Abstract
Advances in screening, early detection, and therapeutic innovations have significantly improved survival rates, transforming prostate cancer into a chronic condition for many men. However, these strides have also revealed persistent challenges in survivorship, including treatment-related side effects, disparities in care, and inequities in outcomes. This review explores the complex landscape of prostate cancer survivorship, with a focus on demographic disparities, barriers to care, symptom burden, and treatment patterns. Our findings highlight how factors such as race, socioeconomic status, and insurance type heavily influence patient outcomes. For instance, Black and Latiné patients often face delays in treatment initiation and are less likely to receive definitive therapies than White patients, leading to poorer survival outcomes. Furthermore, those with Medicaid or no insurance are more likely to receive systemic therapy only or no treatment at all, exacerbating existing inequities. Addressing gaps in diagnosis, treatment access, and survivorship care is essential to developing targeted interventions and policies that promote equitable, patient-centered care for prostate cancer survivors.
1. Introduction
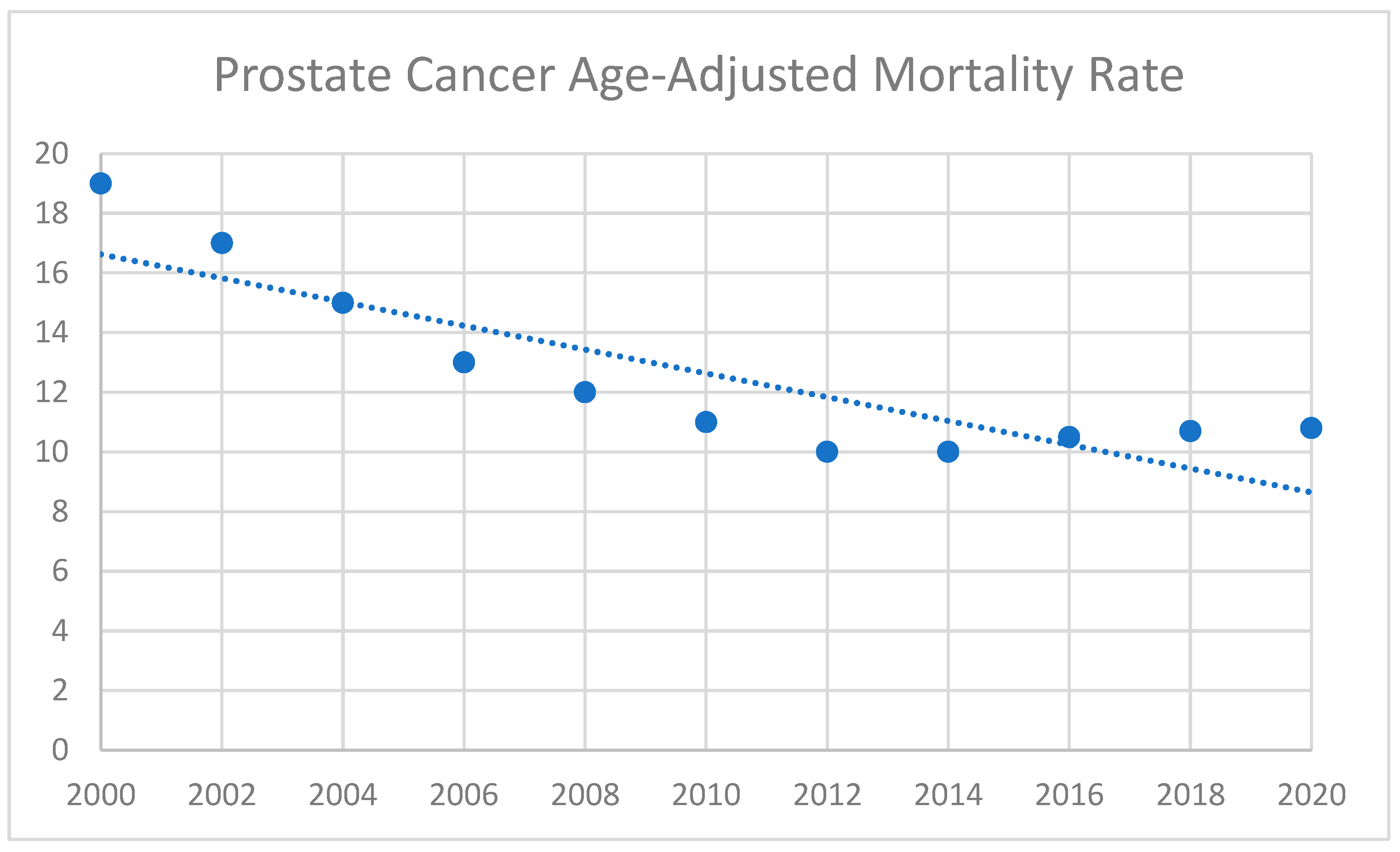
Prostate cancer is among the most frequently diagnosed cancers in men worldwide and remains a leading contributor to cancer-related mortality [1]. Advances in screening, early detection, and therapeutic innovations have greatly extended survival, turning prostate cancer into a chronic condition for many patients [2]. Prostate cancer survival data from the Centers for Disease Control (CDC) WONDER database that highlight this trend are shown in Figure 1. Consequently, survivorship has become a central concern in oncology, addressing the long-term physical, emotional, and social impacts faced by individuals post-treatment. In prostate cancer, these issues are particularly pronounced due to the persistent side effects of treatment and the growing population of men living longer after diagnosis [3].
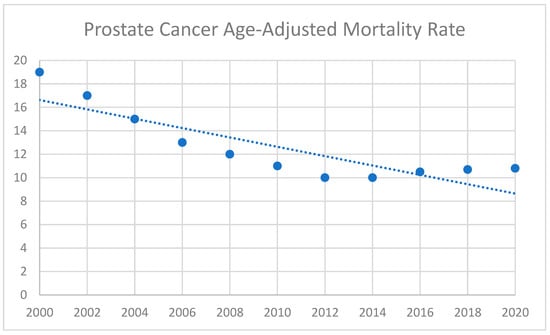
Figure 1.
Prostate cancer mortality. Data from the Centers for Disease Control (CDC) WONDER database showing the age-adjusted mortality rate (per 100,000) from 2000 to 2020.
Advancements in therapies, including surgery, radiation, and systemic treatments, have significantly extended survival [3]. Yet, as survival rates have improved, more patients live with treatment-related side effects such as urinary incontinence, sexual dysfunction, bowel dysfunction, and hormonal changes [1,2]. These side effects not only affect physical well-being but also lead to emotional and psychological burdens, underscoring the need for comprehensive survivorship care plans that address quality of life in addition to survival outcomes.
Disparities in oncology care also shape survivorship. Differences in access to care, treatment utilization, and outcomes are influenced by socioeconomic status, race, education, and insurance type [4]. Black and Hispanic patients, for example, are more likely to experience delays in treatment and poorer survival outcomes. Additionally, uninsured patients are less likely to receive definitive care than those with private insurance [4,5]. Such disparities highlight systemic barriers to equitable cancer care and underscore the importance of targeted interventions to reduce gaps in outcomes.
While prostate cancer survivorship has become an increasingly important area of research, notable gaps in the literature remain, as shown in Table 1. Existing research emphasizes short-term clinical outcomes or narrowly defined cohorts, often overlooking the long-term physical, emotional, and psychosocial challenges faced by diverse patient populations. Additionally, studies frequently under-represent racial and ethnic minorities, uninsured or underinsured individuals, and those from lower socioeconomic backgrounds. Furthermore, survivorship frameworks tend to lack specificity regarding care coordination and the role of community-based interventions in mitigating inequities. This narrative review aims to address these gaps by examining disparities across the survivorship continuum and highlighting strategies to deliver more equitable, patient-centered care.

Table 1.
Comparison of major reviews on prostate cancer survivorship.
2. Disparities in Prostate Cancer Diagnosis
2.1. Demographic Profiles of Prostate Cancer Patients
The American Urological Association (AUA) and the Society of Urologic Oncology (SUO) report that prostate cancer remains the most common solid organ malignancy among men in the U.S., with a significant incidence in older adults, particularly those around the age of 65 [10]. The National Comprehensive Cancer Network (NCCN) notes that prostate cancer incidence has been increasing annually by 3% since 2014, driven by diagnoses in older men [11]. However, these aggregate demographic trends mask the disproportionate burden borne by racial and ethnic minority populations and individuals of lower socioeconomic status, who remain under-represented in clinical trials and registries.
2.2. Impact of Socioeconomic Factors and Insurance Coverage
Socioeconomic status (SES) and insurance type are pivotal determinants of prostate cancer diagnosis and treatment outcomes. Smani et al., using data from the National Cancer Database, found that uninsured and Medicaid-insured patients, particularly younger men under 55 years old, had significantly higher odds of being diagnosed with advanced prostate cancer compared to those with private insurance [12]. Similarly, patients in lower-income brackets were more likely to present with advanced-stage disease, highlighting financial barriers to early detection and care. Late-stage diagnoses were also more common among patients with Medicaid (31.6%) and those who were uninsured (32.4%), compared to patients with private insurance (19.2%) or Medicare (21.9%) [13]. Neighborhood socioeconomic status (nSES), which reflects the economic and social conditions of a community, is also crucial in driving disparities [14]. Press et al. found that nSES was the most substantial factor associated with elevated PSA levels and high-risk disease in Black men [15]. These findings underscore the cumulative impact of structural inequities, which contribute to delayed diagnosis, reduced access to screening, and higher-risk disease at presentation.
2.3. Racial Disparities in Diagnosis and Symptom Presentation
Prostate-specific antigen (PSA) screening is lower among Black men, despite higher prostate cancer incidence and mortality in this population [16]. National guidelines do not provide clear guidance for this high-risk group, but several models have shown that annual screening in Black men would reduce mortality. In these models, limiting screening to men younger than 70 years old can help reduce overdiagnosis [17]. Racial disparities are also well-documented in symptom presentation and management, particularly among African American men. Multiple studies have shown that Black men are significantly more likely to present with advanced or metastatic disease compared to their White counterparts. For example, Chornokur et al. reported higher rates of advanced disease at diagnosis among African American men, while Mahal et al. found an adjusted odds ratio (OR) of 1.65 for Black men presenting with metastatic disease compared to non-Black men [18,19,20]. These trends suggest systemic delays in diagnosis and limited access to early detection services within Black communities.
Functional disparities also exist prior to treatment. Orom et al. found that Black and Hispanic men exhibited worse pretreatment urinary function compared to White men, indicating disparities in underlying health status that may influence both treatment decisions and quality of life outcomes [21].
In terms of overall incidence, Black men face a disproportionately higher burden of prostate cancer, with an age-adjusted incidence rate of 302.6 cases per 100,000 men compared to 186.6 for White men, 153.2 for Hispanic men, and lower rates among Asian and American Indian/Alaska Native populations [22]. They are also more likely to present with high-risk disease features, including elevated PSA levels, higher Gleason scores, and advanced-stage tumors at diagnosis [15]. Even after adjusting for these clinical factors, Black men face worse cancer-specific survival rates compared to White men [23]. These findings underscore the urgent need to address racial disparities in early detection and pretreatment care to improve outcomes.
3. Disparities in Prostate Cancer Treatment
3.1. Socioeconomic and Insurance-Based Disparities
Socioeconomic status (SES) and insurance type are among the strongest predictors of access to high-quality prostate cancer treatment. Patients with Medicaid or Medicare experience longer delays in treatment initiation and are significantly less likely to receive advanced or definitive therapies compared to those with private insurance [9]. A meta-analysis by Gallagher et al. showed that lower education levels were associated with a higher likelihood of receiving non-active treatments such as active surveillance or watchful waiting [24]. Individuals from lower-income neighborhoods or communities with lower educational attainment are also less likely to receive guideline-concordant treatment. For example, patients residing in areas with higher median income and education levels are more likely to receive advanced therapies, such as proton beam therapy (PBT) [25].
3.2. Racial and Ethnic Disparities in Treatment Utilization
Racial disparities in treatment selection and access remain a pervasive issue. Black patients are more likely to receive systemic therapy alone (OR 1.93) or no treatment (OR 1.46) compared to White patients, despite evidence that definitive treatments such as surgery or radiation improve survival [13,26,27,28]. Freedland et al. found that Black patients were less likely to receive treatment compared to non-Latiné White (NLW) patients, while Latiné patients born outside the U.S. exhibited better survival despite presenting with more advanced disease and lower socioeconomic status [25]. Hispanic patients also face elevated odds of receiving suboptimal treatment. These disparities directly contribute to worse overall survival among racial and ethnic minority populations [29]. Additionally, Black and Hispanic patients are more likely to experience delays in initiating treatment [13]. These delays are clinically meaningfully, often resulting in disease progression and reduced therapeutic benefit. Cultural, structural, and language-related factors further compound disparities in healthcare utilization and outcomes.
3.3. Access to High-Quality Surgical and Radiation Care
Access to high-volume hospitals and advanced technologies is associated with improved prostate cancer outcomes, yet racial and socioeconomic disparities persist in referrals and utilization. For instance, Black patients and those from socioeconomically disadvantaged backgrounds are less likely to receive care at high-volume hospitals or access advanced modalities such as proton beam therapy (PBT) [25]. Nonetheless, when access is equitable, outcomes are comparable. Matched-pair analyses show no significant differences in quality-of-life outcomes between Black and White patients treated with PBT, highlighting that disparities are primarily driven by systemic barriers rather than inherent biological differences. A study by Krimphove et al. showed that Black men with advanced prostate cancer had worse overall survival but when controlling for access to care and treatment, Black men actually demonstrated better overall survival [30]. A large retrospective study of the Veterans Affairs (VA) United States healthcare system of over 20 million veterans found that the overall survival rates in Black, Hispanic, and White men were similar [31]. These findings suggest that targeting access to care is crucial to reducing disparities in prostate cancer outcomes.
3.4. Intersection of Mental Health and Treatment Disparities
Disparities in mental health care among prostate cancer patients also mirror treatment inequities. For example, White patients are more likely to be diagnosed with depression and to receive appropriate mental health interventions, even when both groups are undergoing androgen deprivation therapy (ADT), which is a known risk factor for depressive symptoms [32]. These findings point to disparities in symptom recognition, provider referral patterns, and access to mental health services, which can further influence overall treatment adherence and survivorship outcomes.
3.5. Implications and Need for Equity Focused
The combined impact of socioeconomic, racial, and mental health disparities underscores the need for culturally sensitive, equity-focused interventions across the prostate cancer care continuum. Expanding access to early detection, timely and definitive therapies, and integrated mental health support are critical to improving both survival and quality of life. Future research should prioritize understanding barriers to care and developing targeted strategies to ensure timely, comprehensive treatments for all patients, regardless of background.
4. Disparities in Prostate Cancer Survivorship
4.1. Implications for Survivorship Care
Disparities in prostate cancer diagnosis and treatment extend into survivorship, influencing both the quality and consistency of ongoing care. Patients from historically underserved communities, whether due to racial, socioeconomic, or insurance-related barriers, may struggle to access consistent follow-up appointments, timely rehabilitation for treatment-related side effects, or essential psychosocial support programs [33,34,35]. These challenges can lead to gaps in symptom management, reduced adherence to preventive measures, and diminished overall quality of life. Addressing these inequities is crucial for guiding the development of targeted interventions, policy reforms, and patient education initiatives that promote coordinated, patient-centered survivorship care.
4.2. Age-Related Differences
Younger men with prostate cancer often report higher levels of psychological distress, including depression, stress, and anxiety, compared to older patients. This heightened distress is frequently tied to disease-specific symptoms such as sexual dysfunction and urinary issues, which younger patients may perceive as more impactful on their quality of life [36,37]. Furthermore, younger patients with high symptom burdens are more likely to experience cancer-specific distress, underscoring the need for age-appropriate psychological and supportive care interventions [38,39]. This age-related vulnerability highlights the need for age-appropriate survivorship models that integrate mental health support and targeted symptom management.
4.3. Socioeconomic Influences on Symptom Burden
Socioeconomic status (SES) significantly impacts the prevalence and severity of survivorship symptoms. Patients with higher education and income levels generally report lower symptom burdens. These patients have better health-related quality of life (HRQOL) scores, particularly in physical function, mental health, and overall well-being. They are less likely to experience severe urinary, bowel, and sexual dysfunction, and they report fewer psychological symptoms such as depression and anxiety [40,41].
Conversely, patients from lower socioeconomic backgrounds experience a higher prevalence of symptoms and poorer functional outcomes. These patients often report more severe urinary incontinence, bowel dysfunction, and sexual dysfunction. They also have higher rates of psychological distress, including depression and anxiety, which are exacerbated by financial difficulties and lower access to supportive care services. These disparities may reflect differences in access to resources, health literacy, and healthcare utilization [1,21,42,43,44,45]. A community partnered approach is beneficial and necessary in addressing these disparities.
4.4. Marital Status and Social Support
Marital status is another factor influencing HRQOL among prostate cancer survivors. Married patients tend to experience better mental health, lower urinary and sexual symptom burden, and greater emotional well-being, in part due to spousal support [35]. In contrast, unmarried patients, including those who are divorced, widowed, or never married, experience higher levels of psychological distress, including depression and anxiety, and report worse functional outcomes. Studies have shown that unmarried men are at a higher risk of all-cause and prostate-cancer-specific mortality. This increased risk is partly due to a lack of social support, which affects treatment adherence and overall well-being [46,47]. Unmarried patients are at higher risk of under-ascertainment of symptoms during treatment, such as radiation therapy, which can lead to inadequate symptom management and poorer outcomes. Enhancing survivorship must include attention to social support systems [43].
4.5. Comorbidities and Symptom Burden
Patients with preexisting comorbidities often experience more severe symptom burdens during survivorship. Hypertension and arthritis are associated with increased fatigue and reduced physical function, while diabetes is linked to worse urinary and sexual dysfunction [48,49]. Depression in particular is highly impactful, leading to higher levels of psychological distress and interfering with symptom self-management [50]. Moreover, patients with serious cardiovascular comorbidities are less likely to receive definitive therapies like surgery or radiation. These treatment decisions may also contribute to a different symptom trajectory and impact patients’ overall quality of life [51]. Survivorship planning must account for coexisting medical conditions to mitigate compounding effects on quality of life.
4.6. Treatment-Related Symptomatology
Treatments for prostate cancer are associated with distinct and sometimes persistent side effects that can significantly impact quality of life. Understanding how these therapies compare is critical to informing shared decision making and survivorship planning. Radical prostatectomy is most frequently associated with urinary incontinence and erectile dysfunction, particularly within the first year following surgery. While urinary function often improves over time, a significant proportion of men report persistent leakage. Sexual function also can remain impaired even several years after treatment. Studies show that 15–30% of men report moderate-to-severe urinary bother 5 years after prostatectomy, and 50–70% continue to experience erectile dysfunction [52]. External beam radiotherapy and brachytherapy are more commonly associated with bowel dysfunction, including urgency, frequency, and rectal bleeding. Urinary symptoms also occur but often subside over time. One comparative study showed that external beam radiation therapy with low-dose-rate brachytherapy was associated with worse urinary irritative/obstructive and bowel functions but better urinary incontinence outcomes 5 years after treatment [53]. Sexual dysfunction develops more gradually than after surgery, though many men ultimately report similar levels of dysfunction within 2–5 years post-treatment [45,54]. Meanwhile, androgen deprivation therapy (ADT) is associated with significant systemic side effects, including fatigue, depressive symptoms, and poor mental well-being. These effects are particularly pronounced in patients with higher baseline levels of depression or significant fatigue [2,55,56]. Active surveillance, while avoiding acute side effects, may worsen anxiety and distress due to the uncertainty of disease progression [45,54].
Comparative Summary:
- Surgery leads to the most immediate and severe urinary and sexual dysfunction, though bowel function is generally preserved.
- Radiation carries a higher risk of long-term bowel symptoms and gradual sexual decline, with fewer urinary side effects.
- Androgen deprivation therapy (ADT) causes systemic side effects, especially in the long term.
- Active Surveillance preserves function but carries the psychological burden of uncertainty.
Therapy-specific outcomes also vary depending on demographic and clinical factors. For example, younger patients and those from underserved populations may experience greater psychological or functional burden. Furthermore, the availability of rehabilitation and support services often dictates long-term outcomes. Integrating symptom management into survivorship care plans tailored by treatment modality and patient background is essential to improve quality of life across populations.
4.7. Detection Method and Functional Outcomes
The mode of prostate cancer detection significantly influences subsequent symptom experiences. Men diagnosed following symptomatic presentation, as opposed to PSA-based screening, often report poorer functional outcomes, including urinary incontinence, bowel dysfunction, and reduced sexual and hormonal vitality. These functional deficits persist across sociodemographic and clinical factors, highlighting the need for targeted survivorship care interventions [1].
4.8. Genetic Predispositions in Symptom Burden and Cancer Management
Emerging evidence suggests that biological factors such as genetic ancestry and tumor genomics also play a role in disparities observed in survivorship outcomes. Tumor profiling has revealed that African ancestry may be associated with more aggressive disease biology, which may influence both treatment needs and symptom burden [57,58]. While sociocultural and healthcare access factors remain significant, biological predispositions may play a role in differences in disease progression and treatment responses to different cohorts of patients. Several studies suggest that genetic ancestry is associated with tumor aggressiveness and may influence symptom severity and therapy management [57].
Gene expression assays such as Prolaris and Oncotype DX identify the upregulation of cell cycle progression (CCP) genes, which correlate with higher aggressiveness and potentially more intensive treatment requirements and subsequent side effects [59]. Decipher genomic classifier scores are similarly linked to increased risk of metastasis and recurrence, contributing to treatment escalation and long-term HRQOL impairment [60].
Tissue-based immune signatures provide insight into the tumor microenvironment, modulating both therapeutic responses and contributing to systemic symptoms. For example, tumors with higher expression of interferon signaling and immune checkpoint pathways may be associated with increased systemic inflammation and fatigue during treatment, especially among racial minorities [61]. More recently, advances in liquid biopsy techniques, such as circulating tumor DNA (ctDNA) profiling, offer novel insights into the genomic landscape of prostate cancer and its relationship to symptom burden. Elevated levels of ctDNA are associated with increased tumor volume and aggressiveness, which can manifest as more severe urinary symptoms, bone pain, fatigue, and other systemic effects, especially in patients with metastatic castration-resistant prostate cancer (mCRPC) [62].
Mutations in DNA repair genes such as BRCA2 and ATM also have prognostic and predictive value, signaling both higher risk and greater vulnerability to treatment-related toxicities [63]. The integration of genomic classifiers and tumor marker profiling into survivorship care planning holds potential for improving symptom anticipation and tailoring supportive care. Future research should prioritize prospective studies that correlate genomic profiles with patient-reported symptom outcomes to reduce disparities in long-term quality of life and survivorship care.
5. Strategies to Enhance Prostate Cancer Survivorship Care
5.1. Policy and Advocacy
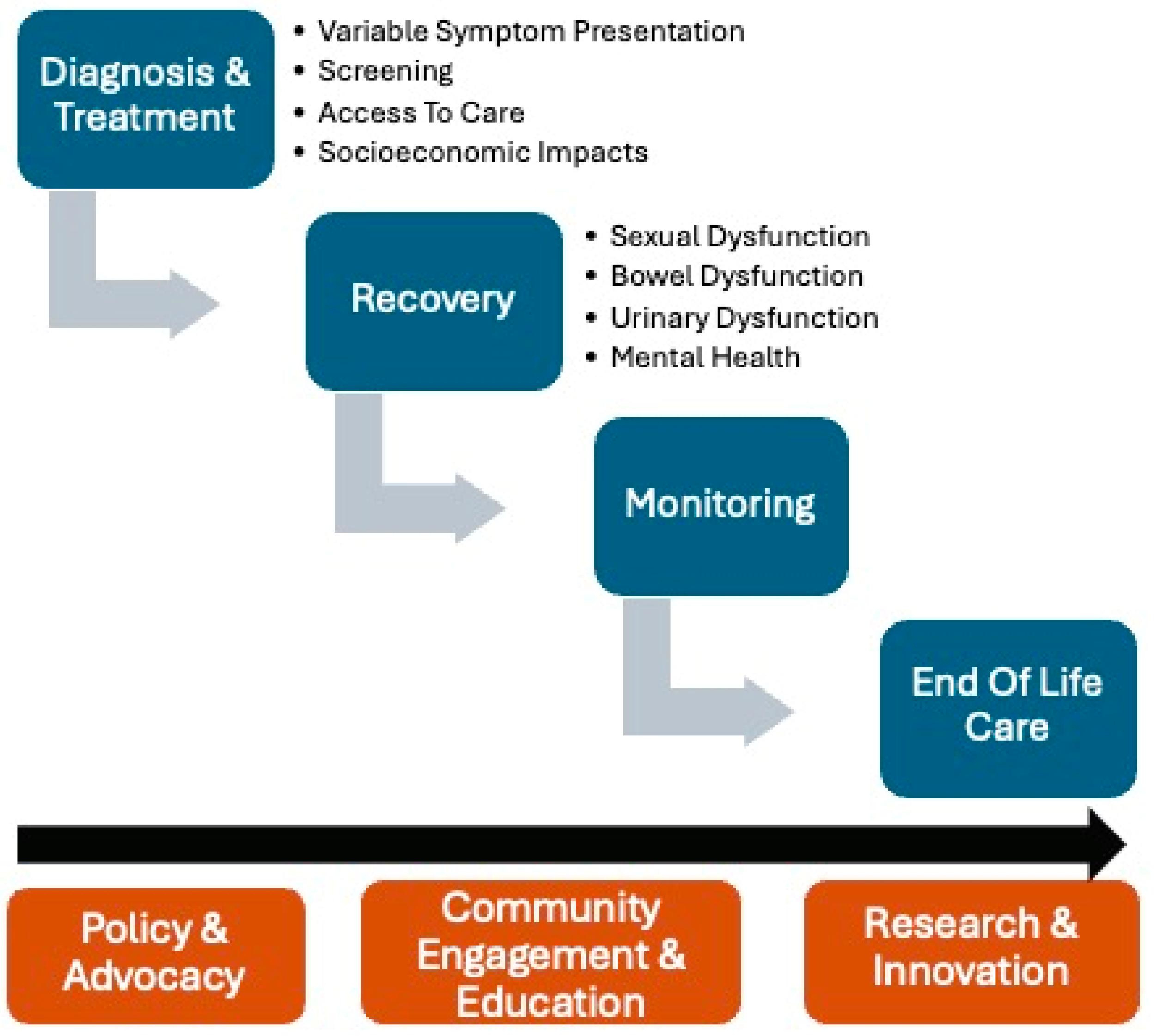
Improving prostate cancer survivorship care requires policies that prioritize equitable access to comprehensive and patient-centered care. These different facets are summarized in Figure 2. This begins with advocating for expanded insurance coverage and reduced out-of-pocket costs, ensuring that follow-up care, rehabilitation, and mental health services are accessible to all survivors, regardless of socioeconomic status [29,64]. Policymakers should also prioritize funding for survivorship research, targeting interventions to address long-term treatment side effects like urinary incontinence and sexual dysfunction [29]. Advocacy efforts must include equitable distribution of emerging technologies, such as precision medicine and advanced diagnostic tools, to underserved populations. These policies can bridge the gap between survival and quality of life, ensuring that survivorship care becomes a universal standard [65].
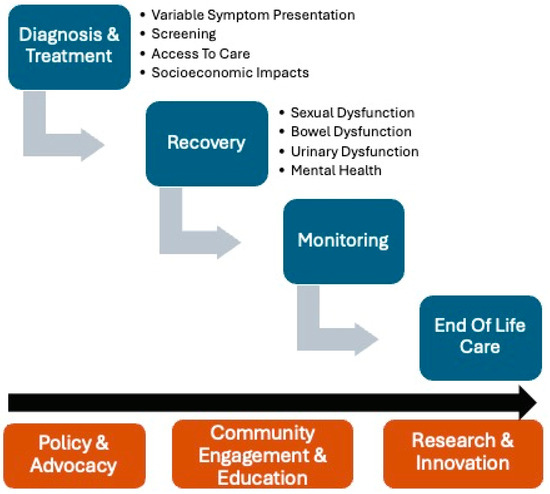
Figure 2.
A visual summary of facets to strategies to enhance prostate cancer survivorship care.
5.2. Community Engagement and Education
Community outreach is essential for empowering prostate cancer survivors, particularly in underserved populations. Educational campaigns tailored to diverse cultural contexts can enhance awareness of survivorship resources, including rehabilitation and mental health services. Establishing partnerships with community organizations to provide support groups, navigation services, and local workshops can address barriers such as transportation and language [33,66,67]. Examples like the IMPACT program in California and similar initiatives demonstrate how localized interventions can significantly improve outcomes for vulnerable populations [68,69]. The IMPACT program not only reduced financial barriers to care by providing access to free or low-cost treatments but also addressed systemic disparities through patient navigation and culturally tailored education, leading to earlier treatment initiation, improved adherence, and better overall health outcomes for low-income and uninsured men. Through sustained community engagement, survivorship care can be integrated into patients’ lives, fostering long-term wellness and reducing disparities.
5.3. Research and Innovation
Increased funding for survivorship-focused research is pivotal for developing targeted interventions and personalized care strategies [70]. Longitudinal studies exploring the psychosocial and functional outcomes of prostate cancer treatments can identify critical gaps in care [6]. Additionally, leveraging technology such as telemedicine and wearable health monitoring devices offers innovative solutions for managing long-term symptoms and improving patient–provider communication. Research initiatives should prioritize inclusivity, ensuring that under-represented populations are adequately represented in clinical trials and study cohorts [71,72]. By fostering a culture of innovation and equity in research, healthcare providers can address the complex needs of prostate cancer survivors and enhance their quality of life.
6. Conclusions and Future Directions
Reducing disparities in prostate cancer treatment and survivorship requires a multifaceted approach. Efforts to mitigate disparities in prostate cancer treatment must focus on improving access to definitive therapies, reducing delays in treatment initiation, and ensuring equitable utilization of advanced technologies. Policymakers and healthcare systems should prioritize interventions that address socioeconomic and racial barriers, such as expanding insurance coverage, increasing community health education, and improving access to high-volume treatment centers.
Author Contributions
Conceptualization, A.G., D.P., and Y.S.-L.; Methodology, A.G., D.P., K.Z.A., and Y.S.-L.; Writing-original draft preparation, A.G., D.P., and E.T.; Writing—review and editing, A.G., D.P., E.T., K.Z.A., and Y.S.-L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Donnelly, D.W.; Vis, L.C.; Kearney, T.; Sharp, L.; Bennett, D.; Wilding, S.; Downing, A.; Wright, P.; Watson, E.; Wagland, R.; et al. Quality of life among symptomatic compared to PSA-detected prostate cancer survivors—Results from a UK wide patient-reported outcomes study. BMC Cancer 2019, 19, 947. [Google Scholar] [CrossRef] [PubMed]
- Wilding, S.; Downing, A.; Wright, P.; Selby, P.; Watson, E.; Wagland, R.; Donnelly, D.W.; Hounsome, L.; Butcher, H.; Mason, M.; et al. Cancer-related symptoms, mental well-being, and psychological distress in men diagnosed with prostate cancer treated with androgen deprivation therapy. Qual. Life Res. 2019, 28, 2741–2751. [Google Scholar] [CrossRef]
- Lasorsa, F.; Biasatti, A.; Orsini, A.; Bignante, G.; Farah, G.M.; Pandolfo, S.D.; Lambertini, L.; Reddy, D.; Damiano, R.; Ditonno, P.; et al. Focal Therapy for Prostate Cancer: Recent Advances and Insights. Curr. Oncol. 2024, 32, 15. [Google Scholar] [CrossRef] [PubMed]
- Bagley, A.F.; Anscher, M.S.; Choi, S.; Frank, S.J.; Hoffman, K.E.; Kuban, D.A.; McGuire, S.E.; Nguyen, Q.-N.; Chapin, B.; Aparicio, A.; et al. Association of Sociodemographic and Health-Related Factors with Receipt of Nondefinitive Therapy Among Younger Men with High-Risk Prostate Cancer. JAMA Netw. Open 2020, 3, e201255. [Google Scholar] [CrossRef]
- Abodunrin, F.; Adeoye, O.; Nelson, N.; Amadi, N.I.; Silberstein, P.T.; Tupper, C. Socioeconomic and demographic patterns associated with treatment delay in prostate cancer: An analysis of the National Cancer Database. J. Clin. Oncol. 2023, 41 (Suppl. 16), e17122. [Google Scholar] [CrossRef]
- Narayan, V.M.; Harrison, M.; Cheng, H.H.; Yu, E.Y.; Morgans, A.K.; Sanda, M.G.; Smith, M.R.; Sartor, O.; Beer, T.M. Improving Research for Prostate Cancer Survivorship: A Statement from the Survivorship Research in Prostate Cancer (SuRECaP) Working Group. Urol. Oncol. 2020, 38, 83–93. [Google Scholar] [CrossRef]
- Crawford-Williams, F.; March, S.; Goodwin, B.C.; Ralph, N.; Israel, M.; Dunn, J. Interventions for Prostate Cancer Survivorship: A Systematic Review of Reviews. Psychooncology 2018, 27, 2339–2348. [Google Scholar] [CrossRef]
- Bourke, L.; Boorjian, S.A.; Briganti, A.; Klotz, L.; Mucci, L.; Resnick, M.J.; Rosario, D.J.; Skolarus, T.A.; Penson, D.F. Survivorship and Improving Quality of Life in Men with Prostate Cancer. Eur. Urol. 2015, 68, 374–383. [Google Scholar] [CrossRef]
- Adam, S.; Feller, A.; Rohrmann, S.; Arndt, V. Health-Related Quality of Life among Long-Term (≥5 Years) Prostate Cancer Survivors by Primary Intervention: A Systematic Review. Health Qual. Life Outcomes 2018, 16, 22. [Google Scholar] [CrossRef]
- Lowrance, W.; Dreicer, R.; Jarrard, D.F.; Scarpato, K.R.; Kim, S.K.; Kirkby, E.; Buckley, D.I.; Griffin, J.C.; Cookson, M.S. Updates to Advanced Prostate Cancer: AUA/SUO Guideline (2023). J. Urol. 2023, 209, 1082–1090. [Google Scholar] [CrossRef]
- Schaeffer, E.M.; Srinivas, S.; Adra, N.; An, Y.; Barocas, D.; Bitting, R.; Bryce, A.; Chapin, B.; Cheng, H.H.; D’Amico, A.V.; et al. Prostate Cancer, Version 4.2023, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2023, 21, 1067–1096. [Google Scholar] [CrossRef] [PubMed]
- Smani, S.; Novosel, M.; Sutherland, R.; Jeong, F.; Jalfon, M.; Marks, V.; Rajwa, P.; Nolazco, J.I.; Washington, S.L.; Renzulli, J.F.; et al. Association between sociodemographic factors and diagnosis of lethal prostate cancer in early life. Urol. Oncol. Semin. Orig. Investig. 2024, 42, 28.e9–28.e28. [Google Scholar] [CrossRef]
- Abodunrin, F.; Adeoye, O.; Masih, D.; Nelson, N.; Silberstein, P.T.; Tupper, C. Late-stage prostate cancer and associated socioeconomic and demographic factors: A National Cancer Database Study. J. Clin. Oncol. 2023, 41 (Suppl. 16), e17115. [Google Scholar] [CrossRef]
- Robinette, J.W.; Charles, S.T.; Gruenewald, T.L. Neighborhood Socioeconomic Status and Health: A Longitudinal Analysis. J. Community Health 2017, 42, 865–871. [Google Scholar] [CrossRef] [PubMed]
- Press, D.J.; Shariff-Marco, S.; Lichtensztajn, D.Y.; Lauderdale, D.; Murphy, A.B.; Inamdar, P.P.; DeRouen, M.C.; Hamilton, A.S.; Yang, J.; Lin, K.; et al. Contributions of Social Factors to Disparities in Prostate Cancer Risk Profiles among Black Men and Non-Hispanic White Men with Prostate Cancer in California. Cancer Epidemiol. Biomarkers Prev. 2022, 31, 404–412. [Google Scholar] [CrossRef]
- Francini, E.; Montagnani, F.; Nuzzo, P.V.; Gonzalez-Velez, M.; Alimohamed, N.S.; Cigliola, A.; Moreno, I.; Rubio, J.; Crivelli, F.; Shaw, G.; et al. Clinical outcomes of abiraterone acetate + prednisone (AA) + bone resorption inhibitors (BRI) versus AA alone as first-line therapy for castration-resistant prostate cancer (CRPC) with bone metastases (BM) in an international multicenter database. J. Clin. Oncol. 2020, 38 (Suppl. 6), 30. [Google Scholar] [CrossRef]
- Nyame, Y.A.; Gulati, R.; Heijnsdijk, E.A.M.; Tsodikov, A.; Mariotto, A.B.; Gore, J.L.; Etzioni, R. The Impact of Intensifying Prostate Cancer Screening in Black Men: A Model-Based Analysis. JNCI J. Natl. Cancer Inst. 2021, 113, 1336–1342. [Google Scholar] [CrossRef]
- Chornokur, G.; Dalton, K.; Borysova, M.E.; Kumar, N.B. Disparities at presentation, diagnosis, treatment, and survival in African American men, affected by prostate cancer. Prostate 2011, 71, 985–997. [Google Scholar] [CrossRef]
- Mahal, B.A.; Chen, Y.-W.; Muralidhar, V.; Mahal, A.R.; Choueiri, T.K.; Hoffman, K.E.; Hu, J.C.; Sweeney, C.J.; Yu, J.B.; Feng, F.Y.; et al. Racial disparities in prostate cancer outcome among prostate-specific antigen screening eligible populations in the United States. Ann. Oncol. 2017, 28, 1098–1104. [Google Scholar] [CrossRef]
- Mahal, B.A.; Chen, Y.; Efstathiou, J.A.; Muralidhar, V.; Hoffman, K.E.; Yu, J.B.; Feng, F.Y.; Beard, C.J.; Martin, N.E.; Orio, P.F.; et al. National trends and determinants of proton therapy use for prostate cancer: A National Cancer Data Base study. Cancer 2016, 122, 1505–1512. [Google Scholar] [CrossRef]
- Orom, H.; Biddle, C.; Underwood, W.; Homish, G.G.; Olsson, C.A. Racial or Ethnic and Socioeconomic Disparities in Prostate Cancer Survivors’ Prostate-specific Quality of Life. Urology 2018, 112, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Du, X.L.; Gao, D.; Li, Z. Incidence trends in prostate cancer among men in the United States from 2000 to 2020 by race and ethnicity, age and tumor stage. Front. Oncol. 2023, 13, 1292577. [Google Scholar] [CrossRef]
- Abudoubari, S.; Bu, K.; Mei, Y.; Maimaitiyiming, A.; An, H.; Tao, N. Prostate cancer epidemiology and prognostic factors in the United States. Front. Oncol. 2023, 13, 1142976. [Google Scholar] [CrossRef]
- Gallagher, B.D.T.; Coughlin, E.C.; Nair-Shalliker, V.; McCaffery, K.; Smith, D.P. Socioeconomic differences in prostate cancer treatment: A systematic review and meta-analysis. Cancer Epidemiol. 2022, 79, 102164. [Google Scholar] [CrossRef] [PubMed]
- Freedland, A.R.; Sanchez Mendez, J.; Liu, L.; Hamilton, A.S.; Zhang, J.; Hwang, A.E.; Ballas, L.; Abreu, A.L.; Deapen, D.; Stern, M.C. Prostate Cancer Disparities in Clinical Characteristics and Survival among Black and Latino Patients Considering Nativity: Findings from the California Cancer Registry. Cancer Epidemiol. Biomarkers Prev. 2024, 33, 1512–1522. [Google Scholar] [CrossRef] [PubMed]
- Rusthoven, C.G.; Carlson, J.A.; Waxweiler, T.V.; Raben, D.; Dewitt, P.E.; Crawford, E.D.; Maroni, P.D.; Kavanagh, B.D. The Impact of Definitive Local Therapy for Lymph Node-Positive Prostate Cancer: A Population-Based Study. Int. J. Radiat. Oncol. 2014, 88, 1064–1073. [Google Scholar] [CrossRef]
- Culp, S.H.; Schellhammer, P.F.; Williams, M.B. Might Men Diagnosed with Metastatic Prostate Cancer Benefit from Definitive Treatment of the Primary Tumor? A SEER-Based Study. Eur. Urol. 2014, 65, 1058–1066. [Google Scholar] [CrossRef]
- Washington, C.G.; Deville, C. Health Disparities and Inequities in the Utilization of Proton Therapy for Prostate Cancer. Cancers 2024, 16, 3837. [Google Scholar] [CrossRef]
- Bradley, C.J.; Kitchen, S.; Bhatia, S.; Bynum, J.; Darien, G.; Lichtenfeld, J.L.; Oyer, R.; Shulman, L.N.; Sheldon, L.K. Policies and Practices to Address Cancer’s Long-Term Adverse Consequences. J. Natl. Cancer Inst. 2022, 114, 1065–1071. [Google Scholar] [CrossRef]
- Krimphove, M.J.; Cole, A.P.; Fletcher, S.A.; Harmouch, S.S.; Berg, S.; Lipsitz, S.R.; Sun, M.; Nabi, J.; Nguyen, P.L.; Hu, J.C.; et al. Evaluation of the contribution of demographics, access to health care, treatment, and tumor characteristics to racial differences in survival of advanced prostate cancer. Prostate Cancer Prostatic Dis. 2019, 22, 125–136. [Google Scholar] [CrossRef]
- Riviere, P.; Luterstein, E.; Kumar, A.; Vitzthum, L.K.; Deka, R.; Sarkar, R.R.; Bryant, A.K.; Bruggeman, A.; Einck, J.P.; Murphy, J.D.; et al. Survival of African American and non-Hispanic white men with prostate cancer in an equal-access health care system. Cancer 2020, 126, 1683–1690. [Google Scholar] [CrossRef] [PubMed]
- Mandel, A.L.; Simhal, R.K.; Shah, Y.B.; Wang, K.R.; Lallas, C.D.; Shah, M.S. Racial Disparities in Diagnosis and Treatment of Depression Associated with Androgen Deprivation Therapy for Prostate Cancer. Urology 2024, 186, 75–80. [Google Scholar] [CrossRef]
- Rock, C.L.; Thomson, C.A.; Sullivan, K.R.; Howe, C.L.; Kushi, L.H.; Caan, B.J.; Neuhouser, M.L.; Bandera, E.V.; Wang, Y.; Robien, K.; et al. American Cancer Society nutrition and physical activity guideline for cancer survivors. CA Cancer J. Clin. 2022, 72, 230–262. [Google Scholar] [CrossRef]
- Andersen, B.L.; Lacchetti, C.; Ashing, K.; Berek, J.S.; Berman, B.S.; Bolte, S.; Dizon, D.S.; Given, B.; Nekhlyudov, L.; Pirl, W.; et al. Management of Anxiety and Depression in Adult Survivors of Cancer: ASCO Guideline Update. J. Clin. Oncol. 2023, 41, 3426–3453. [Google Scholar] [CrossRef] [PubMed]
- Bower, J.E.; Lacchetti, C.; Alici, Y.; Barton, D.L.; Bruner, D.; Canin, B.E.; Escalante, C.P.; Ganz, P.A.; Garland, S.N.; Gupta, S.; et al. Management of Fatigue in Adult Survivors of Cancer: ASCO–Society for Integrative Oncology Guideline Update. J. Clin. Oncol. 2024, 42, 2456–2487. [Google Scholar] [CrossRef]
- Noriega Esquives, B.; Lee, T.K.; Moreno, P.I.; Fox, R.S.; Yanez, B.; Miller, G.E.; Estabrook, R.; Begale, M.J.; Flury, S.C.; Perry, K.; et al. Symptom burden profiles in men with advanced prostate cancer undergoing androgen deprivation therapy. J. Behav. Med. 2022, 45, 366–377. [Google Scholar] [CrossRef] [PubMed]
- Esser, P.; Mehnert-Theuerkauf, A.; Friedrich, M.; Johansen, C.; Brähler, E.; Faller, H.; Härter, M.; Koch, U.; Schulz, H.; Wegscheider, K.; et al. Risk and associated factors of depression and anxiety in men with prostate cancer: Results from a German multicenter study. Psychooncology 2020, 29, 1604–1612. [Google Scholar] [CrossRef]
- Cataldo, J.K.; Paul, S.; Cooper, B.; Skerman, H.; Alexander, K.; Aouizerat, B.; Blackman, V.; Merriman, J.; Dunn, L.; Ritchie, C.; et al. Differences in the symptom experience of older versus younger oncology outpatients: A cross-sectional study. BMC Cancer 2013, 13, 6. [Google Scholar] [CrossRef]
- Peters, L.; Brederecke, J.; Franzke, A.; De Zwaan, M.; Zimmermann, T. Psychological Distress in a Sample of Inpatients with Mixed Cancer—A Cross-Sectional Study of Routine Clinical Data. Front. Psychol. 2020, 11, 591771. [Google Scholar] [CrossRef]
- Penson, D.F.; Stoddard, M.L.; Pasta, D.J.; Lubeck, D.P.; Flanders, S.C.; Litwin, M.S. The association between socioeconomic status, health insurance coverage, and quality of life in men with prostate cancer. J. Clin. Epidemiol. 2001, 54, 350–358. [Google Scholar] [CrossRef]
- Aarts, M.J.; Mols, F.; Thong, M.S.Y.; Louwman, M.W.; Coebergh, J.W.W.; Van De Poll-Franse, L.V. Long-term Prostate Cancer Survivors with Low Socioeconomic Status Reported Worse Mental Health–related Quality of Life in a Population-based Study. Urology 2010, 76, 1224–1230. [Google Scholar] [CrossRef] [PubMed]
- Puri, D.; Pandit, K.; Choi, N.; Rose, B.S.; McKay, R.R.; Bagrodia, A. Striving for Equity: Examining Health Disparities in Urologic Oncology. Cancers 2024, 16, 3559. [Google Scholar] [CrossRef]
- Sud, S.; Gerringer, B.C.; Wacaser, B.S.; Tan, X.; Tatko, S.S.; Royce, T.J.; Wang, A.Z.; Chen, R.C. Underascertainment of Clinically Meaningful Symptoms During Prostate Cancer Radiation Therapy—Does This Vary by Patient Characteristics? Int. J. Radiat. Oncol. 2021, 110, 1122–1128. [Google Scholar] [CrossRef] [PubMed]
- Braga, R.; Araújo, N.; Costa, A.; Lopes, C.; Silva, I.; Correia, R.; Carneiro, F.; Braga, I.; Pacheco-Figueiredo, L.; Oliveira, J.; et al. Association between sociodemographic and clinical features, health behaviors, and health literacy of patients with prostate cancer and prostate cancer prognostic stage. Eur. J. Cancer Prev. 2024, 33, 243–251. [Google Scholar] [CrossRef]
- Sharp, L.; O’Leary, E.; Kinnear, H.; Gavin, A.; Drummond, F.J. Cancer-related symptoms predict psychological wellbeing among prostate cancer survivors: Results from the PiCTure study. Psychooncology 2016, 25, 282–291. [Google Scholar] [CrossRef]
- Khan, S.; Nepple, K.G.; Kibel, A.S.; Sandhu, G.; Kallogjeri, D.; Strope, S.; Grubb, R.; Wolin, K.Y.; Sutcliffe, S. The association of marital status and mortality among men with early-stage prostate cancer treated with radical prostatectomy: Insight into post-prostatectomy survival strategies. Cancer Causes Control 2019, 30, 871–876. [Google Scholar] [CrossRef] [PubMed]
- Knipper, S.; Preisser, F.; Mazzone, E.; Mistretta, F.A.; Palumbo, C.; Tian, Z.; Briganti, A.; Shariat, S.F.; Saad, F.; Tilki, D.; et al. Contemporary analysis of the effect of marital status on survival of prostate cancer patients across all stages: A population-based study. Urol. Oncol. Semin. Orig. Investig. 2019, 37, 702–710. [Google Scholar] [CrossRef]
- Benzo, R.M.; Moreno, P.I.; Fox, R.S.; Silvera, C.A.; Walsh, E.A.; Yanez, B.; Balise, R.R.; Oswald, L.B.; Penedo, F.J. Comorbidity burden and health-related quality of life in men with advanced prostate cancer. Support. Care Cancer 2023, 31, 496. [Google Scholar] [CrossRef]
- Karakiewicz, P.I.; Bhojani, N.; Neugut, A.; Shariat, S.F.; Jeldres, C.; Graefen, M.; Perrotte, P.; Peloquin, F.; Kattan, M.W. The Effect of Comorbidity and Socioeconomic Status on Sexual and Urinary Function and on General Health-Related Quality of Life in Men Treated with Radical Prostatectomy for Localized Prostate Cancer. J. Sex. Med. 2008, 5, 919–927. [Google Scholar] [CrossRef]
- Prasad, S.M.; Eggener, S.E.; Lipsitz, S.R.; Irwin, M.R.; Ganz, P.A.; Hu, J.C. Effect of Depression on Diagnosis, Treatment, and Mortality of Men with Clinically Localized Prostate Cancer. J. Clin. Oncol. 2014, 32, 2471–2478. [Google Scholar] [CrossRef]
- Hall, H.I.; Satariano, W.A.; Thompson, T.; Ragland, K.E.; Van Den Eeden, S.K.; Selvin, S. Initial treatment for prostate carcinoma in relation to comorbidity and symptoms. Cancer 2002, 95, 2308–2315. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.C.; Basak, R.; Meyer, A.-M.; Kuo, T.-M.; Carpenter, W.R.; Agans, R.P.; Broughman, J.R.; Reeve, B.B.; Nielsen, M.E.; Usinger, D.S.; et al. Association Between Choice of Radical Prostatectomy, External Beam Radiotherapy, Brachytherapy, or Active Surveillance and Patient-Reported Quality of Life Among Men with Localized Prostate Cancer. JAMA 2017, 317, 1141–1150. [Google Scholar] [CrossRef]
- De, B.; Pasalic, D.; Barocas, D.A.; Wallis, C.J.D.; Huang, L.-C.; Zhao, Z.; Koyama, T.; Tang, C.; Goodman, M.; Hamilton, A.S.; et al. Patient-reported Outcomes After External Beam Radiotherapy with Low Dose Rate Brachytherapy Boost vs Radical Prostatectomy for Localized Prostate Cancer: Five-year Results From a Prospective Comparative Effectiveness Study. J. Urol. 2022, 208, 1226–1239. [Google Scholar] [CrossRef]
- Lehto, U.S.; Tenhola, H.; Taari, K.; Aromaa, A. Patients’ perceptions of the negative effects following different prostate cancer treatments and the impact on psychological well-being: A nationwide survey. Br. J. Cancer 2017, 116, 864–873. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.; Shim, S.R.; Kim, C.H. Changes in Beck Depression Inventory scores in prostate cancer patients undergoing androgen deprivation therapy or prostatectomy. PLoS ONE 2020, 15, e0234264. [Google Scholar] [CrossRef]
- Bensley, J.G.; Dhillon, H.M.; Evans, S.M.; Evans, M.; Bolton, D.; Davis, I.D.; Dodds, L.; Frydenberg, M.; Kearns, P.; Lawrentschuk, N.; et al. Self-reported lack of energy or feeling depressed 12 months after treatment in men diagnosed with prostate cancer within a population-based registry. Psychooncology 2022, 31, 496–503. [Google Scholar] [CrossRef]
- Mahal, B.A.; Alshalalfa, M.; Kensler, K.H.; Chowdhury-Paulino, I.; Kantoff, P.; Mucci, L.A.; Schaeffer, E.M.; Spratt, D.; Yamoah, K.; Nguyen, P.L.; et al. Racial Differences in Genomic Profiling of Prostate Cancer. N. Engl. J. Med. 2020, 383, 1083–1085. [Google Scholar] [CrossRef]
- Bologna, E.; Ditonno, F.; Licari, L.C.; Franco, A.; Manfredi, C.; Mossack, S.; Pandolfo, S.D.; De Nunzio, C.; Simone, G.; Leonardo, C.; et al. Tissue-Based Genomic Testing in Prostate Cancer: 10-Year Analysis of National Trends on the Use of Prolaris, Decipher, ProMark, and Oncotype DX. Clin. Pract. 2024, 14, 508–520. [Google Scholar] [CrossRef] [PubMed]
- Spratt, D.E.; Zhang, J.; Santiago-Jiménez, M.; Dess, R.T.; Davis, J.W.; Den, R.B.; Dicker, A.P.; Kane, C.J.; Pollack, A.; Stoyanova, R.; et al. Development and Validation of a Novel Integrated Clinical-Genomic Risk Group Classification for Localized Prostate Cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2018, 36, 581–590. [Google Scholar] [CrossRef]
- Spratt, D.E.; Yousefi, K.; Deheshi, S.; Ross, A.E.; Den, R.B.; Schaeffer, E.M.; Trock, B.J.; Zhang, J.; Glass, A.G.; Dicker, A.P.; et al. Individual Patient-Level Meta-Analysis of the Performance of the Decipher Genomic Classifier in High-Risk Men After Prostatectomy to Predict Development of Metastatic Disease. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2017, 35, 1991–1998. [Google Scholar] [CrossRef]
- Yuan, J.; Kensler, K.H.; Hu, Z.; Zhang, Y.; Zhang, T.; Jiang, J.; Xu, M.; Pan, Y.; Long, M.; Montone, K.T.; et al. Integrative comparison of the genomic and transcriptomic landscape between prostate cancer patients of predominantly African or European genetic ancestry. PLoS Genet. 2020, 16, e1008641. [Google Scholar] [CrossRef]
- Annala, M.; Vandekerkhove, G.; Khalaf, D.; Taavitsainen, S.; Beja, K.; Warner, E.W.; Sunderland, K.; Kollmannsberger, C.; Eigl, B.J.; Finch, D.; et al. Circulating Tumor DNA Genomics Correlate with Resistance to Abiraterone and Enzalutamide in Prostate Cancer. Cancer Discov. 2018, 8, 444–457. [Google Scholar] [CrossRef] [PubMed]
- Goodall, J.; Mateo, J.; Yuan, W.; Mossop, H.; Porta, N.; Miranda, S.; Perez-Lopez, R.; Dolling, D.; Robinson, D.R.; Sandhu, S.; et al. Circulating Cell-Free DNA to Guide Prostate Cancer Treatment with PARP Inhibition. Cancer Discov. 2017, 7, 1006–1017. [Google Scholar] [CrossRef] [PubMed]
- Gallicchio, L.; Tonorezos, E.; de Moor, J.S.; Elena, J.; Farrell, M.; Green, P.; Mitchell, S.A.; Mollica, M.A.; Perna, F.; Saiontz, N.G.; et al. Evidence Gaps in Cancer Survivorship Care: A Report From the 2019 National Cancer Institute Cancer Survivorship Workshop. J. Natl. Cancer Inst. 2021, 113, 1136–1142. [Google Scholar] [CrossRef] [PubMed]
- Kline, R.M.; Arora, N.K.; Bradley, C.J.; Brauer, E.R.; Graves, D.L.; Lunsford, N.B.; McCabe, M.S.; Nasso, S.F.; Nekhlyudov, L.; Rowland, J.H.; et al. Long-Term Survivorship Care After Cancer Treatment—Summary of a 2017 National Cancer Policy Forum Workshop. J. Natl. Cancer Inst. 2018, 110, 1300–1310. [Google Scholar] [CrossRef]
- Leader, A.E.; Rebbeck, T.R.; Oh, W.K.; Patel, A.V.; Winer, E.P.; Bailey, L.O.; Gomella, L.G.; Lumpkins, C.Y.; Garraway, I.P.; Aiello, L.B.; et al. Adaptation of the socioecological model to address disparities in engagement of Black men in prostate cancer genetic testing. BMC Public Health 2024, 24, 2533. [Google Scholar] [CrossRef]
- Stevens Hobbs, K.; Hall, L.L.; Farrington, T.; Moore, A.; Barnett, L.; Aguilera-Funez, N.; Crawford, K.; George, J. Advancing equity in prostate cancer outcomes using community-facing navigation in the cancer continuum of care. J. Clin. Oncol. 2022, 40 (Suppl. 28), 120. [Google Scholar] [CrossRef]
- Stafford, H.S.; Saltzstein, S.L.; Shimasaki, S.; Sanders, C.; Downs, T.M.; Robins Sadler, G. Racial/Ethnic and Gender Disparities in Renal Cell Carcinoma Incidence and Survival. J. Urol. 2008, 179, 1704–1708. [Google Scholar] [CrossRef]
- Prostate Cancer Treatment Program. Available online: https://www.dhcs.ca.gov/services/cancer/PCTP/Pages/default.aspx (accessed on 20 December 2024).
- Alfano, C.M.; Leach, C.R.; Smith, T.G.; Miller, K.D.; Alcaraz, K.I.; Cannady, R.S.; Wender, R.C.; Brawley, O.W. Equitably improving outcomes for cancer survivors and supporting caregivers: A blueprint for care delivery, research, education, and policy. CA Cancer J. Clin. 2019, 69, 35–49. [Google Scholar] [CrossRef]
- Thavaseelan, S.; Burnett, A.L.; Chang, S.; Davies, B.; Dy, G.; Greene, K.; Griebling, T.L.; Santiago-Lastra, Y.; McIntire, L.L.; McNeil, B.; et al. AUA Diversity & Inclusion Task Force: Blueprint and Process for Justice, Equity, Diversity and Inclusion. J. Urol. 2022, 208, 498–504. [Google Scholar] [CrossRef]
- Polite, B.N.; Adams-Campbell, L.L.; Brawley, O.W.; Bickell, N.; Carethers, J.M.; Flowers, C.R.; Foti, M.; Gomez, S.L.; Griggs, J.J.; Lathan, C.S.; et al. Charting the Future of Cancer Health Disparities Research: A Position Statement From the American Association for Cancer Research, the American Cancer Society, the American Society of Clinical Oncology, and the National Cancer Institute. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2017, 35, 3075–3082. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).