
Obesity Increases Maternal Complications in Pregnant Women of Sinop: A Retrospective Cohort Study

Abstract
1. Introduction
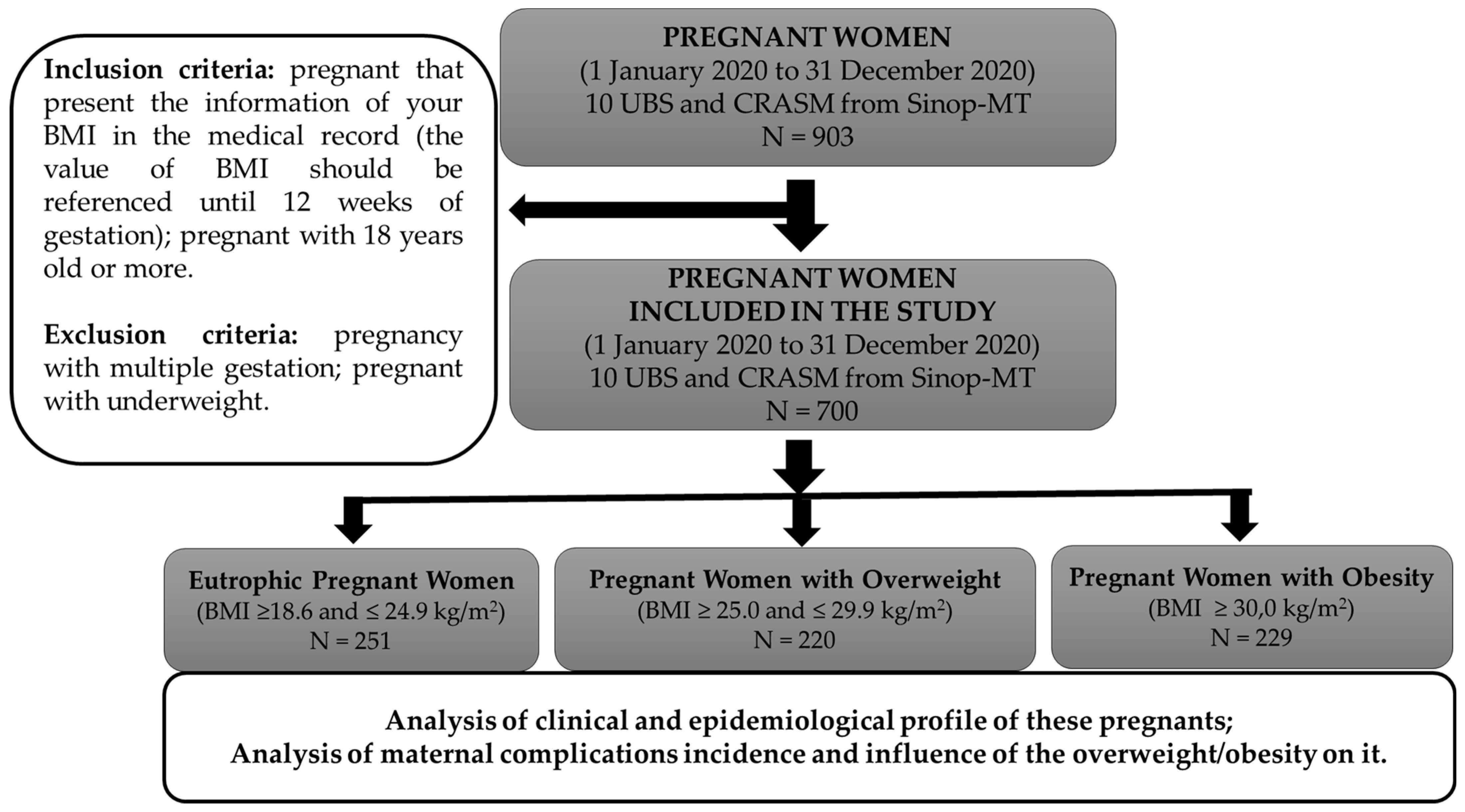
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kahn, B.B.; Flier, J.S. Obesity and insulin resistance. J. Clin. Investig. 2000, 106, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Mohamed-Ali, V.; Pinkney, J.; Coppack, S. Adipose tissue as an endocrine and paracrine organ. Int. J. Obes. 1998, 22, 1145–1158. [Google Scholar] [CrossRef] [PubMed]
- ABESO; da obesidade, M. Assoc. Bras. Para o Estud. Da Obesidade e Da Síndrome Metabólica. 2021. Available online: https://abeso.org.br/obesidade-e-sindrome-metabolica/mapa-da-obesidade/ (accessed on 5 February 2024).
- Dhurandhar, N.V. What is obesity? Int. J. Obes. 2022, 46, 1081–1082. [Google Scholar] [CrossRef]
- Chooi, Y.C.; Ding, C.; Magkos, F. The epidemiology of obesity. Metabolism 2019, 92, 6–10. [Google Scholar] [CrossRef] [PubMed]
- WHO. World Heath Organization. Obes. Overweight. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 29 June 2022).
- Kopelman, P.G. Obesity as a medical problem. Nature 2000, 404, 635–643. [Google Scholar] [CrossRef] [PubMed]
- David, L.S.; Lima, C.D.A.; Santos, V.M.; Pena, G.D.G.; Brito, M.F.S.F.; Silva, R.R.V.; de Pinho, L. Prevalence and associated factors on overweight/obesity in pregnant women assisted by the Family Health Strategy. Rev. Bras. Saúde Matern. Infant. 2023, 23, e20220354. [Google Scholar] [CrossRef]
- Timur, B.B.; Timur, H.; Tokmak, A.; Isik, H.; Eyi, E.G.Y. The Influence of Maternal Obesity on Pregnancy Complications and Neonatal Outcomes in Diabetic and Nondiabetic Women. Geburtshilfe Frauenheilkd. 2018, 78, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Leung, T.Y.; Leung, T.N.; Sahota, D.S.; Chan, O.K.; Chan, L.W.; Fung, T.Y.; Lau, T.K. Trends in maternal obesity and associated risks of adverse pregnancy outcomes in a population of Chinese women. BJOG 2008, 115, 1529–1537. [Google Scholar] [CrossRef] [PubMed]
- Machado, C.; Monteiro, S.; Oliveira, M.J. Impact of overweight and obesity on pregnancy outcomes in women with gestational diabetes–results from a retrospective multicenter study. Arch. Endocrinol. Metab. 2020, 64, 45–51. [Google Scholar] [CrossRef]
- Khalak, R.; Cummings, J.; Dexter, S. Maternal obesity: Significance on the preterm neonate. Int. J. Obes. 2015, 39, 1433–1436. [Google Scholar] [CrossRef]
- Bedell, S.; Hutson, J.; de Vrijer, B.; Eastabrook, G. Effects of Maternal Obesity and Gestational Diabetes Mellitus on the Placenta: Current Knowledge and Targets for Therapeutic Interventions. Curr. Vasc. Pharmacol. 2020, 19, 176–192. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.-W.; Soh, S.E.; Tint, M.-T.; Loy, S.L.; Yap, F.; Tan, K.H.; Lee, Y.S.; Shek, L.P.-C.; Godfrey, K.M.; Gluckman, P.D.; et al. Combined analysis of gestational diabetes and maternal weight status from pre-pregnancy through post-delivery in future development of type 2 diabetes. Sci. Rep. 2021, 11, 5021. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Xie, Y.; Zhao, M.; Huang, H.; Liu, C.; Huang, F.; Zhang, Y. Effects of moderate-intensity resistance exercise on blood glucose and pregnancy outcome in patients with gestational diabetes mellitus: A randomized controlled trial. J. Diabetes Complicat. 2022, 36, 108186. [Google Scholar] [CrossRef] [PubMed]
- Kemp, B.J.; Creighton, R.M.; Cupples, G.; Kelly, B.; McAuley, E.; Fleck, O.; Wallace, H.; Graham, U.; McCance, D.R. Mothers’ experiences of a lifestyle intervention for weight reduction 12 months after gestational diabetes mellitus: Qualitative findings from the PAIGE2 study. Midwifery 2024, 129, 103911. [Google Scholar] [CrossRef] [PubMed]
- Adamczak, L.; Mantaj, U.; Sibiak, R.; Gutaj, P.; Wender-Ozegowska, E. Physical activity, gestational weight gain in obese patients with early gestational diabetes and the perinatal outcome—A randomised–controlled trial. BMC Pregnancy Childbirth 2024, 24, 104. [Google Scholar] [CrossRef] [PubMed]
- Basu, A.; Feng, D.; Planinic, P.; Ebersole, J.L.; Lyons, T.J.; Alexander, J.M. Dietary Blueberry and Soluble Fiber Supplementation Reduces Risk of Gestational Diabetes in Women with Obesity in a Randomized Controlled Trial. J. Nutr. 2021, 151, 1128–1138. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, N.; Joisten, C. Impact of physical activity on course and outcome of pregnancy from pre- to postnatal. Eur. J. Clin. Nutr. 2021, 75, 1698–1709. [Google Scholar] [CrossRef] [PubMed]
- Muktabhant, B.; Lawrie, T.A.; Lumbiganon, P.; Laopaiboon, M. Diet or exercise; or both, for preventing excessive weight gain in pregnancy. Cochrane Database Syst. Rev. 2015, CD007145. [Google Scholar] [CrossRef] [PubMed]
- Różańska-Walędziak, A.; Walędziak, M.; Mierzejewska, A.; Skopińska, E.; Jędrysik, M.; Chełstowska, B. Nutritional Implications of Bariatric Surgery on Pregnancy Management—A Narrative Review of the Literature. Medicina 2023, 59, 1864. [Google Scholar] [CrossRef]
- Walędziak, M.; Kacperczyk-Bartnik, J.; Bartnik, P.; Czajkowski, K.; Kwiatkowski, A.; Różańska-Walędziak, A. The influence of gestational weight gain after bariatric procedures on selected pregnancy outcomes: A single center study. Sci. Rep. 2021, 11, 21120. [Google Scholar] [CrossRef]
- IBGE. IBGE (INSTITUTO Bras. Geogr. E ESTATÍSTICA)/Cid.|Mato Grosso|Sinop|História Fotos. 2023. Available online: https://cidades.ibge.gov.br/brasil/mt/sinop/historico (accessed on 16 October 2023).
- Frick, M.N.; Frizzo, G.G. Prevalência de anemia e seus fatores determinantes em gestantes de município do Estado do RS. Rev. Contexto Saúde 2018, 18, 69–76. [Google Scholar] [CrossRef]
- SBD–Sociedade Brasileira de Diabetes, Diretrizes Sociedade Brasileira de Diabetes 2019–2020., São Paulo, 2020. Available online: https://www.saude.ba.gov.br/wp-content/uploads/2020/02/Diretrizes-Sociedade-Brasileira-de-Diabetes-2019-2020.pdf (accessed on 5 February 2024).
- Sortica, G.H.; Cardozo, A.C.; Silva, G.L.; Azevedo, M.; Lemos, N.A. Guia do Pré-Natal na Atenção Básica, 1st ed.; Secretaria de Estado da Saúde do Rio Grande do Sul-Departamento de Ações em Saúde/Departamento de Assistência Hospitalar e Ambulatorial/Assessoria Técnica de Planejamento: Porto Alegre, Brazil, 2018. [Google Scholar]
- Silva, J.C.; do Amaral, A.R.; Ferreira, B.D.S.; Willeman, I.K.M.; e Silva, M.R.; Salles, W.B. Obesidade materna e suas consequências na gestação e no parto: Uma revisão sistemática. FEMINA 2014, 42, 135–140. [Google Scholar]
- Nomura, R.M.Y.; Paiva, L.V.; Costa, V.N.; Liao, A.W.; Zugaib, M. Influência do estado nutricional materno, ganho de peso e consumo energético sobre o crescimento fetal, em gestações de alto risco. Rev. Bras. Ginecol. Obstet. 2012, 34, 107–112. [Google Scholar] [CrossRef]
- Konno, S.C.; Benicio, M.H.D.A.; Barros, A.J.D. Fatores associados à evolução ponderal de gestantes: Uma análise multinível. Rev. Saúde Pública 2007, 41, 995–1002. [Google Scholar] [CrossRef]
- Leite, A.C.D.N.M.T.; Araújo, K.K.B.C. Diástase dos retos abdominais em puérperas e sua relação com variáveis obstétricas. Fisioter. Mov. 2012, 25, 389–397. [Google Scholar] [CrossRef]
- de Souza, C.K.L. Frequência da Classificação Sanguínea no Laboratório de Análises Clínicas (LAC) do Hospital Distrital de Itaporanga (HDI); Trabalho de Conclusão de Curso (Graduação em Farmácia)—Universidade Esatdual da Paraíba, Centro de Ciências Biológicas e da Saúde: Campina Grande-Paraíba, Brazil, 2012. [Google Scholar]
- BRASIL. Manual Técnico. Pré-Natal e Puerpério: Atenção Qualificada e Humanizada; Ministério da Saúde: Brasília, Brazil, 2005.
- Tilg, H.; Moschen, A.R. Adipocytokines: Mediators linking adipose tissue, inflammation and immunity. Nat. Rev. Immunol. 2006, 6, 772–783. [Google Scholar] [CrossRef]
- Monod, C.; Kotzaeridi, G.; Linder, T.; Yerlikaya-Schatten, G.; Wegener, S.; Mosimann, B.; Henrich, W.; Tura, A.; Göbl, C.S. Maternal overweight and obesity and its association with metabolic changes and fetal overgrowth in the absence of gestational diabetes mellitus: A prospective cohort study. Acta Obstet. Gynecol. Scand. 2024, 103, 257–265. [Google Scholar] [CrossRef]
- O’Malley, E.G.; Reynolds, C.M.E.; Killalea, A.; O’Kelly, R.; Sheehan, S.R.; Turner, M.J. Maternal obesity and dyslipidemia associated with gestational diabetes mellitus (GDM). Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 246, 67–71. [Google Scholar] [CrossRef]
- Kivelä, J.; Sormunen-Harju, H.; Girchenko, P.V.; Huvinen, E.; Stach-Lempinen, B.; Kajantie, E.; Villa, P.M.; Reynolds, R.M.; Hämäläinen, E.K.; Lahti-Pulkkinen, M.; et al. Longitudinal Metabolic Profiling of Maternal Obesity, Gestational Diabetes, and Hypertensive Pregnancy Disorders. J. Clin. Endocrinol. Metab. 2021, 106, e4372–e4388. [Google Scholar] [CrossRef] [PubMed]
- Callaway, L.K.; Chang, A.M.; McIntyre, H.D.; Prins, J.B. The prevalence and impact of overweight and obesity in an Australian obstetric population. Med. J. Aust. 2006, 184, 56–59. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Shen, Z.; Zhan, Y.; Wang, Y.; Ma, S.; Zhang, S.; Liu, J.; Wu, S.; Feng, Y.; Chen, Y.; et al. Effects of pre-pregnancy body mass index and gestational weight gain on maternal and infant complications. BMC Pregnancy Childbirth 2020, 20, 390. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro, L.G.V.; Soares, C.L.R.; Lima, B.L.O.; Sanches, N.M.; Oliveira, R.K.; de Queiroz, D.A.; de Queiroz, E.A.I.F. Obesidade, gestação e complicações maternas e neonatais: Uma revisão sistemática. Sci. Electron. Arch. 2023, 16, 68–85. [Google Scholar] [CrossRef]
- Saha, D.; Roy, P.; Koley, A.K.; Saha, A.; Dey, B.C.; Ari, M.; Ganguly, T.K.; Mukhopadhyaya, A.K. Maternal bmi—How it affect obstetric behaviour and pregnancy outcome. J. Evol. Med. Dent. Sci. 2013, 2, 6622–6630. [Google Scholar] [CrossRef]
- Neal, K.; Ullah, S.; Glastras, S.J. Obesity Class Impacts Adverse Maternal and Neonatal Outcomes Independent of Diabetes. Front. Endocrinol. 2022, 13, 832678. [Google Scholar] [CrossRef]
- West, S.; Ollila, M.; Franks, S.; Piltonen, T.; Jokelainen, J.; Nevalainen, J.; Puukka, K.; Ruokonen, A.; Järvelin, M.; Auvinen, J.; et al. Overweight, obesity and hyperandrogenemia are associated with gestational diabetes mellitus: A follow-up cohort study. Acta Obstet. Gynecol. Scand. 2020, 99, 1311–1319. [Google Scholar] [CrossRef]
- Denison, F.; Norwood, P.; Bhattacharya, S.; Duffy, A.; Mahmood, T.; Morris, C.; Raja, E.; Norman, J.; Lee, A.; Scotland, G. Association between maternal body mass index during pregnancy, short-term morbidity, and increased health service costs: A population-based study. BJOG Int. J. Obstet. Gynaecol. 2014, 121, 72–81. [Google Scholar] [CrossRef]
- Fuchs, F.; Senat, M.-V.; Rey, E.; Balayla, J.; Chaillet, N.; Bouyer, J.; Audibert, F. Impact of maternal obesity on the incidence of pregnancy complications in France and Canada. Sci. Rep. 2017, 7, 10859. [Google Scholar] [CrossRef]
- He, M.; Curran, P.; Raker, C.; Martin, S.; Larson, L.; Bourjeily, G. Placental findings associated with maternal obesity at early pregnancy. Pathol.-Res. Pract. 2016, 212, 282–287. [Google Scholar] [CrossRef]

{kind=link}
| Variables | Eutrophic | Overweight | Obese | Total | p |
|---|---|---|---|---|---|
| Pregnant women (n (%)) | 251 (35.9) | 220 (31.4) | 229 (32.7) | 700 (100.0) | - |
| Age (years) & | 23 (20–27) | 27 (23–31) *** | 27 (23–33) *** | 25 (22–30) | <0.0001 |
| Body weight (kg) & | 56.5 (52.9–61.4) | 70.0 (65.2–37.7) *** | 88.7 (82.1–97.2) ***/### | 70.0 (60.0–83.20) | <0.0001 |
| Height (m) & | 1.60 (1.56–1.64) | 1.60 (1.56–1.65) | 1.61 (1.57–1.67) * | 1.60 (1.56–1.65) | 0.02 |
| BMI (kg/m2) & | 22.5 (21.1–23.8) | 27.2 (26.2–28.4) *** | 33.6 (31.6–37.0) ***/### | 27.1 (23.6–31.5) | <0.0001 |
| Marital status | 251 (35.9) | 220 (31.4) | 229 (32.7) | 700 (100.0) | 0.07 |
| Single | 38 (15.1) | 17 (7.8) | 17 (7.4) | 72 (10.2) | |
| Married/common-law marriage | 77 (30.7) | 76 (34.5) | 65 (28.3) | 218 (31.2) | |
| Others | 46 (18.3) | 31 (14.1) | 22 (9.7) | 99 (14.2) | |
| Unavailable data | 90 (35.9) | 96 (43.6) | 125 (54.6) | 311 (44.4) | |
| Ethnicity | 251 (35.9) | 220 (31.4) | 229 (32.7) | 700 (100.0) | 0.94 |
| Asian | 2 (0.8) | 1 (0.5) | 1 (0.4) | 4 (0.6) | |
| White | 49 (19.5) | 45 (20.5) | 29 (12.7) | 123 (17.6) | |
| Hispanic | 93 (37.1) | 71 (32.2) | 57 (24.9) | 221 (31.6) | |
| Black | 7 (2.8) | 3 (1.3) | 4 (1.8) | 14 (2.0) | |
| Unavailable data | 100 (39.8) | 100 (45.5) | 138 (60.2) | 338 (48.2) | |
| Number of pregnancies | 251 (35.9) | 220 (31.4) | 229 (32.7) | 700 (100.0) | 0.0004 |
| 1 | 101 (40.2) | 63 (28.7) | 46 (20.0) | 210 (30.0) | |
| 2 | 65 (25.9) | 48 (21.8) | 60 (26.2) | 173 (24.8) | |
| 3 | 46 (18.3) | 43 (19.5) | 40 (17.5) | 129 (18.4) | |
| 4 | 14 (5.6) | 25 (11.3) | 28 (12.2) | 67 (9.6) | |
| >4 | 12 (4.8) | 22 (10.0) | 22 (9.7) | 56 (8.0) | |
| Unavailable data | 13 (5.2) | 19 (8.7) | 33 (14.4) | 65 (9.2) | |
| ABO-Rh | 251 (35.9) | 220 (31.4) | 229 (32.7) | 700 (100.0) | 0.63 |
| A+ | 40 (15.9) | 29 (13.1) | 26 (11.3) | 95 (13.6) | |
| A− | 5 (2.0) | 5 (2.2) | 4 (1.8) | 14 (2.0) | |
| B+ | 11 (4.4) | 13 (6.0) | 8 (3.5) | 32 (4.6) | |
| B− | 1 (0.4) | 1 (0.5) | 1 (0.4) | 3 (0.4) | |
| AB+ | 6 (2.4) | 7 (3.1) | 2 (0.8) | 15 (2.1) | |
| AB− | 0 (0.0) | 2 (1.0) | 1 (0.4) | 3 (0.4) | |
| O+ | 82 (32.7) | 59 (26.9) | 48 (21.0) | 189 (27.0) | |
| O− | 15 (6.0) | 6 (2.7) | 2 (0.8) | 23 (3.3) | |
| Unavailable data | 91 (36.2) | 98 (44.5) | 137 (60.0) | 326 (46.6) | |
| First trimester exams | |||||
| Blood count | |||||
| Hemoglobin & | 12.8 (12.1–13.6) | 13.1 (12.3–13.7) | 13.1 (12.5–13.9) | 13.1 (12.2–13.7) | 0.15 |
| Hematocrit & | 37.6 (35.9–39.2) | 38.3 (36.3–39.9) | 38.9 (36.8–41.0) * | 38.2 (36.3–39.9) | 0.03 |
| Anemia | 251 (35.9) | 220 (31.4) | 229 (32.7) | 700 (100.0) | 0.46 |
| Yes | 8 (3.2) | 6 (2.7) | 2 (0.9) | 16 (2.3) | |
| No | 122 (48.6) | 103 (46.8) | 80 (34.9) | 305 (43.6) | |
| Unavailable data | 121 (48.2) | 111 (50.5) | 147 (64.2) | 379 (54.1) | |
| Glycemia (mg/dL) & | 80 (76–84) | 84 (79–88) * | 85 (78–90) ** | 82 (78–88) | <0.001 |
| Blood glucose range | 251 (35.9) | 220 (31.4) | 229 (32.7) | 700 (100.0) | 0.18 |
| <92 mg/dL | 121 (48.2) | 94 (42.7) | 71 (31.0) | 286 (40.9) | |
| 92 to 125 mg/dL (GDM) | 12 (4.8) | 13 (5.9) | 15 (6.6) | 40 (5.7) | |
| Unavailable data | 118 (47) | 113 (51.4) | 143 (62.4) | 374 (53.4) | |
| Second or third trimester exams | |||||
| Blood count | |||||
| Hemoglobin | 12.0 ± 0.8 | 12.0 ± 0.9 | 12.1 ± 1.0 | 12.0 ± 0.9 | 0.14 |
| Hematocrit | 35.8 ± 2.2 | 35.9 ± 2.7 | 36.7 ± 2.5 | 35.9 ± 2.5 | 0.07 |
| Anemia | 251 (35.9) | 220 (31.4) | 229 (32.7) | 700 (100.0) | 0.32 |
| Yes | 7 (2.8) | 3 (1.4) | 6 (2.6) | 16 (2.3) | |
| No | 65 (25.9) | 41 (18.6) | 29 (12.7) | 135 (19.3) | |
| Unavailable data | 179 (71.3) | 176 (80) | 194 (84.7) | 549 (78.4) | |
| Glycemia (mg/dL) & | 77 (72–82) | 77 (75–83) | 81 (76–86) | 78 (74–83) | 0.08 |
| Blood glucose range | 251 (35.9) | 220 (31.4) | 229 (32.7) | 700 (100.0) | 0.63 |
| <92 mg/dL | 56 (22.3) | 35 (15.9) | 25 (10.9) | 116 (16.6) | |
| 92 to 125 mg/dL (GDM) | 3 (1.2) | 3 (1.4) | 3 (1.3) | 9 (1.3) | |
| Unavailable data | 192 (76.5) | 182 (82.7) | 201 (87.8) | 575 (82.1) |
| Variable | Eutrophic | Overweight | Obese | Total | p |
|---|---|---|---|---|---|
| Pregnant women (n (%)) | 251 (35.9) | 220 (31.4) | 229 (32.7) | 700 (100.0) | -- |
| Disease diagnosed before pregnancy | |||||
| Diabetes mellitus | 251 (35.9) | 220 (31.4) | 229 (32.7) | 700 (100.0) | 0.03 |
| Yes | 2 (0.8) | 4 (1.8) | 9 (3.9) | 15 (2.2) | |
| No | 214 (85.3) | 176 (80.0) | 159 (69.4) | 549 (78.4) | |
| No information | 35 (13.9) | 40 (18.2) | 61 (26.7) | 136 (19.4) | |
| Arterial hypertension | 251 (35.9) | 220 (31.4) | 229 (32.7) | 700 (100.0) | <0.0001 |
| Yes | 0 (0.0) | 7 (3.2) | 18 (7.9) | 25 (3.6) | |
| No | 218 (86.9) | 174 (79.1) | 154 (67.2) | 546 (78.0) | |
| No information | 33 (13.1) | 39 (17.7) | 57 (24.9) | 129 (18.4) | |
| Dyslipidemia | 251 (35.9) | 220 (31.4) | 229 (32.7) | 700 (100.0) | 0.09 |
| Yes | 0 (0.0) | 3 (1.4) | 4 (1.8) | 7 (1.0) | |
| No | 217 (86.5) | 175 (79.5) | 159 (69.4) | 551 (78.7) | |
| No information | 34 (13.5) | 42 (19.1) | 66 (28.8) | 142 (20.3) | |
| Maternal complications | |||||
| Gestational diabetes | 251 (35.9) | 220 (31.4) | 229 (32.7) | 700 (100.0) | <0.0001 |
| Yes | 6 (2.4) | 14 (6.4) | 28 (12.2) | 48 (6.8) | |
| No | 204 (81.3) | 157 (71.4) | 142 (62.0) | 503 (71.9) | |
| No information | 41 (16.3) | 49 (22.3) | 59 (25.8) | 149 (21.3) | |
| Gestational hypertension | 251 (35.9) | 220 (31.4) | 229 (32.7) | 700 (100.0) | <0.0001 |
| Yes | 3 (1.2) | 15 (6.8) | 29 (12.7) | 47 (6.7) | |
| No | 204 (81.3) | 153 (69.5) | 133 (58.0) | 490 (70.0) | |
| No information | 44 (17.5) | 52 (23.7) | 67 (29.3) | 163 (23.3) | |
| Pre-eclampsia | 251 (35.9) | 220 (31.4) | 229 (32.7) | 700 (100.0) | 0.003 |
| Yes | 0 (0.0) | 4 (1.8) | 9 (3.9) | 13 (1.9) | |
| No | 206 (82.1) | 162 (73.6) | 155 (67.7) | 523 (74.7) | |
| No information | 45 (17.9) | 54 (24.6) | 65 (28.4) | 164 (23.4) | |
| Eclampsia | 251 (35.9) | 220 (31.4) | 229 (32.7) | 700 (100.0) | 0.32 |
| Yes | 0 (0.0) | 0 (0.0) | 1 (0.4) | 1 (0.1) | |
| No | 207 (82.5) | 165 (75) | 161 (70.3) | 533 (76.2) | |
| No information | 44 (17.5) | 55 (25) | 67 (29.3) | 166 (23.7) |
| Variable | Eutrophic | Overweight/ Obese | Total | RR | p |
|---|---|---|---|---|---|
| Pregnant women (n (%)) | 251 (35.9) | 449 (64.1) | 700 (100.0) | -- | -- |
| Disease diagnosed before pregnancy | |||||
| Diabetes mellitus | 251 (35.9) | 449 (64.1) | 700 (100.0) | ||
| Yes | 2 (0.8) | 13 (2.9) | 15 (2.2) | 4.03 | 0.04 |
| No | 214 (85.2) | 335 (74.7) | 549 (78.4) | (1.03–15.9) | |
| No information | 35 (14.0) | 101 (22.4) | 136 (19.4) | ||
| Arterial hypertension | 251 (35.9) | 449 (64.1) | 700 (100.0) | ||
| Yes | 0 (0.0) | 25 (5.6) | 25 (3.6) | Infinity | <0.0001 |
| No | 218 (86.9) | 328 (73.1) | 546 (78.0) | (2.00–infinity) | |
| No information | 33 (13.1) | 96 (21.3) | 129 (18.4) | ||
| Dyslipidemia | 251 (35.9) | 449 (64.1) | 700 (100.0) | ||
| Yes | 0 (0.0) | 7 (1.6) | 7 (1.0) | Infinity | 0.03 |
| No | 217 (86.5) | 334 (74.3) | 551 (78.8) | (1.17–infinity) | |
| No information | 34 (13.5) | 108 (24.1) | 142 (20.2) | ||
| Maternal complications | |||||
| Gestational diabetes | 251 (35.9) | 449 (64.1) | 700 (100.0) | ||
| Yes | 6 (2.4) | 42 (9.4) | 48 (6.8) | 4.31 | 0.0001 |
| No | 204 (81.3) | 299 (66.6) | 503 (71.9) | (1.93–9.79) | |
| No information | 41 (16.3) | 108 (24.0) | 149 (21.3) | ||
| Gestational hypertension | 251 (35.9) | 449 (64.1) | 700 (100.0) | ||
| Yes | 3 (1.2) | 44 (9.8) | 47 (6.7) | 9.20 | <0.0001 |
| No | 204 (81.3) | 286 (63.7) | 490 (70.0) | (3.10–27.77) | |
| No information | 44 (17.5) | 119 (26.5) | 163 (23.3) | ||
| Pre-eclampsia | 251 (35.9) | 449 (64.1) | 700 (100.0) | ||
| Yes | 0 (0.0) | 13 (2.9) | 13 (1.9) | Infinity | 0.004 |
| No | 206 (82.1) | 317 (70.6) | 523 (74.7) | (2.00–infinity) | |
| No information | 45 (17.9) | 119 (26.5) | 164 (23.4) | ||
| Eclampsia | 251 (35.9) | 449 (64.1) | 700 (100.0) | 0.43 | |
| Yes | 0 (0.0) | 1 (0.2) | 1 (0.1) | Infinity | |
| No | 207 (82.5) | 326 (72.6) | 533 (76.2) | (0.17–infinity) | |
| No information | 44 (17.5) | 122 (27.2) | 166 (23.7) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pinheiro, L.G.V.; Sanches, N.M.; Soares, C.L.R.; Lima, B.L.O.; Ramos, E.B.; Ferreira, M.S.; Loiola, M.O.; Silva, R.R.; Prates, J.S.N.; Silva, V.C.; et al. Obesity Increases Maternal Complications in Pregnant Women of Sinop: A Retrospective Cohort Study. Obesities 2024, 4, 118-131. https://doi.org/10.3390/obesities4020012
Pinheiro LGV, Sanches NM, Soares CLR, Lima BLO, Ramos EB, Ferreira MS, Loiola MO, Silva RR, Prates JSN, Silva VC, et al. Obesity Increases Maternal Complications in Pregnant Women of Sinop: A Retrospective Cohort Study. Obesities. 2024; 4(2):118-131. https://doi.org/10.3390/obesities4020012
Chicago/Turabian StylePinheiro, Lilian G. V., Nathalia M. Sanches, Catharine L. R. Soares, Bruna L. O. Lima, Eduarda B. Ramos, Mariany S. Ferreira, Matheus O. Loiola, Rafaella R. Silva, João Sérgio N. Prates, Viviani C. Silva, and et al. 2024. "Obesity Increases Maternal Complications in Pregnant Women of Sinop: A Retrospective Cohort Study" Obesities 4, no. 2: 118-131. https://doi.org/10.3390/obesities4020012
APA StylePinheiro, L. G. V., Sanches, N. M., Soares, C. L. R., Lima, B. L. O., Ramos, E. B., Ferreira, M. S., Loiola, M. O., Silva, R. R., Prates, J. S. N., Silva, V. C., Queiroz, D. A., & Queiroz, E. A. I. F. (2024). Obesity Increases Maternal Complications in Pregnant Women of Sinop: A Retrospective Cohort Study. Obesities, 4(2), 118-131. https://doi.org/10.3390/obesities4020012