
Thoracic Extradural Psammomatous Meningioma on T6–T8: A Case Report and Literature Review

 ,
,  , , and
, , and
Abstract
1. Introduction
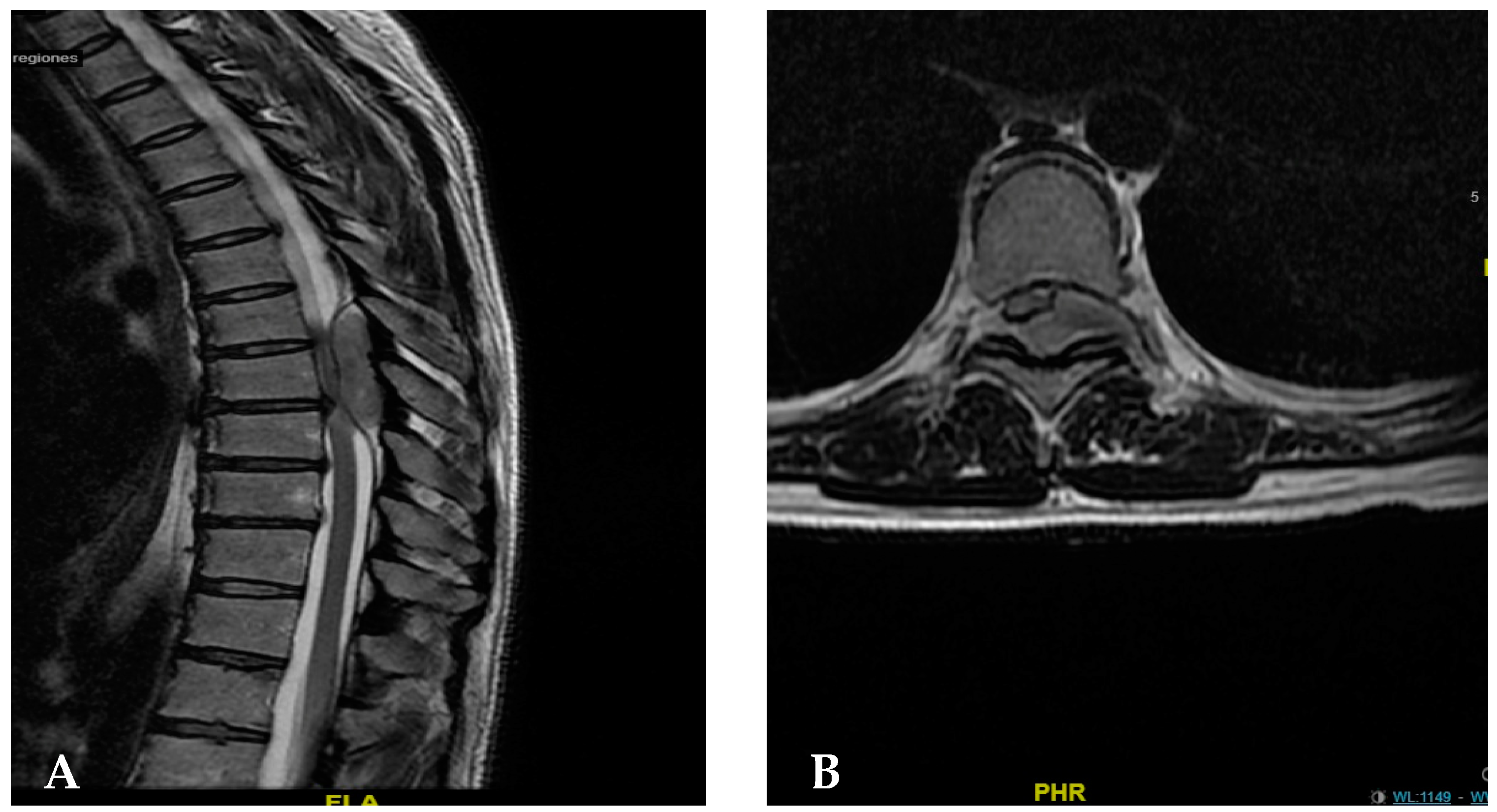
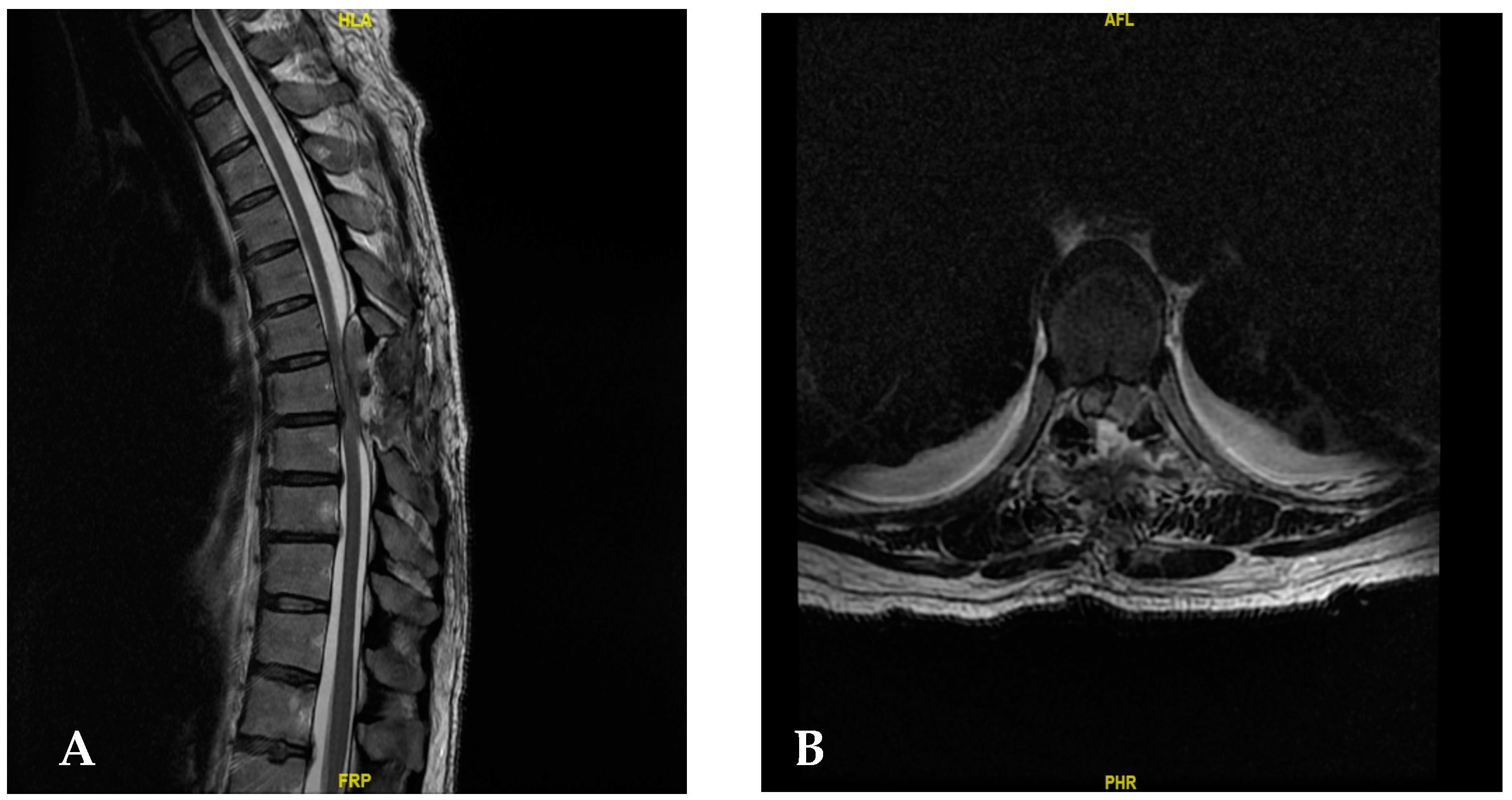
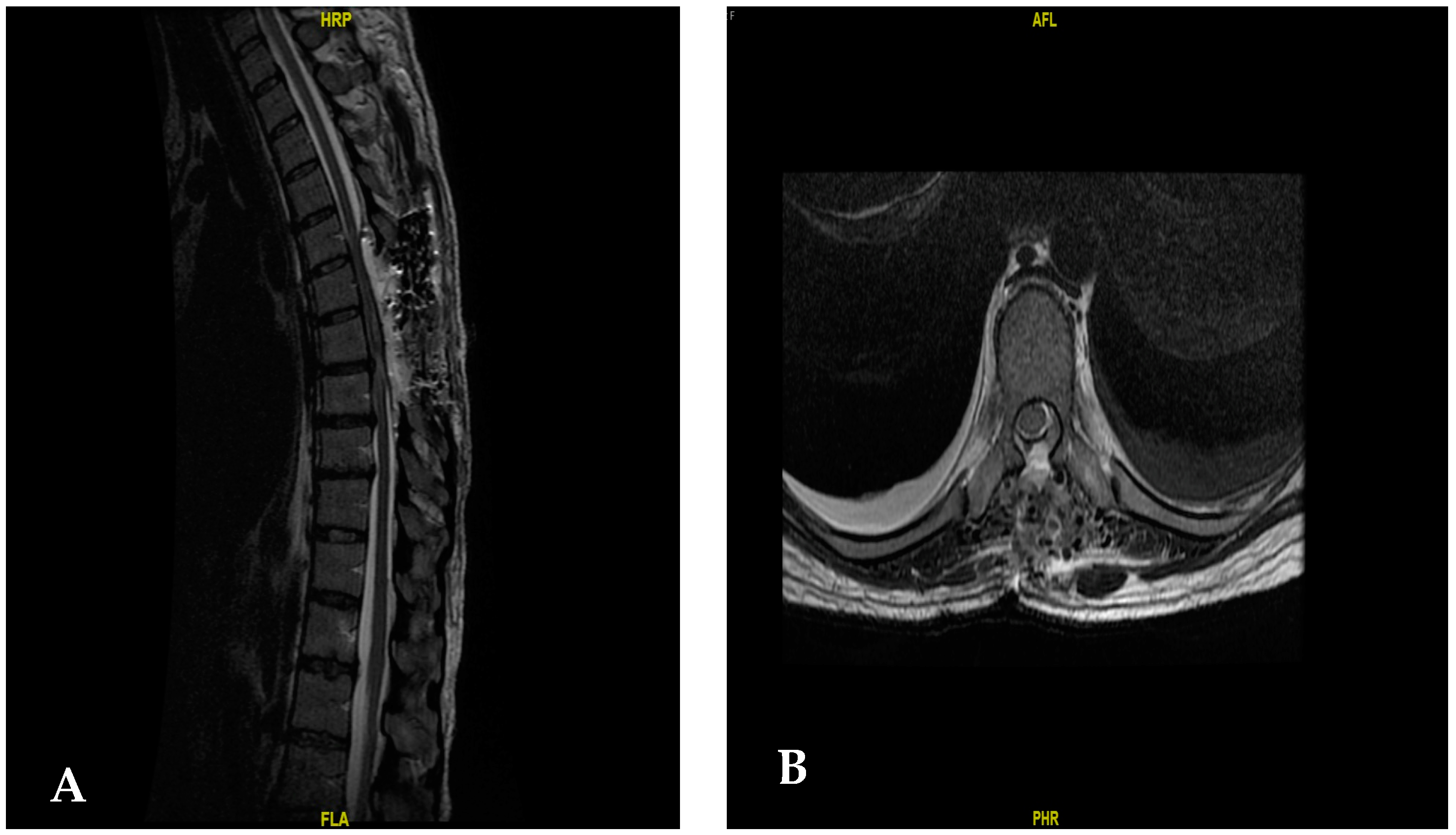
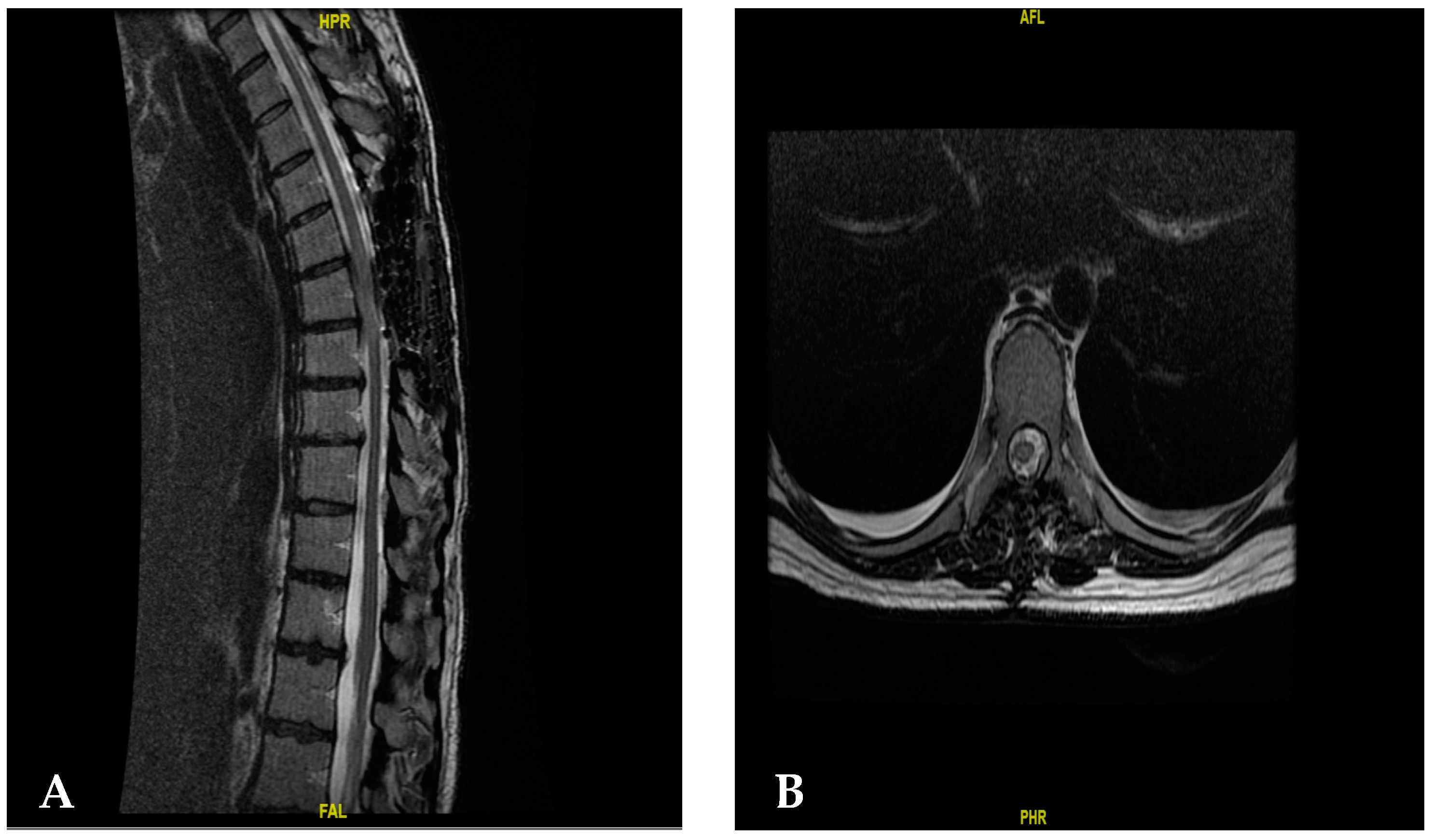
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ledbetter, L.N.; Leever, J.D. Imaging of Intraspinal Tumors. Radiol. Clin. N. Am. 2019, 57, 341–357. [Google Scholar] [CrossRef] [PubMed]
- Schwake, M.; Adeli, A.; Sporns, P.; Ewelt, C.; Schmitz, T.; Sicking, J.; Hess, K.; Spille, D.C.; Paulus, W.; Stummer, W.; et al. Spinal meningiomas–Risks and potential of an increasing age at the time of surgery. J. Clin. Neurosci. 2018, 57, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.; Tan, W.L.B.; Wei, W.; Vellayappan, B.A. An overview of the tumors affecting the spine-Inside to out. Neurooncol. Pract. 2020, 7, i10–i17. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, A.; Nunez, L.; Timaran-Montenegro, D.; Riascos, R. Imaging of Common and Infrequent Extradural Tumors. Neuroimaging Clin. N. Am. 2023, 33, 443–457. [Google Scholar] [CrossRef]
- Bezu, M.T.; Nour, A.S.; Tefera, T.G.; Shumbash, K.Z.; Woldemariam, M.A. Preliminary Review of Spine Tumor Radiologic, Intra-Operative and Histopathology Findings, Addis Ababa, Ethiopia. Ethiop. J. Health Sci. 2022, 32, 41–46. [Google Scholar] [CrossRef]
- Guo, L.; Holdefer, R.N.; Kothbauer, K.F. Monitoring spinal surgery for extramedullary tumors and fractures. Handb. Clin. Neurol. 2022, 186, 245–255. [Google Scholar] [CrossRef]
- Bettaswamy, G.; Ambesh, P.; Das, K.K.; Sahu, R.; Srivastava, A.; Mehrotra, A.; Jaiswal, A.; Jaiswal, S.; Behari, S. Extradural spinal meningioma: Revisiting a rare entity. J. Craniovertebral Junction Spine 2016, 7, 65–68. [Google Scholar] [CrossRef]
- Park, B.J.; Dougherty, M.C.; Noeller, J.; Nourski, K.V.; Gold, C.J.; Menezes, A.H.; Hitchon, C.A.; Bathla, G.; Yamaguchi, S.; Hitchon, P.W. Spinal Meningioma in Adults: Imaging Characteristics, Surgical Outcomes, and Risk Factors for Recurrence. World Neurosurg. 2022, 164, e852–e860. [Google Scholar] [CrossRef]
- Matsuda, S.; Kajihara, Y.; Abiko, M.; Mitsuhara, T.; Takeda, M.; Karlowee, V.; Yamaguchi, S.; Amatya, V.J.; Kurisu, K. Concurrent Schwannoma and Meningioma Arising in the Same Spinal Level: A Report of Two Cases. NMC Case Rep. J. 2018, 5, 105–109. [Google Scholar] [CrossRef]
- Garaud, S.; Boto, J.; Egervari, K.; Vargas, M.I. Extradural Spinal Meningioma Mimicking a Schwannoma: Magnetic Resonance Imaging Findings. Can. J. Neurol. Sci. 2022, 49, 467–469. [Google Scholar] [CrossRef]
- Ho, U.C.; Chang, K.; Lin, Y.H.; Huang, Y.C.; Tsuang, F.Y. Primary intraosseous meningioma of the vertebra: Illustrative case. J. Neurosurg. Case Lessons 2021, 2, CASE213621. [Google Scholar] [CrossRef] [PubMed]
- Utsunomiya, Y.; Mori, N.; Matsui, Y.; Katsushima, H.; Hashimoto, K.; Furuta, A. Intraosseous metaplastic meningioma: A case report. Radiol. Case Rep. 2021, 16, 3300–3303. [Google Scholar] [CrossRef]
- Sivaraju, L.; Thakar, S.; Ghosal, N.; Hegde, A.S. Cervical En-Plaque Extradural Meningioma Involving Brachial Plexus. World Neurosurg. 2017, 108, 994.e7–994.e10. [Google Scholar] [CrossRef] [PubMed]
- Tulloch, I.; Georges, H.; Phadke, R.; Hardwidge, C. A thoracic extradural chordoid meningioma: A unique case report and literature review. Br. J. Neurosurg. 2020, 34, 112–114. [Google Scholar] [CrossRef]
- Lois, L.A.; Ratnakar, S.P.; Leong, C.K.; Yian, S.Y. Radiology Case. Radiol. Cases 2018, 12, 1–10. [Google Scholar]
- Yaldiz, C.; Asil, K.; Ceylan, D.; Erdem, S.A. A Dumbbell-shaped Meningioma in the Thoracic Spine: A Case Report. J. Spine 2014, 3, 168. [Google Scholar] [CrossRef]
- Hersh, E.H.; Sarkiss, C.A.; Ladner, T.R.; Lee, N.; Kothari, P.; Lakomkin, N.; Caridi, J.M. Perioperative Risk Factors for Thirty-Day Morbidity and Mortality in the Resection of Extradural Thoracic Spine Tumors. World Neurosurg. 2018, 114, e950–e956. [Google Scholar] [CrossRef] [PubMed]
- Tuli, J.; Drzymalski, D.M.; Lidov, H.; Tuli, S. Extradural in plaque spinal meningioma with intraneural invasion. World Neurosurg. 2012, 77, 202.e5–202.e13. [Google Scholar] [CrossRef]
- Koeller, K.K.; Shih, R.Y. Intradural extramedullary spinal neoplasms: Radiologic-pathologic correlation. Radiographics 2019, 39, 468–490. [Google Scholar] [CrossRef]
- Ghanchi, H.; Hariri, O.R.; Takayanagi, A.; Li, G. Multiple Extradural Spinal Meningiomas in a Patient with Acquired Immunodeficiency Syndrome: Case Report and Literature Review. World Neurosurg. 2018, 117, 366–370. [Google Scholar] [CrossRef]
- Yokoya, S.; Hisaoka, S.; Fujiwara, G.; Oka, H.; Hino, A. Posttraumatic rapid growing extradural meningioma: A case report on the effectiveness of echosonography. Surg. Neurol. Int. 2022, 13, 61. [Google Scholar] [CrossRef] [PubMed]
- Seo, E.H.; Cha, J.G.; Yoon, Y.S.; Moon, A.R. Extradural Spinal Lymphoplasmacyte-Rich Meningioma in the Thoracic Spine: A Case Report and Literature Review. J. Korean Soc. Radiol. 2022, 83, 924–930. [Google Scholar] [CrossRef] [PubMed]
- Jeong, S.K.; Seong, H.Y.; Roh, S.W. Extra-intradural Spinal Meningioma: A Case Report. Korean J. Spine 2014, 11, 202–204. [Google Scholar] [CrossRef]
- Frank, B.L.; Harrop, J.S.; Hanna, A.; Ratliff, J. Cervical Extradural Meningioma: Case Report and Literature Review. J. Spinal Cord Med. 2008, 31, 302–305. [Google Scholar] [CrossRef]
- Suzuki, A.; Nakamura, H.; Konishi, S.; Yamano, Y. Dumbbell-shaped meningioma with cystic degeneration in the thoracic spine: A case report. Spine 2002, 27, E193–E196. [Google Scholar] [CrossRef]
- Restrepo, C.S.; Herrera, D.A.; Lemos, J.A. Extraforaminal meningioma with extrapleural space extension. Am. J. Roentgenol. 2006, 186, 1314–1316. [Google Scholar] [CrossRef] [PubMed]
- Santiago, B.M.; Rodeia, P.; Cunha, E.; Sa, M. Extradural thoracic spinal meningioma. Neurol India 2009, 57, 98. [Google Scholar] [CrossRef] [PubMed]
- Buchfelder, M.; Nomikos, P.; Paulus, W.; Rupprecht, H. Spinal-thoracic dumbbell meningioma: A case report. Spine 2001, 26, 1500–1504. [Google Scholar] [CrossRef]
- Kim, M.S.; Eun, J.P.; Park, J.S. A dumbbell-shaped meningioma mimicking a schwannoma in the thoracic spine. J. Korean Neurosurg. Soc. 2011, 50, 264–267. [Google Scholar] [CrossRef]
- Yang, Y.; Li, D.; Cao, X.Y.; Hao, S.Y.; Wang, L.; Wu, Z.; Zhang, J.T. Clinical features, treatment, and prognostic factors of chordoid meningioma: Radiological and pathological features in 60 cases of chordoid meningioma. World Neurosurg. 2016, 93, 198–207. [Google Scholar] [CrossRef]
- Khayal, H.B.; Abograra, A.; Iashhab, M. Extradural spinal meningioma in a nine-year-old girl: A case report and review of the literature. Open Access J. Neurol. Neurosurg. 2017, 5, 555659. [Google Scholar]
- Hong, W.; Kim, E.S.; Lee, Y.; Lee, K.; Koh, S.H.; Song, H.; Kwon, M.J. Spinal Extradural Meningioma: A Case Report and Review of the Literature. J. Korean Soc. Radiol. 2018, 79, 11–17. [Google Scholar] [CrossRef]
- Wang, Z.L.; Mou, J.H.; Sun, D.; Liu, P. Case Report: Upper Thoracic Purely Extradural Spinal Meningioma with Nerve Root Attachment: A Case Report and Literature Review. Front. Surg. 2022, 16, 918094. [Google Scholar] [CrossRef]
- Gader, G.; Masmoudi, M.; Ghedira, K.; Krifa, M.I.; Chelly, I.; Zammel, I.; Badri, M. Lumbar spine epidural meningioma: Report of a rare case. Spinal Cord Ser. Cases 2023, 9, 53. [Google Scholar] [CrossRef] [PubMed]
- Redhu, R.; Pavithra, H.N. Spinal extradural meningioma: Report of two cases. J. Craniovertebral Junction Spine 2024, 15, 254–257. [Google Scholar] [CrossRef]
- Arvind, V.; Nevzati, E.; Ghaly, M.; Nasim, M.; Farshad, M.; Guggenberger, R.; Sciubba, D.; Spiessberger, A. Primary extradural tumors of the spinal column: A comprehensive treatment guide for the spine surgeon based on the 5th Edition of the World Health Organization bone and soft-tissue tumor classification. J. Craniovertebral Junction Spine 2021, 12, 336–360. [Google Scholar] [CrossRef]
- Chay, W.; Kirshblum, S. Predicting Outcomes After Spinal Cord Injury. Phys. Med. Rehabil. Clin. N. Am. 2020, 31, 331–343. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author Year | Age/Gender | Location (Level) | Examination (Presentation) | Intervention | Histopathology | Result |
|---|---|---|---|---|---|---|
| [25] | 58/Male | T10, T11, T12 | Normal examination, abnormal mass in thoracic X-ray | T11–12 Hemi-laminectomy + thoracoscopy | Fibroblastic meningioma | Complete excision |
| [26] | 57/Female | C7–T2 | Loss of strength in lower extremities. Increased reflexes, | Total laminectomy + adjuvant RT | Psamomatous meningioma, infiltration | Complete excision, no recurrence |
| [24] | 45/Female | C5–C7 | Posterior cervicothoracic chronic pain Mild bladder disturbance | C5–C7 laminectomy and left-sided foraminotomies with C5–T1 instrumentation | Psamomatous meningioma | No recurrence, No symptoms |
| [27] | 42/Male | T2–T3 | Paraparesis | T2–T3 laminectomy | Psamomatous meningioma | Complete excision |
| [28] | 72/Female | Paresis of the lower extremities | Laminectomy + Thoracotomy | Meningioma | Complete excision | |
| [29] | 50/Male | T6–T7 | Paresthesia | T6 hemi-laminectomy | Grade 1 meningothelial meningioma | Complete resection |
| [18] | 42/Female | T5–T6 | Progressive weakness in the lower extremities Numbness below T3 over the course of 4 months | T4–T6 laminectomy | WHO grade I meningioma with nerve root invasion | Full recovery of motor function |
| [16] | 48/Female | C7–T2 | Hypoesthesia below T1 | T1 total laminectomy | Psamomatous meningioma | Complete excision |
| [23] | 49/Female | T12–L1 | Leg pain for 5 years Hyperesthesia of the left leg without motor deficit | T12 total Laminectomy | Psamomatous meningioma | Not reported |
| [30] | 55/Female | T6–T8 | 2-year progressive back pain Weakness on both legs | T6–T8 laminectomy | Angiomatous meningioma | Improvement of motor weakness |
| [7] | 50/Male | C1–C4 | Neck pain associated with tingling, Burning paresthesia in all limbs for 8 months, Progressive spastic quadriparesis with bladder disturbances during the last week. | C2–C4 laminectomy | WHO grade I Meningothelial Meningioma | Completely symptom-free |
| [31] | 9/Female | T5–T6 | Paraparesis of the lower limbs with bilateral foot dropInability to walk | T5–T7 laminectomy | Chordoid meningioma | Improvement of motor weakness |
| [32] | 58/Female | T7 | Paraparesis of both legs and had difficulty maintaining her balance due to weakness. | T7 partial laminectomy | WHO grade II atypical meningioma | Improvement of motor weakness |
| [33] | 39/Male | T1–T3 | Pain in his left chest and back with | T1–T3 Partial laminectomy | Grade 1 meningothelial meningioma | Improvement of symptoms |
| [22] | 22/Female | T9–T10 | back pain for 2 months and weakness and sensory loss for 2 weeks | T9 Right unilateral laminectomy | Lymphoplasmacyte-Rich Meningioma | Not reported |
| [34] | 64/male | L3–L4 | Cauda equine syndrome | L3–L4 Laminectomy | benign meningioma | Improvement of symptoms |
| [35] | 45/female | C7–T2 | 1-year history of progressive weakness and paraesthesia of both lower legs | C7–T2 laminectomy | WHO grade 1 meningioma | Improvement of motor weakness |
| [35] | 50/Female | T2–T3 | progressive weakness and numbness in both lower limbs | T2–T3 laminectomy | Psamomatous meningioma | Improvement of motor weakness, recurrence of the lesion |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albavera-Gutiérrez, R.R.; Espíndola-Rodríguez, A.; Castro-Fuentes, C.A.; Martínez, A.K.A.; Valencia-Ledezma, O.E.; Salgado-Camacho, J.M.; Mendoza, L.B.; Nava, E.N. Thoracic Extradural Psammomatous Meningioma on T6–T8: A Case Report and Literature Review. Surgeries 2024, 5, 920-928. https://doi.org/10.3390/surgeries5040074
Albavera-Gutiérrez RR, Espíndola-Rodríguez A, Castro-Fuentes CA, Martínez AKA, Valencia-Ledezma OE, Salgado-Camacho JM, Mendoza LB, Nava EN. Thoracic Extradural Psammomatous Meningioma on T6–T8: A Case Report and Literature Review. Surgeries. 2024; 5(4):920-928. https://doi.org/10.3390/surgeries5040074
Chicago/Turabian StyleAlbavera-Gutiérrez, Roberto Renan, Arturo Espíndola-Rodríguez, Carlos Alberto Castro-Fuentes, Ana Karen Aguayo Martínez, Omar Esteban Valencia-Ledezma, Juan Manuel Salgado-Camacho, Luis Bernal Mendoza, and Ernesto Nuñez Nava. 2024. "Thoracic Extradural Psammomatous Meningioma on T6–T8: A Case Report and Literature Review" Surgeries 5, no. 4: 920-928. https://doi.org/10.3390/surgeries5040074
APA StyleAlbavera-Gutiérrez, R. R., Espíndola-Rodríguez, A., Castro-Fuentes, C. A., Martínez, A. K. A., Valencia-Ledezma, O. E., Salgado-Camacho, J. M., Mendoza, L. B., & Nava, E. N. (2024). Thoracic Extradural Psammomatous Meningioma on T6–T8: A Case Report and Literature Review. Surgeries, 5(4), 920-928. https://doi.org/10.3390/surgeries5040074