Abstract
Animals in the veterinary and experimental settings, including nonhuman primates (NHPs), often require repeated and prolonged vascular access for indications including blood sampling or administration of fluids, blood products, medication, or other therapies. A vascular access approach should be tailored to experimental or clinical use meeting the needs of the individual animal such that benefits outweigh risks. The optimal device and placement technique is based on the inherent advantages and disadvantages of specific anatomic sites and planned use. Totally implanted vascular access ports (VAPs) enable reliable central venous access for frequent sample collection and/or intravenous therapies. VAPs minimize discomfort with IV access to facilitate cooperation with handling and minimize stress-induced physiologic changes which can confound biologic data and drug responses. VAPs do not limit species-typical behavior and social group activities and are compatible with animal enrichment programs that include play and swim because there are no externalized components. VAPs are typically used long-term and demonstrate excellent durability with high patency and low complication rates over time, presenting a safe and dependable vascular access approach.
1. Introduction
In both the experimental and clinical settings, vascular access is often required either for acquiring blood samples or performing intravascular (IV) administration of blood products, medication, or other fluids, as necessitated by study design or clinical care. In cases where repeated access is required, especially long-term, totally implantable vascular access ports (VAPs) are ideal in facilitating reliable IV access, increasing comfort, and reducing the risks of certain complications typically associated with frequent, repeated vascular access [1,2,3,4]. Totally implantable VAPs consist of a port head with a needle-penetrable self-sealing septum attached to an indwelling catheter (Figure 1) and are completely under the skin with no externalized components. VAPs have been utilized in human medicine for over 40 years [5] and have been increasingly used in veterinary medical applications across a variety of species in both research and clinical settings to realize similar benefits of improved care and welfare when frequent or long-term vascular access is required. Herein we focus on the use of VAPs for achieving central vascular access; however, ports have also demonstrated important value for providing reliable access to other medically relevant fluids and systems, including bile, cerebrospinal fluid, and organs [6,7,8,9,10,11,12], which further highlights their utility and application in animals.
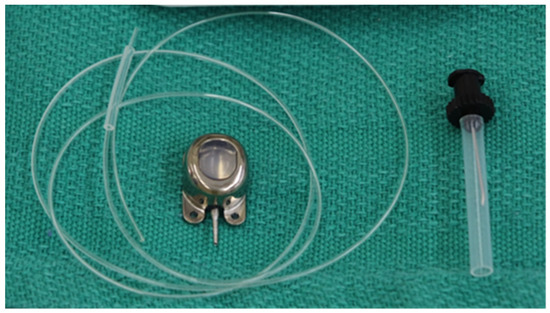
Figure 1.
Vascular access port components including port head, sheath, and catheter. Huber needle shown on the right.
To maximize the utility of a VAP for a given animal, there are several factors to consider, including whether VAP placement is clinically or experimentally indicated, optimal location and technique of surgical placement, postoperative patient care, long-term device management and access technique, and potential complications to be aware of. Many of these considerations are dependent on the individual animal together with the intended purpose of VAP and should be considered on a case-by-case basis to meet the needs of the situation. With proper application and management, VAPs can provide simplified, long-term dependable vascular access offering a range of advantages benefiting both the animal and their care providers. In this review, the application of VAPs will be presented in the context of NHPs; however, the concepts and techniques demonstrated may be widely applied to other animals in a laboratory or veterinary setting.
2. Indications and Advantages of Vascular Access Port Placement
VAPs were first developed in 1982 for the chronic delivery of chemotherapeutic agents in human cancer patients [5]. They were initially developed to overcome the disadvantages of external central venous catheters such as catheter dislodgement, increased risk of infection, and thrombosis, as well as provide greater convenience to patients [13]. Soon after, the use of ports became more common in biomedical research using animals due to the sampling requirements characteristic of these models and the relative ease of using VAPs for serial sampling. Ports have now been utilized in multiple species (Table 1) for a wide range of applications such as vascular access or similar catheter extravascular applications.
Frequent blood sampling remains among the most commonly performed procedures in experimental animals and is a major indication for VAP placement. Furthermore, chronic central venous access is indicated in animals that will require long-term intravenous fluid boluses, continuous fluid administration, or chronic intravenous drug therapy. Additionally, central venous access is also necessary for the administration of infusates such as chemotherapeutic or cytotoxic agents that cannot be administered peripherally. Central access may also be necessary in cases where peripheral veins are compromised or in health conditions causing difficult access.
While chronic central venous access can be accomplished with externalized catheters, totally implantable ports have their advantages, particularly in animals. In general, VAPs require less frequent catheter care than externalized devices. Because there is no exit site for VAPs, they have a significantly lower infection risk than externalized catheters which have chronic exit wounds [14]. Similarly, externalized venous catheters may be a source of interest or irritation for animals, causing them to interfere with and potentially dislodge the catheter. This may also contribute to increased infection risk. While a protective garment may be used to prevent the animal from reaching the catheter, garment-imposed restriction in both movement and certain species-typical behaviors may be aversive to the animal. VAPs overcome these challenges by utilizing the skin as a natural barrier, minimizing the likelihood that an animal disturbs the catheter and obviating the need for protective garments and chronic wound care. Consequently, VAPs enable species-typical behaviors and allow for normal socialization in animals [15].
In general, there are no absolute contraindications to VAP placement; however, there are some relative contraindications that should be carefully considered. Special consideration should be used with animals at an increased risk of bleeding, including those on anticoagulants or with coagulopathy. Animals with ongoing bacteremia or an active infection should not have a VAP implanted due to the risk of seeding a secondary VAP infection. Any infection should be completely treated and resolved prior to consideration of implantation. Similarly, immunocompromised animals with neutropenia (ANC < 1000/µL) may have an increased risk of sepsis to the extent that implantation should be delayed until resolution of the neutropenia if possible. Lastly, the intended venous site should be evaluated for possible occlusion, thrombosis or size constraints which could compromise the utility of the port [15].

Table 1.
Usage of VAPs in the veterinary and experimental animal literature.
Table 1.
Usage of VAPs in the veterinary and experimental animal literature.
| Year | Citation | Purpose | Animal |
|---|---|---|---|
| 1985 | Garner and Laks, “Chronic catheter for BP measurement” [16] | Arterial VAP used to monitor cardiac output and blood pressure monitoring | Dog |
| 1986 | Bailie et al., “VAP implantation in swine” [17] | Simplify venous access in miniature pigs via jugular vein VAP | Miniature Pig |
| 1987 | Mann et al., “BP measurement in dog” [18] | Using arterial VAP to monitor blood pressure in dogs | Dog |
| 1988 | Garner et al., “BP measurement in rats” [19] | Arterial VAP for blood pressure monitoring in rats | Rat |
| 1991 | Perry-Clark and Meunier, “VAP in rabbits” [20] | Jugular VAP for chronic infusions and venous sampling | New Zealand White Rabbit |
| 1994 | Wojnicki et al., “VAPs in Rhesus” [21] | Jugular VAP for blood sampling and drug administration in drug abuse model | Rhesus Macaque |
| 1994 | Bacher et al., “CSF sampling in Rhesus” [7] | Chronic port access to CSF for intrathecal drug monitoring | Rhesus Macaque |
| 1995 | Rockar et al., “CSF retrieval in dogs” [8] | Development of port placement technique for CSF sampling | Dog |
| 1995 | Kwei et al., “Intestinal and portal VAP” [22] | Portal and intestinal VAPs for drug absorption studies | Dog |
| 1996 | Landi et al., “VAP infection in monkeys” [23] | Evaluation of infection after VAP placement for venous blood sampling | Cynomolgus Macaque |
| 1998 | Kissinger et al., “Bile collection in dogs” [6] | Implanted catheter placed within biliary tree for bile collection | Dog |
| 1999 | Cowart et al., “Optimizing VAP in pigs” [24] | Optimizing VAPs in young pigs to minimize complications | Pig |
| 2002 | Henry et al., “VAP in cats” [25] | Jugular vein VAP for blood sampling in cats | Cat |
| 2003 | Gilberto et al., “Alternative CSF sampling method” [9] | Improved technique for subcutaneous port placement for CSF sampling | Rhesus Macaque |
| 2004 | Kunta et al., “Intestinal VAP in rabbits” [26] | Venous, portal, and intestinal placed VAPs for drug metabolism studies | Rabbit |
| 2009 | Graham et al., “Novel technique for VAP placement” [27] | New percutaneous saphenous vein VAP technique versus conventional jugular/femoral vein | NHP (Cynomolgus, Rhesus, Baboon) |
| 2011 | Graham et al., “Long-term portal VAP” [10] | Portal vein VAP for islet cell transplantation | NHP (Cynomolgus, Rhesus) |
| 2011 | Aubert et al., “VAP use in feline blood donors” [28] | Application of VAP for frequent use in blood donor animals | Cat |
| 2013 | Farrow et al., “Jugular VAP placement for sampling in cats” [29] | Evaluation of implanted VAPs for long-term blood sampling in cats | Cat |
| 2015 | Guérios et al., “Surgical placement of VAPs in dogs and cats” [30] | Technique for placement and management of VAPs in dogs and cats | Dog and Cat |
| 2020 | Mutch et al., “Long term management of VAPs” [15] | Management of VAPs for long-term sampling and fluid/drug administration | NHP (Cynomolgus, Rhesus) |
| 2022 | Pálek et al., “IV access in experimental surgery” [31] | Suitability of VAPs in the external jugular vein for use in experimental surgery | Pig |
| 2023 | Ehrmann et al., “Vascular access button for chronic access in rabbits” [32] | Long-term vascular access technique for chronic blood sampling and drug administration | Rabbit |
VAP, vascular access port; NHP, nonhuman primate.
3. Surgical Technique
3.1. Location Considerations
The VAP placement location is generally determined by the target vessel and the desired location of the port head for optimal access. There are general guidelines that are helpful in making this determination as well as species-specific considerations. Overall, the location of insertion should be selected with careful consideration of sensitivity of associated incision(s) using techniques that minimize the number of incisions and avoid sites that are pressured by routine activity. Surgical site infections pose unique risk in the placement of any device, as device contamination results in necessitated removal. For example, incisions in bacterially dense regions, like the groin, have demonstrated higher rates of infection, an important consideration in site selection [33,34,35]. Lastly, placement should not limit species-typical behaviors nor should animal movements restrict catheter function resulting in mechanical failure, such as acute bending of the port head in jugular vein cannulation or at the hip joint in femoral vein cannulation [15,21,27]. Species-specific considerations for location are addressed here:
- Nonhuman primates. Conventional VAP implantation sites in NHPs include the jugular or femoral veins using a cutdown approach with a tunneled catheter to the dorsum of the animal where a second incision is made to create a pocket for the port head [21,23,36]. The necessity of two separate incisions and long tunnel increases procedural invasiveness and has a relatively high rate of infections, mechanical or thrombotic occlusions, and dehiscence or erosion have been reported [21,23,36,37,38,39]. Moreover, this approach requires that animals be restrained, typically using manual or chemical restraint, to position them for VAP access.
To address these limitations, our group developed a single-incision peripheral insertion (SIPI) technique that minimizes invasiveness, reduces operative time, simplifying anesthesia, and allows animals to present the port head cooperatively to caregivers, avoiding the need for restraint or separation from their social groups [27]. A simple cutdown to the saphenous vein is used to introduce the catheter to the IVC and the same incision is advantaged to create a pocket for port head placement on the lateral aspect of the leg for ease of access. This approach was successful in reducing infection rates to <10% together with improved patency, >95% at 6 months and >80% at 1 year [15].
- 2.
- Pigs. Port and catheter placement in pigs has been extensively reviewed with the most common site for placement being the external jugular vein [17,24,40,41]. Special consideration must be given to location of the port head, because pigs may persistently rub surgical sites which can lead to trauma, infection, and wound breakdown. Given this, port heads are often placed on the dorsum of the pig, typically at the neck or chest wall.
- 3.
- Dogs. The external jugular vein, femoral vein, and lateral saphenous vein have all been utilized for VAP placement in dogs. The external jugular vein is used with preference, with most studies reporting a <5% complication rate [25,30,42]. However, the factors driving this preference are not fully clear as comparison between the external jugular vein and the lateral saphenous vein sites for VAP placement demonstrated higher complications in JV placements as compared to SV placements. Catheter tip malposition occurred in 17.4% of JV placements versus 0% of SV cases [43] and 30.4% of dogs implanted with a JV VAP developed a seroma; increased seroma risk may be related to the more extensive dissection used for JV placement [28,30].
- 4.
- Cats. Similar to dogs, the external jugular vein or femoral veins are used for the majority of VAP placements. As with pigs and dogs, the port heads are typically placed on the dorsum of cats [28,44].
- 5.
- Rabbits. The external jugular vein or the femoral vein are the primary sites for VAP placement [20,45]. To avoid disruption of the port head, it is usually placed on the dorsum. The position of the port head in this species can be affected by the need for restraint. Placement of the port head on the neck dorsally may require manipulation of the ears during sterile prep, making access difficult during restraint, so mid-back alongside the vertebral column is alternatively used [32].
3.2. Anesthesia and Surgical Prep Considerations
Anesthesia management during VAP placement should consider individual animal characteristics, surgical invasiveness, duration of surgery, and site expertise for this procedure. Even in relatively short duration cases such as VAP placement, general anesthesia is typically used, while carrying its usual risks and potential complications. Virtually all anesthetic agents depress cardiovascular and respiratory function, which can be of particular concern in older or sick animals. Hypotension, hypoxemia, hypercapnia, and cardiac dysrhythmias are associated with the use of general anesthesia [46,47,48]. Proper airway management typically requires intubation and mechanical ventilation which is associated with specific complications that are both minor, such as coughing or oral cavity trauma, and major, including esophageal intubation, laryngeal edema, or tracheal stenosis [49,50]. Nevertheless, performing VAP placement with general anesthesia provides important benefits; intubation provides a protected airway for the animal during the procedure and promotes favorable vitals during the case, including improved oxygen saturation, that expedite post-procedure recovery to the animal’s benefit. Additionally, general anesthesia can be titrated with rapid response, in comparison with a limitation of most sedative agents where there is a window of efficacy that requires redosing or increased initial exposure that can affect recovery timing.
Our preferred approach for VAP implantation in NHPs is to introduce the catheter through the saphenous vein to the IVC (the SIPI technique) which has the benefit of very brief case times. This gives us the option for either sedation or general anesthesia, making the selection with the best interest of the individual animal’s characteristics. Commonly used medications for anesthesia and sedation in NHPs are presented below (Table 2).
Table 2.
Common anesthetics and sedatives for use in cynomolgus and rhesus macaques.
Prior to the administration of general anesthesia or sedatives, a fasting period that includes removal of solid food items for 6–12 h with free access to fluids is recommended in order to prevent aspiration. After anesthetic induction, the intended surgical site should be clipped of hair in anticipation of surgical prep. If using the saphenous vein approach, circumferential clipping from the ankle to 1 inch above the knee is performed. The animal should then be moved to the operating room, placed on supplemental thermal support, and positioned according to the approach. To access the saphenous vein, the NHP is generally placed right lateral recumbent for a left approach or left lateral recumbent for a right approach. All monitoring devices should be placed to ensure the anesthetist has adequate access; possible devices and monitoring may include an oxygen saturation probe, EKG, temperature probe, and blood pressure monitoring.
Care should be taken to establish a sterile surgical field by using an antiseptic surgical scrub on the intended surgical site as well as practicing proper aseptic technique with draping and gowning. We recommend a single preoperative dose of antibiotics within 1 h of intended incision, cefazolin 25–50 mg/kg IM or equivalent cephalosporin class.
3.3. General Surgical Principles
As with almost all surgeries, Halsted’s basic principles of surgical technique also apply to VAP placement. These include gentle handling of tissues, meticulous hemostasis, strict aseptic technique, minimizing tissue tension, obliterating dead space, and accurate tissue apposition [13,27,33]. In the case of vascular access catheters, including ports, particular thought must be utilized in determining which vessel to access and where the port should be placed in order to avoid tissue irritation, wound dehiscence, or erosion. Also, the catheter and port head must be secured adequately or positioned appropriately to prevent unintentional catheter tip migration. The tip should be positioned in a high-flow or turbulent vessel while minimizing wall contact to avoid irritation and inflammation that could cause erosion or clotting [34,36,50].
3.4. Single-Incision Peripheral Insertion Technique
For conventional VAP placement techniques, Swindle et al. [39] provide an excellent overall review for VAP placement in animals. While many of the principles are similar, we will highlight the single-incision peripheral insertion (SIPI) technique as an alternative well-established approach in NHPs. In comparison with the jugular VAP approach, the SIPI approach is less invasive, requiring a single incision versus the traditional two separate incisions. Also, the peripheral insertion minimizes direct trauma to central vessels, allows for relative ease of removal, and avoids chest wall placement, therefore negating the need for restraint and promoting species-typical behavior [27]. After establishing an adequate plane of anesthesia, the animal is positioned and aseptically prepped. The intended incision site is infiltrated with a local anesthetic.
The lateral (or caudal) saphenous vein can be identified on the posterolateral aspect of the knee just distal to the popliteal fossa. A vertical 1–1.5 cm incision is made lateral to the saphenous vein distal to the knee and using blunt dissection, the saphenous vein is visualized (Figure 2) and looped separately with two absorbable sutures at both the proximal and distal end (Figure 3). In preparation for introduction, a flexible J guidewire is advanced into a catheter of adequate length (25–35 cm) so that it is just past the tip, about 2–3 mm.

Figure 2.
Saphenous vein dissected out with right angle clamp in a cynomolgus macaque.
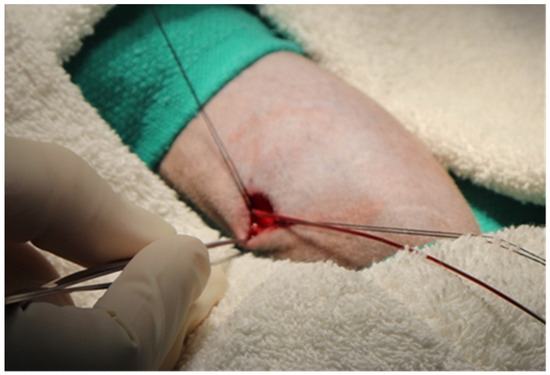
Figure 3.
Saphenous vein encircled by suture proximally and distally for retraction in a cynomolgus macaque.
The catheter over guidewire is then passed proximately into the lumen of the saphenous vein and advanced centrally into the inferior vena cava (Figure 4). Once the catheter reaches the mark, the guidewire is removed and the catheter is flushed with normal saline to ensure patency. The proximal suture can then be removed. Of note, care should be taken not to handle the catheter with any sharp or toothed instruments to avoid damaging it. Also, if resistance is felt while advancing, the catheter can be rinsed with normal saline, or other times, the positioning of the leg can be adjusted from extended to flexed at the hip while gently advancing.
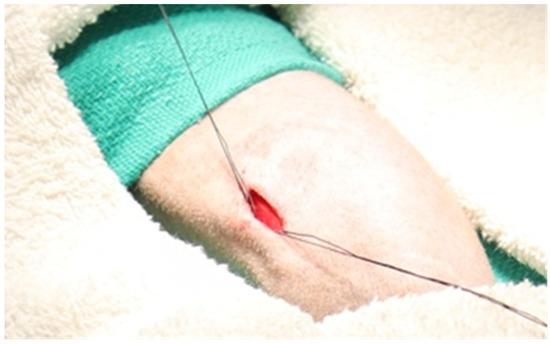
Figure 4.
Guidewire advanced proximally within the lumen of the saphenous vein in a cynomolgus macaque.
Attention is then turned to the creation of the port pocket for the port head. The same incision used to cannulate the saphenous vein is utilized to make this pocket. The pocket is created within the subcutaneous tissue proximally on the leg using blunt dissection, with the intent that the port head should be implanted on a stable muscle plane without in-depth fixation. This dissection can be accomplished with blunt scissors or a hemostat; however, care must be taken to make the pocket slightly larger than the port head and deep enough to prevent erosion through the skin. Particular attention should be paid to the pocket location in relation to the incision in order to prevent port placement directly under the incision which can cause irritation and possible dehiscence.
Then, the proper catheter length is determined to reach the port head and it is trimmed accordingly. The catheter sheath is then attached to the port, ensuring that the sheath is slid up to the port head for additional security, before securing the connection with non-absorbable sutures. A Huber needle and syringe are used to assess patency of the port before (Figure 5A) and after placement into the pocket (Figure 5B). The port head is then placed into the pocket with no fixation in a close-fitting pocket. If the subcutaneous pocket is too large, there is a risk for rotation of the port head; in this case, the port head can be secured into place with non-absorbable sutures. Care should be taken to ensure the suture passes through the fascia and not just subcutaneous tissue in order to be properly secured.
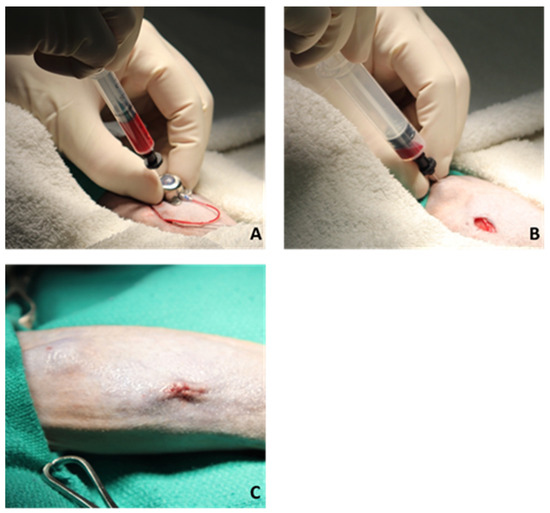
Figure 5.
Assessing port patency and incision closure in a cynomolgus macaque. (A) Prior to pocket placement, (B) After pocket placement., (C) Three-layer suture closure with skin.
Lastly, the incision is then closed in a normal fashion (Figure 5C), typically in three layers with an absorbable monofilament suture such as polydioxanone monofilament. The first and second layer is run in a continuous fashion within the superficial fascia and subcutaneous tissue in order to obliterate as much dead space as possible to minimize seroma formation. The final layer is a running subcuticular stitch ensuring that the knots are buried to prevent spitting and irritation. A topical skin adhesive is then applied over the incision as an additional protective barrier. The VAP is then flushed with normal saline and locked using a lock solution containing either an anticoagulant or thrombolytic in saline to prevent clotting.
4. Postoperative Care and Management
After surgical placement of the VAP, it is imperative that animals receive adequate monitoring, care, and analgesia, as would be implemented in other surgical cases. Animals should be directly monitored post-surgery until they are no longer ataxic and are in a condition that would be suitable for discharge. Due to the nature of the small incision required for this procedure, bandaging for protection of the surgical site is often not necessary; however, light bandages, spray bandages, or tissue glue may be applied to the site to protect from animal manipulation depending on the location of the procedure and individual animal needs [29,39,56]. While generally considered a minimally invasive surgery, postoperative analgesia is essential to ensure animal comfort during recovery. This typically involves NSAIDs for addressing potential inflammation, opioids for inducing analgesia by acting through the central and peripheral nervous system, or a combination of both [15,39]. Selection of specific analgesics should be made with consideration of an individual animal’s underlying health status and any relevant contraindications. In NHPs, we recommend a single dose of buprenorphine pre-operatively, followed with NSAID coverage for 3 days postoperatively. Examples of possible analgesic options specific to NHPs and appropriate doses for this minimally invasive procedure are provided in Table 3, based on our experience and laboratory animal analgesic guidelines. Professional judgement should be used to guide specific drug and dose selection.
Table 3.
Common analgesics for use in cynomolgus and rhesus macaques for minor procedures.
Postoperative prophylactic antibiotic use following VAP placement varies across protocols, and evidence of its benefits is limited; in general, routine use of antibiotics postoperatively is not recommended except in cases of known surgical contamination [39] but should instead be considered individually on an as-needed basis. It is important to note that several previous studies have shown no benefit of postoperative antibiotic use on the risk of surgical-site infection [57], including in NHPs [37]. Similarly, the propensity for antibiotic use to introduce drug-associated complications, including bacterial resistance and risk or diarrhea, needs to be considered when making this decision.
In the days and weeks following the VAP placement procedure, the surgical site should be monitored for proper healing. In the first several days post-procedure, mild and localized bruising, redness, and/or swelling are possible in the area around the port head or incision site. These are typically not a cause for concern, and steady improvement towards resolution should be observed within a few days. If conditions do not improve or begin to worsen, the animal should be closely observed for potential irritation of the incision site or risk of infection. In the absence of complication, the incision site should be completely healed within a few weeks.
5. Vascular Access Port Use and Maintenance
Proper VAP management is essential to promote long-term function and reduce the risk of certain complications. A dedicated staff should be trained in appropriate use and maintenance techniques, as expert management both reduces the risk of infection and promotes VAP longevity by minimizing physical wear on the port head and preventing catheter occlusion.
Strict aseptic technique should be used to reduce the likelihood of introducing infectious agents through the VAP every time it is used. The skin surrounding the VAP site should be prepared by cleansing any physical dirt or debris from the surrounding area and applying an appropriate antiseptic solution, such as povidone iodine, chlorhexidine, betadine scrub, or an equivalent solution, for the recommended contact time to adequately disinfect the skin overlying the port head. In some cases, fur may be clipped from the site to facilitate easier access [28,29,58], but this is often not necessary and even adds risk via skin abrasions and introduces an additional potentially unfavorable stimuli to the animal being handled.
Access of the port should always be performed using a sterile non-coring needle (e.g., Huber needle), designed to prevent damage to the VAP’s septum during insertion and removal. Non-coring needles are able to penetrate the septum for access without risk of shearing, both promoting VAP longevity and eliminating the risk of septum damage that could result in foreign body introduction to the catheter. The selection of needle gauge and configuration is dependent on the size of the port head and its location, frequency or duration of access, and volume or type of fluids to be administered or sampled. To access the port, the appropriate Huber needle should be inserted perpendicular to the port head; once inserted, rotation and rocking of the needle should be avoided to limit damage to the device septum. Sterile syringes or solution sets from which blood will be collected or fluids, medications, or other biologic products that will be administered can then be attached to the inserted needle hub for the performance of the required sampling or fluid administration. The attached syringe should be drawn back to aspirate the indwelling locking solution and blood to the estimated dead space volume of the catheter and discarded. Once any sample collection or fluid administration is complete, the VAP should be flushed with normal saline at a volume at least three times the estimated dead space volume of the catheter and locked by administering a suitable anticoagulant locking solution while maintaining positive pressure throughout to prevent blood backflow within the catheter. The volume of the lock solution instilled should fill the catheter dead space. Locking solutions are typically composed of either heparinized saline, taurolidine and citrate solutions, or, in cases where vascular access will be less frequent, an appropriate thrombolytic solution, such as alteplase. There is no specific requirement for maintenance flushing; the best practice is to use the minimum frequency required to maintain patency in order to decrease unnecessary risk of infection and mechanical wear. Recognizing differences in implant sites and lock selections, various maintenance schedules have been reported that range from as frequent as every 2 weeks with others flushing only every 3 months with high success in maintaining patency [15,29].
6. Complications
Like any medical device and other vascular access techniques, infrequent complications with VAPs are possible even in the context of excellent device management. These complications can include infection, mechanical device failure due to loss of patency or device manipulation, or erosion with a loss of integrity of the skin overlying the device [15].
Because VAPs are utilized to give reliable vascular access, patency is constantly evaluated during use and maintenance. Patency is defined as either one-way, the ability to infuse through the port, or two-way, the ability to infuse and withdraw through the port. When two-way patency is lost, there is often a physical catheter obstruction like a blood clot or a mechanical deficit like a kink. Flush patent VAPs (one-way) are often affected by a fibrin sheath or flap at the catheter tip which can create a ball-valve effect hindering blood withdrawal [59,60]. In the literature, catheter occlusion is reported to occur in between 1.5% and 13% of VAPs [61,62]. In this situation, the external port head and catheter should be inspected and a flush attempted. Positional changes can be attempted to straighten the pathway of the catheter or correct tip malposition. Leakage at the port or port catheter connection can be a result of wear and results in saline infiltration in the subcutaneous space, ultimately requiring surgical repair to replace a damaged port.
In a flush patent line that fails to withdraw, patency is often restored using pulsatile turbulent flushing or by using thrombolytic agents, the most common being tissue plasminogen activator (tPA) to catheter fill volume [63,64]. Longer dwell times and more than one attempt may be needed to restore function.
A rare complication that has been observed in both humans and animals [15,65,66] occurs when device malfunction results from patient manipulation/twisting of the port head that results in the catheter winding around the port head, a condition referred to as “Twiddler’s syndrome” that necessitates surgical correction. Other rare but high-mortality complications include accidental arterial puncture, cardiac arrythmia, air embolism, or heart tamponade. These are typically associated with approaches to access the superior vena cava such as the internal jugular approach which can be minimized or completely avoided utilizing the inferior vena cava.
Widely variable rates of infection have been reported in animals compared with the human literature that generally describe rates <10% [67,68]. Still, VAPs are associated with significantly less risk of infection in comparison to external catheters, with complication rates dependent on species, implant site, and duration and use characteristics. Factors that increase the risk of infection include implant site, animal disruption of an incision, incomplete healing, or improper access technique which can then result in contamination of the VAP. Infection may present as swelling, erythema, heat, ulceration, and associated pain. Overall clinical evaluation should be performed as bacteremia and sepsis may present as inappetence, fever, lethargy, or general malaise. There are no successful approaches to decontaminate devices; as such, infection is an indication for prompt removal [69].
VAP explant following complication should carefully remove all components, eliminate dead spaces or fibrous capsules, as well as debride and lavage particularly following the explant of contaminated implants. The explant site is often approximated with monofilament absorbable sutures leaving the distal end of the incision to secondary wound closure to allow for potential drainage and promote healing.
7. Conclusions
Since their introduction in the early 1980s, VAPs have proven to be an essential tool for chronic blood collection and intravascular drug administration in experimental animal research as well as in the veterinary setting. Due to their implantable design and lack of an exit site wound, VAPs have been shown to minimize infection rates compared to externalized catheters. Furthermore, VAP implantation into the central vasculature ensures correct drug delivery while reducing the risk of extravasation relative to peripheral administration. VAPs avoid repeat venipuncture, reducing trauma and allowing for the preservation of peripheral blood vessels [50]. This enhances animal comfort and allows for species-typical behavior, social housing, and unrestricted movement, all while eliminating the need for catheter protective devices [37]. Long-term success and patency in NHPs has been achieved with a selection of favorable implant sites and careful consideration of handling that appreciates species-typical behaviors and husbandry, together with exceptional attention to the handling and maintenance of the VAP by expert, dedicated caregivers that is comparable to the human clinical setting [15].
Author Contributions
Conceptualization, S.H.O., D.J.L. and M.L.G.; investigation, S.H.O., D.J.L. and M.L.G.; data curation, S.H.O., D.J.L. and M.L.G.; writing—original draft preparation, S.H.O., D.J.L. and M.L.G.; writing—review and editing, S.H.O., D.J.L. and M.L.G.; visualization, S.H.O., D.J.L. and M.L.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The authors would like to thank the University of Minnesota Preclinical Research Center for providing the photographs used in the figures for this review.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Gyves, J.; Ensminger, W.; Niederhuber, J.; Liepman, M.; Cozzi, E.; Doan, K.; Dakhil, S.; Wheeler, R. Totally implanted system for intravenous chemotherapy in patients with cancer. Am. J. Med. 1982, 73, 841–845. [Google Scholar] [CrossRef] [PubMed]
- Bow, E.J.; Kilpatrick, M.G.; Clinch, J.J. Totally Implantable Venous Access Ports Systems for Patients Receiving Chemotherapy for Solid Tissue Malignancies: A Randomized Controlled Clinical Trial Examining the Safety, Efficacy, Costs, and Impact on Quality of Life. J. Clin. Oncol. 1999, 17, 1267. [Google Scholar] [CrossRef] [PubMed]
- Wu, O.; Boyd, K.; Paul, J.; McCartney, E.; Ritchie, M.; Mellon, D.; Kelly, L.; Dixon-Hughes, J.; Moss, J. Hickman catheter and implantable port devices for the delivery of chemotherapy: A phase II randomised controlled trial and economic evaluation. Br. J. Cancer 2016, 114, 979–985. [Google Scholar] [CrossRef] [PubMed]
- Zaghal, A.; Khalife, M.; Mukherji, D.; El Majzoub, N.; Shamseddine, A.; Hoballah, J.; Marangoni, G.; Faraj, W. Update on totally implantable venous access devices. Surg. Oncol. 2012, 21, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Niederhuber, J.E.; Ensminger, W.; Gyves, J.W.; Liepman, M.; Doan, K.; Cozzi, E. Totally implanted venous and arterial access system to replace external catheters in cancer treatment. Surgery 1982, 92, 706–712. [Google Scholar] [PubMed]
- Kissinger, J.T.; Garver, E.M.; Schnell, M.A.; Schantz, J.D.; Coatney, R.W.; Meunier, L.V.D. A new method to collect bile and access the duodenum in conscious dogs. J. Am. Assoc. Lab. Anim. Sci. 1998, 37, 89–93. [Google Scholar]
- Bacher, J.D.; Balis, F.M.; McCully, C.L.; Godwin, K.S. Cerebral subarachnoid sampling of cerebrospinal fluid in the rhesus monkey. Lab. Anim. Sci. 1994, 44, 148–152. [Google Scholar]
- Rockar, R.A.; Sadanaga, K.K.; Burkett, D.E.; Mitroka, J.G.; Bonner, R.A.; Weinstein, M.J. Cerebrospinal fluid retrieval in the conscious dog: A methods development study. J. Investig. Surg. 1995, 8, 85–94. [Google Scholar] [CrossRef]
- Gilberto, D.B.; Zeoli, A.H.; Szczerba, P.J.; Gehret, J.R.; Holahan, M.A.; Sitko, G.R.; Johnson, C.A.; Cook, J.J.; Motzel, S.L. An alternative method of chronic cerebrospinal fluid collection via the cisterna magna in conscious rhesus monkeys. J. Am. Assoc. Lab. Anim. Sci. 2003, 42, 53–59. [Google Scholar]
- Graham, M.L.; Mutch, L.A.; Rieke, E.F.; Dunning, M.; Zolondek, E.K.; Schutten, M.M.; Hering, B.J.; Schuurman, H.-J. Long-term hepatic vascular access in the nonhuman primate for recurrent portal vein infusion. J. Investig. Surg. 2011, 24, 59–66. [Google Scholar] [CrossRef]
- Mao, W.; Guo, S.; Ye, D.; Cao, Y.; Jiang, X.; Huang, Y.; Yuan, H.; Jiao, L. Surgical application of an implantable biliary access device in the treatment of refractory recurrent cholangiolithiasis. Quant. Imaging Med. Surg. 2023, 13, 3333–3342. [Google Scholar] [CrossRef]
- Pino, M.G.; Ganguly, R.; Rich, K.A.; Fox, A.; Mattox, L.; Keckley, E.; Joseph, M.; Malbrue, R.; Youngblood, B.; Krishna, V.; et al. Continual cerebrospinal fluid sampling in the neonatal domestic piglet for biomarker and discovery studies. J. Neurosci. Methods 2022, 366, 109403. [Google Scholar] [CrossRef] [PubMed]
- Sonobe, M. Clinical Indications, Preoperative Assessment, Set-up and Organizational Aspects. In Totally Implantable Venous Access Devices: Management in Mid- and Long-Term Clinical Setting; Niederhuber, J.E., Di Carlo, I., Biffi, R., Eds.; Springer: Milan, Italy, 2012; pp. 37–42. [Google Scholar] [CrossRef]
- Gurkan, S.; Seber, S.; Gur, O.; Yetisyigit, T.; Okan Donbaloglu, M.; Ozkaramanli Gur, D. Retrospective evaluation of totally implantable venous access port devices: Early and late complications. J. BUON 2015, 20, 338–345. [Google Scholar]
- Mutch, L.A.; Klinker, S.T.; Janecek, J.J.; Niewinski, M.N.; Lee, R.M.; Graham, M.L. Long-Term Management of Vascular Access Ports in Nonhuman Primates Used in Preclinical Efficacy and Tolerability Studies. J. Investig. Surg. 2020, 33, 493–504. [Google Scholar] [CrossRef] [PubMed]
- Garner, D.; Laks, M.M. New implanted chronic catheter device for determining blood pressure and cardiac output in conscious dog. Am. J. Physiol.-Heart Circ. Physiol. 1985, 249, H681–H684. [Google Scholar] [CrossRef] [PubMed]
- Bailie, M.; Wixson, S.; Landi, M. Vascular-access-port implantation for serial blood sampling in conscious swine. Lab. Anim. Sci. 1986, 36, 431–433. [Google Scholar]
- Mann, W.; Landi, M.; Horner, E.; Woodward, P.; Campbell, S.; Kinter, L. A simple procedure for direct blood pressure measurements in conscious dogs. Lab. Anim. Sci. 1987, 37, 105–108. [Google Scholar] [PubMed]
- Garner, D.; McGivern, R.; Jagels, G.; Laks, M.M. A new method for direct measurement of systolic and diastolic pressures in conscious rats using Vascular-Access-Ports. Lab. Anim. Sci. 1988, 38, 205–207. [Google Scholar]
- Perry-Clark, L.; Meunier, L. Vascular access ports for chronic serial infusion and blood sampling in New Zealand white rabbits. Lab. Anim. Sci. 1991, 41, 495–497. [Google Scholar]
- Wojnicki, F.; Bacher, J.D.; Glowa, J.R. Use of subcutaneous vascular access ports in rhesus monkeys. Lab. Anim. Sci. 1994, 44, 491–494. [Google Scholar]
- Kwei, G.Y.; Gehret, J.R.; Novak, L.B.; Drag, M.D.; Goodwin, T. Chronic catheterization of the intestines and portal vein for absorption experimentation in beagle dogs. Lab. Anim. Sci. 1995, 45, 683–685. [Google Scholar] [PubMed]
- Landi, M.; Schantz, J.; Jenkins, E.; Warnick, C.; Kissinger, J. ICLAS proceedings: A survey of vascular access port infection in cynomolgus monkeys (Macaca fascicularis). Scand. J. Lab. Anim. Science. Suppl. 1996. [Google Scholar]
- Cowart, R.P.; Payne, J.T.; Turk, J.R.; Tyler, J.W.; Casteel, A.W. Factors optimizing the use of subcutaneous vascular access ports in weaned pigs. J. Am. Assoc. Lab. Anim. Sci. 1999, 38, 67–70. [Google Scholar]
- Henry, C.; Russell, L.; Tyler, J. Comparison of hematologic and biochemical values for blood samples obtained via jugular venipuncture and via vascular access ports in cats. J. Am. Vet. Med. Assoc. 2002, 220, 482–485. [Google Scholar] [CrossRef] [PubMed]
- Kunta, J.R.; Lee, S.-H.; Perry, B.A.; Lee, Y.-H.; Sinko, P.J. Differentiation of gut and hepatic first-pass loss of verapamil in intestinal and vascular access-ported (IVAP) rabbits. Drug Metab. Dispos. 2004, 32, 1293–1298. [Google Scholar] [CrossRef] [PubMed]
- Graham, M.L.; Rieke, E.F.; Dunning, M.; Mutch, L.A.; Craig, A.M.; Zolondek, E.K.; Hering, B.J.; Schuurman, H.J.; Bianco, R.W. A novel alternative placement site and technique for totally implantable vascular access ports in non-human primates. J. Med. Primatol. 2009, 38, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Aubert, I.; Abrams-Ogg, A.C.; Sylvestre, A.M.; Dyson, D.H.; Allen, D.G.; Johnstone, I.B. The use of vascular access ports for blood collection in feline blood donors. Can. J. Vet. Res. 2011, 75, 25–34. [Google Scholar]
- Farrow, H.A.; Rand, J.S.; Burgess, D.M.; Coradini, M.; Vankan, D.M. Jugular vascular access port implantation for frequent, long-term blood sampling in cats: Methodology, assessment, and comparison with jugular catheters. Res. Vet. Sci. 2013, 95, 681–686. [Google Scholar] [CrossRef]
- Guérios, S.D.; Silva, D.M.; Souza, C.H.; Bacon, N.J. Surgical placement and management of jugular vascular access ports in dogs and cats: Description of technique. Rev. Colomb. Cienc. Pecu. 2015, 28, 265–271. [Google Scholar] [CrossRef][Green Version]
- Pálek, R.; Rosendorf, J.; Šarčevič, S.; Ševčík, J.; Brzoň, O.; Kepková, L.; Krystl, P.; Brousil, M.; Červenková, L.; Třeška, V. Permanent intravenous access in experimental surgery–our experience. Rozhl. Chir. Mesic. Ceskoslovenske Chir. Spol. 2022, 101, 577–583. [Google Scholar]
- Ehrmann, J.; Johnson, W.; de Castro, A.; Donnelly, M. Implantation of a Vascular Access Button for Chronic Blood Sampling and Drug Administration in the Rabbit. Surgeries 2023, 4, 141–151. [Google Scholar] [CrossRef]
- Bertone, S.A.; Fisher, M.C.; Mortensen, J.E. Quantitative skin cultures at potential catheter sites in neonates. Infect. Control. Hosp. Epidemiol. 1994, 15, 315–318. [Google Scholar] [CrossRef] [PubMed]
- Goetz, A.M.; Wagener, M.M.; Miller, J.M.; Muder, R.R. Risk of infection due to central venous catheters: Effect of site of placement and catheter type. Infect. Control. Hosp. Epidemiol. 1998, 19, 842–845. [Google Scholar] [CrossRef] [PubMed]
- Arvaniti, K.; Lathyris, D.; Blot, S.; Apostolidou-Kiouti, F.; Koulenti, D.; Haidich, A.B. Cumulative Evidence of Randomized Controlled and Observational Studies on Catheter-Related Infection Risk of Central Venous Catheter Insertion Site in ICU Patients: A Pairwise and Network Meta-Analysis. Crit. Care Med. 2017, 45, e437–e448. [Google Scholar] [CrossRef] [PubMed]
- Lindsey, D.C.; Thompson, T.E.; Emerson, T.E., Jr. A simple technique which maintains vascular patency after catheterization. Lab. Anim. Sci. 1990, 40, 643–644. [Google Scholar]
- Graham, M.L.; Rieke, E.F.; Wijkstrom, M.; Dunning, M.; Aasheim, T.C.; Graczyk, M.J.; Pilon, K.J.; Hering, B.J. Risk factors associated with surgical site infection and the development of short-term complications in macaques undergoing indwelling vascular access port placement. J. Med. Primatol. 2008, 37, 202–209. [Google Scholar] [CrossRef] [PubMed]
- Kinsora, J.J., Jr.; Christoffersen, C.L.; Swalec, J.M.; Juneau, P.L. The novel use of vascular access ports for intravenous self-administration and blood withdrawal studies in squirrel monkeys. J. Neurosci. Methods 1997, 75, 59–68. [Google Scholar] [CrossRef]
- Swindle, M.M.; Nolan, T.; Jacobson, A.; Wolf, P.; Dalton, M.J.; Smith, A.C. Vascular access port (VAP) usage in large animal species. Contemp. Top. Lab. Anim. Sci. 2005, 44, 7–17. [Google Scholar]
- Chuang, M.; Orvieto, M.; Laven, B.; Gerber, G.; Wardrip, C.; Ritch, C.; Shalhav, A. Comparison of external catheters with subcutaneous vascular access ports for chronic vascular access in a porcine model. Contemp. Top. Lab. Anim. Sci. 2005, 44, 24–27. [Google Scholar]
- Swindle, M.M.; Smith, A.C.; Goodrich, J.A. Chronic cannulation and fistulization procedures in swine: A review and recommendations. J. Investig. Surg. 1998, 11, 7–20. [Google Scholar] [CrossRef]
- Culp, W.T.; Mayhew, P.D.; Reese, M.S.; Duda, L.; Glassman, M.M.; Brown, D.C. Complications associated with use of subcutaneous vascular access ports in cats and dogs undergoing fractionated radiotherapy: 172 cases (1996–2007). J. Am. Vet. Med. Assoc. 2010, 236, 1322–1327. [Google Scholar] [CrossRef] [PubMed]
- Mayer, M.N.; Grier, C.K.; Yoshikawa, H.; Ringwood, P.B. Complications associated with the use of vascular access ports in dogs receiving external beam radiation therapy. J. Am. Vet. Med. Assoc. 2008, 233, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Webb, A.I.; Bliss, J.M.; Herbst, L.H. Use of vascular access ports in the cat. Lab. Anim. Sci. 1995, 45, 110–114. [Google Scholar] [PubMed]
- Huynh, M.; Boyeaux, A.; Pignon, C. Assessment and care of the critically ill rabbit. Vet. Clin. Exot. Anim. Pract. 2016, 19, 379–409. [Google Scholar] [CrossRef] [PubMed]
- Gaynor, J.S.; Dunlop, C.I.; Wagner, A.E.; Wertz, E.M.; Golden, A.E.; Demme, W.C. Complications and mortality associated with anesthesia in dogs and cats. J. Am. Anim. Hosp. Assoc. 1999, 35, 13–17. [Google Scholar] [CrossRef] [PubMed]
- Sano, H.; Barker, K.; Odom, T.; Lewis, K.; Giordano, P.; Walsh, V.; Chambers, J.P. A survey of dog and cat anaesthesia in a sample of veterinary practices in New Zealand. N. Z. Vet. J. 2018, 66, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Morrison, J.A.; Spofford, N.; Yang, M.; Saito, E.; Lambert, L.; Faunt, K. Development and implementation of veterinary anesthesia medical quality standards for primary care. Vet. Anaesth. Analg. 2022, 49, 233–242. [Google Scholar] [CrossRef]
- Klonner, M.E.; Springer, S.; Braun, C. Complications secondary to endotracheal intubation in dogs and cats: A questionnaire-based survey among veterinary anaesthesiologists. Vet. Anaesth. Analg. 2023, 50, 220–229. [Google Scholar] [CrossRef]
- Bernal, J.; Adrian, S.; Burkart, H.; Laffins, M. Guideline for Vascular Access Port Use and Maintenance in Large Animals for Biomedical Research. Surgeries 2022, 3, 219–228. [Google Scholar] [CrossRef]
- Abee, C.R.; Mansfield, K.; Tardif, S.D.; Morris, T. Nonhuman Primates in Biomedical Research: Biology and Management; Academic Press: Cambridge, MA, USA, 2012; Volume 1. [Google Scholar]
- Authier, S.; Chaurand, F.; Legaspi, M.; Breault, C.; Troncy, E. Comparison of three anesthetic protocols for intraduodenal drug administration using endoscopy in rhesus monkeys (Macaca mulatta). J. Am. Assoc. Lab. Anim. Sci. 2006, 45, 73–79. [Google Scholar]
- Fish, R.; Danneman, P.J.; Brown, M.; Karas, A. Anesthesia and Analgesia in Laboratory Animals; Academic Press: Cambridge, MA, USA, 2011. [Google Scholar]
- Fowler, K.A.; Huerkamp, M.J.; Pullium, J.K.; Subramanian, T. Anesthetic protocol: Propofol use in Rhesus macaques (Macaca mulatta) during magnetic resonance imaging with stereotactic head frame application. Brain Res./Brain Res. Protoc. 2001, 7, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Young, J.T.; Vlasova, R.M.; Howell, B.R.; Knickmeyer, R.C.; Morin, E.; Kuitchoua, K.I.; Lubach, G.R.; Noel, J.; Hu, X.; Shi, Y.; et al. General anaesthesia during infancy reduces white matter micro-organisation in developing rhesus monkeys. Br. J. Anaesth. 2021, 126, 845–853. [Google Scholar] [CrossRef] [PubMed]
- Morrison, J.A.; Lauer, S.K.; Baldwin, C.J.; Evans, R.B.; Andreasen, C.B.; Kinyon, J.M.; Swanson, E. Evaluation of the use of subcutaneous implantable vascular access ports in feline blood donors. J. Am. Vet. Med. Assoc. 2007, 230, 855–861. [Google Scholar] [CrossRef] [PubMed]
- Fry, D.E. The surgical infection prevention project: Processes, outcomes, and future impact. Surg. Infect. 2006, 7, s-17–s-26. [Google Scholar] [CrossRef]
- Valentini, F.; Fassone, F.; Pozzebon, A.; Gavazza, A.; Lubas, G. Use of totally implantable vascular access port with mini-invasive Seldinger technique in 12 dogs undergoing chemotherapy. Res. Vet. Sci. 2013, 94, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Kurul, S.; Saip, P.; Aydin, T. Totally implantable venous-access ports: Local problems and extravasation injury. Lancet Oncol. 2002, 3, 684–692. [Google Scholar] [CrossRef] [PubMed]
- Chang, D.-H.; Mammadov, K.; Hickethier, T.; Borggrefe, J.; Hellmich, M.; Maintz, D.; Kabbasch, C. Fibrin sheaths in central venous port catheters: Treatment with low-dose, single injection of urokinase on an outpatient basis. Ther. Clin. Risk Manag. 2017, 13, 111–115. [Google Scholar] [CrossRef]
- Aldrighetti, L.; Caterini, R.; Ronzoni, M.; Jannello, A.; Ferla, G. Role of totally implantable systems for long-term vascular access in the treatment of the neoplastic patient. Minerva Chir. 1995, 50, 447–454. [Google Scholar]
- Clari, M.; Spoto, M.; Franceschi, G.; Acuto, M.; Tonella, S.; Caristia, S.; Buratti, G.; Gaboardi, S.; Rasero, L.; Campagna, S.; et al. Short Versus Long Timing of Flushing of Totally Implantable Venous Access Devices When Not Used Routinely: A Systematic Review and Meta-analysis. Cancer Nurs. 2021, 44, 205–213. [Google Scholar] [CrossRef]
- Ponec, D.; Irwin, D.; Haire, W.D.; Hill, P.A.; Li, X.; McCluskey, E.R. Recombinant Tissue Plasminogen Activator (Alteplase) for Restoration of Flow in Occluded Central Venous Access Devices: A Double-Blind Placebo-Controlled Trial—The Cardiovascular Thrombolytic to Open Occluded Lines (COOL) Efficacy Trial. J. Vasc. Interv. Radiol. 2001, 12, 951–955. [Google Scholar] [CrossRef]
- Baskin, J.L.; Pui, C.-H.; Reiss, U.; Wilimas, J.A.; Metzger, M.L.; Ribeiro, R.C.; Howard, S.C. Management of occlusion and thrombosis associated with long-term indwelling central venous catheters. Lancet 2009, 374, 159–169. [Google Scholar] [CrossRef]
- Gebarski, S.S.; Gebarski, K.S. Chemotherapy port “Twiddler’s syndrome”. A need for preinjection radiography. Cancer 1984, 54, 38–39. [Google Scholar] [CrossRef]
- Ince, M.E.; Ozkan, G.; Ors, N.; Yildirim, A.K.; Doganci, S. Complications and pitfalls of central venous port catheters: Experience with 782 patients with cancer. Ir. J. Med. Sci. 2020, 189, 1371–1377. [Google Scholar] [CrossRef]
- Barbetakis, N.; Asteriou, C.; Kleontas, A.; Tsilikas, C. Totally implantable central venous access ports. Analysis of 700 cases. J. Surg. Oncol. 2011, 104, 654–656. [Google Scholar] [CrossRef]
- Chang, L.; Tsai, J.S.; Huang, S.J.; Shih, C.C. Evaluation of infectious complications of the implantable venous access system in a general oncologic population. Am. J. Infect. Control. 2003, 31, 34–39. [Google Scholar] [CrossRef]
- Ji, L.; Yang, J.; Miao, J.; Shao, Q.; Cao, Y.; Li, H. Infections Related to Totally Implantable Venous-Access Ports: Long-Term Experience in One Center. Cell Biochem. Biophys. 2015, 72, 235–240. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).