


Effectiveness of Adjunctive Hyaluronic Acid Application in Surgical Treatment of Gingival Recession Sites

 ,
, 
 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Registration
2.2. Focused Question
2.3. Sources of Evidence
2.4. Search Strategies
2.5. Eligibility Criteria
2.5.1. Inclusion Criteria
2.5.2. Exclusion Criteria
- in vitro and in vivo animal studies;
- articles written in a language other than English;
- case series, case reports and literature reviews;
- studies that did not report the surgical treatment of gingival recessions in combination with HA;
- studies that performed periodontal regeneration in conjunction with HA.
2.5.3. Selection of Sources of Evidence
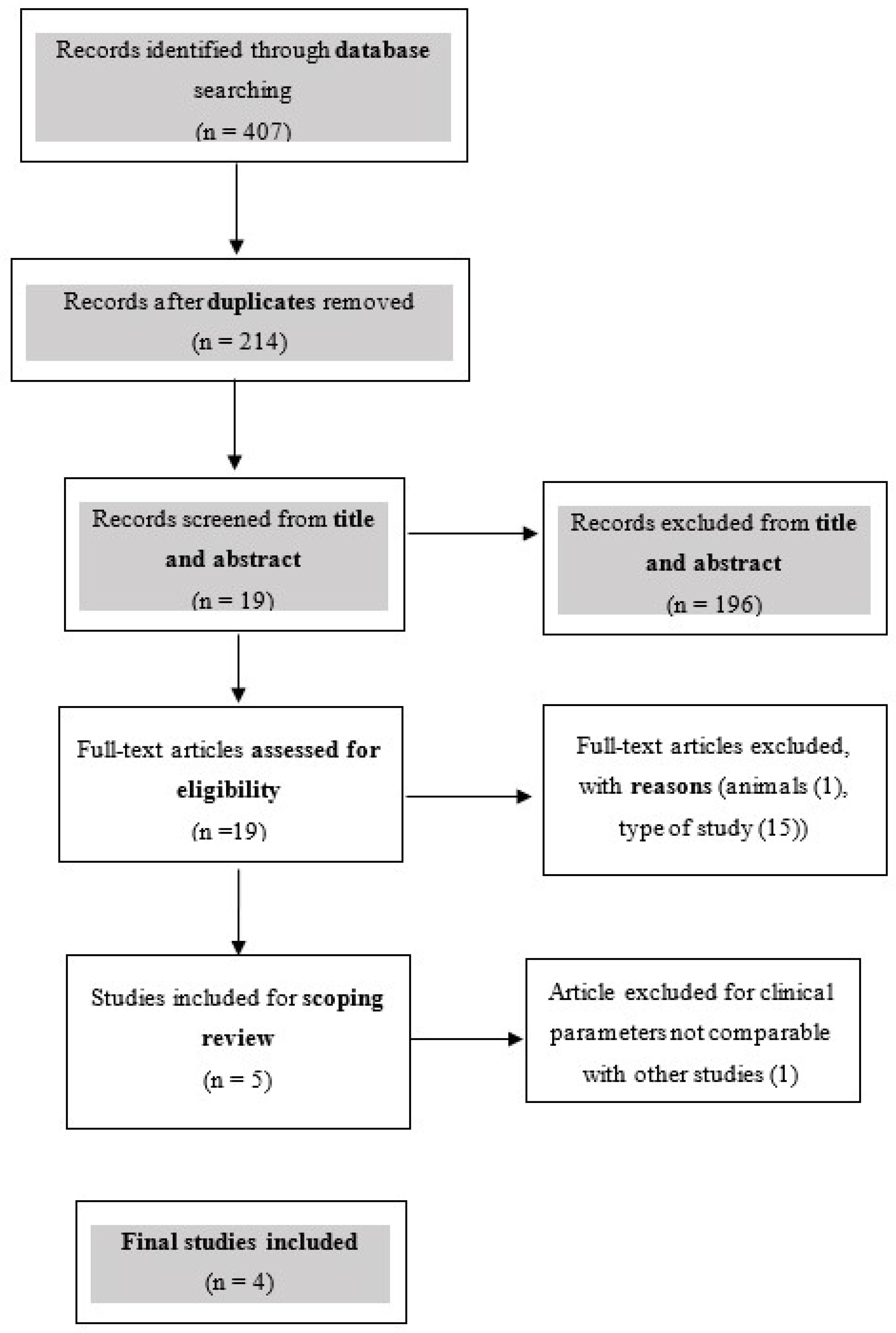
3. Results
Search and Selection Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89 (Suppl. 1), S313–S318. [Google Scholar] [CrossRef] [PubMed]
- Cortellini, P.; Bissada, N.F. Mucogingival conditions in the natural dentition: Narrative review, case definitions, and diagnostic considerations. J. Periodontol. 2018, 89 (Suppl. 1), S204–S213. [Google Scholar] [CrossRef]
- Patel, R.R.; Richards, P.S.; Inglehart, M.R. Periodontal health, quality of life, and smiling patterns—An exploration. J. Periodontol. 2008, 79, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Zucchelli, G.; Mounssif, I. Periodontal plastic surgery. Periodontology 2000 2015, 68, 333–368. [Google Scholar] [CrossRef] [PubMed]
- Meza Mauricio, J.; Furquim, C.P.; Bustillos-Torrez, W.; Soto-Peñaloza, D.; Peñarrocha-Oltra, D.; Retamal-Valdes, B.; Faveri, M. Does enamel matrix derivative application provide additional clinical benefits in the treatment of maxillary Miller class I and II gingival recession? A systematic review and meta-analysis. Clin. Oral. Investig. 2021, 25, 1613–1626. [Google Scholar] [CrossRef] [PubMed]
- Miller, P.D., Jr. A classification of marginal tissue recession. Int. J. Periodontics Restor. Dent. 1985, 5, 8–13. [Google Scholar]
- Cairo, F.; Nieri, M.; Cincinelli, S.; Mervelt, J.; Pagliaro, U. The interproximal clinical attachment level to classify gingival recessions and predict root coverage outcomes: An explorative and reliability study. J. Clin. Periodontol. 2011, 38, 661–666. [Google Scholar] [CrossRef]
- McGuire, M.K.; Scheyer, E.T.; Schupbach, P. A Prospective, Case-Controlled Study Evaluating the Use of Enamel Matrix Derivative on Human Buccal Recession Defects: A Human Histologic Examination. J. Periodontol. 2016, 87, 645–653. [Google Scholar] [CrossRef]
- McGuire, M.K.; Cochran, D.L. Evaluation of human recession defects treated with coronally advanced flaps and either enamel matrix derivative or connective tissue. Part 2: Histological evaluation. J. Periodontol. 2003, 74, 1126–1135. [Google Scholar] [CrossRef]
- França-Grohmann, I.L.; Sangiorgio, J.P.M.; Bueno, M.R.; Casarin, R.C.V.; Silvério Ruiz, K.G.; Nociti, F.H., Jr.; Casati, M.Z.; Sallum, E.A. Treatment of dehiscence-type defects with collagen matrix and/or enamel matrix derivative: Histomorphometric study in minipigs. J. Periodontol. 2020, 91, 967–974. [Google Scholar] [CrossRef]
- Chambrone, L.; Pini Prato, G.P. Clinical insights about the evolution of root coverage procedures: The flap, the graft, and the surgery. J. Periodontol. 2019, 90, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, E.L.; Roberts, J.L.; Moseley, R.; Griffiths, P.C.; Thomas, D.W. Evaluation of the physical and biological properties of hyaluronan and hyaluronan fragments. Int. J. Pharm. 2011, 420, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Meyer, K.; Palmer, J.W. The polysaccharide of the vitreous humor. J. Biol. Chem. 1934, 107, 629–634. [Google Scholar] [CrossRef]
- Fraser, J.R.; Laurent, T.C.; Laurent, U.B. Hyaluronan: Its nature, distribution, functions and turnover. J. Intern. Med. 1997, 242, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Laurent, T.C.; Fraser, J.R. Hyaluronan. Faseb. J. 1992, 6, 2397–2404. [Google Scholar] [CrossRef] [PubMed]
- Pirnazar, P.; Wolinsky, L.; Nachnani, S.; Haake, S.; Pilloni, A.; Bernard, G.W. Bacteriostatic effects of hyaluronic acid. J. Periodontol. 1999, 70, 370–374. [Google Scholar] [CrossRef] [PubMed]
- Fallacara, A.; Baldini, E.; Manfredini, S.; Vertuani, S. Hyaluronic Acid in the Third Millennium. Polymers 2018, 10, 701. [Google Scholar] [CrossRef]
- Dahiya, P.; Kamal, R. Hyaluronic Acid: A boon in periodontal therapy. N. Am. J. Med. Sci. 2013, 5, 309–315. [Google Scholar] [CrossRef]
- Prato, G.P.; Rotundo, R.; Magnani, C.; Soranzo, C.; Muzzi, L.; Cairo, F. An autologous cell hyaluronic acid graft technique for gingival augmentation: A case series. J. Periodontol. 2003, 74, 262–267. [Google Scholar] [CrossRef]
- Casale, M.; Moffa, A.; Vella, P.; Sabatino, L.; Capuano, F.; Salvinelli, B.; Lopez, M.A.; Carinci, F.; Salvinelli, F. Hyaluronic acid: Perspectives in dentistry. A systematic review. Int. J. Immunopathol. Pharmacol. 2016, 29, 572–582. [Google Scholar] [CrossRef]
- Pilloni, A.; Schmidlin, P.R.; Sahrmann, P.; Sculean, A.; Rojas, M.A. Effectiveness of adjunctive hyaluronic acid application in coronally advanced flap in Miller class I single gingival recession sites: A randomized controlled clinical trial. Clin. Oral. Investig. 2019, 23, 1133–1141. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.; Srinivas, M.; Pai, J.; Suragimath, G.; Prasad, K.; Polepalle, T. Efficacy of hyaluronic acid (hyaluronan) in root coverage procedures as an adjunct to coronally advanced flap in Millers Class I recession: A clinical study. J. Indian Soc. Periodontol. 2014, 18, 746–750. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Stern, C.; Aromataris, E.; Lockwood, C.; Jordan, Z. What kind of systematic review should I conduct? A proposed typology and guidance for systematic reviewers in the medical and health sciences. BMC Med. Res. Methodol. 2018, 18, 5. [Google Scholar] [CrossRef] [PubMed]
- Bateson, M. Systematic Reviews to Support Evidence-Based Medicine: How to Review and Apply Findings of Healthcare Research. Postgrad. Med. J. 2004, 80, 123. [Google Scholar]
- Al-Ardah, A.J.; AlHelal, A.; Proussaefs, P.; AlBader, B.; Al Humaidan, A.A.; Lozada, J. Managing Titanium Mesh Exposure With Partial Removal of the Exposed Site: A Case Series Study. J. Oral. Implant. 2017, 43, 482–490. [Google Scholar] [CrossRef]
- Nandanwar, J.; Bhongade, M.; Puri, S.; Dhadse, P.; Datir, M.; Kasatwar, A. Comparison of effectiveness of hyaluronic acid in combination with polylactic acid/polyglycolic acid membrane and subepithelial connective tissue graft for the treatment of multiple gingival recession defects in human: A clinical study. J. Datta Meghe Inst. Med. Sci. Univ. 2018, 13, 48–53. [Google Scholar] [CrossRef]
- Lanzrein, C.; Guldener, K.; Imber, J.C.; Katsaros, C.; Stähli, A.; Sculean, A. Treatment of multiple adjacent recessions with the modified coronally advanced tunnel or laterally closed tunnel in conjunction with cross-linked hyaluronic acid and subepithelial connective tissue graft: A report of 15 cases. Quintessence Int. 2020, 51, 710–719. [Google Scholar] [CrossRef]
- Guldener, K.; Lanzrein, C.; Eliezer, M.; Katsaros, C.; Stähli, A.; Sculean, A. Treatment of single mandibular recessions with the modified coronally advanced tunnel or laterally closed tunnel, hyaluronic acid, and subepithelial connective tissue graft: A report of 12 cases. Quintessence Int. 2020, 51, 456–463. [Google Scholar] [CrossRef]
- Baldi, C.; Pini-Prato, G.; Pagliaro, U.; Nieri, M.; Saletta, D.; Muzzi, L.; Cortellini, P. Coronally advanced flap procedure for root coverage. Is flap thickness a relevant predictor to achieve root coverage? A 19-case series. J. Periodontol. 1999, 70, 1077–1084. [Google Scholar] [CrossRef]
- Zucchelli, G.; Stefanini, M.; Ganz, S.; Mazzotti, C.; Mounssif, I.; Marzadori, M. Coronally Advanced Flap with Different Designs in the Treatment of Gingival Recession: A Comparative Controlled Randomized Clinical Trial. Int. J. Periodontics Restor. Dent. 2016, 36, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Sculean, A.; Cosgarea, R.; Stähli, A.; Katsaros, C.; Arweiler, N.B.; Brecx, M.; Deppe, H. The modified coronally advanced tunnel combined with an enamel matrix derivative and subepithelial connective tissue graft for the treatment of isolated mandibular Miller Class I and II gingival recessions: A report of 16 cases. Quintessence Int. 2014, 45, 829–835. [Google Scholar] [CrossRef] [PubMed]
- Sculean, A.; Allen, E.P. The Laterally Closed Tunnel for the Treatment of Deep Isolated Mandibular Recessions: Surgical Technique and a Report of 24 Cases. Int. J. Periodontics Restor. Dent. 2018, 38, 479–487. [Google Scholar] [CrossRef]
- West, D.C.; Hampson, I.N.; Arnold, F.; Kumar, S. Angiogenesis induced by degradation products of hyaluronic acid. Science 1985, 228, 1324–1326. [Google Scholar] [CrossRef] [PubMed]
- Scully, M.F.; Kakkar, V.V.; Goodwin, C.A.; O’Regan, M. Inhibition of fibrinolytic activity by hyaluronan and its alcohol ester derivatives. Thromb. Res. 1995, 78, 255–258. [Google Scholar] [CrossRef] [PubMed]
- Trombelli, L.; Simonelli, A.; Pramstraller, M.; Guarnelli, M.E.; Fabbri, C.; Maietti, E.; Farina, R. Clinical efficacy of a chlorhexidine-based mouthrinse containing hyaluronic acid and an antidiscoloration system in patients undergoing flap surgery: A triple-blind, parallel-arm, randomized controlled trial. Int. J. Dent. Hyg. 2018, 16, 541–552. [Google Scholar] [CrossRef] [PubMed]
- Vänttinen, E.; Viljanto, J. Tensile strength of new connective tissue formed in pretreated viscose cellulose implants. Ann. Med. Exp. Biol. Fenn. 1965, 43, 257–259. [Google Scholar]
- Pilloni, A.; Bernard, G.W. The effect of hyaluronan on mouse intramembranous osteogenesis in vitro. Cell Tissue Res. 1998, 294, 323–333. [Google Scholar] [CrossRef]
- Pilloni, A.; Rimondini, L.; De Luca, M.; Bernard, G.W. Effect of hyaluronan on calcification-nodule formation from human periodontal ligament cell culture. J. Appl. Biomater. Biomech. 2003, 1, 84–90. [Google Scholar]
- Wikesjö, U.M.; Selvig, K.A. Periodontal wound healing and regeneration. Periodontology 2000 1999, 19, 21–39. [Google Scholar] [CrossRef]
- Johannsen, A.; Tellefsen, M.; Wikesjö, U.; Johannsen, G. Local delivery of hyaluronan as an adjunct to scaling and root planing in the treatment of chronic periodontitis. J. Periodontol. 2009, 80, 1493–1497. [Google Scholar] [CrossRef] [PubMed]
- Jentsch, H.; Pomowski, R.; Kundt, G.; Göcke, R. Treatment of gingivitis with hyaluronan. J. Clin. Periodontol. 2003, 30, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Ficho, A.C.; de Souza Faloni, A.P.; Pennisi, P.R.C.; Borges, L.G.F.; de Macedo Bernadino, Í.; Paranhos, L.R.; Queiroz, T.P.; Santos, P.L. Is interdental papilla filling using hyaluronic acid a stable approach to treat black triangles? A systematic review. J. Esthet. Restor. Dent. 2021, 33, 458–465. [Google Scholar] [CrossRef] [PubMed]
- Ballini, A.; Cantore, S.; Capodiferro, S.; Grassi, F.R. Esterified hyaluronic acid and autologous bone in the surgical correction of the infra-bone defects. Int. J. Med. Sci. 2009, 6, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S.; Kediege, S.D.; Gupta, A.; Jain, K. Evaluation of gengigel® application in the management of furcation with coronally advanced flap through surgical re-entry-a split mouth clinical study. J. Clin. Diagn. Res. 2017, 11, ZC27–ZC32. [Google Scholar] [CrossRef]
- Ibraheem, W.; Jedaiba, W.H.; Alnami, A.M.; Hussain Baiti, L.A.; Ali Manqari, S.M.; Bhati, A.; Almarghlani, A.; Assaggaf, M. Efficacy of hyaluronic acid gel and spray in healing of extraction wound: A randomized controlled study. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 3444–3449. [Google Scholar] [CrossRef]
- Stähli, A.; Duong, H.Y.; Imber, J.C.; Roccuzzo, A.; Salvi, G.E.; Katsaros, C.; Ramseier, C.A.; Sculean, A. Recession coverage using the modified coronally advanced tunnel and connective tissue graft with or without enamel matrix derivative: 5-year results of a randomised clinical trial. Clin. Oral. Investig. 2022, 27, 105–113. [Google Scholar] [CrossRef]
- Górski, B.; Szerszeń, M.; Kaczyński, T. Effect of 24% EDTA root conditioning on the outcome of modified coronally advanced tunnel technique with subepithelial connective tissue graft for the treatment of multiple gingival recessions: A randomized clinical trial. Clin. Oral. Investig. 2022, 26, 1761–1772. [Google Scholar] [CrossRef]
- Rasperini, G.; Acunzo, R.; Limiroli, E. Decision Making in Gingival Recession Treatment: Scientific Evidence and Clinical Experience. Clin. Adv. Periodontics 2011, 1, 41–52. [Google Scholar] [CrossRef]
- Pini Prato, G.; Pagliaro, U.; Baldi, C.; Nieri, M.; Saletta, D.; Cairo, F.; Cortellini, P. Coronally advanced flap procedure for root coverage. Flap with tension versus flap without tension: A randomized controlled clinical study. J. Periodontol. 2000, 71, 188–201. [Google Scholar] [CrossRef]
- Pini-Prato, G.; Baldi, C.; Pagliaro, U.; Nieri, M.; Saletta, D.; Rotundo, R.; Cortellini, P. Coronally advanced flap procedure for root coverage. Treatment of root surface: Root planning versus polishing. J. Periodontol. 1999, 70, 1064–1076. [Google Scholar] [CrossRef]
- Lang, N.P.; Lindhe, J. Clinical Periodontology and Implant Dentistry; 2 Volume Set; Wiley: Hoboken, NJ, USA, 2015. [Google Scholar]
- Chambrone, L.; Tatakis, D.N. Periodontal soft tissue root coverage procedures: A systematic review from the AAP Regeneration Workshop. J. Periodontol. 2015, 86, S8–S51. [Google Scholar] [CrossRef] [PubMed]
- Cairo, F.; Nieri, M.; Pagliaro, U. Efficacy of periodontal plastic surgery procedures in the treatment of localized facial gingival recessions. A systematic review. J. Clin. Periodontol. 2014, 41 (Suppl. 15), S44–S62. [Google Scholar] [CrossRef] [PubMed]
- Chambrone, L.; Lima, L.A.; Pustiglioni, F.E.; Chambrone, L.A. Systematic review of periodontal plastic surgery in the treatment of multiple recession-type defects. J. Can. Dent. Assoc. 2009, 75, 203a–203f. [Google Scholar]
- Chambrone, L.; Sukekava, F.; Araújo, M.G.; Pustiglioni, F.E.; Chambrone, L.A.; Lima, L.A. Root-coverage procedures for the treatment of localized recession-type defects: A Cochrane systematic review. J. Periodontol. 2010, 81, 452–478. [Google Scholar] [CrossRef] [PubMed]
- Pini Prato, G.P.; Baldi, C.; Nieri, M.; Franseschi, D.; Cortellini, P.; Clauser, C.; Rotundo, R.; Muzzi, L. Coronally advanced flap: The post-surgical position of the gingival margin is an important factor for achieving complete root coverage. J. Periodontol. 2005, 76, 713–722. [Google Scholar] [CrossRef]
- Saletta, D.; Pini Prato, G.; Pagliaro, U.; Baldi, C.; Mauri, M.; Nieri, M. Coronally advanced flap procedure: Is the interdental papilla a prognostic factor for root coverage? J. Periodontol. 2001, 72, 760–766. [Google Scholar] [CrossRef]
- Hwang, D.; Wang, H.L. Flap thickness as a predictor of root coverage: A systematic review. J. Periodontol. 2006, 77, 1625–1634. [Google Scholar] [CrossRef]
- Al-Khateeb, R.; Olszewska-Czyz, I. Biological molecules in dental applications: Hyaluronic acid as a companion biomaterial for diverse dental applications. Heliyon 2020, 6, e03722. [Google Scholar] [CrossRef]
- Liu, H.; Yin, Y.; Yao, K.; Ma, D.; Cui, L.; Cao, Y. Influence of the concentrations of hyaluronic acid on the properties and biocompatibility of Cs-Gel-HA membranes. Biomaterials 2004, 25, 3523–3530. [Google Scholar] [CrossRef]
- Castellanos, A.; de la Rosa, M.; de la Garza, M.; Caffesse, R.G. Enamel matrix derivative and coronal flaps to cover marginal tissue recessions. J. Periodontol. 2006, 77, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Dias, A.T.; de Menezes, C.C.; Kahn, S.; Fischer, R.G.; da Silva Figueredo, C.M.; Fernandes, G.V.d.O. Gingival recession treatment with enamel matrix derivative associated with coronally advanced flap and subepithelial connective tissue graft: A split-mouth randomized controlled clinical trial with molecular evaluation. Clin. Oral. Investig. 2022, 26, 1453–1463. [Google Scholar] [CrossRef] [PubMed]
- Miron, R.J.; Caluseru, O.M.; Guillemette, V.; Zhang, Y.; Gemperli, A.C.; Chandad, F.; Sculean, A. Influence of enamel matrix derivative on cells at different maturation stages of differentiation. PLoS ONE 2013, 8, e71008. [Google Scholar] [CrossRef]
- Pini-Prato, G.P.; Cairo, F.; Nieri, M.; Franceschi, D.; Rotundo, R.; Cortellini, P. Coronally advanced flap versus connective tissue graft in the treatment of multiple gingival recessions: A split-mouth study with a 5-year follow-up. J. Clin. Periodontol. 2010, 37, 644–650. [Google Scholar] [CrossRef] [PubMed]
- Cairo, F.; Rotundo, R.; Miller, P.D.; Pini Prato, G.P. Root coverage esthetic score: A system to evaluate the esthetic outcome of the treatment of gingival recession through evaluation of clinical cases. J. Periodontol. 2009, 80, 705–710. [Google Scholar] [CrossRef] [PubMed]
- Rotundo, R.; Nieri, M.; Mori, M.; Clauser, C.; Prato, G.P. Aesthetic perception after root coverage procedure. J. Clin. Periodontol. 2008, 35, 705–712. [Google Scholar] [CrossRef]
- Cairo, F.; Barootchi, S.; Tavelli, L.; Barbato, L.; Wang, H.L.; Rasperini, G.; Graziani, F.; Tonetti, M. Aesthetic-And patient-related outcomes following root coverage procedures: A systematic review and network meta-analysis. J. Clin. Periodontol. 2020, 47, 1403–1415. [Google Scholar] [CrossRef]


{kind=link}
| Participants | Subjects in a State of Good Overall Health, Characterized by Recession Type 1 or 2 According to the Miller Classification of Recession Defects |
|---|---|
| Interventions | Application of hyaluronic acid in the surgical treatment of gingival recessions. |
| Comparisons | The same surgical procedures without hyaluronic acid. |
| Outcomes | Reduction in recession depth, gain of clinical attachment level, probing depth assessment. |
| Study Design | Randomized controlled clinical trials, controlled clinical trials, retrospective and prospective case–control studies. |
| Article | Design | Number of Patients | Age | Number of Recession | Recession Type | Single/Multiple | HA | Surgical Technique | Test | Control | Outcome | Follow-Up |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2014 Kumar [22] | RCT split | 10 (7M-3F) | - | 20 | RT1 | Single | Linear hyaluronic acid (Gengigel 0.2% gel which is 0.2% hyaluronan gel marketed by Ricerfarma pharmaceuticals, Milan, Italy) | CAF [30] | CAF+HA (10) | CAF (10) | RD, PD, CAL, CRC, MRC | 1, 3, 6, 12, 24 Weeks |
| 2019 Pilloni [21] | RCT | 30 (16M-14F) | 30 | 30 | RT1 | Single | 1,6% cross-linked HA, 0.2% linear HA (Hyadent BG, Regedent) | CAF [31] | CAF+HA (15) | CAF (15) | RD, PD, CAL, KT, CRC, MRC, VAS | 18 months |
| 2020 Guldener [29] | CASE SERIES | 12 (2M-10F) | 26.8±9.2 | 12 | RT1 | Single | 1,6% cross-linked HA, 0.2% linear HA (Hyadent BG, Regedent) | MCAT+sCTG +HA [32] or LCT+sCTG +HA [33] | - | - | RD, PD, CAL, KT, CRC, MRC | Range 6 to 30 months |
| 2020 Lanzrein [28] | CASE SERIEs | 15 (5M-10F) | 38.6±15.8 | - | RT1 and RT2 | Multiple | 1,6% cross-linked HA, 0.2% linear HA (Hyadent BG, Regedent) | MCAT+sCTG+HA [32] LCT+sCTG+HA [33] | - | - | RD, PD, CAL, KT, CRC, MRC, RES | Range 6 to 33 months |
| FU | RD | PD | CAL | MRC | CRC | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | Follow-Up | p Value (Control versus Test) | Baseline | Follow-Up | p Value (Control versus Test) | Baseline | Follow-Up | p Value (Control versus Test) | Follow-Up | Follow-Up | ||
| 2014 Kumar [22] | 24 weeks | Test: 3.20 mm | Test: 1.10 mm | p > 0.05 | Test: 1.80 mm | Test: 1.70 mm | p = 0.917 | Test: 5 mm | Test: 2.80 mm | p = 0.71 | Test: 68.3% | Test: 40% |
| Control: 2.90 mm | Control: 1.00 mm | Control: 2.00 mm | Control: 2.00 mm | Control: 4.90 mm | Control: 3.00 mm | Control: 61.6% | Control: 20% | |||||
| 2019 Pilloni [21] | 18 months | Test: 3.0 [1.0] mm | Test: 0.0 [0.0] mm | p = 0.011 | Test: 1.0 [0.0] mm | Test: 1.0 [1.0] mm | p = 0.717 | Test: 4.0 [1.0] mm | Test: 1.0 [0.0] mm | p = 0.023 | Test: 93.8% | Test: 80% |
| Control: 3.0 [1.0] mm | Control: 1.0 [1.0] mm | Control: 1.0 [0.0] mm | Control: 2.0 [1.0] mm | Control: 4.0 [1.0] mm | Control: 2.0 [0.0] mm | Control: 73.1% | Control: 30% | |||||
| 2020 Guldener [29] | 6 ± 33 months | 4.6 [0.9] mm | 0.5 [0.6] mm | 1.8 [0.9] mm | 1.3 [0.5] | 6.4 mm | 1.8 [0.5] | 96.09% | 50% | |||
| 2020 Lanzrein [28] | 6 ± 30 months | 3.3 [0.8] mm | 0.8 [1.0] mm | 1.3 [0.5] mm | 1.5 [0.5] mm | 4.6 mm | 2.3 mm | 85.1% | 20% | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manfredini, M.; Beretta, M.; Maiorana, C.; Tandurella, M.; Salina, F.E.; Poli, P.P. Effectiveness of Adjunctive Hyaluronic Acid Application in Surgical Treatment of Gingival Recession Sites. Prosthesis 2023, 5, 635-646. https://doi.org/10.3390/prosthesis5030045
Manfredini M, Beretta M, Maiorana C, Tandurella M, Salina FE, Poli PP. Effectiveness of Adjunctive Hyaluronic Acid Application in Surgical Treatment of Gingival Recession Sites. Prosthesis. 2023; 5(3):635-646. https://doi.org/10.3390/prosthesis5030045
Chicago/Turabian StyleManfredini, Mattia, Mario Beretta, Carlo Maiorana, Marco Tandurella, Federica Eugenia Salina, and Pier Paolo Poli. 2023. "Effectiveness of Adjunctive Hyaluronic Acid Application in Surgical Treatment of Gingival Recession Sites" Prosthesis 5, no. 3: 635-646. https://doi.org/10.3390/prosthesis5030045
APA StyleManfredini, M., Beretta, M., Maiorana, C., Tandurella, M., Salina, F. E., & Poli, P. P. (2023). Effectiveness of Adjunctive Hyaluronic Acid Application in Surgical Treatment of Gingival Recession Sites. Prosthesis, 5(3), 635-646. https://doi.org/10.3390/prosthesis5030045