1. Introduction
Obesity has reached pandemic proportions globally, with rapidly rising prevalence in developing nations, including India [
1]. The World Health Organization (WHO) defines obesity as having a body mass index (BMI) of 30 kg/m
2 or higher [
2]. BMI and waist circumference (WC) are simple indices commonly used to classify overweight and obesity in adults and predict obesity-related health risks [
3]. Obesity is a chronic disorder that is associated with the development of non-communicable diseases. In fact, increased BMI is a major risk factor for diabetes, cardiovascular diseases, non-alcoholic fatty liver disease (NAFLD), non-alcoholic steatohepatitis (NASH)/metabolic dysfunction-associated steatohepatitis (MASH), some cancers, and many other non-communicable diseases and plays a role in increasing premature death and disability in adulthood [
4,
5].
In 2022, an estimated 13% of the global adult population, approximately 890 million individuals, were classified as obese. This number is projected to exceed 1 billion by 2030. If current trends persist, the number of obese adults is expected to grow from 810 million in 2020 to 1.53 billion by 2035 and reach 3.80 billion by 2050 [
2]. The substantial burden of obesity in India was confirmed by a recent publication from the Indian Council of Medical Research (ICMR)-India Diabetes (INDIAB) study, which documented that there are an alarming 254 million and 351 million adults with generalized and abdominal obesity, respectively, in India [
6].
Pathophysiologically, the obese phenotype arises from a complex interplay of positive energy balance, adipocyte hypertrophy and hyperplasia, ectopic lipid deposition, and impaired energy expenditure. At the cellular level, defective mitochondrial fatty-acid oxidation (FAO) in skeletal muscle, liver, and adipose tissue is increasingly recognized as a mechanistic nexus that couples lipid oversupply to insulin resistance, oxidative stress, and impaired metabolic flexibility. Augmentation of mitochondrial FAO, therefore, constitutes a biologically plausible strategy to shift substrate utilization away from lipid storage toward oxidative disposal [
7].
It has also been reported that adults with obesity spend double the annual medical care costs than those with a healthy body mass index (BMI < 25 kg/m
2). Furthermore, the greater the costs, higher the class of obesity [
8]. There are different approaches for dealing with obesity, which may include lifestyle management, diet therapy, physical activity, and behavioral modification, and may also need pharmacotherapy or surgery based on the level of risk [
9]. Although there are various dietary supplements for weight management on the market, there is insufficient evidence regarding their effectiveness [
10,
11]. L-Carnitine is one of the supplements that claims to be efficacious for weight loss [
12].
Carnitine or beta-hydroxy-gamma-methyl ammonium butyrate is a hydrophilic molecule that consists of two amino acids: lysine and methionine [
4]. L-Carnitine is necessary for mitochondrial transport and the metabolism of long-chain fatty acids, thus for myocardial energetic metabolism. Fatty acids cross mitochondrial membranes as acylcarnitine derivatives to enter pathways for oxidation, acylation, chain shortening, or chain elongation–desaturation. L-Carnitine-dependent fatty acid transport plays a central role in lipid metabolism. Supplementation has been associated with enhanced fatty acid utilization and reductions in circulating triglyceride levels in selected populations [
13]. These mechanistic attributes render L-Carnitine a credible adjunct to lifestyle interventions aimed at reducing adiposity and improving body composition.
Clinical evidence for L-Carnitine’s efficacy in weight management is heterogeneous. A systematic review and meta-analysis of 37 randomized controlled clinical trials with dose–response analysis showed a modest reduction in body weight, BMI, and fat mass, especially among adults with overweight/obesity [
14]. Studies have reported several benefits of Carnitine supplementation, including reducing inflammation, improving lipid profile, improving quality of life, antioxidant effects, and weight control [
4]. Recent randomized investigations employing L-Carnitine L-Tartrate formulations have expanded safety and pharmacodynamic characterization in humans, but clinical endpoints in obesity-specific cohorts remain incompletely defined and frequently underpowered [
15].
While randomized controlled trials and meta-analyses have evaluated the effects of L-Carnitine supplementation on body weight and metabolic parameters, evidence from real-world clinical settings remains limited. In particular, Indian clinical data on L-carnitine use in obesity are sparse, with only a few small interventional and observational studies available. This highlights a gap in context-specific, practice-based evidence describing the use of L-Carnitine formulations in routine clinical care.
In real-world practice, where adherence, behavioral variability, and concurrent lifestyle modifications are less controlled than in clinical trials, observed outcomes may differ from those reported under experimental conditions. Moreover, integrated real-world data encompassing anthropometric measures, body composition, and patient-reported quality-of-life outcomes remain scarce. The present study was therefore designed to provide exploratory real-world observational data on these outcomes following initiation of L-Carnitine L-Tartrate supplementation in Indian adults with overweight and obesity.
2. Materials and Methods
2.1. Study Design and Settings
This was a prospective, single-center, uncontrolled observational clinical study conducted in a real-world outpatient setting in Redkar Hospital and Research Centre. No randomization, blinding, or comparator (placebo or active) group was used. Participants newly initiated on L-Carnitine L-Tartrate as part of routine care were followed longitudinally over an 8-week period, reflecting routine clinical practice.
As this study was designed as a prospective real-world observational investigation intended to evaluate outcomes associated with routine clinical use of L-Carnitine L-Tartrate, a placebo or untreated control group was not incorporated. Participants were enrolled after initiation of supplementation as part of standard physician-directed care in routine practice settings. The primary objective was to generate exploratory, practice-based evidence reflecting real-world treatment patterns, adherence, and patient outcomes rather than to establish comparative efficacy under controlled experimental conditions. Therefore, the study employed a single-arm observational design without randomization or placebo control.
The study was conducted between 27 October 2025 and 26 December 2025. The scheduling of visits consisted of four points: Baseline/Visit 1 (Day 0), Visit 2 at Week 4 (Day 28), Visit 3 at Week 6 (Day 42), and Visit 4 at Week 8 (Day 56), as shown in
Figure 1.
2.2. Ethical Approval and Regulatory Compliance
The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki, the International Conference on Harmonisation–Good Clinical Practice (ICH–GCP) guidelines, and applicable Indian regulatory requirements, including ICMR and Indian GCP guidelines, and the New Drugs and Clinical Trials Rules 2019 issued by the Ministry of Health and Family Welfare.
Prior approval from an Institutional Ethics Committee (IEC) was obtained for the study protocol, informed consent process, case report forms, and all relevant study documents before initiation of the study.
2.3. Study Population
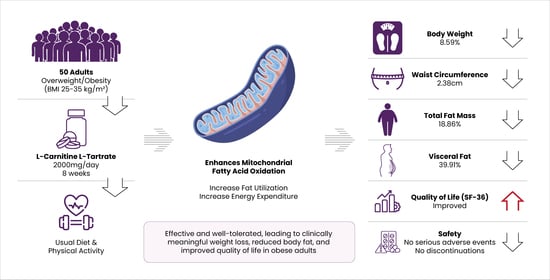
Eligible participants comprised adult men and women aged 21–65 years with overweight or class I obesity, defined by a BMI ranging from 25 to 35 kg/m2. Participants were required to be newly initiated on FAST&UP Lean Body Effervescent Tablets and agreeable to continue standard physician-advised lifestyle measures, including diet and physical activity, throughout the study period. The observed outcomes were achieved without the implementation of a structured dietary program, predefined caloric restriction, or supervised exercise regimen, reflecting the potential applicability of the intervention under real-world lifestyle conditions. While adherence to lifestyle advice was encouraged, formal quantitative monitoring of dietary intake and physical activity was not incorporated into the study design.
Additional eligibility requirements included willingness to consume the study product strictly as prescribed, attend all scheduled follow-up visits, adhere to protocol-mandated procedures, and provide written informed consent voluntarily before study enrollment. The inclusion criteria were designed to capture a broadly representative adult population receiving supplementation in routine practice rather than a highly selected or clinically distinct subgroup.
Participants were excluded if they were pregnant or lactating, had documented hypersensitivity to L-Carnitine L-Tartrate or any formulation excipients, or had clinically significant hepatic dysfunction, severe renal impairment, or hypertension. Participants with obesity due to known hormonal changes (hypothyroidism, polycystic ovary syndrome, or type 2 diabetes mellitus) were not eligible. Further exclusion criteria encompassed recent use (within 2 months before screening) of weight-loss supplements or pharmacotherapies, hormonal treatments, pro-/pre-/synbiotics, multivitamins, antacids, antibiotics, corticosteroids, or laxatives, as well as concurrent or recent participation in another interventional weight-management trial. Participants who had followed a structured therapeutic diet within the 3 months preceding study inclusion were also excluded.
2.4. Recruitment Process
Participants were recruited from the obesity and lifestyle-related disorders outpatient clinic at Redkar Hospital and Research Centre between 27 October 2025 and 26 December 2025. During this period, adults attending the clinic who met the age and BMI eligibility criteria and were newly initiated on L-Carnitine L-Tartrate as part of routine care were screened for inclusion. Recruitment followed a consecutive sampling approach, whereby all eligible and consenting patients presenting during the study period were invited to participate. A total of 50 participants were screened, all of whom met the inclusion and exclusion criteria, provided written informed consent, and were enrolled; thus, 50 participants comprised both the safety and effectiveness analysis sets.
2.5. Study Product
The investigational product was FAST&UP Lean Body, an oral effervescent formulation containing L-Carnitine L-Tartrate (1000 mg/tablet). Participants were instructed to consume two tablets daily (total daily dose: 2000 mg) dissolved in 250 mL of water, 30 min before physical activity, administered daily for 8 weeks.
2.6. Outcome Measures
The primary outcome was the mean absolute and percentage change in body weight from baseline to follow-up visits, measured using a calibrated digital weighing scale. Absolute and percentage changes were calculated using standardized formulae.
Secondary outcomes included comprehensive anthropometric, body composition, quality of life, satisfaction, compliance, and safety assessments.
Changes in BMI, waist circumference, hip circumference, and waist–hip ratio (WHR) were determined from baseline to follow-up using standardized measurement techniques.
Detailed body composition parameters, including lean body mass, fat (%), body fat weight (kg), skeletal muscle mass (%), skeletal muscle weight (kg), muscle (%), muscle weight, water (%), weight of water (kg), visceral fat, obesity degree (%), body age, weight without fat (kg), and actual age, were assessed using bioelectrical impedance analysis (Omron Karada Scan). While body composition measurements can be influenced by factors such as hydration status, recent food intake, physical activity, and measurement conditions—particularly in individuals with elevated BMI—the method remains a valuable and practical tool for assessing overall trends and directional changes in fat and fat-free compartments over time. Health-related quality of life was evaluated using the validated RAND SF-36 questionnaire Health Survey (SF-36) at baseline, Week 4, and Week 8. Patient-reported and physician-reported global satisfaction were recorded at Week 8 using a 4-point ordinal scale. Medication compliance, including adherence and discontinuation, was monitored throughout the study, and all adverse events were recorded to assess product safety.
2.7. Statistical Analysis Plan and Sample Size
A total of 50 participants were included in the study.
Data collected from the case report forms were entered into a Microsoft Excel database and analyzed using an intention-to-treat approach.
Statistical analyses were performed using a within-subject approach. Categorical variables were summarized as frequencies and percentages, while continuous variables were summarized as mean ± standard deviation. Changes from baseline to each follow-up visit (Week 4, Week 6, and Week 8) were evaluated using paired t-tests, as measurements were obtained repeatedly from the same participants.
To account for multiple pairwise comparisons, Bonferroni correction was applied, and the adjusted significance threshold was calculated by dividing the nominal alpha level (0.05) by the number of comparisons. All reported p-values remained below the adjusted threshold. Assumptions of normality for paired differences were assessed prior to analysis. A two-sided p-value < 0.05 (after adjustment) was considered statistically significant.
As this study was designed as an exploratory real-world observational investigation, the sample size was determined pragmatically based on the number of eligible participants available during the study period rather than a formal statistical power calculation. Given the single-arm, observational design, all analyses were descriptive and within-subject, and no between-group comparisons were performed. The results should therefore be interpreted as exploratory and hypothesis-generating.
3. Results
3.1. Demographic and Baseline Characteristics
Of the 50 participants enrolled, all completed the study as per protocol, with no deviations reported. The mean age of the study population was 37.09 ± 7.90 years, with a median age of 37.17 years. With respect to sex distribution, the majority of participants were male (40, 80.00%), while 10 females (20.00%) were included in the study population.
Primary outcome: Mean absolute and percent change in body weight from baseline to end of study visit.
A progressive reduction in body weight was observed over the 8-week observation period. Compared with baseline, mean body weight decreased at Week 4 and continued to decline through Weeks 6 and 8 within the study population. By Week 6, 32 out of 50 participants (64%) had experienced a reduction in body weight of ≥4 kg relative to baseline.
Reductions at all post-baseline visits reached statistical significance (p < 0.001), demonstrating a consistent downward trend over time. The upward trend in t-values across visits further supports the strengthening effect size over time.
Overall, the findings demonstrate a sustained and statistically significant reduction in body weight over the 8-week observation period in this single-arm cohort, shown in
Table 1 and
Figure 2.
3.2. Secondary Outcomes
Analysis of secondary outcomes demonstrated within-subjects changes across multiple anthropometric, body composition, and body age over the 8-week observation period in this single-arm cohort.
Among anthropometric parameters, waist and hip circumferences showed a consistent and statistically significant reduction at all post-baseline visits. BMI showed a tendency toward reduction, indicating a favorable direction.
With respect to body composition parameters, significant reductions were observed in body fat weight and visceral fat across all follow-up visits, while body fat percentage achieved statistical significance in Week 8. Reductions were observed in both fat mass and fat-free mass parameters, which may reflect overall weight loss in the absence of structured resistance training. Muscle percentage showed a small but statistically significant increase over time; however, absolute muscle mass parameters declined, which may reflect proportional changes secondary to overall weight loss rather than a true increase in muscle tissue.
Additionally, body age showed a statistically significant reduction from baseline to Week 8 (
Table 2 and
Figure 3).
3.3. Quality of Life Outcomes (SF-36 Domain Scores)
Patient-reported outcomes indicated changes in quality-of-life scores over the study period. Across several SF-36 domains, including physical functioning, general health perception, and social functioning, a trend toward more favorable responses was observed by Week 8 within the study population.
Improvements were also noted in role limitations and social functioning, with reduced interference of physical and emotional problems in routine activities. Additionally, trends toward enhanced vitality and emotional well-being were observed, reflected by improved perceptions of energy levels and reductions in negative mood states.
Overall, these findings suggest a favorable impact on patient-reported quality of life during the 8-week study period. However, as SF-36 scores are self-reported and the study lacked a control group, these changes may partially reflect expectation or reporting bias and cannot be conclusively attributed to L-Carnitine L-Tartrate itself. However, the improvements observed in SF-36 scores provide encouraging patient-reported evidence of enhanced quality of life and well-being following supplementation. These findings support the potential benefits of L-Carnitine L-Tartrate and warrant further evaluation in larger, controlled clinical studies to strengthen attribution of the observed effects. Detailed item-wise response distributions are provided in
Supplementary Table S1.
3.4. Patient and Physician Global Satisfaction
At Visit 4, patient-reported global assessment demonstrated favorable outcomes, with 50% of participants rating their experience as “Moderately satisfactory” and the remaining 50% as “Very satisfactory.” No participants reported ratings of “Not satisfactory” or “Minimally satisfactory,” indicating a uniformly positive patient perception of treatment response.
Similarly, the physician’s global assessment at Visit 4 reflected consistent positive evaluations. Half of patients were rated as “Moderately satisfactory,” while the remaining 50% were assessed as “Very satisfactory.” No patient was categorized as “Not satisfactory” or “Minimally satisfactory,” suggesting overall favorable clinical response as assessed by the investigator.
The observed improvements in anthropometric parameters, body composition, and patient-reported outcomes demonstrate favorable within-subject trends over the study period, supporting the potential clinical relevance of the intervention and providing a strong basis for further confirmatory research.
3.5. Summary of Adverse Events
No adverse events were reported during the 8-week study period. No serious adverse events, treatment-related discontinuations, or clinically significant safety concerns were observed.
4. Discussion
The primary contribution of this study lies in its real-world observational design, which captures treatment patterns and outcomes in routine clinical practice rather than under controlled experimental conditions. The inclusion of detailed body composition parameters and patient-reported quality-of-life measures provides a broader perspective on potential changes beyond body weight alone. Such multidimensional, practice-based data are relatively limited in the existing literature and may complement evidence derived from randomized controlled trials.
In this 8-week prospective observational investigation conducted in overweight and obese adults, daily administration of L-Carnitine L-Tartrate at a dose of 2000 mg was associated with statistically significant and progressively increasing reductions in body mass and related anthropometric indices. Mean body weight decreased from 73.69 ± 7.73 kg at baseline to 67.36 ± 7.87 kg at Week 8, representing a mean absolute reduction of 6.33 kg (8.59%; p < 0.001). The trajectory of weight loss demonstrated early-onset and sustained progression, with mean percentage reductions of 2.44% in Week 4 and 5.92% in Week 6. By Week 6, 64% of participants achieved a ≥4 kg reduction in body weight, a magnitude commonly regarded as clinically meaningful in the context of weight management. These encouraging findings highlight the potential effectiveness of the study product and support the need for further controlled clinical evaluation.
Concomitant improvements were observed in measures of central and peripheral adiposity. These patterns are consistent with previous reports of modest improvements in anthropometric indices among adults with overweight or obesity, but in the absence of a control group, we cannot exclude the contribution of lifestyle changes, regression to the mean, or other non-specific factors to the observed reductions in abdominal and visceral fat. At Week 8, waist and hip circumferences were reduced by 2.38 cm and 2.96 cm, respectively (both p < 0.001), suggesting attenuation of abdominal fat deposition. Body composition analysis revealed a mean reduction in total fat mass of 3.90 kg (18.86%; p < 0.001), accompanied by a 39.91% decrease in visceral adiposity (p < 0.001). A statistically significant decline in body fat percentage was also observed at Week 8 (−29.25%; p = 0.042), further supporting a preferential effect on adipose tissue compartments. These findings are consistent with previous reports demonstrating modest improvements in anthropometric indices among adults with overweight or obesity. The observed reductions in abdominal and visceral fat further support the potential beneficial role of the intervention and provide a strong rationale for larger, controlled studies to further validate these encouraging outcomes.
Patient-reported outcomes demonstrated improvement across multiple domains of the Short Form-36 (SF-36) questionnaire, reflecting enhanced health-related quality of life. Both participant- and physician-reported global assessments indicated uniformly favorable perceptions of therapeutic benefit. No treatment-emergent adverse events were documented during the study period, suggesting an acceptable tolerability profile within the observed timeframe.
Our findings align with prior randomized and meta-analytic evidence suggesting modest but significant weight reductions associated with L-Carnitine supplementation [
4,
16]. Prior meta-analytic aggregation of randomized controlled trials (
n = 9) demonstrated a pooled mean difference of approximately −1.33 kg relative to placebo, with more pronounced effects among individuals with overweight or obesity [
12]. Other individual studies have reported mean reductions of approximately −2.67 kg [
13]. In comparison, the present cohort demonstrated a numerically greater reduction in body weight (−6.33 kg; 8.59%), with 64% of participants achieving ≥4 kg weight loss by Week 6. Importantly, the present study reflects real-world implementation, thereby complementing controlled trial data and providing practical insight into effectiveness in routine clinical settings.
Previous randomized trials and meta-analyses have generally reported modest and variable effects of L-Carnitine supplementation on body weight and related outcomes. The findings of the present study should therefore be interpreted within the context of its observational design and real-world setting. Differences in study design, population characteristics, outcome assessment methods, and concomitant lifestyle factors may contribute to variability in observed outcomes across studies. Rather than serving as confirmatory evidence of efficacy, the present findings provide descriptive insights into short-term changes observed in routine clinical practice and may help to inform hypothesis generation for future controlled investigation.
Recent literature increasingly supports the role of nutraceuticals as strategies in obesity and inflammation-related metabolic disorders. A systematic review and network meta-analysis has highlighted that nutraceuticals such as n3-polyunsaturated fatty acids (n3-PUFA), inulin, butyrate, and vitamin B complexes exert modest benefits primarily through anti-inflammatory effects, modulation of gut microbiota, and metabolic cofactor activity. However, these interventions often demonstrate variable and less consistent effects on anthropometric outcomes compared with metabolically targeted compounds. In contrast, L-Carnitine exerts a direct metabolic effect by facilitating mitochondrial fatty acid transport and β-oxidation, thereby enhancing lipid utilization and reducing adiposity. This mechanistic specificity explains the comparatively greater and more consistent reductions in body weight, fat mass, and visceral adiposity observed in the present study [
17].
Talenezhad et al. reported dose-dependent weight and fat mass reductions with higher L-Carnitine doses and longer durations [
14], aligning with the 2000 mg/day regimen used in the present study. In contrast to several dietary supplements commonly marketed for weight loss, such as green tea, conjugated linoleic acid, or several others, whose effects are often modest and inconsistent [
18]. By incorporating quantitative body composition analysis, our study demonstrated a reduction in body fat weight of −3.90 kg (−18.86%), a decline in body fat percentage of −29.25%, and a marked decrease in visceral adiposity of −39.91% over 8 weeks. The parallel decline in waist circumference (−2.27%) further substantiates attenuation of central adiposity, a clinically salient surrogate of cardiometabolic risk [
19].
Concomitant reductions in total fat mass (−3.90 kg) and body fat percentage (−29.25%), and BMI (−2.15 kg/m
2), compared with earlier findings of −0.28 kg/m
2 [
20] indicate that overall weight loss reflected changes across multiple body composition compartments rather than exclusive adipose tissue loss. Given the mechanistic role of visceral fat in cardiometabolic risk propagation, these compartment-specific reductions are clinically meaningful and extend beyond simple weight loss metrics [
21,
22].
Interventional studies in metabolic syndrome and NAFLD have reported favorable effects of L-Carnitine on triglyceride concentrations and indices of insulin resistance [
23,
24]. The marked reduction in visceral adiposity (−39.91%) in this study may have important metabolic implications, considering the well-established association between excess visceral fat, ectopic lipid accumulation, and insulin resistance. These observations support the positioning of L-Carnitine not merely as a weight-loss supplement but as a metabolically relevant adjunct within structured obesity care. The marked reduction in visceral adiposity (−39.91%) observed in this study may have important metabolic implications.
Emerging evidence further supports the role of L-Carnitine in improving insulin sensitivity, particularly when combined with physical activity. A recent preclinical study demonstrated that L-Carnitine supplementation in conjunction with exercise significantly improved insulin resistance and metabolic parameters in obese models of type 2 diabetes. These findings reinforce the metabolic relevance of L-Carnitine beyond weight reduction, particularly in the context of insulin resistance and cardiometabolic risk [
25].
Beyond the observed anthropometric and body composition modifications, the analysis of patient-reported outcomes demonstrated statistically and clinically relevant improvements across multiple domains of the standardized health-related quality of life questionnaire, underscoring the broader functional implications of weight reduction. Specifically, enhancements in physical functioning, attenuation of role limitations attributable to physical health, and increased vitality scores suggest that the magnitude of weight loss achieved was accompanied by measurable gains in functional capacity and perceived energy levels. These findings are consistent with prior evidence indicating that even moderate reductions in body weight can yield significant improvements in health-related quality of life, particularly in domains linked to physical performance and daily activity engagement [
26].
The concordantly favorable global assessments reported by both participants and investigators further substantiate the alignment between objective anthropometric improvements and subjective perceptions of benefit. Such convergence between clinician-evaluated outcomes and patient-experienced health status is particularly relevant in the context of obesity management, where psychosocial determinants, self-efficacy, and functional autonomy substantially influence therapeutic engagement. Improvements in self-perceived physical capability and overall well-being may, in turn, facilitate sustained adherence to behavioral and lifestyle interventions, thereby potentiating the durability of therapeutic effects beyond the immediate intervention period.
L-Carnitine plays a central role in mitochondrial long-chain fatty acid translocation via the carnitine shuttle, thereby permitting entry of acyl moieties into the mitochondrial matrix for β-oxidative catabolism. Upregulation of this pathway enhances lipid substrate oxidation and may shift whole-body fuel partitioning toward increased utilization of fatty acids, culminating in depletion of adipose tissue reserves [
27,
28]. The observed reduction in visceral fat (−39.91%) is consistent with the proposed mechanistic pathway, as visceral adiposity is metabolically active and responsive to alterations in fatty acid flux.
Beyond its canonical function in β-oxidation, L-Carnitine serves as a critical regulator of mitochondrial bioenergetic integrity, facilitating acyl-group buffering, ATP generation, and intermediary metabolic processes, including ketogenesis and gluconeogenesis. It also contributes to cellular detoxification and membrane stabilization [
27]. Collectively, these pleiotropic metabolic effects provide a plausible biological substrate not only for reductions in adiposity but also for the enhanced vitality and physical functioning reflected in SF-36 outcomes.
A reduction in body weight within the range of 5–10% has been consistently associated with measurable improvements in insulin sensitivity, lipid homeostasis, and systemic blood pressure regulation [
29]. In this context, the mean body weight reduction of 8.59% observed over 8 weeks in the present study falls within this clinically meaningful threshold. Notably, 64% of participants achieved a ≥4 kg reduction in body weight by Week 6, indicating that a substantial proportion of the cohort attained meaningful weight loss within a relatively short duration. Together, these findings suggest that L-Carnitine L-Tartrate supplementation may contribute to clinically relevant weight reduction in routine practice settings.
Notably, this investigation was conducted under routine clinical conditions rather than within the constraints of a tightly regulated experimental framework. Observational evidence of this nature provides complementary insight to randomized controlled trials by reflecting real-world adherence dynamics, behavioral variability, and practice-based implementation. The high study completion rate and absence of reported adverse events indicate a favorable tolerability and acceptability profile, considerations of critical importance in chronic obesity management, where therapeutic discontinuation frequently limits long-term effectiveness.
No treatment-emergent adverse events were documented during the intervention period, and no participants discontinued supplementation secondary to safety-related concerns. This observation is consistent with the extant literature, wherein L-Carnitine has demonstrated a favorable tolerability profile, with predominantly mild and transient gastrointestinal disturbances reported as the most frequent adverse effects [
4]. The absence of clinically significant safety signals in the present cohort supports its tolerability within the observed time frame of L-Carnitine as a well-tolerated treatment in obesity management. L-Carnitine may be particularly relevant for individuals seeking adjunctive, non-pharmacologic strategies for weight reduction or for that intolerant to conventional anti-obesity pharmacotherapies.
Collectively, these findings support the consideration of L-Carnitine L-Tartrate as a clinically relevant, well-tolerated treatment in overweight and obese adults. Considering the substantial clinical burden of obesity and its cardiometabolic sequelae, a responder rate of 64% within 6 weeks represents a potentially impactful outcome in everyday practice. It demonstrates reductions in central adiposity and visceral fat, combined with favorable patient-reported outcomes and tolerability, positioning it as a practical supportive strategy within contemporary obesity management frameworks.
4.1. Strengths and Limitations of the Study
This study possesses several strengths. It was prospectively designed, achieved complete follow-up, reduced attrition bias, and evaluated multidimensional outcomes, including detailed body composition and patient-reported quality of life. The inclusion of visceral fat and fat mass measurements provides clinically relevant insight beyond simple weight reduction. Real-world applicability enhances external validity and complements evidence from randomized trials.
The observational single-arm design of this study provides preliminary real-world insights into the potential effects of L-Carnitine L-Tartrate supplementation; however, the absence of a control or comparator group limits direct causal interpretation of the observed outcomes. The study included a modest sample size (n = 50) with an intervention duration of 8 weeks, offering short-term evidence that may support the design of larger and longer-duration controlled studies in the future. In addition, body composition was assessed using bioelectrical impedance analysis, a practical and widely used method that may be influenced by hydration status and related measurement conditions, particularly during shorter follow-up periods.
In addition, biochemical metabolic markers were not evaluated, limiting mechanistic interpretation of the findings. In the absence of randomization, placebo control, or an active comparator, the observed changes reflect overall real-world outcomes associated with the intervention period, which may be influenced by multiple contributing factors. Alongside L-Carnitine L-Tartrate supplementation, concurrent lifestyle modifications, participant engagement, behavioral adherence, physical activity, dietary adjustments, and natural temporal trends may all have played a role in the observed outcomes, highlighting the multifactorial nature of real-world weight management responses. Health-related quality-of-life and global satisfaction outcomes were based on self-reported questionnaires in an open-label setting, introducing the potential for expectation and reporting bias.
Furthermore, while detailed quantitative data on dietary intake, caloric restriction, and physical activity were not systematically collected, participants were encouraged to follow general lifestyle recommendations, reflecting a flexible and real-world study approach. Adherence to these recommendations was not objectively monitored, allowing the observed outcomes to reflect outcomes under routine, non-restrictive conditions. As such, the observed magnitude of weight loss likely reflects a holistic combination of factors, including supplementation alongside general lifestyle influences, consistent with real-world conditions. This integrated effect supports the overall potential of L-Carnitine L-Tartrate within a broader wellness context and highlights the need for further controlled studies to better delineate its specific contribution.
Accordingly, the present findings provide valuable exploratory, real-world insights that complement evidence generated from randomized controlled trials and help inform future research directions. While not intended to establish definitive efficacy or mechanistic conclusions, the study offers a useful observational framework that supports hypothesis generation and guides the design of more rigorous future investigations.
4.2. Future Directions
Future research should include randomized controlled trials with larger, diverse populations and longer follow-up durations to evaluate the durability of weight loss. Inclusion of biochemical endpoints (lipids, insulin resistance markers) and DEXA for body composition assessment would enhance mechanistic clarity. Comparative effectiveness studies versus standard pharmacologic agents or other nutraceuticals and cost-effectiveness analyses are also warranted.






{kind=link}
{kind=link}
{kind=link}
{kind=link}