
The Impact of Body Mass Index in Patients with Severe Burn Injury

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
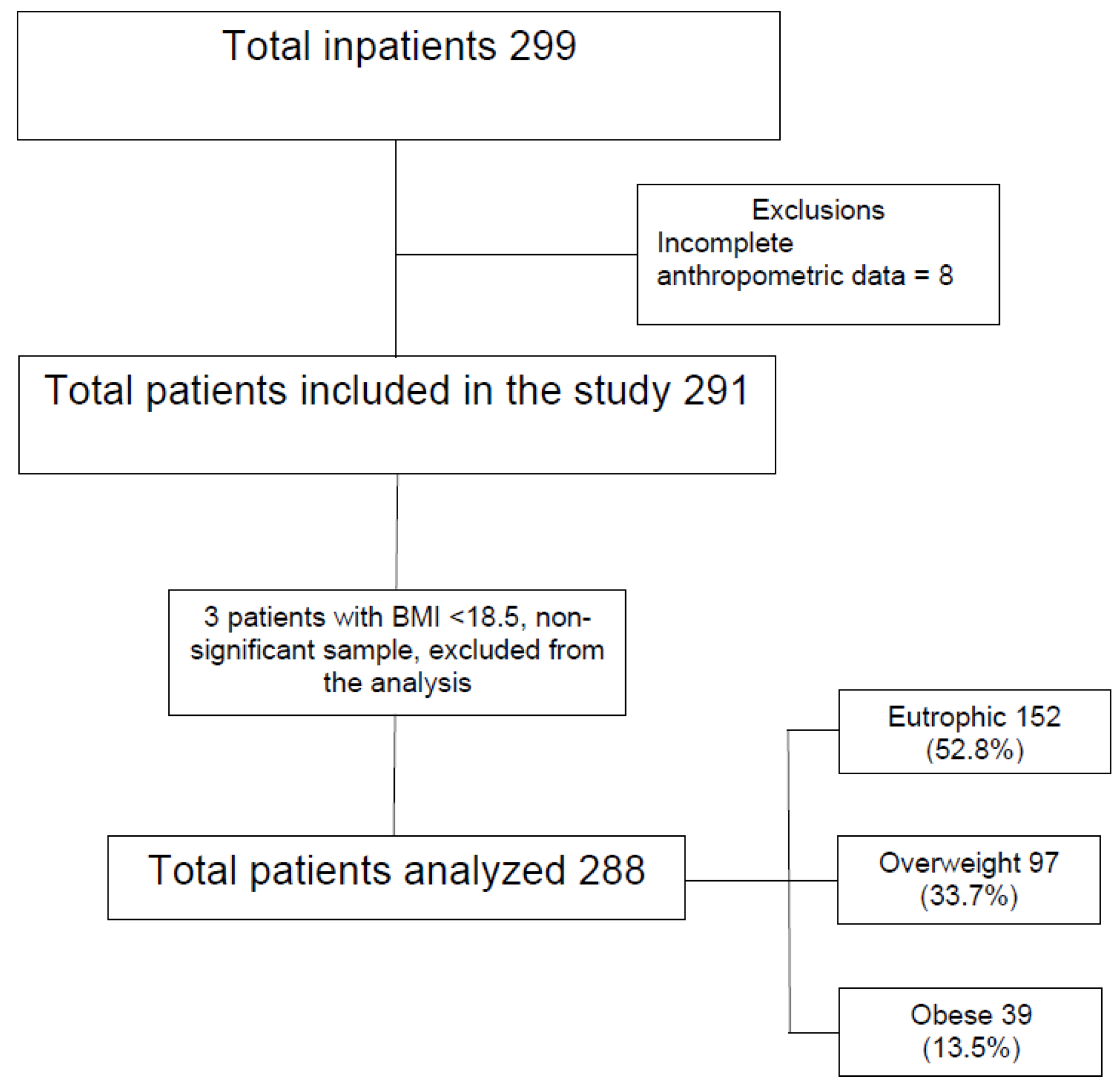
2.1. Study Design and Patients
2.2. Measurements
2.3. Ethics
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ogden, C.L.; Carrol, M.D.; Kite, B.K.; Flegal, K.M. Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA 2014, 311, 806–814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic; Report of a WHO Consultation; WHO: Geneva, Switzerland, 2000; Volume 894, pp. 1–253. [Google Scholar]
- Ministry of Health; Department of Health Surveillance; Department of Health Analysis and Surveillance of Non-Communicable Diseases. Vigitel Brasil. 2018. Available online: http://bvsms.saude.gov.br/bvs/publicacoes/vigitel_brasil_2018_vigilancia_fatores_risco.pdf (accessed on 23 December 2020).
- World Health Organization. Data Repository of the Global Health Observatory. Available online: https://apps.who.int/gho/data/node.imr (accessed on 23 December 2020).
- Calle, E.E.; Thun, M.J.; Petrelli, J.M.; Rodriguez, C.; Heath, C.W. Body-mass index and mortality in a prospective cohort of U.S. adults. N. Engl. J. Med. 1999, 341, 1097–1105. [Google Scholar] [CrossRef] [PubMed]
- Peeters, A.; Barendregt, J.J.; Willekens, F.; Mackenbach, J.P.; Al Mamun, A.; Bonneux, L. NEDCOM, the Netherlands Epidemiology and Demography Compression of Morbidity Research Group. Obesity in adulthood and its consequences for life expectancy: A life-table analysis. Ann. Intern. Med. 2003, 138, 24–32. [Google Scholar] [CrossRef] [PubMed]
- U.S. Preventive Services Task Force. Screening for Obesidy in adults recommendations and rationale. Ann. Intern. Med. 2003, 139, 930–932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nasraway, S.A., Jr.; Albert, M.; Donnelly, A.M.; Ruthazer, R.; Shikora, S.A.; Saltzman, E. Morbid obesity in an independent determinant of death among surgical critical ill patients. Crit. Care Med. 2006, 34, 964–970. [Google Scholar] [CrossRef] [PubMed]
- Akinnusi, M.E.; Pineda, L.A.; El Solh, A.A. Effect of obesity on intensive care morbidity and mortality: A meta-analysis. Crit Care Med. 2008, 36, 151–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliveros, H.; Villamor, E. Obesity and mortality in critically ill adults: A systematic review and meta-analysis. Obesity 2008, 16, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Hogue, C.W., Jr.; Stearns, J.D.; Colantuoni, E.; Robinson, K.A.; Stiereer, T.; Mitter, N.; Pronovost, P.J.; Needham, D.M. The impact of obesity on outcomes after critical illlnesss: A meta-analysis. Intensive Care Med. 2009, 35, 1152–1170. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, E.; Teal, N.; Dudley, J.; May, W.; Bower, J.D.; Salahudeen, A.K. Influence of excess weight on mortality and hospital stay in 1346 hemodialysis patients. Kidney Int. 1999, 55, 1560–1567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, A.T.; Tsai, C.L.; Hwang, L.Y.; Lai, D.; Markham, C.; Patel, B. Obesity and mortality, length of stay and hospital cost among patients with sepsis: A nationwide inpatient retrospective cohort study. PLoS ONE 2016, 11, e0154599. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Liu, X.; Chen, Q.; Liu, C.; Huang, C.; Fang, X. The role of increased body mass index in outcomes of sepsis: A systematic review and meta-analysis. BMC Anesthesiol. 2017, 17, 118. [Google Scholar] [CrossRef] [PubMed]
- Zhi, G.; Xin, W.; Ying, W.; Guohong, X.; Shuying, L. “Obesity Paradox” in Acute Respiratory Distress Syndrome: Asystematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0163677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ni, Y.N.; Luo, J.; Yu, H.; Wang, Y.W.; Hu, Y.H.; Liu, D.; Liang, B.M.; Liang, Z.A. Can body mass index predict clinical outcomes for patients with acute lung injury/acute respiratory distress syndrome? A meta-analysis. Crit. Care 2017, 21, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutagalung, R.; Marques, J.; Kobylka, K.; Zeidan, M.; Kabisch, B.; Brunkhorst, F.; Reinhart, K.; Sakr, Y. The obesity paradox in surgical intensive care unit patients. Intensive Care Med. 2011, 37, 1793–1799. [Google Scholar] [CrossRef] [PubMed]
- Rios-Diaz, A.J.; Lin, E.; Williams, K.; Jiang, W.; Patel, V.; Shimizu, N.; Metcalfe, D.; Olufajo, O.A.; Cooper, Z.; Havens, J.; et al. The obesity paradox in patients with severe soft tissue infections. Am. J. Surg. 2017, 214, 385–398. [Google Scholar] [CrossRef] [PubMed]
- Lester, E.L.; Dvorak, J.E.; Maluso, P.J.; Bendjemil, S.; Messer, T.; Poulakidas, S.; Bokhari, F. Obesity Paradox in the Burn Patient. J. Burn Care Res. 2020, 41, 30–32. [Google Scholar] [CrossRef]
- Saadat, G.H.; Toor, R.; Mazhar, F.; Bajani, F.; Tatebe, L.; Schlanser, V.; Kaminsky, M.; Messer, T.; Starr, F.; Dennis, A.; et al. Severe burn injury: Body mass index and the Baux score. Burns 2021, 47, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Tobiasen, J.; Hiebert, J.M.; Edlich, R.F. The abbreviated burn severity index. Ann. Emerg. Med. 1982, 11, 260–262. [Google Scholar] [CrossRef]
- Tanita, M.T.; Capeletti, M.M.; Moreira, T.A.; Petinelli, R.P.; Cardoso, L.T.; Grion, C.M. Risk Factors for acute respiratory distress syndrome in severe burns: Prospective cohort study. Int. J. Burn Trauma 2020, 10, 1–14. [Google Scholar]

{kind=link}
| BMI 18.5–24.9 | BMI 25.0–29.9 | BMI ≥30.0 | p-Value | |
|---|---|---|---|---|
| Age: median (q1–q2) | 36.3 (24.9–55.4) | 42.7 (30.8–52.9) | 43.9 (32.8–59.7) | 0.091 |
| Male sex % | 102 (67%) | 65 (67%) | 26 (66.7%) | 0.999 |
| TBSA: median (q1–q2) | 20.0 (12.6–29.8) | 25.0 (14.0–37.5) | 23.5 (10.0–32.0) | 0.243 |
| Inhalation injury | 27 (17.8%) | 23 (23.7%) | 8 (20.5%) | 0.520 |
| ABSI: median (q1–q2) | 6.0 (5.0–7.0) | 7.0 (5.0–8.0) | 6.0 (5.0–7.0) | 0.218 |
| Hypertension | 13 (8.6%) | 13 (13.4%) | 12 (30.8%) | 0.001 |
| Diabetes | 3 (2%) | 8 (8.2%) | 4 (10.3%) | 0.029 |
| Smoking | 18 (11.8%) | 16 (16.5%) | 7 (17.9%) | 0.459 |
| Alcoholism and/or Drug addiction | 25 (16.4%) | 12 (12.4%) | 3 (7.7%) | 0.321 |
| Body Mass Index Categories | |||||
|---|---|---|---|---|---|
| All Patients | BMI 18.5–24.9 | BMI 25.0–29.9 | BMI ≥ 30.0 | p-Value | |
| Length of ICU stay (days): median (ITQ) | 11.0 (5.0–19.0) | 9.0 (4.0–16.8) | 13.0 (5.5–20.0) | 16.0 (7.0–29.0) | p = 0.004 * |
| Length of hospital stay (days): median (ITQ) | 19.0 (11.0–32.0) | 18.0 (10.0–29.0) | 21.0 (13.0–30.0) | 22.0 (12.0–39.0) | p = 0.176 * |
| Mortality | 96 (33.3%) | 46 (30.3%) | 36 (37.1%) | 14 (35.9%) | p = 0.501 ** |
| Variables | Hazard Ratio | 95%CI | p-Value |
|---|---|---|---|
| Body Mass Index | |||
| Overweight | 0.753 | 0.478–1.188 | 0.223 |
| Obesity | 0.648 | 0.350–1.201 | 0.168 |
| Age | 1.026 | 1.014–1.038 | <0.001 |
| Males | 1.239 | 0.793–1.935 | 0.346 |
| Total body surface area | 1.047 | 1.036–1.058 | <0.001 |
| Inhalation injury | 1.658 | 1.061–2.590 | 0.026 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Walger, A.C.V.; Cardoso, L.T.Q.; Tanita, M.T.; Matsuo, T.; Carrilho, A.J.F.; Grion, C.M.C. The Impact of Body Mass Index in Patients with Severe Burn Injury. Eur. Burn J. 2022, 3, 425-431. https://doi.org/10.3390/ebj3030037
Walger ACV, Cardoso LTQ, Tanita MT, Matsuo T, Carrilho AJF, Grion CMC. The Impact of Body Mass Index in Patients with Severe Burn Injury. European Burn Journal. 2022; 3(3):425-431. https://doi.org/10.3390/ebj3030037
Chicago/Turabian StyleWalger, Aline C. V., Lucienne T. Q. Cardoso, Marcos T. Tanita, Tiemi Matsuo, Alexandre J. F. Carrilho, and Cintia M. C. Grion. 2022. "The Impact of Body Mass Index in Patients with Severe Burn Injury" European Burn Journal 3, no. 3: 425-431. https://doi.org/10.3390/ebj3030037
APA StyleWalger, A. C. V., Cardoso, L. T. Q., Tanita, M. T., Matsuo, T., Carrilho, A. J. F., & Grion, C. M. C. (2022). The Impact of Body Mass Index in Patients with Severe Burn Injury. European Burn Journal, 3(3), 425-431. https://doi.org/10.3390/ebj3030037