Abstract
Background: Immediate implant placement (IIP) or Type I implants have become more attractive than conventional implant placements as it reduces the number of surgical procedures and allows faster delivery of the final restoration compared to conventional implant placements. However, the survival of Type I implants varies depending on multiple factors. Purpose: To evaluate the survival rate of Type I implants, and to describe the factors influencing their failure. Materials and methods: A developed search strategy was applied to identify randomised controlled trials on single-unit immediate implants including at least six human participants with a minimum follow-up time of 12 months and published between 1 January 1999 and 1 January 2020 in several databases. The data were extracted independently using validated data extraction forms. Information on survival rates, number of implants placed, loading protocols, setting of the study, location of implants in the jaw, antibiotic protocol, grafting methods, and implant geometry were obtained and assessed. Results: Twenty-six randomised controlled trials with an average follow-up time of 24 months (range = 12–120 months) were included and analysed to give a survival rate ranging between 83.7 and 100%. Fifteen studies reported implant failures, of which twelve reported early losses (loss before definitive restoration). Nine early losses were due to lack of osseointegration, two did not report the reason for implant failure, and one was reported as iatrogenic. Of the eleven studies with 100% survival rates, the common trend observed was the use of titanium implants and an antibiotic regimen using amoxicillin. Conclusions: The survival rate for immediate single implant placement ranged from 83.7 to 100%. Implant failure was not consistently reported and when reported, failure due to lack of osseointegration prior to placement of the definitive restoration was the most common descriptor. Other attributed reasons included infection abscess, mobility after immediate loading, and iatrogenic complications.
1. Summary Box
- What is known:
There are several systematic reviews on the survival of immediate implants which did not differentiate between single-unit and multiple-unit implants, or between different loading protocols. These reviews also have limitations, such as inclusion of non-randomised controlled trials and no risk of bias assessment.
- What this study adds:
The current review was designed to overcome the limitations of these previous systematic reviews and to update the current knowledge on the survival rate of single-unit immediate implants. This study suggests that immediate implants can be a predictable procedure with high survival rates based on the most current randomised controlled trials.
2. Introduction
Implants are an attractive treatment option for single tooth replacement, especially when traditional restorative options may be too destructive or inconvenient for the patient, such as a conventional 3-unit, cantilevered, or resin-bonded fixed partial denture, or a removable partial denture. Despite the increasing popularity of implants, they require complex, multidisciplinary treatment planning and strict inclusion criteria [1].
Conventional implant placement typically requires longer periods of healing before the final restoration can be placed, which may increase the psychological impact of tooth loss [2]. Type I or immediate implant placement (IIP), therefore, has become the more appealing option for both patients and dentists due to the reduced number of surgical procedures and, hence, shorter treatment time [1]. However, IIP should be based on case selection as successful placement is not always guaranteed [1]. Primary stability, which is paramount in the success of dental implant treatment is often difficult in IIP due to the lack of hard tissue immediately post-extraction. In order to achieve primary stability, a 3–5 mm apical, palatal, and intraradicular bone is needed [2]. Furthermore, bony defects and unfavourable bony morphology post-extraction present a challenge to osseointegration [3]. When an implant fails to osteointegrate, its removal can cause trauma. As implants do not display bundle bone, the remaining defect after removal of failed implants do not behave like post-extraction sockets [4]. Therefore, a re-attempt at implant placement may not be possible and the patient may be left with less or even no option to replace their missing dentition [5,6].
The survival of an implant is defined as the presence of the implant upon recall examination, despite its conditions. Conversely, implant failure is the absence of the implant on recall examination. These definitions are derived from the Third International Team of Implantology (ITI) consensus meeting [7]. Implant failure can be further grouped into four main reasons: biological, mechanical, iatrogenic, or inadequate patient adaptation requiring removal of implants. Biological issues are related to osseointegration and can be classified into early and late loss depending on whether it was lost before or after implant loading, respectively [8].
There are several systematic reviews on the survival of immediate implants with different independent variables applied across a range of implant systems from numerous manufacturers [9,10,11,12,13,14,15]. Some of these studies did not differentiate between single-unit and multiple-unit implants, or between different loading protocols. Some of these reviews also included non-randomised controlled trials and did not investigate the risk of bias (refer to Table 1). The current review is designed to overcome the limitations of these previous systematic reviews. The objective of this systematic review is to evaluate the survival rate of single-unit immediate implants using recent randomised controlled trials, and to establish a link between the reasons for failure and factors that may influence its survival.

Table 1.
List of published systematic reviews on immediate implants and their limitations.
3. Materials and Methods
This systematic review was registered as a protocol in the International Prospective Register of Systematic Reviews (PROSPERO) platform (CRD42020173150), and the reporting was carried out following the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [16].
3.1. Search Strategy
A detailed search strategy was used for the PubMed database to identify all articles published between 1 January 1999 and 1 January 2020 in relation to the stated aims of this review. In addition, a manual search of Clinical Oral Implants Research and the European Journal of Oral Implantology was attempted to identify any relevant studies. The reference list from the included studies was also screened for further inclusions into this study.
Focused question: what is the survival rate of single-unit immediate implant and what is the reason for implant failure?
The following PICO strategy was designed to select the studies to be included in this review [17]:
Participants: Subjects requiring a single implant in the maxillary and mandibular areas.
Intervention: Implant placement using the immediate placement protocol (Type 1).
Comparison: Delayed implant treatment protocols (Type 4) used for the replacement of a single tooth in the maxillary and mandibular region.
Outcomes: Implant survival, implant failure, and the reasons for failure.
Eligibility criteria:
For a study to be included it must meet the following inclusion criteria:
- Randomised controlled trial;
- Study included a minimum of six human subjects or more, including split mouth studies;
- Used single-unit immediate implants;
- Minimum follow-up time of one year;
- Full-text study published in English
3.2. Study Selection
After the initial electronic search of titles by two authors (N.K. and B.K.), the titles and abstracts of all the studies identified via electronic searches were independently scanned by two reviewers (N.K. and L.A.M.). The next step was to review all selected abstracts to determine selection of full-text articles after applying the inclusion criteria. The full texts of all studies of possible relevance were then obtained for independent review and assessment by the two reviewers. Disagreements among reviewers were resolved by discussion. All studies meeting the inclusion criteria then underwent data extraction. Studies rejected at this or subsequent stages were removed and the reasons for exclusion were recorded (Figure 1).
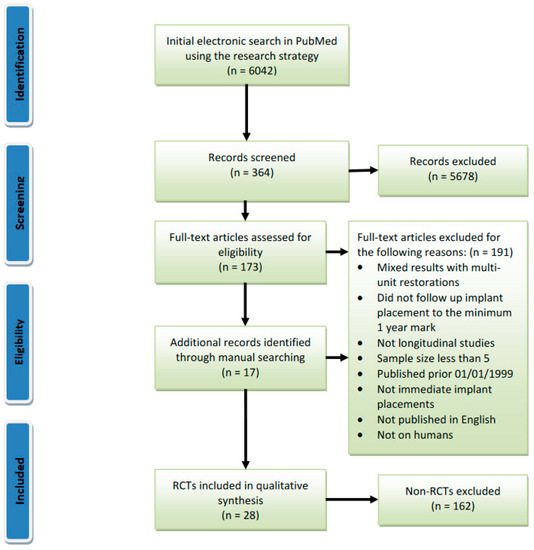
Figure 1.
PRISMA flow chart of the screened and included studies.
3.3. Data Extraction
The data were independently extracted by a group of seven review authors (N.K., W.T., P.S., P.G.S., J.G., C.T., D.C.) using validated data extraction forms. Any discrepancies between the reviewers were resolved by discussion and consensus after consultation with the other author (L.A.M.).
The implants in the included studies were grouped into four categories based on implant placement and loading protocol: immediate placement and immediate loading (IPL); immediate placement and immediate restoration with a non-occluding provisional crown (IPR); immediate placement and delayed restoration, which includes both early and conventional loading (IPDL); and delayed placement, regardless of loading technique (DP). This review classifies implant placement and implant loading protocols according to the Third International Team of Implantology (ITI) Consensus conference in 2003 [18,19].
The information on survival rates, number of implants placed, loading protocols, setting, location of implants in the jaw, antibiotic protocols, grafting methods, and implant systems were obtained (see Table 2). These parameters were assessed to determine if they influenced the survival rates reported by the studies.
3.4. Risk of Bias Assessment
The quality of the included studies was assessed by six independent reviewers (W.T., P.S., P.G.S., J.G., C.T., D.C.) following the Cochrane Risk of Bias tool for randomised controlled trials [20]. This tool encompasses seven criteria: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other bias. All studies were judged against these criteria as having low, unclear, or high risk of bias. The overall risk of bias was low if all criteria were considered to be at low risk of bias, unclear if there was at least one criterion with unclear risk of bias, and high if there was at least one criterion with a high risk of bias.
[Diagram is in a PDF file as requested by CIDRR author guidelines.]
Table 2.
Summary table of included studies.
Table 2.
Summary table of included studies.
| Study | Group | Settings | Follow-Up Time (Months) | Imp Survival % (IPL) | Imp Survival % (IPR) | Imp Survival % (IPDL) | Imp Survival % (DP) | Reason for Implant Failure | Antibiotics | Bone Grafting | Implant System/ Platform/ Geometry | Location in Jaw: No. of Imps |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Canullo et al., 2009/2017 [21,22] | IPR | Mc (2 PP) | 25, 120 | N/A | 100 | N/A | N/A | N/A | Augmentin: 1 h pre-op and 6 days post-op | Bovine bone matrix (Bio-Oss Collagen, Geistlich-Pharma, Wolhusen, Switzerland) | Global imp, 5.5 mm, 13 mm | Mx: 19 |
| Tallarico et al., 2016/2017 [23,24] | IPDL vs. DP | PP | 12 (6 months post loading) | N/A | N/A | 100 | 100 | N/A | Amoxicillin/Clindamycin: 1 h pre-op | Corticocancellous heterologous bone (OsteoBiol Gen-Os; Tecnoss srl, Giaveno, Italy) | Osstem TSIII Ultra-Wide 7 mm-diameter. 8.5 mm long (n = 4), 10 mm long (n = 18), and 11.5 mm long (n = 2) | Mx: 12 Md: 12 |
| Cannizzaro et al., 2010 [25] | IPL, IPR vs. DP | Mc (4 PP) | 36 | 40 | 80 | N/A | 97 | 1 IPL imp failed as bruxism habit was only diagnosed after failure; 4 imps failed to osseointegrate | Amoxicillin/Clindamycin: pre-op and 6 days post-op if graft was performed | Autogenous bone or bone substitutes | Z-Look3 zirconia implants, 3.25–6 mm, 10–15.5 mm | Mx: 29 Md: 11 |
| Shibly et al., 2012 [26] | IPL vs. IPDL | U | 3, 6, 12 | 96.6 | N/A | 93.3 | N/A | 1 imp failed due to mobility; 1 imp failed from acute infection 3 months after placement; 1 imp failed with no reason for implant failure given | Amoxicillin: 2 days pre-op and 10 days post-op | Sterile demineralized freeze-dried bone (DFDBA)—OraGRAFT, LifeNet Health, Virginia Beach, VA, USA. | NobelReplace™ Straight Groovy, with TiUnite® surface, Nobel Biocare | Mx: 36 Md: 19 |
| Block et al., 2009 [27] | IPR vs. IPDL | Not specified | 1, 2, 3, 4, 10, 16, 22 28 | N/A | 84.6 | 96.6 | N/A | 5 implants failed with no reason given | Cephalosporin: 7 days post-op | Human mineralized bone allograft | 3i, 11.5–13 mm | Mx: 55 |
| Canullo et al., 2010 [28] | IPR | Mc (3 PP) | 36 | N/A | 100 | N/A | N/A | N/A | Augmentin: 1 h pre-op | Nano-structured hydroxyapatite (Sintlife, Faenza, Italy) | Global Implant, 5.5 mm, 13 mm | Mx: 32 |
| De Rouck et al., 2009 [29] | IPR vs. IPDL | U | 12 | N/A | 96 | 92 | N/A | 1 imp failed due to mobility at 1 month; 2 imps failed due to mobility and pain at 3 months | Amoxicillin: 1 h pre-op and 5 days post-op | Bio-Oss®, (Geistlich Biomaterials, Mediplus, Rixensart, Belgium) | NobelReplace Tapered TiUnite, mostly diameter 4.3 mm, 16 mm | Mx: 30 |
| Degidi et al., 2014 [30] | IPR | PP | 24 | N/A | 100 | N/A | N/A | N/A | Amoxicillin: 1 h pre-op and 5 days post-op | Not specified | Square-threaded, grit-blasted, and acid-etched implant with a tapered connection (ANKYLOS®, DENTSPLY) | Mx: 53 |
| Esposito et al., 2015 [31] | IPR/IPDL vs. DP | Mc (3 PP) | 12 | N/A | 96.3 Study did not give separate results for IPR and IPDL imp | 100 | 1 imp failed due to mobility and pain at 1 month; 1 imp failed due to mobility at 4 months and imp crown was loose 20 days earlier | Amoxicillin/Clindamycin: 1 h pre-op and 6 days post-op if grafting was performed | Bio-Oss (Geistlich Pharma AG, Wolhusen, Switzerland) | Tapered titanium EZ Plus dental implants (MegaGen Implant, Gyeongbuk, Republic of Korea) with an internal connection, and RBM-treated surfaces, already provided with their definitive straight abutments | Mx: 106 | |
| Felice et al., 2015 [32] | IPR/IPDL vs. DP | Mc (4 PP) | 4, 12 | N/A | 92 Study did not give separate results for IPR and IPDL imp | 100 | 2 imps failed with unpleasant sensation/pain and mobility after 2 months after loading | Amoxicillin/Clindamycin: 1 h pre-op and 6 days post-op if grafting was performed | Frios Algipore (Dentsply, Friadent) | XiVE S plus (Dentsply Friadent, Mannheim, Germany) titanium, self-tapping, conical implants with an internal hexagon.Length choices: 8.0, 9.5, 11.0, 13.0, or 15.0 mm and diameters choices: 3.8, 4.5, or 5.5 mm | Mx: 48 | |
| Grandi et al., 2014 [33] | IPR | Mc | 12 | N/A | 100 | N/A | N/A | N/A | Augmentin/Clarithromycin: pre-op and 6/7 days post-op | Bio-Oss (Geistlich Bio-Oss, Geistlich Pharma, Wolhusen, Switzerland) | Tapered implants with internal connection and double acid-etched surface | Mx: 36 |
| Migliorati et al., 2015 [34] | IPR | Not specified | 0, 0.5, 12, 24 | N/A | 100 | N/A | N/A | N/A | Amoxicillin/Clindamycin: 1 h pre-op | Bio-Oss (Geistlich Pharma North America, Inc., Princeton, NJ, USA) | Tapered Effect or Bone Level SLActive, Straumann Co., Basel, Switzerland | Mx: 48 |
| Palatella et al., 2008 [35] | IPR vs. DP | U | 24 | N/A | 100 | N/A | 100 | N/A | Augmentin: 5 days post-op | - | Tapered effect (Institut Straumann AG, Waldenburg, Switzerland | Mx: 18 |
| Pieri et al., 2011 [36] | IPR | U | 12 | N/A | 97.4 | N/A | N/A | 1 imp failed with an abscess associated with a fistula | Augmentin: pre-op and 1 week post-op | Mixture of autogenous bone and Bio-Oss | Samo Smiler, root-shaped, microthreads in coronal portion, microporous and nanoroughened calcium and phosphorus-enriched titanium oxide surface. Platform switched when using Morse taper abutment | Mx: 38 |
| Slagter et al., 2015 [37] | IPR vs. IPDL | U | 12 | N/A | 100 | 100 | N/A | N/A | Amoxicillin: 7 days pre-op | Mixture of autogenous bone and Bio-Oss | NobelActive, Nobel BIocare AB | Mx: 40 |
| Yoshino et al., 2014 [38] | IPR | U | 12 | N/A | 100 | N/A | N/A | N/A | Did not specify antibiotic regime | BioOss, Osteohealth | Bone Level, Straumann USA. Dimensions: 3.3 mm, 14 mm (n = 5), 4.1 mm, 14 mm (n = 14), and 4.8 mm, 14 mm (n = 1) | Mx: 20 |
| Zuiderveld et al., 2018 [39] | IPR | U | 12 | N/A | 96.7 | N/A | N/A | 2 imps failed to osseointegrate | Amoxicillin/Clindamycin: 1 day pre-op and 7 days post-op | Bio-Oss and autogenous bone | Not specified | Mx: 60 |
| Cecchinato et al., 2015 [40] | IPDL | Mc | 36 | N/A | N/A | 98.9 | N/A | 1 imp was mobile at 16 weeks | No antibiotics used | Not specified | Either a cylindrical, 3.5 mm or 4.0 mm implant or a conical/cylindrical 4.5 or 5.0 mm implant (Osseospeed, DENTSPLY Implants) | Mx: 92 |
| Cordaro et al., 2009 [41] | IPDL | PP | 0, 1.5, 3, 6, 12, 18 | N/A | N/A | 96.6 | N/A | 1 imp failed due to prosthetic overload from under-trimming the removable prosthesis | No antibiotics used | Not specified | Tapered TE implants (Straumann) | Not specified (n = 30) |
| Cucchi et al., 2017 [42] | IPDL vs. DP | Mc | 12, 36 | N/A | N/A | 95.5 | 100 | 2 imps failed to osseointegrate | Amoxicillin: 1 h pre-op and 6 h post-op | Resorbable B-tricalcium phosphate (Oxofix, Biotec BTK, Dueville, Vicenza, Italy, BTK Italy) | BT SAFE Bone Level—double lead threads with a hexagonal conical connection and integrated platform shifting | Mx: 25 Md: 24 |
| De Angelis et al., 2011 [43] | IPDL | Mc (4 PP) | 12 | N/A | N/A | 91.3 | N/A | 6 imps were mobile at abutment connection at 3–4 months; 1 imp failed after 3-month loading at 6–7 months after placement | Amoxicillin/clindamycin: 1 h pre-op and 6 days post-op | Endobon® (Biomet 3i), a bovine-derived, deproteinised, osteoconductive hydroxyapatite ceramic | NanoTite™ Tapered Certain® Prevail® titanium alloy (Ti6Al4V) implants (Biomet 3i, Palm Beach, FL, USA) with internal connection. Dual acid etched and then partially covered with nanoscale calcium phosphate crystals. Biomet 3i platform-switched abutments | Mx: 50 Md: 30 |
| Koh et al., 2011 [44] | IPDL | U | 12 | N/A | N/A | 95.5 | N/A | 1 imp failed with no reason given | Amoxicillin/Azithromycin: pre-op and 7/3 days post-op | Mixture of cortical and cancellous particulates allograft (MinerOss) | Tapered internal implant, BioHorizon, Birmingham, AL | Mx: 21 |
| Prosper et al., 2003 [45] | IPDL | U | 3, 6, 9, 12, 24, 36, 48 | N/A | N/A | 100 | N/A | N/A | Augmentin: 6 days post-op | Synthetic hydroxyapatite (Biosite; Vebas, Milan, Italy) | Sandblasted, titanium (Bioactive Covering, Winsix, London, United Kingdom), self-threading cylindric screw, 5.9, 11, or 13 mm | Mx: 75 Md: 36 |
| Urban et al., 2011 [46] | IPDL | Not specified | 0.25, 12 | N/A | N/A | 83.7 | N/A | 15 imps failed to osseointegrate | Phenoxymethylpenicillin: 5 days pre-op | Autologous bone | Brånemark System, Mk III Groovy, Wide Platform implant (NobelBiocare, Göteborg, Sweden) with an external hex connection, 5.0 mm and a thread spacing of 0.8 mm | Mx: 45 Md: 47 |
| Crespi et al., 2008 [47] | IPL vs. IPDL | U | 24 | 100 | N/A | 100 | N/A | N/A | Amoxicillin: 1 h pre-op and 1 week post-op | Not specified | 40 outlink, Sweden & Marina, Pafova implants. 30 implants: 5 mm, 10 implants: 3.75 mm, 13 mm | Mx: 40 |
| Van Nimwegen et al., 2018 [48] | IPR | U | 12 | N/A | 96.7 | N/A | N/A | 2 imps failed to osseointegrate | Amoxicillin: pre-op and 7 days post-op | Mixture of autogenous bone and Bio-Oss | NobelActive (Nobel Biocare) | Mx: 60 |
IPR: immediately placed and restored, IPDL: immediately placed and delayed loading, IPL: immediately placed and loaded, DP: delayed placement, RCT: randomised control trial, PS-RCT: prospective randomised control trial, Mc: multicentre, PP: private practice, N/A: not applicable, RBM: resorbable blast media, IIP: immediately placed implants, Mx: maxillary, Md: mandibular.
4. Results
The first electronic search yielded 6042 citations that could be reviewed. After the abstracts were screened, 5674 of these were rejected. Full text assessment was conducted on 368 studies. A total of 193 articles were excluded: 69 studies were excluded on the grounds of mixed results with multi-unit restorations, 55 were rejected as they did not follow-up implant placement to the minimum 1-year mark, 30 were not longitudinal studies, 13 had a sample size less than six, 14 were published prior to 1 January 1999, 10 studies did not do IIP, one study was not published in English, and one study was not on humans (see Table 4).
Furthermore, 17 additional studies were included after manually searching the reference lists of non-excluded studies. An overall total of 192 longitudinal studies were accepted. A further 164 articles were rejected as they were not randomised controlled trials, and 28 articles were accepted; however, two studies were published twice at two different time points during their experiment so their results were combined [21,22,23,24]. A total of 26 randomised controlled trials were included in this study, with an average follow-up time of 24 months (range 12 to 120 months). A diagram detailing the search strategy is shown in the Figure 1.
Subsequently, the bias was assessed using the Cochrane Risk of Bias Tool for randomised controlled trials. A summary is provided in Table 3.
Table 3.
Risk of Bias Analysis. Analysis was done according to the Cochrane Risk of Bias Tool for randomised controlled trials.
4.1. Survival Rates
The overall range of survival rates was 40–100%. One study gave survival rates for IPL implants, of 80% [25]. They used zirconia implants, which considered to be rare at that time [26]. Another study has as high as 93.3% survival ate [27]. Fourteen studies gave survival rates for IPR, ranging from 80 to 100% [21,22,25,28,29,30,31,32,33,34,35,36,37,38,39,40,41]. For implants that were IPDL, thirteen studies gave survival rates ranging from 83.7 to 100% [23,24,28,30,32,33,39,42,43,44,45,46,47,48]. Six studies compared immediate implants to conventional DP implants and the survival rates for DP implants in these studies ranged from 97 to 100% [23,24,25,32,33,37,44].
When a study reported a 100% survival rate for immediate implants, regardless of loading protocol (i.e., either IPL, IPR, or IPDL group), all the comparison groups (IPL, IPR, or IPDL) also presented with a 100% survival rate. Eleven RCTs presented with 100% survival rates in immediate implants [21,22,23,24,29,31,34,35,37,39,40,47]. Conversely, three studies reported survival rates less than 90% [25,28,48]. One study in particular reported very a low survival rate of 40% for IPL and 80% for IPR [25].
4.2. Reasons Given for Implant Failure
There were fifteen studies which reported implant failure. Two studies gave no reason for the implant failures [28,46]. The implants failed early in twelve of these studies while four studies reported late implant failure, with three studies presenting both early and late implant failures (refer to Table 4). Nine studies gave lack of osseointegration as the reason for implant failure [7,25,30,36,41,42,44,45,48]. Other reasons for the implant failure included infection [27], abscess [38], mobility after loading in the IPL group [25], a patient who met the exclusion criteria but was included inadvertently [25], and an iatrogenic mistake where the clinician did not provide enough relief between an implant and the provisional denture [43].
Table 4.
Table of Excluded Studies. A total of 189 articles were excluded for the following reasons outlined in the headings [51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135,136,137,138,139,140,141,142,143,144,145,146,147,148,149,150,151,152,153,154,155,156,157,158,159,160,161,162,163,164,165,166,167,168,169,170,171,172,173,174,175,176,177,178,179,180,181,182,183,184,185,186,187,188,189,190,191,192,193,194,195,196,197,198,199,200,201,202,203,204,205,206,207,208,209,210,211,212,213,214,215,216,217,218,219,220,221,222,223,224,225,226,227,228,229,230,231,232,233,234,235,236,237,238,239]. A further 162 articles were excluded as they were not randomised controlled trials; these articles are not tabulated above but are included in the references [36,69,77,83,101,107,112,113,118,189,198,210,226,240,241,242,243,244,245,246,247,248,249,250,251,252,253,254,255,256,257,258,259,260,261,262,263,264,265,266,267,268,269,270,271,272,273,274,275,276,277,278,279,280,281,282,283,284,285,286,287,288,289,290,291,292,293,294,295,296,297,298,299,300,301,302,303,304,305,306,307,308,309,310,311,312,313,314,315,316,317,318,319,320,321,322,323,324,325,326,327,328,329,330,331,332,333,334,335,336,337,338,339,340,341,342,343,344,345,346,347,348,349,350,351,352,353,354,355,356,357,358,359,360,361,362,363,364,365,366,367,368,369,370,371,372,373,374,375,376,377,378,379,380,381,382,383,384,385,386,387,388].
4.3. Patient Selection Criteria
A list of the patient selection criteria in each study is summarised in Table 5. Most studies required their patients to be systemically healthy (n = 24), with no acute infection, either periapical or periodontal, in the area of implant placement (n = 22) and having an intact tooth socket or sufficient buccal bone after extraction (n = 22). These studies are listed in Table 6.
Table 5.
Inclusion and exclusion criteria of included studies.
Table 6.
List of articles that specified the above patient inclusion criteria.
Ten studies did not specify inclusion or exclusion of smokers and ten studies included smokers of ≤10 cigarettes a day. Three studies that did not specify smoking and six studies that included smoking ≤10 cigarettes a day achieved 100% survival rates. Three studies excluded smoking completely and three studies included smokers of ≤20 cigarettes a day, and all achieved survival rates >95%. Of the eleven studies achieving 100% survival rates across all categories, most included patients who smoked ≤10 cigarettes a day. Smoking inclusion is tabulated in Table 7.
Table 7.
Studies that included or excluded smokers.
4.4. Loading Protocol
Three studies investigated the effect of IPL implants. Four out of 51 IPL implants failed from the three studies. Only one out of these three studies reported a survival rate of <90%. One of these studies compared IPL and IPDL with survival rates of 96.6% (1 out of 26 implants failed) and 93.3% (2 out of 29 implants failed), respectively [27]. Even though the survival rate for the IPL implants was slightly higher, they did not find that the difference was significant.
One study by Cucchi et al. [44] loaded the implants early where definitive crowns were placed one week after implant placement. Two implants were lost out of the 49 implants that were placed in fresh extraction sockets (95.5% survival rate).
The remaining studies placed definitive restorations 3–6 months after placements (IPR or IPDL implants). All 11 studies that achieved a 100% survival rate had at least one experimental group using IPR or IPDL implants. Twelve studies reported survival rates between 91.3 and 98.9%, and three studies reported survival rates between 80 and 84.6% for IPR or IPDL implants. These are tabulated in Table 8.
Table 8.
Studies divided based on loading protocols used for the implants.
4.5. Antibiotic Therapy
Most studies used amoxicillin (n = 21). Among them, six studies used amoxicillin with clavulanic acid, six studies allowed substitution with clindamycin, and two studies allowed substitution of amoxicillin with azithromycin [46] or clarithromycin [34] if the patients were allergic to penicillin. All but one of these studies yielded a survival rate greater than 90% [25], with eleven of these studies yielding 100% survival across all categories of placement and loading. One study did not specify which antibiotic they used, but the study yielded 100% survival [40]. Two studies used phenoxymethylpenicillin [48] and cephalosporin [28], respectively, and both studies yielded survival rates below 90%. Two other studies did not use antibiotics, but yielded survival rates of 96.6% and 98.9%. The studies are listed in Table 9.
Table 9.
Studies divided based on the type of antibiotics used.
Twelve studies used antibiotics both pre-operatively and post-operatively. Of these studies, four had 100% survival rates and the rest had survival rates greater than 90%. Four studies only used antibiotics post-operatively, three of which had survival rates of 100% and one with a survival rate less than 90%. Five studies only used antibiotics pre-operatively, four of which had 100% survival rates and one had a survival rate lower than 90%. Three studies only used post-operative antibiotics if a graft was used, and survival rates ranged from 40 to 95.9%. The studies are listed in Table 10.
Table 10.
Studies divided based on antibiotics regimen.
4.6. Setting
Twelve studies were conducted in a private practice (PP), of which nine were multicentre (Mc) studies, eleven studies were conducted in a university setting (U), and three studies did not specify the location of the study (NS).
Of the studies that achieved 100% survival rates for immediate implants, five were conducted in private practices, four were in universities, and one with an unspecified setting. Of the studies with a survival rate of less than 90% for immediate implants, one was conducted in a private practice [25] and had survival rates of 40% for IPL and 80% for IPR implants. The other two did not specify the setting [28,48]. The studies are listed in Table 11.
Table 11.
Studies divided based on the setting in which the study was conducted.
4.7. Grafting Materials
Five studies did not use bone grafts, all of which had survival rates from 95 to 100%. Nine studies used xenografts, seven of which were bovine. Bio-Oss® (Geistlich Pharma AG, Wolhusen, Switzerland) was the graft of choice in four of those studies [30,32,34,40]. Canullo et al., 2009/2016, and Migliorati et al., 2013, used Bio-oss® Collagen (Geistlich-Pharma AG, Wolhusen, Switzerland) and Bio-Oss® Collagen (Geistlich PharmaNorth America, Inc., Princeton, NJ, USA), respectively [21,22,35]. Endobon® (Biomet 3i) is a bovine-derived osteoconductive hydroxyapatite used by De Angelis et al., 2011, and Felice et al., 2015, used an algae-derived bone substitute (FRIOS® Algipore®, Dentsply, Friadent, Mannheim, Germany) [33,45]. Lastly, Tallarico et al., 2016/2017, used a corticocancellous heterologous bone graft (OsteoBiol Gen-Os; Tecnoss srl, Giaveno, Italy) [23,24]. Of the xenografts, four of these documented a 100% survival rate for the IPR group [21,22,34,35,40] and one study documented 100% survival in the IPDL groups [23,24]. Overall, the survival rate ranged from 91.3 to 100%. Three studies used a mixture of autograft and xenograft (Bio-Oss®; Geistlich Pharma AG, Wolhusen, Switzerland) and the survival rate ranged from 96.7 to 100% [38,39,50]
Autografts were used by three studies, two with IPR groups with survival rates of 80% [25] and 96.7% [25,41] and one with an IPDL survival rate of 84% [48]. The survival rate of autografts ranged from 80 to 100%. Allografts were also used by three studies. Block et al. [28] reported a 84.6% rate in IPR, Koh et al. [46] reported 95.5% in IPDL, and Shibly et al. [27] who used sterile, demineralized, freeze-dried bone (OraGRAFT, LifeNet Health, Virginia Beach, VA, USA) reported 96.6% and 93.3% for IPL and IPDL, respectively [27]. The survival rate for allografts ranged from 84.6 to 96.6%. Hydroxyapatite alloplasts (Sintlife, Faenza, Italy) and (Biosite; Vebas, Milan, Italy) were incorporated in two studies [29,47]. Cucchi et al., 2017, used the alloplast B-tricalcium phosphate (Oxofix, Biotec BTK, Dueville, Vicenza, Italy, BTK Italy) [44]. Alloplasts were revealed to have 95.5–100% survival rates. The studies are listed on Table 12.
Table 12.
Studies listed by bone graft type.
4.8. Implants System/Geometry
All implants were titanium implants, except Cannizzaro et al. who used zirconia implants [25]. Tapered implants were the most common feature found in nine studies, with survival rates ranging from 91.3 to 100%. Four of the tapered implant studies reported 100% survival, all of which were in the IPR group [31,34,35,37]. Eight studies involved platform-switching implants. All survival rates were greater than 91.3–100%. Seven studies used wide or ultra-wide diameter implants and scored a survival rate between 83.7 and 100%. Tallarico et al., 2016/17, used wide implants and reported 100% in both its IPDL and DP groups [23,24]. Likewise, Prosper et al., 2003 also showed 100% survival in IPDL [47]; however Urban et al. noted a 83% survival rate and Cecchinato et al., 2015, reported 98.9% for the IPDL group [48]. Canullo et al., 2009/2016, and Canullo et al., 2010, both had 100% survival rates for the IPR group [21,22,29]. The studies are listed in Table 13.
Table 13.
Studies divided based on implant system and geometry.
4.9. Location of the Implant
Eighteen RCTs placed implants in the maxilla only, where eleven reported survival rates of 100%, six reported survival rates between 92 and 98.9%, and one RCT in the IPR group reported a survival rate of 84.6% [28]. Two out of the eighteen RCTs placed immediate implants in the maxillary anterior region only. Both studies reported 100% survival rates for IPR and DP implants. Five studies reported survival rates of IPR implants in the aesthetic zone (14–24), where three of the studies reported 100% survival rates and the other two reported 96.7% survival rates. Ten studies also included the second premolars. Six out of the ten RCTs reported 100% survival rates for the IPR group. The lowest survival rate for IPR implants involving maxillary anterior and premolar teeth was 84.6% reported by Block et al. [28]. The study also reported a 96.6% survival rate for the IPDL group. One other RCT only involved the maxillary posteriors and reported a survival rate for IPDL implants of 98.9%.
Eight RCTs involved placement of implants in both arches. Two RCT reported 100% survival rate for both IPDL and DP implants replacing posterior teeth. Cucchi et al. also noted similar results for DP posterior implants; however, the IPDL implants survival rate was only 95.5% [44]. Three other RCTs reported survival rates between 91.3 and 96.6% for IPDL posterior implants. One other study [25] investigated IPL, IPR, and DP implants involving both arches and reported survival rates of 40%, 80%, and 97%, respectively. The lowest survival rate for IPDL posterior implants was 83.7% [48]. The studies are listed on Table 14.
Table 14.
Studies divided based on location of the implants in the jaw.
5. Discussion
This systematic review analysed 26 randomised controlled trials to evaluate the survival rates of immediately placed single implants and describe the reasons for failure.
After analysis of the included articles, the survival rate of immediate single implants, regardless of loading, ranged from 40 to 100% over an average follow-up period of 24 months (range 12–120 months). One study that produced a drastically low survival rate of 40% for IPL and 80% for IPR was excluded as an outlier due to limitations, such as low sample size of IPL implants (n = 5), the use of zirconia implants, and that only one out of the four clinicians involved in the study had experience with zirconia implants [25]. After exclusion of this outlier, the survival rate range is 83.7–100%. Eleven RCTs presented with 100% survival rates in immediate implants. Similar to other reviews [10,11,13], most of the studies that were included in this review reported survival rates above 90%, except for three studies that reported survival rates of immediate implants ranging from 40 to 84.6% [25,28,48].
A previous systematic review on single immediate implants found a survival rate ranging between 94 and 100%, which is higher than our present study [14]. However, they included studies with a follow-up of less than a year. There was also a recent meta-analysis on single immediate implants, which resulted in a survival rate of 94.9% over a follow-up period of 12–96 months [13]. Two other meta-analyses on immediate implants also found similar survival rates, however they did not differentiate the results for single and multiple-units. Lang et al. [10] found a 2-year survival rate of 98.4% and a 4-year survival rate of 97.5%. Mello et al. [9] found a survival rate of 95.2% over a follow-up period of 6 months; however, they did not define ‘survival’, whereas the other reviews defined survival as the presence of the implant in the mouth, in accordance with the present review.
Most studies reported implant failure before placement of the definitive prosthesis and the main reason was failure of osseointegration, which is consistent with a previous systematic review [13]. Failure of osseointegration is commonly assessed by: clinical mobility of the implant, radiolucency between implant and bone, and the sound when a metal instrument taps the implant [389]. Two studies did not name a reason for implant failure, including Block et al. that reported a survival rate below 90% for IPR implants [28,46]. According to the study by Levin, a failure of osseointegration is typically due to overheating, trauma and contamination during surgery, lack of primary stability, micromotion, and overloading [390].
Of the 11 studies with 100% survival rates for immediate implants, the only consistent trend is the use of titanium implants and an amoxicillin antibiotic regime either pre- and/or post-operatively [21,22,23,24,26,29,31,34,35,37,39,40,47]. The preference for placement of implants in the maxilla and the use of grafting was also observed among these studies. Furthermore, the 100% survival rate trend may also be reflective of additional factors, such as operator experience and reporting bias.
In the study by Urban et al., 15 out of 92 implants failed [48]. A total of 11 out of the 15 failed implants were placed after tooth extraction due to apical periodontitis; however, the study did not utilise post-operative antibiotics nor did they debride the socket prior to the insertion of the implant. Most studies reporting high survival rates in apically infected sites debrided the extraction socket prior to insertion and implemented a post-operative antibiotic therapy to prevent bacterial transmission to the implant site [7,391]. Moreover, Urban et al. did not exclude smokers and used bone grafts in all implants [48], and previous studies have found significantly higher rates of implant failure in patients who smoke cigarettes, especially in those patients with bone grafts [392].
The effect of smoking on implant failure has been well-documented in the literature. Nicotine in cigarette smoke is detrimental to healing and osseointegration of implants [392,393]. On the other hand, smoking did not seem to play a visible role in survival in our current review, as similar survival rates were found in studies that included smokers in the inclusion criteria as compared to those that excluded them. It was noted that most studies either included smokers of less than or equal to ten cigarettes per day (n = 10) or did not exclude smoking (n = 10) (See Table 4). Not excluding smokers makes it difficult to discern the true number of smokers in the study and may hide the true impact of smoking on implant survival rates. Other than smoking, most studies tended to have stringent inclusion criteria and included only optimal situations where the patients are systemically healthy, and the site of implant placement has sufficient bone and lack of infection. The present study did not observe other patterns related to the remaining inclusion criteria.
The setting of a study may indicate the presence of factors that influence the results, such as operator experience and potential reporting bias. Of the included studies, there were an almost equal number of studies from private practices and universities, with three done in unknown settings. If the study by Cannizarro et al. [25] was excluded as an outlier, private practice survival rates ranged from 91.3 to 100%, whereas it ranged from 92 to 100% in universities. As both settings yielded similar results, bias arising from operator experience and selective reporting may be minimal.
Out of the 26 RCTs included in this study, only 3 investigated IPL implants [25,113,375]. Even though IPL implants significantly shorten treatment time, definitive prosthetic rehabilitation of an implant earlier than 3–4 months has not been recommended in the literature as it may jeopardise its stability [25,272,394,395]. Loading the implant with occlusal forces before complete healing can create micromotion which can prevent osseointegration and production of a fibrous scar tissue between the implant and bone [394]. This is supported by the high failure rate of IPL implants reported by Cannizarro et al. [25]. On the contrary, if the study by Cannizarro et al. [25] is excluded as an outlier, this review found that IPL implants have excellent results with survival rates of 96.6–100%. Even though this was concluded from a small sample size of two RCTs [27,113], this is supported by the findings from a previous systematic review that found a survival rate of 95.6% [396].
DP implants that were immediately loaded or loaded one week after placement also showed excellent survival rates, suggesting this may be a suitable treatment alternative. Again, as this was founded only on two RCTs [25,44], there is not enough evidence to corroborate the findings. Nevertheless, other studies have reported similar results [272,397].
Providing immediate non-occluding provisional restoration on the same day as implant placement is more desirable, as the patient does not have to be left without a tooth during the healing period while avoiding overloading the implants. Even though the provisional restorations can introduce micromovements that may interrupt osseointegration [398], immediate provisionalisation of post-extractive implants have been described as a reliable technique [36]. The current review found that IPDL implants have similar survival rates compared to IPR implants, where the survival rates for each group ranged from 83 to 100% and 80 to 100%, respectively.
According to the literature, the highest rate of implant failure was reported with post-extraction implants placed in the posterior maxilla due to poorer bone quality and the location of the base of maxillary sinus, which prevents the implant from achieving primary stability [224,399]. In agreement with this, the included studies that only placed IPDL implants in the posterior regions of both arches reported that most of the lost implants were placed in the posterior maxilla [44,48].
The majority of the RCTs that placed implants in the premaxillary zone achieved 100% survival rates, indicating that implants placed in this area can have predictable outcomes. According to the current review, IPR implants placed in the anterior maxilla only achieved 100% success rates. However, there were only two RCTs that exclusively placed implants in the anterior maxilla [31,37].
Interestingly, of the four studies that did not restrict the location of implant placement, none reported a 100% survival rate [25,27,43,45]. From these four studies, two failed implants replaced the mandibular second premolar [25,27]. The posterior mandible often receives heavy masticatory forces during function which may contribute to failure of these implants [399]. Furthermore, the height between the mandibular canal and the alveolar crest often limits the length of the implant which may be insufficient to achieve primary stability [399]. Hence, careful case selection and planning is required when placing implants in this area. Most of the included studies did not report the location of the lost implants, hence further investigation is required.
There is contradicting evidence on the benefits of antibiotics in implant therapy [10,13,400,401,402,403,404,405]. Furthermore, problems including antibiotic resistance and allergies can arise. Among the studies in the current review, only two studies [42,43] did not use an antibiotic regimen but both yielded high survival rates (96.6–98.9%). Whereas the studies yielding low survival rates used an antibiotic regimen. Hence, this review could not conclude that higher survival rates are solely due to the use of antibiotics.
There has been evidence that pre-operative antibiotics reduce early implant failure, by reducing the amount of bacteria in the surgical site [403,406,407,408,409]. On the other hand, the evidence on the benefit of post-operative antibiotics on implant therapy has been unclear [406,408]. In immediate implants, however, two systematic reviews found that the prescription of pre- and post-operative or only post-operative antibiotics significantly reduced early implant failure, especially when compared to use of pre-operative antibiotics only [10,13]. The present review found that half of the studies prescribing antibiotics used it both pre- and post-operatively. It was noted that none of these studies had survival rates below 90%, suggesting that there may be some benefit to this regimen. However, this suggestion should be treated with caution considering that only four of the eleven studies with 100% survival rates used this regimen.
In terms of the type of antibiotic, amoxicillin was the most commonly used (n = 21) and was used by all studies achieving 100% survival rates. Two of the three studies achieving survival rates less than 90% did not use amoxicillin as an antibiotic [28,48]. Hence, when antibiotics are used, amoxicillin may achieve higher survival rates. Another study also found amoxicillin as the most frequently prescribed antibiotic after implant placement [410]. Its efficacy is likely due to its moderate spectrum that encompasses odontogenic bacteria, along with an acceptable dosing schedule for good patient compliance [411]. There is limited data in the present review about the efficacy of alternative antibiotics for IIP in the case of a penicillin allergy. Clindamycin was used as an alternative to amoxicillin in only six studies [25,32,33,35,41,45], and clarithromycin and azithromycin were only used in one study each [34,46].
The use of bone grafts did not appear to influence survival rates in the studies which used bone grafts compared to those that did not. However, there is a consensus in the literature that bone grafts are advantageous in the inhibition of peri-implant bone loss in immediate extraction sockets [412]. When comparing the survival rates of the present included studies using autografts and allografts to other graft materials, xenografts and alloplasts had more consistently high survival rates. The accelerated resorption rates of autografts have made other grafting materials more desirable as they do not completely resorb and so the stability is retained long-term [413]. Another retrospective study using both immediate and delayed implants found the clinical survival rate for autografts to be 94.4–97.9% within a two-year follow-up, compared to 100% for bovine xenografts [414].
In the present study, only 1 in the 26 studies used zirconia implants, which is likely due to the lack of long-term data compared to the well-researched titanium implant [415]. Zirconia is an attractive alternative as it is said to attract less bacterial plaque, produce a low inflammatory infiltrate, and provide good tissue integration, which makes it desirable in limiting peri-implant biological complications [415]. However, a systematic review and meta-analysis with immediate and delayed placement of zirconia implants reported a 92% survival rate after one year whereas titanium implants boasted 97% after five years [416]. It is possible that the use of zirconia implants in the study by Cannizarro et al. [25] contributed to its poor survival rate.
Tapered implants were a popular design choice amongst the studies. The larger diameter threads at the coronal portion compared to the tapping portion led to better bone compaction at the crest at which the implants were placed [417]. This improved primary stability and may prevent early failure as seen in the nine studies using tapered implants, all reaching a survival rate of 100%. Platform-switching was the second most common design and is likely attributed to the numerous studies that have supported the significant reduction in peri-implant marginal bone loss [418,419]. The literature has reported that the survival rates between platform-switching implants and platform-matching implants were comparable and the type of platform was not considered to be the determinant of implant survival [419]. For the studies that used titanium implants only, the survival rates of platform-switched implants ranged from 91 to 100% whilst the survival rates for platform-matched implants ranged from 84 to 100% which suggests that platform-switching may influence survival. Wide diameter implants, defined as ≥4.5 mm (Renouard and Nisand 2006), presented mostly 100% survival rates (seven out of eight studies) [418]. Its ability to close the implant socket gap and engage more bone makes it easier to achieve primary stability, which reduces the need for bone grafts [23,419]. The wide diameter also prevents the implants from being overloaded which can diminish osseointegration [419]. A meta-analysis has reported that wide implants had a strong survival rate of 92% after five years [419].
The limitations of the studies are as follows. First, most of the included studies were of an unclear risk of bias and eight had a high risk of bias. Secondly, other confounding factors such as follow-up period and the patient history could present heterogeneity amongst the included studies. Finally, the small number of samples per placement or loading category makes it difficult to draw definitive conclusions.
6. Conclusions
This systematic review investigated 26 randomised control trials and found a survival rate of 83.7–100% for single immediately placed implants. Implant failure was not consistently reported and when reported, failure due to lack of osseointegration prior to placement of the definitive restoration was the most common descriptor. Others attributed reasons included infection abscess, mobility after immediate loading, and iatrogenic complication. Several factors may influence the survival of immediate implants, such as loading protocols, location of implants in the jaw, antibiotic protocol, grafting methods, and implant geometry; however, the current literature lacks a large volume of homogenous studies reporting on immediately placed implants and so further investigation is required.
Author Contributions
P.S.—data collection and analysis, drafting article, critical revision of article; P.G.S.—data collection and analysis, drafting article, critical revision of article; W.T.—data collection and analysis, drafting article, critical revision of article; L.A.M.—concept and study design, data collection, critical revision of article; N.K.—concept and study design, data collection, critical revision of article; B.K.—concept and study design, data collection, critical revision of article; O.K.—concept and study design, critical revision of article. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data available in additional tables.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bhola, M.; Neely, A.L.; Kolhatkar, S. Immediate Implant Placement: Clinical Decisions, Advantages, and Disadvantages. J. Prosthodont. 2008, 17, 576–581. [Google Scholar] [CrossRef]
- Hebel, K.; Gajjar, R.; Hofstede, T. Single-tooth replacement: Bridge vs. implant-supported restoration. J. (Can. Dent. Assoc.) 2000, 66, 435. [Google Scholar]
- Wilson, T.G., Jr.; Schenk, R.; Buser, D.; Cochran, D. Implants Placed in Immediate Extraction Sites: A Report of Histologic and Histometric Analyses of Human Biopsies. Int. J. Oral Maxillofac. Implant. 1998, 13, 333–341. [Google Scholar]
- Solderer, A.; Al-Jazrawi, A.; Sahrmann, P.; Jung, R.; Attin, T.; Schmidlin, P.R. Removal of failed dental implants revisited: Questions and answers. Clin. Exp. Dent. Res. 2019, 5, 712–724. [Google Scholar] [CrossRef] [PubMed]
- Chee, W.; Jivraj, S. Failures in implant dentistry. Br. Dent. J. 2007, 202, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Pjetursson, B.E.; Heimisdottir, K. Dental implants—Are they better than natural teeth? Eur. J. Oral Sci. 2018, 126, 81–87. [Google Scholar] [CrossRef]
- International Team for Implantology. Implant Survival and Complications. In Proceedings of the Third ITI Consensus Conference, Gstaad, Switzerland, August 2003; pp. 7–154. [Google Scholar]
- Esposito, M.; Hirsch, J.-M.; Lekholm, U.; Thomsen, P. Biological factors contributing to failures of osseointegrated oral implants, (II). Etiopathogenesis. Eur. J. Oral Sci. 1998, 106, 721–764. [Google Scholar] [CrossRef] [PubMed]
- Atieh, M.A.; Payne, A.G.T.; Duncan, W.J.; de Silva, R.K.; Cullinan, M.P. Immediate Placement or Immediate Restoration/Loading of Single Implants for Molar Tooth Replacement: A Systematic Review and Meta-analysis. Int. J. Oral Maxillofac. Implant. 2010, 25, 401–415. [Google Scholar]
- Chen, S.T.; Buser, D. Esthetic outcomes following immediate and early implant placement in the anterior maxilla—A systematic review. Int. J. Oral Maxillofac. Implant. 2014, 29, 186–215. [Google Scholar] [CrossRef]
- Cosyn, J.; De Lat, L.; Seyssens, L.; Doornewaard, R.; Deschepper, E.; Vervaeke, S. The effectiveness of immediate implant placement for single tooth replacement compared to delayed implant placement: A systematic review and meta-analysis. J. Clin. Periodontol. 2019, 46, 224–241. [Google Scholar] [CrossRef]
- Lang, N.P.; Pun, L.; Lau, K.Y.; Li, K.Y.; Wong, M.C. A systematic review on survival and success rates of implants placed immediately into fresh extraction sockets after at least 1 year. Clin. Oral Implant. Res. 2012, 23, 39–66. [Google Scholar] [CrossRef] [PubMed]
- Mello, C.C.; Lemos, C.A.A.; Verri, F.R.; dos Santos, D.M.; Goiato, M.C.; Pellizzer, E.P. Immediate implant placement into fresh extraction sockets versus delayed implants into healed sockets: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2017, 46, 1162–1177. [Google Scholar] [CrossRef]
- Pigozzo, M.N.; Rebelo da Costa, T.; Sesma, N.; Laganá, D.C. Immediate versus early loading of single dental implants: A systematic review and meta-analysis. J. Prosthet. Dent. 2018, 120, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Pjetursson, B.E.; Brägger, U.; Lang, N.P.; Zwahlen, M. Comparison of survival and complication rates of tooth-supported fixed dental prostheses (FDPs) and implant-supported FDPs and single crowns (SCs). Clin. Oral Implant. Res. 2007, 18, 97–113. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Needleman, I.G. A guide to systematic reviews. J. Clin. Periodontol. 2002, 29, 6–9. [Google Scholar] [CrossRef]
- Hämmerle, C.H.; Chen, S.T.; Wilson, T.G., Jr. Consensus statements and recommended clinical procedures regarding the placement of implants in extraction sockets. Int. J. Oral Maxillofac. Implant. 2004, 19, 26–28. [Google Scholar]
- Cochran, D.L.; Morton, D.; Weber, H.P. Consensus statements and recommended clinical procedures regarding loading protocols for endosseous dental implants. Int. J. Oral Maxillofac. Implant. 2004, 19, 109–113. [Google Scholar]
- Higgins, J.P.T.; Altman, D.G.; Sterne, J.A.C. (Eds.) Chapter 8: Assessing Risk of Bias in Included Studies. In Cochrane Handbook for Systematic Reviews of Interventions Version 510 (Updated March 2011); The Cochrane Collaboration: London, UK, 2011. [Google Scholar]
- Canullo, L.; Caneva, M.; Tallarico, M. Ten-year hard and soft tissue results of a pilot double-blinded randomized controlled trial on immediately loaded post-extractive implants using platform-switching concept. Clin. Oral Implant. Res. 2017, 28, 1195–1203. [Google Scholar] [CrossRef]
- Canullo, L.; Goglia, G.; Iurlaro, G.; Iannello, G. Short-term bone level observations associated with platform switching in immediately placed and restored single maxillary implants: A preliminary report. Int. J. Prosthodont. 2009, 22, 277. [Google Scholar]
- Tallarico, M.; Xhanari, E.; Pisano, M.; De Riu, G.; Tullio, A.; Meloni, S.M. Single post-extractive ultra-wide 7 mm-diameter implants versus implants placed in molar healed sites after socket preservation for molar replacement: 6-month post-loading results from a randomised controlled trial. Eur. J. Oral Implantol. 2016, 9, 263. [Google Scholar] [PubMed]
- Tallarico, M.; Xhanari, E.; Pisano, M.; Gatti, F.; Meloni, S.M. Molar replacement with 7 mm-wide diameter implants: To place the implant immediately or to wait 4 months after socket preservation? 1 year after loading results from a randomised controlled trial. Eur. J. Oral Implantol. 2017, 10, 169. [Google Scholar] [PubMed]
- Cannizzaro, G.; Torchio, C.; Felice, P.; Leone, M.; Esposito, M. Immediate occlusal versus non-occlusal loading of single zirconia implants. A multicentre pragmatic randomised clinical trial. Eur. J. Oral. Implantol. 2010, 3, 111–120. [Google Scholar]
- Shibly, O.; Kutkut, A.; Patel, N.; Albandar, J.M. Immediate implants with immediate loading vs. conventional loading: 1-year randomized clinical trial. Clin. Implant. Dent. Relat. Res. 2012, 14, 663–671. [Google Scholar] [CrossRef] [PubMed]
- Block, M.S.; Mercante, D.E.; Lirette, D.; Mohamed, W.; Ryser, M.; Castellon, P. Prospective evaluation of immediate and delayed provisional single tooth restorations. J. Oral Maxillofac. Surg. 2009, 67, 89–107. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Bignozzi, I.; Cocchetto, R.; Cristalli, M.P.; Iannello, G. Immediate positioning of a definitive abutment versus repeated abutment replacements in post-extractive implants: 3-year follow-up of a randomised multicentre clinical trial. Eur. J. Oral Implantol. 2010, 3, 285. [Google Scholar] [PubMed]
- De Rouck, T.; Collys, K.; Wyn, I.; Cosyn, J. Instant provisionalization of immediate single-tooth implants is essential to optimize esthetic treatment outcome. Clin. Oral Implant. Res. 2009, 20, 566–570. [Google Scholar] [CrossRef]
- Degidi, M.; Nardi, D.; Daprile, G.; Piattelli, A. Nonremoval of Immediate Abutments in Cases Involving Subcrestally Placed Postextractive Tapered Single Implants: A Randomized Controlled Clinical Study. Clin. Implant. Dent. Relat. Res. 2014, 16, 794–805. [Google Scholar] [CrossRef]
- Esposito, M.; Barausse, C.; Pistilli, R.; Jacotti, M.; Grandi, G.; Tuco, L.; Felice, P. Immediate loading of post-extractive versus delayed placed single implants in the anterior maxilla: Outcome of a pragmatic multicenter randomised controlled trial 1-year after loading. Eur. J. Oral Implantol. 2015, 8, 347. [Google Scholar]
- Felice, P.; Pistilli, R.; Barausse, C.; Trullenque-Eriksson, A.; Esposito, M. Immediate non-occlusal loading of immediate post-extractive versus delayed placement of single implants in preserved sockets of the anterior maxilla: 1-year post-loading outcome of a randomised controlled trial. Eur. J. Oral Implantol. 2015, 8, 361. [Google Scholar]
- Grandi, T.; Guazzi, P.; Samarani, R.; Maghaireh, H.; Grandi, G. One abutment-one time versus a provisional abutment in immediately loaded post-extractive single implants: A 1-year follow-up of a multicentre randomised controlled trial. Eur. J. Oral Implantol. 2014, 7, 141. [Google Scholar] [PubMed]
- Migliorati, M.; Amorfini, L.; Signori, A.; Biavati, A.S.; Benedicenti, S. Clinical and Aesthetic Outcome with Post-Extractive Implants with or without Soft Tissue Augmentation: A 2-Year Randomized Clinical Trial. Clin. Implant. Dent. Relat. Res. 2015, 17, 983–995. [Google Scholar] [CrossRef] [PubMed]
- Palattella, P.; Torsello, F.; Cordaro, L. Two-year prospective clinical comparison of immediate replacement vs. immediate restoration of single tooth in the esthetic zone. Clin. Oral Implant. Res. 2008, 19, 1148–1153. [Google Scholar] [CrossRef]
- Pieri, F.; Aldini, N.N.; Marchetti, C.; Corinaldesi, G. Influence of implant-abutment interface design on bone and soft tissue levels around immediately placed and restored single-tooth implants: A randomized controlled clinical trial. Int. J. Oral Maxillofac. Implant. 2011, 26, 169. [Google Scholar]
- Slagter, K.W.; Meijer, H.J.A.; Bakker, N.A.; Vissink, A.; Raghoebar, G.M. Feasibility of immediate placement of single-tooth implants in the aesthetic zone: A 1-year randomized controlled trial. J. Clin. Periodontol. 2015, 42, 773–782. [Google Scholar] [CrossRef]
- Yoshino, S.; Kan, J.Y.K.; Rungcharassaeng, K.; Roe, P.; Lozada, J.L. Effects of connective tissue grafting on the facial gingival level following single immediate implant placement and provisionalization in the esthetic zone: A 1-year randomized controlled prospective study. Int. J. Oral Maxillofac. Implant. 2014, 29, 432–440. [Google Scholar] [CrossRef]
- Zuiderveld, E.G.; Meijer, H.J.A.; den Hartog, L.; Vissink, A.; Raghoebar, G.M. Effect of connective tissue grafting on peri-implant tissue in single immediate implant sites: A RCT. J. Clin. Periodontol. 2018, 45, 253–264. [Google Scholar] [CrossRef] [PubMed]
- Cecchinato, D.; Lops, D.; Salvi, G.E.; Sanz, M. A prospective, randomized, controlled study using OsseoSpeed™ implants placed in maxillary fresh extraction socket: Soft tissues response. Clin. Oral Implant. Res. 2015, 26, 20–27. [Google Scholar] [CrossRef]
- Cordaro, L.; Torsello, F.; Roccuzzo, M. Clinical outcome of submerged vs. non-submerged implants placed in fresh extraction sockets. Clin. Oral Implant. Res. 2009, 20, 1307–1313. [Google Scholar] [CrossRef]
- Cucchi, A.; Vignudelli, E.; Franco, S.; Levrini, L.; Castellani, D.; Pagliani, L.; Rea, M.; Modena, C.; Sandri, G.; Longhi, C. Tapered, double-lead threads single implants placed in fresh extraction sockets and healed sites of the posterior jaws: A multicenter randomized controlled trial with 1 to 3 years of follow-up. BioMed Res. Int. 2017, 2017, 8017116–8017175. [Google Scholar] [CrossRef]
- De Angelis, N.; Felice, P.; Pellegrino, G.; Camurati, A.; Gambino, P.; Esposito, M. Guided bone regeneration with and without a bone substitute at single post-extractive implants: 1-year post-loading results from a pragmatic multicentre randomised controlled trial. Eur. J. Oral Implantol. 2011, 4, 313. [Google Scholar]
- Koh, R.U.; Oh, T.J.; Rudek, I.; Neiva, G.F.; Misch, C.E.; Rothman, E.D.; Wang, H.L. Hard and soft tissue changes after crestal and subcrestal immediate implant placement. J. Periodontol. 2011, 82, 1112–1120. [Google Scholar] [CrossRef] [PubMed]
- Prosper, L.; Gherlone, E.F.; Redaelli, S.; Quaranta, M. Four-year follow-up of larger-diameter implants placed in fresh extraction sockets using a resorbable membrane or a resorbable alloplastic material. Int. J. Oral Maxillofac. Implant. 2003, 18, 856. [Google Scholar]
- Urban, T.; Kostopoulos, L.; Wenzel, A. Immediate implant placement in molar regions: A 12-month prospective, randomized follow-up study. Clin. Oral Implant. Res. 2012, 23, 1389–1397. [Google Scholar] [CrossRef] [PubMed]
- Crespi, R.; Capparé, P.; Gherlone, E.; Romanos, G.E. Immediate versus delayed loading of dental implants placed in fresh extraction sockets in the maxillary esthetic zone: A clinical comparative study. Int. J. Oral Maxillofac. Implant. 2008, 23, 753–758. [Google Scholar]
- van Nimwegen, W.G.; Raghoebar, G.M.; Zuiderveld, E.G.; Jung, R.E.; Meijer, H.J.A.; Muehlemann, S. Immediate placement and provisionalization of implants in the aesthetic zone with or without a connective tissue graft: A 1-year randomized controlled trial and volumetric study. Clin. Oral Implant. Res. 2018, 29, 671–678. [Google Scholar] [CrossRef]
- Amato, F.; Polara, G.; Spedicato, G.A. Tissue Dimensional Changes in Single-Tooth Immediate Extraction Implant Placement in the Esthetic Zone: A Retrospective Clinical Study. Int. J. Oral Maxillofac. Implant. 2018, 33, 439–447. [Google Scholar] [CrossRef]
- Al Nashar, A.; Yakoob, H. Evaluation of the use of plasma rich in growth factors with immediate implant placement in periodontally compromised extraction sites: A controlled prospective study. Int. J. Oral Maxillofac. Surg. 2015, 44, 507–512. [Google Scholar] [CrossRef]
- Chu, S.; Salama, M.; Salama, H.; Garber, D.; Saito, H.; Sarnachiaro, G.; Tarnow, D. The dual-zone therapeutic concept of managing immediate implant placement and provisional restoration in anterior extraction sockets. Compend. Contin. Educ. Dent. 2012, 33, 524–532, 534. [Google Scholar]
- Becker, B.E.; Becker, W.; Ricci, A.; Geurs, N. A Prospective Clinical Trial of Endosseous Screw-Shaped Implants Placed at the Time of Tooth Extraction without Augmentation. J. Periodontol. 1998, 69, 920–926. [Google Scholar] [CrossRef]
- Aires, I.; Berger, J. Immediate Placement in Extraction Sites Followed by Immediate Loading: A Pilot Study and Case Presentation. Implant. Dent. 2002, 11, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Boardman, N.; Darby, I.; Chen, S. A retrospective evaluation of aesthetic outcomes for single-tooth implants in the anterior maxilla. Clin. Oral Implant. Res. 2016, 27, 443–451. [Google Scholar] [CrossRef]
- Kohal, R.; Klaus, G.; Strub, J. Clinical investigation of a new dental immediate implant system. The reimplant-system. Dtsch. Zahnarztl. Z. 2001, 57, 495–497. [Google Scholar]
- De Sanctis, M.; Vignoletti, F.; Discepoli, N.; Zucchelli, G.; Sanz, M. Immediate implants at fresh extraction sockets: Bone healing in four different implant systems. J. Clin. Periodontol. 2009, 36, 705–711. [Google Scholar] [CrossRef] [PubMed]
- Assaf, J.H.; Assaf, D.d.C.; Antoniazzi, R.P.; Osório, L.B.; França, F.M.G. Correction of Buccal Dehiscence during Immediate Implant Placement Using the Flapless Technique: A Tomographic Evaluation. J. Periodontol. 2017, 88, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Alves, C.C.; Correia, A.R.; Neves, M. Immediate implants and immediate loading in periodontally compromised patients-a 3-year prospective clinical study. Int. J. Periodontics Restor. Dent. 2010, 30, 447–455. [Google Scholar]
- Cornelini, R.; Scarano, A.; Covani, U.; Petrone, G.; Piattelli, A. Immediate one-stage postextraction implant: A human clinical and histologic case report. Int. J. Oral Maxillofac. Implant. 2000, 15, 432–437. [Google Scholar]
- Becker, W.; Lynch, S.E.; Lekholm, U.; Becker, B.E.; Caffesse, R.; Donath, K.; Sanchez, R. A Comparison of ePTFE Membranes Alone or in Combination with Platelet-Derived Growth Factors and Insulin-Like Growth Factor-I or Demineralized Freeze-Dried Bone in Promoting Bone Formation around Immediate Extraction Socket Implants. J. Periodontol. 1992, 63, 929–940. [Google Scholar] [CrossRef]
- Becker, W. Immediate implant placement: Treatment planning and surgical steps for successful outcomes. Br. Dent. J. 2006, 201, 199–205. [Google Scholar] [CrossRef]
- Buser, D.; Chappuis, V.; Kuchler, U.; Bornstein, M.M.; Wittneben, J.G.; Buser, R.; Cavusoglu, Y.; Belser, U.C. Long-term Stability of Early Implant Placement with Contour Augmentation. J. Dent. Res. 2013, 92, 176S–182S. [Google Scholar] [CrossRef]
- Basa, S.; Varol, A.; Turker, N. Alternative Bone Expansion Technique for Immediate Placement of Implants in the Edentulous Posterior Mandibular Ridge: A Clinical Report. Int. J. Oral Maxillofac. Implant. 2004, 19, 554–558. [Google Scholar]
- Anitua, E.; Piñas, L.; Alkhraisat, M.H. Long-Term Outcomes of Immediate Implant Placement into Infected Sockets in Association with Immediate Loading: A Retrospective Cohort Study. J. Periodontol. 2016, 87, 1135–1140. [Google Scholar] [CrossRef]
- de Molon, R.S.; de Avila, E.D.; de Barros-Filho, L.A.B.; Ricci, W.A.; Tetradis, S.; Cirelli, J.A.; Borelli de Barros, L.A. Reconstruction of the Alveolar Buccal Bone Plate in Compromised Fresh Socket after Immediate Implant Placement Followed by Immediate Provisionalization. J. Esthet. Restor. Dent. 2015, 27, 122–135. [Google Scholar] [CrossRef] [PubMed]
- Garber, D.A. The esthetic dental implant: Letting restoration be the guide. J. Am. Dent. Assoc. 1995, 126, 319–325. [Google Scholar] [CrossRef]
- Becker, C.M.; Wilson Jr, T.G.; Jensen, O.T. Minimum criteria for immediate provisionalization of single-tooth dental implants in extraction sites: A 1-year retrospective study of 100 consecutive cases. J. Oral Maxillofac. Surg. 2011, 69, 491–497. [Google Scholar] [CrossRef]
- Casap, N.; Zeltser, C.; Wexler, A.; Tarazi, E.; Zeltser, R. Immediate Placement of Dental Implants Into Debrided Infected Dentoalveolar Sockets. J. Oral Maxillofac. Surg. 2007, 65, 384–392. [Google Scholar] [CrossRef]
- Bell, C.; Bell, R.E. Immediate Restoration of NobelActive Implants Placed into Fresh Extraction Sites in the Anterior Maxilla. J. Oral Implantol. 2014, 40, 455–458. [Google Scholar] [CrossRef] [PubMed]
- Blus, C.; Szmukler-Moncler, S. Split-crest and immediate implant placement with ultra-sonic bone surgery: A 3-year life-table analysis with 230 treated sites. Clin. Oral Implant. Res. 2006, 17, 700–707. [Google Scholar] [CrossRef]
- Harvey, B.V. Optimizing the esthetic potential of implant restorations through the use of immediate implants with immediate provisionals. J. Periodontol. 2007, 78, 770–776. [Google Scholar] [CrossRef]
- Gelb, D.A. Immediate implant surgery: Three-year retrospective evaluation of 50 consecutive cases. Int. J. Oral Maxillofac. Implant. 1993, 8, 388–399. [Google Scholar]
- Bruno, V.; Badino, M.; Sacco, R.; Catapano, S. The use of a prosthetic template to maintain the papilla in the esthetic zone for immediate implant placement by means of a radiographic procedure. J. Prosthet. Dent. 2012, 108, 394–397. [Google Scholar] [CrossRef] [PubMed]
- Eghbali, A.; De Bruyn, H.; De Rouck, T.; Cleymaet, R.; Wyn, I.; Cosyn, J. Single Implant Treatment in Healing versus Healed Sites of the Anterior Maxilla: A Clinical and Radiographic Evaluation. Clin. Implant. Dent. Relat. Res. 2012, 14, 336–346. [Google Scholar] [CrossRef] [PubMed]
- Botticelli, D.; Berglundh, T.; Lindhe, J. Hard-tissue alterations following immediate implant placement in extraction sites. J. Clin. Periodontol. 2004, 31, 820–828. [Google Scholar] [CrossRef]
- Bogaerde, L.V.; Pedretti, G.; Sennerby, L.; Meredith, N. Immediate/Early Function of Neoss Implants Placed in Maxillas and Posterior Mandibles: An 18-Month Prospective Case Series Study. Clin. Implant. Dent. Relat. Res. 2010, 12, e83–e94. [Google Scholar] [CrossRef]
- Park, J.-B. Immediate Placement of Dental Implants into Fresh Extraction Socket in the Maxillary Anterior Region: A Case Report. J. Oral Implantol. 2010, 36, 153–157. [Google Scholar] [CrossRef]
- Gomez-Roman, G.; Schulte, W.; d’Hoedt, B.; Axman-Krcmar, D. The Frialit-2 implant system: Five-year clinical experience in single-tooth and immediately postextraction applications. Int. J. Oral Maxillofac. Implant. 1997, 12, 299–309. [Google Scholar]
- Le, B.; Borzabadi-Farahani, A.; Pluemsakunthai, W. Is buccolingual angulation of maxillary anterior implants associated with the crestal labial soft tissue thickness? Int. J. Oral Maxillofac. Surg. 2014, 43, 874–878. [Google Scholar] [CrossRef]
- Caiazzo, A.; Brugnami, F.; Mehra, P. Buccal plate preservation with immediate post-extraction implant placement and provisionalization: Preliminary results of a new technique. Int. J. Oral Maxillofac. Surg. 2013, 42, 666–670. [Google Scholar] [CrossRef] [PubMed]
- Cosyn, J.; De Bruyn, H.; Cleymaet, R. Soft tissue preservation and pink aesthetics around single immediate implant restorations: A 1-year prospective study. Clin. Implant. Dent. Relat. Res. 2013, 15, 847–857. [Google Scholar] [CrossRef]
- Paul, S. Risk versus gain in the flapless immediate approach for anterior implant esthetics: Case reports. Eur. J. Esthet. Dent. 2007, 2, 14–27. [Google Scholar]
- Hämmerle, C.H.; Brägger, U.; Schmid, B.; Lang, N.P. Successful bone formation at immediate transmucosal implants: A clinical report. Int. J. Oral Maxillofac. Implant. 1998, 13, 522–530. [Google Scholar]
- Chang, S.-W.; Shin, S.-Y.; Hong, J.-R.; Yang, S.-M.; Yoo, H.-M.; Park, D.-S.; Oh, T.-S.; Kye, S.-B. Immediate implant placement into infected and noninfected extraction sockets: A pilot study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2009, 107, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Proussaefs, P.; Kan, J.; Lozada, J.; Kleinman, A.; Farnos, A. Effects of immediate loading with threaded hydroxyapatite-coated root-form implants on single premolar replacements: A preliminary report. Int. J. Oral Maxillofac. Implant. 2002, 17, 567–572. [Google Scholar]
- Calvo Guirado, J.L.; Saez Yuguero, M.R.; Pardo Zamora, G.; Muñoz Barrio, E. Immediate provisionalization on a new implant design for esthetic restoration and preserving crestal bone. Implant. Dent. 2007, 16, 155–164. [Google Scholar] [CrossRef]
- Covani, U.; Cornelini, R.; Barone, A. Bucco-Lingual Bone Remodeling around Implants Placed into Immediate Extraction Sockets: A Case Series. J. Periodontol. 2003, 74, 268–273. [Google Scholar] [CrossRef]
- Penarrocha, M.; Lamas, J.; Penarrocha, M.; Garcia, B. Immediate maxillary lateral incisor implants with nonocclusal loading provisional crowns. J. Prosthodont. 2008, 17, 55–59. [Google Scholar] [CrossRef]
- Lang, N.P.; Brägger, U.; Hämmerle, C.H.; Sutter, F. Immediate transmucosal implants using the principle of guided tissue regeneration. I. Rationale, clinical procedures and 30-month results. Clin. Oral Implant. Res. 1994, 5, 154–163. [Google Scholar] [CrossRef]
- Chen, S.T.; Buser, D. Clinical and Esthetic Outcomes of Implants Placed in Postextraction Sites. Int. J. Oral Maxillofac. Implant. 2009, 24, 186–217. [Google Scholar]
- Ryser, M.R.; Block, M.S.; Mercante, D.E. Correlation of papilla to crestal bone levels around single tooth implants in immediate or delayed crown protocols. J. Oral. Maxillofac. Surg. 2005, 63, 1184–1195. [Google Scholar] [CrossRef]
- Chen, S.T.; Darby, I.B.; Reynolds, E.C.; Clement, J.G. Immediate Implant Placement Postextraction without Flap Elevation. J. Periodontol. 2009, 80, 163–172. [Google Scholar] [CrossRef]
- Covani, U.; Bortolaia, C.; Barone, A.; Sbordone, L. Bucco-Lingual Crestal Bone Changes after Immediate and Delayed Implant Placement. J. Periodontol. 2004, 75, 1605–1612. [Google Scholar] [CrossRef] [PubMed]
- Rebele, S.F.; Zuhr, O.; Hurzeler, M.B. Pre-extractive interradicular implant bed preparation: Case presentations of a novel approach to immediate implant placement at multirooted molar sites. Int. J. Periodontics Restor. Dent. 2013, 33, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Rosenquist, B.; Grenthe, B. Immediate placement of implants into extraction sockets: Implant survival. Int. J. Oral Maxillofac. Implant. 1996, 11, 205–209. [Google Scholar] [CrossRef]
- Daif, E.T.P. Effect of a Multiporous Beta-Tricalicum Phosphate on Bone Density around Dental Implants Inserted into Fresh Extraction Sockets. J. Oral Implantol. 2013, 39, 339–344. [Google Scholar] [CrossRef]
- Sarnowski, A.A.; Paul, B.F. A retrospective analysis of 12 immediate-implant restorations in the maxillary premolar region. Compend. Contin. Educ. Dent. 2012, 33, e83–e87. [Google Scholar]
- Chu, S.J.; Salama, M.A.; Garber, D.A.; Salama, H.; Sarnachiaro, G.O.; Sarnachiaro, E.; Gotta, S.L.; Reynolds, M.A.; Saito, H.; Tarnow, D.P. Flapless postextraction socket implant placement, Part 2: The effects of bone grafting and provisional restoration on peri-implant soft tissue height and thickness—A retrospective study. Int. J. Periodontics Restor. Dent. 2015, 35, 803–809. [Google Scholar] [CrossRef]
- Crespi, R.; Capparè, P.; Gherlone, E.; Romanos, G.E. Immediate occlusal loading of implants placed in fresh sockets after tooth extraction. Int. J. Oral Maxillofac. Implant. 2007, 22, 955–962. [Google Scholar]
- Ross, S.B.; Pette, G.A. Immediate implant placement and provisionalization using a customized anatomic temporary abutment (CATA) to achieve gingival margin stability. Compend. Contin. Educ. Dent. 2013, 34, 344–350. [Google Scholar]
- Schwartz-Arad, D.; Chaushu, G. The ways and wherefores of immediate placement of implants into fresh extraction sites: A literature review. J. Periodontol. 1997, 68, 915–923. [Google Scholar] [CrossRef]
- Enríquez-Sacristán, C.; Barona-Dorado, C.; Calvo-Guirado, J.L.; Leco-Berrocal, I.; Martínez-González, J.M. Immediate post-extraction implants subject to immediate loading: A meta-analytic study. Med. Oral Patol. Oral Y Cirugía Bucal 2011, 16, e919–e924. [Google Scholar] [CrossRef]
- Schropp, L.; Kostopoulos, L.; Wenzel, A. Bone healing following immediate versus delayed placement of titanium implants into extraction sockets: A prospective clinical study. Int. J. Oral Maxillofac. Implant. 2003, 18, 189–199. [Google Scholar]
- Chu, S.J.; Saito, H.; Salama, M.A.; Garber, D.A.; Salama, H.; Sarnachiaro, G.O.; Reynolds, M.A.; Tarnow, D.P. Flapless Postextraction Socket Implant Placement, Part 3: The Effects of Bone Grafting and Provisional Restoration on Soft Tissue Color Change—A Retrospective Pilot Study. Int. J. Periodontics Restor. Dent. 2018, 38, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Crespi, R.; Capparè, P.; Gherlone, E. Radiographic evaluation of marginal bone levels around platform-switched and non-platform-switched implants used in an immediate loading protocol. Int. J. Oral Maxillofac. Implant. 2009, 24, 920–926. [Google Scholar]
- Schiroli, G. Immediate tooth extraction, placement of a Tapered Screw-Vent implant, and provisionalization in the esthetic zone: A case report. Implant. Dent. 2003, 12, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Schwartz-Arad, D.; Chaushu, G. Immediate Implant Placement: A Procedure without Incisions. J. Periodontol. 1998, 69, 743–750. [Google Scholar] [CrossRef]
- Froum, S.J.; Cho, S.-C.; Francisco, H.; Park, Y.-S.; Elian, N.; Tarnow, D.P. Immediate implant placement and provisionalization--two case reports. Pract. Proced. Aesthetic Dent. PPAD 2007, 19, 621–628. [Google Scholar]
- Schropp, L.; Kostopoulos, L.; Wenzel, A.; Isidor, F. Clinical and radiographic performance of delayed-immediate single-tooth implant placement associated with peri-implant bone defects. A 2-year prospective, controlled, randomized follow-up report. J. Clin. Periodontol. 2005, 32, 480–487. [Google Scholar] [CrossRef]
- Covani, U.; Crespi, R.; Cornelini, R.; Barone, A. Immediate implants supporting single crown restoration: A 4-year prospective study. J. Periodontol. 2004, 75, 982–988. [Google Scholar] [CrossRef]
- Crespi, R.; Capparè, P.; Gherlone, E. A 4-Year Evaluation of the Peri-Implant Parameters of Immediately Loaded Implants Placed in Fresh Extraction Sockets. J. Periodontol. 2010, 81, 1629–1634. [Google Scholar] [CrossRef]
- Trimpou, G.; Weigl, P.; Krebs, M.; Parvini, P.; Nentwig, G.H. Rationale for esthetic tissue preservation of a fresh extraction socket by an implant treatment concept simulating a tooth replantation. Dent. Traumatol. 2010, 26, 105–111. [Google Scholar] [CrossRef]
- Simion, M.; Baldoni, M.; Zaffe, D. Jawbone enlargement using immediate implant placement associated with a split-crest technique and guided tissue regeneration. Int. J. Periodontics Restor. Dent. 1992, 12, 462–473. [Google Scholar]
- Fugazzotto, P.A.; Hains, F.O. Immediate implant placement in posterior areas, Part 2: The maxillary arch. Compend. Contin. Educ. Dent. 2013, 34, 518–528. [Google Scholar]
- Covani, U.; Cornelini, R.; Barone, A. Buccal Bone Augmentation around Immediate Implants with and without Flap Elevation: A Modified Approach. Int. J. Oral Maxillofac. Implant. 2008, 23, 841–846. [Google Scholar]
- Capelli, M.; Esposito, M.; Zuffetti, F.; Galli, F.; Del Fabbro, M.; Testori, T. A 5-year report from a multicentre randomised clinical trial: Immediate non-occlusal versus early loading of dental implants in partially edentulous patients. Eur. J. Oral Implantol. 2010, 3, 209–219. [Google Scholar]
- Turkyilmaz, I.; Suarez, J.C.; Company, A.M. Immediate implant placement and provisional crown fabrication after a minimally invasive extraction of a peg-shaped maxillary lateral incisor: A clinical report. J. Contemp. Dent. Pract. 2009, 10, E073–E080. [Google Scholar]
- Tritten, C.B.; Bragger, U.; Fourmousis, I.; Lang, N.P. Guided bone regeneration around an immediate transmucosal implant for single tooth replacement: A case report. Pract. Periodontics Aesthet Dent. 1995, 7, 29–38. [Google Scholar] [PubMed]
- Fugazzotto, P.A.; Hains, F.O. Immediate implant placement in posterior areas: The mandibular arch. Compend. Contin. Educ. Dent. 2012, 33, 494–496. [Google Scholar]
- Di Girolamo, M.; Arullani, C.; Calcaterra, R.; Manzi, J.; Arcuri, C.; Baggi, L. Preservation of extraction socket in immediate implant placement: A clinical study. Oral Implantol. 2016, 9, 222. [Google Scholar]
- Crespi, R.; Capparè, P.; Gherlone, E. Electrical mallet provides essential advantages in split-crest and immediate implant placement. Oral Maxillofac. Surg. 2014, 18, 59–64. [Google Scholar] [CrossRef]
- Werbitt, M.J.; Goldberg, P.V. The immediate implant: Bone preservation and bone regeneration. Int. J. Periodontics Restor. Dent. 1992, 12, 206–217. [Google Scholar]
- Gluckman, H.; Pontes, C.C.; Du Toit, J. Radial plane tooth position and bone wall dimensions in the anterior maxilla: A CBCT classification for immediate implant placement. J. Prosthet. Dent. 2018, 120, 50–56. [Google Scholar] [CrossRef] [PubMed]
- El-Chaar, E.S. Immediate Placement and Provisionalization of Implant-Supported, Single-Tooth Restorations: A Retrospective Study. Int. J. Periodontics Restor. Dent. 2011, 31, 408–419. [Google Scholar] [CrossRef] [PubMed]
- Crespi, R.; Capparè, P.; Gastaldi, G.; Gherlone, E.F. Buccal-Lingual Bone Remodeling in Immediately Loaded Fresh Socket Implants: A Cone Beam Computed Tomography Study. Int. J. Periodontics Restor. Dent. 2018, 38, 43–49. [Google Scholar] [CrossRef]
- Wilson, T.G., Jr. Guided tissue regeneration around dental implants in immediate and recent extraction sites: Initial observations. Int. J. Periodontics Restor. Dent. 1992, 12, 185–193. [Google Scholar]
- Greenstein, G.; Cavallaro, J. Immediate dental implant placement: Technique, part I. Dent Today 2014, 33, 98, 100–104. [Google Scholar] [PubMed]
- Evian, C.I.; Emling, R.; Rosenberg, E.S.; Waasdorp, J.A.; Halpern, W.; Shah, S.; Garcia, M. Retrospective analysis of implant survival and the influence of periodontal disease and immediate placement on long-term results. Int. J. Oral Maxillofac. Implant. 2004, 19, 393–398. [Google Scholar]
- Danza, M.; Guidi, R.; Carinci, F. Spiral Family Implants Inserted in Postextraction Bone Sites. Implant. Dent. 2009, 18, 270–278. [Google Scholar] [CrossRef]
- Wohrle, P.S. Single-tooth replacement in the aesthetic zone with immediate provisionalization: Fourteen consecutive case reports. Pract. Periodontics Aesthet. Dent. 1998, 10, 1107–1114. [Google Scholar]
- Holst, S.; Hegenbarth, E.A.; Schlegel, K.A.; Holst, A.I. Restoration of a nonrestorable central incisor using forced orthodontic eruption, immediate implant placement, and an all-ceramic restoration: A clinical report. J. Prosthet. Dent. 2007, 98, 251–255. [Google Scholar] [CrossRef]
- Felice, P.; Soardi, E.; Piattelli, M.; Pistilli, R.; Jacotti, M.; Esposito, M. Immediate non-occlusal loading of immediate post-extractive versus delayed placement of single implants in preserved sockets of the anterior maxilla: 4-month post-loading results from a pragmatic multicentre randomised controlled trial. Eur. J. Oral Implantol. 2011, 4, 329–344. [Google Scholar]
- Davarpanah, M.; Caraman, M.; Szmukler-Moncler, S.; Jakubowicz-Kohen, B.; Alcolforado, G. Preliminary Data of a Prospective Clinical Study on the Osseotite NT Implant: 18-month Follow-up. Int. J. Oral Maxillofac. Implant. 2005, 20, 448–454. [Google Scholar]
- Kan, J.Y.; Rungcharassaeng, K. Immediate placement and provisionalization of maxillary anterior single implants: A surgical and prosthodontic rationale. Pract. Periodontics Aesthet. Dent. 2000, 12, 817–824. [Google Scholar] [PubMed]
- Felice, P.; Zucchelli, G.; Cannizzaro, G.; Barausse, C.; Diazzi, M.; Trullenque-Eriksson, A.; Esposito, M. Immediate, immediate-delayed (6 weeks) and delayed (4 months) post-extractive single implants: 4-month post-loading data from a randomised controlled trial. Eur. J. Oral Implantol. 2016, 9, 233–247. [Google Scholar]
- Degidi, M.; Piattelli, A.; Carinci, F. Immediate Loaded Dental Implants: Comparison between Fixtures Inserted in Postextractive and Healed Bone Sites. J. Craniofacial Surg. 2007, 18, 965–971. [Google Scholar] [CrossRef] [PubMed]
- Kan, J.Y.; Rungcharassaeng, K.; Kois, J.C. Removable ovate pontic for peri-implant architecture preservation during immediate implant placement. Pract. Proced. Aesthet Dent. 2001, 13, 711–715. [Google Scholar] [PubMed]
- Fernandez Diaz, J.O.; Naval Gias, L. Rehabilitation of edentulous posterior atrophic mandible: Inferior alveolar nerve lateralization by piezotome and immediate implant placement. Int. J. Oral Maxillofac. Surg. 2013, 42, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Degidi, M.; Piattelli, A. Comparative Analysis Study of 702 Dental Implants Subjected to Immediate Functional Loading and Immediate Nonfunctional Loading to Traditional Healing Periods with a Follow-up of up to 24 Months. Int. J. Oral Maxillofac. Implant. 2005, 20, 99–107. [Google Scholar] [CrossRef]
- Kan, J.Y.; Rungcharassaeng, K.; Lozada, J.L. Bilaminar subepithelial connective tissue grafts for immediate implant placement and provisionalization in the esthetic zone. J. Calif. Dent. Assoc. 2005, 33, 865–871. [Google Scholar]
- Ferrus, J.; Cecchinato, D.; Pjetursson, E.B.; Lang, N.P.; Sanz, M.; Lindhe, J. Factors influencing ridge alterations following immediate implant placement into extraction sockets. Clin. Oral Implant. Res. 2010, 21, 22–29. [Google Scholar] [CrossRef]
- Del Fabbro, M.B.P.; Boggian, C.D.D.S.; Taschieri, S.M.D.D.D.S. Immediate Implant Placement into Fresh Extraction Sites with Chronic Periapical Pathologic Features Combined with Plasma Rich in Growth Factors: Preliminary Results of Single-Cohort Study. J. Oral Maxillofac. Surg. 2009, 67, 2476–2484. [Google Scholar] [CrossRef]
- Kan, J.Y.K.; Rungcharassaeng, K.; Deflorian, M.; Weinstein, T.; Wang, H.L.; Testori, T. Immediate implant placement and provisionalization of maxillary anterior single implants. Periodontol 2000 2018, 77, 197–212. [Google Scholar] [CrossRef]
- Granić, M.; Katanec, D.; Vučićević Boras, V.; Sušić, M.; Jurič, I.B.; Gabrić, D. Implant stability comparison of immediate and delayed maxillary implant placement by use of resonance frequency analysis—A clinical study. Acta Clin. Croat. 2015, 54, 3–8. [Google Scholar] [PubMed]
- Deng, F.; Zhang, H.; Zhang, H.; Shao, H.; He, Q.; Zhang, P. A comparison of clinical outcomes for implants placed in fresh extraction sockets versus healed sites in periodontally compromised patients: A 1-year follow-up report. Int. J. Oral Maxillofac. Implant. 2010, 25, 1036–1040. [Google Scholar]
- Kher, U.; Tunkiwala, A.; Umrigar, Z. Management of Fenestration Defects During Flapless Immediate Implant Placement in the Esthetic Zone. Int. J. Periodontics. Restor. Dent. 2015, 35, e90–e96. [Google Scholar] [CrossRef] [PubMed]
- Groenendijk, E.; Staas, T.A.; Graauwmans, F.E.J.; Bronkhorst, E.; Verhamme, L.; Maal, T.; Meijer, G.J. Immediate implant placement: The fate of the buccal crest. A retrospective cone beam computed tomography study. Int. J. Oral Maxillofac. Surg. 2017, 46, 1600–1606. [Google Scholar] [CrossRef] [PubMed]
- Koh, R.U.; Rudek, I.; Wang, H.L. Immediate implant placement: Positives and negatives. Implant. Dent. 2010, 19, 98–108. [Google Scholar] [CrossRef]
- Grunder, U. Crestal ridge width changes when placing implants at the time of tooth extraction with and without soft tissue augmentation after a healing period of 6 months: Report of 24 consecutive cases. Int. J. Periodontics Restor. Dent. 2011, 31, 9–17. [Google Scholar]
- Erakat, M.S.; Chuang, S.-K.; Yoo, R.H.; Weed, M.; Dodson, T.B. Immediate loading of splinted locking-taper implants: 1-year survival estimates and risk factors for failure. Int. J. Oral Maxillofac. Implant. 2008, 23, 105–110. [Google Scholar]
- Hossain, M.A.; Uddoula, M.S.; Mahmuduzzaman, M.; Rahman, M.A. Clinical Evaluation of Bucco-lingual Crestal Bone Remodeling in Mandibular Posterior Implants placed immediately and Delayed into Extraction Sites. Mymensingh Med. J. 2017, 26, 87–91. [Google Scholar]
- Finne, K.; Rompen, E.; Toljanic, J. Prospective multicenter study of marginal bone level and soft tissue health of a one-piece implant after two years. J Prosthet Dent 2007, 97 (Suppl. S6), S79–S85. [Google Scholar] [CrossRef]
- Lemongello, G.J. Customized provisional abutment and provisional restoration for an immediately-placed implant. Pract. Proced. Aesthet. Dent. 2007, 19, 419–424. [Google Scholar] [PubMed]
- Huynh-Ba, G.; Pjetursson, B.E.; Sanz, M.; Cecchinato, D.; Ferrus, J.; Lindhe, J.; Lang, N.P. Analysis of the socket bone wall dimensions in the upper maxilla in relation to immediate implant placement. Clin. Oral Implant. Res. 2010, 21, 37–42. [Google Scholar] [CrossRef]
- Fugazzotto, P.A. Implant placement in maxillary first premolar fresh extraction sockets: Description of technique and report of preliminary results. J. Periodontol. 2002, 73, 669–674. [Google Scholar] [CrossRef]
- Levine, R.A.; Ganeles, J.; Kan, J.; Fava, P.L. 10 Keys for Successful Esthetic-Zone Single Implants: Importance of Biotype Conversion for Lasting Success. Compend. Contin. Educ. Dent. 2018, 39, 522–529. [Google Scholar]
- Jofre, J.; Valenzuela, D.; Quintana, P.; Asenjo-Lobos, C. Protocol for immediate implant replacement of infected teeth. Implant. Dent. 2012, 21, 287–294. [Google Scholar] [CrossRef]
- Fugazzotto, P.A. Implant placement at the time of maxillary molar extraction: Treatment protocols and report of results. J. Periodontol. 2008, 79, 216–223. [Google Scholar] [CrossRef]
- Meltzer, A.M. Primary stability and initial bone-to-implant contact: The effects on immediate placement and restoration of dental implants. J. Implant. Reconstr. Dent. 2009, 1, 35–41. [Google Scholar]
- Kamperos, G.; Zambara, I.; Petsinis, V.; Zambaras, D. The Impact of Buccal Bone Defects and Immediate Placement on the Esthetic Outcome of Maxillary Anterior Single-Tooth Implants. J. Oral. Implantol. 2016, 42, 337–341. [Google Scholar] [CrossRef]
- Gokcen-Rohlig, B.; Meric, U.; Keskin, H. Clinical and radiographic outcomes of implants immediately placed in fresh extraction sockets. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 109, e1–e7. [Google Scholar] [CrossRef]
- Palti, A. Immediate placement and loading of implants in extraction sites: Procedures in the aesthetic zone. Dent. Implantol. Update 2004, 15, 41–47. [Google Scholar] [PubMed]
- Kolinski, M.L.; Cherry, J.E.; McAllister, B.S.; Parrish, K.D.; Pumphrey, D.W.; Schroering, R.L. Evaluation of a variable-thread tapered implant in extraction sites with immediate temporization: A 3-year multicenter clinical study. J. Periodontol. 2014, 85, 386–394. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Roman, G.; Kruppenbacher, M.; Weber, H.; Schulte, W. Immediate postextraction implant placement with root-analog stepped implants: Surgical procedure and statistical outcome after 6 years. Int. J. Oral Maxillofac. Implant. 2001, 16, 503–513. [Google Scholar]
- Ramsey, C.D. Single-tooth replacement of a maxillary central incisor via immediate implant placement. Pract. Proced. Aesthet. Dent. 2007, 19, 355–357. [Google Scholar] [PubMed]
- Lang, N.P.; Tonetti, M.S.; Suvan, J.E.; Pierre Bernard, J.; Botticelli, D.; Fourmousis, I.; Hallund, M.; Jung, R.; Laurell, L.; Salvi, G.E.; et al. Immediate implant placement with transmucosal healing in areas of aesthetic priority. A multicentre randomized-controlled clinical trial I. Surgical outcomes. Clin. Oral Implant. Res. 2007, 18, 188–196. [Google Scholar] [CrossRef]
- Grunder, U.; Polizzi, G.; Goene, R.; Hatano, N.; Henry, P.; Jackson, W.J.; Kawamura, K.; Kohler, S.; Renouard, F.; Rosenberg, R.; et al. A 3-year prospective multicenter follow-up report on the immediate and delayed-immediate placement of implants. Int. J. Oral Maxillofac. Implant. 1999, 14, 210–216. [Google Scholar]
- Saadoun, A.P. Immediate implant placement and temporization in extraction and healing sites. Compend. Contin. Educ. Dent. 2002, 23, 309–312, 314. [Google Scholar]
- Lee, E.A.; Gonzalez-Martin, O.; Fiorellini, J. Lingualized flapless implant placement into fresh extraction sockets preserves buccal alveolar bone: A cone beam computed tomography study. Int. J. Periodontics Restor. Dent. 2014, 34, 61–68. [Google Scholar] [CrossRef]
- Han, C.H.; Mangano, F.; Mortellaro, C.; Park, K.B. Immediate Loading of Tapered Implants Placed in Postextraction Sockets and Healed Sites. J. Craniofac. Surg. 2016, 27, 1220–1227. [Google Scholar] [CrossRef]
- Waki, T.; Kan, J.Y. Immediate placement and provisionalization of maxillary anterior single implant with guided bone regeneration, connective tissue graft, and coronally positioned flap procedures. Int. J. Esthet. Dent. 2016, 11, 174–185. [Google Scholar]
- Levin, B.P.; Chu, S.J. Changes in Peri-implant Soft Tissue Thickness with Bone Grafting and Dermis Allograft: A Case Series of 15 Consecutive Patients. Int. J. Periodontics Restor. Dent. 2018, 38, 719–727. [Google Scholar] [CrossRef]
- Hayacibara, R.M.; Gonçalves, C.S.; Garcez-Filho, J.; Magro-Filho, O.; Esper, H.; Hayacibara, M.F. The success rate of immediate implant placement of mandibular molars: A clinical and radiographic retrospective evaluation between 2 and 8 years. Clin. Oral Implant. Res. 2013, 24, 806–811. [Google Scholar] [CrossRef] [PubMed]
- Weigl, P.; Strangio, A. The impact of immediately placed and restored single-tooth implants on hard and soft tissues in the anterior maxilla. Eur. J. Oral. Implantol. 2016, 9 (Suppl. S1), S89–S106. [Google Scholar]
- Lops, D.; Chiapasco, M.; Rossi, A.; Bressan, E.; Romeo, E. Incidence of inter-proximal papilla between a tooth and an adjacent immediate implant placed into a fresh extraction socket: 1-year prospective study. Clin. Oral Implant. Res. 2008, 19, 1135–1140. [Google Scholar] [CrossRef] [PubMed]
- Heinemann, F.; Biffar, R.; Schwahn, C.; Mundt, T. Bone level changes in dental implants with platform-switched design after immediate and delayed placement in the maxilla. Int. J. Periodontics Restor. Dent. 2013, 33, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Yan, Q.; Xiao, L.Q.; Su, M.Y.; Mei, Y.; Shi, B. Soft and Hard Tissue Changes Following Immediate Placement or Immediate Restoration of Single-Tooth Implants in the Esthetic Zone: A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Implant. 2016, 31, 1327–1340. [Google Scholar] [CrossRef]
- Malo, P.; Rangert, B.; Dvarsater, L. Immediate function of Branemark implants in the esthetic zone: A retrospective clinical study with 6 months to 4 years of follow-up. Clin. Implant. Dent. Relat. Res. 2000, 2, 138–146. [Google Scholar] [CrossRef]
- Heinemann, F.; Bourauel, C.; Hasan, I.; Gedrange, T. Influence of the implant cervical topography on the crestal bone resorption and immediate implant survival. J. Physiol. Pharmacol. 2009, 60 (Suppl. S8), 99–105. [Google Scholar]
- Matarasso, S.; Salvi, G.E.; Iorio Siciliano, V.; Cafiero, C.; Blasi, A.; Lang, N.P. Dimensional ridge alterations following immediate implant placement in molar extraction sites: A six-month prospective cohort study with surgical re-entry. Clin. Oral Implant. Res. 2009, 20, 1092–1098. [Google Scholar] [CrossRef]
- Horwitz, J.; Zuabi, O.; Peled, M.; Machtei, E.E. Immediate and delayed restoration of dental implants in periodontally susceptible patients: 1-year results. Int. J. Oral Maxillofac. Implant. 2007, 22, 423–429. [Google Scholar]
- Miyamoto, Y.; Obama, T. Dental cone beam computed tomography analyses of postoperative labial bone thickness in maxillary anterior implants: Comparing immediate and delayed implant placement. Int. J. Periodontics Restor. Dent. 2011, 31, 215–225. [Google Scholar]
- Jo, H.Y.; Hobo, P.K.; Hobo, S. Freestanding and multiunit immediate loading of the expandable implant: An up-to-40-month prospective survival study. J. Prosthet. Dent. 2001, 85, 148–155. [Google Scholar] [CrossRef] [PubMed]
- Nemcovsky, C.E.; Artzi, Z.; Moses, O. Rotated split palatal flap for soft tissue primary coverage over extraction sites with immediate implant placement. Description of the surgical procedure and clinical results. J. Periodontol. 1999, 70, 926–934. [Google Scholar] [CrossRef]
- Khorsand, A.; Rasouli-Ghahroudi, A.A.; Naddafpour, N.; Shayesteh, Y.S.; Khojasteh, A. Effect of Microthread Design on Marginal Bone Level around Dental Implants Placed in Fresh Extraction Sockets. Implant. Dent. 2016, 25, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Nemcovsky, C.E.; Moses, O.; Artzi, Z.; Gelernter, I. Clinical coverage of dehiscence defects in immediate implant procedures: Three surgical modalities to achieve primary soft tissue closure. Int. J. Oral Maxillofac. Implant. 2000, 15, 843–852. [Google Scholar]
- Laviv, A.; Levin, L.; Usiel, Y.; Schwartz-Arad, D. Survival of immediately provisionalized dental implants: A case-control study with up to 5 years follow-up. Clin. Implant. Dent. Relat. Res. 2010, 12, e23–e27. [Google Scholar] [CrossRef]
- Nemcovsky, C.E.; Artzi, Z. Comparative study of buccal dehiscence defects in immediate, delayed, and late maxillary implant placement with collagen membranes: Clinical healing between placement and second-stage surgery. J. Periodontol. 2002, 73, 754–761. [Google Scholar] [CrossRef]
- Malchiodi, L.; Corrocher, G.; Cucchi, A.; Ghensi, P.; Bissolotti, G.; Nocini, P.F. Long-term results of immediately loaded fast bone regeneration-coated implants placed in fresh extraction sites in the upper jaw. J. Oral Implantol. 2010, 36, 251–261. [Google Scholar] [CrossRef]
- Parel, S.M.; Schow, S.R. Early clinical experience with a new one-piece implant system in single tooth sites. J. Oral Maxillofac. Surg. 2005, 63, 2–10. [Google Scholar] [CrossRef]
- Malchiodi, L.; Ghensi, P.; Cucchi, A.; Corrocher, G. A comparative retrospective study of immediately loaded implants in postextraction sites versus healed sites: Results after 6 to 7 years in the maxilla. Int. J. Oral Maxillofac. Implant. 2011, 26, 373–384. [Google Scholar]
- Peron, C.; Romanos, G. Immediate Placement and Occlusal Loading of Single-Tooth Restorations on Partially Threaded, Titanium-Tantalum Combined Dental Implants: 1-Year Results. Int. J. Periodontics Restor. Dent. 2016, 36, 393–399. [Google Scholar] [CrossRef]
- Malo, P.; Friberg, B.; Polizzi, G.; Gualini, F.; Vighagen, T.; Rangert, B. Immediate and early function of Branemark System implants placed in the esthetic zone: A 1-year prospective clinical multicenter study. Clin Implant. Dent. Relat Res 2003, 5 (Suppl. S1), 37–46. [Google Scholar] [CrossRef]
- Pirker, W.; Kocher, A. Immediate, non-submerged, root-analogue zirconia implants placed into single-rooted extraction sockets: 2-year follow-up of a clinical study. Int. J. Oral Maxillofac. Surg. 2009, 38, 1127–1132. [Google Scholar] [CrossRef]
- Mankoo, T. Maintenance of interdental papillae in the esthetic zone using multiple immediate adjacent implants to restore failing teeth--a report of ten cases at 2 to 7 years follow-up. Eur. J. Esthet. Dent. 2008, 3, 304–322. [Google Scholar]
- Redemagni, M.; Cremonesi, S.; Garlini, G.; Maiorana, C. Soft tissue stability with immediate implants and concave abutments. Eur. J. Esthet. Dent. 2009, 4, 328–337. [Google Scholar] [PubMed]
- McAllister, B.S.; Cherry, J.E.; Kolinski, M.L.; Parrish, K.D.; Pumphrey, D.W.; Schroering, R.L. Two-year evaluation of a variable-thread tapered implant in extraction sites with immediate temporization: A multicenter clinical trial. Int. J. Oral Maxillofac. Implant. 2012, 27, 611–618. [Google Scholar]
- Rieder, D.; Eggert, J.; Krafft, T.; Weber, H.P.; Wichmann, M.G.; Heckmann, S.M. Impact of placement and restoration timing on single-implant esthetic outcome—A randomized clinical trial. Clin. Oral Implant. Res. 2016, 27, e80–e86. [Google Scholar] [CrossRef]
- Meltzer, A.M. Immediate implant placement and restoration in infected sites. Int. J. Periodontics Restor. Dent. 2012, 32, e169–e173. [Google Scholar]
- Rungcharassaeng, K.; Kan, J.Y.; Yoshino, S.; Morimoto, T.; Zimmerman, G. Immediate implant placement and provisionalization with and without a connective tissue graft: An analysis of facial gingival tissue thickness. Int. J. Periodontics Restor. Dent. 2012, 32, 657–663. [Google Scholar]
- Mura, P. Immediate loading of tapered implants placed in postextraction sockets: Retrospective analysis of the 5-year clinical outcome. Clin. Implant. Dent. Relat. Res. 2012, 14, 565–574. [Google Scholar] [CrossRef]
- Noelken, R.; Neffe, B.A.; Kunkel, M.; Wagner, W. Maintenance of marginal bone support and soft tissue esthetics at immediately provisionalized OsseoSpeed implants placed into extraction sites: 2-year results. Clin. Oral Implant. Res. 2014, 25, 214–220. [Google Scholar] [CrossRef]
- Saito, H.; Chu, S.J.; Reynolds, M.A.; Tarnow, D.P. Provisional Restorations Used in Immediate Implant Placement Provide a Platform to Promote Peri-implant Soft Tissue Healing: A Pilot Study. Int. J. Periodontics Restor. Dent. 2016, 36, 47–52. [Google Scholar] [CrossRef]
- Noelken, R.; Kunkel, M.; Jung, B.A.; Wagner, W. Immediate nonfunctional loading of NobelPerfect implants in the anterior dental arch in private practice--5-year data. Clin. Implant. Dent. Relat. Res. 2014, 16, 21–31. [Google Scholar] [CrossRef]
- Sanz, M.; Cecchinato, D.; Ferrus, J.; Pjetursson, E.B.; Lang, N.P.; Lindhe, J. A prospective, randomized-controlled clinical trial to evaluate bone preservation using implants with different geometry placed into extraction sockets in the maxilla. Clin. Oral Implant. Res. 2010, 21, 13–21. [Google Scholar] [CrossRef]
- Noelken, R.; Oberhansl, F.; Kunkel, M.; Wagner, W. Immediately provisionalized OsseoSpeed(™) Profile implants inserted into extraction sockets: 3-year results. Clin. Oral Implant. Res. 2016, 27, 744–749. [Google Scholar] [CrossRef] [PubMed]
- Sarnachiaro, G.O.; Chu, S.J.; Sarnachiaro, E.; Gotta, S.L.; Tarnow, D.P. Immediate Implant Placement into Extraction Sockets with Labial Plate Dehiscence Defects: A Clinical Case Series. Clin. Implant. Dent. Relat. Res. 2016, 18, 821–829. [Google Scholar] [CrossRef] [PubMed]
- Noelken, R.; Moergel, M.; Kunkel, M.; Wagner, W. Immediate and flapless implant insertion and provisionalization using autogenous bone grafts in the esthetic zone: 5-year results. Clin. Oral Implant. Res. 2018, 29, 320–327. [Google Scholar] [CrossRef]
- Scarano, A. Traditional Postextractive Implant Site Preparation Compared with Pre-extractive Interradicular Implant Bed Preparation in the Mandibular Molar Region, Using an Ultrasonic Device: A Randomized Pilot Study. Int. J. Oral Maxillofac. Implant. 2017, 32, 655–660. [Google Scholar] [CrossRef] [PubMed]
- Ormianer, Z.; Palti, A. Retrospective clinical evaluation of tapered screw-vent implants: Results after up to eight years of clinical function. J. Oral Implantol. 2008, 34, 150–160. [Google Scholar] [CrossRef] [PubMed]
- Somanathan, R.V.; Simůnek, A.; Bukac, J.; Brázda, T.; Kopecká, D. Soft tissue esthetics in Implant. Dent.istry. Acta Med. (Hradec Kral.) 2007, 50, 183–186. [Google Scholar] [CrossRef]
- Ormianer, Z.; Piek, D.; Livne, S.; Lavi, D.; Zafrir, G.; Palti, A.; Harel, N. Retrospective clinical evaluation of tapered implants: 10-year follow-up of delayed and immediate placement of maxillary implants. Implant. Dent. 2012, 21, 350–356. [Google Scholar] [CrossRef]
- Tomasi, C.; Sanz, M.; Cecchinato, D.; Pjetursson, B.; Ferrus, J.; Lang, N.P.; Lindhe, J. Bone dimensional variations at implants placed in fresh extraction sockets: A multilevel multivariate analysis. Clin. Oral Implant. Res. 2010, 21, 30–36. [Google Scholar] [CrossRef]
- Paolantonio, M.; Dolci, M.; Scarano, A.; d’Archivio, D.; di Placido, G.; Tumini, V.; Piattelli, A. Immediate implantation in fresh extraction sockets. A controlled clinical and histological study in man. J. Periodontol. 2001, 72, 1560–1571. [Google Scholar] [CrossRef] [PubMed]
- van Kesteren, C.J.; Schoolfield, J.; West, J.; Oates, T. A prospective randomized clinical study of changes in soft tissue position following immediate and delayed implant placement. Int. J. Oral Maxillofac. Implant. 2010, 25, 562–570. [Google Scholar]
- Penarrocha-Diago, M.; Demarchi, C.L.; Maestre-Ferrin, L.; Carrillo, C.; Penarrocha-Oltra, D.; Penarrocha-Diago, M.A. A retrospective comparison of 1,022 implants: Immediate versus nonimmediate. Int. J. Oral Maxillofac. Implant. 2012, 27, 421–427. [Google Scholar]
- Vandeweghe, S.; Nicolopoulos, C.; Thevissen, E.; Jimbo, R.; Wennerberg, A.; De Bruyn, H. Immediate loading of screw-retained all-ceramic crowns in immediate versus delayed single implant placement. Int. J. Prosthodont. 2013, 26, 458–464. [Google Scholar] [CrossRef]
- Penarrocha-Oltra, D.; Demarchi, C.L.; Maestre-Ferrin, L.; Penarrocha-Diago, M.; Penarrocha-Diago, M. Comparison of immediate and delayed implants in the maxillary molar region: A retrospective study of 123 implants. Int. J. Oral Maxillofac. Implant. 2012, 27, 604–610. [Google Scholar]
- Vidigal, G.M., Jr.; Groisman, M.; Clavijo, V.G.; Barros Paulinelli Santos, I.G.; Fischer, R.G. Evaluation of Pink and White Esthetic Scores for Immediately Placed and Provisionally Restored Implants in the Anterior Maxilla. Int. J. Oral Maxillofac. Implant. 2017, 32, 625–632. [Google Scholar] [CrossRef]
- Perry, J.; Lenchewski, E. Clinical performance and 5-year retrospective evaluation of Frialit-2 implants. Int. J. Oral Maxillofac. Implant. 2004, 19, 887–891. [Google Scholar]
- West, J.D.; Oates, T.W. Identification of stability changes for immediately placed dental implants. Int. J. Oral Maxillofac. Implant. 2007, 22, 623–630. [Google Scholar]
- Polizzi, G.; Grunder, U.; Goené, R.; Hatano, N.; Henry, P.; Jackson, W.J.; Kawamura, K.; Renouard, F.; Rosenberg, R.; Triplett, G.; et al. Immediate and delayed implant placement into extraction sockets: A 5-year report. Clin. Implant. Dent. Relat. Res. 2000, 2, 93–99. [Google Scholar] [CrossRef]
- Younis, L.; Taher, A.; Abu-Hassan, M.I.; Tin, O. Evaluation of bone healing following immediate and delayed dental implant placement. J. Contemp. Dent. Pract. 2009, 10, 35–42. [Google Scholar] [CrossRef]
- Siebers, D.; Gehrke, P.; Schliephake, H. Delayed function of dental implants: A 1- to 7-year follow-up study of 222 implants. Int. J. Oral Maxillofac. Implant. 2010, 25, 1195–1202. [Google Scholar]
- Siebert, T.; Jurkovic, R.; Statelova, D.; Strecha, J. Immediate Implant Placement in a Patient with Osteoporosis Undergoing Bisphosphonate Therapy: 1-Year Preliminary Prospective Study. J. Oral Implantol. 2015, 41, 360–365. [Google Scholar] [CrossRef]
- Simsek, B.; Simsek, S. Evaluation of success rates of immediate and delayed implants after tooth extraction. Chin. Med. J. 2003, 116, 1216–1219. [Google Scholar] [PubMed]
- Stefanski, S.; Svensson, B.; Thor, A. Implant survival following sinus membrane elevation without grafting and immediate implant installation with a one-stage technique: An up-to-40-month evaluation. Clin. Oral Implant. Res. 2017, 28, 1354–1359. [Google Scholar] [CrossRef] [PubMed]
- Tsai, E.S.; Crohin, C.C.; Weber, H.P. A five-year evaluation of implants placed in extraction sockets. J. West. Soc. Periodontol. Abstr. 2000, 48, 37–47. [Google Scholar]
- van Steenberghe, D.; Callens, A.; Geers, L.; Jacobs, R. The clinical use of deproteinized bovine bone mineral on bone regeneration in conjunction with immediate implant installation. Clin. Oral Implant. Res. 2000, 11, 210–216. [Google Scholar] [CrossRef]
- Vanden Bogaerde, L.; Rangert, B.; Wendelhag, I. Immediate/early function of Branemark System TiUnite implants in fresh extraction sockets in maxillae and posterior mandibles: An 18-month prospective clinical study. Clin Implant. Dent. Relat Res 2005, 7 (Suppl. S1), S121–S130. [Google Scholar] [CrossRef]
- Vidal, R.; Greenwell, H.; Hill, M.; Papageorgakopoulos, G.; Scheetz, J.P. Success rate of immediate implants placed and restored by novice operators. Implant. Dent. 2010, 19, 81–90. [Google Scholar] [CrossRef]
- Villa, R.; Rangert, B. Immediate and early function of implants placed in extraction sockets of maxillary infected teeth: A pilot study. J. Prosthet. Dent. 2007, 97 (Suppl. S6), S96–S108. [Google Scholar] [CrossRef]
- Wagenberg, B.; Froum, S.J. A retrospective study of 1925 consecutively placed immediate implants from 1988 to 2004. Int. J. Oral Maxillofac. Implant. 2006, 21, 71–80. [Google Scholar]
- Wagenberg, B.D.; Froum, S.J.; Eckert, S.E. Long-term bone stability assessment around 1,187 immediately placed implants with 1- to 22-year follow-up. Int. J. Oral Maxillofac. Implant. 2013, 28, 605–612. [Google Scholar] [CrossRef] [PubMed]
- Wagenberg, B.; Froum, S.J. Long-Term Bone Stability around 312 Rough-Surfaced Immediately Placed Implants with 2-12-Year Follow-Up. Clin. Implant. Dent. Relat. Res. 2015, 17, 658–666. [Google Scholar] [CrossRef]
- Wilson, T.G., Jr.; Carnio, J.; Schenk, R.; Cochran, D. Immediate implants covered with connective tissue membranes: Human biopsies. J. Periodontol. 2003, 74, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Wychowanski, P.; Wolinski, J.; Kacprzak, M.; Tomkiewicz, W.; Bartlomiej, I.; Szubinska-Lelonkiewicz, D.; Wojtowicz, A.; Nevins, M. Immediate Palatal Molar Implants: A Simple, Safe, Minimally Invasive Technique. Int. J. Periodontics Restor. Dent. 2017, 37, e297–e301. [Google Scholar] [CrossRef]
- Aguilar-Salvatierra, A.; Calvo-Guirado, J.L.; González-Jaranay, M.; Moreu, G.; Delgado-Ruiz, R.A.; Gómez-Moreno, G. Peri-implant evaluation of immediately loaded implants placed in esthetic zone in patients with diabetes mellitus type 2: A two-year study. Clin. Oral Implant. Res. 2016, 27, 156–161. [Google Scholar] [CrossRef]
- Amato, F.; Polara, G. Immediate Implant Placement in Single-Tooth Molar Extraction Sockets: A 1-to 6-Year Retrospective Clinical Study. Int. J. Periodontics Restor. Dent. 2018, 38, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Arora, H.; Ivanovski, S. Correlation between pre-operative buccal bone thickness and soft tissue changes around immediately placed and restored implants in the maxillary anterior region: A 2-year prospective study. Clin. Oral Implant. Res. 2017, 28, 1188–1194. [Google Scholar] [CrossRef]
- Arora, H.; Ivanovski, S. Clinical and aesthetic outcomes of immediately placed single-tooth implants with immediate vs. delayed restoration in the anterior maxilla: A retrospective cohort study. Clin. Oral Implant. Res. 2018, 29, 346–352. [Google Scholar] [CrossRef]
- Arora, H.; Ivanovski, S. Evaluation of the influence of implant placement timing on the esthetic outcomes of single tooth implant treatment in the anterior maxilla: A retrospective study. J. Esthet. Restor. Dent. 2018, 30, 338–345. [Google Scholar] [CrossRef]
- Arora, H.; Ivanovski, S. Immediate and early implant placement in single-tooth gaps in the anterior maxilla: A prospective study on ridge dimensional, clinical, and aesthetic changes. Clin. Oral Implant. Res. 2018, 29, 1143–1154. [Google Scholar] [CrossRef] [PubMed]
- Arora, H.; Khzam, N.; Roberts, D.; Bruce, W.L.; Ivanovski, S. Immediate implant placement and restoration in the anterior maxilla: Tissue dimensional changes after 2–5 year follow up. Clin. Implant. Dent. Istry Relat. Res. 2017, 19, 694–702. [Google Scholar] [CrossRef] [PubMed]
- Atalay, B.; Öncü, B.; Emes, Y.; Bultan, Ö.; Aybar, B.; Yalçin, S. Immediate implant placement without bone grafting: A retrospective study of 110 cases with 5 years of follow-up. Implant. Dent. 2013, 22, 360–365. [Google Scholar] [CrossRef] [PubMed]
- Atieh, M.A.; Alsabeeha, N.H.; Duncan, W.J.; de Silva, R.K.; Cullinan, M.P.; Schwass, D.; Payne, A.G. Immediate single implant restorations in mandibular molar extraction sockets: A controlled clinical trial. Clin. Oral Implant. Res. 2013, 24, 484–496. [Google Scholar] [CrossRef]
- Avvanzo, P.; Ciavarella, D.; Avvanzo, A.; Giannone, N.; Carella, M.; Lo Muzio, L. Immediate placement and temporization of implants: Three-to five-year retrospective results. J. Oral Implantol. 2009, 35, 136–142. [Google Scholar] [CrossRef]
- Balaji, P.; Balaji, S.; Ugandhar, P. Immediate implant in single rooted teeth-Study on primary stability and bone formation. Indian J. Dent. Res. 2015, 26, 421. [Google Scholar] [CrossRef]
- Barone, A.; Rispoli, L.; Vozza, I.; Quaranta, A.; Covani, U. Immediate restoration of single implants placed immediately after tooth extraction. J. Periodontol. 2006, 77, 1914–1920. [Google Scholar] [CrossRef] [PubMed]
- Barone, A.; Toti, P.; Quaranta, A.; Derchi, G.; Covani, U. The clinical outcomes of immediate versus delayed restoration procedures on immediate implants: A comparative cohort study for single-tooth replacement. Clin. Implant. Dent. Relat. Res. 2015, 17, 1114–1126. [Google Scholar] [CrossRef]
- Becker, W.; Dahlin, C.; Lekholm, U.; Bergstrom, C.; van Steenberghe, D.; Higuchi, K.; Becker, B.E. Five-year evaluation of implants placed at extraction and with dehiscences and fenestration defects augmented with ePTFE membranes: Results from a prospective multicenter study. Clin. Implant. Dent. Relat. Res. 1999, 1, 27–32. [Google Scholar] [CrossRef]
- Becker, W.; Sennerby, L.; Bedrossian, E.; Becker, B.E.; Lucchini, J.P. Implant stability measurements for implants placed at the time of extraction: A cohort, prospective clinical trial. J. Periodontol. 2005, 76, 391–397. [Google Scholar] [CrossRef]
- Benic, G.I.; Mokti, M.; Chen, C.J.; Weber, H.P.; Hämmerle, C.H.; Gallucci, G.O. Dimensions of buccal bone and mucosa at immediately placed implants after 7 years: A clinical and cone beam computed tomography study. Clin. Oral Implant. Res. 2012, 23, 560–566. [Google Scholar] [CrossRef]
- Berberi, A.N.; Noujeim, Z.N.; Kanj, W.H.; Mearawi, R.J.; Salameh, Z.A. Immediate placement and loading of maxillary single-tooth implants: A 3-year prospective study of marginal bone level. J. Contemp. Dent. Pract. 2014, 15, 202. [Google Scholar] [CrossRef]
- Bianchi, A.E.; Sanfilippo, F. Single-tooth replacement by immediate implant and connective tissue graft: A 1–9-year clinical evaluation. Clin. Oral Implant. Res. 2004, 15, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Blus, C.; Szmukler-Moncler, S. Atraumatic tooth extraction and immediate implant placement with Piezosurgery: Evaluation of 40 sites after at least 1 year of loading. Int. J. Periodontics Restor. Dent. 2010, 30, 355. [Google Scholar]
- Bonnet, F.; Karouni, M.; Antoun, H. Esthetic evaluation of periimplant soft tissue of immediate single-implant placement and provisionalization in the anterior maxilla. Int. J. Esthet. Dent. 2018, 13, 378–392. [Google Scholar]
- Botticelli, D.; Renzi, A.; Lindhe, J.; Berglundh, T. Implants in fresh extraction sockets: A prospective 5-year follow-up clinical study. Clin. Oral Implant. Res. 2008, 19, 1226–1232. [Google Scholar] [CrossRef]
- Brignardello-Petersen, R. Immediately placed and restored single-tooth implants in the anterior maxilla shown to have good esthetic outcomes 1 year after treatment. J. Am. Dent. Assoc. 2017, 148, e103. [Google Scholar] [CrossRef] [PubMed]
- Brown, S.D.; Payne, A.G. Immediately restored single implants in the aesthetic zone of the maxilla using a novel design: 1-year report. Clin. Oral Implant. Res. 2011, 22, 445–454. [Google Scholar] [CrossRef]
- Bruno, V.; O’Sullivan, D.; Badino, M.; Catapano, S. Preserving soft tissue after placing implants in fresh extraction sockets in the maxillary esthetic zone and a prosthetic template for interim crown fabrication: A prospective study. J. Prosthet. Dent. 2014, 111, 195–202. [Google Scholar] [CrossRef]
- Cabello, G.; Rioboo, M.; Fábrega, J.G. Immediate placement and restoration of implants in the aesthetic zone with a trimodal approach: Soft tissue alterations and its relation to gingival biotype. Clin. Oral Implant. Res. 2013, 24, 1094–1100. [Google Scholar] [CrossRef]
- Cafiero, C.; Annibali, S.; Gherlone, E.; Grassi, F.; Gualini, F.; Magliano, A.; Romeo, E.; Tonelli, P.; Lang, N.P.; Salvi, G. Immediate transmucosal implant placement in molar extraction sites: A 12-month prospective multicenter cohort study. Clin. Oral Implant. Res. 2008, 19, 476–482. [Google Scholar] [CrossRef]
- Calvo Guirado, J.L.; Sáez Yuguero, R.; Ferrer Pérez, V.; Moreno Pelluz, A. Immediate anterior implant placement and early loading by provisional acrylic crowns: A prospective study after a one-year follow-up Period. J. Ir. Dent. Assoc. 2002, 48, 43–49. [Google Scholar] [PubMed]
- Calvo-Guirado, J.L.; Gómez-Moreno, G.; Aguilar-Salvatierra, A.; Guardia, J.; Delgado-Ruiz, R.A.; Romanos, G.E. Marginal bone loss evaluation around immediate non-occlusal microthreaded implants placed in fresh extraction sockets in the maxilla: A 3-year study. Clin. Oral Implant. Res. 2015, 26, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Guirado, J.L.; Ortiz-Ruiz, A.J.; López-Marí, L.; Delgado-Ruiz, R.; Maté-Sánchez, J.; Bravo Gonzalez, L.A. Immediate maxillary restoration of single-tooth implants using platform switching for crestal bone preservation: A 12-month study. Int. J. Oral Maxillofac. Implant. 2009, 24, 275–281. [Google Scholar]
- Canullo, L.; Rasperini, G. Preservation of peri-implant soft and hard tissues using platform switching of implants placed in immediate extraction sockets: A proof-of-concept study with 12-to 36-month follow-up. Int. J. Oral Maxillofac. Implant. 2007, 22, 995–1000. [Google Scholar]
- Cardaropoli, D.; Tamagnone, L.; Roffredo, A.; Gaveglio, L. Soft tissue contour changes at immediate postextraction single-tooth implants with immediate restoration: A 12-month prospective cohort study. Int. J. Periodontics Restor. Dent. 2015, 35, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Carlino, P.; Pepe, V.; Pollice, G.; Grassi, F. Immediate transmucosal implant placement in fresh maxillary and mandibular molar extraction sockets: Description of technique and preliminary results. Minerva Stomatol. 2008, 57, 471. [Google Scholar] [PubMed]
- Chaushu, G.; Chaushu, S.; Tzohar, A.; Dayan, D. Immediate loading of single-tooth implants: Immediate versus non-immediate implantation. A clinical report. Int. J. Oral Maxillofac. Implant. 2001, 16, 267–272. [Google Scholar]
- Chen, S.T.; Darby, I.B.; Adams, G.G.; Reynolds, E.C. A prospective clinical study of bone augmentation techniques at immediate implants. Clin. Oral Implant. Res. 2005, 16, 176–184. [Google Scholar] [CrossRef]
- Chen, S.T.; Darby, I.B.; Reynolds, E.C. A prospective clinical study of non-submerged immediate implants: Clinical outcomes and esthetic results. Clin. Oral Implant. Res. 2007, 18, 552–562. [Google Scholar] [CrossRef]
- Chen, Y.; Yuan, S.; Zhou, N.; Man, Y. Transcrestal sinus floor augmentation with immediate implant placement applied in three types of fresh extraction sockets: A clinical prospective study with 1-year follow-up. Clin. Implant. Dent. Relat. Res. 2017, 19, 1034–1043. [Google Scholar] [CrossRef]
- Chung, S.; Rungcharassaeng, K.; Kan, J.Y.K.; Roe, P.; Lozada, J.L. Immediate Single Tooth Replacement with Subepithelial Connective Tissue Graft Using Platform Switching Implants: A Case Series. J. Oral Implantol. 2011, 37, 559–569. [Google Scholar] [CrossRef]
- Cooper, L.F.; Raes, F.; Reside, G.J.; Garriga, J.S.; Tarrida, L.G.; Wiltfang, J.; Kern, M.; de Bruyn, H. Comparison of radiographic and clinical outcomes following immediate provisionalization of single-tooth dental implants placed in healed alveolar ridges and extraction sockets. Int. J. Oral Maxillofac. Implant. 2010, 25, 1222–1232. [Google Scholar]
- Cooper, L.F.; Reside, G.J.; Raes, F.; Garriga, J.S.; Tarrida, L.G.; Wiltfang, J.; Kern, M.; De Bruyn, H. Immediate provisionalization of dental implants placed in healed alveolar ridges and extraction sockets: A 5-year prospective evaluation. Int. J. Oral Maxillofac. Implant. 2014, 29, 709–717. [Google Scholar] [CrossRef] [PubMed]
- Cornelini, R.; Barone, A.; Covani, U. Connective tissue grafts in postextraction implants with immediate restoration: A prospective controlled clinical study. Pract. Proced. Aesthetic Dent. PPAD 2008, 20, 337–343. [Google Scholar] [PubMed]
- Cornelini, R.; Cangini, F.; Covani, U.; Wilson Jr, T.G. Immediate restoration of implants placed into fresh extraction sockets for single-tooth replacement: A prospective clinical study. Int. J. Periodontics Restor. Dent. 2005, 25, 439–447. [Google Scholar] [CrossRef]
- Cosyn, J.; Eghbali, A.; De Bruyn, H.; Collys, K.; Cleymaet, R.; De Rouck, T. Immediate single-tooth implants in the anterior maxilla: 3-year results of a case series on hard and soft tissue response and aesthetics. J. Clin. Periodontol. 2011, 38, 746–753. [Google Scholar] [CrossRef]
- Cosyn, J.; Eghbali, A.; Hanselaer, L.; De Rouck, T.; Wyn, I.; Sabzevar, M.M.; Cleymaet, R.; De Bruyn, H. Four modalities of single implant treatment in the anterior maxilla: A clinical, radiographic, and aesthetic evaluation. Clin. Implant. Dent. Relat. Res. 2013, 15, 517–530. [Google Scholar] [CrossRef]
- Cosyn, J.; Eghbali, A.; Hermans, A.; Vervaeke, S.; De Bruyn, H.; Cleymaet, R. A 5-year prospective study on single immediate implants in the aesthetic zone. J. Clin. Periodontol. 2016, 43, 702–709. [Google Scholar] [CrossRef]
- Covani, U.; Canullo, L.; Toti, P.; Alfonsi, F.; Barone, A. Tissue stability of implants placed in fresh extraction sockets: A 5-year prospective single-cohort study. J. Periodontol. 2014, 85, e323–e332. [Google Scholar] [CrossRef]
- Covani, U.; Chiappe, G.; Bosco, M.; Orlando, B.; Quaranta, A.; Barone, A. A 10-year evaluation of implants placed in fresh extraction sockets: A prospective cohort study. J. Periodontol. 2012, 83, 1226–1234. [Google Scholar] [CrossRef] [PubMed]
- Covani, U.; Marconcini, S.; Galassini, G.; Cornelini, R.; Santini, S.; Barone, A. Connective tissue graft used as a biologic barrier to cover an immediate implant. J. Periodontol. 2007, 78, 1644–1649. [Google Scholar] [CrossRef] [PubMed]
- Crespi, R.; Capparé, P.; Crespi, G.; Lo Giudice, G.; Gastaldi, G.; Gherlone, E. Immediate implant placement in sockets with asymptomatic apical periodontitis. Clin. Implant. Dent. Relat. Res. 2017, 19, 20–27. [Google Scholar] [CrossRef]
- Crespi, R.; Capparè, P.; Polizzi, E.; Gherlone, E. Fresh-Socket Implants of Different Collar Length: Clinical Evaluation in the Aesthetic Zone. Clin. Implant. Dent. Relat. Res. 2015, 17, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Cristalli, M.P.; Marini, R.; La Monaca, G.; Sepe, C.; Tonoli, F.; Annibali, S. Immediate loading of post-extractive single-tooth implants: A 1-year prospective study. Clin. Oral Implant. Res. 2015, 26, 1070–1079. [Google Scholar] [CrossRef]
- De Bruyn, H.; Raes, F.; Cooper, L.F.; Reside, G.; Garriga, J.S.; Tarrida, L.G.; Wiltfang, J.; Kern, M. Three-years clinical outcome of immediate provisionalization of single Osseospeed™ implants in extraction sockets and healed ridges. Clin. Oral Implant. Res. 2013, 24, 217–223. [Google Scholar] [CrossRef]
- de Carvalho, B.C.F.; de Carvalho, E.M.O.F.; Xediek Consani, R.L. Flapless single-tooth immediate implant placement. Int. J. Oral Maxillofac. Implant. 2013, 2, 783–789. [Google Scholar] [CrossRef] [PubMed]
- De Kok, I.J.; Chang, S.S.; Moriarty, J.D.; Cooper, L.F. A retrospective analysis of peri-implant tissue responses at immediate load/provisionalized microthreaded implants. Int. J. Oral Maxillofac. Implant. 2006, 21, 405–412. [Google Scholar]
- De Rouck, T.; Collys, K.; Cosyn, J. Immediate single-tooth implants in the anterior maxilla: A 1-year case cohort study on hard and soft tissue response. J. Clin. Periodontol. 2008, 35, 649–657. [Google Scholar] [CrossRef]
- Degidi, M.; Daprile, G.; Nardi, D.; Piattelli, A. Buccal bone plate in immediately placed and restored implant with Bio-Oss® collagen graft: A 1-year follow-up study. Clin. Oral Implant. Res. 2013, 24, 1201–1205. [Google Scholar] [CrossRef] [PubMed]
- Degidi, M.; Daprile, G.; Nardi, D.; Piattelli, A. Immediate Provisionalization of Implants Placed in Fresh Extraction Sockets Using a Definitive Abutment: The Chamber Concept. Int. J. Periodontics Restor. Dent. 2013, 33, 559–565. [Google Scholar] [CrossRef] [PubMed]
- Degidi, M.; Nardi, D.; Daprile, G.; Piattelli, A. Buccal bone plate in the immediately placed and restored maxillary single implant: A 7-year retrospective study using computed tomography. Implant. Dent. 2012, 21, 62–66. [Google Scholar] [CrossRef]
- Degidi, M.; Nardi, D.; Piattelli, A. Peri-implant tissue and radiographic bone levels in the immediately restored single-tooth implant: A retrospective analysis. J. Periodontol. 2008, 79, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Di Alberti, L.; Donnini, F.; Di Alberti, C.; Camerino, M.; Sgaramella, N.; Lo Muzio, L. Clinical and radiologic evaluation of 70 immediately loaded single implants in the maxillary esthetic zone: Preliminary results after 1 year of functional loading. Int. J. Oral Maxillofac. Implant. 2012, 27, 181–186. [Google Scholar]
- Evans, C.D.; Chen, S.T. Esthetic outcomes of immediate implant placements. Clin. Oral Implant. Res. 2008, 19, 73–80. [Google Scholar] [CrossRef]
- Fagan, M.C.; Owens, H.; Smaha, J.; Kao, R.T. Simultaneous hard and soft tissue augmentation for implants in the esthetic zone: Report of 37 consecutive cases. J. Periodontol. 2008, 79, 1782–1788. [Google Scholar] [CrossRef]
- Ferrara, A.; Galli, C.; Mauro, G.; Macaluso, G.M. Immediate provisional restoration of postextraction implants for maxillary single-tooth replacement. Int. J. Periodontics Restor. Dent. 2006, 26, 371–377. [Google Scholar]
- Fugazzotto, P. A retrospective analysis of immediately placed implants in 418 sites exhibiting periapical pathology: Results and clinical considerations. Int. J. Oral Maxillofac. Implant. 2012, 27, 194–202. [Google Scholar]
- Fugazzotto, P.A. A retrospective analysis of implants immediately placed in sites with and without periapical pathology in sixty-four patients. J. Periodontol. 2012, 83, 182–186. [Google Scholar] [CrossRef]
- Fürhauser, R.; Mailath-Pokorny, G.; Haas, R.; Busenlechner, D.; Watzek, G.; Pommer, B. Immediate Restoration of Immediate Implants in the Esthetic Zone of the Maxilla Via the Copy-Abutment Technique: 5-Year Follow-Up of Pink Esthetic Scores. Clin. Implant. Dent. Relat. Res. 2017, 19, 28–37. [Google Scholar] [CrossRef]
- Ganeles, J.; Norkin, F.J.; Zfaz, S. Single-Tooth Implant Restorations in Fresh Extraction Sockets of the Maxillary Esthetic Zone: Two-Year Results of a Prospective Cohort Study. Int. J. Periodontics Restor. Dent. 2017, 37, e154–e162. [Google Scholar] [CrossRef] [PubMed]
- Garber, D.A.; Salama, M.; Salama, H. Immediate total tooth replacement. Compend. Contin. Educ. Dent. 2001, 22, 210–216. [Google Scholar] [PubMed]
- Goldstein, M.; Boyan, B.D.; Schwartz, Z. The palatal advanced flap: A pedicle flap for primary coverage of immediately placed implants. Clin. Oral Implant. Res. 2002, 13, 644–650. [Google Scholar] [CrossRef] [PubMed]
- Grandi, T.; Garuti, G.; Samarani, R.; Guazzi, P.; Forabosco, A. Immediate loading of single post-extractive implants in the anterior maxilla: 12-month results from a multicenter clinical study. J. Oral Implantol. 2012, 38, 477–484. [Google Scholar] [CrossRef]
- Grandi, T.; Guazzi, P.; Samarani, R.; Grandi, G. Immediate provisionalisation of single post-extractive implants versus implants placed in healed sites in the anterior maxilla: 1-year results from a multicentre controlled cohort study. Eur. J. Oral Implantol. 2013, 6, 285–295. [Google Scholar]
- Guarnieri, R.; Belleggia, F.; Grande, M. Immediate versus delayed treatment in the anterior maxilla using single implants with a laser-microtextured collar: 3-year results of a case series on hard-and soft-tissue response and esthetics. J. Prosthodont. 2016, 25, 135–145. [Google Scholar] [CrossRef]
- Guarnieri, R.; Ceccherini, A.; Grande, M. Single-tooth replacement in the anterior maxilla by means of immediate implantation and early loading: Clinical and aesthetic results at 5 years. Clin. Implant. Dent. Relat. Res. 2015, 17, 314–326. [Google Scholar] [CrossRef]
- Guarnieri, R.; Placella, R.; Testarelli, L.; Iorio-Siciliano, V.; Grande, M. Clinical, radiographic, and esthetic evaluation of immediately loaded laser microtextured implants placed into fresh extraction sockets in the anterior maxilla: A 2-year retrospective multicentric study. Implant. Dent. 2014, 23, 144. [Google Scholar] [CrossRef]
- Hartlev, J.; Kohberg, P.; Ahlmann, S.; Andersen, N.T.; Schou, S.; Isidor, F. Patient satisfaction and esthetic outcome after immediate placement and provisionalization of single-tooth implants involving a definitive individual abutment. Clin. Oral Implant. Res. 2014, 25, 1245–1250. [Google Scholar] [CrossRef]
- Hartlev, J.; Kohberg, P.; Ahlmann, S.; Gotfredsen, E.; Andersen, N.T.; Isidor, F.; Schou, S. Immediate placement and provisionalization of single-tooth implants involving a definitive individual abutment: A clinical and radiographic retrospective study. Clin. Oral Implant. Res. 2013, 24, 652–658. [Google Scholar] [CrossRef]
- Hassan, K.S.; Kassim, A.; Al Ogaly, A.-U.R. A comparative evaluation of immediate dental implant with autogenous versus synthetic guided bone regeneration. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2008, 106, e8–e15. [Google Scholar] [CrossRef]
- Hattingh, A.; Hommez, G.; De Bruyn, H.; Huyghe, M.; Vandeweghe, S. A prospective study on ultra-wide diameter dental implants for immediate molar replacement. Clin. Implant. Dent. Relat. Res. 2018, 20, 1009–1015. [Google Scholar] [CrossRef] [PubMed]
- Hof, M.; Pommer, B.; Ambros, H.; Jesch, P.; Vogl, S.; Zechner, W. Does timing of implant placement affect implant therapy outcome in the aesthetic zone? A clinical, radiological, aesthetic, and patient-based evaluation. Clin. Implant. Dent. Relat. Res. 2015, 17, 1188–1199. [Google Scholar] [CrossRef] [PubMed]
- Hu, C.; Gong, T.; Lin, W.; Yuan, Q.; Man, Y. Immediate implant placement into posterior sockets with or without buccal bone dehiscence defects: A retrospective cohort study. J. Dent. 2017, 65, 95–100. [Google Scholar] [CrossRef]
- Hui, E.; Chow, J.; Li, D.; Liu, J.; Wat, P.; Law, H. Immediate provisional for single-tooth implant replacement with Brånemark system: Preliminary report. Clin. Implant. Dent. Relat. Res. 2001, 3, 79–86. [Google Scholar] [CrossRef]
- Jiansheng, H.; Dongying, X.; Xianfeng, W.; Baoyi, X.; Qiong, L.; Jincai, Z. Clinical evaluation of short and wide-diameter implants immediately placed into extraction sockets of posterior areas: A 2-year retrospective study. J. Oral Implantol. 2012, 38, 729–737. [Google Scholar] [CrossRef] [PubMed]
- Juodzbalys, G.; Wang, H.-L. Socket Morphology--Based Treatment for Implant Esthetics: A Pilot Study. Int. J. Oral Maxillofac. Implant. 2010, 25, 970–978. [Google Scholar]
- Juodzbalys, G.; Wang, H.L. Soft and hard tissue assessment of immediate implant placement: A case series. Clin. Oral Implant. Res. 2007, 18, 237–243. [Google Scholar] [CrossRef]
- Kahnberg, K.-E. Immediate implant placement in fresh extraction sockets: A clinical report. Int. J. Oral Maxillofac. Implant. 2009, 24, 282–288. [Google Scholar]
- Kan, J.Y.; Rungcharassaeng, K.; Liddelow, G.; Henry, P.; Goodacre, C.J. Periimplant tissue response following immediate provisional restoration of scalloped implants in the esthetic zone: A one-year pilot prospective multicenter study. J. Prosthet. Dent. 2007, 97, S109–S118. [Google Scholar] [CrossRef]
- Kan, J.Y.; Rungcharassaeng, K.; Lozada, J.L.; Zimmerman, G. Facial gingival tissue stability following immediate placement and provisionalization of maxillary anterior single implants: A 2-to 8-year follow-up. Int. J. Oral Maxillofac. Implant. 2011, 26, 179–187. [Google Scholar]
- Kan, J.Y.; Rungcharassaeng, K.; Morimoto, T.; Lozada, J. Facial gingival tissue stability after connective tissue graft with single immediate tooth replacement in the esthetic zone: Consecutive case report. J. Oral Maxillofac. Surg. 2009, 67, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Kan, J.Y.; Rungcharassaeng, K.; Sclar, A.; Lozada, J.L. Effects of the facial osseous defect morphology on gingival dynamics after immediate tooth replacement and guided bone regeneration: 1-year results. J. Oral Maxillofac. Surg. 2007, 65, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Kan, J.Y.; Rungcharassaeng, K.; Umezu, K.; Kois, J.C. Dimensions of peri-implant mucosa: An evaluation of maxillary anterior single implants in humans. J. Periodontol. 2003, 74, 557–562. [Google Scholar] [CrossRef]
- Khzam, N.; Mattheos, N.; Roberts, D.; Bruce, W.L.; Ivanovski, S. Immediate placement and restoration of dental implants in the esthetic region: Clinical case series. J. Esthet. Restor. Dent. 2014, 26, 332–344. [Google Scholar] [CrossRef]
- Koirala, D.P.; Singh, S.V.; Chand, P.; Siddharth, R.; Jurel, S.K.; Aggarwal, H.; Tripathi, S.; Ranabhatt, R.; Mehrotra, D. Early loading of delayed versus immediately placed implants in the anterior mandible: A pilot comparative clinical study. J. Prosthet. Dent. 2016, 116, 340–345. [Google Scholar] [CrossRef]
- Kolerman, R.; Mijiritsky, E.; Barnea, E.; Dabaja, A.; Nissan, J.; Tal, H. Esthetic Assessment of Implants Placed into Fresh Extraction Sockets for Single-Tooth Replacements Using a Flapless Approach. Clin. Implant. Dent. Relat. Res. 2017, 19, 351–364. [Google Scholar] [CrossRef]
- Kolerman, R.; Nissan, J.; Mijiritsky, E.; Hamoudi, N.; Mangano, C.; Tal, H. Esthetic assessment of immediately restored implants combined with GBR and free connective tissue graft. Clin. Oral Implant. Res. 2016, 27, 1414–1422. [Google Scholar] [CrossRef]
- Kolerman, R.; Nissan, J.; Rahmanov, A.; Zenziper, E.; Slutzkey, S.; Tal, H. Radiological and biological assessment of immediately restored anterior maxillary implants combined with GBR and free connective tissue graft. Clin. Implant. Dent. Relat. Res. 2016, 18, 1142–1152. [Google Scholar] [CrossRef]
- Kuchler, U.; Chappuis, V.; Gruber, R.; Lang, N.P.; Salvi, G.E. Immediate implant placement with simultaneous guided bone regeneration in the esthetic zone: 10-year clinical and radiographic outcomes. Clin. Oral Implant. Res. 2016, 27, 253–257. [Google Scholar] [CrossRef]
- Lee, Y.-M.; Kim, D.-Y.; Kim, J.Y.; Kim, S.-H.; Koo, K.-T.; Kim, T.-I.; Seol, Y.-J. Peri-implant soft tissue level secondary to a connective tissue graft in conjunction with immediate implant placement: A 2-year follow-up report of 11 consecutive cases. Int. J. Periodontics Restor. Dent. 2012, 32, 213–222. [Google Scholar]
- Li, P.; Zhu, H.; Huang, D. Autogenous DDM versus Bio-Oss granules in GBR for immediate implantation in periodontal postextraction sites: A prospective clinical study. Clin. Implant. Dent. Relat. Res. 2018, 20, 923–928. [Google Scholar] [CrossRef] [PubMed]
- Lindeboom, J.A.; Tjiook, Y.; Kroon, F.H. Immediate placement of implants in periapical infected sites: A prospective randomized study in 50 patients. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2006, 101, 705–710. [Google Scholar] [CrossRef]
- Locante, W.M. Single-tooth replacements in the esthetic zone with an immediate function implant: A preliminary report. J. Oral Implantol. 2004, 30, 369–375. [Google Scholar] [CrossRef]
- Lops, D.; Romeo, E.; Chiapasco, M.; Procopio, R.M.; Oteri, G. Behaviour of soft tissues healing around single bone-level-implants placed immediately after tooth extraction A 1 year prospective cohort study. Clin. Oral Implant. Res. 2013, 24, 1206–1213. [Google Scholar] [CrossRef] [PubMed]
- Lorenzoni, M.; Pertl, C.; Zhang, K.; Wimmer, G.; Wegscheider, W.A. Immediate loading of single-tooth implants in the anterior maxilla. Preliminary results after one year. Clin. Oral Implant. Res. 2003, 14, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud Aly, T.; Mohamed Arafat, S. Immediate loading of implants placed into fresh extraction sockets with periapical lesions without augmentation. Smile Dent. J. 2008, 3, 6–22. [Google Scholar]
- Malchiodi, L.; Cucchi, A.; Ghensi, P.; Nocini, P.F. Evaluation of the esthetic results of 64 nonfunctional immediately loaded postextraction implants in the maxilla: Correlation between interproximal alveolar crest and soft tissues at 3 years of follow-up. Clin. Implant. Dent. Relat. Res. 2013, 15, 130–142. [Google Scholar] [CrossRef] [PubMed]
- Malchiodi, L.; Scarano, A.; Corrocher, G.; Trevisiol, L.; Quaranta, A.; Gerosa, R. Experimental study of a new surgical technique for anatomic remodeling of atrophic socket in maxillary postextraction single implant. Minerva Stomatol. 2008, 57, 519–528. [Google Scholar]
- Mangano, F.; Mangano, C.; Ricci, M.; Sammons, R.L.; Shibli, J.A.; Piattelli, A. Single-tooth Morse taper connection implants placed in fresh extraction sockets of the anterior maxilla: An aesthetic evaluation. Clin. Oral Implant. Res. 2012, 23, 1302–1307. [Google Scholar] [CrossRef]
- Mangano, F.G.; De Franco, M.; Caprioglio, A.; Macchi, A.; Piattelli, A.; Mangano, C. Immediate, non-submerged, root-analogue direct laser metal sintering (DLMS) implants: A 1-year prospective study on 15 patients. Lasers Med. Sci. 2014, 29, 1321–1328. [Google Scholar] [CrossRef] [PubMed]
- Mangano, F.G.; Mangano, C.; Ricci, M.; Sammons, R.L.; Shibli, J.A.; Piattelli, A. Esthetic evaluation of single-tooth Morse taper connection implants placed in fresh extraction sockets or healed sites. J. Oral Implantol. 2013, 39, 172–181. [Google Scholar] [CrossRef] [PubMed]
- Mangano, F.G.; Mastrangelo, P.; Luongo, F.; Blay, A.; Tunchel, S.; Mangano, C. Aesthetic outcome of immediately restored single implants placed in extraction sockets and healed sites of the anterior maxilla: A retrospective study on 103 patients with 3 years of follow-up. Clin. Oral Implant. Res. 2017, 28, 272–282. [Google Scholar] [CrossRef] [PubMed]
- Mijiritsky, E.; Mardinger, O.; Mazor, Z.; Chaushu, G. Immediate provisionalization of single-tooth implants in fresh-extraction sites at the maxillary esthetic zone: Up to 6 years of follow-up. Implant. Dent. 2009, 18, 326–333. [Google Scholar] [CrossRef]
- Montoya-Salazar, V.; Castillo-Oyagüe, R.; Torres-Sánchez, C.; Lynch, C.D.; Gutiérrez-Pérez, J.-L.; Torres-Lagares, D. Outcome of single immediate implants placed in post-extraction infected and non-infected sites, restored with cemented crowns: A 3-year prospective study. J. Dent. 2014, 42, 645–652. [Google Scholar] [CrossRef]
- Morimoto, T.; Tsukiyama, Y.; Morimoto, K.; Koyano, K. Facial bone alterations on maxillary anterior single implants for immediate placement and provisionalization following tooth extraction: A superimposed cone beam computed tomography study. Clin. Oral Implant. Res. 2015, 26, 1383–1389. [Google Scholar] [CrossRef]
- Noelken, R.; Kunkel, M.; Wagner, W. Immediate implant placement and provisionalization after long-axis root fracture and complete loss of the facial bony lamella. Int. J. Periodontics Restor. Dent. 2011, 31, 175. [Google Scholar]
- Noelken, R.; Moergel, M.; Pausch, T.; Kunkel, M.; Wagner, W. Clinical and esthetic outcome with immediate insertion and provisionalization with or without connective tissue grafting in presence of mucogingival recessions: A retrospective analysis with follow-up between 1 and 8 years. Clin. Implant. Dent. Relat. Res. 2018, 20, 285–293. [Google Scholar] [CrossRef]
- Norton, M.R. A short-term clinical evaluation of immediately restored maxillary TiOblast single-tooth implants. Int. J. Oral Maxillofac. Implant. 2004, 19, 1333–1343. [Google Scholar]
- Norton, M.R. The influence of insertion torque on the survival of immediately placed and restored single-tooth implants. Int. J. Oral Maxillofac. Implant. 2011, 26, 1333–1343. [Google Scholar]
- Ormianer, Z.; Schiroli, G. Maxillary single-tooth replacement utilizing a novel ceramic restorative system: Results to 30 months. J. Oral Implantol. 2006, 32, 190–199. [Google Scholar] [CrossRef] [PubMed]
- Paul, S.; Held, U. Immediate supracrestal implant placement with immediate temporization in the anterior dentition: A retrospective study of 31 implants in 26 patients with up to 5.5-years follow-up. Clin. Oral Implant. Res. 2013, 24, 710–717. [Google Scholar] [CrossRef] [PubMed]
- Peñarrocha-Diago, M.; Carrillo-Garcîa, C.; Boronat-Lopez, A.; García-Mira, B. Comparative study of wide-diameter implants placed after dental extraction and implants positioned in mature bone for molar replacement. Int. J. Oral Maxillofac. Implant. 2008, 23, 497–501. [Google Scholar]
- Perrotti, V.; Vozza, I.; Tumedei, M.; Pompa, G.; Iaculli, F.; Quaranta, A. Rehabilitation of Postextractive Socket in the Premaxilla: A 12-Year Study on 27 Titanium Plasma Spray Resorbable Calcium Phosphate Coated Single Implants. Implant. Dent.istry 2018, 27, 452–460. [Google Scholar] [CrossRef] [PubMed]
- Prosper, L.; Crespi, R.; Valenti, E.; Capparé, P.; Gherlone, E. Five-year follow-up of wide-diameter implants placed in fresh molar extraction sockets in the mandible: Immediate versus delayed loading. Int. J. Oral Maxillofac. Implant. 2010, 25, 607–612. [Google Scholar]
- Quaranta, A.; Perrotti, V.; Putignano, A.; Malchiodi, L.; Vozza, I.; Guirado, J.L.C. Anatomical remodeling of buccal bone plate in 35 premaxillary post-extraction immediately restored single TPS implants: 10-year radiographic investigation. Implant. Dent. 2016, 25, 186–192. [Google Scholar] [CrossRef]
- Raes, F.; Cooper, L.F.; Tarrida, L.G.; Vandromme, H.; De Bruyn, H. A case-control study assessing oral-health-related quality of life after immediately loaded single implants in healed alveolar ridges or extraction sockets. Clin. Oral Implant. Res. 2012, 23, 602–608. [Google Scholar] [CrossRef]
- Raes, F.; Cosyn, J.; Crommelinck, E.; Coessens, P.; De Bruyn, H. Immediate and conventional single implant treatment in the anterior maxilla: 1-year results of a case series on hard and soft tissue response and aesthetics. J. Clin. Periodontol. 2011, 38, 385–394. [Google Scholar] [CrossRef]
- Raes, F.; Cosyn, J.; De Bruyn, H. Clinical, aesthetic, and patient-related outcome of immediately loaded single implants in the anterior maxilla: A prospective study in extraction sockets, healed ridges, and grafted sites. Clin. Implant. Dent. Istry Relat. Res. 2013, 15, 819–835. [Google Scholar] [CrossRef]
- Raes, S.; Cosyn, J.; Noyelle, A.; Raes, F.; De Bruyn, H. Clinical Outcome After 8 to 10 Years of Immediately Restored Single Implants Placed in Extraction Sockets and Healed Ridges. Int. J. Periodontics Restor. Dent. 2018, 38, 337–345. [Google Scholar] [CrossRef]
- Ribeiro, F.S.; Pontes, A.E.F.; Marcantonio, E.; Piattelli, A.; Neto, R.J.B.; Marcantonio Jr, E. Success rate of immediate nonfunctional loaded single-tooth implants: Immediate versus delayed implantation. Implant. Dent. 2008, 17, 109–117. [Google Scholar] [CrossRef]
- Rodrigo, D.; Martin, C.; Sanz, M. Biological complications and peri-implant clinical and radiographic changes at immediately placed dental implants. A prospective 5-year cohort study. Clin. Oral Implant. Res. 2012, 23, 1224–1231. [Google Scholar] [CrossRef] [PubMed]
- Roe, P.; Kan, J.Y.; Rungcharassaeng, K.; Caruso, J.M.; Zimmerman, G.; Mesquida, J. Horizontal and vertical dimensional changes of peri-implant facial bone following immediate placement and provisionalization of maxillary anterior single implants: A 1-year cone beam computed tomography study. Int. J. Oral Maxillofac. Implant. 2012, 27, 393–400. [Google Scholar]
- Romeo, E.; Lops, D.; Rossi, A.; Storelli, S.; Rozza, R.; Chiapasco, M. Surgical and prosthetic management of interproximal region with single-implant restorations: 1-year prospective study. J. Periodontol. 2008, 79, 1048–1055. [Google Scholar] [CrossRef]
- Carlos Martins da Rosa, J.; Cristina Pértile de Oliveira Rosa, A.; Eduardo Francischone, C.; Salles Sotto-Maior, B. Esthetic outcomes and tissue stability of implant placement in compromised sockets following immediate dentoalveolar restoration: Results of a prospective case series at 58 months follow-up. Int. J. Periodontics Restor. Dent. 2014, 34, 198–208. [Google Scholar] [CrossRef]
- Ross, S.B.; Pette, G.A.; Parker, W.B.; Hardigan, P. Gingival margin changes in maxillary anterior sites after single immediate implant placement and provisionalization: A 5-year retrospective study of 47 patients. Int. J. Oral Maxillofac. Implant. 2014, 29, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Saito, H.; Chu, S.J.; Zamzok, J.; Brown, M.; Smith, R.; Sarnachiaro, G.; Hochman, M.; Fletcher, P.; Reynolds, M.A.; Tarnow, D.P. Flapless Postextraction Socket Implant Placement: The Effects of a Platform Switch-Designed Implant on Peri-implant Soft Tissue Thickness—A Prospective Study. Int. J. Periodontics Restor. Dent. 2018, 38, s9–s15. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Cecchinato, D.; Ferrus, J.; Salvi, G.E.; Ramseier, C.; Lang, N.P.; Lindhe, J. Implants placed in fresh extraction sockets in the maxilla: Clinical and radiographic outcomes from a 3-year follow-up examination. Clin. Oral Implant. Res. 2014, 25, 321–327. [Google Scholar] [CrossRef]
- Sato, R.K.; Thomé, G.; Fontão, F.N.G.; de Melo Filho, A.; Melo, A.C.M. Morse Taper Implants Immediately Loaded in Fresh Extraction Sockets: A Prospective Cohort Study. Implant. Dent. 2017, 26, 345–350. [Google Scholar] [CrossRef]
- Schwartz-Arad, D.; Grossman, Y.; Chaushu, G. The clinical effectiveness of implants placed immediately into fresh extraction sites of molar teeth. J. Periodontol. 2000, 71, 839–844. [Google Scholar] [CrossRef]
- Shibly, O.; Kutkut, A.; Albandar, J.M. One-year re-entry results of guided bone regeneration around immediately placed implants with immediate or conventional loading: A case series. J. Int. Acad. Periodontol. 2012, 14, 62–68. [Google Scholar]
- Siciliano, V.I.; Salvi, G.E.; Matarasso, S.; Cafiero, C.; Blasi, A.; Lang, N.P. Soft tissues healing at immediate transmucosal implants placed into molar extraction sites with buccal self-contained dehiscences. A 12-month controlled clinical trial. Clin. Oral Implant. Res. 2009, 20, 482–488. [Google Scholar] [CrossRef]
- Siegenthaler, D.W.; Jung, R.E.; Holderegger, C.; Roos, M.; Hämmerle, C.H. Replacement of teeth exhibiting periapical pathology by immediate implants. A prospective, controlled clinical trial. Clin. Oral Implant. Res. 2007, 18, 727–737. [Google Scholar] [CrossRef] [PubMed]
- Soardi, C.M.; Bianchi, A.E.; Zandanel, E.; Spinato, S. Clinical and radiographic evaluation of immediately loaded one-piece implants placed into fresh extraction sockets. Quintessence Int. 2012, 43, 449–456. [Google Scholar] [PubMed]
- Spinato, S.; Agnini, A.; Chiesi, M.; Agnini, A.M.; Wang, H.L. Comparison between graft and no-graft in an immediate placed and immediate nonfunctional loaded implant. Implant. Dent. 2012, 21, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Steigmann, M.; Wang, H.L. Esthetic buccal flap for correction of buccal fenestration defects during flapless immediate implant surgery. J. Periodontol. 2006, 77, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Takeshita, K.; Vandeweghe, S.; Vervack, V.; Sumi, T.; Bruyn, H.D.; Jimbo, R. Immediate Implant Placement and Loading of Single Implants in the Esthetic Zone: Clinical Outcome and Esthetic Evaluation in a Japanese Population. Int. J. Periodontics Restor. Dent. 2015, 35, 715–723. [Google Scholar] [CrossRef]
- Tarnow, D.P.; Chu, S.J.; Salama, M.A.; Stappert, C.F.; Salama, H.; Garber, D.A.; Sarnachiaro, G.O.; Sarnachiaro, E.; Luis Gotta, S.; Saito, H. Flapless postextraction socket implant placement in the esthetic zone: Part 1. The effect of bone grafting and/or provisional restoration on facial-palatal ridge dimensional change-a retrospective cohort study. Int. J. Periodontics Restor. Dent. 2014, 34, 322–331. [Google Scholar] [CrossRef]
- Tortamano, P.; Otávio Alves Camargo, L.; Stella Bello-Silva, M.; Hirokuni Kanashiro, L. Immediate implant placement and restoration in the esthetic zone: A prospective study with 18 months of follow-up. Int. J. Oral Maxillofac. Implant. 2010, 25, 345–350. [Google Scholar]
- Truninger, T.C.; Philipp, A.O.; Siegenthaler, D.W.; Roos, M.; Hämmerle, C.H.; Jung, R.E. A prospective, controlled clinical trial evaluating the clinical and radiological outcome after 3 years of immediately placed implants in sockets exhibiting periapical pathology. Clin. Oral Implant. Res. 2011, 22, 20–27. [Google Scholar] [CrossRef]
- Tsirlis, A.T. Clinical evaluation of immediate loaded upper anterior single implants. Implant. Dent. 2005, 14, 94–103. [Google Scholar] [CrossRef] [PubMed]
- Tsuda, H.; Rungcharassaeng, K.; Kan, J.Y.; Roe, P.; Lozada, J.L.; Zimmerman, G. Peri-implant tissue response following connective tissue and bone grafting in conjunction with immediate single-tooth replacement in the esthetic zone: A case series. Int. J. Oral Maxillofac. Implant. 2011, 26, 427. [Google Scholar]
- Valentini, P.; Abensur, D.; Albertini, J.F.; Rocchesani, M. Immediate Provisionalization of Single Extraction-Site Implants in the Esthetic Zone: A Clinical Evaluation. Int. J. Periodontics Restor. Dent. 2010, 30, 41. [Google Scholar]
- Velasco-Ortega, E.; Wojtovicz, E.; España-Lopez, A.; Jimenez-Guerra, A.; Monsalve-Guil, L.; Ortiz-Garcia, I.; Serrera-Figallo, M.-A. Survival rates and bone loss after immediate loading of implants in fresh extraction sockets (single gaps). A clinical prospective study with 4 year follow-up. Med. Oral Patol. Oral Y Cir. Bucal 2018, 23, e230. [Google Scholar] [CrossRef]
- Parithimarkalaignan, S.; Padmanabhan, T.V. Osseointegration: An update. J. Indian Prosthodont. Soc. 2013, 13, 2–6. [Google Scholar] [CrossRef]
- Levin, L. Dealing with dental implant failures. J. Appl. Oral Sci. 2008, 16, 171–175. [Google Scholar] [CrossRef]
- Waasdorp, J.A.; Evian, C.I.; Mandracchia, M. Immediate Placement of Implants Into Infected Sites: A Systematic Review of the Literature. J. Periodontol. 2010, 81, 801–808. [Google Scholar] [CrossRef] [PubMed]
- Levin, L.; Schwartz-Arad, D. The effect of cigarette smoking on dental implants and related surgery. Implant. Dent. 2006, 14, 357–361. [Google Scholar] [CrossRef] [PubMed]
- Alsaadi, G.; Quirynen, M.; Komárek, A.; van Steenberghe, D. Impact of local and systemic factors on the incidence of late oral implant loss. Clin. Oral Implant. Res. 2008, 19, 670–676. [Google Scholar] [CrossRef]
- Zhu, Y.; Zheng, X.; Zeng, G.; Xu, Y.; Qu, X.; Zhu, M.; Lu, E. Clinical efficacy of early loading versus conventional loading of dental implants. Sci. Rep. 2015, 5, 15995. [Google Scholar] [CrossRef]
- Testori, T.; Zuffetti, F.; Capelli, M.; Galli, F.; Weinstein, R.L.; Del Fabbro, M. Immediate versus conventional loading of post-extraction implants in the edentulous jaws. Clin. Implant. Dent. Relat. Res. 2014, 16, 926–935. [Google Scholar] [CrossRef] [PubMed]
- Del Fabbro, M.; Ceresoli, V.; Taschieri, S.; Ceci, C.; Testori, T. Immediate loading of postextraction implants in the esthetic area: Systematic review of the literature. Clin. Implant. Dent. Relat. Res. 2015, 17, 52–70. [Google Scholar] [CrossRef] [PubMed]
- Villa, R.; Rangert, B. Early Loading of Interforaminal Implants Immediately Installed after Extraction of Teeth Presenting Endodontic and Periodontal Lesions. Clin. Implant. Dent. Relat. Res. 2005, 7, s28–s35. [Google Scholar] [CrossRef] [PubMed]
- Lata, J.; Parmar, M. Placement of single tooth implant in healed socket with immediate temporization: Clinical study. Contemp. Clin. Dent. 2012, 3, 412–415. [Google Scholar] [CrossRef] [PubMed]
- Tolstunov, L. Implant Zones of the Jaws: Implant Location and Related Success Rate. J. Oral Implantol. 2007, 33, 211–220. [Google Scholar] [CrossRef]
- Ata-Ali, J.; Ata-Ali, F. Do antibiotics decrease implant failure and postoperative infections? A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2013, 43, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Kashani, H.; Hilon, J.; Rasoul, M.H.; Friberg, B. Influence of a single preoperative dose of antibiotics on the early implant failure rate. A randomized clinical trial. Clin. Implant. Dent. Relat. Res. 2019, 21, 278–283. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, N.; Saad, N. Effects of antibiotics on dental implants: A review. J. Clin. Med. Res. 2012, 4, 1–6. [Google Scholar] [CrossRef]
- Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Prophylactic antibiotic regimen and dental implant failure: A meta-analysis. J. Oral Rehabil. 2014, 41, 941–956. [Google Scholar] [CrossRef]
- Givens, E., Jr.; Bencharit, S.; Byrd, W.C.; Phillips, C.; Hosseini, B.; Tyndall, D. Immediate placement and provisionalization of implants into sites with periradicular infection with and without antibiotics: An exploratory study. J. Oral Implantol. 2015, 41, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Sharaf, B.; Jandali-Rifai, M.; Susarla, S.M.; Dodson, T.B. Do Perioperative Antibiotics Decrease Implant Failure? J. Oral Maxillofac. Surg. 2011, 69, 2345–2350. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Grusovin, M.G.; Worthington, H.V. Interventions for replacing missing teeth: Antibiotics at dental implant placement to prevent complications. Cochrane Database Syst. Rev. 2013, 2013, CD004152. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez Sánchez, F.; Rodríguez Andrés, C.; Arteagoitia, I. Which antibiotic regimen prevents implant failure or infection after dental implant surgery? A systematic review and meta-analysis. J. Cranio-Maxillo-Facial Surg. 2018, 46, 722–736. [Google Scholar] [CrossRef] [PubMed]
- Romandini, M.; De Tullio, I.; Congedi, F.; Kalemaj, Z.; D‘Ambrosio, M.; Laforí, A.; Quaranta, C.; Buti, J.; Perfetti, G. Antibiotic prophylaxis at dental implant placement: Which is the best protocol? A systematic review and network meta-analysis. J. Clin. Periodontol. 2019, 46, 382–395. [Google Scholar] [CrossRef]
- Kim, A.; Abdelhay, N.; Levin, L.; Walters, J.D.; Gibson, M.P. Antibiotic prophylaxis for implant placement: A systematic review of effects on reduction of implant failure. Br. Dent. J. 2020, 228, 943–951. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Tennant, M.; Walsh, L.J.; Kruger, E. Is there a consensus on antibiotic usage for dental implant placement in healthy patients? Aust. Dent. J. 2018, 63, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Gregoire, C. How are odontogenic infections best managed? J. Can. Dent. Assoc. 2010, 76, a37. [Google Scholar]
- Jun, S.H.; Park, C.-J.; Hwang, S.-H.; Lee, Y.K.; Zhou, C.; Jang, H.-S.; Ryu, J.-J. The influence of bone graft procedures on primary stability and bone change of implants placed in fresh extraction sockets. Maxillofac. Plast. Reconstr. Surg. 2018, 40, 8. [Google Scholar] [CrossRef] [PubMed]
- Willenbacher, M.; Al-Nawas, B.; Berres, M.; Kämmerer, P.W.; Schiegnitz, E. The Effects of Alveolar Ridge Preservation: A Meta-Analysis. Clin. Implant. Dent. Relat. Res. 2016, 18, 1248–1268. [Google Scholar] [CrossRef]
- Sbordone, L.; Levin, L.; Guidetti, F.; Sbordone, C.; Glikman, A.; Schwartz-Arad, D. Apical and marginal bone alterations around implants in maxillary sinus augmentation grafted with autogenous bone or bovine bone material and simultaneous or delayed dental implant positioning. Clin. Oral Implant. Res. 2011, 22, 485–491. [Google Scholar] [CrossRef] [PubMed]
- Cionca, N.; Hashim, D.; Mombelli, A. Zirconia dental implants: Where are we now, and where are we heading? Periodontol. 2000 2017, 73, 241–258. [Google Scholar] [CrossRef] [PubMed]
- Hashim, D.; Cionca, N.; Courvoisier, D.; Mombelli, A. A systematic review of the clinical survival of zirconia implants. Clin. Oral Investig. 2016, 20, 1403–1417. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, D.; Sennerby, L.; Meredith, N. Measurements Comparing the Initial Stability of Five Designs of Dental Implants: A Human Cadaver Study. Clin. Implant. Dent. Relat. Res. 2000, 2, 85–92. [Google Scholar] [CrossRef]
- Strietzel, F.P.; Neumann, K.; Hertel, M. Impact of platform switching on marginal peri-implant bone-level changes. A systematic review and meta-analysis. Clin. Oral Implant. Res. 2015, 26, 342–358. [Google Scholar] [CrossRef]
- Rocha, S.; Wagner, W.; Wiltfang, J.; Nicolau, P.; Moergel, M.; Messias, A.; Behrens, E.; Guerra, F. Effect of platform switching on crestal bone levels around implants in the posterior mandible: 3 years results from a multicentre randomized clinical trial. J. Clin. Periodontol. 2016, 43, 374–382. [Google Scholar] [CrossRef]
- Renouard, F.; Nisand, D. Impact of implant length and diameter on survival rates. Clin. Oral Implant. Res. 2006, 17, 35–51. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.-T.; Chen, Y.-W.; Starr, J.R.; Chuang, S.-K. Survival analysis of wide dental implant: Systematic review and meta-analysis. Clin. Oral Implant. Res. 2016, 27, 1251–1264. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).