


Patient-Specific Instrumentation with Laser-Guide-Navigated THA: Clinical and CT Evaluation of the First 100 Cases

 and
and
Abstract
:1. Introduction
2. Materials and Methods
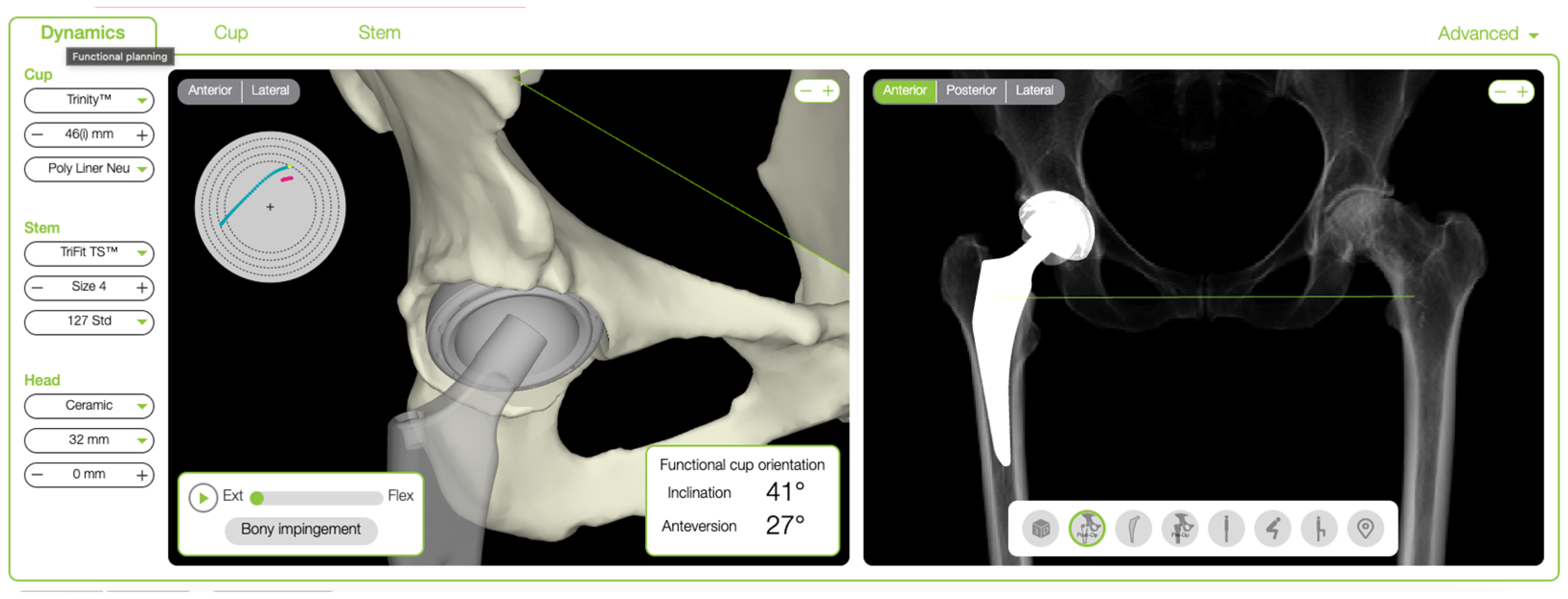
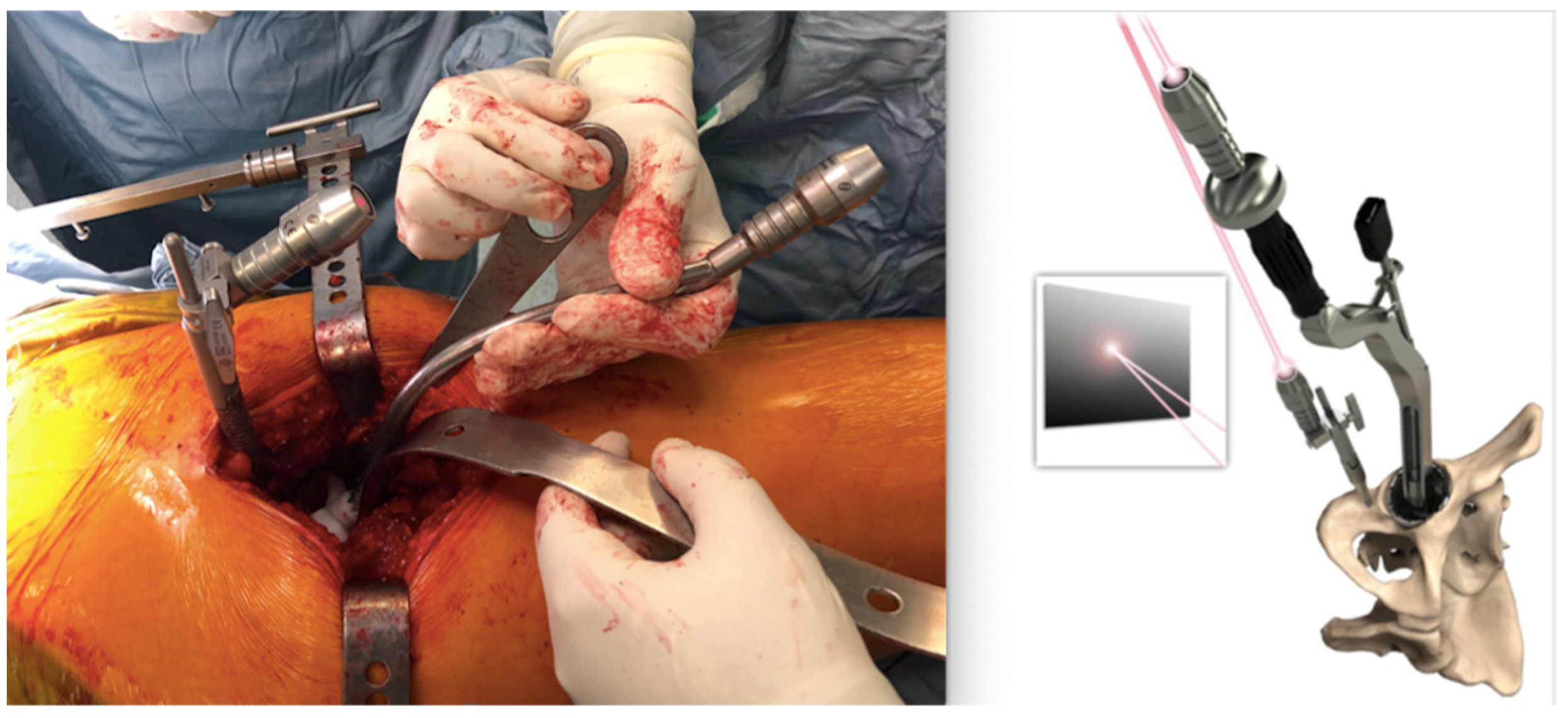
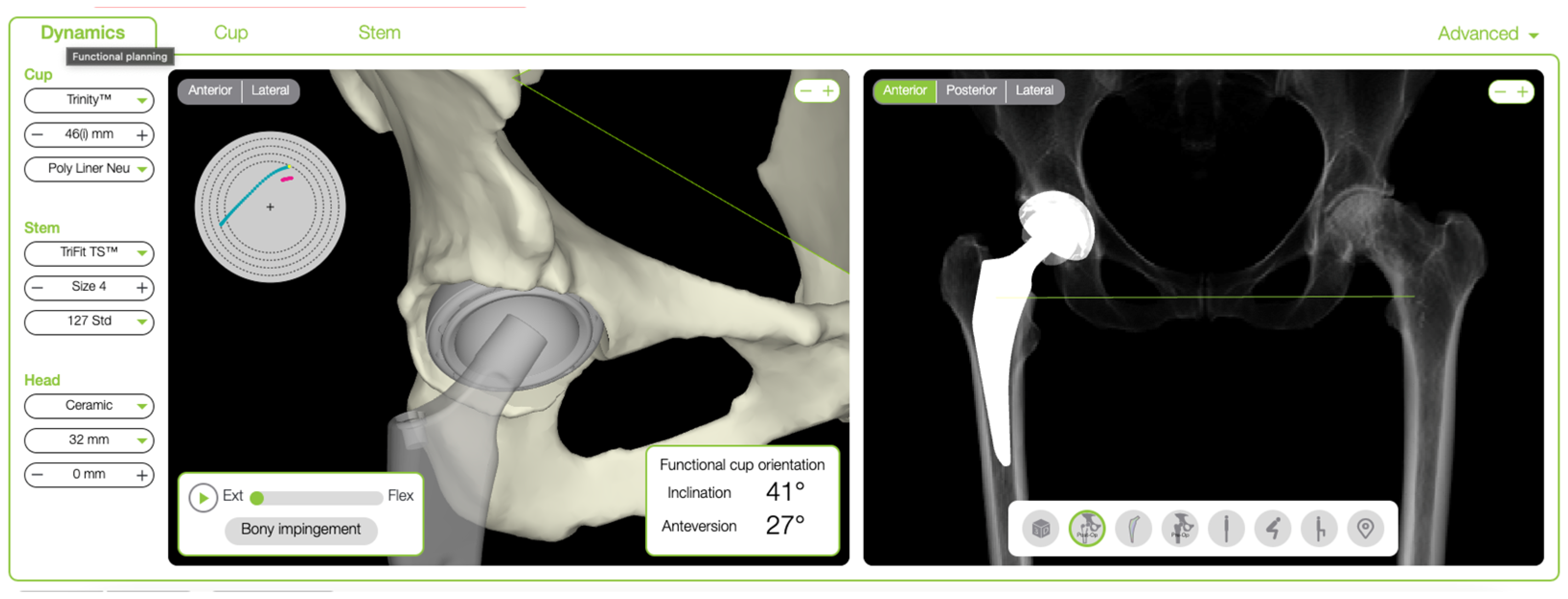
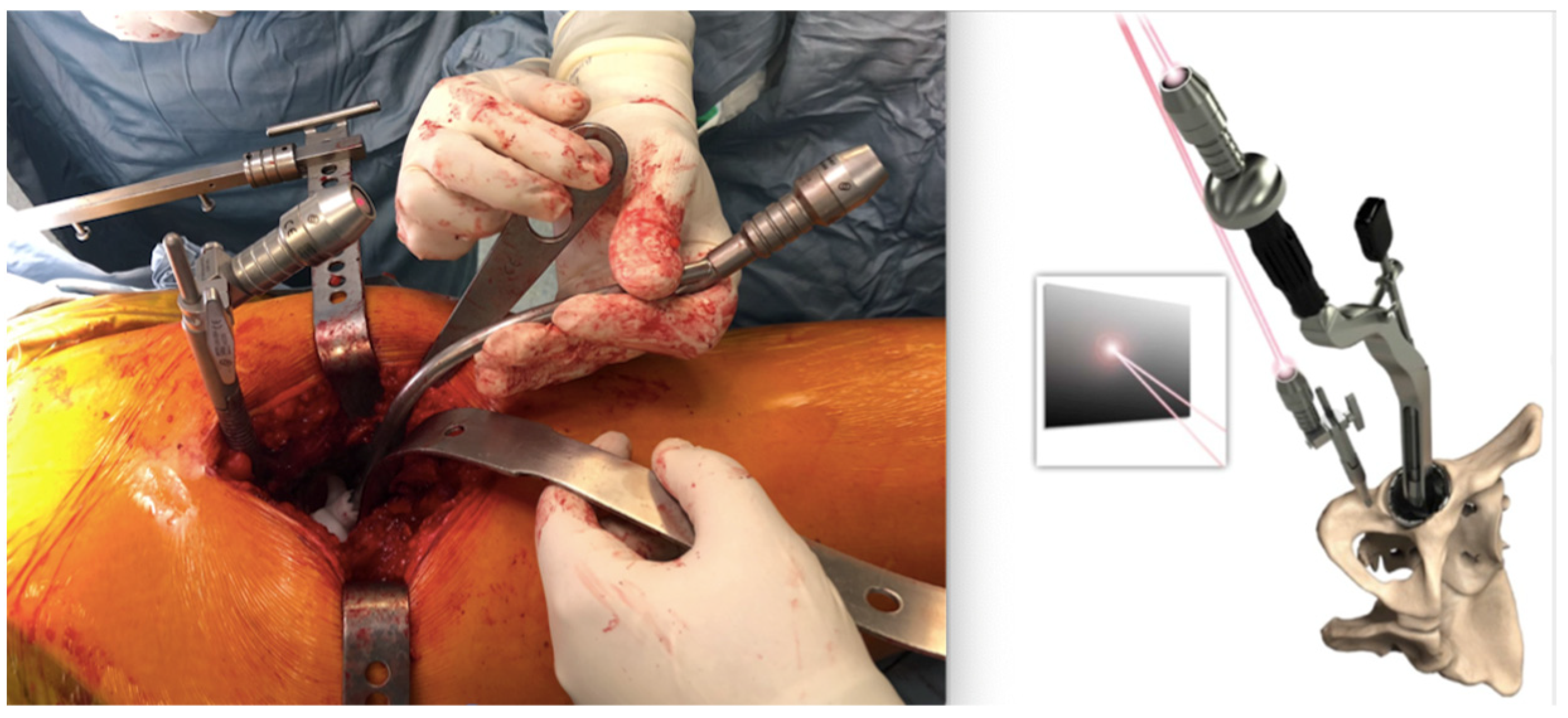
2.1. Surgical Technique
2.2. Postoperative CT Evaluation
2.3. Clinical Outcomes Measures
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Innmann, M.M.; Maier, M.W.; Streit, M.R.; Grammatopoulos, G.; Bruckner, T.; Gotterbarm, T.; Merle, C. Additive Influence of Hip Offset and Leg Length Reconstruction on Postoperative Improvement in Clinical Outcome After Total Hip Arthroplasty. J. Arthroplast. 2018, 33, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Soong, M.; Rubash, H.E.; Macaulay, W. Dislocation After Total Hip Arthroplasty. J. Am. Acad. Orthop. Surg. 2004, 12, 314–321. [Google Scholar] [CrossRef] [PubMed]
- Miki, H.; Kyo, T.; Kuroda, Y.; Nakahara, I.; Sugano, N. Risk of edge-loading and prosthesis impingement due to posterior pelvic tilting after total hip arthroplasty. Clin. Biomech. 2014, 29, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Biedermann, R.; Tonin, A.; Krismer, M.; Rachbauer, F.; Eibl, G.; Stöckl, B. Reducing the risk of dislocation after total hip arthroplasty. J. Bone Jt. Surg. 2005, 87, 762–769. [Google Scholar] [CrossRef] [PubMed]
- Widmer, K.H. The Impingement-free, Prosthesis-specific, and Anatomy-adjusted Combined Target Zone for Component Posi-tioning in THA Depends on Design and Implantation Parameters of both Components. Clin. Orthop. Relat. Res. 2020, 478, 1904–1918. [Google Scholar] [CrossRef]
- Lewinnek, E.G.; Lewis, J.L.; Tarr, R.; Compere, C.L.; Zimmerman, J.R. Dislocations after total hip-replacement arthroplasties. Minerva Anestesiol. 1978, 60, 217–220. [Google Scholar] [CrossRef]
- Abdel, M.P.; von Roth, P.; Jennings, M.T.; Hanssen, A.D.; Pagnano, M.W. What Safe Zone? The Vast Majority of Dislocated THAs Are Within the Lewinnek Safe Zone for Acetabular Component Position. Clin. Orthop. Relat. Res. 2015, 474, 386–391. [Google Scholar] [CrossRef]
- Reize, P.; Geiger, E.V.; Suckel, A.; Rudert, M.; Wülker, N. Influence of surgical experience on accuracy of acetabular cup positioning in total hip arthroplasty. Am. J. Orthop. 2008, 37, 360–363. [Google Scholar]
- Esposito, C.I.; Gladnick, B.P.; Lee, Y.-Y.; Lyman, S.; Wright, T.M.; Mayman, D.J.; Padgett, D.E. Cup Position Alone Does Not Predict Risk of Dislocation After Hip Arthroplasty. J. Arthroplast. 2014, 30, 109–113. [Google Scholar] [CrossRef]
- McLawhorn, A.S.; Sculco, P.K.; Weeks, K.D.; Nam, D.; Mayman, D.J. Targeting a New Safe Zone: A Step in the Development of Patient-Specific Component Positioning for Total Hip Arthroplasty. Am. J. Orthop. 2015, 44, 270–276. [Google Scholar]
- Pierrepont, J.; Hawdon, G.; Miles, B.P.; Connor, B.O.; Baré, J.; Walter, L.R.; Marel, E.; Solomon, M.; McMahon, S.; Shimmin, A.J. Variation in functional pelvic tilt in patients undergoing total hip arthroplasty. Bone Jt. J. 2017, 99, 184–191. [Google Scholar] [CrossRef]
- Kanawade, V.; Dorr, L.D.; Wan, Z. Predictability of Acetabular Component Angular Change with Postural Shift from Standing to Sitting Position. J. Bone Jt. Surg. 2014, 96, 978–986. [Google Scholar] [CrossRef]
- DiGioia, A.M.I.; Hafez, A.M.; Jaramaz, B.; Levison, T.J.; Moody, E.J. Functional Pelvic Orientation Measured from Lateral Standing and Sitting Radiographs. Clin. Orthop. Relat. Res. 2006, 453, 272–276. [Google Scholar] [CrossRef]
- Yang, G.; Li, Y.; Zhang, H. The Influence of Pelvic Tilt on the Anteversion Angle of the Acetabular Prosthesis. Orthop. Surg. 2019, 11, 762–769. [Google Scholar] [CrossRef] [PubMed]
- Eftekhary, N.; Shimmin, A.; Lazennec, J.Y.; Buckland, A.; Schwarzkopf, R.; Dorr, L.D.; Mayman, D.; Padgett, D.; Vigdorchik, J. A systematic approach to the hip-spine relationship and its applications to total hip arthroplasty. Bone Jt. J. 2019, 101-B, 808–816. [Google Scholar] [CrossRef] [PubMed]
- Buckland, A.J.; Puvanesarajah, V.; Vigdorchik, J.; Schwarzkopf, R.; Jain, A.; Klineberg, E.O.; Hart, R.A.; Callaghan, J.J.; Hassanzadeh, H. Dislocation of a primary total hip arthroplasty is more common in patients with a lumbar spinal fusion. Bone Jt. J. 2017, 99-B, 585–591. [Google Scholar] [CrossRef]
- DelSole, E.M.; Vigdorchik, J.M.; Schwarzkopf, R.; Errico, T.J.; Buckland, A.J. Total Hip Arthroplasty in the Spinal Deformity Population: Does Degree of Sagittal Deformity Affect Rates of Safe Zone Placement, Instability, or Revision? J. Arthroplast. 2017, 32, 1910–1917. [Google Scholar] [CrossRef]
- Langston, J.; Pierrepont, J.; Gu, Y.; Shimmin, A. Risk factors for increased sagittal pelvic motion causing unfavourable orientation of the acetabular component in patients undergoing total hip arthroplasty. Bone Jt. J. 2018, 100-B, 845–852. [Google Scholar] [CrossRef] [PubMed]
- Spencer-Gardner, L.; Pierrepont, J.; Topham, M.; Baré, J.; McMahon, S.; Shimmin, A.J. Patient-specific instrumentation improves the accuracy of acetabular component placement in total hip arthroplasty. Bone Jt. J. 2016, 98-B, 1342–1346. [Google Scholar] [CrossRef]
- Snijders, E.T.; Willemsen, K.; van Gaalen, S.M.; Castelein, R.M.; Weinans, H.; de Gast, A. Lack of consensus on optimal acetabular cup orientation because of variation in assessment methods in total hip arthroplasty: A systematic review. HIP Int. 2018, 29, 41–50. [Google Scholar] [CrossRef]
- Dimitriou, D.; Tsai, T.-Y.; Kwon, Y.-M. The effect of femoral neck osteotomy on femoral component position of a primary cementless total hip arthroplasty. Int. Orthop. 2015, 39, 2315–2321. [Google Scholar] [CrossRef]
- Belzunce, M.A.; Henckel, J.; Di Laura, A.; Hart, A. Uncemented femoral stem orientation and position in total hip arthroplasty: A CT study. J. Orthop. Res. 2020, 38, 1486–1496. [Google Scholar] [CrossRef] [PubMed]
- Knight, J.L.; Atwater, R.D. Preoperative planning for total hip arthroplasty. J. Arthroplast. 1992, 7, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Saxler, G.; Marx, A.; Vandevelde, D.; Langlotz, U.; Tannast, M.; Wiese, M.; Michaelis, U.; Kemper, G.; Grützner, P.A.; Steffen, R.; et al. The accuracy of free-hand cup positioning–A CT based measurement of cup placement in 105 total hip arthroplasties. Int. Orthop. 2004, 28, 198–201. [Google Scholar] [CrossRef] [PubMed]
- DiGioia, A.M.; Jaramaz, B.; Plakseychuk, A.Y.; Moody, J.E.; Nikou, C.; LaBarca, R.S.; Levison, T.J.; Picard, F. Comparison of a mechanical acetabular alignment guide with computer placement of the socket. J. Arthroplast. 2002, 17, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Behrend, H.; Giesinger, K.; Giesinger, J.M.; Kuster, M.S. The “forgotten joint” as the ultimate goal in joint arthroplasty. J. Arthroplast. 2012, 27, 430–436.e1. [Google Scholar] [CrossRef]
- Bellamy, N.; Buchanan, W.W.; Goldsmith, C.H.; Campbell, J.; Stitt, L.W. Validation study of WOMAC: A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J. Rheumatol. 1988, 15, 1833–1840. [Google Scholar]
- Schloemann, D.T.; Edelstein, A.I.; Barrack, R.L. Changes in acetabular orientation during total hip arthroplasty. Bone Jt. J. 2019, 101-B, 45–50. [Google Scholar] [CrossRef]
- Lembeck, B.; Mueller, O.; Reize, P.; Wuelker, N. Pelvic tilt makes acetabular cup navigation inaccurate. Acta Orthop. 2005, 76, 517–523. [Google Scholar] [CrossRef]
- Attenello, J.D.; Harpstrite, J.K. Implications of Spinopelvic Mobility on Total Hip Arthroplasty: Review of Current Literature. Hawai’i J. Health Soc. Welf. 2019, 78, 31–40. [Google Scholar]
- Kanto, M.; Maruo, K.; Tachibana, T.; Fukunishi, S.; Nishio, S.; Takeda, Y.; Arizumi, F.; Kusuyama, K.; Kishima, K.; Yoshiya, S. Influence of Spinopelvic Alignment on Pelvic Tilt after Total Hip Arthroplasty. Orthop. Surg. 2019, 11, 438–442. [Google Scholar] [CrossRef] [PubMed]
- Phan, D.; Bederman, S.S.; Schwarzkopf, R. The influence of sagittal spinal deformity on anteversion of the acetabular component in total hip arthroplasty. Bone Jt. J. 2015, 97-B, 1017–1023. [Google Scholar] [CrossRef]
- Gorin, M.; Roger, B.; Lazennec, J.-Y.; Charlot, N.; Arafati, N.; Bissery, A.; Saillant, G. Hip-spine relationship: A radio-anatomical study for optimization in acetabular cup positioning. Surg. Radiol. Anat. 2004, 26, 136–144. [Google Scholar] [CrossRef] [PubMed]
- Rivière, C.; Lazic, S.; Villet, L.; Wiart, Y.; Allwood, S.M.; Cobb, J. Kinematic alignment technique for total hip and knee arthroplasty. EFORT Open Rev. 2018, 3, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Maillot, C.; Harman, C.; Villet, L.; Cobb, J.; Rivière, C. Modern cup alignment techniques in total hip arthroplasty: A systematic review. Orthop. Traumatol. Surg. Res. 2019, 105, 907–913. [Google Scholar] [CrossRef] [PubMed]
- Pongkunakorn, A.; Diewwattanawiwat, K.; Chatmaitri, S. Smartphone-assisted technique in total hip arthroplasty can improve the precision of acetabular cup placement: A randomised controlled trial. HIP Int. 2019, 31, 50–57. [Google Scholar] [CrossRef]
- Beckmann, J.; Stengel, D.; Tingart, M.; Götz, J.; Grifka, J.; Lüring, C. Navigated cup implantation in hip arthroplasty. Acta Orthop. 2009, 80, 538–544. [Google Scholar] [CrossRef]
- Kayani, B.; Konan, S.; Ayuob, A.; Ayyad, S.; Haddad, F.S. The current role of robotics in total hip arthroplasty. EFORT Open Rev. 2019, 4, 618–625. [Google Scholar] [CrossRef]
- Henckel, J.; Holme, T.J.; Radford, W.; Skinner, J.A.; Hart, A.J. 3D-printed Patient-specific Guides for Hip Arthroplasty. J. Am. Acad. Orthop. Surg. 2018, 26, e342–e348. [Google Scholar] [CrossRef]
- Small, T.; Krebs, V.; Molloy, R.; Bryan, J.; Klika, A.K.; Barsoum, W.K. Comparison of acetabular shell position using patient specific instruments vs. standard surgical instruments: A randomized clinical trial. J. Arthroplast. 2014, 29, 1030–1037. [Google Scholar] [CrossRef]
- Pierrepont, J.W.; Stambouzou, C.Z.; Miles, B.P.; O’Connor, P.B.; Walter, L.; Ellis, A.; Molnar, R.; Baré, J.V.; Solomon, M.; McMahon, S.; et al. Patient Specific Component Alignment in Total Hip Arthroplasty. Reconstr. Rev. 2016, 6, 27–33. [Google Scholar] [CrossRef]
- Solarino, G.; Zagra, L.; Piazzolla, A.; Morizio, A.; Vicenti, G.; Moretti, B. Results of 200 Consecutive Ceramic-on-Ceramic Cementless Hip Arthroplasties in Patients Up To 50 Years of Age: A 5-24 Years of Follow-Up Study. J. Arthroplast. 2019, 34, S232–S237. [Google Scholar] [CrossRef] [PubMed]
- Zagra, L.; Benazzo, F.; Dallari, D.; Falez, F.; Solarino, G.; D’apolito, R.; Castelli, C.C. Current concepts in hip–spine relationships: Making them practical for total hip arthroplasty. EFORT Open Rev. 2022, 7, 59–69. [Google Scholar] [CrossRef] [PubMed]
- Jasty, M.; Webster, W.; Harris, W. Management of limb length inequality during total hip replacement. Clin. Orthop. Relat. Res. 1996, 333, 165–171. [Google Scholar] [CrossRef]
- Schneider, A.K.; Pierrepont, J.W.; Hawdon, G.; McMahon, S. Clinical accuracy of a patient-specific femoral osteotomy guide in minimally-invasive posterior hip arthroplasty. HIP Int. 2018, 28, 636–641. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean Planned Value (Range) | Mean Postoperative Value (Range) | p-Value | |
|---|---|---|---|
| Cup Inclination | 39.4° (32°–45°) | 37.2° (30°–45°) | 0.345 |
| Cup Anteversion | 20.8° (12°–28°) | 18.8° (12°–30°) | 0.093 |
| Osteotomy Hight | 10.26 mm (5–24 mm) | 10 mm (4–28 mm) | 0.234 |
| Offsett Change | 1 mm (0–5 mm) | 3 mm (1–8 mm) | 0.134 |
| Length Change | 2.5 mm (1–3 mm) | 3.1 mm (2–5 mm) | 0.098 |
| Absolute Deviation, Mean | % Within ±5° (n) | % Within ±10° (n) | |
|---|---|---|---|
| Cup Inclination | 4.3° | 78 | 98 |
| Cup Anteversion | 3.8° | 81 | 97 |
| Absolute Deviation, Mean (Range) | % Within ±2 mm (n) | % Within ±4 mm (n) | |
|---|---|---|---|
| Osteotomy Height | 1.6 mm (0–4 mm) | 75 | 100 |
| Offset Change | 2.3 mm (1–4 mm). | 78 | 100 |
| Length Change | 1.9 mm (1–6 mm). | 68 | 80 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Previ, L.; Viglietta, E.; Giuliani, V.; Corsetti, F.; Redler, A.; Speranza, A.; De Carli, A.; Iorio, R. Patient-Specific Instrumentation with Laser-Guide-Navigated THA: Clinical and CT Evaluation of the First 100 Cases. Prosthesis 2023, 5, 1111-1119. https://doi.org/10.3390/prosthesis5040077
Previ L, Viglietta E, Giuliani V, Corsetti F, Redler A, Speranza A, De Carli A, Iorio R. Patient-Specific Instrumentation with Laser-Guide-Navigated THA: Clinical and CT Evaluation of the First 100 Cases. Prosthesis. 2023; 5(4):1111-1119. https://doi.org/10.3390/prosthesis5040077
Chicago/Turabian StylePrevi, Leonardo, Edoardo Viglietta, Veronica Giuliani, Federico Corsetti, Andrea Redler, Attilio Speranza, Angelo De Carli, and Raffaele Iorio. 2023. "Patient-Specific Instrumentation with Laser-Guide-Navigated THA: Clinical and CT Evaluation of the First 100 Cases" Prosthesis 5, no. 4: 1111-1119. https://doi.org/10.3390/prosthesis5040077
APA StylePrevi, L., Viglietta, E., Giuliani, V., Corsetti, F., Redler, A., Speranza, A., De Carli, A., & Iorio, R. (2023). Patient-Specific Instrumentation with Laser-Guide-Navigated THA: Clinical and CT Evaluation of the First 100 Cases. Prosthesis, 5(4), 1111-1119. https://doi.org/10.3390/prosthesis5040077