–108. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Hinotsu, S.; Akaza, H.; Miki, T.; Fujimoto, H.; Shinohara, N.; Kikuchi, E.; Mizutani, Y.; Koga, H.; Okajima, E.; Okuyama, A.; et al. Bladder Cancer Develops 6 Years Earlier in Current Smokers: Analysis of Bladder Cancer Registry Data Collected by the Cancer Registration Committee of the Japanese Urological Association. Int. J. Urol. 2009, 16, 64–69. [Google Scholar] [CrossRef]
- Linn, J.F.; Sesterhenn, I.; Mostofi, F.K.; Schoenberg, M. The Molecular Characteristics of Bladder Cancer in Young Patients. J. Urol. 1998, 159, 1493–1496. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer Statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef]
- Freedman, N.D.; Silverman, D.T.; Hollenbeck, A.R.; Schatzkin, A.; Abnet, C.C. Association between Smoking and Risk of Bladder Cancer among Men and Women. JAMA 2011, 306, 737–745. [Google Scholar] [CrossRef]
- Saginala, K.; Barsouk, A.; Aluru, J.S.; Rawla, P.; Padala, S.A.; Barsouk, A. Epidemiology of Bladder Cancer. Med. Sci. 2020, 8, 15. [Google Scholar] [CrossRef] [PubMed]
- Pollak, M. The Insulin and Insulin-Like Growth Factor Receptor Family in Neoplasia: An Update. Nat. Rev. Cancer 2012, 12, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.W.; Zhao, L.G.; Yang, Y.; Ma, X.; Wang, Y.Y.; Xiang, Y.B. Obesity and Risk of Bladder Cancer: A Dose-Response Meta-Analysis of 15 Cohort Studies. PLoS ONE 2015, 10, e0119313. [Google Scholar] [CrossRef] [PubMed]
- Parkin, D.M.; Hämmerl, L.; Ferlay, J.; Kantelhardt, E.J. Cancer in Africa 2018: The Role of Infections. Int. J. Cancer 2020, 146, 2089–2103. [Google Scholar] [CrossRef]
- Mostafa, M.H.; Sheweita, S.A.; O’Connor, P.J. Relationship between Schistosomiasis and Bladder Cancer. Clin. Microbiol. Rev. 1999, 12, 97–111. [Google Scholar] [CrossRef]
- Rambau, P.F.; Chalya, P.L.; Jackson, K. Schistosomiasis and Urinary Bladder Cancer in North Western Tanzania: A Retrospective Review of 185 Patients. Infect. Agents Cancer 2013, 8, 19. [Google Scholar] [CrossRef]
- Nassour, A.-J.; Jain, A.; Hui, N.; Siopis, G.; Symons, J.; Woo, H. Relative Risk of Bladder and Kidney Cancer in Lynch Syndrome: Systematic Review and Meta-Analysis. Cancers 2023, 15, 506. [Google Scholar] [CrossRef]
- Złowocka-Perłowska, E.; Tołoczko-Grabarek, A.; Narod, S.A.; Lubiński, J. Germline BRCA1 and BRCA2 Mutations and the Risk of Bladder or Kidney Cancer in Poland. Hered. Cancer Clin. Pract. 2022, 20, 13. [Google Scholar] [CrossRef]
- Figueroa, J.D.; Ye, Y.; Siddiq, A.; Garcia-Closas, M.; Chatterjee, N.; Prokunina-Olsson, L.; Cortessis, V.K.; Kooperberg, C.; Cussenot, O.; Benhamou, S.; et al. Genome-Wide Association Study Identifies Multiple Loci Associated with Bladder Cancer Risk. Hum. Mol. Genet. 2014, 23, 1387–1398. [Google Scholar] [CrossRef]
- Hayashi, T.; Fujita, K.; Hayashi, Y.; Hatano, K.; Kawashima, A.; McConkey, D.J.; Nonomura, N. Mutational Landscape and Environmental Effects in Bladder Cancer. Int. J. Mol. Sci. 2020, 21, 6072. [Google Scholar] [CrossRef]
- Lozano, F.; Raventos, C.X.; Carrion, A.; Trilla, E.; Morote, J. Current Status of Genetic Urinary Biomarkers for Surveillance of Non-Muscle Invasive Bladder Cancer: A Systematic Review. BMC Urol. 2020, 20, 99. [Google Scholar] [CrossRef] [PubMed]
- Pineda, S.; Milne, R.L.; Calle, M.L.; Rothman, N.; López de Maturana, E.; Herranz, J.; Kogevinas, M.; Chanock, S.J.; Tardón, A.; Márquez, M.; et al. Genetic Variation in the TP53 Pathway and Bladder Cancer Risk: A Comprehensive Analysis. PLoS ONE 2014, 9, e89952. [Google Scholar] [CrossRef] [PubMed]
- Złowocka-Perłowska, E.; Dębniak, T.; Słojewski, M.; Lemiński, A.; Soczawa, M.; van de Wetering, T.; Trubicka, J.; Kluźniak, W.; Wokołorczyk, D.; Cybulski, C.; et al. Recurrent PALB2 Mutations and the Risk of Cancers of Bladder or Kidney in Polish Population. Hered. Cancer Clin. Pract. 2021, 19, 6. [Google Scholar] [CrossRef] [PubMed]
- Cumberbatch, M.G.; Rota, M.; Catto, J.W.; La Vecchia, C. The Role of Tobacco Smoke in Bladder and Kidney Carcinogenesis: A Comparison of Exposures and Meta-analysis of Incidence and Mortality Risks. Eur. Urol. 2016, 70, 458–466. [Google Scholar] [CrossRef]
- Kiriluk, K.J.; Prasad, S.M.; Patel, A.R.; Steinberg, G.D.; Smith, N.D. Bladder Cancer Risk from Occupational and Environmental Exposures. Urol. Oncol. 2012, 30, 199–211. [Google Scholar] [CrossRef] [PubMed]
- Moore, L.E.; Baris, D.R.; Figueroa, J.D.; Garcia-Closas, M.; Karagas, M.R.; Schwenn, M.R.; Johnson, A.T.; Lubin, J.H.; Hein, D.W.; Dagnall, C.L.; et al. GSTM1 Null and NAT2 Slow Acetylation Genotypes, Smoking Intensity and Bladder Cancer Risk: Results from the New England Bladder Cancer Study and NAT2 Meta-Analysis. Carcinogenesis 2011, 32, 182–189. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Harling, M.; Schablon, A.; Schedlbauer, G.; Dulon, M.; Nienhaus, A. Bladder Cancer among Hairdressers: A Meta-Analysis. Occup. Environ. Med. 2010, 67, 351–358. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Koutros, S.; Silverman, D.T.; Baris, D.; Zahm, S.H.; Morton, L.M.; Colt, J.S.; Hein, D.W.; Moore, L.E.; Johnson, A.; Schwenn, M.; et al. Hair Dye Use and Risk of Bladder Cancer in the New England Bladder Cancer Study. Int. J. Cancer 2011, 129, 2894–2904. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Alberg, A.J.; Hébert, J.R. Cigarette Smoking and Bladder Cancer: A New Twist in an Old Saga? J. Natl. Cancer Inst. 2009, 101, 1525–1526. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bell, D.A.; Taylor, J.A.; Paulson, D.F.; Robertson, C.N.; Mohler, J.L.; Lucier, G.W. Genetic Risk and Carcinogen Exposure: A Common Inherited Defect of the Carcinogen-Metabolism Gene Glutathione S-Transferase M1 (GSTM1) That Increases Susceptibility to Bladder Cancer. J. Natl. Cancer Inst. 1993, 85, 1159–1164. [Google Scholar] [CrossRef] [PubMed]
- Lesseur, C.; Gilbert-Diamond, D.; Andrew, A.S.; Ekstrom, R.M.; Li, Z.; Kelsey, K.T.; Marsit, C.J.; Karagas, M.R. A Case-Control Study of Polymorphisms in Xenobiotic and Arsenic Metabolism Genes and Arsenic-Related Bladder Cancer in New Hampshire. Toxicol. Lett. 2012, 210, 100–106. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hung, R.J.; Boffetta, P.; Brennan, P.; Malaveille, C.; Gelatti, U.; Placidi, D.; Carta, A.; Hautefeuille, A.; Porru, S. Genetic Polymorphisms of MPO, COMT, MnSOD, NQO1, Interactions with Environmental Exposures and Bladder Cancer Risk. Carcinogenesis 2004, 25, 973–978. [Google Scholar] [CrossRef] [PubMed]
- Mbemi, A.; Khanna, S.; Njiki, S.; Yedjou, C.G.; Tchounwou, P.B. Impact of Gene-Environment Interactions on Cancer Development. Int. J. Environ. Res. Public Health 2020, 17, 8089. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yao, B.; Yan, Y.; Ye, X.; Fang, H.; Xu, H.; Liu, Y.; Li, S.; Zhao, Y. Intake of Fruit and Vegetables and Risk of Bladder Cancer: A Dose-Response Meta-Analysis of Observational Studies. Cancer Causes Control 2014, 25, 1645–1658. [Google Scholar] [CrossRef] [PubMed]
- Steinmaus, C.M.; Nuñez, S.; Smith, A.H. Diet and Bladder Cancer: A Meta-Analysis of Six Dietary Variables. Am. J. Epidemiol. 2000, 151, 693–702. [Google Scholar] [CrossRef] [PubMed]
- Qin, J.; Xie, B.; Mao, Q.; Kong, D.; Lin, Y.; Zheng, X. Tea Consumption and Risk of Bladder Cancer: A Meta-Analysis. World J. Surg. Oncol. 2012, 10, 172. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mao, Q.Q.; Dai, Y.; Lin, Y.W.; Qin, J.; Xie, L.P.; Zheng, X.Y. Milk Consumption and Bladder Cancer Risk: A Meta-Analysis of Published Epidemiological Studies. Nutr. Cancer 2011, 63, 1263–1271. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; An, S.; Hou, L.; Chen, P.; Lei, C.; Tan, W. Red and Processed Meat Intake and Risk of Bladder Cancer: A Meta-Analysis. Int. J. Clin. Exp. Med. 2014, 7, 2100–2110. [Google Scholar] [PubMed] [PubMed Central]
- Tang, J.E.; Wang, R.J.; Zhong, H.; Yu, B.; Chen, Y. Vitamin A and Risk of Bladder Cancer: A Meta-Analysis of Epidemiological Studies. World J. Surg. Oncol. 2014, 12, 130. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wang, Y.Y.; Wang, X.L.; Yu, Z.J. Vitamin C and E Intake and Risk of Bladder Cancer: A Meta-Analysis of Observational Studies. Int. J. Clin. Exp. Med. 2014, 7, 4154–4164. [Google Scholar] [PubMed] [PubMed Central]
- Liao, Y.; Huang, J.L.; Qiu, M.X.; Ma, Z.W. Impact of Serum Vitamin D Level on Risk of Bladder Cancer: A Systematic Review and Meta-Analysis. Tumour Biol. 2015, 36, 1567–1572. [Google Scholar] [CrossRef] [PubMed]
- Amaral, A.F.; Cantor, K.P.; Silverman, D.T.; Malats, N. Selenium and Bladder Cancer Risk: A Meta-Analysis. Cancer Epidemiol. Biomarkers Prev. 2010, 19, 2407–2415. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Myung, S.K.; Kim, Y.; Ju, W.; Choi, H.J.; Bae, W.K. Effects of Antioxidant Supplements on Cancer Prevention: Meta-Analysis of Randomized Controlled Trials. Ann. Oncol. 2010, 21, 166–179. [Google Scholar] [CrossRef] [PubMed]
- Keimling, M.; Behrens, G.; Schmid, D.; Jochem, C.; Leitzmann, M.F. The Association between Physical Activity and Bladder Cancer: Systematic Review and Meta-Analysis. Br. J. Cancer 2014, 110, 1862–1870. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rogers, C.J.; Colbert, L.H.; Greiner, J.W.; Perkins, S.N.; Hursting, S.D. Physical Activity and Cancer Prevention: Pathways and Targets for Intervention. Sports Med. 2008, 38, 271–296. [Google Scholar] [CrossRef] [PubMed]
- Al-Zalabani, A.H.; Stewart, K.F.; Wesselius, A.; Schols, A.M.; Zeegers, M.P. Modifiable Risk Factors for the Prevention of Bladder Cancer: A Systematic Review of Meta-Analyses. Eur. J. Epidemiol. 2016, 31, 811–851. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Heidar, N.A.; Bhat, T.A.; Shabir, U.; Hussein, A.A. The Urinary Microbiome and Bladder Cancer. Life 2023, 13, 812. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hussein, A.A.; Elsayed, A.S.; Durrani, M.; Jing, Z.; Iqbal, U.; Gomez, E.C.; Singh, P.K.; Liu, S.; Smith, G.; Tang, L.; et al. Investigating the Association between the Urinary Microbiome and Bladder Cancer: An Exploratory Study. Urol. Oncol. 2021, 39, 370.e9–370.e19. [Google Scholar] [CrossRef] [PubMed]
- El-Mosalamy, H.; Salman, T.M.; Ashmawey, A.M.; Osama, N. Role of Chronic E. coli Infection in the Process of Bladder Cancer—An Experimental Study. Infect. Agent Cancer 2012, 7, 19. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Curtiss, N.; Balachandran, A.; Krska, L.; Peppiatt-Wildman, C.; Wildman, S.; Duckett, J. Age, menopausal status and the bladder microbiome. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 228, 126–129. [Google Scholar] [CrossRef] [PubMed]
- Leslie, S.W.; Soon-Sutton, T.L.; Aeddula, N.R. Bladder Cancer. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Jiang, S.; Redelman-Sidi, G. BCG in Bladder Cancer Immunotherapy. Cancers 2022, 14, 3073. [Google Scholar] [CrossRef] [PubMed]
- Colbert, L.; Jia, Y.; Sharma, A.; Hu, J.; Xu, Z.; Suzman, D.L.; Das, A.; Bross, P.; Kluetz, P.G.; Fashoyin-Aje, L.A.; et al. FDA Approval Summary: Nadofaragene Firadenovec-vncg for Bacillus Calmette–Guérin–Unresponsive Non–Muscle-Invasive Bladder Cancer. Clin. Cancer Res. 2025, 31, 1182–1185. [Google Scholar] [CrossRef] [PubMed]
- Waheed, A.; Gul, M.H.; Wardak, A.B.; Raja, H.A.A.; Hussaini, H. Nogapendekin alfa inbakicept-PMLN: First approval milestone for BCG-unresponsive noninvasive bladder cancer: Editorial. Ann. Med. Surg. 2024, 86, 6386–6388. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Abou Chakra, M.; McElree, I.M.; Packiam, V.T.; Mott, S.L.; O’Donnell, M.A. Early experience with sequential intravesical gemcitabine and docetaxel for micropapillary variant non-muscle invasive bladder cancer. Urol. Oncol. 2024, 42, 289.e13–289.e21. [Google Scholar] [CrossRef] [PubMed]
- Meghani, K.; Cooley, L.F.; Choy, B.; Kocherginsky, M.; Swaminathan, S.; Munir, S.S.; Svatek, R.S.; Kuzel, T.; Meeks, J.J. First-in-human Intravesical Delivery of Pembrolizumab Identifies Immune Activation in Bladder Cancer Unresponsive to Bacillus Calmette-Guérin. Eur. Urol. 2022, 82, 602–610. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kim, L.H.C.; Patel, M.I. Transurethral Resection of Bladder Tumour (TURBT). Transl. Androl. Urol. 2020, 9, 3056–3072. [Google Scholar] [CrossRef]
- Liu, H.; Zhou, Z.; Yao, H.; Mao, Q.; Chu, Y.; Cui, Y.; Wu, J. Robot-Assisted Radical Cystectomy vs Open Radical Cystectomy in Patients with Bladder Cancer: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. World J. Surg. Oncol. 2023, 21, 240. [Google Scholar] [CrossRef]
- Li, Z.J.; Wang, D.Y.; Liu, Z.H. Clinical Efficacy and Quality of Life Assessment of Partial Cystectomy and Plasmakinetic Transurethral Resection of Tumor in Bladder Cancer Patients. Cancer Manag. Res. 2022, 14, 389–398. [Google Scholar] [CrossRef]
- Heymach, J.V.; Harpole, D.; Mitsudomi, T.; Taube, J.M.; Galffy, G.; Hochmair, M.; Winder, T.; Zukov, R.; Garbaos, G.; Gao, S.; et al. Perioperative Durvalumab for Resectable Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2023, 389, 1672–1684. [Google Scholar] [CrossRef]
- McFerrin, C.; Davaro, F.; May, A.; Raza, S.; Siddiqui, S.; Hamilton, Z. Trends in Utilization of Neoadjuvant and Adjuvant Chemotherapy for Muscle-Invasive Bladder Cancer. Investig. Clin. Urol. 2020, 61, 565–572. [Google Scholar] [CrossRef]
- Pfister, C.; Gravis, G.; Fléchon, A.; Chevreau, C.; Mahammedi, H.; Laguerre, B.; Guillot, A.; Joly, F.; Soulié, M.; Allory, Y.; et al. VESPER Trial Investigators. Dose-Dense Methotrexate, Vinblastine, Doxorubicin, and Cisplatin or Gemcitabine and Cisplatin as Perioperative Chemotherapy for Patients With Nonmetastatic Muscle-Invasive Bladder Cancer: Results of the GETUG-AFU V05 VESPER Trial. J. Clin. Oncol. 2022, 40, 2013–2022. [Google Scholar] [CrossRef] [PubMed]
- Powles, T.; Catto, J.W.F.; Galsky, M.D.; Al-Ahmadie, H.; Meeks, J.J.; Nishiyama, H.; Vu, T.Q.; Antonuzzo, L.; Wiechno, P.; Atduev, V.; et al. NIAGARA Investigators. Perioperative Durvalumab with Neoadjuvant Chemotherapy in Operable Bladder Cancer. N. Engl. J. Med. 2024, 14, 1773–1786. [Google Scholar] [CrossRef] [PubMed]
- Bajorin, D.F.; Witjes, J.A.; Gschwend, J.E.; Schenker, M.; Valderrama, B.P.; Tomita, Y.; Bamias, A.; Lebret, T.; Shariat, S.F.; Park, S.H.; et al. Adjuvant Nivolumab versus Placebo in Muscle-Invasive Urothelial Carcinoma. N. Engl. J. Med. 2021, 3, 2102–2114, Erratum in N. Engl. J. Med. 2021, 26, 864. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Apolo, A.B.; Ballman, K.V.; Sonpavde, G.; Berg, S.; Kim, W.Y.; Parikh, R.; Teo, M.Y.; Sweis, R.F.; Geynisman, D.M.; Grivas, P.; et al. Adjuvant Pembrolizumab versus Observation in Muscle-Invasive Urothelial Carcinoma. N. Engl. J. Med. 2025, 392, 45–55. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Swinton, M.; Mariam, N.B.G.; Tan, J.L.; Murphy, K.; Elumalai, T.; Soni, M.; Ferrera, A.; Richardson, C.; Walshaw, R.; Mistry, H.; et al. Bladder-Sparing Treatment with Radical Dose Radiotherapy Is an Effective Alternative to Radical Cystectomy in Patients with Clinically Node-Positive Nonmetastatic Bladder Cancer. J. Clin. Oncol. 2023, 41, 4406–4415. [Google Scholar] [CrossRef]
- Mathes, J.; Rausch, S.; Todenhöfer, T.; Stenzl, A. Trimodal therapy for muscle-invasive bladder cancer. Expert Rev. Anticancer. Ther. 2018, 18, 1219–1229. [Google Scholar] [CrossRef]
- Zargar, H.; Aning, J.; Ischia, J.; So, A.; Black, P. Optimizing intravesical mitomycin C therapy in non-muscle-invasive bladder cancer. Nat. Rev. Urol. 2014, 11, 220–230. [Google Scholar] [CrossRef]
- Suzman, D.L.; Agrawal, S.; Ning, Y.M.; Maher, V.E.; Fernandes, L.L.; Karuri, S.; Tang, S.; Sridhara, R.; Schroeder, J.; Goldberg, K.B.; et al. FDA Approval Summary: Atezolizumab or Pembrolizumab for the Treatment of Patients with Advanced Urothelial Carcinoma Ineligible for Cisplatin-Containing Chemotherapy. Oncologist 2019, 24, 563–569. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Raja, R.; Kuziora, M.; Brohawn, P.Z.; Higgs, B.W.; Gupta, A.; Dennis, P.A.; Ranade, K. Early Reduction in ctDNA Predicts Survival in Patients with Lung and Bladder Cancer Treated with Durvalumab. Clin. Cancer Res. 2018, 24, 6212–6222. [Google Scholar] [CrossRef] [PubMed]
- Zajac, M.; Boothman, A.M.; Ben, Y.; Gupta, A.; Jin, X.; Mistry, A.; Sabalos, C.; Nielsen, A.; Manriquez, G.; Barker, C.; et al. Analytical Validation and Clinical Utility of an Immunohistochemical Programmed Death Ligand-1 Diagnostic Assay and Combined Tumor and Immune Cell Scoring Algorithm for Durvalumab in Urothelial Carcinoma. Arch. Pathol. Lab. Med. 2019, 143, 722–731. [Google Scholar] [CrossRef] [PubMed]
- Basile, G.; Bandini, M.; Gibb, E.A.; Ross, J.S.; Raggi, D.; Marandino, L.; Costa de Padua, T.; Crupi, E.; Colombo, R.; Colecchia, M.; et al. Neoadjuvant Pembrolizumab and Radical Cystectomy in Patients with Muscle-Invasive Urothelial Bladder Cancer: 3-Year Median Follow-Up Update of PURE-01 Trial. Clin. Cancer Res. 2022, 28, 5107–5114. [Google Scholar] [CrossRef] [PubMed]
- Fléchon, A.; Morales-Barrera, R.; Powles, T.; Alva, A.; Özgüroğlu, M.; Csöszi, T.; Loriot, Y.; Rodriguez-Vida, A.; Géczi, L.; Cheng, S.Y.; et al. Association of Tumor Mutational Burden and PD-L1 with the Efficacy of Pembrolizumab with or without Chemotherapy versus Chemotherapy in Advanced Urothelial Carcinoma. Clin. Cancer Res. 2024, 30, 5353–5364. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zeng, H.; Zhou, Q.; Wang, Z.; Zhang, H.; Liu, Z.; Huang, Q.; Wang, J.; Chang, Y.; Bai, Q.; Xia, Y.; et al. Stromal LAG-3+ Cells Infiltration Defines Poor Prognosis Subtype Muscle-Invasive Bladder Cancer with Immunoevasive Contexture. J. Immunother. Cancer 2020, 8, e000651. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sridhar, S.S.; Powles, T.; Climent Durán, M.A.; Park, S.H.; Massari, F.; Thiery-Vuillemin, A.; Valderrama, B.P.; Ullén, A.; Tsuchiya, N.; Aragon-Ching, J.B.; et al. Avelumab First-Line Maintenance for Advanced Urothelial Carcinoma: Analysis from JAVELIN Bladder 100 by Duration of First-Line Chemotherapy and Interval Before Maintenance. Eur. Urol. 2024, 85, 154–163. [Google Scholar] [CrossRef]
- Ding, M.; Lin, J.; Qin, C.; Fu, Y.; Du, Y.; Qiu, X.; Wei, P.; Xu, T. Novel CAR-T Cells Specifically Targeting SIA-CIgG Demonstrate Effective Antitumor Efficacy in Bladder Cancer. Adv. Sci. 2024, 11, e2400156. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hoffman-Censits, J.H.; Lombardo, K.A.; Parimi, V.; Kamanda, S.; Choi, W.; Hahn, N.M.; McConkey, D.J.; McGuire, B.M.; Bivalacqua, T.J.; Kates, M.; et al. Expression of Nectin-4 in Bladder Urothelial Carcinoma, in Morphologic Variants, and Nonurothelial Histotypes. Appl. Immunohistochem. Mol. Morphol. 2021, 29, 619–625. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chandran, E.B.A.; Iannantuono, G.M.; Atiq, S.O.; Akbulut, D.; Sinaii, N.; Simon, N.I.; Banday, A.R.; Boudjadi, S.; Gurram, S.; Nassar, A.H.; et al. Mismatch Repair Deficiency and Microsatellite Instability in Urothelial Carcinoma: A Systematic Review and Meta-Analysis. BMJ Oncol. 2024, 3, e000335. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Liu, D.; Xu, S.; Chang, T.; Ma, S.; Wang, K.; Sun, G.; Chen, S.; Xu, Y.; Zhang, H. Predicting Prognosis and Distinguishing Cold and Hot Tumors in Bladder Urothelial Carcinoma Based on Necroptosis-Associated lncRNAs. Front. Immunol. 2022, 13, 916800. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Giudice, G.C.; Sonpavde, G.P. Vaccine Approaches to Treat Urothelial Cancer. Hum. Vaccines Immunother. 2024, 20, 2379086. [Google Scholar] [CrossRef]
- Shen, J.; Dai, D.; Zhao, W.; Liu, T.; Zhao, Y.; Xu, Y.; Qi, Y.; Hong, J.; Shi, X.; Yang, Z.; et al. A Novel Co-Receptor with Mutated TIGIT to Enhance PSCA CAR-T Therapy for Bladder Cancer. J. Clin. Oncol. 2024, 42, e14574. [Google Scholar] [CrossRef]
- Zhang, G.; Wang, Y.; Lu, S.; Ding, F.; Wang, X.; Zhu, C.; Wang, Y.; Wang, K. Molecular Understanding and Clinical Outcomes of CAR T Cell Therapy in the Treatment of Urological Tumors. Cell Death Dis. 2024, 15, 359. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.M.; Su, F.; Kalyana-Sundaram, S.; Khazanov, N.; Ateeq, B.; Cao, X.; Lonigro, R.J.; Vats, P.; Wang, R.; Lin, S.F.; et al. Identification of Targetable FGFR Gene Fusions in Diverse Cancers. Cancer Discov. 2013, 3, 636–647. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Parker, B.C.; Annala, M.J.; Cogdell, D.E.; Granberg, K.J.; Sun, Y.; Ji, P.; Li, X.; Gumin, J.; Zheng, H.; Hu, L.; et al. The Tumorigenic FGFR3-TACC3 Gene Fusion Escapes miR-99a Regulation in Glioblastoma. J. Clin. Investig. 2013, 123, 855–865. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Minner, S.; Sauter, G. Tumoren des ableitenden Harntrakts. Aktuelle und alte Probleme [Tumors of the urinary system. Current and old problems]. Pathologe 2009, 30 (Suppl. S2), 179–184. [Google Scholar] [CrossRef]
- Perera, T.P.S.; Jovcheva, E.; Mevellec, L.; Vialard, J.; De Lange, D.; Verhulst, T.; Paulussen, C.; Van De Ven, K.; King, P.; Freyne, E.; et al. Discovery and Pharmacological Characterization of JNJ-42756493 (Erdafitinib), a Functionally Selective Small-Molecule FGFR Family Inhibitor. Mol. Cancer Ther. 2017, 16, 1010–1020. [Google Scholar] [CrossRef] [PubMed]
- Cancer Genome Atlas Research Network. Comprehensive Molecular Characterization of Urothelial Bladder Carcinoma. Nature 2014, 507, 315–322. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Aggen, D.H.; Drake, C.G. Biomarkers for Immunotherapy in Bladder Cancer: A Moving Target. J. Immunother. Cancer 2017, 5, 94. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chow, N.H.; Chan, S.H.; Tzai, T.S.; Ho, C.L.; Liu, H.S. Expression Profiles of ErbB Family Receptors and Prognosis in Primary Transitional Cell Carcinoma of the Urinary Bladder. Clin. Cancer Res. 2001, 7, 1957–1962. [Google Scholar] [PubMed]
- Baselga, J.; Swain, S.M. Novel Anticancer Targets: Revisiting ERBB2 and Discovering ERBB3. Nat. Rev. Cancer 2009, 9, 463–475. [Google Scholar] [CrossRef] [PubMed]
- Koshkin, V.S.; O’donnell, P.; Yu, E.Y.; Grivas, P.; Donnell, P.O. Systematic Review: Targeting HER2 in Bladder Cancer. Bladder Cancer 2019, 5, 1–12. [Google Scholar] [CrossRef]
- Zvereva, M.; Pisarev, E.; Hosen, I.; Kisil, O.; Matskeplishvili, S.; Kubareva, E.; Kamalov, D.; Tivtikyan, A.; Manel, A.; Vian, E.; et al. Activating Telomerase TERT Promoter Mutations and Their Application for the Detection of Bladder Cancer. Int. J. Mol. Sci. 2020, 21, 6034. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nagata, M.; Muto, S.; Horie, S. Molecular Biomarkers in Bladder Cancer: Novel Potential Indicators of Prognosis and Treatment Outcomes. Dis. Markers 2016, 2016, 8205836. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Shariat, S.F.; Tokunaga, H.; Zhou, J.; Kim, J.; Ayala, G.E.; Benedict, W.F.; Lerner, S.P. p53, p21, pRB, and p16 Expression Predict Clinical Outcome in Cystectomy with Bladder Cancer. J. Clin. Oncol. 2004, 22, 1014–1024. [Google Scholar] [CrossRef] [PubMed]
- Lyu, Q.; Lin, A.; Cao, M.; Xu, A.; Luo, P.; Zhang, J. Alterations in TP53 Are a Potential Biomarker of Bladder Cancer Patients Who Benefit from Immune Checkpoint Inhibition. Cancer Control 2020, 27, 1073274820976665. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ahangar, M.; Mahjoubi, F.; Mowla, S.J. Bladder Cancer Biomarkers: Current Approaches and Future Directions. Front. Oncol. 2024, 14, 1453278. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kopparapu, P.K.; Boorjian, S.A.; Robinson, B.D.; Downes, M.; Gudas, L.J.; Mongan, N.P.; Persson, J.L. Expression of VEGF and Its Receptors VEGFR1/VEGFR2 Is Associated with Invasiveness of Bladder Cancer. Anticancer Res. 2013, 33, 2381–2390. [Google Scholar] [PubMed]
- Mohammed, A.A.; El-Tanni, H.; El-Khatib, H.M.; Mirza, A.A.; Mirza, A.A.; Alturaifi, T.H. Urinary Bladder Cancer: Biomarkers and Target Therapy, New Era for More Attention. Oncol. Rev. 2016, 10, 320. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gao, Q.; Liu, Y.; Xie, H.; Zhong, Y.; Liao, X.; Zhan, H.; Zhou, Q.; Ding, M.; Yang, K.; Li, A.; et al. Lentivirus-Mediated shRNA Targeting MUTYH Inhibits Malignant Phenotypes of Bladder Cancer SW780 Cells. OncoTargets Ther. 2018, 11, 6101–6109. [Google Scholar] [CrossRef]
- Mitra, A.P. Molecular Substratification of Bladder Cancer: Moving Towards Individualized Patient Management. Ther. Adv. Urol. 2016, 8, 215–233. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Daneshmand, S.; Zaucha, R.; Vasdev, N.; Gartrell, B.A.; Lotan, Y.; Hussain, S.A.; Lee, E.K.; Procopio, G.; Galanternik, F.; Pignot, G.; et al. Marker Lesion Study of Oral Erdafitinib in Patients with Intermediate-Risk Non-Muscle–Invasive Bladder Cancer with FGFR3/2 Alterations in THOR-2: Updated Cohort 3 Results. Urol. Oncol. 2024, 42, S58. [Google Scholar] [CrossRef]
- Sternberg, C.N.; Petrylak, D.P.; Bellmunt, J.; Nishiyama, H.; Necchi, A.; Gurney, H.; Lee, J.L.; van der Heijden, M.S.; Rosenbaum, E.; Penel, N.; et al. FORT-1: Phase II/III Study of Rogaratinib Versus Chemotherapy in Patients with Locally Advanced or Metastatic Urothelial Carcinoma Selected Based on FGFR1/3 mRNA Expression. J. Clin. Oncol. 2023, 41, 629–639. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Necchi, A.; Pouessel, D.; Leibowitz, R.; Gupta, S.; Fléchon, A.; García-Donas, J.; Bilen, M.A.; Debruyne, P.R.; Milowsky, M.I.; Friedlander, T.; et al. Pemigatinib for Metastatic or Surgically Unresectable Urothelial Carcinoma with FGF/FGFR Genomic Alterations: Final Results from FIGHT-201. Ann. Oncol. 2024, 35, 200–210. [Google Scholar] [CrossRef] [PubMed]
- Huan, J.; Grivas, P.; Birch, J.; Hansel, D.E. Emerging Roles for Mammalian Target of Rapamycin (mTOR) Complexes in Bladder Cancer Progression and Therapy. Cancers 2022, 14, 1555. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- McPherson, V.; Reardon, B.; Bhayankara, A.; Scott, S.N.; Boyd, M.E.; Garcia-Grossman, I.R.; Regazzi, A.M.; McCoy, A.S.; Kim, P.H.; Al-Ahmadie, H.; et al. A Phase 2 Trial of Buparlisib in Patients with Platinum-Resistant Metastatic Urothelial Carcinoma. Cancer 2020, 126, 4532–4544. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rosenberg, J.E.; Ballman, K.A.; Halabi, S.; Atherton, P.J.; Mortazavi, A.; Sweeney, C.; Stadler, W.M.; Teply, B.A.; Picus, J.; Tagawa, S.T.; et al. Randomized Phase III Trial of Gemcitabine and Cisplatin with Bevacizumab or Placebo in Patients with Advanced Urothelial Carcinoma: Results of CALGB 90601 (Alliance). J. Clin. Oncol. 2021, 39, 2486–2496. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Galffy, G.; Lugowska, I.; Poddubskaya, E.V.; Cho, B.C.; Ahn, M.J.; Han, J.Y.; Su, W.C.; Hauke, R.J.; Dyar, S.H.; Lee, D.H.; et al. A Phase II Open-Label Trial of Avelumab Plus Axitinib in Previously Treated Non-Small-Cell Lung Cancer or Treatment-Naïve, Cisplatin-Ineligible Urothelial Cancer. ESMO Open 2023, 8, 101173. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhu, K.; Yang, X.; Tai, H.; Zhong, X.; Luo, T.; Zheng, H. HER2-Targeted Therapies in Cancer: A Systematic Review. Biomark. Res. 2024, 12, 16. [Google Scholar] [CrossRef]
- Tang, D.; Yan, Y.; Li, Y.; Li, Y.; Tian, J.; Yang, L.; Ding, H.; Bashir, G.; Zhou, H.; Ding, Q.; et al. Targeting DAD1 Gene with CRISPR-Cas9 System Transmucosally Delivered by Fluorinated Polylysine Nanoparticles for Bladder Cancer Intravesical Gene Therapy. Theranostics 2024, 14, 203–219. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Xu, Y.; Sun, X.; Liu, G.; Li, H.; Yu, M.; Zhu, Y. Integration of Multi-Omics and Clinical Treatment Data Reveals Bladder Cancer Therapeutic Vulnerability Gene Combinations and Prognostic Risks. Front. Immunol. 2024, 14, 1301157. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Xu, H.; Liu, Z.; Weng, S.; Dang, Q.; Ge, X.; Zhang, Y.; Ren, Y.; Xing, Z.; Chen, S.; Zhou, Y.; et al. Artificial Intelligence-Driven Consensus Gene Signatures for Improving Bladder Cancer Clinical Outcomes Identified by Multi-Center Integration Analysis. Mol. Oncol. 2022, 16, 4023–4042. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kim, H.S.; Seo, H.K. Emerging Treatments for Bacillus Calmette-Guérin-Unresponsive Non-Muscle-Invasive Bladder Cancer. Investig. Clin. Urol. 2021, 62, 361–377. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nagayama, A.; Ellisen, L.W.; Chabner, B.; Bardia, A. Antibody-Drug Conjugates for the Treatment of Solid Tumors: Clinical Experience and Latest Developments. Target Oncol. 2017, 12, 719–739. [Google Scholar] [CrossRef] [PubMed]
- Parslow, A.C.; Parakh, S.; Lee, F.T.; Gan, H.K.; Scott, A.M. Antibody-Drug Conjugates for Cancer Therapy. Biomedicines 2016, 4, 14. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kim, J.H.; Chang, I.H. A Novel Strategy for Treatment of Bladder Cancer: Antibody-Drug Conjugates. Investig. Clin. Urol. 2022, 63, 373–384. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rosenberg, J.E.; O’Donnell, P.H.; Balar, A.V.; McGregor, B.A.; Heath, E.I.; Yu, E.Y.; Galsky, M.D.; Hahn, N.M.; Gartner, E.M.; Pinelli, J.M.; et al. Pivotal Trial of Enfortumab Vedotin in Urothelial Carcinoma After Platinum and Anti-Programmed Death 1/Programmed Death Ligand 1 Therapy. J. Clin. Oncol. 2019, 37, 2592–2600. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Samanta, D.; Almo, S.C. Nectin Family of Cell-Adhesion Molecules: Structural and Molecular Aspects of Function and Specificity. Cell Mol. Life Sci. 2015, 72, 645–658. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nadal, R.; Clara, J.A.; Valderrama, B.P.; Bellmunt, J. Current Therapy for Metastatic Urothelial Carcinoma. Hematol. Oncol. Clin. North Am. 2021, 35, 469–493. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.; Weinstock, C.; Zhang, L.; Charlab, R.; Dorff, S.E.; Gong, Y.; Hsu, V.; Li, F.; Ricks, T.K.; Song, P.; et al. FDA Approval Summary: Enfortumab Vedotin for Locally Advanced or Metastatic Urothelial Carcinoma. Clin. Cancer Res. 2021, 27, 922–927. [Google Scholar] [CrossRef]
- Brave, M.H.; Maguire, W.F.; Weinstock, C.; Zhang, H.; Gao, X.; Li, F.; Yu, J.; Fu, W.; Zhao, H.; Pierce, W.F.; et al. FDA Approval Summary: Enfortumab Vedotin Plus Pembrolizumab for Locally Advanced or Metastatic Urothelial Carcinoma. Clin. Cancer Res. 2024, 30, 4815–4821. [Google Scholar] [CrossRef]
- Sahota, S.; Vahdat, L.T. Sacituzumab Govitecan: An Antibody-Drug Conjugate. Expert Opin. Biol. Ther. 2017, 17, 1027–1031. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, D.M.; Sharkey, R.M. Antibody-Drug Conjugates Targeting TROP-2 and Incorporating SN-38: A Case Study of Anti-TROP-2 Sacituzumab Govitecan. MAbs 2019, 11, 987–995. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tagawa, S.T.; Balar, A.V.; Petrylak, D.P.; Kalebasty, A.R.; Loriot, Y.; Fléchon, A.; Jain, R.K.; Agarwal, N.; Bupathi, M.; Barthelemy, P.; et al. TROPHY-U-01: A Phase II Open-Label Study of Sacituzumab Govitecan in Patients with Metastatic Urothelial Carcinoma Progressing After Platinum-Based Chemotherapy and Checkpoint Inhibitors. J. Clin. Oncol. 2021, 39, 2474–2485. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Benjamin, D.J.; Kalebasty, A.R.; Mar, N. Implications and Lessons from the Withdrawal of Sacituzumab Govitecan for Treating Advanced Urothelial Carcinoma. Eur. Urol. Oncol. 2025, 8, 242–244. [Google Scholar] [CrossRef] [PubMed]
- Powles, T.; Tagawa, S.; Vulsteke, C.; Gross-Goupil, M.; Park, S.; Necchi, A.; De Santis, M.; Duran, I.; Morales-Barrera, R.; Guo, J.; et al. Sacituzumab govitecan in advanced urothelial carcinoma: TROPiCS-04, a phase III randomized trial. Ann. Oncol. 2025, 36, 561–571. [Google Scholar] [CrossRef] [PubMed]
- Srinivasalu, V.K.; Robbrecht, D. Advancements in First-Line Treatment of Metastatic Bladder Cancer: EV-302 and Checkmate-901 Insights and Future Directions. Cancers 2024, 16, 2398. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fleischmann, A.; Rotzer, D.; Seiler, R.; Studer, U.E.; Thalmann, G.N. Her2 Amplification Is Significantly More Frequent in Lymph Node Metastases from Urothelial Bladder Cancer than in the Primary Tumours. Eur. Urol. 2011, 60, 350–357. [Google Scholar] [CrossRef] [PubMed]
- Robertson, A.G.; Kim, J.; Al-Ahmadie, H.; Bellmunt, J.; Guo, G.; Cherniack, A.D.; Hinoue, T.; Laird, P.W.; Hoadley, K.A.; Akbani, R.; et al. Comprehensive Molecular Characterization of Muscle-Invasive Bladder Cancer. Cell 2017, 171, 540–556.e25. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hayashi, T.; Seiler, R.; Oo, H.Z.; Jäger, W.; Moskalev, I.; Awrey, S.; Dejima, T.; Todenhöfer, T.; Li, N.; Fazli, L.; et al. Targeting HER2 with T-DM1, an Antibody Cytotoxic Drug Conjugate, Is Effective in HER2 Overexpressing Bladder Cancer. J. Urol. 2015, 194, 1120–1131. [Google Scholar] [CrossRef] [PubMed]
- Di Paolo, C.; Willuda, J.; Kubetzko, S.; Lauffer, I.; Tschudi, D.; Waibel, R.; Plückthun, A.; Stahel, R.A.; Zangemeister-Wittke, U. A Recombinant Immunotoxin Derived from a Humanized Epithelial Cell Adhesion Molecule-Specific Single-Chain Antibody Fragment Has Potent and Selective Antitumor Activity. Clin. Cancer Res. 2003, 9, 2837–2848. [Google Scholar] [PubMed]
- Fong, D.; Seeber, A.; Terracciano, L.; Kasal, A.; Mazzoleni, G.; Lehne, F.; Gastl, G.; Spizzo, G. Expression of EpCAM(MF) and EpCAM(MT) Variants in Human Carcinomas. J. Clin. Pathol. 2014, 67, 408–414. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kowalski, M.; Entwistle, J.; Cizeau, J.; Niforos, D.; Loewen, S.; Chapman, W.; MacDonald, G.C. A Phase I Study of an Intravesically Administered Immunotoxin Targeting EpCAM for the Treatment of Nonmuscle-Invasive Bladder Cancer in BCG-Refractory and BCG-Intolerant Patients. Drug Des. Devel. Ther. 2010, 4, 313–320. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kowalski, M.; Guindon, J.; Brazas, L.; Moore, C.; Entwistle, J.; Cizeau, J.; Jewett, M.A.; MacDonald, G.C. A Phase II Study of Oportuzumab Monatox: An Immunotoxin Therapy for Patients with Noninvasive Urothelial Carcinoma In Situ Previously Treated with Bacillus Calmette-Guérin. J. Urol. 2012, 188, 1712–1718. [Google Scholar] [CrossRef] [PubMed]
- Breij, E.C.; de Goeij, B.E.; Verploegen, S.; Schuurhuis, D.H.; Amirkhosravi, A.; Francis, J.; Miller, V.B.; Houtkamp, M.; Bleeker, W.K.; Satijn, D.; et al. An Antibody-Drug Conjugate That Targets Tissue Factor Exhibits Potent Therapeutic Activity Against a Broad Range of Solid Tumors. Cancer Res. 2014, 74, 1214–1226. [Google Scholar] [CrossRef] [PubMed]
- Patry, G.; Hovington, H.; Larue, H.; Harel, F.; Fradet, Y.; Lacombe, L. Tissue Factor Expression Correlates with Disease-Specific Survival in Patients with Node-Negative Muscle-Invasive Bladder Cancer. Int. J. Cancer 2008, 122, 1592–1597. [Google Scholar] [CrossRef] [PubMed]
- de Bono, J.S.; Concin, N.; Hong, D.S.; Thistlethwaite, F.C.; Machiels, J.P.; Arkenau, H.T.; Plummer, R.; Jones, R.H.; Nielsen, D.; Windfeld, K.; et al. Tisotumab Vedotin in Patients with Advanced or Metastatic Solid Tumours (InnovaTV 201): A First-in-Human, Multicentre, Phase 1–2 Trial. Lancet Oncol. 2019, 20, 383–393. [Google Scholar] [CrossRef]
- Narayan, V.M.; Meeks, J.J.; Jakobsen, J.S.; Shore, N.D.; Sant, G.R.; Konety, B.R. Mechanism of Action of Nadofaragene Firadenovec-VNCG. Front. Oncol. 2024, 14, 1359725. [Google Scholar] [CrossRef]
- Konety, B.R.; Shore, N.D.; Sant, G.R. Clinical Use of Nadofaragene Firadenovec-VNCG. Ther. Adv. Urol. 2024, 16, 17562872241280005. [Google Scholar] [CrossRef]
- Zhou, Q.; Fang, L.; Tang, Y.; Wang, Q.; Tang, X.; Zhu, L.; Peng, N.; Wang, B.; Song, W.; Fu, H. Exosome-Mediated Delivery of Artificial Circular RNAs for Gene Therapy of Bladder Cancer. J. Cancer 2024, 15, 1770–1778. [Google Scholar] [CrossRef]
- Casper, J.; Schenk, S.H.; Parhizkar, E.; Detampel, P.; Dehshahri, A.; Huwyler, J. Polyethylenimine (PEI) in Gene Therapy: Current Status and Clinical Applications. J. Control Release 2023, 362, 667–691. [Google Scholar] [CrossRef]
- McNall, S.; Hooper, K.; Sullivan, T.; Rieger-Christ, K.; Clements, M. Treatment Modalities for Non-Muscle Invasive Bladder Cancer: An Updated Review. Cancers 2024, 16, 1843. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Goulet, M.-L.; Dauphinee, S.M.; Veilleux, D.; Louis, K.S.; Lazure, D.; Stevenson, S.; Bilimoria, D.; Zamzameer, F.; Chen, X.; Sublemontier, S.; et al. Abstract PR006: EG-70 (Detalimogene Voraplasmid), a Novel, Non-Viral Intravesical Gene Therapy for BCG-Unresponsive Non-Muscle-Invasive Bladder Cancer: Preclinical Characterization and Translation into the Clinic. Clin. Cancer Res. 2024, 30, PR006. [Google Scholar] [CrossRef]
- Hannouneh, Z.A.; Hijazi, A.; Alsaleem, A.A.; Hami, S.; Kheyrbek, N.; Tanous, F.; Khaddour, K.; Abbas, A.; Alshehabi, Z. Novel Immunotherapeutic Options for BCG-Unresponsive High-Risk Non-Muscle-Invasive Bladder Cancer. Cancer Med. 2023, 12, 21944–21968. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kochergin, M.; Fahmy, O.; Asimakopoulos, A.; Theil, G.; Zietz, K.; Bialek, J.; Tiberi, E.; Gakis, G. Photodynamic Therapy: Current Trends and Potential Future Role in the Treatment of Bladder Cancer. Int. J. Mol. Sci. 2024, 25, 960. [Google Scholar] [CrossRef] [PubMed]
- Kurabayashi, A.; Fukuhara, H.; Furihata, K.; Iwashita, W.; Furihata, M.; Inoue, K. Photodynamic Diagnosis and Therapy in Non-Muscle-Invasive Bladder Cancer. Cancers 2024, 16, 2299. [Google Scholar] [CrossRef]
- Zhang, C.; Zhao, J.; Wang, W.; Geng, H.; Wang, Y.; Gao, B. Current Advances in the Application of Nanomedicine in Bladder Cancer. Biomed. Pharmacother. 2023, 157, 114062. [Google Scholar] [CrossRef] [PubMed]
- Yan, X.; Al-Hayek, S.; Huang, H.; Zhu, Z.; Zhu, W.; Guo, H. Photodynamic Effect of 5-Aminolevulinic Acid-Loaded Nanoparticles on Bladder Cancer Cells: A Preliminary Investigation. Scand. J. Urol. 2013, 47, 145–151. [Google Scholar] [CrossRef]
- Lin, T.Y.; Li, Y.; Liu, Q.; Chen, J.L.; Zhang, H.; Lac, D.; Zhang, H.; Ferrara, K.W.; Wachsmann-Hogiu, S.; Li, T.; et al. Novel Theranostic Nanoporphyrins for Photodynamic Diagnosis and Trimodal Therapy for Bladder Cancer. Biomaterials 2016, 104, 339–351. [Google Scholar] [CrossRef]
- Winnicka, A.; Brzeszczyńska, J.; Saluk, J.; Wigner-Jeziorska, P. Nanomedicine in Bladder Cancer Therapy. Int. J. Mol. Sci. 2024, 25, 10388. [Google Scholar] [CrossRef]
- He, L.; Wang, L.; Yu, X.; Tang, Y.; Jiang, Z.; Yang, G.; Liu, Z.; Li, W. Full-Course NIR-II Imaging-Navigated Fractionated Photodynamic Therapy of Bladder Tumours with X-Ray-Activated Nanotransducers. Nat. Commun. 2024, 15, 8240. [Google Scholar] [CrossRef]
- Ashrafizadeh, M.; Zarrabi, A.; Karimi-Maleh, H.; Taheriazam, A.; Mirzaei, S.; Hashemi, M.; Hushmandi, K.; Makvandi, P.; Nazarzadeh Zare, E.; Sharifi, E.; et al. (Nano)platforms in Bladder Cancer Therapy: Challenges and Opportunities. Bioeng. Transl. Med. 2022, 8, e10353. [Google Scholar] [CrossRef]
- Liang, Y.; Wang, Y.; Wang, L.; Liang, Z.; Li, D.; Xu, X.; Chen, Y.; Yang, X.; Zhang, H.; Niu, H. Self-Crosslinkable Chitosan-Hyaluronic Acid Dialdehyde Nanoparticles for CD44-Targeted siRNA Delivery to Treat Bladder Cancer. Bioact. Mater. 2021, 6, 433–446. [Google Scholar] [CrossRef]
- Ahir, M.; Upadhyay, P.; Ghosh, A.; Sarker, S.; Bhattacharya, S.; Gupta, P.; Ghosh, S.; Chattopadhyay, S.; Adhikary, A. Delivery of Dual miRNA Through CD44-Targeted Mesoporous Silica Nanoparticles for Enhanced and Effective Triple-Negative Breast Cancer Therapy. Biomater. Sci. 2020, 8, 2939–2954. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Lin, X.; Pang, G.; Deng, J.; Xie, Q.; Zhang, Z. Significance of KDM6A Mutation in Bladder Cancer Immune Escape. BMC Cancer 2021, 21, 635. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Cui, J.; Zhao, Y.; Liu, X.; Chen, L.; Xia, Y.; Wang, Y.; Chen, S.; Sun, S.; Shi, B.; et al. KDM6A-ARHGDIB Axis Blocks Metastasis of Bladder Cancer by Inhibiting Rac1. Mol. Cancer 2021, 20, 77. [Google Scholar] [CrossRef]
- Kong, N.; Zhang, R.; Wu, G.; Sui, X.; Wang, J.; Kim, N.Y.; Blake, S.; De, D.; Xie, T.; Cao, Y.; et al. Intravesical Delivery of KDM6A-mRNA via Mucoadhesive Nanoparticles Inhibits the Metastasis of Bladder Cancer. Proc. Natl. Acad. Sci. USA 2022, 119, e2112696119. [Google Scholar] [CrossRef]
- Terán-Navarro, H.; Zeoli, A.; Salines-Cuevas, D.; Marradi, M.; Montoya, N.; Gonzalez-Lopez, E.; Ocejo-Vinyals, J.G.; Dominguez-Esteban, M.; Gutierrez-Baños, J.L.; Campos-Juanatey, F.; et al. Gold Glyconanoparticles Combined with 91-99 Peptide of the Bacterial Toxin, Listeriolysin O, Are Efficient Immunotherapies in Experimental Bladder Tumors. Cancers 2022, 14, 2413. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhao, Z.; Ukidve, A.; Kim, J.; Mitragotri, S. Targeting Strategies for Tissue-Specific Drug Delivery. Cell 2020, 181, 151–167. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Liu, Z.; Wang, J.; Li, L.; Wang, F.; Zhu, Z.; Wang, X. Nanomedicine for Combination Urologic Cancer Immunotherapy. Pharmaceutics 2023, 15, 546. [Google Scholar] [CrossRef]
- Lv, M.; Shang, S.; Liu, K.; Wang, Y.; Xu, P.; Song, H.; Zhang, J.; Sun, Z.; Yan, Y.; Zhu, Z.; et al. Revitalizing Bacillus Calmette-Guérin Immunotherapy for Bladder Cancer: Nanotechnology and Bioengineering Approaches. Pharmaceutics 2024, 16, 1067. [Google Scholar] [CrossRef]
- Zhou, Q.; Ding, W.; Qian, Z.; Zhu, Q.; Sun, C.; Yu, Q.; Tai, Z.; Xu, K. Immunotherapy Strategy Targeting Programmed Cell Death Ligand 1 and CD73 with Macrophage-Derived Mimetic Nanovesicles to Treat Bladder Cancer. Mol. Pharm. 2021, 18, 4015–4028. [Google Scholar] [CrossRef]
- Liu, F.; Guo, C.; Li, X.; Li, Y.; Xu, S.; James, T.D.; Wang, L. A Versatile Nano-Transformer for Efficient Localization-Specific Imaging and Synergistic Therapy of Bladder Cancer. Nano Today 2024, 54, 102116. [Google Scholar] [CrossRef]
- Simó, C.; Serra-Casablancas, M.; Hortelao, A.C.; Di Carlo, V.; Guallar-Garrido, S.; Plaza-García, S.; Rabanal, R.M.; Ramos-Cabrer, P.; Yagüe, B.; Aguado, L.; et al. Urease-Powered Nanobots for Radionuclide Bladder Cancer Therapy. Nat. Nanotechnol. 2024, 19, 554–564. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Yu, T.; Zhou, B.; Wei, J.; Fang, Y.; Lu, J.; Guo, L.; Chen, W.; Liu, Z.P.; Luo, J. Mg(II)-Catechin Nanoparticles Delivering siRNA Targeting EIF5A2 Inhibit Bladder Cancer Cell Growth In Vitro and In Vivo. Biomaterials 2016, 81, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Arista-Romero, M.; Cascante, A.; Fornaguera, C.; Borrós, S. Role of Survivin in Bladder Cancer: Issues to Be Overcome When Designing an Efficient Dual Nano-Therapy. Pharmaceutics 2021, 13, 1959. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wei, J.; Cheang, T.; Tang, B.; Xia, H.; Xing, Z.; Chen, Z.; Fang, Y.; Chen, W.; Xu, A.; Wang, S.; et al. The Inhibition of Human Bladder Cancer Growth by Calcium Carbonate/CaIP6 Nanocomposite Particles Delivering AIB1 siRNA. Biomaterials 2013, 34, 1246–1254. [Google Scholar] [CrossRef] [PubMed]
- Sari Motlagh, R.; Ghoreifi, A.; Yanagisawa, T.; Kawada, T.; Kikic, Z.; Gill, I.; Daneshmand, S.; Djaladat, H.; Shariat, S.F. Survival of Patients with Chronic Kidney Disease Treated with Radical Cystectomy and Risk Factors of Glomerular Filtration Rate Loss Following Radical Cystectomy: Two Systematic Reviews and Meta-analyses of Interplay Between Radical Cystectomy and Renal Function. Eur. Urol. Focus 2023, 10, 169–181. [Google Scholar] [CrossRef] [PubMed]
- Panunzio, A.; Gozzo, A.; Mazzucato, G.; Ornaghi, P.I.; Di Filippo, G.; Soldano, A.; De Maria, N.; Cianflone, F.; Orlando, R.; Boldini, M.; et al. Impairment in Activities of Daily Living Assessed by the Barthel Index Predicts Adverse Oncological Outcomes After Radical Cystectomy for Bladder Cancer. Clin. Genitourin. Cancer 2023, 21, e495–e501.e2. [Google Scholar] [CrossRef] [PubMed]
- Ben-David, R.; Tillu, N.; Cumarasamy, S.; Alerasool, P.; Rich, J.M.; Kaufmann, B.; Elkun, Y.; Attalla, K.; Mehrazin, R.; Wiklund, P.; et al. Longitudinal Tumor-informed Circulating Tumor DNA Status Predicts Disease Upstaging and Poor Prognosis for Patients Undergoing Radical Cystectomy. Eur. Urol. Oncol. 2024, 7, 1105–1112. [Google Scholar] [CrossRef] [PubMed]
- Russo, P.; Marino, F.; Rossi, F.; Bizzarri, F.P.; Ragonese, M.; Dibitetto, F.; Filomena, G.B.; Marafon, D.P.; Ciccarese, C.; Iacovelli, R.; et al. Is Systemic Immune-Inflammation Index a Real Non-Invasive Biomarker to Predict Oncological Outcomes in Patients Eligible for Radical Cystectomy? Medicina 2023, 59, 2063. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nardelli, C.; Aveta, A.; Pandolfo, S.D.; Tripodi, L.; Russo, F.; Imbimbo, C.; Castaldo, G.; Pastore, L. Microbiome Profiling in Bladder Cancer Patients Using the First-morning Urine Sample. Eur. Urol. Open Sci. 2023, 59, 18–26. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pucci, C.; Martinelli, C.; Ciofani, G. Innovative approaches for cancer treatment: Current perspectives and new challenges. ecancermedicalscience 2019, 13, 961. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
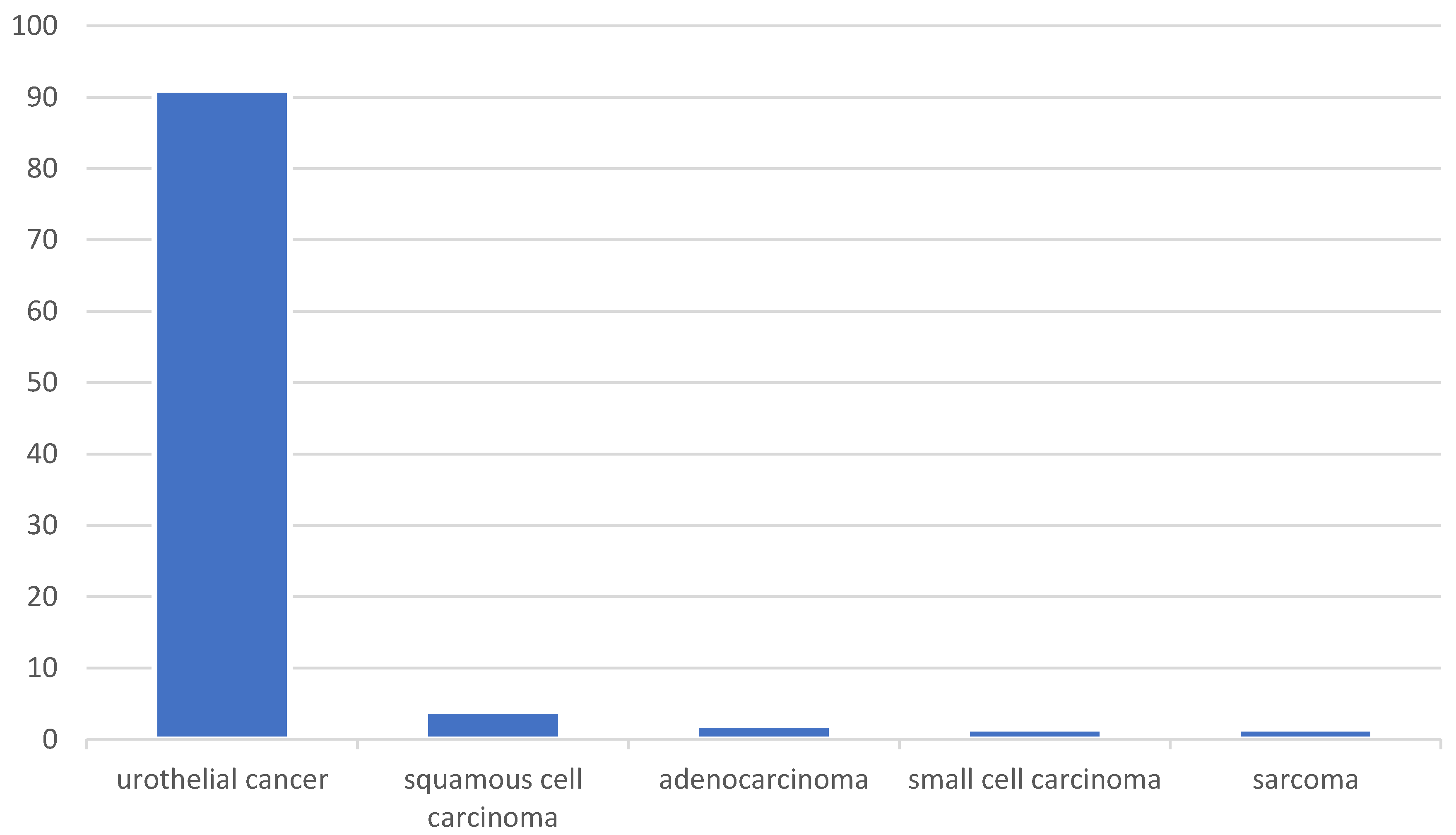
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).