
A Comparison of the Efficacy of Online HAPIFED versus Online Cognitive Behavioural Therapy for Binge Eating Disorder: A Randomized Controlled Trial
 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
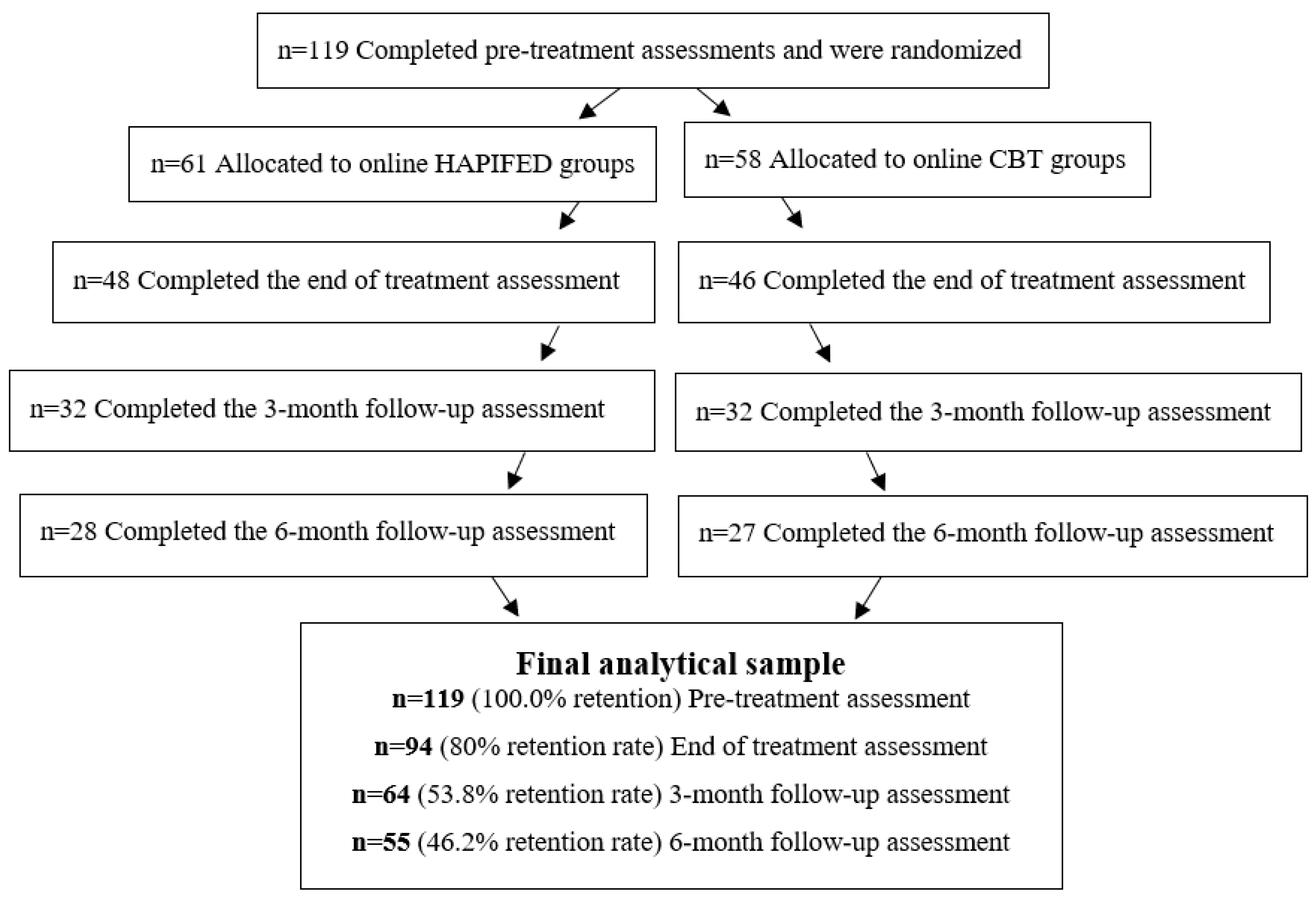
2.1. Participants and Study Design
2.2. Trial Registration
2.3. Interventions
2.3.1. Online HAPIFED
2.3.2. Online CBT
2.4. Assessments
2.4.1. Demographic Characteristics
2.4.2. Eating Disorder Examination Questionnaire (EDE-Q)
2.4.3. Loss of Control over Eating Scale (LOCES)
2.4.4. Difficulties in Emotion Regulation Scale (DERS)
2.4.5. Depression Anxiety and Stress Scale (DASS-21)
2.5. Statistical Analyses
3. Results
Body Weight
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Session Number | Type of Intervention | ||
|---|---|---|---|
| Nutritional Orientation | Physical Activity Orientation | Psychological Interventions | |
| 1 | -Introduction of healthcare professionals -Overview of the treatment program -How to use the HAPIFED App -Collaborative weighing -Participants’ introductions and expectations for the treatment | ||
| 2 | -Quality of foods -Structured eating -The binge eating cycle | ------------ | -Using the HAPIFED App -Personalizing the BED formulation |
| 3 | ------------ | -Understanding your relationship with physical activity | -Events, emotions, and eating -Proactive problem solving |
| 4 | -Identifying hunger and satiety cues | ------------ | -Events, emotions, and eating -Proactive problem solving |
| 5 | ------------ | -Myths about physical activity and exercise | -Events, emotions, and eating -Proactive problem solving -Addressing barriers to treatment progress |
| 6 | -Planning and organization around foods and eating | ------------ | -Addressing the urge to eat when not feeling physically hungry: “surfing the urge” |
| 7 | ------------ | -Weight loss versus fat loss | -Addressing the urge to eat when not feeling physically hungry: “surfing the urge” |
| 8 | -Mindful eating practice -Social aspects of eating | ------------ | -Understanding mindful eating |
| 9 | ------------ | -Reasons for physical activity/exercising | -Concerns about body shape and weight: focussing on the positive aspects of your body |
| 10 | -Brazilian healthy eating guidelines | ------------ | -Identifying my positive aspects |
| 11 | ------------ | -Memory, emotions, and readiness to exercise | -Body image: developing other domains of self-evaluation |
| 12 | -Progress with treatment and future goals | ------------ | -Developing a long-term maintenance plan |
| 13 | -Preparation for the end of the treatment program -Relapse prevention -Discussion about individualized long-term maintenance plans | ||
| 14 | -Booster session: identifying achievements and addressing difficulties | ||
| 15 | -Booster session: identifying achievements and addressing difficulties | ||
| Session Number | Therapy Topics |
|---|---|
| 1 | -Introduction of therapists -Overview of the therapy program -Participants’ introductions and expectations for the treatment -Personalization of the BED formulation |
| 2 | -Review of the personalization of the BED formulation -Instructions for self-monitoring -Collaborative weighing and addressing weight concerns |
| 3 | -Review of self-monitoring and collaborative weighing -Psychoeducation about BED -Regular eating |
| 4 | -Review of self-monitoring and regular eating -Addressing the urge to eat between meals and snacks |
| 5 | -Review of addressing the urge to eat between meals and snacks -Assessment of progress with the therapy and identification of barriers to change |
| 6 | -Review of the progress with the therapy and identification of barriers to change -Binge eating episode analysis and proactive problem solving |
| 7 | -Review of binge eating episode analysis and proactive problem solving -Addressing dietary restraint/restriction and binge eating |
| 8 | -Continuation of addressing dietary restraint/restriction and binge eating |
| 9 | -Review of dietary restraint/restriction and binge eating -Body image: developing other domains of self-evaluation |
| 10 | -Review of body image: developing other domains of self-evaluation -Body image: body checking, body avoidance, and comparison with others |
| 11 | -Review of body image: body checking, body avoidance, and comparison with others -Addressing body image: “feeling fat” |
| 12 | -Review of addressing body image: “feeling fat” -Dealing with setbacks and the “BED mindset” |
| 13 | -Review of dealing with setbacks and the “BED mindset” -Ending treatment well |
| 14 | -Booster session: identifying achievements and addressing difficulties |
| 15 | -Booster session: identifying achievements and addressing difficulties |
References
- Javaras, K.N.; Pope, H.G.; Lalonde, J.K.; Roberts, J.L.; Nillni, Y.I.; Laird, N.M.; Bulik, C.M.; Crow, S.J.; McElroy, S.L.; Walsh, B.T.; et al. Co-occurrence of binge eating disorder with psychiatric and medical disorders. J. Clin. Psychiatry 2008, 69, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Berglund, P.A.; Chiu, W.T.; Deitz, A.C.; Hudson, J.I.; Shahly, V.; Aguilar-Gaxiola, S.; Alonso, J.; Angermeyer, M.C.; Benjet, C.; et al. The Prevalence and Correlates of Binge Eating Disorder in the World Health Organization World Mental Health Surveys. Biol. Psychiatry 2013, 73, 904–914. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Shahly, V.; Hudson, J.I.; Supina, D.; Berglund, P.A.; Chiu, W.T.; Gruber, M.; Aguilar-Gaxiola, S.; Alonso, J.; Andrade, L.H.; et al. A comparative analysis of role attainment and impairment in binge-eating disorder and bulimia nervosa: Results from the WHO World Mental Health Surveys. Epidemiol. Psychiatr. Sci. 2014, 23, 27–41. [Google Scholar] [CrossRef]
- de Jonge, P.; Alonso, J.; Stein, D.J.; Kiejna, A.; Aguilar-Gaxiola, S.; Viana, M.C.; Liu, Z.; O’Neill, S.; Bruffaerts, R.; Caldas-de-Almeida, J.M.; et al. Associations between DSM-IV mental disorders and diabetes mellitus: A role for impulse control disorders and depression. Diabetologia 2014, 57, 699–709. [Google Scholar] [CrossRef] [PubMed]
- Raevuori, A.; Suokas, J.; Haukka, J.; Gissler, M.; Linna, M.; Grainger, M.; Suvisaari, J. Highly increased risk of type 2 diabetes in patients with binge eating disorder and bulimia nervosa. Int. J. Eat. Disord. 2015, 48, 555–562. [Google Scholar] [CrossRef] [PubMed]
- Wassenaar, E.; Friedman, J.; Mehler, P.S. Medical Complications of Binge Eating Disorder. Psychiatr. Clin. N. Am. 2019, 42, 275–286. [Google Scholar] [CrossRef] [PubMed]
- Grilo, C.M.; White, M.A.; Barnes, R.D.; Masheb, R.M. Psychiatric disorder co-morbidity and correlates in an ethnically diverse sample of obese patients with binge eating disorder in primary care settings. Compr. Psychiatry 2013, 54, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Solmi, F.; Moreno, A.B.; Lewis, G.; Angélica Nunes, M.; Jesus Mendes da Fonseca, M.; Harter Griep, R. Longitudinal association between binge eating and metabolic syndrome in adults: Findings from the ELSA-Brasil cohort. Acta Psychiatr. Scand. 2021, 144, 464–474. [Google Scholar] [CrossRef] [PubMed]
- da Luz, F.Q.; Hay, P.; Touyz, S.; Sainsbury, A. Obesity with Comorbid Eating Disorders: Associated Health Risks and Treatment Approaches. Nutrients 2018, 10, 829. [Google Scholar] [CrossRef] [PubMed]
- Hambleton, A.; Pepin, G.; Le, A.; Maloney, D.; Aouad, P.; Barakat, S.; Boakes, R.; Brennan, L.; Bryant, E.; Byrne, S.; et al. Psychiatric and medical comorbidities of eating disorders: Findings from a rapid review of the literature. J. Eat. Disord. 2022, 10, 132. [Google Scholar] [CrossRef] [PubMed]
- Momen, N.C.; Plana-Ripoll, O.; Yilmaz, Z.; Thornton, L.M.; McGrath, J.J.; Bulik, C.M.; Petersen, L.V. Comorbidity between eating disorders and psychiatric disorders. Int. J. Eat. Disord. 2022, 55, 505–517. [Google Scholar] [CrossRef] [PubMed]
- Udo, T.; Grilo, C.M. Psychiatric and medical correlates of DSM-5 eating disorders in a nationally representative sample of adults in the United States. Int. J. Eat. Disord. 2019, 52, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Mond, J.M.; Hay, P.J.; Rodgers, B.; Owen, C. Health service utilization for eating disorders: Findings from a community-based study. Int. J. Eat. Disord. 2007, 40, 399–408. [Google Scholar] [CrossRef] [PubMed]
- Hudson, J.I.; Hiripi, E.; Pope Jr, H.G.; Kessler, R.C. The Prevalence and Correlates of Eating Disorders in the National Comorbidity Survey Replication. Biol. Psychiatry 2007, 61, 348–358. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg, D.; Nicklett, E.J.; Roeder, K.; Kirz, N.E. Eating Disorder Symptoms Among College Students: Prevalence, Persistence, Correlates, and Treatment-Seeking. J. Am. Coll. Health 2011, 59, 700–707. [Google Scholar] [CrossRef] [PubMed]
- Kazdin, A.E.; Fitzsimmons-Craft, E.E.; Wilfley, D.E. Addressing critical gaps in the treatment of eating disorders. Int. J. Eat. Disord. 2017, 50, 170–189. [Google Scholar] [CrossRef] [PubMed]
- Thompson, C.; Park, S. Barriers to access and utilization of eating disorder treatment among women. Arch. Womens Ment. Health 2016, 19, 753–760. [Google Scholar] [CrossRef] [PubMed]
- Sproch, L.E.P.; Anderson, K.P.P. Clinician-Delivered Teletherapy for Eating Disorders. Psychiatr. Clin. N. Am. 2019, 42, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Carrard, I.; Crépin, C.; Rouget, P.; Lam, T.; Golay, A.; Van der Linden, M. Randomised controlled trial of a guided self-help treatment on the Internet for binge eating disorder. Behav. Res. Ther. 2011, 49, 482–491. [Google Scholar] [CrossRef] [PubMed]
- Wyssen, A.; Meyer, A.H.; Messerli-Bürgy, N.; Forrer, F.; Vanhulst, P.; Lalanne, D.; Munsch, S. BED-online: Acceptance and efficacy of an internet-based treatment for binge-eating disorder: A randomized clinical trial including waitlist conditions. Eur. Eat. Disord. Rev. 2021, 29, 937–954. [Google Scholar] [CrossRef] [PubMed]
- Grammer, A.C.; Monterubio, G.E.; D’Adamo, L.; Balantekin, K.N.; Taylor, C.B.; Fitzsimmons-Craft, E.E.; Wilfley, D.E. Evaluation of a combined, online intervention for binge-type eating disorders and high body weight in young adults. Eat. Behav. 2023, 50, 101789. [Google Scholar] [CrossRef] [PubMed]
- de Zwaan, M.; Herpertz, S.; Zipfel, S.; Svaldi, J.; Friederich, H.-C.; Schmidt, F.; Mayr, A.; Lam, T.; Schade-Brittinger, C.; Hilbert, A. Effect of Internet-Based Guided Self-help vs. Individual Face-to-Face Treatment on Full or Subsyndromal Binge Eating Disorder in Overweight or Obese Patients: The INTERBED Randomized Clinical Trial. JAMA psychiatry 2017, 74, 987–995. [Google Scholar] [CrossRef] [PubMed]
- Loucas, C.E.; Fairburn, C.G.; Whittington, C.; Pennant, M.E.; Stockton, S.; Kendall, T. E-therapy in the treatment and prevention of eating disorders: A systematic review and meta-analysis. Behav. Res. Ther. 2014, 63, 122–131. [Google Scholar] [CrossRef] [PubMed]
- Barakat, S.; Maguire, S.; Smith, K.E.; Mason, T.B.; Crosby, R.D.; Touyz, S. Evaluating the role of digital intervention design in treatment outcomes and adherence to eTherapy programs for eating disorders: A systematic review and meta-analysis. Int. J. Eat. Disord. 2019, 52, 1077–1094. [Google Scholar] [CrossRef] [PubMed]
- Abrahamsson, N.; Ahlund, L.; Ahrin, E.; Alfonsson, S. Video-based CBT-E improves eating patterns in obese patients with eating disorder: A single case multiple baseline study. J. Behav. Ther. Exp. Psy. 2018, 61, 104–112. [Google Scholar] [CrossRef] [PubMed]
- Frayn, M.; Fojtu, C.; Juarascio, A. COVID-19 and binge eating: Patient perceptions of eating disorder symptoms, tele-therapy, and treatment implications. Curr. Psychol. 2021, 40, 6249–6258. [Google Scholar] [CrossRef] [PubMed]
- Valdez-Aguilar, M.; Vazquez-Arevalo, R.; López-Aguilar, X.; Ruíz Martínez, A.O.; Rosinska, M.; Mancilla-Díaz, J.M. Online multidisciplinary treatment of binge eating disorder in people with high weight: A case series study. J. Eat. Disord. 2023, 11, 86. [Google Scholar] [CrossRef] [PubMed]
- Rom, S.; Miskovic-Wheatley, J.; Barakat, S.; Aouad, P.; Fuller-Tyszkiewicz, M.; Maguire, S. Evaluating the feasibility and potential efficacy of a brief eTherapy for binge-eating disorder: A pilot study. Int. J. Eat. Disord. 2022, 55, 1614–1620. [Google Scholar] [CrossRef] [PubMed]
- da Luz, F.Q.; Swinbourne, J.; Sainsbury, A.; Touyz, S.; Palavras, M.; Claudino, A.; Hay, P. HAPIFED: A Healthy APproach to weIght management and Food in Eating Disorders: A case series and manual development. J. Eat. Disord. 2017, 5, 29. [Google Scholar] [CrossRef]
- Fairburn, C. Cognitive Behavior Therapy and Eating Disorders; Guilford: New York, NY, USA, 2008. [Google Scholar]
- Palavras, M.A.; Hay, P.; Mannan, H.; da Luz, F.Q.; Sainsbury, A.; Touyz, S.; Claudino, A.M. Integrated weight loss and cognitive behavioural therapy (CBT) for the treatment of recurrent binge eating and high body mass index: A randomized controlled trial. Eat. Weight Disord. 2020, 26, 249–262. [Google Scholar] [CrossRef] [PubMed]
- Hay, P.; Palavras, M.A.; da Luz, F.Q.; Dos Anjos Garnes, S.; Sainsbury, A.; Touyz, S.; Appolinario, J.C.; Claudino, A.M. Physical and mental health outcomes of an integrated cognitive behavioural and weight management therapy for people with an eating disorder characterized by binge eating and a high body mass index: A randomized controlled trial. BMC Psychiatry 2022, 22, 355. [Google Scholar] [CrossRef] [PubMed]
- Palavras, M.A.; Hay, P.; Touyz, S.; Sainsbury, A.; da Luz, F.; Swinbourne, J.; Estella, N.M.; Claudino, A. Comparing cognitive behavioural therapy for eating disorders integrated with behavioural weight loss therapy to cognitive behavioural therapy-enhanced alone in overweight or obese people with bulimia nervosa or binge eating disorder: Study protocol for a randomised controlled trial. Trials 2015, 16, 578. [Google Scholar] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D.; the CONSORT Group. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMC Med. 2010, 8, 18. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Gildea, A.; Shukla, S.; Parretti, H.; Khan, O. Referral criteria and assessment for bariatric surgery: Summary of updated NICE guidance. BMJ 2023, 382, 1880. [Google Scholar] [CrossRef] [PubMed]
- da Luz, F.Q.; Mohsin, M.; Jana, T.A.; Marinho, L.S.; Santos, E.d.; Lobo, I.; Pascoareli, L.; Gaeta, T.; Ferrari, S.; Teixeira, P.C.; et al. An Examination of the Relationships between Eating-Disorder Symptoms, Difficulties with Emotion Regulation, and Mental Health in People with Binge Eating Disorder. Behav. Sci. 2023, 13, 234. [Google Scholar] [CrossRef] [PubMed]
- Research Eletronic Data Capture. Available online: https://www.project-redcap.org/ (accessed on 13 March 2023).
- Registro Brasileiro de Ensaios Clínicos. Available online: https://ensaiosclinicos.gov.br/rg/RBR-10hvfd58 (accessed on 5 June 2023).
- Center for Research on Eating Disorders at Oxford. Available online: https://www.credo-oxford.com/#topic0 (accessed on 16 March 2020).
- Berg, K.C.; Peterson, C.B.; Frazier, P.; Crow, S.J. Psychometric evaluation of the eating disorder examination and eating disorder examination-questionnaire: A systematic review of the literature. Int. J. Eat. Disord. 2012, 45, 428–438. [Google Scholar] [CrossRef] [PubMed]
- Machado, P.P.P.; Martins, C.; Vaz, A.R.; Conceição, E.; Bastos, A.P.; Gonçalves, S. Eating Disorder Examination Questionnaire: Psychometric Properties and Norms for the Portuguese Population. Eur. Eat. Disord. Rev. 2014, 22, 448–453. [Google Scholar] [CrossRef] [PubMed]
- Latner, J.D.; Mond, J.M.; Kelly, M.C.; Haynes, S.N.; Hay, P.J. The Loss of Control Over Eating Scale: Development and psychometric evaluation. Int. J. Eat. Disord. 2014, 47, 647–659. [Google Scholar] [CrossRef] [PubMed]
- Luz, F.Q.d.; Sainsbury, A.; Estella, N.M.; Cogo, H.; Touyz, S.W.; Palavras, M.A.; Latner, J.D.; Claudino, A.; Hay, P. An empirical evaluation of the translation to Brazilian Portuguese of the Loss of Control over Eating Scale (LOCES). Rev. Psiquiatr. Clín. 2016, 43, 1–5. [Google Scholar] [CrossRef]
- Gratz, K.L.; Roemer, L. Multidimensional Assessment of Emotion Regulation and Dysregulation: Development, Factor Structure, and Initial Validation of the Difficulties in Emotion Regulation Scale. J. Psychopathol. Behav. Assess. 2004, 26, 41–54. [Google Scholar] [CrossRef]
- Burton, A.L.; Brown, R.; Abbott, M.J. Overcoming difficulties in measuring emotional regulation: Assessing and comparing the psychometric properties of the DERS long and short forms. Cogent Psychol. 2022, 9, 2060629. [Google Scholar] [CrossRef]
- Cancian, A.C.M.; de Souza, L.A.S.; Silva, V.H.P.E.; Machado, W.d.L.; Oliveira, M.d.S. Psychometric properties of the Brazilian version of the Difficulties in Emotion Regulation Scale (DERS). Trends Psychiatry Psychother. 2019, 41, 18–26. [Google Scholar] [CrossRef]
- Lovibond, S.H.; Lovibond, P.F. Manual for the Depression Anxiety Stress Scales, 2nd ed.; Psychology Foundation of Australia: Sydney, NSW, Australia, 1995. [Google Scholar]
- Henry, J.D.; Crawford, J.R. The short-form version of the Depression Anxiety Stress Scales (DASS-21): Construct validity and normative data in a large non-clinical sample. Br. J. Clin. Psychol. 2005, 44, 227–239. [Google Scholar] [CrossRef] [PubMed]
- Vignola, R.C.B.; Tucci, A.M. Adaptation and validation of the depression, anxiety and stress scale (DASS) to Brazilian Portuguese. J. Affect. Disord. 2014, 155, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge Academic: New York, NY, USA, 1988. [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows, Version 27.0; IBM Corp.: Armonk, NY, USA, 2020. [Google Scholar]
- Ryan, D.H.; Yockey, S.R. Weight Loss and Improvement in Comorbidity: Differences at 5%, 10%, 15%, and Over. Curr. Obes. Rep. 2017, 6, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Fitzsimmons-Craft, E.E.; Taylor, C.B.; Graham, A.K.; Sadeh-Sharvit, S.; Balantekin, K.N.; Eichen, D.M.; Monterubio, G.E.; Goel, N.J.; Flatt, R.E.; Karam, A.M.; et al. Effectiveness of a Digital Cognitive Behavior Therapy-Guided Self-Help Intervention for Eating Disorders in College Women: A Cluster Randomized Clinical Trial. JAMA Netw. Open 2020, 3, e2015633. [Google Scholar] [CrossRef] [PubMed]
- Pruessner, L.; Timm, C.; Barnow, S.; Rubel, J.A.; Lalk, C.; Hartmann, S. Effectiveness of a Web-Based Cognitive Behavioral Self-Help Intervention for Binge Eating Disorder: A Randomized Clinical Trial. JAMA Netw. Open 2024, 7, e2411127. [Google Scholar] [CrossRef] [PubMed]
- Pruessner, L.; Hartmann, S.; Rubel, J.A.; Lalk, C.; Barnow, S.; Timm, C. Integrating a web-based intervention into routine care of binge-eating disorder: Study protocol for a randomized controlled trial. Internet Interven. 2022, 21, 28–100514. [Google Scholar] [CrossRef] [PubMed]
- van Beers, E.; Melisse, B.; de Jonge, M.; Peen, J.; van den Berg, E.; de Beurs, E. Web-based guided self-help cognitive behavioral therapy–enhanced versus treatment as usual for binge-eating disorder: A randomized controlled trial protocol. Front. Psychiatry 2024, 15, 1332360. [Google Scholar] [CrossRef] [PubMed]
- Beleigoli, A.M.; Andrade, A.Q.; Cançado, A.G.; Paulo, M.N.; Diniz, M.D.F.H.; Ribeiro, A.L. Web-Based Digital Health Interventions for Weight Loss and Lifestyle Habit Changes in Overweight and Obese Adults: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2019, 21, e298. [Google Scholar] [CrossRef] [PubMed]
- Grenon, R.; Schwartze, D.; Hammond, N.; Ivanova, I.; McQuaid, N.; Proulx, G.; Tasca, G.A. Group psychotherapy for eating disorders: A meta-analysis. Int. J. Eat. Disord. 2017, 50, 997–1013. [Google Scholar] [CrossRef]
| Participants’ Characteristics | Online HAPIFED Groups | Online CBT Groups | Online HAPIFED Groups vs. Online CBT Groups: p-Values |
|---|---|---|---|
| Number (%) | Number (%) | ||
| All participants | 61 (100.0) | 58 (100.0) | |
| Gender | |||
| Male | 5 (8.2) | 6 (10.3) | |
| Female | 56 (91.8) | 52 (89.7) | p = 0.686 |
| Age group | |||
| <30 | 15 (24.6) | 11 (19.0) | |
| 30–39 | 23 (37.7) | 31 (53.4) | |
| 40 and above | 23 (8.2) | 16 (27.6) | p = 0.225 |
| Mean Age (SD) | 36.5 (9.8) | 35.4 (7.5) | p = 0.245 |
| Race | |||
| White | 44 (72.1) | 45 (77.6) | |
| Black or other | 17 (27.9) | 13 (22.4) | p = 0.493 |
| Occupation | |||
| Employed full/part time | 40 (65.6) | 38 (65.5) | |
| Unemployed/Other | 21 (34.4) | 20 (34.5) | p = 0.995 |
| Marital status | |||
| Married/Living with partner | 38 (62.3) | 39 (67.2) | |
| Single/Never married/Other | 23 (37.7) | 19 (32.8) | p = 0.573 |
| Income | |||
| Less than BRL 3.135 | 34 (55.7) | 35 (60.3) | |
| Above BRL 3.135 | 27 (44.3) | 23 (39.7) | p = 0.611 |
| Outcome Measures | Pre-Treatment | End of Treatment | 3-Month Follow-up | 6-Month Follow-up | Pre-Treatment Versus | |
|---|---|---|---|---|---|---|
| Online HAPIFED (n = 61) | Online HAPIFED (n = 48) | Online HAPIFED (n = 32) | Online HAPIFED (n = 28) | End of Treatment | 6-Month Follow-up | |
| Mean (95%CI) | Mean (95%CI) | Mean (95%CI) | Mean (95%CI) | p-Values | p-Values | |
| OBE episodes | 12.8 (10.1–15.5) | 6.2 (2.9–9.5) | 5.3 (0.9–9.6) | 4.1 (0.3–8.6) | 0.001 | 0.001 |
| SBE episodes | 10.4 (8.7–12.1) | 5.4 (3.5–7.2) | 4.7 (2.4–7.0) | 4.3 (1.9–6.7) | 0.001 | 0.001 |
| Dietary restraint | 2.0 (1.6–2.3) | 1.1 (0.8–1.5) | 0.8 (0.4–1.2) | 1.0 (0.5–1.4) | 0.001 | 0.001 |
| Eating concerns | 3.4 (3.0–3.8) | 1.6 (1.2–2.0) | 1.4 (1.0–1.9) | 1.3 (0.9–1.8) | 0.001 | 0.001 |
| Shape concerns | 4.8 (4.5–5.2) | 3.1 (2.7–3.4) | 3.1 (2.6–3.5) | 3.0 (2.5–3.4) | 0.001 | 0.001 |
| Weight concerns | 4.2 (3.9–4.5) | 2.8 (2.5–3.2) | 2.7 (2.3–3.1) | 2.8 (2.4–3.2) | 0.001 | 0.001 |
| EDEQ global | 3.6 (3.3–3.9) | 2.2 (1.8–2.5) | 2.0 (1.6–2.4) | 2.0 (1.6–2.4) | 0.001 | 0.001 |
| LOCES total | 81.3 (76.8–85.9) | 52.6 (47.5–57.6) | 50.6 (44.5–56.6) | 50.9 (44.5–57.3) | 0.001 | 0.001 |
| Depression | 14.5 (12.0–17.0) | 10.0 (7.3–12.8) | 8.9 (5.8–12.0) | 9.9 (6.6–13.2) | 0.001 | 0.018 |
| Anxiety | 9.4 (7.4–11.4) | 6.9 (4.7–9.1) | 7.9 (5.3–10.5) | 7.3 (4.6–10.0) | 0.074 | 0.076 |
| Stress | 19.2 (16.9–21.5) | 14.3 (11.8–16.9) | 14.9 (11.9–17.8) | 16.6 (13.4–19.8) | 0.004 | 0.445 |
| DERS total | 97.3(91.2–103.4) | 86.5 (79.8–93.1) | 84.3 (76.8–91.8) | 81.9 (74.0–89.8) | 0.001 | 0.004 |
| Outcome Measures | Online CBT (n = 58) | Online CBT (n = 46) | Online CBT (n = 32) | Online CBT (n = 27) | End of treatment | 6-month follow-up |
| Mean (95%CI) | Mean (95%CI) | Mean (95%CI) | Mean (95%CI) | p-values | p-values | |
| OBE episodes | 13.4 (10.9–15.8) | 5.5 (2.0–9.1) | 5.3 (0.8–9.9) | 7.3 (2.3–12.4) | 0.005 | 0.052 |
| SBE episodes | 10.7 (9.0–12.4) | 5.1 (3.1–7.0) | 4.8 (2.5–7.1) | 6.2 (3.7–8.6) | 0.001 | 0.110 |
| Dietary restraint | 2.2 (1.8–2.5) | 1.6 (1.2–1.9) | 1.7 (1.2–2.1) | 1.4 (0.9–1.8) | 0.007 | 0.001 |
| Eating concerns | 3.6 (3.3–4.0) | 2.0 (1.6–2.5) | 2.0 (1.6–2.5) | 2.0 (1.5–2.5) | 0.001 | 0.001 |
| Shape concerns | 5.0 (4.7–5.4) | 3.7 (3.4–4.1) | 3.5 (3.1–3.9) | 3.6 (3.1–4.0) | 0.001 | 0.001 |
| Weight concerns | 4.4 (4.0–4.7) | 3.2 (2.8–3.5) | 3.0 (2.5–3.4) | 3.1 (2.7–3.6) | 0.001 | 0.001 |
| EDEQ global | 3.8 (3.5–4.1) | 2.6 (2.3–2.9) | 2.5 (2.2–2.9) | 2.5 (2.1–2.9) | 0.001 | 0.001 |
| LOCES total | 82.5 (77.9–87.1) | 54.2 (48.9–59.4) | 56.1 (50.0–62.1) | 57.3 (50.7–64.0) | 0.001 | 0.001 |
| Depression | 16.9 (14.3–19.4) | 12.9 (10.1–15.7) | 12.1 (9.0–15.3) | 13.9 (10.5–17.3) | 0.004 | 0.097 |
| Anxiety | 11.3 (9.2–13.4) | 7.1 (4.8–9.3) | 8.2 (5.6–10.8) | 8.8 (6.0–11.6) | 0.002 | 0.203 |
| Stress | 22.6 (20.2–24.9) | 16.4 (13.8–18.9) | 15.4 (12.4–18.4) | 17.7 (14.4–21.0) | 0.001 | 0.023 |
| DERS total | 103.5 (97.3–109.7) | 84.6 (77.8–91.4) | 88.8 (81.3–96.3) | 87.8 (79.9–95.8) | 0.001 | 0.002 |
| Outcome Measures | Effect | |||||
|---|---|---|---|---|---|---|
| Treatment Arms (Online HAPIFED Groups, Online CBT Groups) | Assessment Timepoints (Pre-Treatment, End of Treatment, 3-Month Follow-up, and 6-Month Follow-up) | Treatment Arm and Assessment Timepoints | ||||
| F-Value | p-Value | F-Value | p-Value | F-Value | p-Value | |
| Objective binge eating episodes | 0.9 | 0.337 | 14.5 | <0.001 | 0.6 | 0.628 |
| Subjective binge eating episodes | 0.3 | 0.611 | 22.0 | <0.001 | 0.4 | 0.736 |
| Dietary restraint | 5.6 | 0.020 | 13.9 | <0.001 | 1.2 | 0.302 |
| Eating concerns | 4.5 | 0.036 | 74.7 | <0.001 | 0.7 | 0.533 |
| Shape concerns | 5.4 | 0.022 | 64.0 | <0.001 | 1.1 | 0.357 |
| Weight concerns | 1.8 | 0.184 | 50.6 | <0.001 | 0.1 | 0.938 |
| EDE-Q global score | 5.8 | 0.017 | 72.7 | <0.001 | 0.8 | 0.477 |
| LOCES total score | 1.8 | 0.180 | 91.5 | <0.001 | 0.6 | 0.623 |
| Depression | 3.6 | 0.059 | 11.0 | <0.001 | 0.2 | 0.904 |
| Anxiety | 0.5 | 0.460 | 6.3 | <0.001 | 0.5 | 0.689 |
| Stress | 1.6 | 0.212 | 13.9 | <0.001 | 0.6 | 0.610 |
| DERS total score | 0.8 | 0.366 | 23.0 | <0.001 | 1.5 | 0.221 |
| Outcome Measures | Effect Sizes (Cohen’s d): Online HAPIFED Groups | Effect Sizes (Cohen’s d): Online CBT Groups | ||||
|---|---|---|---|---|---|---|
| Pre-Treatment Compared to | Pre-Treatment Compared to | |||||
| End of Treatment | 3-Month Follow-up | 6-Month Follow-up | End of Treatment | 3-Month Follow-up | 6-Month Follow-up | |
| Cohen’s d | Cohen’s d | Cohen’s d | Cohen’s d | Cohen’s d | Cohen’s d | |
| Objective binge eating episodes | 0.59 | 0.73 | 0.85 | 0.50 | 0.52 | 0.49 |
| Subjective binge eating episodes | 0.49 | 0.53 | 0.67 | 0.75 | 0.75 | 0.32 |
| Dietary restraint | 0.48 | 0.93 | 0.81 | 0.42 | 0.42 | 0.78 |
| Eating concerns | 1.24 | 1.37 | 1.56 | 1.16 | 1.03 | 0.92 |
| Shape concerns | 1.21 | 0.93 | 0.98 | 1.15 | 0.97 | 0.97 |
| Weight concerns | 0.96 | 0.83 | 0.81 | 1.04 | 1.07 | 0.87 |
| EDE-Q global score | 1.19 | 1.26 | 1.23 | 1.12 | 1.04 | 1.05 |
| LOCES score | 1.52 | 1.40 | 1.84 | 1.24 | 1.17 | 1.24 |
| Depression | 0.47 | 0.64 | 0.49 | 0.44 | 0.42 | 0.34 |
| Anxiety | 0.27 | 0.19 | 0.36 | 0.50 | 0.35 | 0.26 |
| Stress | 0.45 | 0.37 | 0.15 | 0.63 | 0.53 | 0.48 |
| DERS score | 0.49 | 0.45 | 0.63 | 0.79 | 0.58 | 0.68 |
| Boddy mass index | 0.28 | 0.32 | 0.33 | 0.34 | 0.41 | 0.42 |
| Body weight | 0.28 | 0.32 | 0.33 | 0.28 | 0.40 | 0.53 |
| Mean Body Weight (kg) | Calculated Manually from Overall Mean | Calculated from Individual Level Weight Pairwise | ||||
|---|---|---|---|---|---|---|
| Pre-Treatment | 6-Month Follow-up | Difference (kg) | % Weight Loss: Pre-Treatment to 6-Month Follow-up | Difference (kg) | % Weight Loss: Pre-Treatment to 6-Month Follow-up | |
| Online HAPIFED groups | 96.1 | 89.5 | 6.6 | 6.8% | 2.3 | 2.4 |
| Online CBT groups | 98.4 | 94.5 | 3.9 | 3.9% | 3.8 | 3.8 |
| p = 0.476 | p = 0.256 | p = 0.419 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
da Luz, F.Q.; Mohsin, M.; Teixeira, P.C.; dos Santos, E.; Gaeta, T.; Ferrari, S.; Martin, K.; Dias, A.; Jana, T.A.; Marinho, L.S.; et al. A Comparison of the Efficacy of Online HAPIFED versus Online Cognitive Behavioural Therapy for Binge Eating Disorder: A Randomized Controlled Trial. Obesities 2024, 4, 145-159. https://doi.org/10.3390/obesities4020014
da Luz FQ, Mohsin M, Teixeira PC, dos Santos E, Gaeta T, Ferrari S, Martin K, Dias A, Jana TA, Marinho LS, et al. A Comparison of the Efficacy of Online HAPIFED versus Online Cognitive Behavioural Therapy for Binge Eating Disorder: A Randomized Controlled Trial. Obesities. 2024; 4(2):145-159. https://doi.org/10.3390/obesities4020014
Chicago/Turabian Styleda Luz, Felipe Q., Mohammed Mohsin, Paula C. Teixeira, Edilaine dos Santos, Tamiris Gaeta, Silvia Ferrari, Kayo Martin, Andréia Dias, Tatiana A. Jana, Leticia S. Marinho, and et al. 2024. "A Comparison of the Efficacy of Online HAPIFED versus Online Cognitive Behavioural Therapy for Binge Eating Disorder: A Randomized Controlled Trial" Obesities 4, no. 2: 145-159. https://doi.org/10.3390/obesities4020014
APA Styleda Luz, F. Q., Mohsin, M., Teixeira, P. C., dos Santos, E., Gaeta, T., Ferrari, S., Martin, K., Dias, A., Jana, T. A., Marinho, L. S., Lobo, I., Pascoareli, L., Cordás, T., & Hay, P. (2024). A Comparison of the Efficacy of Online HAPIFED versus Online Cognitive Behavioural Therapy for Binge Eating Disorder: A Randomized Controlled Trial. Obesities, 4(2), 145-159. https://doi.org/10.3390/obesities4020014