

Potential Impact of Screening Examinations on Prognosis of De Novo Malignancies in Adult Patients After Liver Transplantation

 , , and
, , and
Abstract
1. Introduction
2. Patients and Methods
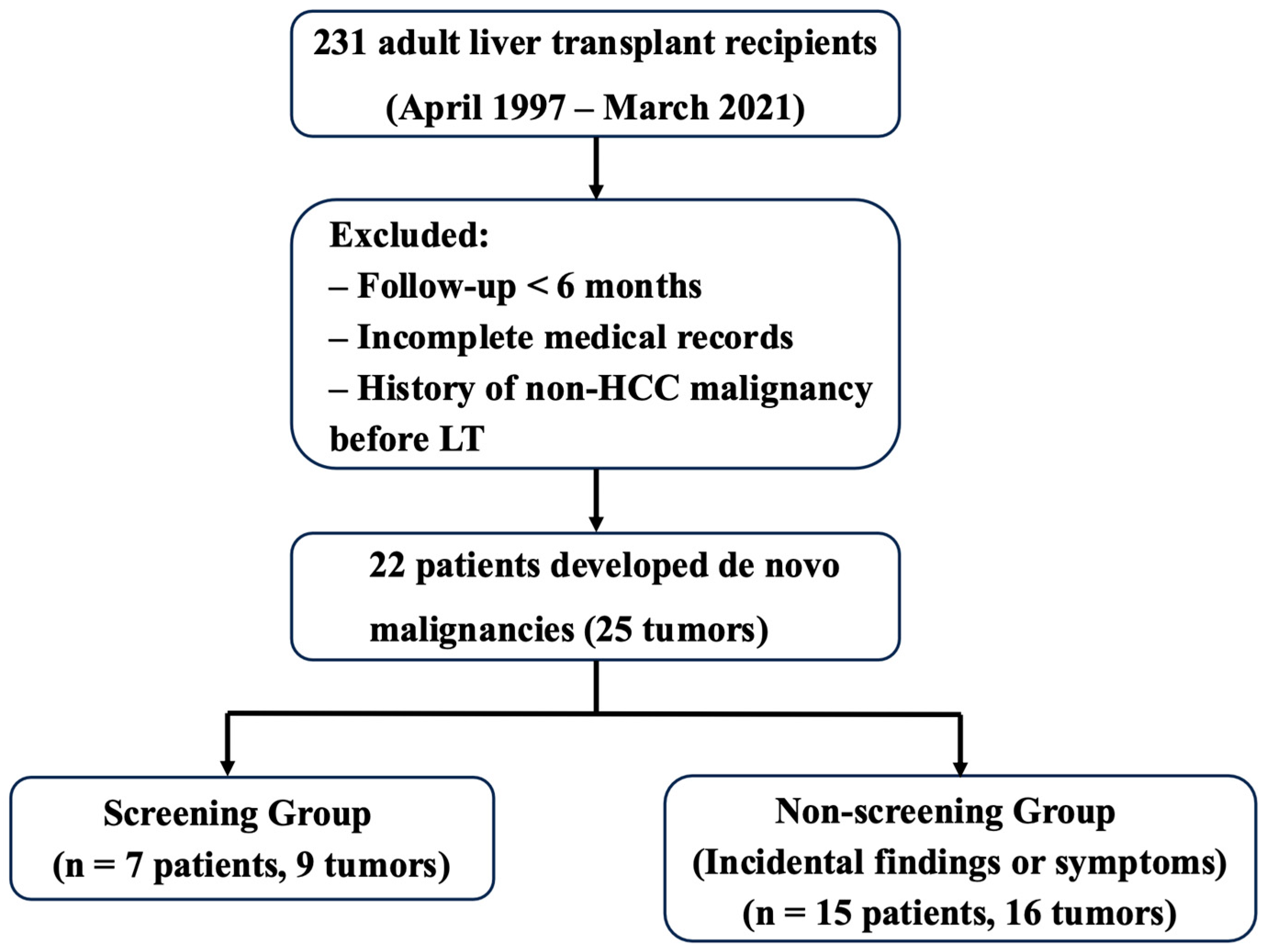
2.1. Patient Selection
2.2. Posttransplant Cancer Surveillance
2.3. Patient Classification
2.4. Data Collection and Endpoints
2.5. Statistical Analysis
3. Results
3.1. DNM After LT
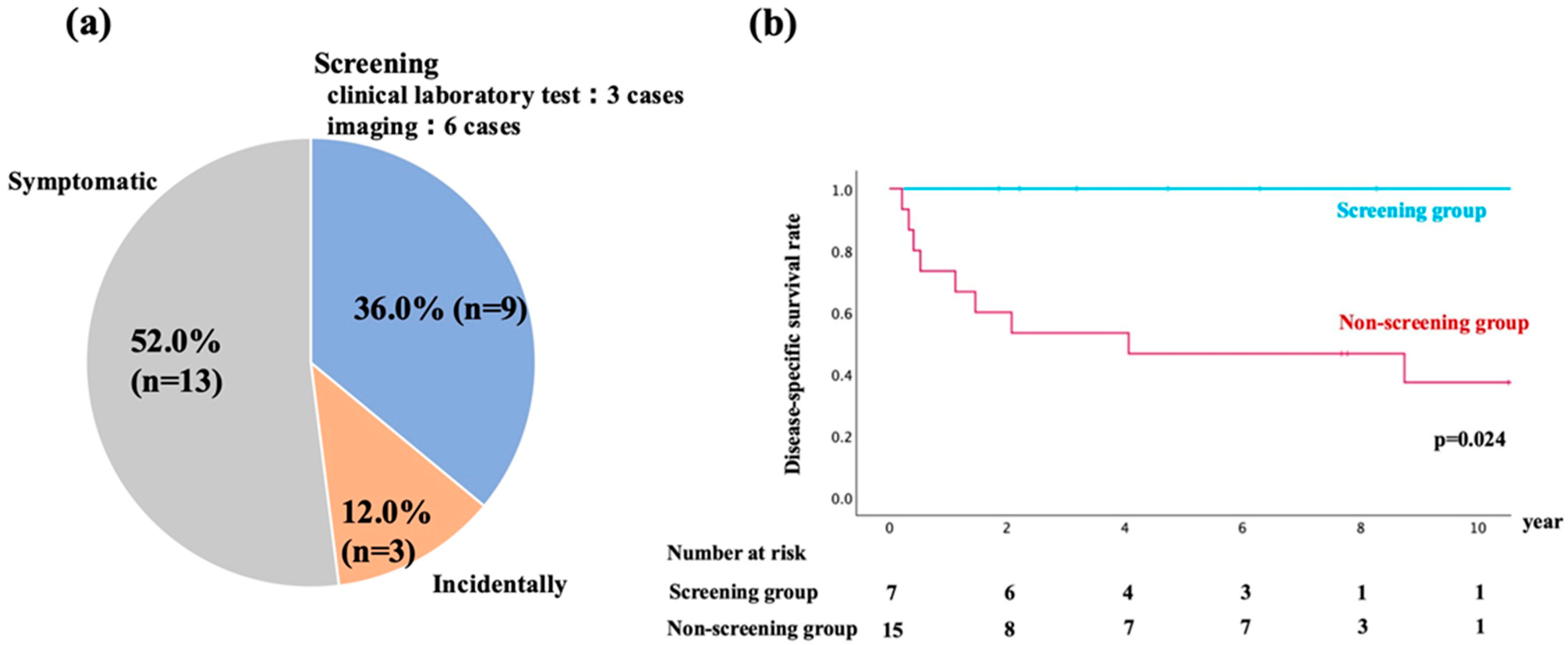
3.2. Details for Detection of DNM
3.3. Survival Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liu, Z.N.; Wang, W.T.; Yan, L.N. Liver Surgery Group. De novo malignancies after liver transplantation with 14 cases at a single center. Transpl. Proc. 2015, 47, 2483–2487. [Google Scholar] [CrossRef] [PubMed]
- Michael, R.C. Roadmap for Improving Patient and Graft Survival in the Next 10 Years. Liver Transpl. 2016, 22, S71–S78. [Google Scholar]
- Jimenez-Romero, C.; Manrique Municio, A.; Marques Medina, E.; Colina, F.; Domene, P.O.; Sanz, R.G.; Meneu Diaz, J.C.; Abradelo de Usera, M.; Moreno Elola, A.; Moreno Gonzalez, E. Incidence of de novo nonmelanoma skin tumors after liver transplantation for alcoholic and nonalcoholic liver diseases. Transpl. Proc. 2006, 38, 2505–2507. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.C.; Ufere, N.N.; Bucuvalas, J.C. Liver transplant survivor-ship. Liver Transpl. 2020, 26, 1030e3. [Google Scholar] [CrossRef]
- Kim, W.R.; Lake, J.R.; Smith, J.M.; Schladt, D.P.; Skeans, M.A.; Noreen, S.M.; M Robinson, A.; Miller, E.; Snyder, J.J.; Israni, A.K.; et al. OPTN/SRTR2017Annual Data Report: Liver. Am. J. Transpl. 2019, 19 (Suppl. 2), e184–e283. [Google Scholar] [CrossRef]
- Jain, A.; Fiaz, O.; Sheikh, B.; Sharma, R.; Safadjou, S.; Kashyap, R.; Bryan, L.; Batzold, P.; Orloff, M. Recurrent nonhepatic and de novo malignancies after liver transplantation. Transplantation 2009, 88, 706–710. [Google Scholar] [CrossRef]
- Yoshida, E.M.; Steinbrecher, U.P.; Donovan, J.A.; Erb, S.R.; Esrason, K.T.; Medkiff, K.A.; Pruthi, J.; Fong, T.-L. Analysis of causes of death in liver transplant recipients who survived more than 3 years. Liver Transpl. 2001, 7, 811–815. [Google Scholar]
- Sérée, O.; Altieri, M.; Guillaume, E.; De Mil, R.; Lobbedez, T.; Robinson, P.; Segol, P.; Salamé, E.; Abergel, A.; Boillot, O.; et al. Longterm risk of solid organ de novo malignancies after liver transplantation: A French national study on 11,226 patients. Liver Transpl. 2018, 24, 1425–1436. [Google Scholar] [CrossRef]
- Pillai, A.A. Management of de novo malignancies after liver transplantation. Transpl. Rev. 2015, 29, 38–41. [Google Scholar] [CrossRef]
- Engels, E.A.; Pfeiffer, R.M.; Fraumeni, J.F., Jr.; Kasiske, B.L.; Israni, A.K.; Snyder, J.J.; Wolfe, R.A.; Goodrich, N.P.; Bayakly, A.R.; Clarke, C.A.; et al. Spectrum of cancer risk among US solid organ transplant recipients. JAMA. 2011, 306, 1891–1901. [Google Scholar] [CrossRef]
- Herrero, J.I. De novo malignancies following liver transplantation: Impact and recommendations. Liver Transpl. 2009, 15 (Suppl. 2), S90–S94. [Google Scholar] [CrossRef] [PubMed]
- Anisha, T.; Sanjiv, S.; Narendra, S.; Saha, S.; Rastogi, A.; Bhangui, P.; Saraf, N.; Srinivasan, T.; Yadav, S.K.; Gautam, D.; et al. De Novo Malignancy After Living Donor Liver Transplantation: A Large Volume Experience. J. Clin. Exp. Hepatol. 2020, 10, 448–452. [Google Scholar]
- Colmenero, J.; Tabrizian, P.; Bhangui, P.; Pinato, D.J.; Rodriguez-Per-alvarez, M.L.; Sapisochin, G.; Bhoori, S.; Pascual, S.; Senzolo, M.; Al-Adra, D.; et al. De Novo malignancy after liver trans- plantation: Risk assessment, prevention, and management-guidelines from the ILTS-SETH consensus conference. Transplantation 2022, 106, e30–e45. [Google Scholar] [CrossRef] [PubMed]
- Tajima, T.; Hata, K.; Tanaka, K.; Iyama, N.; Kusakabe, J.; Kageyama, S.; Ogawa, E.; Okamoto, T.; Haga, H.; Uemoto, S.; et al. Chronological alterations in de novo malignancies after living-donor liver transplantation: A cohort study of 1781 recipients using annual comparisons of standardized incidence ratios. J. Hepato-Biliary-Pancreat. Sci. 2024, 31, 455–467. [Google Scholar] [CrossRef]
- Herrero, J.I.; Lorenzo, M.; Quiroga, J.; Sangro, B.; Pardo, F.; Rotellar, F.; Alvarez-Cienfuegos, J.; Prieto, J. De novo neoplasia after liver transplantation: An analysis of risk factors and influence on survival. Liver Transpl. 2005, 11, 89. [Google Scholar] [CrossRef]
- Tanaka, T.; Michael, D.V. Decision tree analysis to stratify risk of de novo non-melanoma skin cancer following liver transplantation. J. Cancer Res. Clin. Oncol. 2018, 144, 607–615. [Google Scholar] [CrossRef]
- Kaneko, J.; Sugawara, Y.; Tamura, S.; Aoki, T.; Sakamoto, Y.; Hasegawa, K.; Yamashiki, N.; Kokudo, N. De novo malig- nancies after adult-to-adult living-donor liver transplantation with a malignancy surveillance program: Comparison with a Japanese population-based study. Transplantation 2013, 95, 1142e7. [Google Scholar] [CrossRef]
- Mizuno, S.; Hayasaki, A.; Ito, T.; Fujii, T.; Iizawa, Y.; Kato, H.; Murata, Y.; Tanemura, A.; Kuriyama, N.; Azumi, Y.; et al. De novo Malignancy Following Adult-to-Adult Living Donor Liver Transplantation Focusing on Posttransplantation Lymphoproliferative Disorder. Transpl. Proc. 2018, 50, 2699–2704. [Google Scholar] [CrossRef]
- Kobayashi, T.; Miura, K.; Ishikawa, H.; Sakata, J.; Takizawa, K.; Hirose, Y.; Toge, K.; Saito, S.; Abe, S.; Kawachi, Y.; et al. Malignancy After Living Donor Liver Transplantation. Transpl. Proc. 2024, 56, 660–666. [Google Scholar] [CrossRef]
- Masuda, Y.; Mita, A.; Ohno, Y.; Kubota, K.; Notake, T.; Shimizu, A.; Soejima, Y. De novo malignancy after adult-to-adult living donor liver trans- plantation: A single-center long-term experience. Transpl. Proc. 2023, 55, 952–955. [Google Scholar] [CrossRef]
- Finkenstedt, A.; Graziadei, I.W.; Oberaigner, W.; Hilbe, W.; Nachbaur, K.; Mark, W.; Margreiter, R.; Vogel, W. Extensive Surveillance Promotes Early Diagnosis and Improved Survival of De Novo Malignancies in Liver Transplant Recipients. Am. J. Transpl. 2009, 9, 2355–2361. [Google Scholar] [CrossRef] [PubMed]
- Kitahara, C.M.; Sosa, J.A. The changing incidence of thyroid cancer. N. Engl. J. Med. 2016, 375, 1057–1067. [Google Scholar] [CrossRef] [PubMed]
- Tajima, T.; Hata, K.; Haga, H.; Nishikori, M.; Umeda, K.; Kusakabe, J.; Miyauchi, H.; Okamoto, T.; Ogawa, E.; Sonoda, M.; et al. Post-transplant Lymphoproliferative Disorders After Liver Transplantation: A Retrospective Cohort Study Including 1954 Transplants. Liver Transpl. 2021, 27, 1165–1180. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Screening Modality | Details | Frequency |
|---|---|---|
| Physical examination | General physical and symptom-based assessment | Every 3 months |
| Blood tests | Cell blood counts and blood chemistry, including tumor markers | Every 3 months |
| Imaging | Chest and abdominal CT | Annually |
| Endoscopy | EGD and CS | Snnually |
| EBV-PCR | Not routinely performed | Unavailable |
| Sex | Age, y | Etiology for LT | Smoking History | Type of DNM | Duration from LT to DNM, mo | Screening Examination | Curative Treatment for DNM | Recurrence of DNM | Duration After DNM, mo | Status |
|---|---|---|---|---|---|---|---|---|---|---|
| F | 71 | HCV/HCC | no | gastric | 121 | EGD | yes | no | 75 | alive |
| M | 66 | HCC | yes | laryngeal | 84 | EGD | yes | no | 99 | alive |
| F ※ | 54 | PBC | yes | PTLD (Monomorphic/LN) | 30 | EGD | yes | no | 133 | alive |
| M | 64 | ALD | yes | colorectal | 78 | EGD | yes | no | 96 | alive |
| F | 71 | HCV/HCC | no | breast | 107 | CT | yes | no | 22 | alive |
| F ※※ | 65 | ALD | yes | lung | 142 | CT | yes | no | 91 | death of other diseases |
| F ※ | 62 | PBC | no | colorectal | 136 | FOB | yes | no | 26 | alive |
| F | 58 | Cryptogenic | no | gastric | 6 | BT | yes | no | 38 | death of other diseases |
| M | 72 | HBV/HCC | no | prostate | 179 | BT | yes | no | 57 | death of other diseases |
| Sex | Age, y | Etiology for LT | Smoking History | Type of DNM | Duration from LT to DNM, mo | Diagnostic Opportunity | Curative Treatment for DNM | Distant Metastasis at Diagnosis | Regular Screening Performed | Duration After DNM, mo | Status |
|---|---|---|---|---|---|---|---|---|---|---|---|
| F | 39 | Caroli | unknown | PTLD (unknown/GI) | 114 | hematochezia | yes | no | unknown | 158 | alive |
| M | 65 | ALD | yes | PTLD (polymorphic/LN) | 156 | weakness | yes | no | no | 10 | alive |
| F | 64 | FH | yes | PTLD (Monomorphic/LN) | 111 | neck mass | yes | no | no | 126 | alive |
| F | 46 | PSC | unknown | PTLD (unknown/LN) | 121 | slight fever | yes | no | unknown | 154 | alive |
| F | 51 | FH | no | breast | 105 | incidentally | yes | no | yes | 92 | alive |
| M | 67 | HBV | no | renal | 143 | incidentally | yes | no | no | 93 | alive |
| M ※※※ | 66 | PBC | yes | skin | 148 | skin symptoms | yes | no | no | 48 | alive |
| F ※※ | 60 | ALD | yes | laryngeal | 92 | hypoglossalnerve paralysis | yes | no | yes | 121 | alive |
| F | 69 | HCV/ HCC | yes | unknown primary | 58 | incidentally | no | yes | no | 7 | death of cancer |
| F | 23 | BA | unknown | PTLD (Monomorphic/GI) | 4 | hematochezia | no | no | yes | 3 | death of cancer |
| F | 68 | HCV | no | PTLD (Monomorphic/LN) | 118 | dehydration | no | no | yes | 5 | death of cancer |
| M | 50 | HCV | unknown | PTLD (unknown/LN) | 5 | incidentally | no | no | yes | 6 | death of cancer |
| M ※※※ | 70 | PBC | yes | lung | 194 | pleural effusion | no | yes | no | 3 | death of cancer |
| M | 65 | HBV | unknown | thyroid | 50 | buttock pain | no | yes | yes | 18 | death of cancer |
| F | 29 | FH | no | thyroid | 31 | neck mass palpable | yes | no | no | 104 | death of other diseases |
| M | 60 | ALD | yes | cholangio-carcinoma | 6 | incidentally | no | no | yes | 4 | death of other diseases |
| Screening Group (n = 7) | Non-Screening Group (n = 15) | p Value | |
|---|---|---|---|
| Male sex, n (%) | 3 (42.9) | 6 (40.0) | 0.452 |
| Age, y (median, range) | 66 (54–72) | 55 (23–70) | 0.075 |
| Time from LT to malignancy, mo (median, range) | 107 (30–179) | 108 (4–195) | 0.498 |
| MST, year | not reached | 4.1 | 0.024 |
| Distant metastasis at diagnosis, n (%) | 0 (0) | 2 (13.3) | 0.167 |
| Curative treatment for DNM, n (%) | 7 (100) | 9 (60.0) | 0.026 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uemura, S.; Hasegawa, Y.; Obara, H.; Kitago, M.; Yagi, H.; Abe, Y.; Hori, S.; Tanaka, M.; Nakano, Y.; Kitagawa, Y. Potential Impact of Screening Examinations on Prognosis of De Novo Malignancies in Adult Patients After Liver Transplantation. Livers 2025, 5, 26. https://doi.org/10.3390/livers5020026
Uemura S, Hasegawa Y, Obara H, Kitago M, Yagi H, Abe Y, Hori S, Tanaka M, Nakano Y, Kitagawa Y. Potential Impact of Screening Examinations on Prognosis of De Novo Malignancies in Adult Patients After Liver Transplantation. Livers. 2025; 5(2):26. https://doi.org/10.3390/livers5020026
Chicago/Turabian StyleUemura, Sho, Yasushi Hasegawa, Hideaki Obara, Minoru Kitago, Hiroshi Yagi, Yuta Abe, Shutaro Hori, Masayuki Tanaka, Yutaka Nakano, and Yuko Kitagawa. 2025. "Potential Impact of Screening Examinations on Prognosis of De Novo Malignancies in Adult Patients After Liver Transplantation" Livers 5, no. 2: 26. https://doi.org/10.3390/livers5020026
APA StyleUemura, S., Hasegawa, Y., Obara, H., Kitago, M., Yagi, H., Abe, Y., Hori, S., Tanaka, M., Nakano, Y., & Kitagawa, Y. (2025). Potential Impact of Screening Examinations on Prognosis of De Novo Malignancies in Adult Patients After Liver Transplantation. Livers, 5(2), 26. https://doi.org/10.3390/livers5020026