
The Impact of Psychological Factors on Return to Sports after Anterior Cruciate Ligament Reconstruction: A Systematic Review

 ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search
2.3. Study Selection and Data Collection
2.4. Quality Assessment
2.5. Data Synthesis and Analysis
3. Results
3.1. Study Selection
3.2. Studies and Patients Characteristics
3.3. Quality Assessment
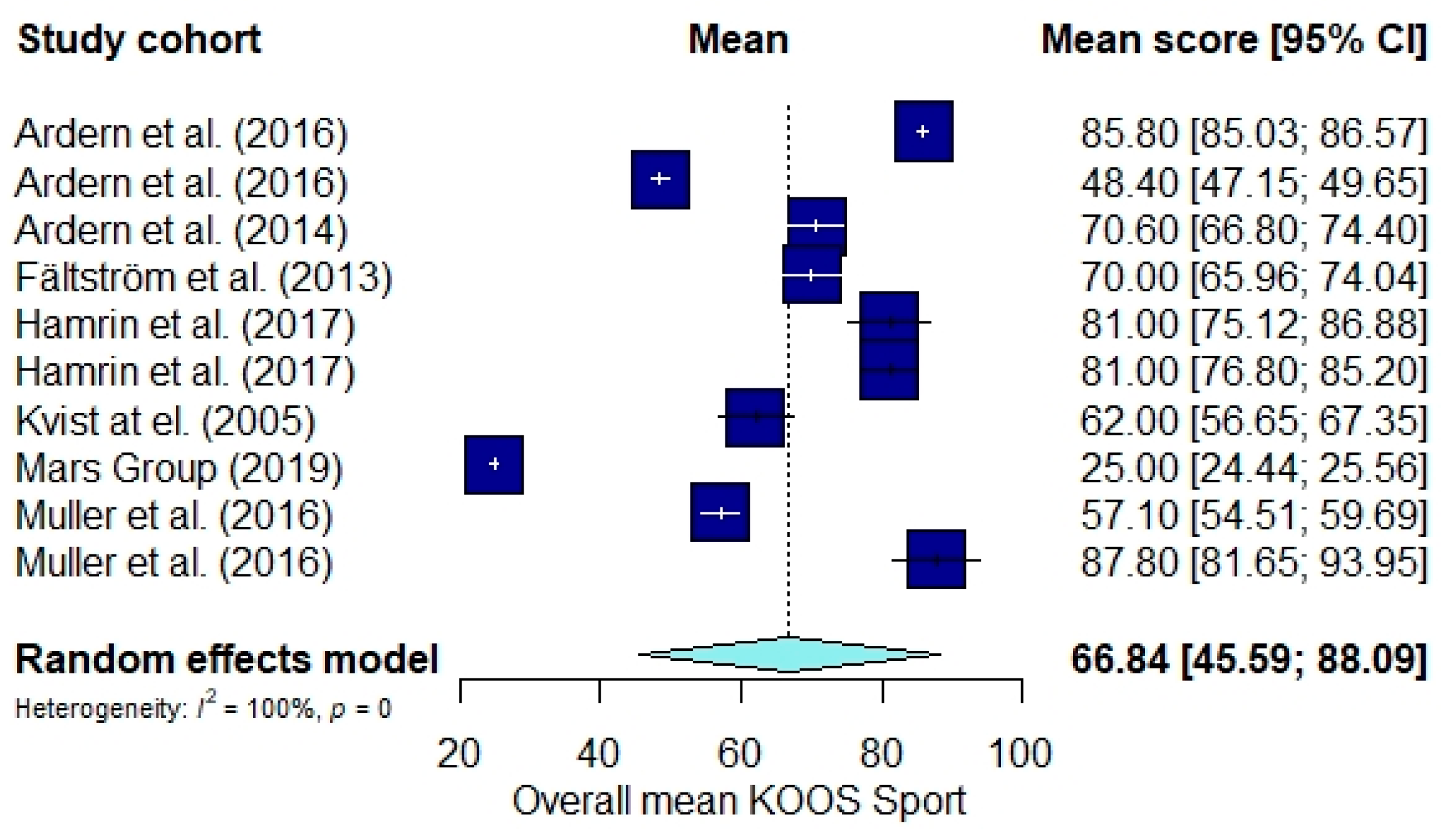
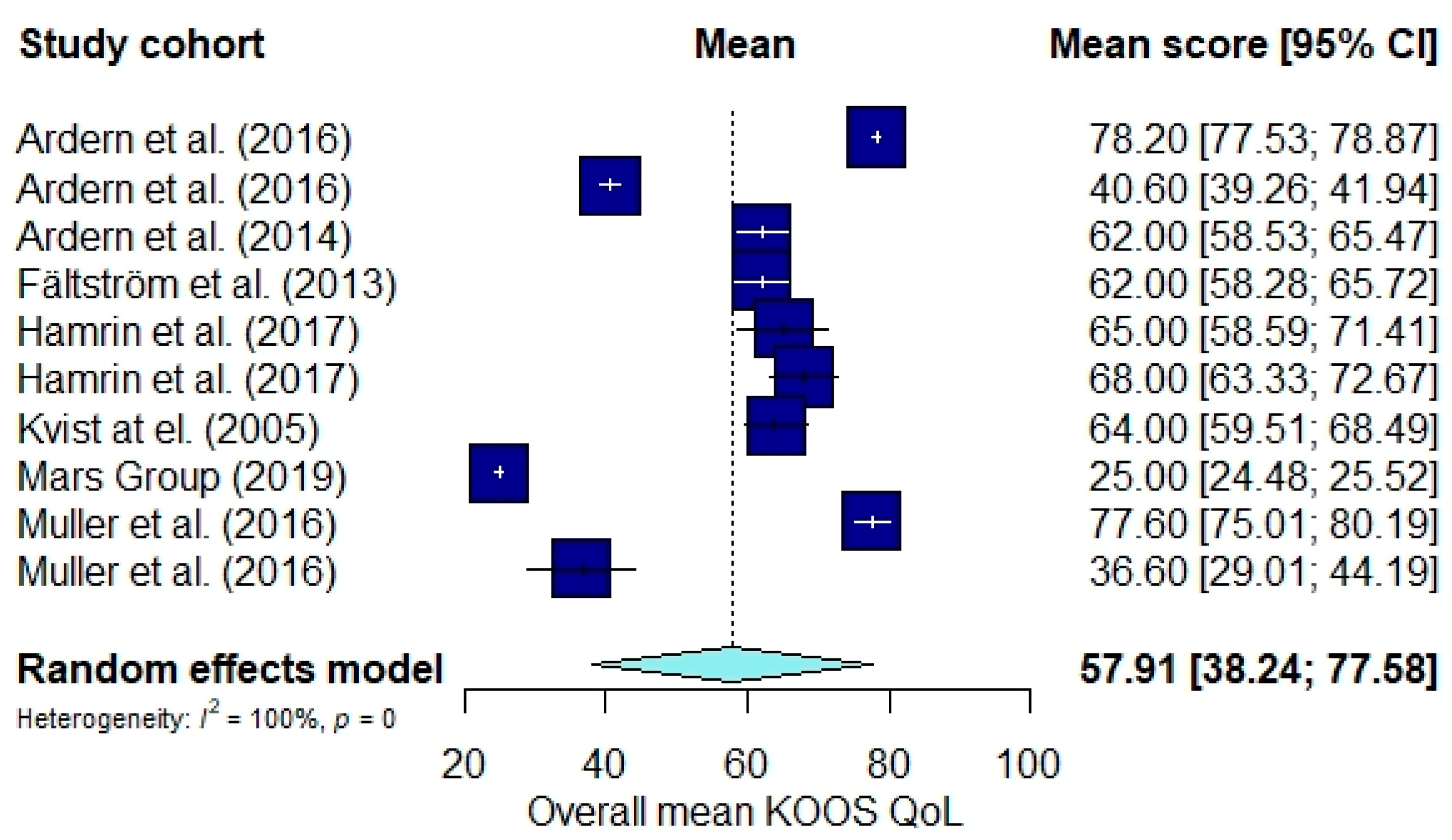
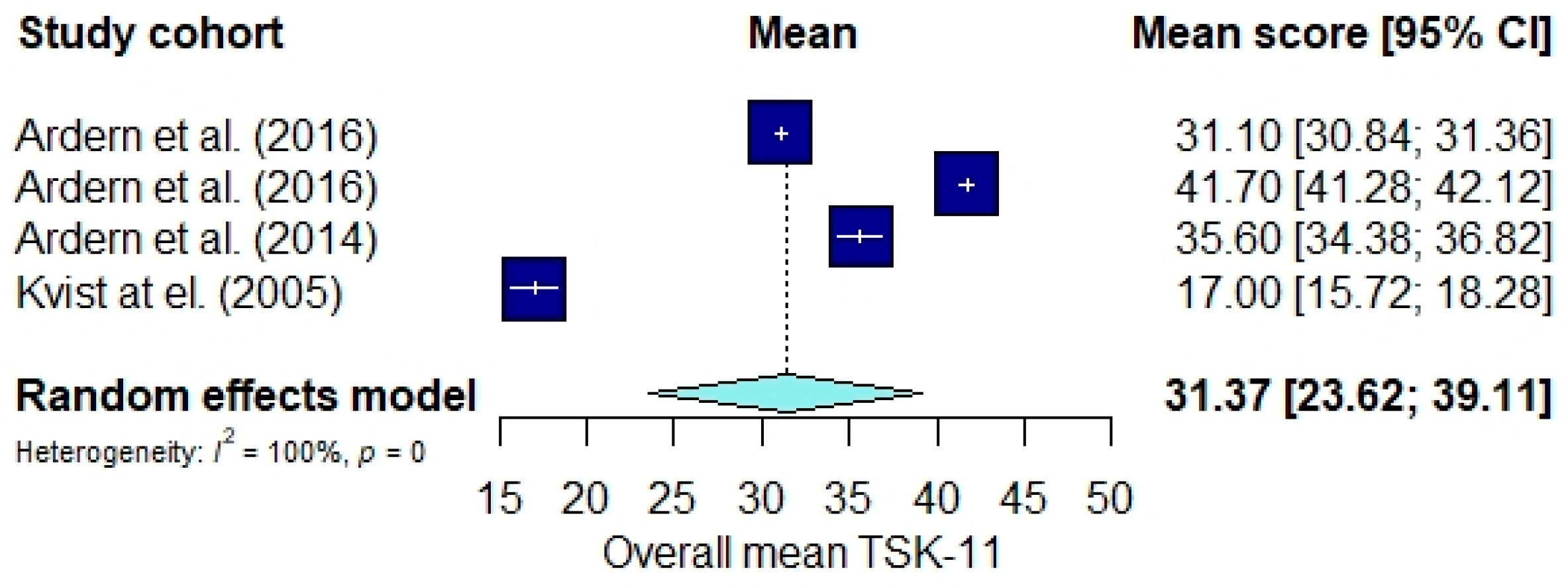
3.4. Results of the Meta-Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| Case Series | CS |
| Cross sectional | CRS |
| Case control | CC |
| Qualitative | Q |
| Cohort | Ch |
| Prospective | P |
| Prospective Observation | PO |
| Prospective Longitudinal | PL |
| Retrospective | R |
| Prospective cohort | PCh |
| Retrospective cohort | RCh |
| Mixed Methods | MM |
| Knee Injury and Osteoarthritis Outcome Score | KOOS Sport |
| Quality of Life | QoL |
| Tampa Scale of Kinesiofobia-11 | TSK-11 |
| Knee-Self Efficacy Scale | K-SES |
| Anterior Cruciate Ligament Quality of Life | ACL QoL |
| International Knee Documentation Committee | IKDC |
| Perceived Available Support in Sport | PASS |
| Activities of Daily Living | ADL |
| Emotional Responses of Athletes to Injury Questionnaire | ERAIQ |
| Single Assessment Numeric Evaluation | SANE |
| Veterans RAND 12-item Health Survey | VR-12 |
| Multidimensional Health Locus of Control | MHLC-C |
| Strategies for Self-Regulated Learning | SRLC |
| A Fear-Avoidance Beliefs Questionnaire | FABQ |
| Modified Disablement in the Physically Active-Mental Summary Component | MDPA-MSC |
| Hospital Anxiety and Depression Scale | HADS |
| Sport Anxiety Scale | SAS |
| Pain Catastrophizing Scale | PCS |
References
- Filbay, S.R.; Ackerman, I.N.; Russell, T.G.; Macri, E.M.; Crossley, K.M. Health-related quality of life after anterior cruciate ligament reconstruction: A systematic review. Am. J. Sports Med. 2014, 42, 1247–1255. [Google Scholar] [CrossRef]
- Longo, U.G.; Nagai, K.; Salvatore, G.; Cella, E.; Candela, V.; Cappelli, F.; Ciccozzi, M.; Denaro, V. Epidemiology of Anterior Cruciate Ligament Reconstruction Surgery in Italy: A 15-Year Nationwide Registry Study. J. Clin. Med. 2021, 10, 223. [Google Scholar] [CrossRef]
- Longo, U.G.; Salvatore, G.; Ruzzini, L.; Ambrogioni, L.R.; de Girolamo, L.; Viganò, M.; Facchini, F.; Cella, E.; Candela, V.; Ciccozzi, M.; et al. Trends of anterior cruciate ligament reconstruction in children and young adolescents in Italy show a constant increase in the last 15 years. Knee Surg. Sports Traumatol. Arthrosc. 2020, 29, 1728–1733. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; Viganò, M.; Candela, V.; de Girolamo, L.; Cella, E.; Thiebat, G.; Salvatore, G.; Ciccozzi, M.; Denaro, V. Epidemiology of Posterior Cruciate Ligament Reconstructions in Italy: A 15-Year Study. J. Clin. Med. 2021, 10, 499. [Google Scholar] [CrossRef] [PubMed]
- Lind, M.; Lund, B.; Faunø, P.; Said, S.; Miller, L.L.; Christiansen, S.E. Medium to long-term follow-up after ACL revision. Knee Surg. Sports Traumatol. Arthrosc. 2011, 20, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Ninkovic, S.; Avramov, S.; Harhaji, V.; Obradovic, M.; Vranjes, M.; Milankov, M. Influence of different levels of sports activities on the quality of life after the reconstruction of anterior cruciate ligament. Med Rev. 2015, 68, 116–121. [Google Scholar] [CrossRef]
- Longo, U.; Rizzello, G.; Berton, A.; Fumo, C.; Maltese, L.; Khan, W.; Denaro, V. Synthetic Grafts for Anterior Cruciate Ligament Reconstruction. Curr. Stem Cell Res. Ther. 2013, 8, 429–437. [Google Scholar] [CrossRef]
- Tengman, E.; Olofsson, L.B.; Nilsson, K.G.; Tegner, Y.; Lundgren, L.; Häger, C.K. Anterior cruciate ligament injury after more than 20 years: I. Physical activity level and knee function. Scand. J. Med. Sci. Sports 2014, 24, e491–e500. [Google Scholar] [CrossRef]
- Longo, U.G.; Rizzello, G.; Frnaceschi, F.; Campi, S.; Maffulli, N.; Denaro, V. The architecture of the ipsilateral quadriceps two years after successful anterior cruciate ligament reconstruction with bone-patellar tendon-bone autograft. Knee 2014, 21, 721–725. [Google Scholar] [CrossRef]
- Anand, B.S.; Feller, J.A.; Richmond, A.K.; Webster, K.E. Return-to-Sport Outcomes After Revision Anterior Cruciate Ligament Reconstruction Surgery. Am. J. Sports Med. 2016, 44, 580–584. [Google Scholar] [CrossRef] [PubMed]
- Burland, J.P.; Toonstra, J.L.; Howard, J.S. Psychosocial Barriers After Anterior Cruciate Ligament Reconstruction: A Clinical Review of Factors Influencing Postoperative Success. Sports Health A Multidiscip. Approach 2019, 11, 528–534. [Google Scholar] [CrossRef]
- Ardern, C.L.; Taylor, N.F.; Feller, J.A.; Webster, K.E. Fear of re-injury in people who have returned to sport following anterior cruciate ligament reconstruction surgery. J. Sci. Med. Sport 2012, 15, 488–495. [Google Scholar] [CrossRef] [PubMed]
- Maffulli, N.; Margiotti, K.; Longo, U.G.; Loppini, M.; Fazio, V.M.; Denaro, V. The genetics of sports injuries and athletic performance. Muscle Ligaments Tendons J. 2013, 3, 173–189. [Google Scholar] [CrossRef]
- Lentz, T.A.; Zeppieri, G.; George, S.Z.; Tillman, S.M.; Moser, M.W.; Farmer, K.W.; Chmielewski, T.L. Comparison of Physical Impairment, Functional, and Psychosocial Measures Based on Fear of Reinjury/Lack of Confidence and Return-to-Sport Status After ACL Reconstruction. Am. J. Sports Med. 2014, 43, 345–353. [Google Scholar] [CrossRef] [PubMed]
- Ardern, C.L.; Webster, K.E.; Taylor, N.F.; Feller, J.A. Return to the preinjury level of competitive sport after anterior cruciate ligament reconstruction surgery: Two-thirds of patients have not returned by 12 months after surgery. Am. J. Sports Med. 2011, 39, 538–543. [Google Scholar] [CrossRef]
- Kvist, J.; Ek, A.; Sporrstedt, K.; Good, L. Fear of re-injury: A hindrance for returning to sports after anterior cruciate ligament reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2005, 13, 393–397. [Google Scholar] [CrossRef]
- Ross, M.D. The relationship between functional levels and fear-avoidance beliefs following anterior cruciate ligament reconstruction. J. Orthop. Traumatol. 2010, 11, 237–243. [Google Scholar] [CrossRef] [Green Version]
- De Mozzi, P.; Longo, U.G.; Galanti, G.; Maffulli, N. Bicuspid aortic valve: A literature review and its impact on sport activity. Br. Med Bull. 2008, 85, 63–85. [Google Scholar] [CrossRef] [Green Version]
- Turk, D.C.; Wilson, H.D. Fear of Pain as a Prognostic Factor in Chronic Pain: Conceptual Models, Assessment, and Treatment Implications. Curr. Pain Headache Rep. 2010, 14, 88–95. [Google Scholar] [CrossRef] [Green Version]
- Piussi, R.; Beischer, S.; Thomeé, R.; Senorski, E.H. Superior knee self-efficacy and quality of life throughout the first year in patients who recover symmetrical muscle function after ACL reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 555–567. [Google Scholar] [CrossRef] [Green Version]
- Ochiai, S.; Hagino, T.; Tonotsuka, H.; Haro, H. Prospective analysis of health-related quality of life and clinical evaluations in patients with anterior cruciate ligament injury undergoing reconstruction. Arch. Orthop. Trauma Surg. 2011, 131, 1091–1094. [Google Scholar] [CrossRef]
- Neal, R.; Haddaway, M.J.P.; Pritchard, C.C.; McGuinness, L.A. PRISMA2020: An R Package and Shiny App for Producing PRISMA 2020-Compliant Flow Diagrams, with Interactivity for Optimised Digital Transparency and Open Synthesis; Wiley: Hoboken, NJ, USA, 2020; Volume 18. [Google Scholar]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ Clin. Res. Ed. 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef] [PubMed]
- Ardern, C.L.; Österberg, A.; Sonesson, S.; Gauffin, H.; Webster, K.E.; Kvist, J. Satisfaction with Knee Function After Primary Anterior Cruciate Ligament Reconstruction Is Associated With Self-Efficacy, Quality of Life, and Returning to the Preinjury Physical Activity. Arthrosc. J. Arthrosc. Relat. Surg. 2016, 32, 1631–1638.e3. [Google Scholar] [CrossRef] [Green Version]
- Ardern, C.L.; Österberg, A.; Tagesson, S.; Gauffin, H.; Webster, K.E.; Kvist, J. The impact of psychological readiness to return to sport and recreational activities after anterior cruciate ligament reconstruction. Br. J. Sports Med. 2014, 48, 1613–1619. [Google Scholar] [CrossRef] [Green Version]
- Hamrin Senorski, E.; Samuelsson, K.; Thomeé, C.; Beischer, S.; Karlsson, J.; Thomeé, R. Return to knee-strenuous sport after anterior cruciate ligament reconstruction: A report from a rehabilitation outcome registry of patient characteristics. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 1364–1374. [Google Scholar] [CrossRef] [Green Version]
- MARS Group; Bigouette, J.P.; Owen, E.C.; Lantz, B.A.; Hoellrich, R.G.; Huston, L.J.; Haas, A.K.; Allen, C.R.; Anderson, A.F.; Cooper, D.E.; et al. Relationship Between Sports Participation After Revision Anterior Cruciate Ligament Reconstruction and 2-Year Patient-Reported Outcome Measures. Am. J. Sports Med. 2019, 47, 2056–2066. [Google Scholar] [CrossRef]
- Muller, B.; Yabroudi, M.A.; Lynch, A.; Lai, C.-L.; Van Dijk, C.N.; Fu, F.H.; Irrgang, J.J. Defining Thresholds for the Patient Acceptable Symptom State for the IKDC Subjective Knee Form and KOOS for Patients Who Underwent ACL Reconstruction. Am. J. Sports Med. 2016, 44, 2820–2826. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Tjong, V.K.; Murnaghan, M.L.; Nyhof-Young, J.M.; Ogilvie-Harris, D.J. A qualitative investigation of the decision to return to sport after anterior cruciate ligament reconstruction: To play or not to play. Am. J. Sports Med. 2014, 42, 336–342. [Google Scholar] [CrossRef]
- Webster, K.E.; Feller, J.A.; Kimp, A.J.; Whitehead, T.S. Low Rates of Return to Preinjury Sport After Bilateral Anterior Cruciate Ligament Reconstruction. Am. J. Sports Med. 2019, 47, 334–338. [Google Scholar] [CrossRef] [PubMed]
- Baez, S.E.; Hoch, M.C.; Hoch, J.M. Psychological factors are associated with return to pre-injury levels of sport and physical activity after ACL reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Chmielewski, T.L.; Jones, D.; Day, T.; Tillman, S.M.; Lentz, T.A.; George, S.Z. The Association of Pain and Fear of Movement/Reinjury With Function During Anterior Cruciate Ligament Reconstruction Rehabilitation. J. Orthop. Sports Phys. Ther. 2008, 38, 746–753. [Google Scholar] [CrossRef]
- DiSanti, J.; Lisee, C.; Erickson, K.; Bell, D.; Shingles, M.; Kuenze, C. Perceptions of Rehabilitation and Return to Sport Among High School Athletes With Anterior Cruciate Ligament Reconstruction: A Qualitative Research Study. J. Orthop. Sports Phys. Ther. 2018, 48, 951–959. [Google Scholar] [CrossRef] [PubMed]
- Filbay, S.R.; Ackerman, I.N.; Russell, T.G.; Crossley, K.M. Return to sport matters-longer-term quality of life after ACL reconstruction in people with knee difficulties. Scand J. Med. Sci. Sports 2017, 27, 514–524. [Google Scholar] [CrossRef] [PubMed]
- Hart, H.F.; Culvenor, A.G.; Guermazi, A.; Crossley, K.M. Worse knee confidence, fear of movement, psychological readiness to return-to-sport and pain are associated with worse function after ACL reconstruction. Phys. Ther. Sport 2020, 41, 1–8. [Google Scholar] [CrossRef]
- Beischer, S.; Senorski, E.H.; Thomeé, C.; Samuelsson, K.; Thomeé, R. How Is Psychological Outcome Related to Knee Function and Return to Sport Among Adolescent Athletes After Anterior Cruciate Ligament Reconstruction? Am. J. Sports Med. 2019, 47, 1567–1575. [Google Scholar] [CrossRef]
- Ardern, C.L.; Taylor, N.F.; Feller, J.A.; Whitehead, T.S.; Webster, K.E. Psychological Responses Matter in Returning to Preinjury Level of Sport After Anterior Cruciate Ligament Reconstruction Surgery. Am. J. Sports Med. 2013, 41, 1549–1558. [Google Scholar] [CrossRef]
- Fältström, A.; Hägglund, M.; Kvist, J. Patient-Reported Knee Function, Quality of Life, and Activity Level After Bilateral Anterior Cruciate Ligament Injuries. Am. J. Sports Med. 2013, 41, 2805–2813. [Google Scholar] [CrossRef] [Green Version]
- Paterno, M.V.; Flynn, K.; Thomas, S.; Schmitt, L.C. Self-Reported Fear Predicts Functional Performance and Second ACL Injury After ACL Reconstruction and Return to Sport: A Pilot Study. Sports Health A Multidiscip. Approach 2018, 10, 228–233. [Google Scholar] [CrossRef]
- Patel, N.K.; Sabharwal, S.; Hadley, C.; Blanchard, E.; Church, S. Factors affecting return to sport following hamstrings anterior cruciate ligament reconstruction in non-elite athletes. Eur. J. Orthop. Surg. Traumatol. 2019, 29, 1771–1779. [Google Scholar] [CrossRef]
- Vega, J.F.; Jacobs, C.A.; Strnad, G.J.; Farrow, L.; Jones, M.; Miniaci, A.; Parker, R.D.; Rosneck, J.; Saluan, P.; Williams, J.S.; et al. Prospective Evaluation of the Patient Acceptable Symptom State to Identify Clinically Successful Anterior Cruciate Ligament Reconstruction. Am. J. Sports Med. 2019, 47, 1159–1167. [Google Scholar] [CrossRef] [PubMed]
- McPherson, A.L.; Feller, J.A.; Hewett, T.E.; Webster, K.E. Psychological Readiness to Return to Sport Is Associated With Second Anterior Cruciate Ligament Injuries. Am. J. Sports Med. 2019, 47, 857–862. [Google Scholar] [CrossRef] [PubMed]
- Filbay, S.R.; Crossley, K.M.; Ackerman, I.N. Activity preferences, lifestyle modifications and re-injury fears influence longer-term quality of life in people with knee symptoms following anterior cruciate ligament reconstruction: A qualitative study. J. Physiother. 2016, 62, 103–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burland, J.P.; Toonstra, J.; Werner, J.L.; Mattacola, C.G.; Howell, D.M.; Howard, J.S. Decision to Return to Sport After Anterior Cruciate Ligament Reconstruction, Part I: A Qualitative Investigation of Psychosocial Factors. J. Athl. Train. 2018, 53, 452–463. [Google Scholar] [CrossRef] [Green Version]
- Langford, J.L.; Webster, K.E.; Feller, J.A. A prospective longitudinal study to assess psychological changes following anterior cruciate ligament reconstruction surgery. Br. J. Sports Med. 2009, 43, 377–378. [Google Scholar] [CrossRef]
- Ross, C.A.; Clifford, A.; Louw, Q.A. Factors informing fear of reinjury after anterior cruciate ligament reconstruction. Physiother. Theory Pr. 2017, 33, 103–114. [Google Scholar] [CrossRef]
- Thomeé, P.; Währborg, P.; Börjesson, M.; Thomeé, R.; Eriksson, B.I.; Karlsson, J. Self-efficacy, symptoms and physical activity in patients with an anterior cruciate ligament injury: A prospective study. Scand. J. Med. Sci. Sports 2007, 17, 238–245. [Google Scholar] [CrossRef]
- Ardern, C.L. Anterior Cruciate Ligament Reconstruction-Not Exactly a One-Way Ticket Back to the Preinjury Level: A Review of Contextual Factors Affecting Return to Sport After Surgery. Sports Health 2015, 7, 224–230. [Google Scholar] [CrossRef] [Green Version]
- Xiao, M.; van Niekerk, M.; Trivedi, N.N.; Hwang, C.E.; Sherman, S.L.; Safran, M.R.; Abrams, G.D. Patients Who Return to Sport After Primary Anterior Cruciate Ligament Reconstruction Have Significantly Higher Psychological Readiness: A Systematic Review and Meta-analysis of 3744 Patients. Am. J. Sports Med. 2022, 3635465221102420. [Google Scholar] [CrossRef] [PubMed]
- Erickson, L.N.; Jacobs, C.A.; Johnson, D.L.; Ireland, M.L.; Noehren, B. Psychosocial factors 3-months after anterior cruciate ligament reconstruction predict 6-month subjective and objective knee outcomes. J. Orthop. Res. 2022, 40, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Espejo, V.; Olmedilla, A.; Abenza-Cano, L.; Garcia-Mas, A.; Ortega, E. Psychological readiness to return to sports practice and risk of recurrence: Case studies. Front. Psychol. 2022, 13, 905816. [Google Scholar] [CrossRef]
- Berton, A.; Longo, U.G.; Candela, V.; Fioravanti, S.; Giannone, L.; Arcangeli, V.; Alciati, V.; Berton, C.; Facchinetti, G.; Marchetti, A.; et al. Virtual Reality, Augmented Reality, Gamification, and Telerehabilitation: Psychological Impact on Orthopedic Patients’ Rehabilitation. J. Clin. Med. 2020, 9, 2567. [Google Scholar] [CrossRef] [PubMed]
- Abrams, G.D.; Harris, J.D.; Gupta, A.K.; McCormick, F.M.; Bush-Joseph, C.A.; Verma, N.N.; Cole, B.J.; Bach, B.R., Jr. Functional Performance Testing After Anterior Cruciate Ligament Reconstruction: A Systematic Review. Orthop. J. Sports Med. 2014, 2, 2325967113518305. [Google Scholar] [CrossRef] [PubMed]
- Maffulli, N.; Longo, U.G.; Testa, V.; Oliva, F.; Capasso, G.; Denaro, V. Italian translation of the VISA-A score for tendinopathy of the main body of the Achilles tendon. Disabil. Rehabil. 2008, 30, 1635–1639. [Google Scholar] [CrossRef]
- Longo, U.G.; King, J.B.; Denaro, V.; Maffulli, N. Double-bundle arthroscopic reconstruction of the anterior cruciate ligament: Does the evidence add up? J. Bone Jt. Surg. Br. 2008, 90, 995–999. [Google Scholar] [CrossRef] [PubMed]
- Maffulli, N.; Longo, U.G. Conservative management for tendinopathy: Is there enough scientific evidence? Rheumatology 2008, 47, 390–391. [Google Scholar] [CrossRef] [Green Version]
- Longo, U.G.; Buchmann, S.; Franceschetti, E.; Maffulli, N.; Denaro, V. A systematic review of single-bundle versus double-bundle anterior cruciate ligament reconstruction. Br. Med Bull. 2012, 103, 147–168. [Google Scholar] [CrossRef]
- Maffulli, N.; Longo, U.G. How do eccentric exercises work in tendinopathy? Rheumatology 2008, 47, 1444–1445. [Google Scholar] [CrossRef] [Green Version]
- Maffulli, N.; Longo, U.G.; Denaro, V. Anterior cruciate ligament tear. N. Engl. J. Med. 2009, 360, 1463. [Google Scholar] [PubMed]
- Longo, U.G.; Ciuffreda, M.; Casciaro, C.; Mannering, N.; Candela, V.; Salvatore, G.; Denaro, V. Anterior cruciate ligament reconstruction in skeletally immature patients: A systematic review. Bone Jt. J. 2017, 99-B, 1053–1060. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| P | Patients with ACL lesions |
| I | Patients undergoing ACL-R |
| C | Patients not undergoing ACL-R |
| O | Evaluate the quality of life and the psychological factors that influence the return to sport |
| S | Randomized control trials (RCT) and non-randomized controlled studies (NRCT) such as prospective (PS), retrospective (RS), Cross-sectional (CS), observational studies (OS), case-series (CS), and case-control (CC) studies were included. |
| Year | Location | Type of Study/LOE | Follow-Up Mean (Range) | Conclusion | |
|---|---|---|---|---|---|
| Ardern et al. [26] | 2016 | Sweden Australia | CS IV | 3 y (1–7 y) | People who reported higher knee-related self-efficacy and quality of life were more likely to be satisfied with the outcome of ACL reconstruction. |
| Ardern et al. [27] | 2014 | Australia Sweden | CrS III | 35 m (12–81 m) | Psychological readiness to return to sport and recreation was the factor most strongly associated with returning to the preinjury activity. |
| Ardern et al. [12] | 2012 | Australia | CrS III | - (2–7 y) | The gender, the timing of surgery following injury, and the level of sport the athletes returned to may be associated with fear of re-injury following surgery. |
| Arden et al. [40] | 2013 | Australia | CC III | - (4–12 m) | Psychological responses before surgery and in early recovery were associated with returning to the preinjury level of sport at 12 months. |
| Baez et al. [34] | 2020 | USA | CrS III | 5 y - | Psychological factors, specifically injury-related fear and self-efficacy, were associated more significantly than functional outcomes with return to sport and physical activity levels. |
| Beischer et al. [39] | 2019 | Sweden | CC III | 8–12 m - | Regardless of age, athletes who had returned to the sport and athletes with more symmetrical muscle function had a stronger psychological profile. |
| Burland et al. [47] | 2018 | USA | Q | 1 y - | After ACL-R, the decision to return to sport was largely influenced by psychosocial factors. |
| Chmielewski et al. [35] | 2008 | USA | CrS IV | - (12 w-1 y) | Fear of movement/reinjury levels appears to decrease during ACL reconstruction rehabilitation. |
| DiSanti et al. [36] | 2018 | USA | CrS III | 5.5±1.4 m | Early identification of athletes at risk of persistent psychosocial barriers and the establishment of peer mentoring groups can be key components for improving mental and physical readiness for Revised Trauma Score (RTS). |
| Fältström et al. [41] | 2013 | Sweden | Ch III | - (2–5 y) | Patients with bilateral ACL injuries reported poorer knee function and quality of life compared with those who had undergone unilateral ACL reconstruction. |
| Filbay et al. [46] | 2016 | Australia | Q | - (5–20 y) | Activity preferences, lifestyle modifications, and fear of re-injury influenced the quality of life in people with knee symptoms following ACLR. |
| Filbay et al. [37] | 2017 | Australia | CrS IV | 9 ± 4 (5–20 y) | Many individuals experience long-term quality of life (QOL) impairment following ACL-R. |
| Hamrin et al. [28] | 2017 | Sweden | PO II | 10 w, 4, 8, 12, 18, and 24 m and then yearly up to 5 y | Patients who returned to sports after ACL-R had better subjective knee function and higher self-efficacy of knee function. |
| Hart et al. [38] | 2020 | Canada Australia USA | CrS III | 1 y (11–15) | Evaluating and considering knee confidence, fear of movement, and psychological readiness should be an important part of comprehensive post-ACLR rehabilitation. |
| Kvist et al. [16] | 2005 | Sweden | CrS III | - 3–4 y) | Fear of re-injury must be considered in the rehabilitation and evaluation of the effects of an ACL reconstruction. |
| Langford et al. [48] | 2009 | Australia | PL II | 3, 6 and 12 m | During rehabilitation, there are significant psychological differences regarding sport resumption between athletes who do and do not resume competitive sport 12 months following ACL reconstruction. |
| Lind et al. [5] | 2012 | Denmark | R IV | 6 y (2–9 y) | The subjective outcome of the scores indicate significant knee impairment with low scores in sports and quality of life. |
| Lentz et al. [14] | 2015 | USA | CC III | - (6 m and 1 y) | Elevated pain-related fear of movement/reinjury, quadriceps weakness, and reduced IKDC score distinguish patients who are unable to return to preinjury sports participation. |
| Mars Group [29] | 2019 | USA | CrS III | 2 y - | Participation in either a single or multiple sports in the 2 years after ACL revision surgery was found to be significantly associated with higher PROMs. |
| McPherson et al. [45] | 2019 | Australia | Ch II | - (2–4 y) | Younger patients with lower psychological readiness are at higher risk for a second ACL injury after returning to sport. |
| Muller et al. [30] | 2016 | USA | Ch II | 3.4 ± 1.3 y (1–5 y) | This study has identified PASS threshold values for the IKDC-SKF and the KOOS subscales. |
| Ninković et al. [6] | 2015 | Serbia | CrS III | 1 y - | The overall life quality a year after the ACL-R does not differ in relation to either the gender of the subjects or the type of sports activity. |
| Paterno et al. [42] | 2018 | USA | PCh II | - (1–2 y) | Patients with greater self-reported fear were less active. |
| Piussi et al. [20] | 2020 | Sweden | CC III | 10 w, 4, 8, and 12 m | Patients who recovered strength and symmetry 12 months after ACL-R correlated with upper knee self-efficacy and higher quality of life. |
| Patel et al. [43] | 2019 | USA UK | RCh III | 50 m (24–224 m) | A significant number of non-elite athletes did not perform RTS after ACL reconstruction, and this was affected by a combination of activity level, sport, self-reported knee instability, and psychosocial factors. |
| Ross et al. [49] | 2017 | South Africa UK | MM | - (12–36 m) | Modifiable fears including pain, mode and length of rehabilitation, and psychological factors should be considered during rehabilitation to potentially improve the return to sport rate. |
| Ross et al. [17] | 2010 | USA | - | 31.7 ± 16.2 m | These results suggest that fear-avoidance beliefs following ACLR can potentially adversely influence functional levels in activities of daily living and sports. |
| Tengman et al. [8] | 2014 | Sweden | CrS III | 20 y | The decreased knee function, knee-related physical activity level, and jump capacity may be associated with fear of movement also in the long-term perspective. |
| Thomee et al. [50] | 2007 | Sweden | P II | 3 m, 6 m,1 y | Self-efficacy belief may be of major importance for the outcome of rehabilitation after sports-related injuries. |
| Tjion et al. [32] | 2015 | Canada | CS IV | (2–10 y) | Recognizing and addressing the psychological factors and lifestyle changes can contribute to the patient’s decision to return to sports. |
| Vega et al. [33,44] | 2019 | USA | Ch II | 1 y - | The PASS question identifies individuals who have experienced clinically successful ACLR with high sensitivity. |
| Webster et al. [33] | 2019 | Australia | CS IV | 5.3 y (2.5–10 y) | Fear of reinjury was the most common reason cited for failure to return to sport after the second reconstruction. |
| Study | Sample Size | Mean Age | Sport and Sport Participation Level |
|---|---|---|---|
| Ardern et al. [26] | 177 (100 men and 70 women) | 18–45 y | 62% playing sub-elite competitive sport. 24% participated in active recreation. 16% playing élite sport. |
| Ardern et al. [27] | 164 - | 18–45 y | sub-elite competitive level (64%). elite competitive level (15%). Recreational level (21%). |
| Ardern et al. [12] | 209 (88 woman and 121 men) | - 31.7 ± 9.7 | Australian football (n = 60, 29%), netball (n = 40, 19%), basketball (n = 32, 15%), and soccer (n = 23, 11%). |
| Arden et al. [40] | 187 - | _ | Recreational or competitive level. |
| Baez et al. [34] | 40 (24 woman and 16 men) | 18–35 y 24.3 ± 4.1 | _ |
| Beischer et al. [39] | 384 (50% women) and 271 athletes (52% women) | 15–30 y | Athletes. |
| Burland et al. [47] | 12 (6 men and 6 women) | 16–44 y 24 ± 8 | Competitive athletics. |
| Chmielewski et al. [35] | 97 (60 men and 37 women) | Group 1: 26.2 ± 9.2 Group 2: 25.3 ± 11.0 Group 3: 24.0 ± 7.7 | - |
| DiSanti et al. [36] | 10 (6 women and 4 men) | 15–18 y 16.8 ± 1.1 | basketball (n = 2), soccer (n = 2), football (n = 2), volleyball (n = 1), skiing (n = 83 1), ice hockey (n = 1), and lacrosse (n = 1) |
| Fältström et al. [41] | 147 (42% female) | 18–45 y 28.5 ± 8.2 | Soccer, Handball, Basketball, Floorball, Downhill skiing, Motor sport, Other sport. |
| Filbay et al. [46] | 17 (10 women and 7 men) | 18–25 y | - |
| Filbay et al. [37] | 162 - | - 38 ± 9 | Athletes. |
| Hamrin et al. [28] | 157 (77 women and 80 men) | 15–30 y | - |
| Hart et al. [38] | 118 - | 18 -50 y | Pivoting sport. |
| Kvist et al. [16] | 84 62 patients (74%) answered the questionnaires (34 men and 28 women). | 16–35 y | soccer, handball, ice hockey, floorball, or American football. |
| Langford et al. [48] | 87 (55 men 32 women) | 18–40 y | Competitive sport. |
| Lind et al. [5] | 128 (50% men) | - 32 | - |
| Lentz et al. [14] | 73 - | 15–50 y | Recreational sport. |
| Mars Group [29] | 1205 - | 12–65 y | Baseball/softball, Basketball, Football, Gymnastics, Skiing, Soccer, Volleyball, Other. |
| McPherson et al. [45] | 329 - | 132 ≤20 y and 197 ≥20 y | - |
| Muller et al. [30] | 251 - | 14–50 y (26.1 ± 9.9) | Light sports activity, moderate sports activity, moderate sports activity, strenuous sports activity. |
| Ninković et al. [6] | 185 (146 men and 39 women) | - | Professional/amateur athletes. |
| Paterno et al. [42] | 40 - | 10–25 y | high-level athletic activity: pivoting and cutting. |
| Piussi et al. [20] | 328 (120 men 37%) | 15–65 y 27.8 ± 10 | - |
| Patel et al. [43] | 78 (46 men) | 16–50 y 31.5 y | Non-élite athletes. |
| Ross et al. [49] | 112 (78 men and 34 women) | 15–50 y | Athletes. |
| Ross et al. [17] | 48 (34 men and 14 women) | - 20.6 ± 1.2 | required military and athletic activities. |
| Tengman et al. [8] | 103 (65 men and 28 women) | 17–28 y 23 | Soccer, alpine, other sport. |
| Thomee et al. [50] | 33 (15 women and 18 men) | 17–55 y 29.2 | Baseline physical activity. |
| Tjion et al. [32] | 31 (22 men and 9women) | 18–40 | Soccer, football, ultimate frisbee, basketball, hockey, and others. A level: recreational, varsity high school, varsity college/university, paid professional. |
| Vega et al. [33,44] | 300 patients | 300 completed follow-ups: 26.2 mage (24.8–27.6) | Athletes. |
| Webster et al. [33] | 107 (62 men and 45 women) | - 2 | football, netball, basketball, and soccer. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Longo, U.G.; De Salvatore, S.; D’Orrico, F.; Bella, M.; Corradini, A.; Rizzello, G.; De Marinis, M.G.; Denaro, V. The Impact of Psychological Factors on Return to Sports after Anterior Cruciate Ligament Reconstruction: A Systematic Review. Osteology 2023, 3, 78-93. https://doi.org/10.3390/osteology3030009
Longo UG, De Salvatore S, D’Orrico F, Bella M, Corradini A, Rizzello G, De Marinis MG, Denaro V. The Impact of Psychological Factors on Return to Sports after Anterior Cruciate Ligament Reconstruction: A Systematic Review. Osteology. 2023; 3(3):78-93. https://doi.org/10.3390/osteology3030009
Chicago/Turabian StyleLongo, Umile Giuseppe, Sergio De Salvatore, Federica D’Orrico, Matilda Bella, Alessandra Corradini, Giacomo Rizzello, Maria Grazia De Marinis, and Vincenzo Denaro. 2023. "The Impact of Psychological Factors on Return to Sports after Anterior Cruciate Ligament Reconstruction: A Systematic Review" Osteology 3, no. 3: 78-93. https://doi.org/10.3390/osteology3030009
APA StyleLongo, U. G., De Salvatore, S., D’Orrico, F., Bella, M., Corradini, A., Rizzello, G., De Marinis, M. G., & Denaro, V. (2023). The Impact of Psychological Factors on Return to Sports after Anterior Cruciate Ligament Reconstruction: A Systematic Review. Osteology, 3(3), 78-93. https://doi.org/10.3390/osteology3030009