
Persufflation—Current State of Play


Abstract
1. Introduction
2. Material and Methods: Literature Research
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
3. Persufflation
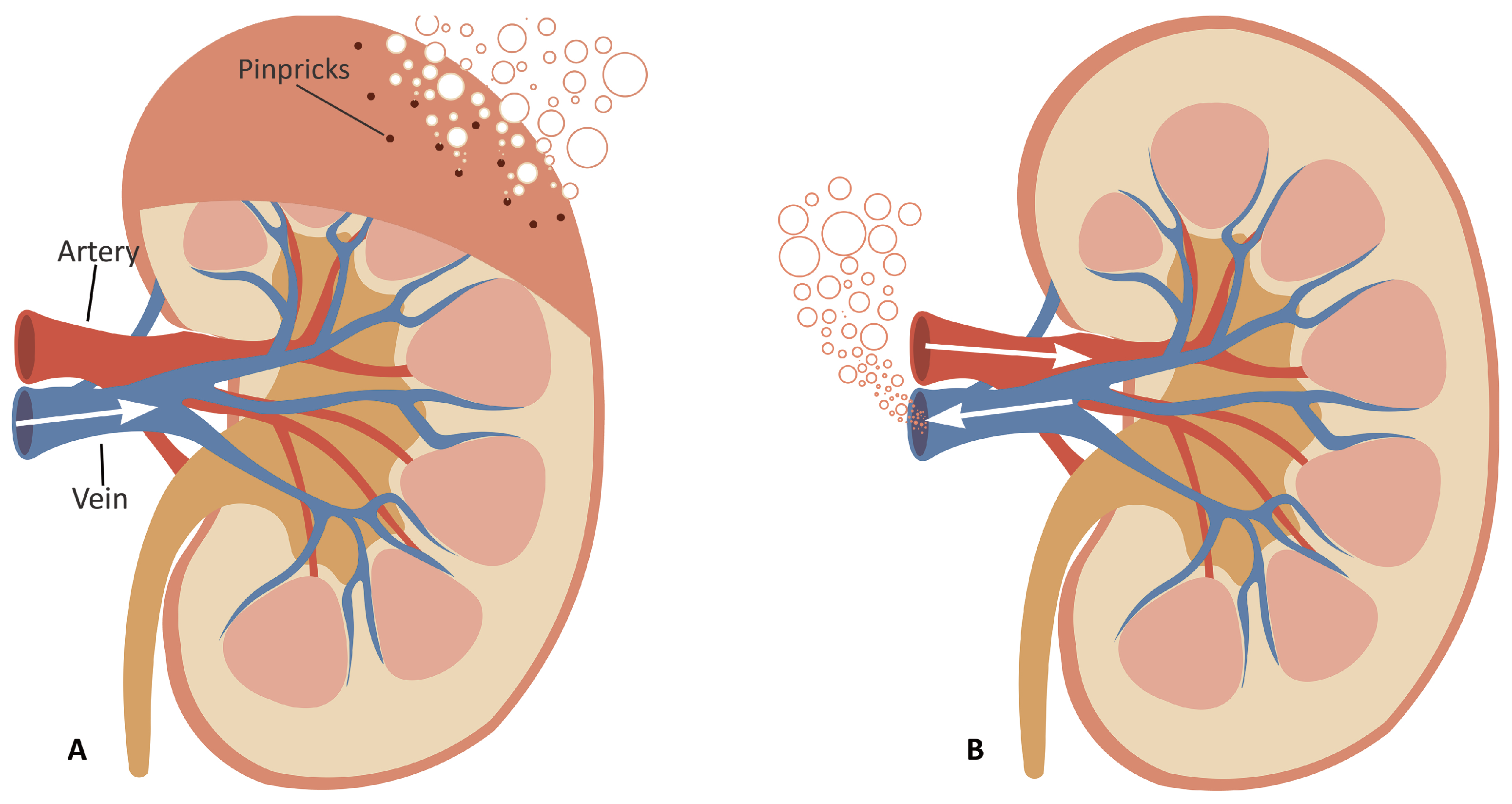
3.1. What Is Persufflation?
3.2. History (1902–2005)
4. Recent Works (Post–2005)
4.1. Liver
4.1.1. Liver Persufflation in a Rat Model
4.1.2. Adjuvant Approaches during Liver Persufflation
4.1.3. Liver Persufflation in a Large Animal and Human Preclinical Models
4.1.4. Clinical Liver Persufflation
4.2. Kidney
Kidney Persufflation in a Large Animal Model
4.3. Pancreas
4.3.1. Pancreas Persufflation in a Rat Model
4.3.2. Pancreas Persufflation in a Large Animal and Human Model
5. Other Applications
6. Alternate Techniques
7. Market Potential
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| A-PSF | Anterograde Persufflation |
| ATP | Adenosine Triphosphate |
| CO | Carbon Monoxide |
| DBD | Donated after Brain Death |
| DCD | Donated after Cardiac Death |
| GFR | Glomerular Filtration Rate |
| HMP | Hypothermic Machine Perfusion |
| HR | Hypothermic Reconditioning |
| IRI | Ischaemia Reperfusion Injury |
| NMP | Normothermic Machine Perfusion |
| NO | Nitric Oxide |
| OPAL | Oxygen Persufflation as Adjunct in Liver preservation |
| PSF | Persufflation |
| R-PSF | Retrograde Persufflation |
| SCS | Static Cold Storage |
| TLM | Two-Layer Methods |
| WIT | Warm Ischaemia Time |
| WOOCR | Whole Organ Oxygen Consumption Rate |
References
- NHSBT. Organ Donation and Transplantation Activity Report 2019/20. 2020. Available online: https://www.odt.nhs.uk/statistics-and-reports/annual-activity-report/ (accessed on 30 April 2021).
- OPTN/SRTR 2018 Annual Data Report. Am. J. Transplant. 2020, 20, 1–10. [CrossRef]
- The Parliment of the UK. Organ Donation (Deemed Consent) Act 2019, c.7. 2019. Available online: https://www.legislation.gov.uk/ukpga/2019/7/contents/enacted (accessed on 19 July 2021).
- Hussain, N. Max and Keira’s law: An overview on the advantages, disadvantages and alternatives to an opt-out organ donation system in the UK. Br. Stud. Dr. J. 2020, 4, 26–31. [Google Scholar] [CrossRef]
- Dept. of Health and Human Services, Centers for Medicare & Medicaid Services. Organ Procurement Organizations (OPOs) (CMS-3380). RIN: 0938-AU02. 2020. Available online: https://www.cms.gov/files/document/112020-opo-final-rule-cms-3380-f.pdf (accessed on 19 July 2021).
- Johnston, T.D.; Thacker, L.R.; Jeon, H.; Lucas, B.A.; Ranjan, D. Sensitivity of expanded-criteria donor kidneys to cold ischaemia time. Clin. Transplant. 2004, 18 (Suppl. 12), 28–32. [Google Scholar] [CrossRef] [PubMed]
- Saidi, R.F.; Elias, N.; Kawai, T.; Hertl, M.; Farrell, M.L.; Goes, N.; Wong, W.; Hartono, C.; Fishman, J.A.; Kotton, C.N.; et al. Outcome of kidney transplantation using expanded criteria donors and donation after cardiac death kidneys: Realities and costs. Am. J. Transplant. 2007, 7, 2769–2774. [Google Scholar] [CrossRef] [PubMed]
- Iwanaga, Y.; Sutherland, D.E.; Harmon, J.V.; Papas, K.K. Pancreas preservation for pancreas and islet transplantation. Curr. Opin. Organ. Transplant. 2008, 13, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Taylor, M.J.; Baicu, S.C. Current state of hypothermic machine perfusion preservation of organs: The clinical perspective. Cryobiology 2010, 60, 20–35. [Google Scholar] [CrossRef]
- Magnus, R. Thätigkeit des überlebenden Säugethierherzens bei Durchströmung mit Gasen. Arch. Exp. Pathol. Pharmakol. 1902, 47, 200–208. [Google Scholar] [CrossRef]
- Barker, C.F.; Markmann, J.F. Historical overview of transplantation. Cold. Spring Harb. Perspect. Med. 2013, 3, a014977. [Google Scholar] [CrossRef]
- Isselhard, W.; Denecke, H.; Witte, J.; Berger, M.; Fischer, J.H. Renal function after hypothermic kidney ischemia with orthograde and retrograde O2-persulflation in situ. Res. Exp. Med. 1972, 157, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Stegemann, J.; Minor, T. Energy charge restoration, mitochondrial protection and reversal of preservation induced liver injury by hypothermic oxygenation prior to reperfusion. Cryobiology 2009, 58, 331–336. [Google Scholar] [CrossRef]
- Lonze, B.E.; Parsikia, A.; Feyssa, E.L.; Khanmoradi, K.; Araya, V.R.; Zaki, R.F.; Segev, D.L.; Ortiz, J.A. Operative start times and complications after liver transplantation. Am. J. Transplant. 2010, 10, 1842–1849. [Google Scholar] [CrossRef]
- Minor, T.; von Horn, C. Rewarming Injury after Cold Preservation. Int. J. Mol. Sci. 2019, 20, 2059. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Wang, Y.; Zhang, J.; Wang, L.; Fu, L.; Cha, B.J.; Buggs, J.; Liu, R. A mouse model of renal ischemia-reperfusion injury solely induced by cold ischemia. Am. J. Physiol. Ren. Physiol. 2019, 317, F616–F622. [Google Scholar] [CrossRef]
- Scott, W.E.; Weegman, B.P.; Ferrer-Fabrega, J.; Stein, S.A.; Anazawa, T.; Kirchner, V.A.; Rizzari, M.D.; Stone, J.; Matsumoto, S.; Hammer, B.E.; et al. Pancreas oxygen persufflation increases ATP levels as shown by nuclear magnetic resonance. Transplant. Proc. 2010, 42, 2011–2015. [Google Scholar] [CrossRef] [PubMed]
- Treckmann, J.; Nagelschmidt, M.; Minor, T.; Saner, F.; Saad, S.; Paul, A. Function and quality of kidneys after cold storage, machine perfusion, or retrograde oxygen persufflation: Results from a porcine autotransplantation model. Cryobiology 2009, 59, 19–23. [Google Scholar] [CrossRef]
- Minor, T.; Paul, A. Hypothermic reconditioning in organ transplantation. Curr. Opin. Organ. Transplant. 2013, 18, 161–167. [Google Scholar] [CrossRef]
- Fischer, J.H. Hypothermic liver preservation using different flush solutions and retrograde oxygen persufflation technique. Eur. Surg. Res. 1980, 12, 19–20. [Google Scholar]
- Merrill, J.P.; Murray, J.E.; Harrison, J.H.; Guild, W.R. Successful homotransplantation of the human kidney between identical twins. J. Am. Med. Assoc. 1956, 160, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Arnold, G.; Müller-Ruchholtz, E.R.; Lochner, W. The prolongation of the survival time of ischemic hearts by perfusing the coronary arteries with gaseous oxygen. Arztl. Forsch. 1968, 22, 257–264. [Google Scholar]
- Burns, B.D.; Robson, J.G.; Smith, G.K. The survival of mammalian tissues perfused with intravascular gas mixtures of oxygen and carbon dioxide. Can. J. Biochem. Physiol. 1958, 36, 499–504. [Google Scholar] [CrossRef]
- Sabiston, D.C.; Talbert, J.L.; Riley, L.H.; Blalock, A. Maintenance of the heart beat by perfusion of the coronary circulation with gaseous oxygen. Ann. Surg. 1959, 150, 361–370. [Google Scholar] [CrossRef]
- Camishion, R.C.; Davies, A.L.; Tokunaga, K.; Solit, R.W. Retrograde perfusion of the coronary arteries with gaseous oxygen cardiopulmonary bypass. Surgery 1966, 59, 145–154. [Google Scholar]
- Isselhard, W.; Berger, M.; Denecke, H.; Witte, J.; Fischer, J.H.; Molzberger, H. Metabolism of canine kidneys in anaerobic ischemia and in aerobic ischemia by persufflation with gaseous oxygen. Pflugers Arch. 1972, 337, 87–106. [Google Scholar] [CrossRef] [PubMed]
- Sachweh, D.; Isselhard, W.; Dennecke, H.; Stelter, W.J.; Berger, M.; Lauschke, H.; Eigler, W.F. Short time kidney preservation by hypothermic oxygen persufflation. Bull. Soc. Int. Chir. 1972, 31, 258–263. [Google Scholar] [PubMed]
- Isselhard, W.; Denecke, H.; Stelter, W.; Berger, M.; Sachweh, D.; Witte, J.; Fischer, J.H. Function and metabolism of canine kidneys after aerobic ischemia by orthograde persufflation with gaseous oxygen. Res. Exp. Med. 1973, 159, 288–297. [Google Scholar] [CrossRef] [PubMed]
- Isselhard, W.; Witte, J.; Denecke, H.; Berger, M.; Fischer, J.H.; Molzberger, H. Function and metabolism of canine kidneys after aerobic ischemia by retrograde persufflation with gaseous oxygen. Res. Exp. Med. 1974, 164, 35–44. [Google Scholar] [CrossRef]
- Rolles, K.; Foreman, J.; Pegg, D.E. A pilot clinical study of retrograde oxygen persufflation in renal preservation. Transplantation 1989, 48, 339–342. [Google Scholar] [PubMed]
- Minor, T.; Isselhard, W. Synthesis of high energy phosphates during cold ischemic rat liver preservation with gaseous oxygen insufflation. Transplantation 1996, 61, 20–22. [Google Scholar] [CrossRef]
- Minor, T.; Isselhard, W.; Klauke, H. Reduction in nonparenchymal cell injury and vascular endothelial dysfunction after cold preservation of the liver by gaseous oxygen. Transplant. Int. 1996, 9 (Suppl. 1), S425–S428. [Google Scholar] [CrossRef]
- Minor, T.; Klauke, H.; Isselhard, W. Improved preservation of the small bowel by luminal gas oxygenation: Energetic status during ischemia and functional integrity upon reperfusion. Transplant. Proc. 1997, 29, 2994–2996. [Google Scholar] [CrossRef]
- Minor, T.; Saad, S.; Nagelschmidt, M.; Kötting, M.; Fu, Z.; Paul, A.; Isselhard, W. Successful transplantation of porcine livers after warm ischemic insult in situ and cold preservation including postconditioning with gaseous oxygen. Transplantation 1998, 65, 1262–1264. [Google Scholar] [CrossRef] [PubMed]
- Kuhn-Régnier, F.; Bloch, W.; Tsimpoulis, I.; Reismann, M.; Dagktekin, O.; Jeschkeit-Schubbert, S.; Funcke, C.; Fries, J.W.; Addicks, K.; de Vivie, E.R.; et al. Coronary oxygen persufflation for heart preservation in pigs: Analyses of endothelium and myocytes. Transplantation 2004, 77, 28–35. [Google Scholar] [CrossRef]
- Fischer, J.H.; Funcke, C.; Yotsumoto, G.; Jeschkeit-Schubbert, S.; Kuhn-Régnier, F. Maintenance of physiological coronary endothelial function after 3.3 h of hypothermic oxygen persufflation preservation and orthotopic transplantation of non-heart-beating donor hearts. Eur. J. Cardiothorac. Surg. 2004, 25, 98–104. [Google Scholar] [CrossRef][Green Version]
- Lauschke, H.; Kötting, M.; Akbar, S.; Minor, T. Use of taurine as antioxidant in resuscitating livers from non-heart-beating donors by gaseous oxygen persufflation. J. Investig. Surg. 2003, 16, 7–11. [Google Scholar] [CrossRef]
- Saad, S.; Minor, T.; Kötting, M.; Fu, Z.X.; Hagn, U.; Paul, A.; Nagelschmidt, M. Extension of ischemic tolerance of porcine livers by cold preservation including postconditioning with gaseous oxygen. Transplantation 2001, 71, 498–502. [Google Scholar] [CrossRef]
- Treckmann, J.W.; Paul, A.; Saad, S.; Hoffmann, J.; Waldmann, K.H.; Broelsch, C.E.; Nagelschmidt, M. Primary organ function of warm ischaemically damaged porcine kidneys after retrograde oxygen persufflation. Nephrol. Dial. Transplant. 2006, 21, 1803–1808. [Google Scholar] [CrossRef] [PubMed]
- Tolba, R.H.; Schildberg, F.A.; Schnurr, C.; Glatzel, U.; Decker, D.; Minor, T. Reduced liver apoptosis after venous systemic oxygen persufflation in non-heart-beating donors. J. Investig. Surg. 2006, 19, 219–227. [Google Scholar] [CrossRef]
- Treckmann, J.; Minor, T.; Saad, S.; Ozcelik, A.; Malagó, M.; Broelsch, C.E.; Paul, A. Retrograde oxygen persufflation preservation of human livers: A pilot study. Liver Transplant. 2008, 14, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Koetting, M.; Dombrowski, F.; Minor, T. No synergistic effect of carbon monoxide and oxygen during static gaseous persufflation preservation of DCD livers. J. Surg. Res. 2011, 171, 859–864. [Google Scholar] [CrossRef]
- Ye, S.; Dong, J.; Han, B. Protective effect of reduced glutathione and venous systemic oxygen persufflation on rat steatotic graft following liver transplantation. J. Surg. Res. 2010, 158, 138–146. [Google Scholar] [CrossRef]
- Koetting, M.; Leuvenink, H.; Dombrowski, F.; Minor, T. Gaseous persufflation with carbon monoxide during ischemia protects the isolated liver and enhances energetic recovery. Cryobiology 2010, 61, 33–37. [Google Scholar] [CrossRef]
- Koetting, M.; Lüer, B.; Efferz, P.; Paul, A.; Minor, T. Optimal time for hypothermic reconditioning of liver grafts by venous systemic oxygen persufflation in a large animal model. Transplantation 2011, 91, 42–47. [Google Scholar] [CrossRef] [PubMed]
- Minor, T.; Koetting, M.; Koetting, M.; Kaiser, G.; Efferz, P.; Lüer, B.; Paul, A. Hypothermic reconditioning by gaseous oxygen improves survival after liver transplantation in the pig. Am. J. Transplant. 2011, 11, 2627–2634. [Google Scholar] [CrossRef] [PubMed]
- Minor, T.; Pütter, C.; Gallinat, A.; Ose, C.; Kaiser, G.; Scherag, A.; Treckmann, J.; Paul, A. Oxygen persufflation as adjunct in liver preservation (OPAL): Study protocol for a randomized controlled trial. Trials 2011, 12, 234. [Google Scholar] [CrossRef]
- Koetting, M.; Minor, T. Donation after cardiac death: Dynamic graft reconditioning during or after ischemic preservation? Artif. Organs 2011, 35, 565–571. [Google Scholar] [CrossRef]
- Srinivasan, P.K.; Yagi, S.; Doorschodt, B.; Nagai, K.; Afify, M.; Uemoto, S.; Tolba, R. Impact of venous systemic oxygen persufflation supplemented with nitric oxide gas on cold-stored, warm ischemia-damaged experimental liver grafts. Liver Transplant. 2012, 18, 219–225. [Google Scholar] [CrossRef]
- Minor, T.; Scott, W.E.; Rizzari, M.D.; Suszynski, T.M.; Lüer, B.; Efferz, P.; Papas, K.K.; Paul, A. Energetic recovery in porcine grafts by minimally invasive liver oxygenation. J. Surg. Res. 2012, 178, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Nagai, K.; Yagi, S.; Afify, M.; Bleilevens, C.; Uemoto, S.; Tolba, R.H. Impact of venous-systemic oxygen persufflation with nitric oxide gas on steatotic grafts after partial orthotopic liver transplantation in rats. Transplantation 2013, 95, 78–84. [Google Scholar] [CrossRef]
- Yagi, S.; Nagai, K.; Kadaba, P.; Afify, M.; Teramukai, S.; Uemoto, S.; Tolba, R.H. A novel organ preservation for small partial liver transplantations in rats: Venous systemic oxygen persufflation with nitric oxide gas. Am. J. Transplant. 2013, 13, 222–228. [Google Scholar] [CrossRef]
- Lüer, B.; Fox, M.; Efferz, P.; Minor, T. Adding pulsatile vascular stimulation to venous systemic oxygen persufflation of liver grafts. Artif. Organs 2014, 38, 404–410. [Google Scholar] [CrossRef]
- Kageyama, S.; Yagi, S.; Tanaka, H.; Saito, S.; Nagai, K.; Hata, K.; Fujimoto, Y.; Ogura, Y.; Tolba, R.; Shinji, U. Graft reconditioning with nitric oxide gas in rat liver transplantation from cardiac death donors. Transplantation 2014, 97, 618–625. [Google Scholar] [CrossRef]
- Khorsandi, S.E.; Jitraruch, S.; Fairbanks, L.; Cotoi, C.; Jassem, W.; Vilca-Melendez, H.; Prachalias, A.; Dhawan, A.; Heaton, N.; Srinivasan, P. The effect of anterograde persufflation on energy charge and hepatocyte function in donation after cardiac death livers unsuitable for transplant. Liver Transplant. 2014, 20, 698–704. [Google Scholar] [CrossRef]
- Porschen, A.; Kadaba Srinivasan, P.; Iwasaki, J.; Afify, M.; Tolba, R.H. Optimal Timing for Venous Systemic Oxygen Persufflation Supplemented with Nitric Oxide Gas in Cold-Stored, Warm Ischemia-Damaged Experimental Liver Grafts. Eur. Surg. Res. 2016, 57, 100–110. [Google Scholar] [CrossRef]
- Jafari, A.; Matthaei, H.; Branchi, V.; Bölke, E.; Tolba, R.H.; Kalff, J.C.; Manekeller, S. Donor liver quality after hypovolemic shock and venous systemic oxygen persufflation in an experimental animal model. Eur. J. Med. Res. 2018, 23, 51. [Google Scholar] [CrossRef]
- Gallinat, A.; Hoyer, D.P.; Sotiropoulos, G.; Treckmann, J.; Benkoe, T.; Belker, J.; Saner, F.; Paul, A.; Minor, T. Oxygen Persufflation in Liver Transplantation Results of a Randomized Controlled Trial. Bioengineering 2019, 6, 35. [Google Scholar] [CrossRef]
- Minor, T.; Lüer, B.; von Horn, C.; Paul, A.; Gallinat, A. Effect of oxygen concentration in anterograde liver persufflation on high energy phosphates and graft function after ischemic preservation. Cryobiology 2020, 92, 248–250. [Google Scholar] [CrossRef]
- de Vries, R.J.; Tessier, S.N.; Banik, P.D.; Nagpal, S.; Cronin, S.E.J.; Ozer, S.; Hafiz, E.O.A.; van Gulik, T.M.; Yarmush, M.L.; Markmann, J.F.; et al. Supercooling extends preservation time of human livers. Nat. Biotechnol. 2019, 37, 1131–1136. [Google Scholar] [CrossRef] [PubMed]
- Álvarez-Mercado, A.I.; Gulfo, J.; Romero Gómez, M.; Jiménez-Castro, M.B.; Gracia-Sancho, J.; Peralta, C. Use of Steatotic Grafts in Liver Transplantation: Current Status. Liver Transplant. 2019, 25, 771–786. [Google Scholar] [CrossRef]
- Kamath, P.S.; Kim, W.R. The model for end-stage liver disease (MELD). Hepatology 2007, 45, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Kalenski, J.; Mancina, E.; Paschenda, P.; Beckers, C.; Bleilevens, C.; Túthová, Ĺ.; Boor, P.; Gross, D.; Tolba, R.H.; Doorschodt, B.M. Comparison of Aerobic Preservation by Venous Systemic Oxygen Persufflation or Oxygenated Machine Perfusion of Warm-Ischemia-Damaged Porcine Kidneys. Eur. Surg. Res. 2016, 57, 10–21. [Google Scholar] [CrossRef] [PubMed]
- Minor, T.; Efferz, P.; Lüer, B. Hypothermic reconditioning by gaseous oxygen persufflation after cold storage of porcine kidneys. Cryobiology 2012, 65, 41–44. [Google Scholar] [CrossRef] [PubMed]
- Moláček, J.; Opatrný, V.; Matějka, R.; Baxa, J.; Třeška, V. Retrograde Oxygen Persufflation of Kidney—Experiment on an Animal. In Vivo 2016, 30, 801–805. [Google Scholar] [CrossRef]
- Moláček, J.; Opatrný, V.; Třeška, V.; Matějka, R.; Hes, O. Options to improve the quality of kidney grafts from expanded criteria donors experimental study. Rozhl. Chir. 2018, 97, 193–201. [Google Scholar]
- Min, C.G. Evaluation of Persufflation and Cold Storage Preservation in Isolated Porcine Kidneys Using Novel Methods for Organ Quality Assessments. Ph.D. Thesis, University of Arizona, Tucson, AZ, USA, 2018. [Google Scholar]
- Reddy, M.S.; Carter, N.; Cunningham, A.; Shaw, J.; Talbot, D. Portal Venous Oxygen Persufflation of the Donation after Cardiac Death pancreas in a rat model is superior to static cold storage and hypothermic machine perfusion. Transplant. Int. 2014, 27, 634–639. [Google Scholar] [CrossRef] [PubMed]
- Kawamura, T.; Kuroda, Y.; Suzuki, Y.; Fujiwara, H.; Yamamoto, K.; Saitoh, Y. A new simple two layer (Euro-Collins’ solution/perfluorochemical) cold storage method for pancreas preservation. Transplant. Proc. 1989, 21, 1376–1377. [Google Scholar]
- Scott, W.E., III. Application of NMR in the Characterization of Existing and Development of New Methods for Pancreas Preservation. Ph.D. Thesis, University of Minnesota, Minneapolis, MN, USA, 2012. [Google Scholar]
- Scott, W.E.; O’Brien, T.D.; Ferrer-Fabrega, J.; Avgoustiniatos, E.S.; Weegman, B.P.; Anazawa, T.; Matsumoto, S.; Kirchner, V.A.; Rizzari, M.D.; Murtaugh, M.P.; et al. Persufflation improves pancreas preservation when compared with the two-layer method. Transplant. Proc. 2010, 42, 2016–2019. [Google Scholar] [CrossRef]
- Kelly, A.C.; Smith, K.E.; Purvis, W.G.; Min, C.G.; Weber, C.S.; Cooksey, A.M.; Hasilo, C.; Paraskevas, S.; Suszynski, T.M.; Weegman, B.P.; et al. Oxygen Perfusion (Persufflation) of Human Pancreata Enhances Insulin Secretion and Attenuates Islet Proinflammatory Signaling. Transplantation 2019, 103, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Hosgood, S.A.; Nicholson, M.L. Reducing Proinflammatory Signaling and Enhancing Insulin Secretion with the Application of Oxygen Persufflation in Human Pancreata. Transplantation 2019, 103, 13–14. [Google Scholar] [CrossRef] [PubMed]
- De Deken, J.; Kocabayoglu, P.; Moers, C. Hypothermic machine perfusion in kidney transplantation. Curr. Opin. Organ. Transplant. 2016, 21, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Quillin, R.C.; Guarrera, J.V. Hypothermic machine perfusion in liver transplantation. Liver Transplant. 2018, 24, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Organ Recovery Systems: LifePort Liver Transporter. 2021. Available online: https://www.organ-recovery.com/lifeport-liver-transporter/ (accessed on 19 July 2021).
- Organ Recovery Systems: LifePort Kidney Transporter. 2021. Available online: https://www.organ-recovery.com/lifeport-kidney-transporter/ (accessed on 19 July 2021).
- Nicholson, M.L.; Hosgood, S.A. Renal transplantation after ex vivo normothermic perfusion: The first clinical study. Am. J. Transplant. 2013, 13, 1246–1252. [Google Scholar] [CrossRef]
- Martins, P.N.; Buchwald, J.E.; Mergental, H.; Vargas, L.; Quintini, C. The role of normothermic machine perfusion in liver transplantation. Int. J. Surg. 2020, 82S, 52–60. [Google Scholar] [CrossRef]
- Nasralla, D.; Coussios, C.C.; Mergental, H.; Akhtar, M.Z.; Butler, A.J.; Ceresa, C.D.L.; Chiocchia, V.; Dutton, S.J.; García-Valdecasas, J.C.; Heaton, N.; et al. A randomized trial of normothermic preservation in liver transplantation. Nature 2018, 557, 50–56. [Google Scholar] [CrossRef]
- OrganOx metra. 2021. Available online: https://www.organox.com/metra-for-liver-transplantation (accessed on 19 July 2021).
- TransMedics OCS. 2021. Available online: https://www.transmedics.com/ocs-hcp/ (accessed on 19 July 2021).
- Boteon, Y.L.; Laing, R.W.; Schlegel, A.; Wallace, L.; Smith, A.; Attard, J.; Bhogal, R.H.; Neil, D.A.H.; Hübscher, S.; Perera, M.T.P.R.; et al. Combined Hypothermic and Normothermic Machine Perfusion Improves Functional Recovery of Extended Criteria Donor Livers. Liver Transplant. 2018, 24, 1699–1715. [Google Scholar] [CrossRef]
- Tempelman, L.A.; Stone, S.G. System for Fluid Perfusion of Biological Matter Comprising Tissue. U.S. Patent 9,357,764, 7 June 2016. [Google Scholar]
- Tempelman, L.A.; Papas, K.K.; Stone, S.G.; Scott, W.E., III; Suszynski, T.M.; Matsumoto, S.; Fabrega, J.F.; Rizzari, M.D. Perfusing an Organ with an In Situ Generated Gas. U.S. Patent 10,091,985, 9 October 2018. [Google Scholar]
- The ScubaTx System. 2021. Available online: https://www.scubatx.com/ (accessed on 14 April 2021).


{kind=link}
| Aim | Year | Author [Ref] | Technique | WIT (min) | PSF Time (h) | TPT (h) | Model |
|---|---|---|---|---|---|---|---|
| HR of DCD Livers | 2006 | Tolba [40] | R-PSF | 30 | 24 | 24 | Rat |
| HR of DCD Livers | 2008 | Treckmann [41] | R-PSF | 20–60 | 1.5–3.3 | 7–13 | Human |
| HR after long-term preservation | 2009 | Stegemann [13] | R-PSF | - | 1.5 | 23.5 | Rat |
| Protection via CO Gas | 2010 | Koetting [42] | R-PSF | 30 | 18 | 18 | Rat |
| HR of steatotic livers | 2010 | Ye [43] | R-PSF | - | 6 | 6 | Rat |
| Protection via CO Gas | 2010 | Koetting [44] | R-PSF | 30 | 18 | 18 | Rat |
| Optimal timing for HR | 2011 | Koetting [45] | R-PSF | - | 1, 2, 3 | 19–21 | Pig |
| HR and Survival rates | 2011 | Minor [46] | R-PSF | - | 2 | 12 | Pig |
| Oxygen PSF as Adjunct in Liver preservation trial | 2011 | Minor [47] | R-PSF | - | 2 | - | Human |
| HR: Before or after CS for DCD livers | 2011 | Koetting [48] | R-PSF | 30 | 2–20 | 20 | Rat |
| Protection via NO Gas | 2012 | Srinivasan [49] | R-PSF | 30 | 24 | 24 | Rat |
| HR with A-PSF | 2012 | Minor [50] | A-PSF | - | 2 | 20 | Pig |
| Protection via NO Gas | 2013 | Nagai [51] | R-PSF | - | 2 | 3 | Rat |
| Protection via NO Gas | 2013 | Yagi [52] | R-PSF | - | 3 | 3 | Rat |
| Pulsatile Pressure | 2014 | Lüer [53] | R-PSF | 30 | 18 | 18 | Rat |
| Protection via NO Gas | 2014 | Kageyama [54] | R-PSF | 30–60 | 3 | 3 | Rat |
| HR of DCD Livers | 2014 | Khorsandi [55] | A-PSF | 15–25 | 2 | 15 | Human |
| Protection via NO Gas | 2016 | Porschen [56] | R-PSF | 30 | 1 | 24 | Pig |
| HR of hypovolemic shocked livers | 2018 | Jafari [57] | R-PSF | - | 1 | 18 | Rat |
| Oxygen PSF as Adjunct in Liver preservation trial | 2019 | Gallinat [58] | R-PSF | - | 2 | 11–20 | Human |
| A-PSF O concentration | 2020 | Minor [59] | A-PSF | - | 2 | 18 | Pig |
| Aim | Year | Author [Ref] | Technique | WIT (min) | PSF Time (h) | TPT (h) | Model |
|---|---|---|---|---|---|---|---|
| HR of DCD kidneys | 2006 | Treckmann [39] | R-PSF | 60,90,120 | 4 | 4 | Pig |
| HR of DCD kidneys | 2009 | Treckmann [18] | R-PSF | 60 | 4 | 4 | Pig |
| HR after long-term preservation | 2012 | Minor [64] | R-PSF | - | 2 | 20 | Pig |
| HR of DCD kidneys | 2016 | Moláček [65] | R-PSF | 20 | 2 | 2 | Pig |
| HR of DCD kidneys and comparison of methods | 2016 | Kalenski [63] | R-PSF | 45 | 24 | 24 | Pig |
| HR of DCD kidneys and comparison of methods | 2018 | Moláček [66] | R-PSF | 20 | 1 | 1 | Pig |
| HR of DCD kidneys and comparison of methods | 2018 | Min [67] | A-PSF | 30 | 24 | 24 | Pig |
| Aim | Year | Author [Ref] | Technique | WIT (min) | PSF Time (h) | TPT (h) | Model |
|---|---|---|---|---|---|---|---|
| Comparison to TLM | 2010 | Scott [71] | A-PSF | - | 24 | 24 | Pig |
| Oxygen Delivery to DCD pancreas | 2010 | Scott [17] | A-PSF | - | - | - | Pig/Human |
| Comparison to TLM | 2012 | Scott [70] | A-PSF | - | - | - | Pig/Human |
| HR of DCD pancreas and comparison of methods | 2014 | Reddy [68] | R-PSF | 30 | 6 | 6 | Rat |
| HR of DCD Human pancreas | 2019 | Kelly [72] | A-PSF | - | 5 | 15 | Human |
| Commentary on previous works | 2019 | Hosgood [73] | A-PSF | - | - | - | Human |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buhagiar, A.J.; Freitas, L.; Scott, W.E., III. Persufflation—Current State of Play. Transplantology 2021, 2, 362-378. https://doi.org/10.3390/transplantology2030035
Buhagiar AJ, Freitas L, Scott WE III. Persufflation—Current State of Play. Transplantology. 2021; 2(3):362-378. https://doi.org/10.3390/transplantology2030035
Chicago/Turabian StyleBuhagiar, Aaron John, Leo Freitas, and William E. Scott, III. 2021. "Persufflation—Current State of Play" Transplantology 2, no. 3: 362-378. https://doi.org/10.3390/transplantology2030035
APA StyleBuhagiar, A. J., Freitas, L., & Scott, W. E., III. (2021). Persufflation—Current State of Play. Transplantology, 2(3), 362-378. https://doi.org/10.3390/transplantology2030035