

Tibial Plateau Fractures among Alpine Skiers: A Retrospective Case Series

{kind=link}
{kind=link}
Abstract
1. Introduction
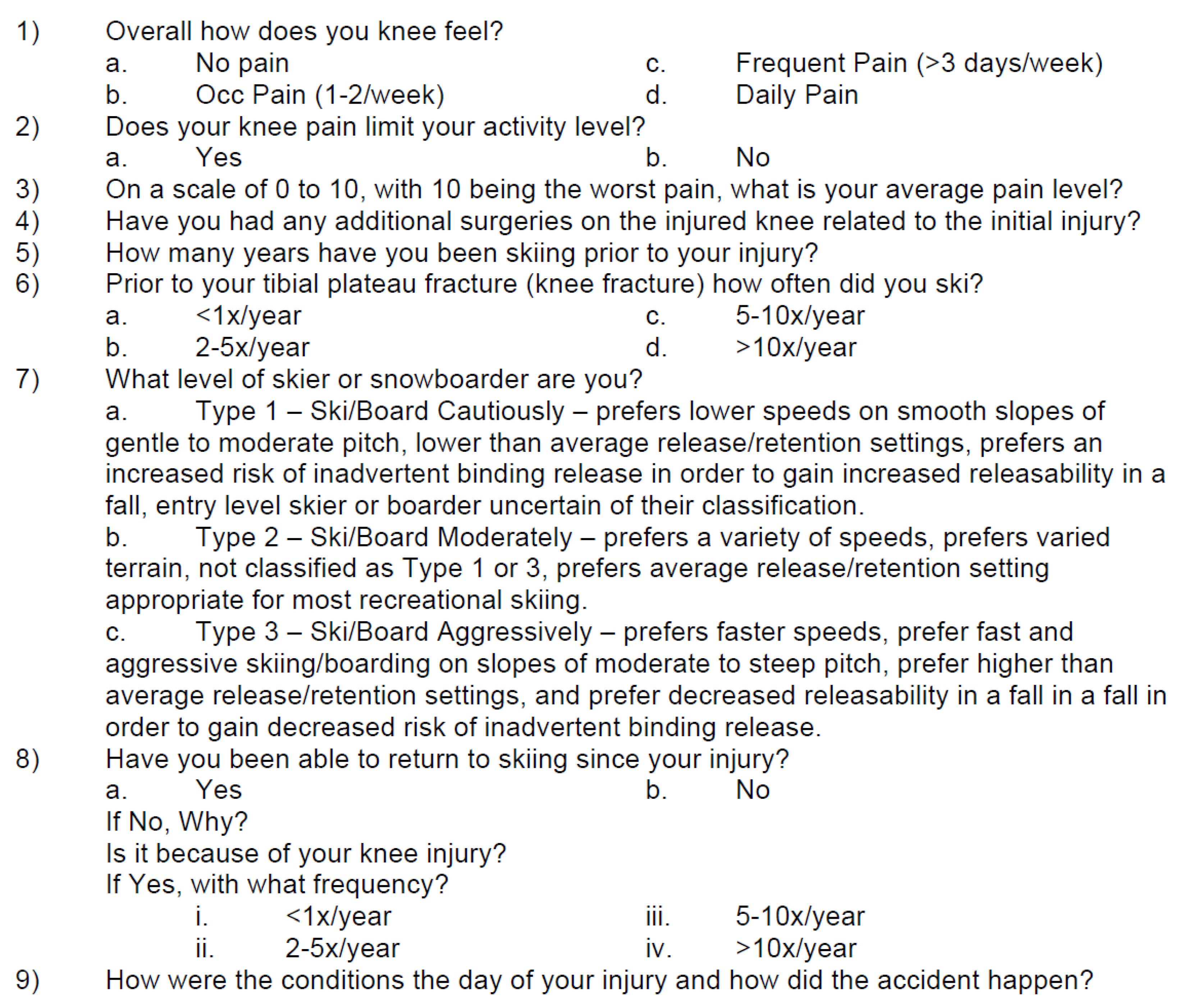
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Snow Industries America. Participation Study 2019–2020. Available online: https://industry.traveloregon.com/wp-content/uploads/2021/04/SIA_Participation_Study_2019-2020_Nov.pdf (accessed on 30 November 2022).
- Koehle, M.S.; Lloyd-Smith, R.; Taunton, J.E. Alpine Ski Injuries and Their Prevention. Sports Med. 2002, 32, 785–793. [Google Scholar] [CrossRef]
- Loibl, M.; Bäumlein, M.; Massen, F.; Gueorguiev, B.; Glaab, R.; Perren, T.; Rillmann, P.; Ryf, C.; Naal, F.D. Sports Activity after Surgical Treatment of Intra-Articular Tibial Plateau Fractures in Skiers. Am. J. Sports Med. 2013, 41, 1340–1347. [Google Scholar] [CrossRef] [PubMed]
- Morin, V.; Pailhé, R.; Sharma, A.; Rouchy, R.C.; Cognault, J.; Rubens-Duval, B.; Saragaglia, D. Moore I Postero-Medial Articular Tibial Fracture in Alpine Skiers: Surgical Management and Return to Sports Activity. Injury 2016, 47, 1282–1287. [Google Scholar] [CrossRef] [PubMed]
- Hunter, R.E. Skiing Injuries. Am. J. Sports Med. 1999, 27, 381–389. [Google Scholar] [CrossRef] [PubMed]
- Mcconkey, J.P.; Meeuwisse, W. Tibial Plateau Fractures in Alpine Skiing. Am. J. Sports Med. 1988, 19, 159–164. [Google Scholar] [CrossRef]
- Tapper, E.M. Ski Injuries from 1939 to 1976: The Sun Valley Experience. Am. J. Sports Med. 1978, 6, 114–121. [Google Scholar] [CrossRef]
- Stenroos, A.; Pakarinen, H.; Jalkanen, J.; Mälkiä, T.; Handolin, L. Tibial Fractures in Alpine Skiing and Snowboarding in Finland: A Retrospective Study on Fracture Types and Injury Mechanisms in 363 Patients. Scand. J. Surgery 2016, 105, 191–196. [Google Scholar] [CrossRef]
- Berkson, E.M.; Virkus, W.W. High-Energy Tibial Plateau Fractures. J. Am. Acad. Orthop. Surg. 2006, 14, 20–31. [Google Scholar] [CrossRef]
- Schatzker, J.; McBroom, R.; Bruce, D. The Tibial Plateau Fracture: The Toronto Experience 1968–1975. Clin. Orthop. Relat. Res. 1979, 138, 94–104. [Google Scholar]
- Langran, M.; Selvaraj, S. Increased Injury Risk Among First-Day Skiers, Snowboarders, and Skiboarders. Am. J. Sports Med. 2004, 32, 96–103. [Google Scholar] [CrossRef]
- Hume, P.A.; Lorimer, A.V.; Griffiths, P.C.; Carlson, I.; Lamont, M. Recreational Snow-Sports Injury Risk Factors and Countermeasures: A Meta-Analysis Review and Haddon Matrix Evaluation. Sports Med. 2015, 45, 1175–1190. [Google Scholar] [CrossRef] [PubMed]
- Ekeland, A.; Rodven, A. Alpine Skiing, Telemarking, Snowboarding, and Skiboarding Injuries Related to Gender and Ability. J. ATSM Int. 2012, 9, 216–227. [Google Scholar]
- Hagel, B.E.; Goulet, C.; Platt, R.W.; Pless, I.B. Injuries among Skiers and Snowboarders in Quebec. Epidemiology 2004, 15, 279–286. [Google Scholar] [CrossRef]
- Bäumlein, M.; Hanke, A.; Gueorguiev, B.; Nerlich, M.; Liodakis, E.; Perren, T.; Rillmann, P.; Ryf, C.; Loibl, M. Long-Term Outcome After Surgical Treatment of Intra-Articular Tibial Plateau Fractures in Skiers. Arch. Orthop. Traum. Surg. 2019, 139, 951–959. [Google Scholar] [CrossRef] [PubMed]
- Westin, M.; Alricsson, M.; Werner, S. Injury Profile of Competitive Alpine Skiers: A Five-Year Cohort Study. Knee Surg. Sport. Traumatol. Arthrosc. 2012, 20, 1175–1181. [Google Scholar] [CrossRef]
- Saragaglia, D.; Giunta, J.C.; Gaillot, J.; Rubens-Duval, B.; Pailhé, R. Are Schatzker and AO Classifications Accurate Enough to Classify Tibial Plateau Fractures in Alpine Skiers? Int. Orthop. 2021, 45, 1863–1869. [Google Scholar] [CrossRef] [PubMed]
- Deibert, M.C.; Aronsson, D.D.; Ettlinger, C.F.; Shealy, J.E. Skiing Injuries in Children, Adolescents, and Adults. J. Bone Joint. Surg. Am. 1998, 80, 25–32. [Google Scholar] [CrossRef]
- Sulheim, S.; Holme, I.; Rødven, A.; Ekeland, A.; Bahr, R. Risk Factors for Injuries in Alpine Skiing, Telemark Skiing and Snowboarding—Case-Control Study. Br. J. Sports Med. 2011, 45, 1303–1309. [Google Scholar] [CrossRef]
- Shealy, J.E.; Ettlinger, C.F.; Johnson, R.J. Aging Trends in Alpine Skiing. J. ASTM Int. 2010, 7, JAI102875. [Google Scholar] [CrossRef]
- Allen, M.D.; Johnstone, J.; Rice, C.L.; Marsh, G.D. Differences in Leg Bone Geometry in Young, Old and Very Old Women. Eur. J. Appl. Physiol. 2011, 111, 2865–2871. [Google Scholar] [CrossRef]
- Flørenes, T.W.; Bere, T.; Nordsletten, L.; Heir, S.; Bahr, R. Injuries among Male and Female World Cup Alpine Skiers. Br. J. Sports Med. 2009, 43, 973–978. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.J.; Ettlinger, C.F.; Shealy, J.E. Update on Injury Trends in Alpine Skiing. J. ASTM Int. 2008, 5, 108–118. [Google Scholar] [CrossRef]
- Hauser, W.; Asang, E.; Mueller, B. Injury Risk in Alpine Skiing. In Skiing Trauma and Skiing Safety: Fifth International Symposium, ATSM STP 860; Johnson, R.J., Mote, C.D., Jr., Eds.; American Society for Testing and Materials: Philadelphia, PA, USA, 1985; pp. 338–348. [Google Scholar]
- Wennergren, D.; Bergdahl, C.; Selse, A.; Ekelund, J.; Sundfeldt, M.; Möller, M. Treatment and Re-Operation Rates in One Thousand and Three Hundred Tibial Fractures from the Swedish Fracture Register. Eur. J. Orth. Surg. Trauma 2021, 31, 143–154. [Google Scholar] [CrossRef] [PubMed]
- Millar, S.C.; Arnold, J.B.; Thewlis, D.; Fraysse, F.; Solomon, L.B. A Systematic Literature Review of Tibial Plateau Fractures: What Classifications Are Used And How Reliable and Useful Are They? Injury 2018, 49, 473–490. [Google Scholar] [CrossRef]
- Masouros, P.T.; Mitrogiannis, G.; Antoniou, G.; Chatzidaki, C.; Kourtzis, D.; Garnavos, C. Interobserver Reliability of Schatzker, AO Foundation-Orthopaedic Trauma Association, and Luo Classifications for Tibial Plateau Fractures: Does Three-Dimensional CT Improve Outcomes? Cureus 2022, 14, e22227. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Williamson, T.R.; Smith, J.N.; Swanson, B.L.; Robinson, J.D.; Swanson, K.R.; Swanson, K.E. Tibial Plateau Fractures among Alpine Skiers: A Retrospective Case Series. Osteology 2023, 3, 71-77. https://doi.org/10.3390/osteology3030008
Williamson TR, Smith JN, Swanson BL, Robinson JD, Swanson KR, Swanson KE. Tibial Plateau Fractures among Alpine Skiers: A Retrospective Case Series. Osteology. 2023; 3(3):71-77. https://doi.org/10.3390/osteology3030008
Chicago/Turabian StyleWilliamson, Tyler R., Joel N. Smith, Britta L. Swanson, John D. Robinson, Keith R. Swanson, and Kyle E. Swanson. 2023. "Tibial Plateau Fractures among Alpine Skiers: A Retrospective Case Series" Osteology 3, no. 3: 71-77. https://doi.org/10.3390/osteology3030008
APA StyleWilliamson, T. R., Smith, J. N., Swanson, B. L., Robinson, J. D., Swanson, K. R., & Swanson, K. E. (2023). Tibial Plateau Fractures among Alpine Skiers: A Retrospective Case Series. Osteology, 3(3), 71-77. https://doi.org/10.3390/osteology3030008