
The “Double-Row Shoelace” Capsulodesis: A Novel Technique for the Repair and Reconstruction of the Scapholunate Ligament of the Wrist
 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patient Selection
- Clinical and radiographic (X-rays and MRI) diagnosis of chronic or subacute scapholunate instability (≥3 months from the initial injury).
- Age between 18 and 65 years.
- Absence of advanced rheumatic or degenerative wrist conditions (SLAC stage < II).
- Comminuted carpal fractures.
- Advanced degenerative changes of the ligament or radiocarpal osteoarthritis (SLAC stage ≥ II).
- Previous failed surgical interventions on the SLL.
2.3. Surgical Technique
2.3.1. Pre-Operative Evaluation
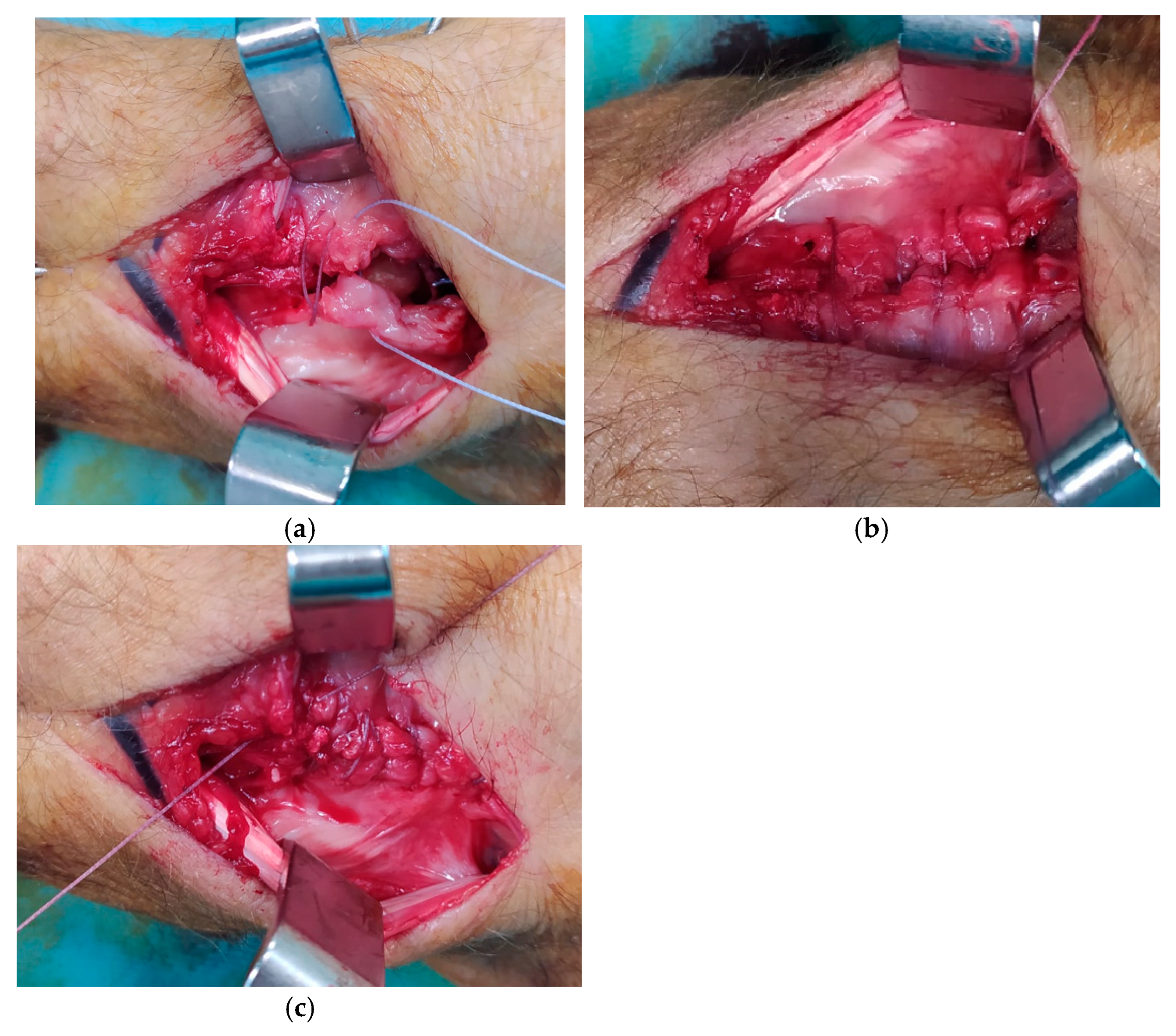
2.3.2. Surgical Procedure
2.3.3. Post-Operative Treatment and Rehabilitation
2.4. Data Elaboration
3. Results
3.1. Pain (VAS)
3.2. Functional Outcomes
3.3. Scapho-Lunate Gap
3.4. Scapho-Lunate Angle
3.5. Complications
3.6. Individual Outcomes
3.7. Summary of Findings
3.8. Statistical Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| SLIL | Scapho-Lunate Interosseus Ligament |
| DISI | Dorsal Intercalated Segment Instability |
| K-wires | Kirshner’s Wires |
| SLAC | Scapho-Lunate Advanced Collapse |
| DCSS | Dorsal Capsule–Scapholunate Septum |
References
- Logan, S.E.; Nowak, M.D. Intrinsic and extrinsic wrist ligaments: Biomechanical and functional differences. Biomed. Sci. Instrum. 1987, 23, 9–13. [Google Scholar]
- Rajan, P.V.; Day, C.S. Scapholunate ligament insufficiency. J. Hand Surg. Am. 2015, 40, 583–585. [Google Scholar] [CrossRef]
- Short, W.H.; Werner, F.W.; Green, J.K.; Masaoka, S. Biomechanical evaluation of the ligamentous stabilizers of the scaphoid and lunate: Part II. J. Hand Surg. Am. 2005, 30, 24–34. [Google Scholar] [CrossRef]
- Short, W.H.; Werner, F.W.; Green, J.K.; Sutton, L.G.; Brutus, J.P. Biomechanical evaluation of the ligamentous stabilizers of the scaphoid and lunate: Part III. J. Hand Surg. Am. 2007, 32, 297–309. [Google Scholar] [CrossRef]
- Smith, D.K.; Gilula, L.A.; Amadio, P.C. Dorsal lunate tilt (DISI configuration): Sign of scaphoid fracture displacement. Radiology 1990, 176, 497–499. [Google Scholar] [CrossRef]
- Strauch, R.J. Scapholunate advanced collapse and scaphoid nonunion advanced collapse arthritis—Update on evaluation and treatment. J. Hand Surg. Am. 2011, 36, 729–735. [Google Scholar] [CrossRef]
- Garcia-Elias, M.; Lluch, A.L.; Stanley, J.K. Three-ligament tenodesis for the treatment of scapholunate dissociation: Indications and surgical technique. J. Hand Surg. Am. 2006, 31, 125–134. [Google Scholar] [CrossRef]
- Blatt, G. Capsulodesis in reconstructive hand surgery. Dorsal capsulodesis for the unstable scaphoid and volar capsulodesis following excision of the distal ulna. Hand Clin. 1987, 3, 81–102. [Google Scholar] [CrossRef]
- Rosenwasser, M.P.; Miyasajsa, K.C.; Strauch, R.J. The RASL procedure: Reduction and association of the scaphoid and lunate using the Herbert screw. Tech. Hand Up. Extrem. Surg. 1997, 1, 263–272. [Google Scholar] [CrossRef]
- Brunelli, G.A.; Brunelli, G.R. A new technique to correct carpal instability with scaphoid rotary subluxation: A preliminary report. J. Hand Surg. 1995, 20, S82–S85. [Google Scholar] [CrossRef]
- Konopka, G.; Chim, H. Optimal management of scapholunate ligament injuries. Orthop. Res. Rev. 2018, 10, 41–54. [Google Scholar] [CrossRef]
- Rajan, P.V.; Day, C.S. Scapholunate Interosseous Ligament Anatomy and Biomechanics. J. Hand Surg. Am. 2015, 40, 1692–1702. [Google Scholar] [CrossRef]
- Zhou, J.Y.; Jodah, R.; Joseph, L.P.; Yao, J. Scapholunate Ligament Injuries. J. Hand Surg. Glob. Online 2024, 6, 245–267. [Google Scholar] [CrossRef]
- Passiatore, M.; De Vitis, R.; Cilli, V.; Milano, G.; Saccomanno, M.F.; Cotroneo, C.; Brozzini, E.; Vigliarolo, D.; Taccardo, G. The Italian Version of the Michigan Hand Outcomes Questionnaire (MHQ): Translation, Cross-Cultural Adaptation and Validation. J. Hand Surg. Asian Pac. 2021, 26, 666–683. [Google Scholar] [CrossRef]
- Padua, R.; Padua, L.; Ceccarelli, E.; Romanini, E.; Zanoli, G.; Amadio, P.C.; Campi, A. Italian version of the Disability of the Arm, Shoulder and Hand (DASH) questionnaire. Cross-cultural adaptation and validation. J. Hand Surg. Br. 2003, 28, 179–186. [Google Scholar] [CrossRef]
- Kitay, A.; Wolfe, S.W. Scapholunate instability: Current concepts in diagnosis and management. J. Hand Surg. 2012, 37, 2175–2196. [Google Scholar] [CrossRef]
- Tommasini Carrara de Sambuy, M.; Burgess, T.M.; Cambon-Binder, A.; Mathoulin, C.L. The anatomy of the dorsal capsulo-scapholunate septum: A cadaveric study. J. Wrist Surg. 2017, 6, 244–247. [Google Scholar] [CrossRef]
- Overstraeten, L.V.; Camus, E.J.; Wahegaonkar, A.; Messina, J.; Tandara, A.A.; Binder, A.C.; Mathoulin, C.L. Anatomical description of the dorsal capsulo-scapholunate septum (DCSS)-arthroscopic staging of scapholunate instability after DCSS sectioning. J. Wrist Surg. 2013, 2, 149–154. [Google Scholar]
- Van Overstraeten, L.; Camus, E.J. Arthroscopic classification of the lesions of the dorsal capsulo-scapholunate septum (DCSS) of the wrist. Tech. Hand Up. Extrem. Surg. 2016, 20, 125–128. [Google Scholar] [CrossRef]
- De Vitis, R.; Passiatore, M.; Perna, A.; Cilli, V.; Ponzo, I.; Taccardo, G. Does the Use of Gelled Platelet-Rich Plasma during Fixation of Subacute Proximal Pole Scaphoid Fractures Help?—A Single Centre Experience. J. Hand Surg. Asian Pac. 2022, 27, 615–622. [Google Scholar] [CrossRef]
- Arnaout, A.; Mathoulin, C. Arthroscopic management of scapholunate complex injuries associated with distal radius fractures. J. Orthop. 2024, 51, 73–80. [Google Scholar] [CrossRef]
- Rocchi, L.; De Vitis, R.; Pietramala, S.; Fulchignoni, C.; D’Orio, M.; Mazzone, V.; Marcuzzi, A. Resurfacing Capitate Pyrocarbon Implant for the treatment of advanced wrist arthritis in the elderly: A retrospective study. Eur. Rev. Med. Pharmacol. Sci. 2022, 26 (Suppl. S1), 92–99. [Google Scholar]
- De Vitis, R.; Passiatore, M.; Cilli, V.; Pamelin, E.; Velluto, C.; Ceravolo, I.; D’Orio, M.; Ferrari, F.; Taccardo, G. Secondary Wrist Arthritis in Active Workers: Does Capitate Pyrocarbon Resurfacing (RCPI) Improve Proximal Row Carpectomy? A Retrospective Cohort Study. J. Hand Surg. Asian Pac. 2021, 26, 625–634. [Google Scholar] [CrossRef]
- Lin, J.S.; Moran, S.L. Proximal row carpectomy or scaphoid excision and four-corner arthrodesis for treatment of scapholunate advanced collapse arthritis. J. Hand Surg. Eur. 2025, 50, 68–75. [Google Scholar] [CrossRef]
- White, N.J.; Raskolnikov, D.; Crow, S.A.; Swart, E.; Rosenwasser, M.P. Reduction and association of the scaphoid and lunate (RASL): Longterm follow-up of a reconstruction technique for chronic scapholunate dissociation. J. Hand Surg. Am. 2017, 35, 16–17. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients | Sex | Age | Pre-op VAS | Post-op VAS | Pre-op qDash | Post-op qDash | Pre-op MHQ | Post-op MHQ | Pre-op SL Gap (mm) | Post-op SL Gap (mm) | Pre-op SL Angle | Post-op SL Angle | Complications |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 65 | 9.00 | 2.00 | 75.25 | 30.25 | 46.4% | 83.2% | 6.20 | 1.80 | 73.00 | 42.00 | |
| 2 | M | 48 | 8.00 | 2.00 | 61.25 | 23.50 | 39.2% | 80.6% | 5.50 | 2.90 | 72.00 | 45.00 | K-wire tracts infection at 15 days post-op |
| 3 | F | 59 | 8.00 | 2.00 | 80.50 | 28.50 | 43.6% | 78.4% | 6.70 | 3.10 | 84.00 | 58.00 | |
| 4 | M | 41 | 6.00 | 2.00 | 56.50 | 26.25 | 56.0% | 81.3% | 5.20 | 2.10 | 71.00 | 39.00 | |
| 5 | M | 44 | 6.00 | 2.00 | 47.25 | 22.75 | 59.6% | 84.3% | 5.30 | 1.00 | 70.00 | 40.00 | K-wire tracts infection at 30 days post-op |
| 6 | M | 39 | 6.00 | 1.00 | 38.25 | 13.25 | 68.3% | 83.4% | 4.90 | 2.20 | 74.00 | 36.00 | |
| 7 | M | 25 | 7.00 | 1.00 | 50.75 | 15.75 | 43.6% | 85.4% | 5.30 | 1.70 | 76.00 | 47.00 | |
| 8 | F | 56 | 7.00 | 1.00 | 55.75 | 19.25 | 46.8% | 77.8% | 5.10 | 3.20 | 70.00 | 54.00 | |
| 9 | M | 50 | 8.00 | 2.00 | 60.5 | 27.75 | 54.7% | 78.8% | 5.40 | 3.10 | 80.00 | 52.00 | |
| 10 | F | 30 | 6.00 | 2.00 | 40.2 | 18.50 | 62.4% | 81.3% | 5.10 | 1.30 | 69.00 | 41.00 | |
| Mean | 7/3 | 45.8 | 7.10 | 1.80 | 56.62 | 22.58 | 52.0% | 81.4% | 5.47 | 2.24 | 73.90 | 45.40 |
| Groups | Patients | Pre-op VAS | Post-op VAS | Pre-op qDash | Post-op qDash | Pre-op MHQ | Post-op MHQ | Pre-op SL Gap (mm) | Post-op SL Gap (mm) | Post-op SL Angle | Pre-op SL Angle |
|---|---|---|---|---|---|---|---|---|---|---|---|
| >50 Y | 1 | 9.00 | 2.00 | 75.25 | 30.25 | 46.4% | 83.2% | 6.20 | 1.80 | 73.00 | 42.00 |
| 3 | 8.00 | 2.00 | 80.50 | 28.50 | 43.6% | 78.4% | 6.70 | 3.10 | 84.00 | 58.00 | |
| 8 | 7.00 | 1.00 | 55.75 | 19.25 | 46.8% | 77.8% | 5.10 | 3.20 | 70.00 | 54.00 | |
| 9 | 8.00 | 2.00 | 60.5 | 27.75 | 54.7% | 78.8% | 5.40 | 3.10 | 80.00 | 52.00 | |
| Mean | 7.75 | 2.00 | 64.11 | 26.25 | 51.8% | 80.4% | 5.85 | 2.33 | 76.50 | 48.25 | |
| <30 Y | 7 | 7.00 | 1.00 | 50.75 | 15.75 | 43.6% | 85.4% | 5.30 | 1.70 | 76.00 | 47.00 |
| 10 | 6.00 | 2.00 | 40.2 | 18.50 | 62.4% | 81.3% | 5.10 | 1.30 | 69.00 | 41.00 | |
| Mean | 6.50 | 1.50 | 45.48 | 17.13 | 53.0% | 83.3% | 5.20 | 1.50 | 72.50 | 44.00 | |
| 30 > Y < 50 | 2 | 8.00 | 2.00 | 61.25 | 23.50 | 39.2% | 80.6% | 5.50 | 2.90 | 72.00 | 45.00 |
| 4 | 6.00 | 2.00 | 56.50 | 26.25 | 56.0% | 81.3% | 5.20 | 2.10 | 71.00 | 39.00 | |
| 5 | 6.00 | 2.00 | 47.25 | 22.75 | 59.6% | 84.3% | 5.30 | 1.00 | 70.00 | 40.00 | |
| 6 | 6.00 | 1.00 | 38.25 | 13.25 | 68.3% | 83.4% | 4.90 | 2.20 | 74.00 | 36.00 | |
| Mean | 6.50 | 1.75 | 50.81 | 21.44 | 55.8% | 82.4% | 5.23 | 2.05 | 71.75 | 40.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cannella, A.; De Vitis, R.; Militerno, A.; Taccardo, G.; Cilli, V.; Rocchi, L.; Sassara, G.M.; Passiatore, M. The “Double-Row Shoelace” Capsulodesis: A Novel Technique for the Repair and Reconstruction of the Scapholunate Ligament of the Wrist. Surgeries 2025, 6, 57. https://doi.org/10.3390/surgeries6030057
Cannella A, De Vitis R, Militerno A, Taccardo G, Cilli V, Rocchi L, Sassara GM, Passiatore M. The “Double-Row Shoelace” Capsulodesis: A Novel Technique for the Repair and Reconstruction of the Scapholunate Ligament of the Wrist. Surgeries. 2025; 6(3):57. https://doi.org/10.3390/surgeries6030057
Chicago/Turabian StyleCannella, Adriano, Rocco De Vitis, Arturo Militerno, Giuseppe Taccardo, Vitale Cilli, Lorenzo Rocchi, Giulia Maria Sassara, and Marco Passiatore. 2025. "The “Double-Row Shoelace” Capsulodesis: A Novel Technique for the Repair and Reconstruction of the Scapholunate Ligament of the Wrist" Surgeries 6, no. 3: 57. https://doi.org/10.3390/surgeries6030057
APA StyleCannella, A., De Vitis, R., Militerno, A., Taccardo, G., Cilli, V., Rocchi, L., Sassara, G. M., & Passiatore, M. (2025). The “Double-Row Shoelace” Capsulodesis: A Novel Technique for the Repair and Reconstruction of the Scapholunate Ligament of the Wrist. Surgeries, 6(3), 57. https://doi.org/10.3390/surgeries6030057