


Preparation of Injectable Dicalcium Phosphate Bone Cement for Potential Orthopedic Applications



Abstract
1. Introduction
2. Materials and Methods
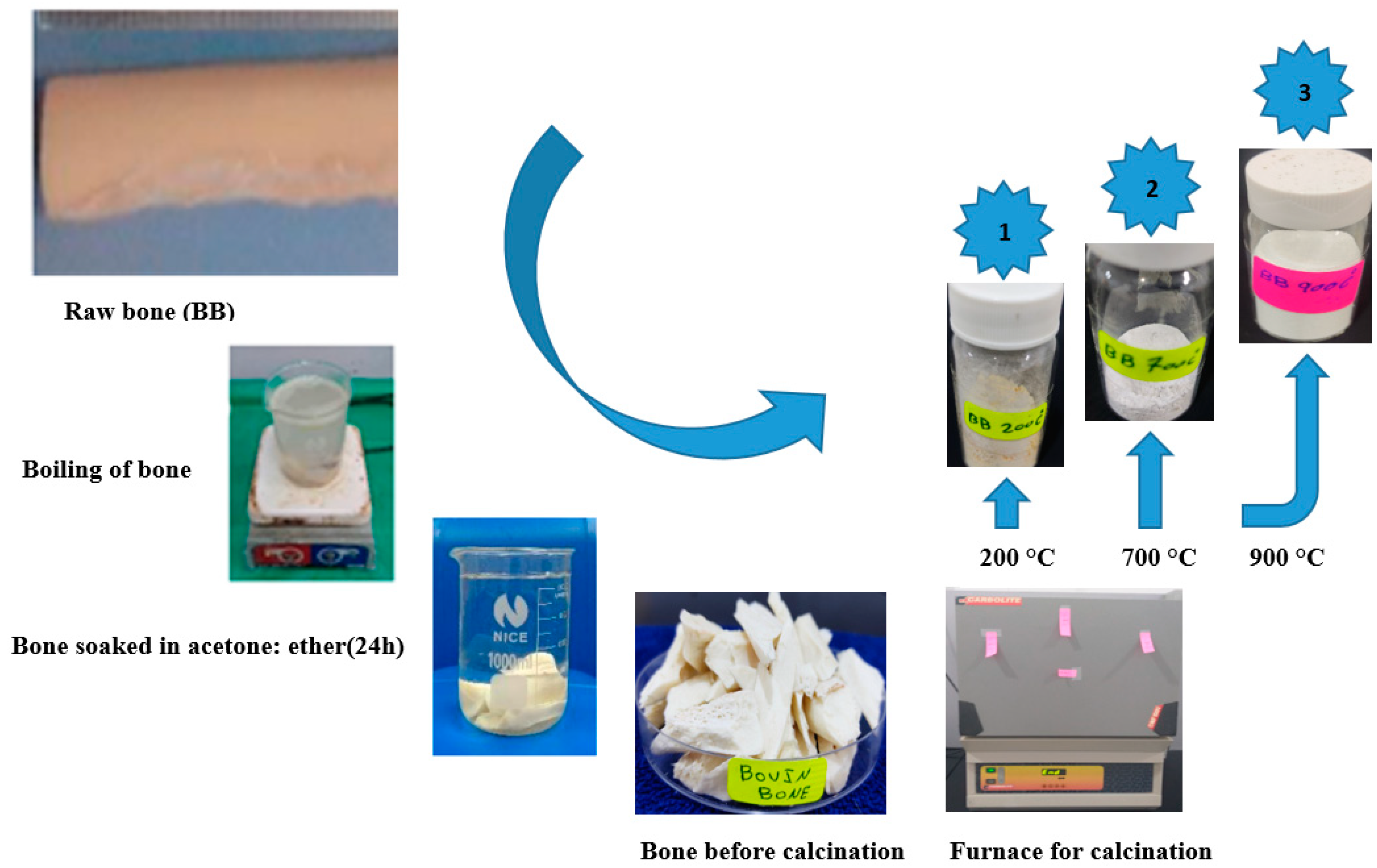
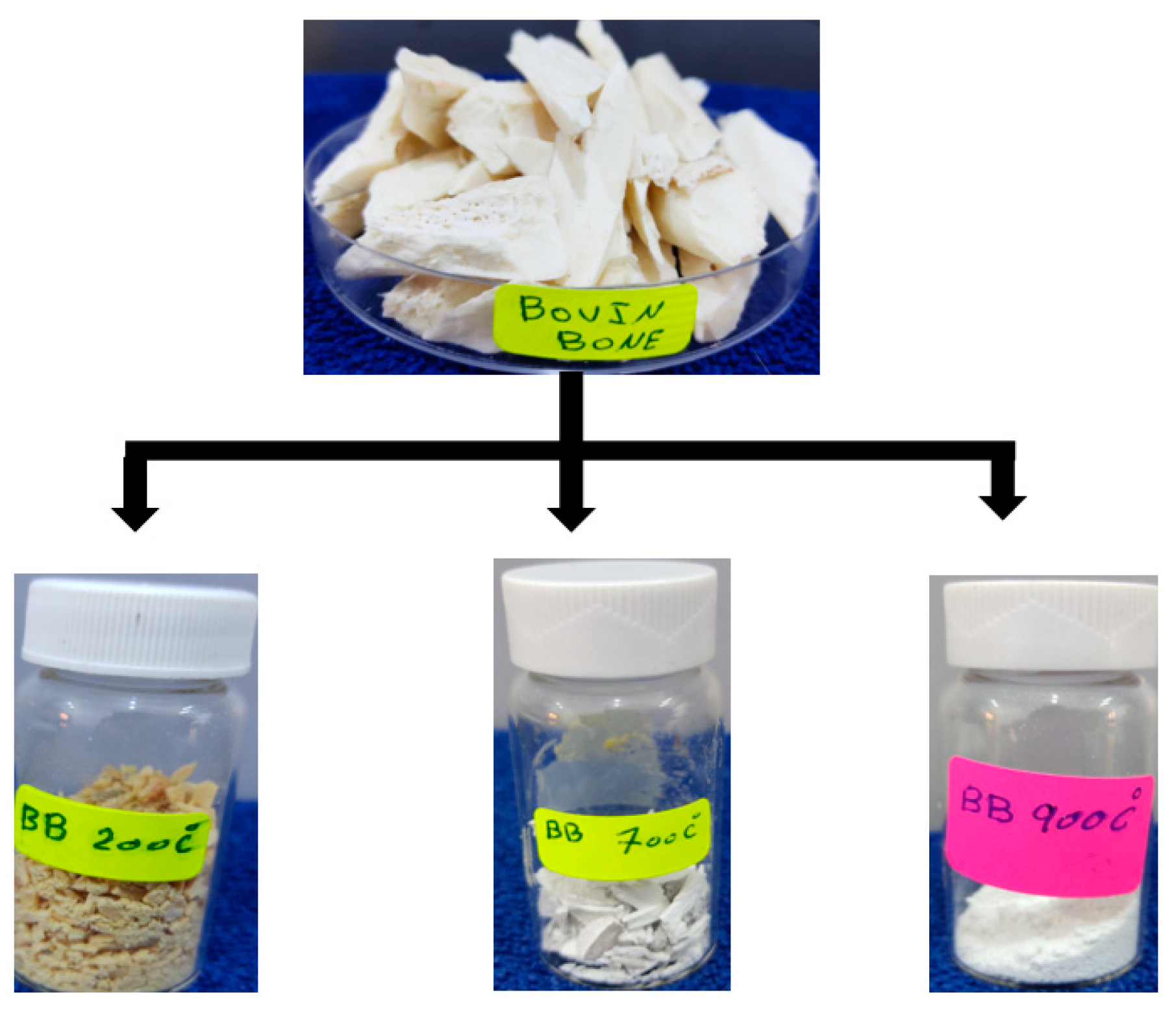
2.1. Preparation of HA
2.2. Cement Preparation
2.3. Setting Time
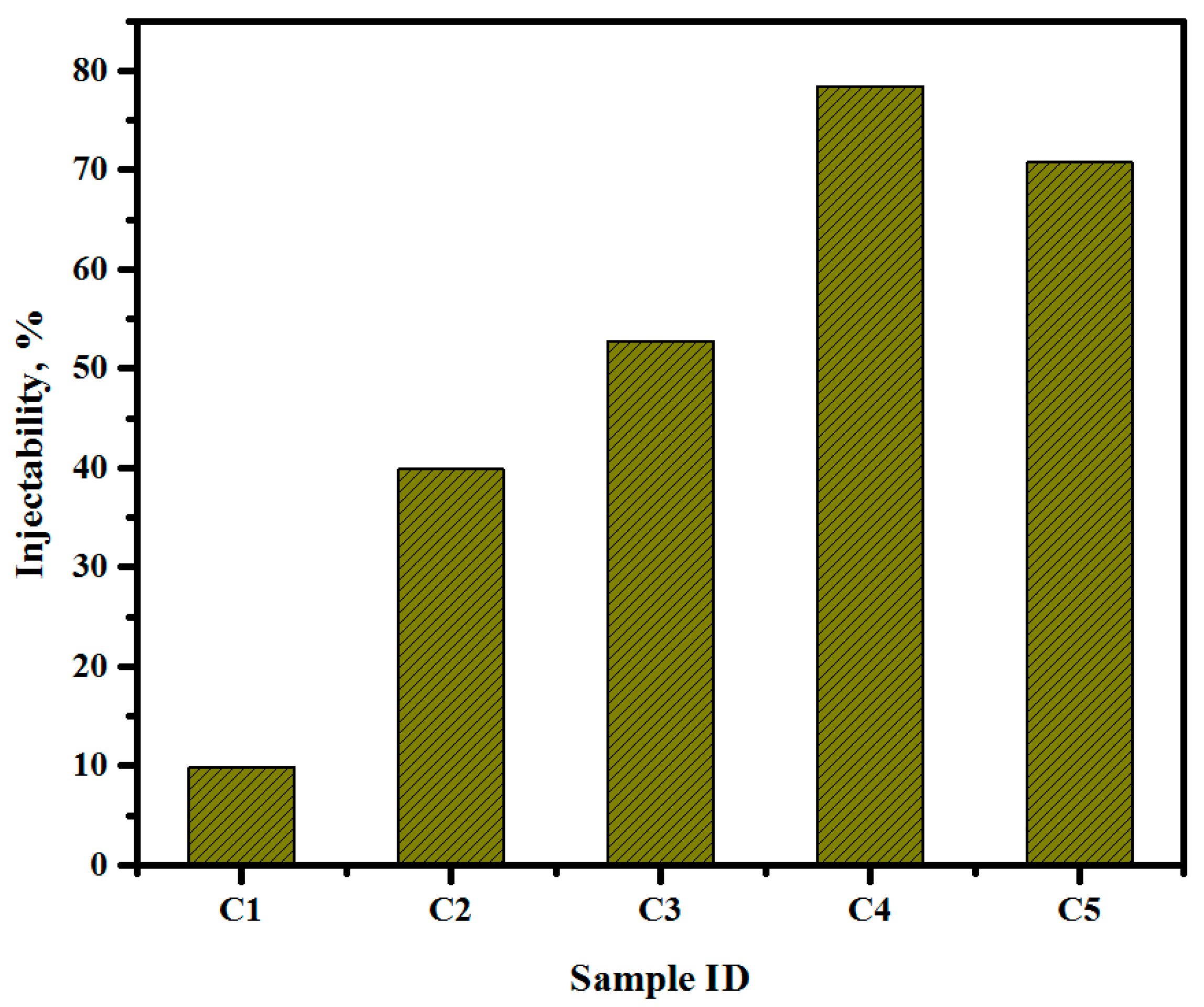
2.4. Injection Ability of Cement Specimen
2.5. Compressive Strength Test
2.6. In Vitro Ion Release Analysis
3. Results and Discussion
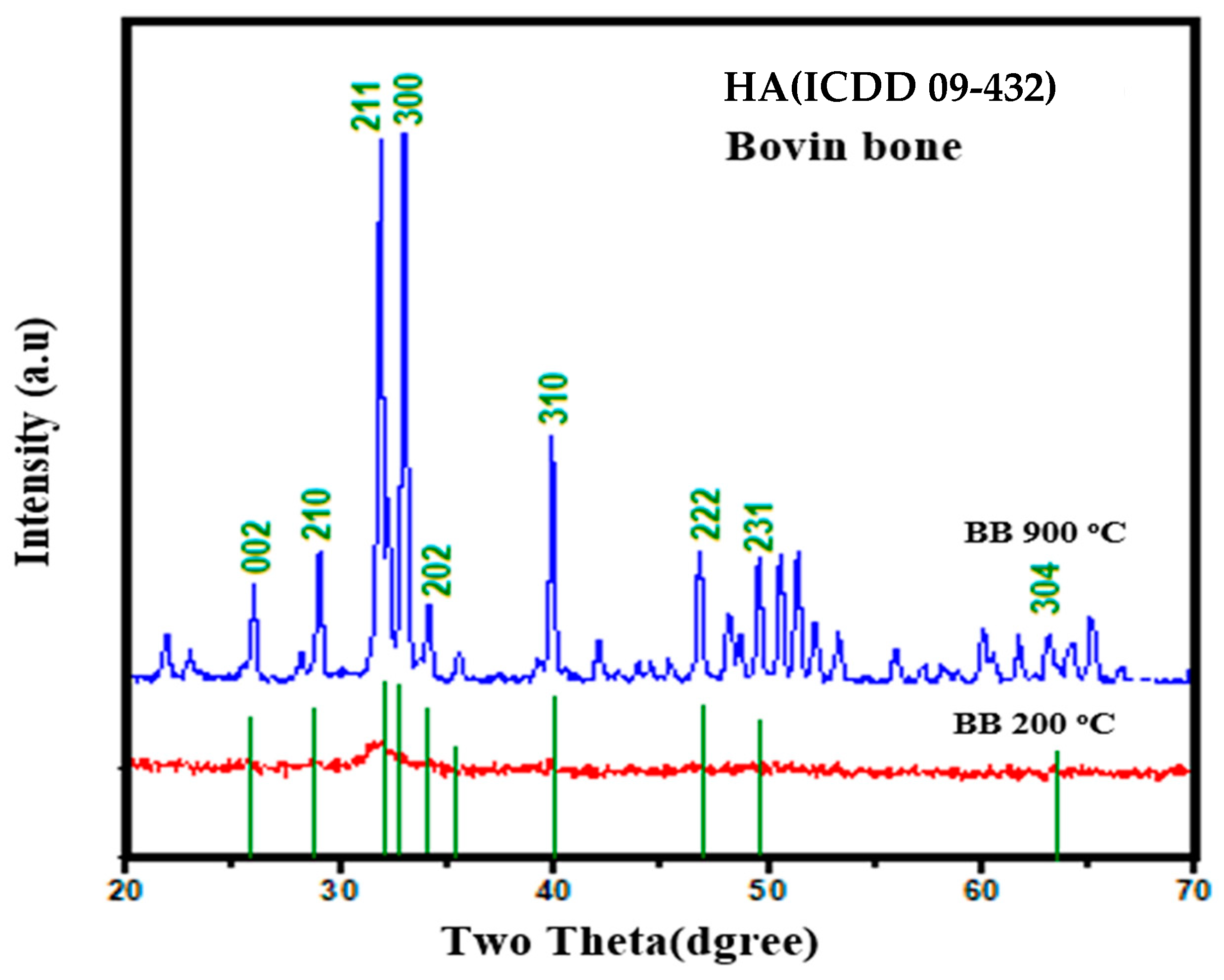
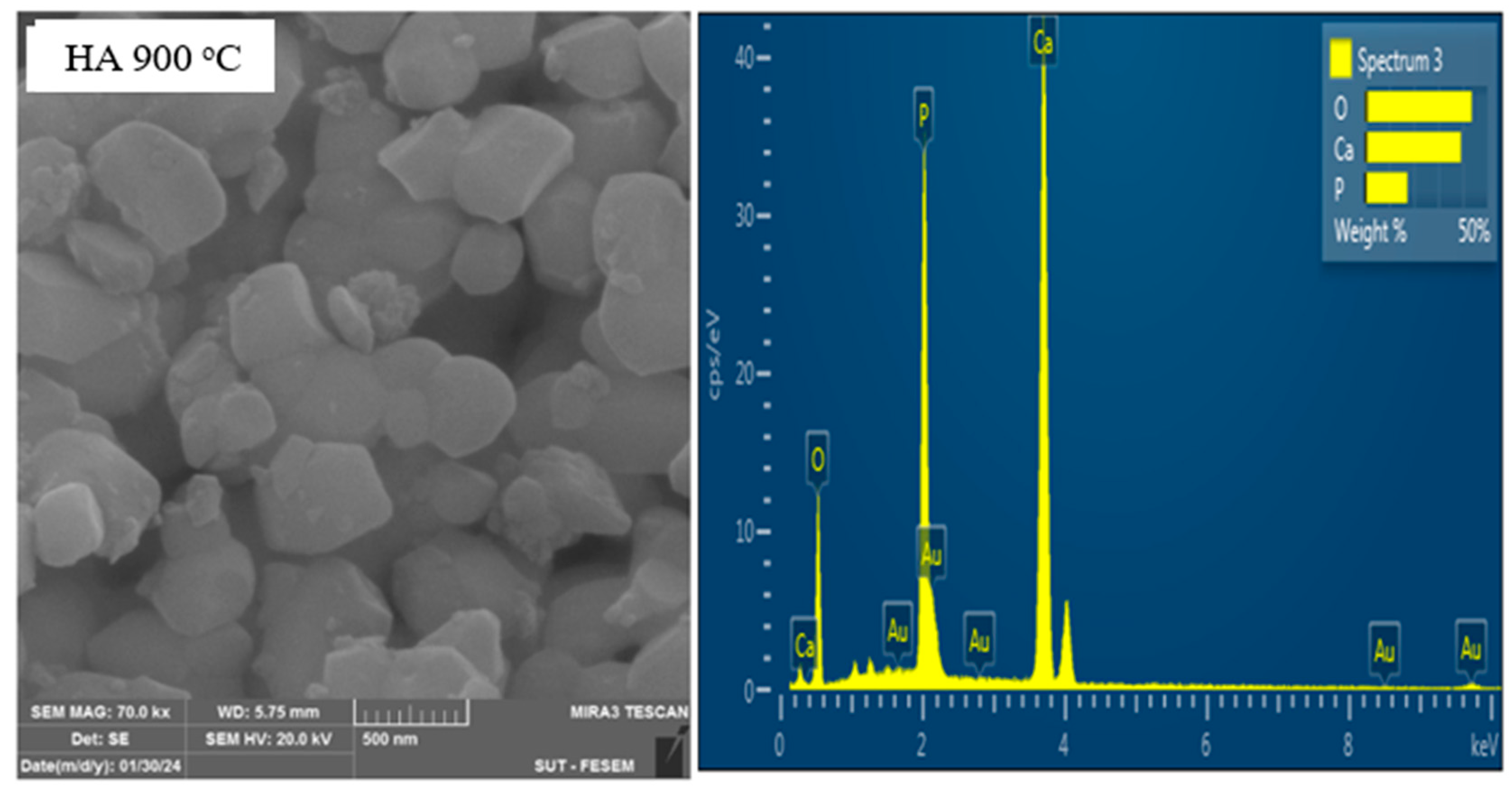
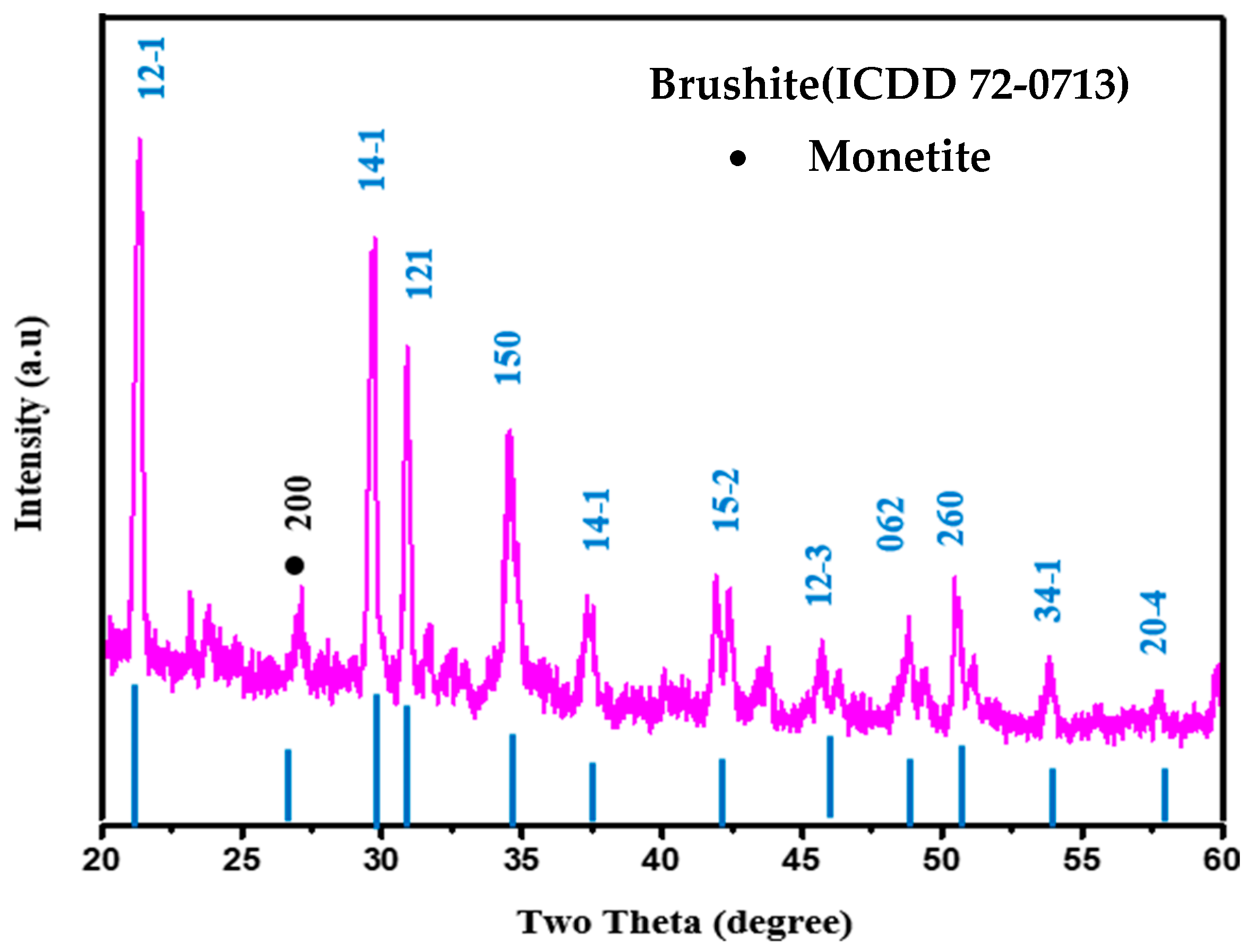
3.1. Phase Analysis of Calcined HA
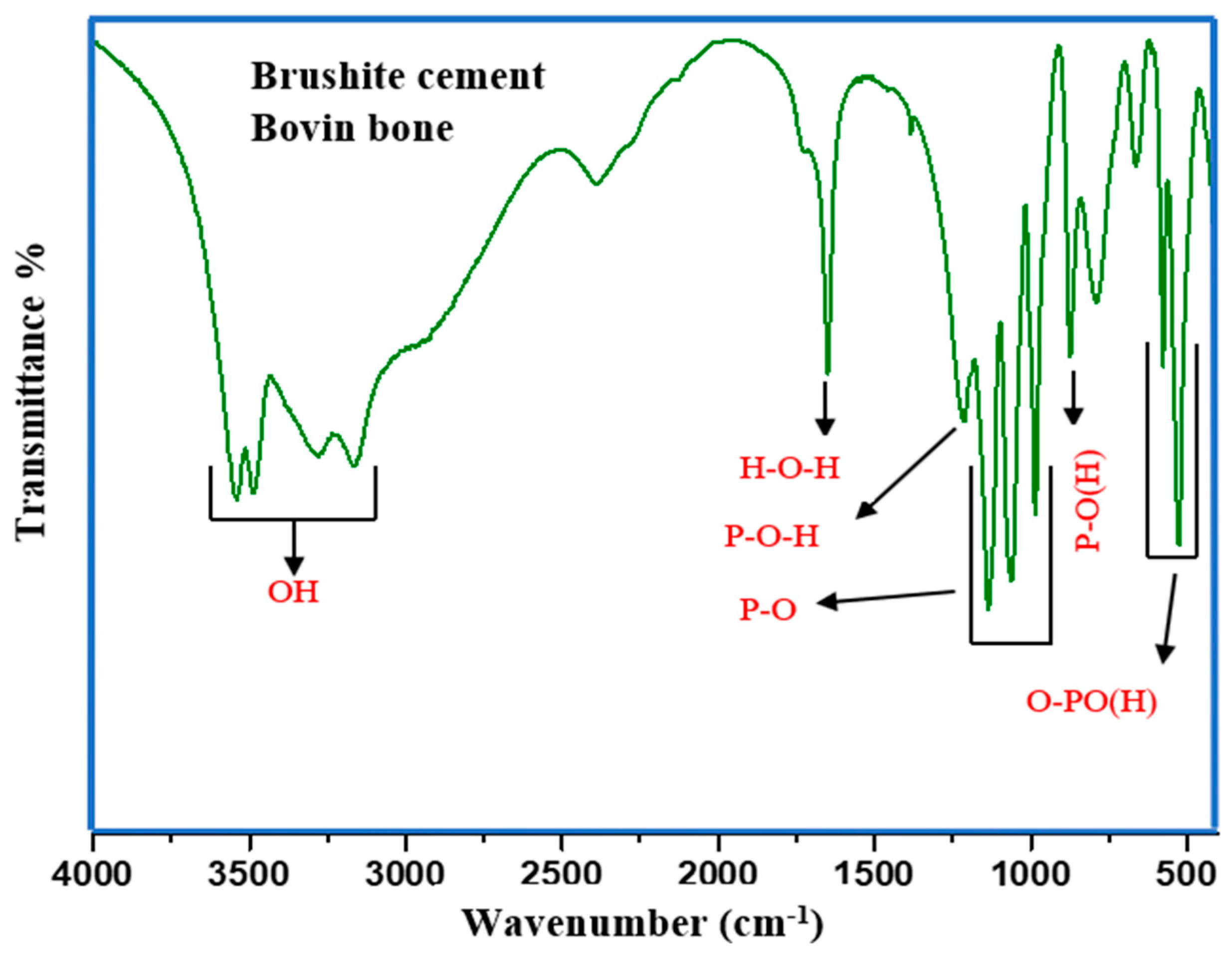
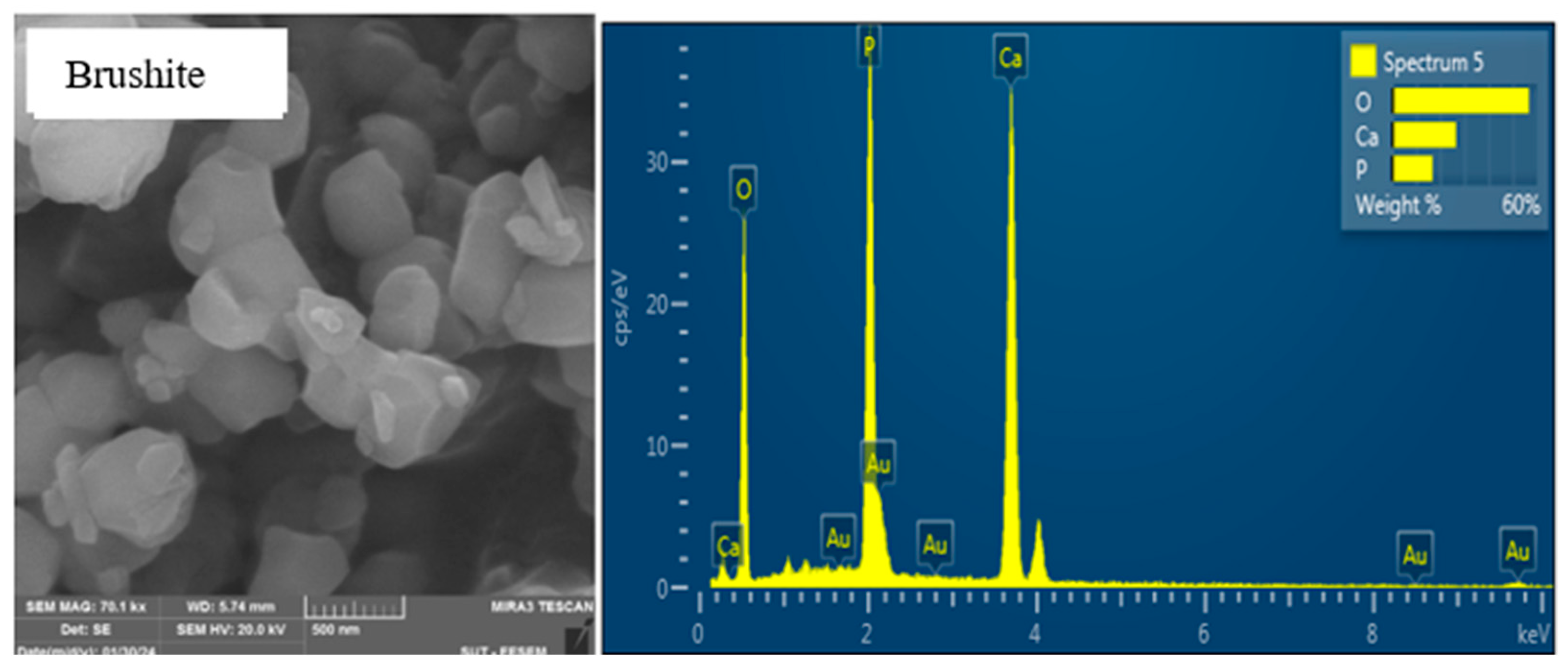
3.2. Structure and Morphology of DCPD Cement
3.3. In Vitro Study (Setting Time and Injectability)
3.4. Release of Ions from Cement Specimen
3.5. Comparison of Injectable Dicalcium Phosphate with Previous Studies
4. Conclusions
- The bovine bone-extracted HA was shown to be a promising substitute for synthetic HA.
- The microstructure of the obtained HA revealed agglomeration and a non-uniform distribution of spherical grains of varied sizes and orientations.
- The crystal structures and phases of both HA and brushite cement were tallied with synthetic HA.
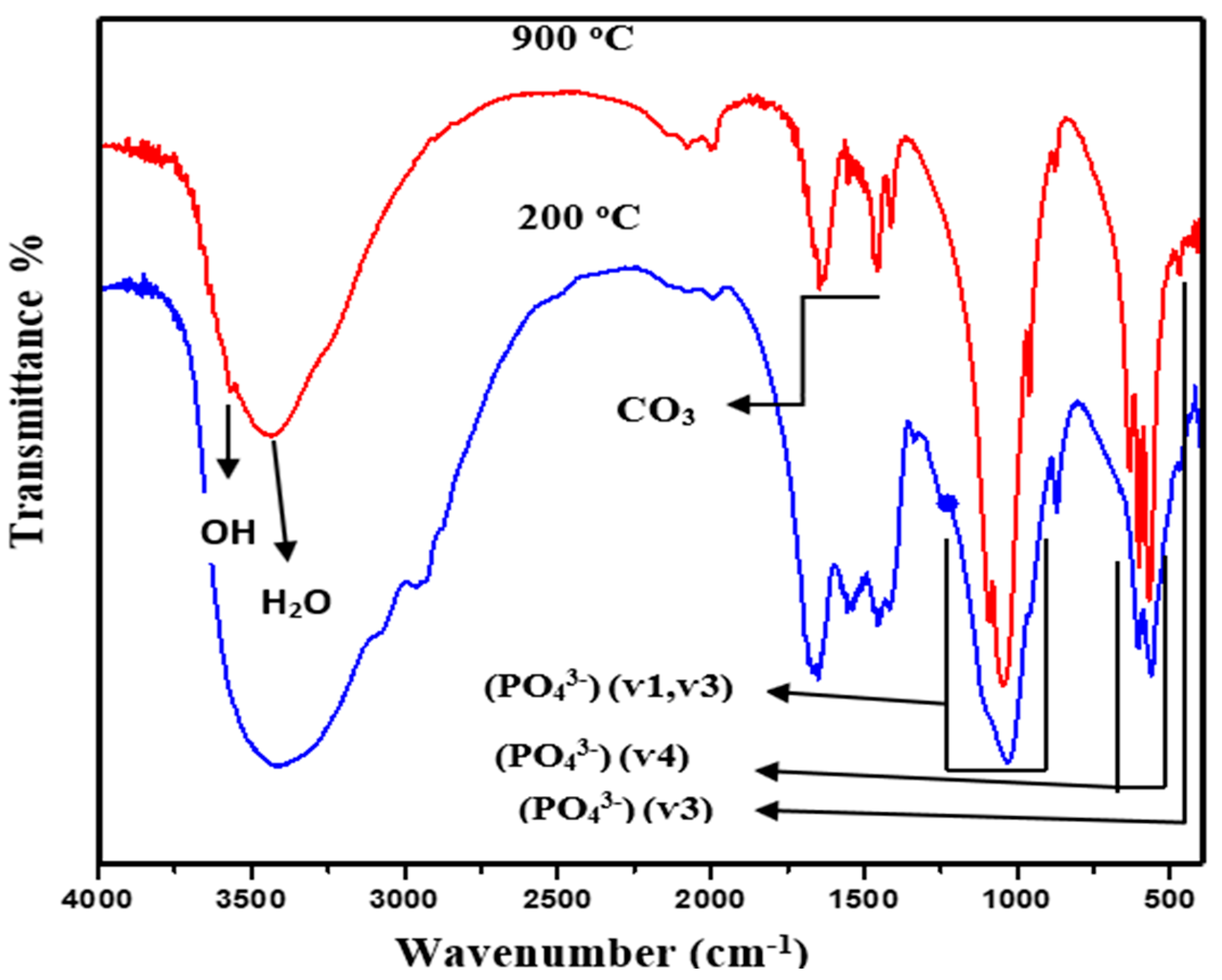
- The analysis results of the FTIR spectra showed various characteristic functional groups of the HA phase and structures.
- It was demonstrated that the prepared injectable dicalcium phosphate bone cement has high potential in orthopedic applications.
- The bovine bone-extracted HA-based injectable inorganic matrix showed excellent mechanical performance and setting times.
- The proposed cement paste is established to be efficient in the continual release of ions desirable for invasive surgical applications.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BC | Bone cement. |
| CPBC | Calcium phosphate-based bone cement. |
| CPC | Calcium phosphate-based cement. |
| CS | Compressive strength. |
| DCP | Di-calcium phosphate. |
| DCPD | Di-calcium phosphate di-hydrate. |
| EDX | Energy dispersive X-ray. |
| FESEM | Field emission scanning electron microscopy. |
| FTIR | Fourier-transformed infrared spectroscopy. |
| HA | Hydroxyapatite. |
| MCPM | Monocalcium phosphate monohydrate. |
| XRD | X-ray diffraction. |
References
- Demir-Oğuz, Ö.; Boccaccini, A.R.; Loca, D. Injectable bone cements: What benefits the combination of calcium phosphates and bioactive glasses could bring? Bioact. Mater. 2023, 19, 217–236. [Google Scholar] [CrossRef]
- Burguera, E.F.; Xu, H.H.; Takagi, S.; Chow, L.C. High early strength calcium phosphate bone cement: Effects of dicalcium phosphate dihydrate and absorbable fibers. J. Biomed. Mater. Res. Part A Off. J. Soc. Biomater. Jpn. Soc. Biomater. Aust. Soc. Biomater. Korean Soc. Biomater. 2005, 75, 966–975. [Google Scholar] [CrossRef]
- Huang, Y.-C.; Hsiao, P.-C.; Chai, H.-J. Hydroxyapatite extracted from fish scale: Effects on MG63 osteoblast-like cells. Ceram. Int. 2011, 37, 1825–1831. [Google Scholar] [CrossRef]
- Habraken, W.; Habibovic, P.; Epple, M.; Bohner, M. Calcium phosphates in biomedical applications: Materials for the future? Mater. Today 2016, 19, 69–87. [Google Scholar] [CrossRef]
- Burguera, E.F.; Xu, H.H.; Weir, M.D. Injectable and rapid-setting calcium phosphate bone cement with dicalcium phosphate dihydrate. J. Biomed. Mater. Res. Part B Appl. Biomater. Off. J. Soc. Biomater. Jpn. Soc. Biomater. Aust. Soc. Biomater. Korean Soc. Biomater. 2006, 77, 126–134. [Google Scholar] [CrossRef]
- Dorozhkin, S.V. Calcium orthophosphate cements for biomedical application. J. Mater. Sci. 2008, 43, 3028–3057. [Google Scholar] [CrossRef]
- Arkin, V.H.; Narendrakumar, U.; Madhyastha, H.; Manjubala, I. Characterization and in vitro evaluations of injectable calcium phosphate cement doped with magnesium and strontium. ACS Omega 2021, 6, 2477–2486. [Google Scholar] [CrossRef] [PubMed]
- Alge, D.L.; Santa Cruz, G.; Goebel, W.S.; Chu, T.-M.G. Characterization of dicalcium phosphate dihydrate cements prepared using a novel hydroxyapatite-based formulation. Biomed. Mater. 2009, 4, 025016. [Google Scholar] [CrossRef]
- Deng, K.; Chen, H.; Dou, W.; Cai, Q.; Wang, X.; Wang, S.; Wang, D. Preparation and characterization of porous HA/β-TCP biphasic calcium phosphate derived from butterfish bone. Mater. Technol. 2022, 37, 1388–1395. [Google Scholar] [CrossRef]
- Bohner, M.; Theiss, F.; Apelt, D.; Hirsiger, W.; Houriet, R.; Rizzoli, G.; Gnos, E.; Frei, C.; Auer, J.A.; von Rechenberg, B. Compositional changes of a dicalcium phosphate dihydrate cement after implantation in sheep. Biomaterials 2003, 24, 3463–3474. [Google Scholar] [CrossRef]
- Manalu, J.; Soegijono, B.; Indrani, D. Characterization of Hydroxyapatite Derived from Bovine Bone. Appl. Sci. 2015, 3, 2777. [Google Scholar]
- Monballiu, A.; Desmidt, E.; Ghyselbrecht, K.; Meesschaert, B. Phosphate recovery as hydroxyapatite from nitrified UASB effluent at neutral pH in a CSTR. J. Environ. Chem. Eng. 2018, 6, 4413–4422. [Google Scholar] [CrossRef]
- Engstrand, J.; Persson, C.; Engqvist, H. The effect of composition on mechanical properties of brushite cements. J. Mech. Behav. Biomed. Mater. 2014, 29, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Sun, R.-X.; Lv, Y.; Niu, Y.-R.; Zhao, X.-H.; Cao, D.-S.; Tang, J.; Sun, X.-C.; Chen, K.-Z. Physicochemical and biological properties of bovine-derived porous hydroxyapatite/collagen composite and its hydroxyapatite powders. Ceram. Int. 2017, 43, 16792–16798. [Google Scholar] [CrossRef]
- Hu, M.-H.; Chu, P.-Y.; Huang, S.-M.; Shih, B.-S.; Ko, C.-L.; Hu, J.-J.; Chen, W.-C. Injectability, processability, drug loading, and antibacterial activity of gentamicin-impregnated mesoporous bioactive glass composite calcium phosphate bone cement in vitro. Biomimetics 2022, 7, 121. [Google Scholar] [CrossRef] [PubMed]
- Tariq, U.; Haider, Z.; Chaudhary, K.; Hussain, R.; Ali, J. Calcium to phosphate ratio measurements in calcium phosphates using LIBS. In Proceedings of the Journal of Physics: Conference Series, Johor Bahru, Malaysia, 26–28 September 2017; p. 012015. [Google Scholar]
- Hsu, H.-C.; Tuan, W.-H.; Lee, H.-Y. In-situ observation on the transformation of calcium phosphate cement into hydroxyapatite. Mater. Sci. Eng. C 2009, 29, 950–954. [Google Scholar] [CrossRef]
- Taha, A.; Akram, M.; Jawad, Z.; Alshemary, A.Z.; Hussain, R. Strontium doped injectable bone cement for potential drug delivery applications. Mater. Sci. Eng. C 2017, 80, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Zhu, L.; Tian, F.; Wang, C.; Wu, W.; Lu, B.; Yan, L.; Jia, S.; Hao, D. In vitro and in vivo evaluation of injectable strontium-modified calcium phosphate cement for bone defect repair in rats. Int. J. Mol. Sci. 2022, 24, 568. [Google Scholar] [CrossRef] [PubMed]
- Shahrezaei, M.; Shahrouzi, J.; Hesaraki, S.; Zamanian, A. The Effect of?-TCP Particle Size on Mechanical and Setting Properties of Calcium Phosphate Bone Cements. J. Arch. Mil. Med. 2014, 2, 16516. [Google Scholar] [CrossRef]
- ASTM-C266; Standard Test Method for Time of Setting of Hydraulic Cement Paste by Gillmore Needles. ASTM: West Conshohocken, PA, USA, 1989.
- ASTM F451-99a; Standard Specification for Acrylic Bone Cement. ASTM: West Conshohocken, PA, USA, 1999.
- Saleh, A.T.; Ling, L.S.; Hussain, R. Injectable magnesium-doped brushite cement for controlled drug release application. J. Mater. Sci. 2016, 51, 7427–7439. [Google Scholar] [CrossRef]
- Schröter, L.; Kaiser, F.; Stein, S.; Gbureck, U.; Ignatius, A. Biological and mechanical performance and degradation characteristics of calcium phosphate cements in large animals and humans. Acta Biomater. 2020, 117, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Grafe, I.A.; Baier, M.; Nöldge, G.; Weiss, C.; Da Fonseca, K.; Hillmeier, J.; Libicher, M.; Rudofsky, G.; Metzner, C.; Nawroth, P. Calcium-phosphate and polymethylmethacrylate cement in long-term outcome after kyphoplasty of painful osteoporotic vertebral fractures. Spine 2008, 33, 1284–1290. [Google Scholar] [CrossRef] [PubMed]
- Apelt, D.; Theiss, F.; El-Warrak, A.; Zlinszky, K.; Bettschart-Wolfisberger, R.; Bohner, M.; Matter, S.; Auer, J.A.; von Rechenberg, B. In vivo behavior of three different injectable hydraulic calcium phosphate cements. Biomaterials 2004, 25, 1439–1451. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, H.; Fujishiro, T.; Belkoff, S.M.; Kobayashi, N.; Turner, A.S.; Seim, H.B., III; Zitelli, J.; Hawkins, M.; Bauer, T.W. Long-term evaluation of a calcium phosphate bone cement with carboxymethyl cellulose in a vertebral defect model. J. Biomed. Mater. Res. Part A Off. J. Soc. Biomater. Jpn. Soc. Biomater. Aust. Soc. Biomater. Korean Soc. Biomater. 2009, 88, 880–888. [Google Scholar] [CrossRef] [PubMed]
- Maenz, S.; Kunisch, E.; Mühlstädt, M.; Böhm, A.; Kopsch, V.; Bossert, J.; Kinne, R.W.; Jandt, K.D. Enhanced mechanical properties of a novel, injectable, fiber-reinforced brushite cement. J. Mech. Behav. Biomed. Mater. 2014, 39, 328–338. [Google Scholar] [CrossRef]
- Ammann, P. Strontium ranelate: A novel mode of action leading to renewed bone quality. Osteoporos. Int. 2005, 16, S11–S15. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample ID | Solid Phase | Liquid Phase |
|---|---|---|
| MCPM to HA | Trisodium Citrate (mL) | |
| C1 | 4:1 | 1.0 (1 M) |
| C2 | 1:4 | 1.0 (0.25 M) |
| C3 | 2:2 | 1.0 (0.5 M) |
| C4 | 1:4 | 0.5 (0.1 M) |
| C5 | 1:2 | 0.5 (0.1 M) |
| Samples | Chemical Formula Ca10(PO4)6 (OH)2 | Lattice Parameter | Xc (%) | D (nm) | ||
|---|---|---|---|---|---|---|
| a (Å) | c (Å) | V (Å3) | ||||
| HA (pre-calcined) | Ca5(PO4)3(OH) | 9.418 | 6.884 | 528.8 | ---- | ---- |
| HA (post-calcined) | Ca10(PO4)6(OH)2 | 9.418 | 6.877 | 527.8 | 87 | 98.12 |
| IR Band Position (cm−1) | Band Assignments |
|---|---|
| 3547−3467; 3266−3146 | O−H stretching vibration of H2O |
| 2936 | (P)O−H stretching modes |
| 2392 | H−O−H bending plus residual free H2O |
| 1620−1720 (broad) | H−O−H bending of H2O molecules |
| 1653 | P−O−H in-plane bending |
| 1207 | P−O−H in-plane bending |
| 1135 | P−O stretching |
| 1065 | P−O stretching |
| 984 | P−O stretching |
| 871 | P−O(OH) stretching |
| 784 | P−O(OH) out-of-plane bending |
| 663 | H2O liberations |
| 569 | O−P−O(H) bending mode |
| Specimen | CS, MPa | |||
|---|---|---|---|---|
| 0 h | 24 h | 72 h | 168 h | |
| C1 | 1.23 | 8.4 | 13.52 | 17.24 |
| C2 | 10.35 | 15.7 | 20.37 | 18.82 |
| C3 | 13.24 | 18.63 | 22.52 | 19.47 |
| C4 | 18.27 | 24.21 | 31.45 | 18.32 |
| C5 | 20.18 | 26.22 | 33.75 | 21.79 |
| Immersion Time (hour) | Release of Ca2+ Ionw (mg/L) in SBF |
|---|---|
| Brushite Cement | |
| 0 | 12.22 |
| 24 | 18.22 |
| 72 | 23.35 |
| 168 | 11.43 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wali, K.J.; Saleh, A.T.; Huseien, G.F. Preparation of Injectable Dicalcium Phosphate Bone Cement for Potential Orthopedic Applications. Eng 2024, 5, 1028-1042. https://doi.org/10.3390/eng5020056
Wali KJ, Saleh AT, Huseien GF. Preparation of Injectable Dicalcium Phosphate Bone Cement for Potential Orthopedic Applications. Eng. 2024; 5(2):1028-1042. https://doi.org/10.3390/eng5020056
Chicago/Turabian StyleWali, Kholoud Jabar, Ali Taha Saleh, and Ghasan Fahim Huseien. 2024. "Preparation of Injectable Dicalcium Phosphate Bone Cement for Potential Orthopedic Applications" Eng 5, no. 2: 1028-1042. https://doi.org/10.3390/eng5020056
APA StyleWali, K. J., Saleh, A. T., & Huseien, G. F. (2024). Preparation of Injectable Dicalcium Phosphate Bone Cement for Potential Orthopedic Applications. Eng, 5(2), 1028-1042. https://doi.org/10.3390/eng5020056