1. Introduction
The Acholi sub-region in northern Uganda is an area of widespread poverty that suffered a prolonged war that lasted for over 20 years. In this conflict, a rebel organisation known as the Lord’s Resistance Army (LRA) fought the Ugandan Government forces and attacked civilian settlements, resulting in large-scale destruction of property, mass displacement and extensive physical injuries to the civilian and combatant populations due to explosions, gunshots and punishment amputations [
1,
2,
3]. The extensive media coverage associated with this conflict triggered large-scale operations by relief agencies such as the United Nations, World Food Programme, International Committee of the Red Cross, AVSI and several other smaller Non-Governmental Organisations (NGOs). These voluntary agencies accounted for the vast majority of health provision during the conflict, as the already limited local health infrastructure was destroyed by war [
4]. However, these services were not sufficient to meet demand, and were often not able to reach the most remote and rural communities, leaving many un-treated. The involvement of these agencies has gradually scaled down since the conflict ended in 2005, whilst limited resources and the remote nature of Acholi mean that the adequate capacity for rehabilitative service provision has not been created by the government in the intervening period. As a result, many individuals who experience MLL either from causes related to the war or due to other causes, may never receive medical treatment, rehabilitative services or assistive devices (e.g., prosthetics).
The significant health benefits associated with the provision of a suitable prosthesis for people with major limb loss (MLL) are widely understood [
5,
6], but difficulties in accessing such services are well recognised in Uganda and many other countries in Sub Saharan Africa. The relatively low priority given to resource provision for less visible chronic health needs such as rehabilitation services is very apparent in many countries, and Uganda (Northern Uganda in particular) is no exception to this pattern [
7]. Despite the formation of positive government policy with respect to disabled people, the disability services of the Ugandan government suffer from differing statistics and definitions of disability, which makes targeting interventions difficult [
8,
9]. Data on disability type and prevalence are also scarce, mostly existing only at the national level, with no understanding of spatial variations of prevalence within Uganda [
8].
In this context, prevalence studies are essential tools to highlight the magnitude of the problem and its potential impact on wellbeing and productivity in order to influence health policy and establish the scale of rehabilitation service requirements in regions such as Acholi. Such detailed local data are of particular importance in a country where a prolonged and violent conflict was concentrated in some of the most remote parts of the country, where data collection is likely to be worst. Nevertheless, there is a notable absence of prevalence studies for limb loss across the Global South, with the few examples in the literature limited to hospital-based studies (e.g., [
10]) or more developed countries (a review is provided in [
11]). It is likely that this is, at least in part, due to the remote nature of the region and the associated lack of high-quality datasets such as maps and data on population and existing health provision; all of which pose significant challenges to both study design and subsequent analysis. The authors, therefore, hope that the novel methods presented here can be adopted and implemented elsewhere in order to promote a better understanding of disability prevalence and the need for rehabilitative services across the Global South.
The present study seeks to address this deficit by systematically determining the prevalence and spatial distribution of Major Limb Loss (MLL) in the Acholi sub-region of Northern Uganda. The study seeks to:
Characterise the causes of MLL in the population in the Acholi sub-region;
Provide an estimate for the number of people with MLL in the Acholi sub-region;
Describe the demographic characteristics of those with MLL in the Acholi sub-region;
Characterise the spatial distribution of people with MLL in the Acholi sub-region;
Examine the implications of these findings for the creation of prosthetic and rehabilitative service provision.
4. Discussion
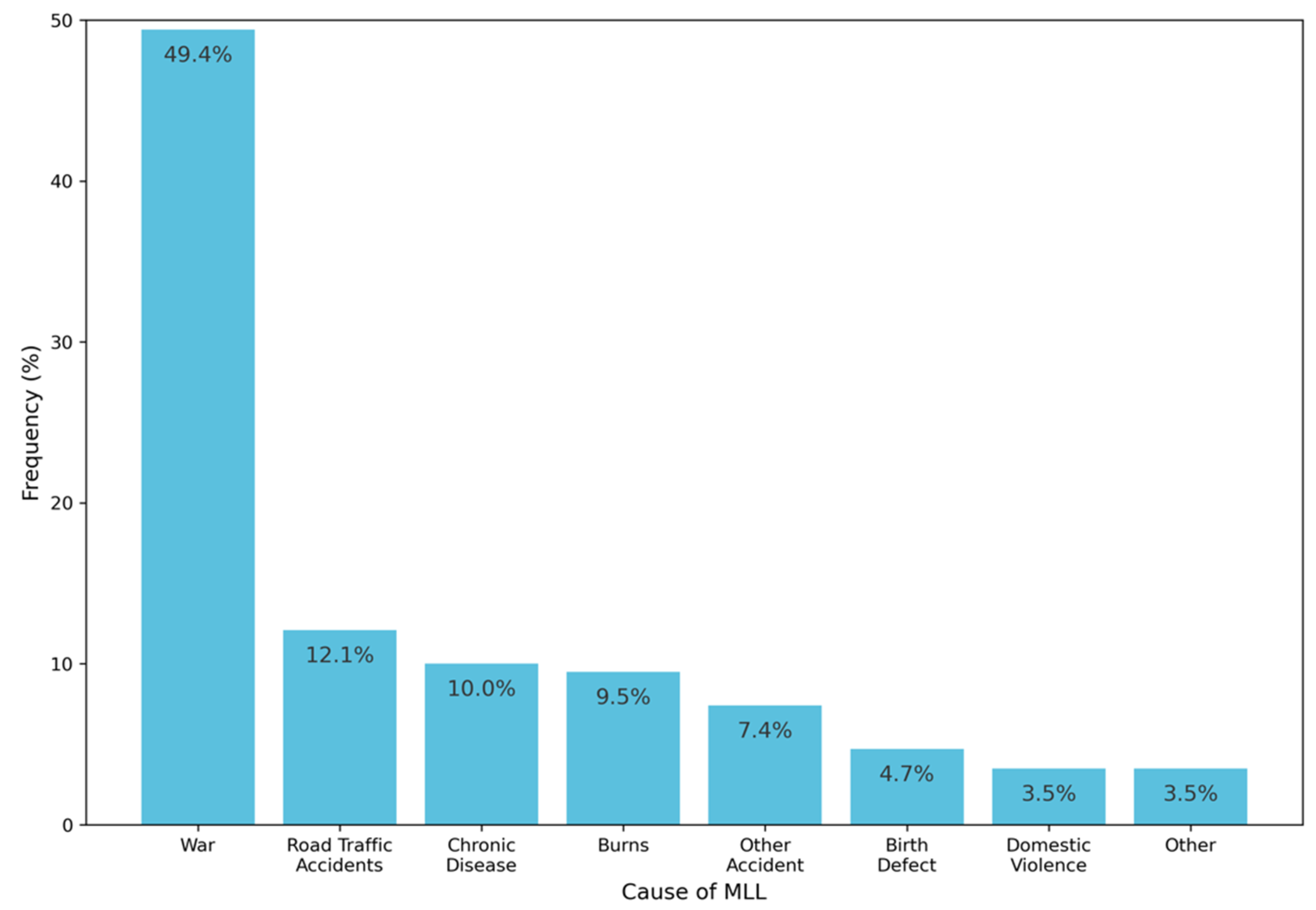
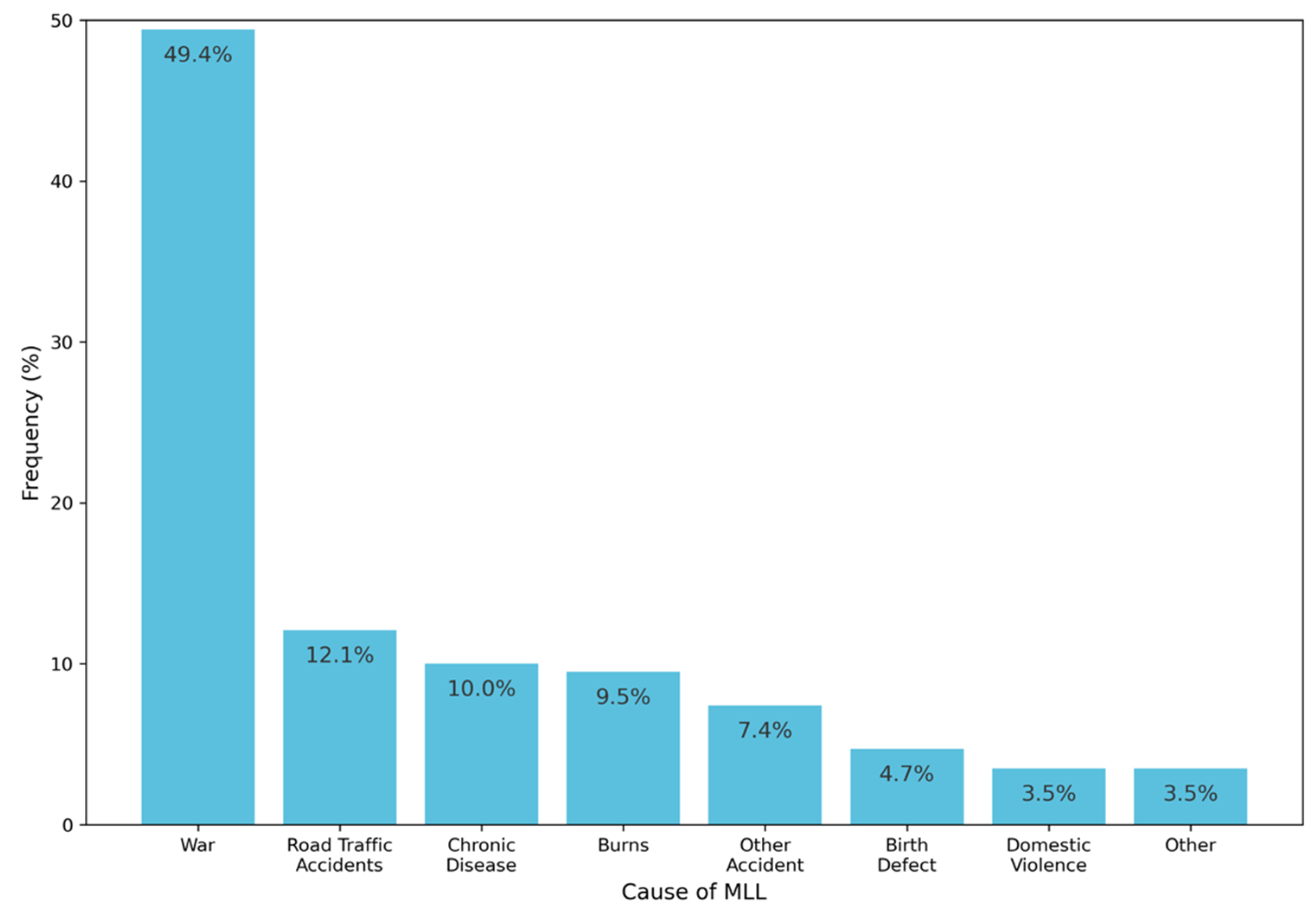
This study comprises the first systematic estimate of MLL prevalence in the Acholi Sub-Region. We estimate that there are approximately 10,117 people with MLL in this region, giving a prevalence rate of approximately 0.5% of the population. In addition to information on the prevalence of MLL, this work also provides the first detailed understanding of the causes of MLL, and their relative magnitudes. There is, of course, an important temporal aspect to these findings, which will have clear implications for future policy and service provision. For example, assuming that no new conflicts develop in the region, it is likely that the effects of the war (which currently explains approximately half of cases in the region) will reduce in relative magnitude, with a corresponding increase in causes such as road traffic accidents and chronic disease, both of which are becoming increasingly prevalent in the region as a result of changing lifestyles and the increasing proliferation of tarmac roads [
10]. This expected shift could increase the likelihood of hospital attendance (e.g., for amputation) for those experiencing MLL, which could be beneficial from the perspective of increasing access to rehabilitative services, as patients receiving an amputation are already ‘in the system’ (as opposed to those who have never received formal medical care). However, a recent hospital-based study of 141 patients between 2007 and 2018 at two of the main hospitals in the region found that less than 1% of patients had been formally referred to rehabilitation services [
10]. Clearly, the lack of provision in the region is a significant driver of this finding, and this work has, for the first time, provided evidence for both the size and spatial distribution of the need for rehabilitative services. These findings must therefore be used to formulate appropriate policy and training, such that a well-integrated rehabilitation service can be introduced to the system so that this urgent demand can be met.
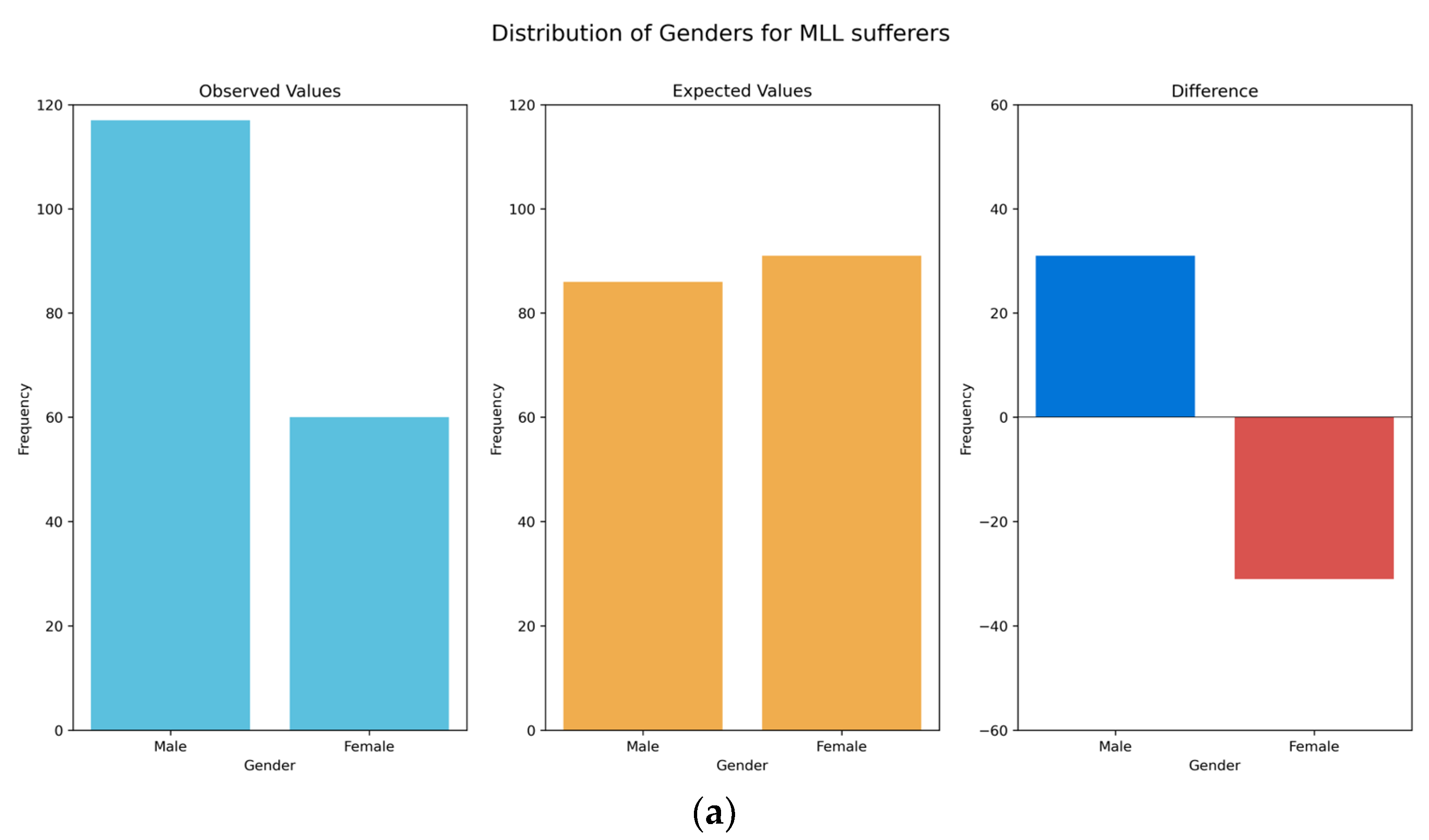
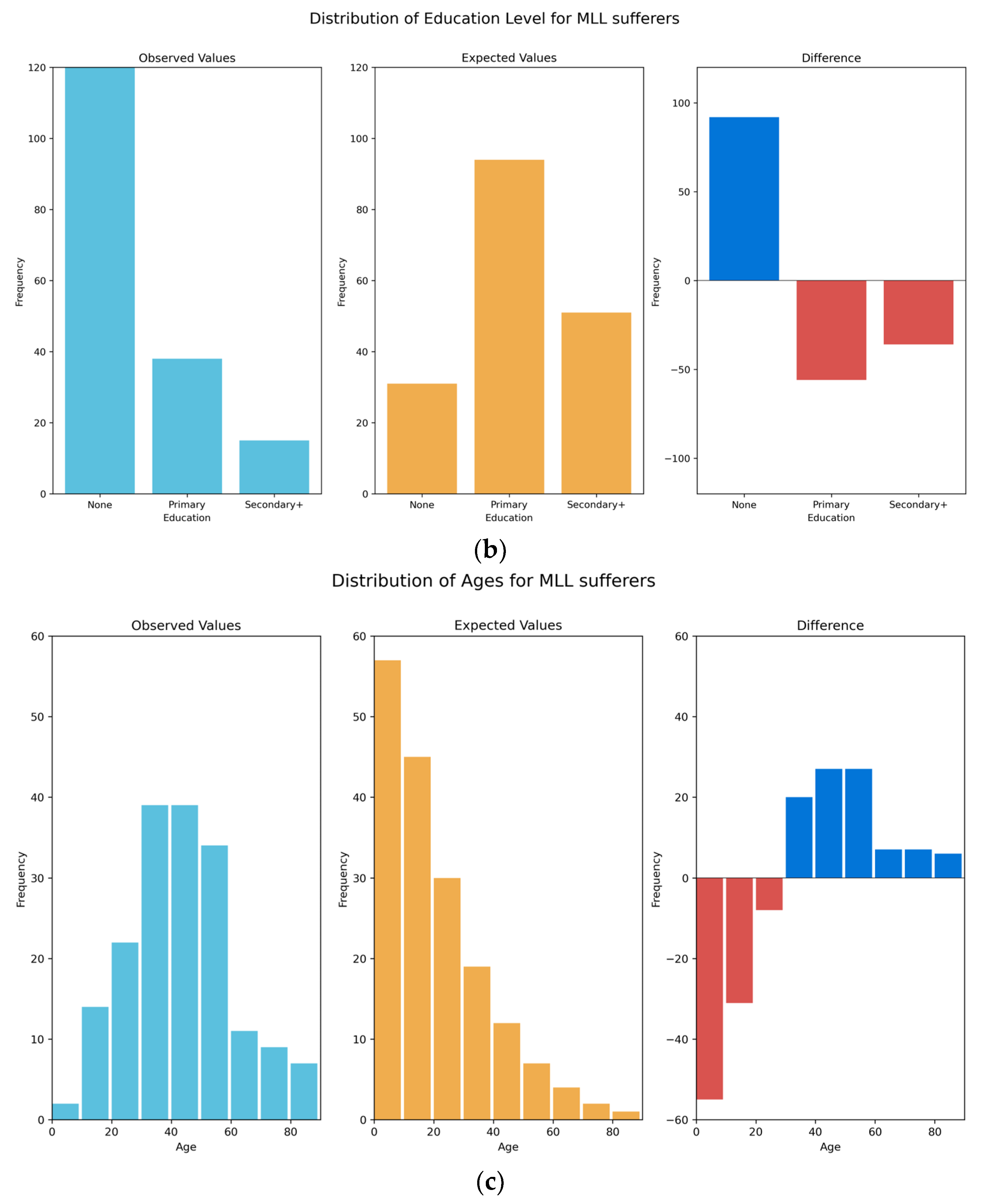
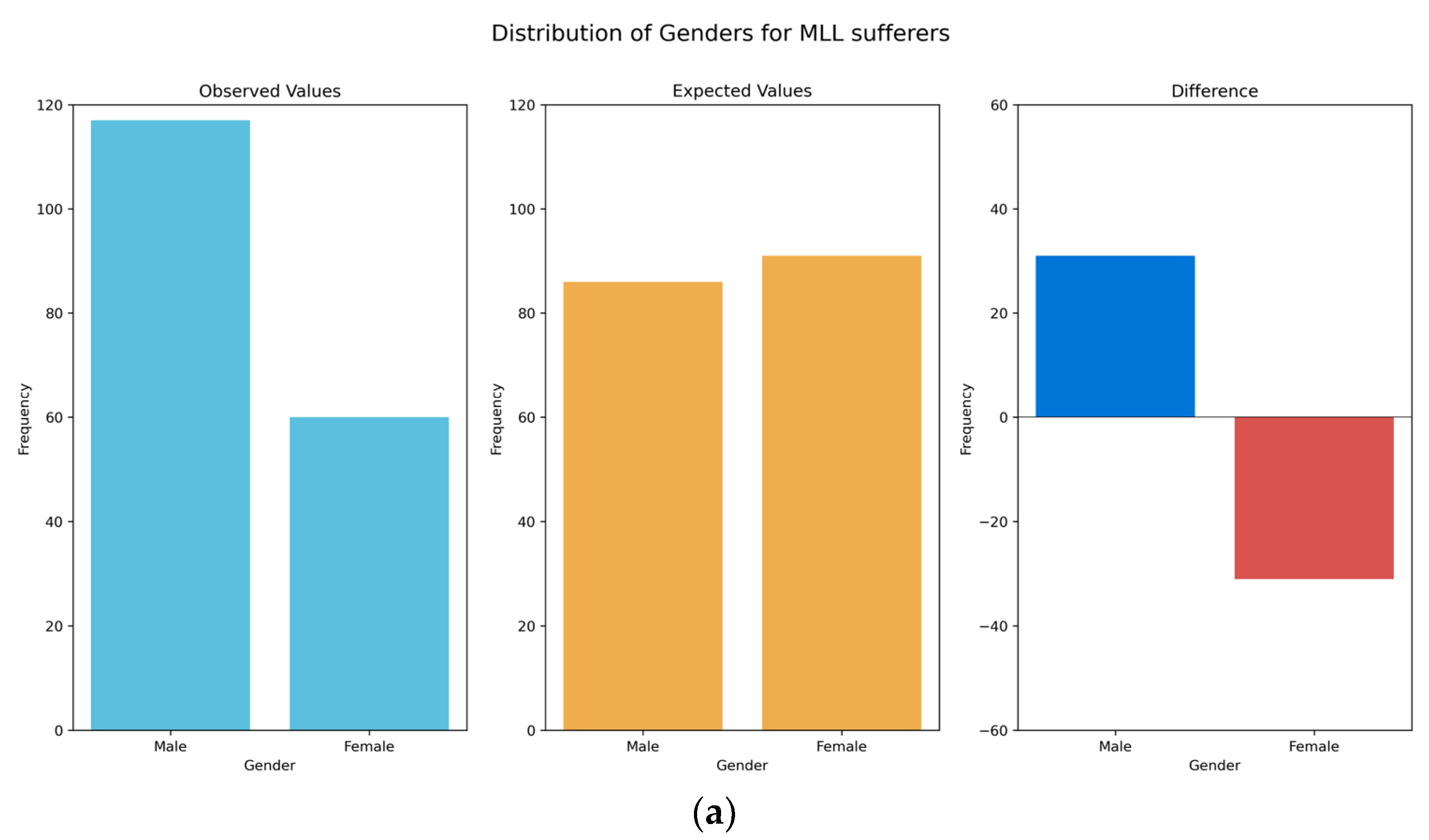
We have also demonstrated that those people with MLL in the region are predominantly male, older and have lower educational attainment when compared to the general population. These results meet with expectations, as males are more likely to have been injured during combat in the LRA insurgency, as well as being more likely to be working in the fields, where they may pick up injuries from remnant land mines or accidents caused during manual labour. The end of the LRA insurgency in around 2005 means that the young are therefore less likely to have been involved in fighting, attacks or other conflict-related injuries than older members of the population, though remnant land mines remain an issue for all. Those who lived through the conflict will also have likely experienced periods of reduced access to healthcare, meaning that less severe injuries might have resulted in MLL that could otherwise have been treated. It is also perhaps less likely that young people will have developed chronic diseases leading to MLL, such as type-2 diabetes, which typically presents later in life. With respect to levels of education, there is likely dual causation, with those who are disabled less likely to be able to afford or access education; whereas those with lower levels of education are more likely to be in situations where they might become injured, such as working in fields where they might become injured by remnant land mines, or driving a motorbike taxi (boda-boda) where they might be involved in a traffic accident. Our findings suggest that almost half of those with MLL have never had access to rehabilitative services or assistive devices of any kind. This reinforces clear inadequacy in rehabilitative service provision in the region and a clear need for urgent government investment.
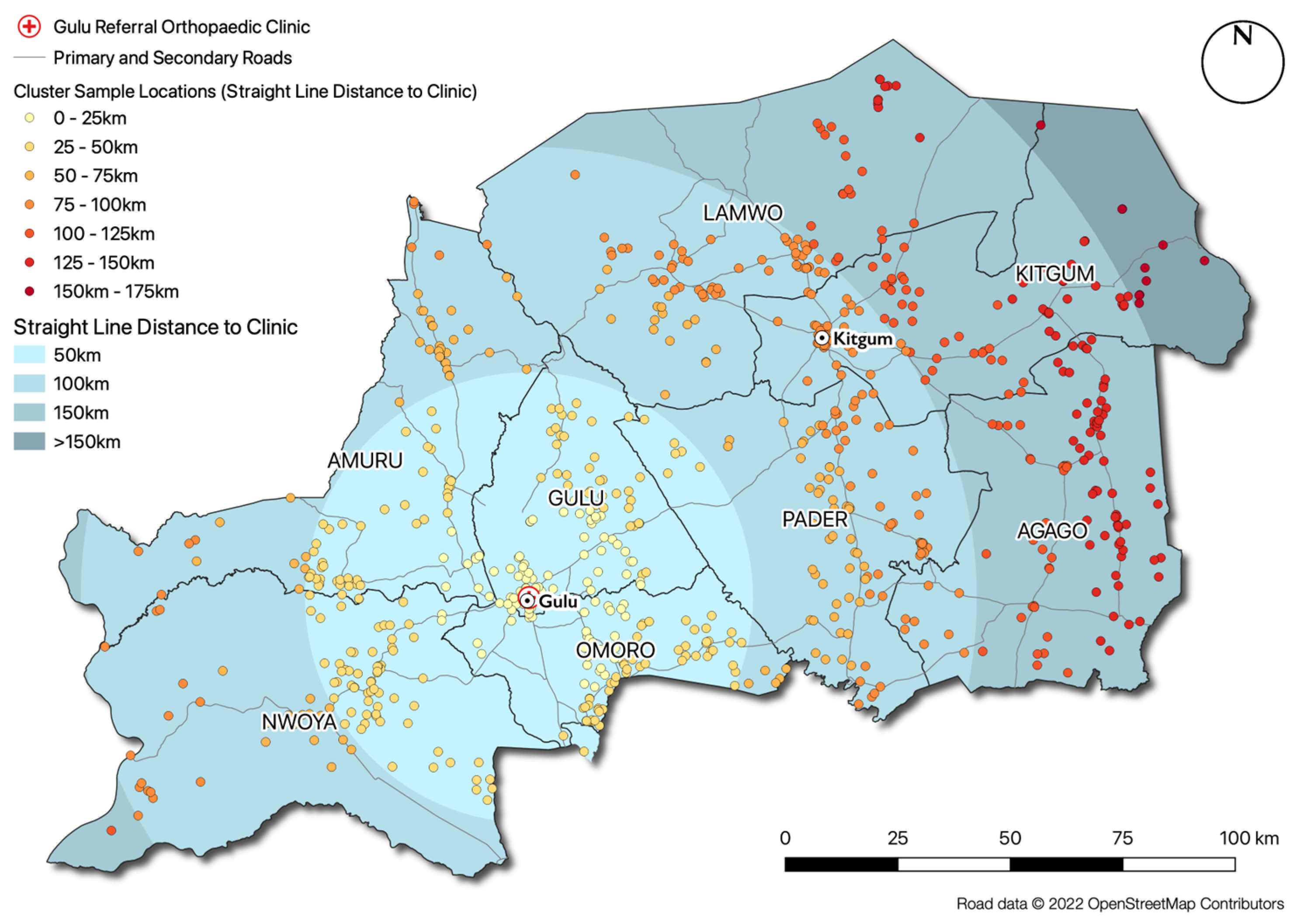
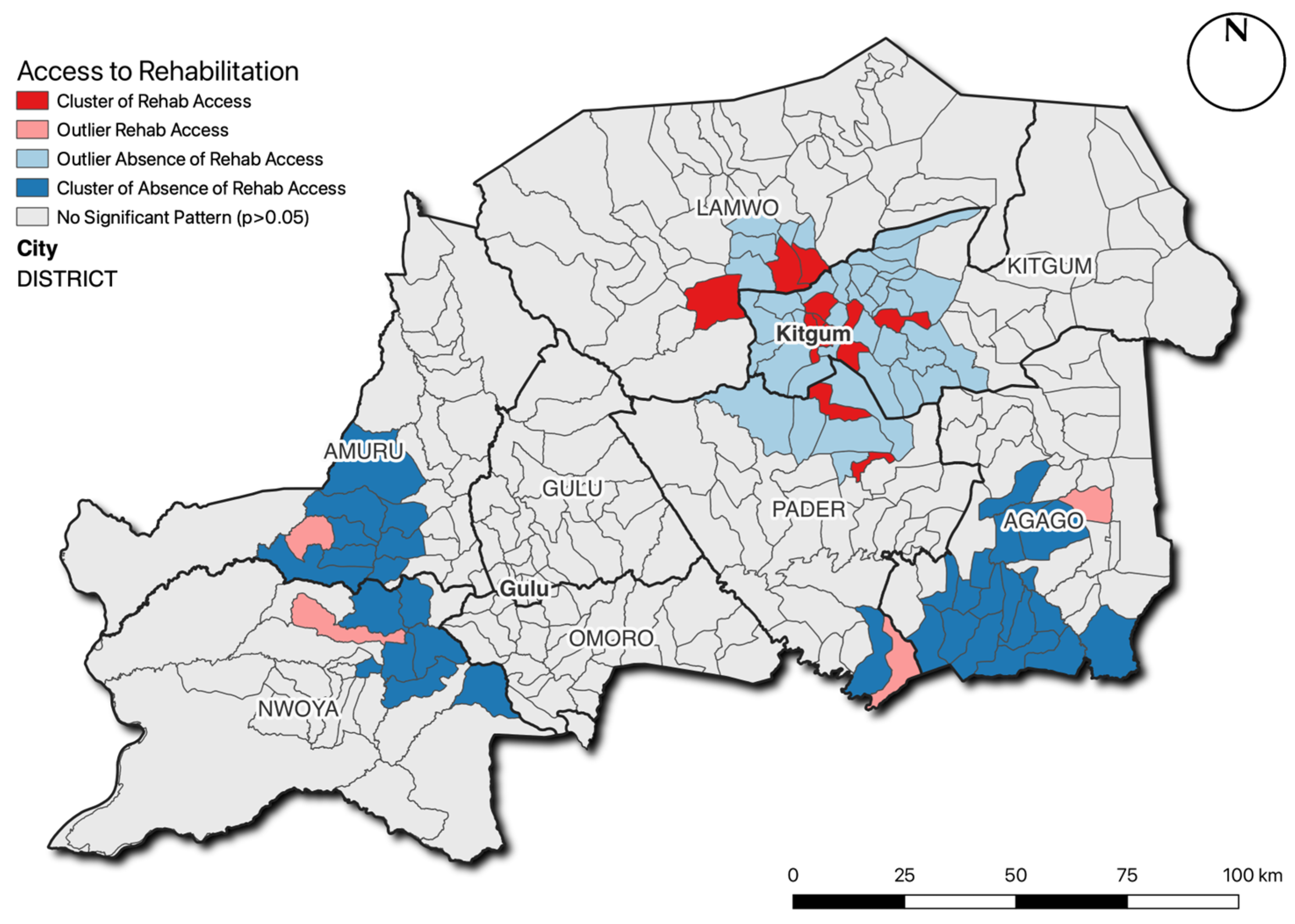
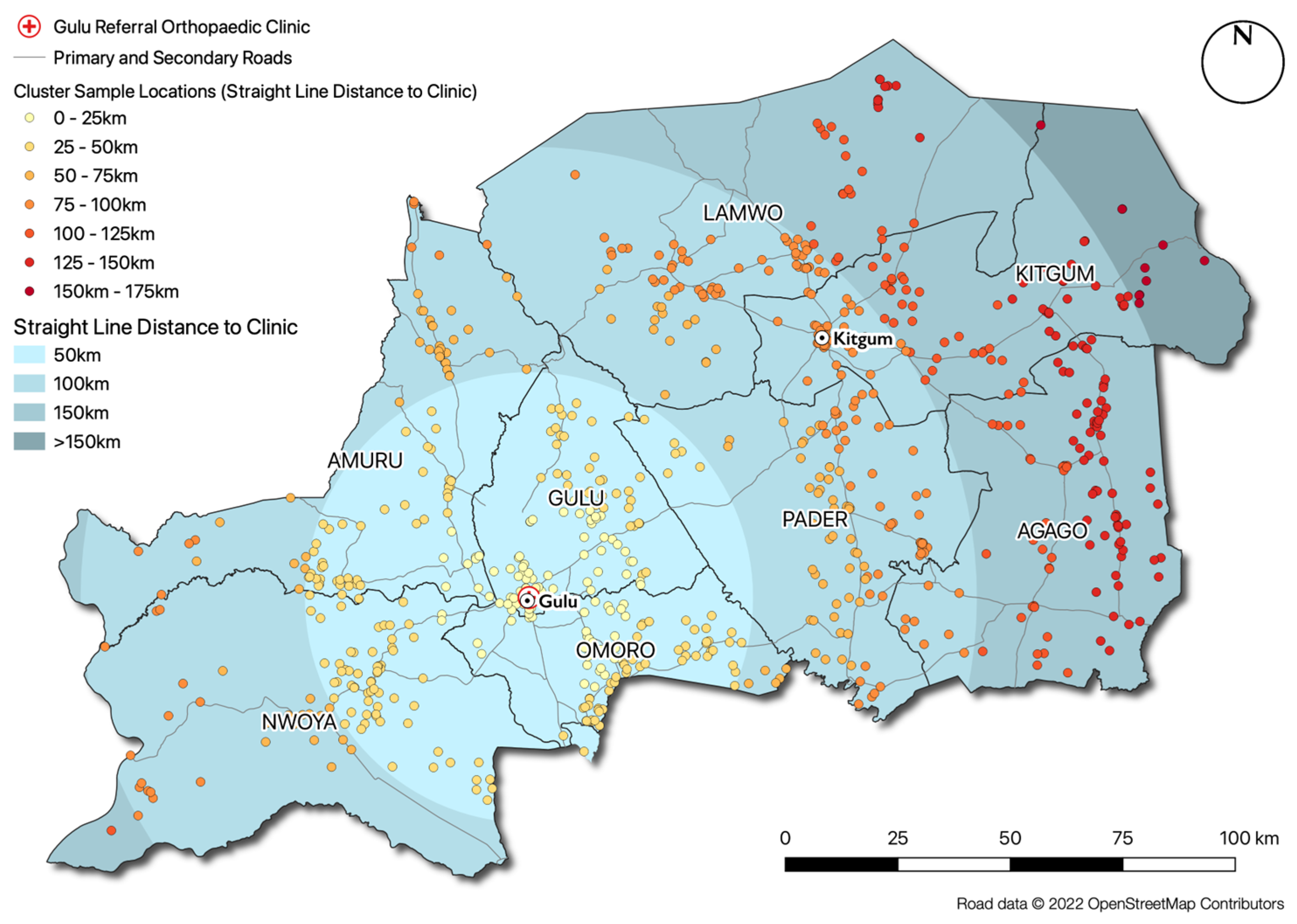
The challenge of creating such a service is illustrated by the findings of the spatial analysis presented in this research, which demonstrates that people with MLL are distributed throughout the entire region, as opposed to spatially clustered in certain locations (e.g., large towns or cities). Based on the current provision of rehabilitation and prosthetic services (a single facility at Gulu Referral Hospital, which was partly funded by this research project), those with MLL would be required to travel an average of over 60 km and a maximum of over 170 km to access these services. The estimated MLL prevalence rate (
c. 0.5% of the population) clearly suggests that there is a substantial need for additional service provisions in this region. The highly dispersed spatial distribution of people with MLL, high levels of poverty in the region and poor road and transport links suggest that alternative service delivery models are urgently required, as it is unlikely that many people with MLL will be able to travel the required distances to receive services using traditional ‘centralised’ models based in the cities. This view is reinforced by the pattern found in
Figure 4, which demonstrates a significant cluster of those who have received rehabilitative services in the immediate vicinity of Kitgum, where centralised NGO activities were concentrated in the immediate post-war period, and significant concentrations of people who have not been able to access these services further away from this location.
As a demonstration of one such alternative service delivery model, the authors have set up an outreach prosthetic limb service operating from Gulu Referral Hospital to demonstrate the potential of such an alternative service delivery model. This outreach service was modelled on a similar approach adopted in post-war Sri Lanka [
29], and seeks to deliver prosthetic limb services at open clinics held in local community centres. This is important, as this approach does not require individuals to travel to the clinic and is therefore much more accessible. People with MLL attending the clinic are assessed by a suitably qualified practitioner free of charge, and those with suitable healthy stumps receive bespoke prosthetic limbs and rehabilitative care free of charge at a location close to their homes. In 2019, this outreach service successfully provided 52 prosthetic limbs to 51 patients (one bilateral). Further evaluation of this and other models of service delivery are urgently needed to evaluate their potential to address these challenges, both in terms of efficiency and acceptance by the local population.
4.1. Study Limitations
There are a number of assumptions that had to be made in this research, chief amongst which was the estimate of the population size of the Acholi sub-region, which is a prediction based upon expected population growth from the 2014 census of household population [
13], and official refugee numbers [
14], both of which are expected to be significant underestimates, and also exclude those living in institutions (e.g., prisons), forest reserves, barracks and other non-household settings [
12]. Further, the 2014 census was based on a sampling (rather than comprehensive) survey, introducing unknown levels of uncertainty in the resulting population figures. This uncertainty is compounded by the difficulty in predicting population change since 2014 due to the extremely rapid population growth and frequent movement of people (including refugees) both into and out of Uganda across adjacent international borders.
In our spatial analysis (Moran’s
I, LISA), there are inevitable edge effects arising from the bounds of the study region (normally manifest in the identification of ‘false hotspots’ at the edges of the study region). Our approach of the use of distance-weighting between zone centroids (as opposed to the more ‘traditional’ adjacency-based approaches) mitigates this effect by increasing the number of ‘neighbours’ that are taken into account for each zone. Nevertheless, it is possible that changes in the extent of the study region (e.g., through an adjustment to Ugandan administrative boundaries) could impact the results of our spatial analysis. For example, increasing the extent of our analysis might have revealed clusters that span the edges of our current area of interest. This effect (the Modifiable Areal Unit Problem) is well understood in the spatial analysis [
30], and though the problem is unavoidable, it nevertheless warrants consideration.
The expected distributions for gender and educational levels were based upon data for the Acholi Sub-Region, taken from the 2014 census. We must assume that these distributions (rather than individual values) have not changed significantly in the 4 years between the publication of the census and the data collection, and we are reliant upon the quality of the census data. The expected distribution of ages was based upon the UBOS Mid-Year Population Projection for 2018, which is a modelled extrapolation from the 2014 census. This is a national dataset (values are not given at regional, sub-regional or district level), and so we must assume that the underlying model is robust, and that the population distribution of the Acholi sub-region is not significantly different to the national population distribution. The risks associated with all three of these expected distributions are mitigated somewhat by the vanishingly small probabilities of the values in our sample being drawn from the expected distributions.
The HRSL dataset [
19] that we used in the cluster sampling process describes estimated population density, rather than individual buildings. There is also a possibility that this dataset might perform less well in rural than urban settings (as there are fewer buildings available in a more-sparse distribution, which can make less-populated areas harder to detect). However, two ‘on the ground’ validation surveys of the area by the authors, as well as visual validation against high-resolution satellite imagery, showed that population patterns in the dataset correlate well with the location of buildings and huts in rural areas. Nevertheless, more detailed maps and population data would permit more precise population estimates to be undertaken and increase the robustness of the sampling strategy [
17].
An error made by some of the trained researchers during data collection meant that precise locations were only collected correctly for 57 of the 181 people with MLL that were interviewed. This was addressed by aggregating people with MLL to the parish level, for which data were available for 167 people with MLL. Given the relatively small size of the parishes in comparison with the study area, their centroids provide a reasonable proxy location for sample locations, meaning that this has had only a minor impact on the analysis of distance distribution and does not affect the quality of the results. One consideration here would be that this approach would overlook significant intra-parish clusters, but the small number of cases per parish makes this unlikely, and there is no way of resolving this with the available dataset.
4.2. Implications of the Findings
The physical and mental wellbeing of people living in parts of the world that are recovering from prolonged conflict is receiving increasing attention [
31,
32]. It is known that people with major disabilities are prone to developing a wide range of secondary health problems because of chronic inactivity, social isolation, unemployment, discrimination and marginalisation. For example, a study of landmine victims in northern Sri Lanka showed that a large proportion of victims lost their earning capacity as a result of their injuries [
33]. Furthermore, the prevalence of post-traumatic stress disorder, acute stress reaction, anxiety disorders and depression amongst the victims were significantly greater than in the general population living in the affected areas [
33]. These residual issues, attributable to the direct or indirect consequences of the conflict, have a serious impact on quality of life, social cohesiveness, productivity and wellbeing and can contribute to the development of recurrent cycles of violence and poverty. This research has demonstrated how a prevalence study can be undertaken in data-poor regions, and the methods for undertaking such a study in data-poor areas (as well as the outreach clinic model) would be easily transferrable to other settings.
The new insights into MLL and disability provided by this research are vitally important, as a better understanding of the prevalence and nature of MLL will, for the first time, provide an evidence base against which medical care and rehabilitation services can be provided to those with MLL in the Acholi sub-region. We have also identified that 8.2% of the population (c. 150,512 people) in this region currently live with other forms of major physical disabilities, which may have a major impact on their life chances and quality of life. These findings reinforce the need for greater focus on developing rehabilitation services to meet the needs of the population. War, as anticipated, has been a major cause of MLL in the region, but several other significant causes of MLL have been identified, which cumulatively account for around half of cases, and notably include road traffic accidents and chronic disease. This is critically important in understanding changing service provision needs in this region, as many NGOs currently providing these services provide support only to those who lost limbs as a result of the war; meaning that approximately half of the population of people with MLL will have no access to rehabilitation services (including prosthetic devices) whatsoever.
The preponderance of lower limb loss over upper limb amputations from combat areas has been reported previously. For example, Bendinelli reported that almost 50% of civilian adults who sustained blast injuries in Cambodia had lower limb injuries [
34]. As a result, most prosthetic limb services in post-conflict LMICs (including Cambodia, Uganda and Sri Lanka) have focused on lower limb prostheses. Our study revealed that approximately 39% of those with MLL had lost upper limbs, with
c. 2% having lost both upper and lower limbs. Blast injuries from the ground upwards are likely to affect lower limbs more than upper limbs, but amputation of both upper and lower limbs was a widely practised punishment by the LRA [
3], which (along with gunshot wounds) is likely to account for this relatively high proportion of upper limb loss in our study population. The question of rehabilitation for these upper limb amputees is compounded by the absence of any upper limb prosthetic limb services in the Acholi sub-region, and further research is required into how these services might be best provided in global contexts such as northern Uganda [
35,
36].
5. Conclusions
The significant health and wellbeing benefits associated with the provision of a suitable prosthesis for people with MLL are widely understood [
5,
6], but access to such services is extremely limited in the Acholi sub-region. Part of the reason for this is the low priority given to chronic health needs by the Ugandan Government [
7], meaning that even the level of need for such services is poorly understood. This research, therefore, provides the first detailed study of MLL in the Acholi sub-region, clearly articulating the prevalence, causes and spatial distribution of MLL in the region. These findings reveal a substantial need for rehabilitative service provision that is not currently being met, with our conservative estimates suggesting that
c. 0.5% of the population are living with MLL, and
c. 47% have never accessed any rehabilitative services whatsoever. Our findings also demonstrate the spatial pattern of the requirement for these services, which suggests that those with MLL are dispersed throughout the region rather than concentrated in population centres, a situation that is not reflected in the centralised service models that are currently used both in Acholi and elsewhere in the country. High levels of poverty and low levels of mobility mean that extensive spatial coverage is required in order to ensure accessibility, and we have demonstrated the efficacy of such a service, which has successfully provided services (including prosthetic limbs) to over 50 people using an outreach-based model.
This study provides a new understanding of the requirement for rehabilitative services in the region and, in doing so, sets an agenda for how these needs can be met through action by researchers, NGOs and government. Further studies are now required to evaluate the acceptability, suitability and cost-effectiveness of approaches, such as outreach rehabilitation services, in order to support their adoption both in Acholi and other post-conflict settings. Further research is also required to examine how those with upper-limb loss might be best supported, as the prevalence of upper limb loss was found to be much higher than expected (c. 39%), yet there is no provision at all for upper limb prosthetic services whatsoever. Further research should also include the application of the methods presented here to other data-scarce regions where the prevalence of MLL, disability and other conditions remain poorly understood. Extant NGOs providing services elsewhere should broaden their remit to remove focus solely from those who experienced MLL due to war and adapt their operations to reflect the spatial patterns of demand that have been revealed in this study.
Finally, the Ugandan Government must use the evidence presented here to increase the priority given to a range of chronic health needs in policy, including MLL and other conditions (e.g., diabetes) that are increasingly contributing to avoidable cases of MLL. Investment is urgently needed in the development of robust, integrated and sustainable rehabilitative services in Acholi, supported by NGOs where appropriate. These services must be designed to reflect the magnitude and spatial patterns of demand that have been identified here, and a robust and efficient referral system put into place in order to increase accessibility for all of those with MLL across Acholi and other regions of Uganda.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}