Are Cry Studies Replicable? An Analysis of Participants, Procedures, and Methods Adopted and Reported in Studies of Infant Cries


Abstract
1. Introduction
2. Materials and Method
2.1. Variable Definition
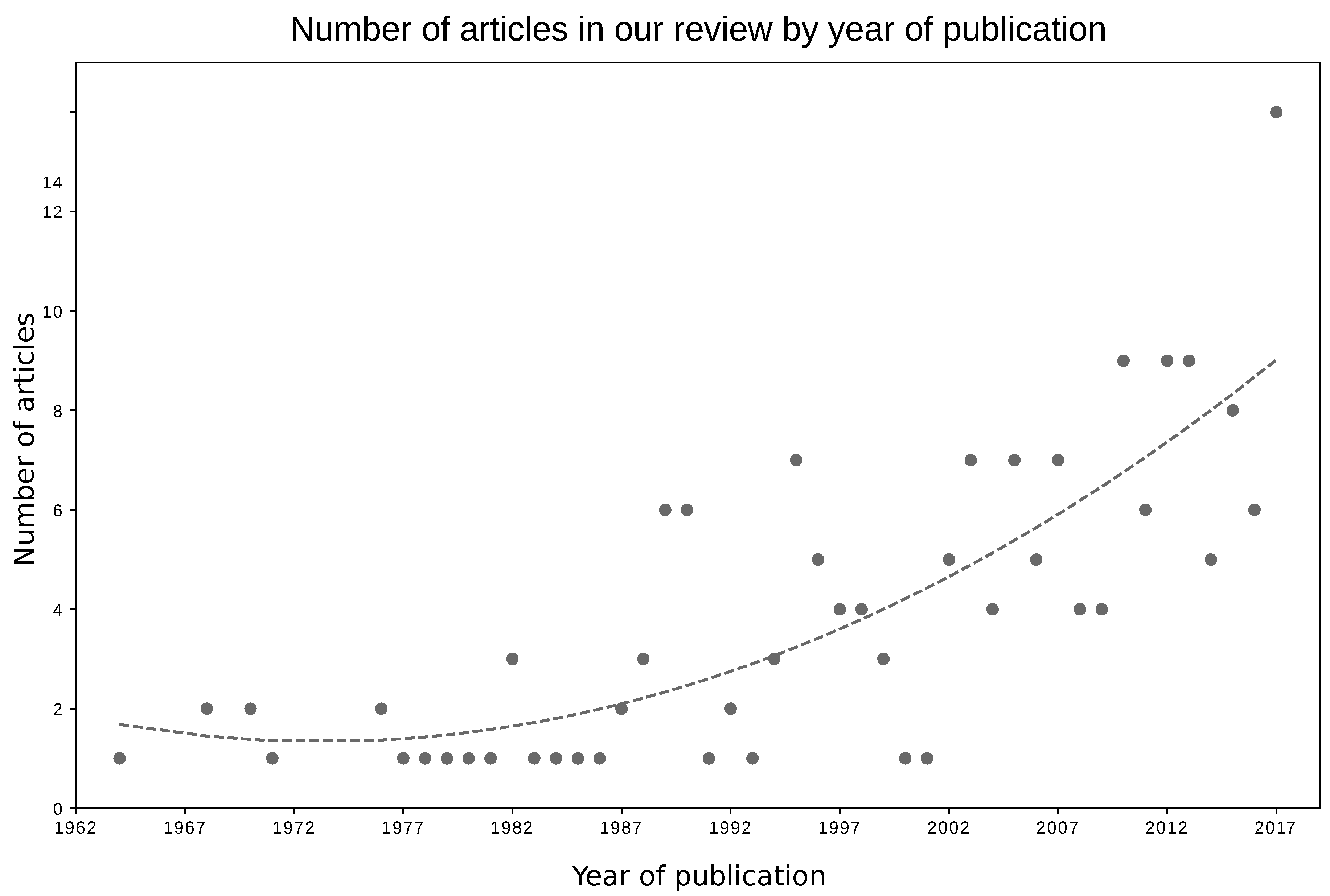
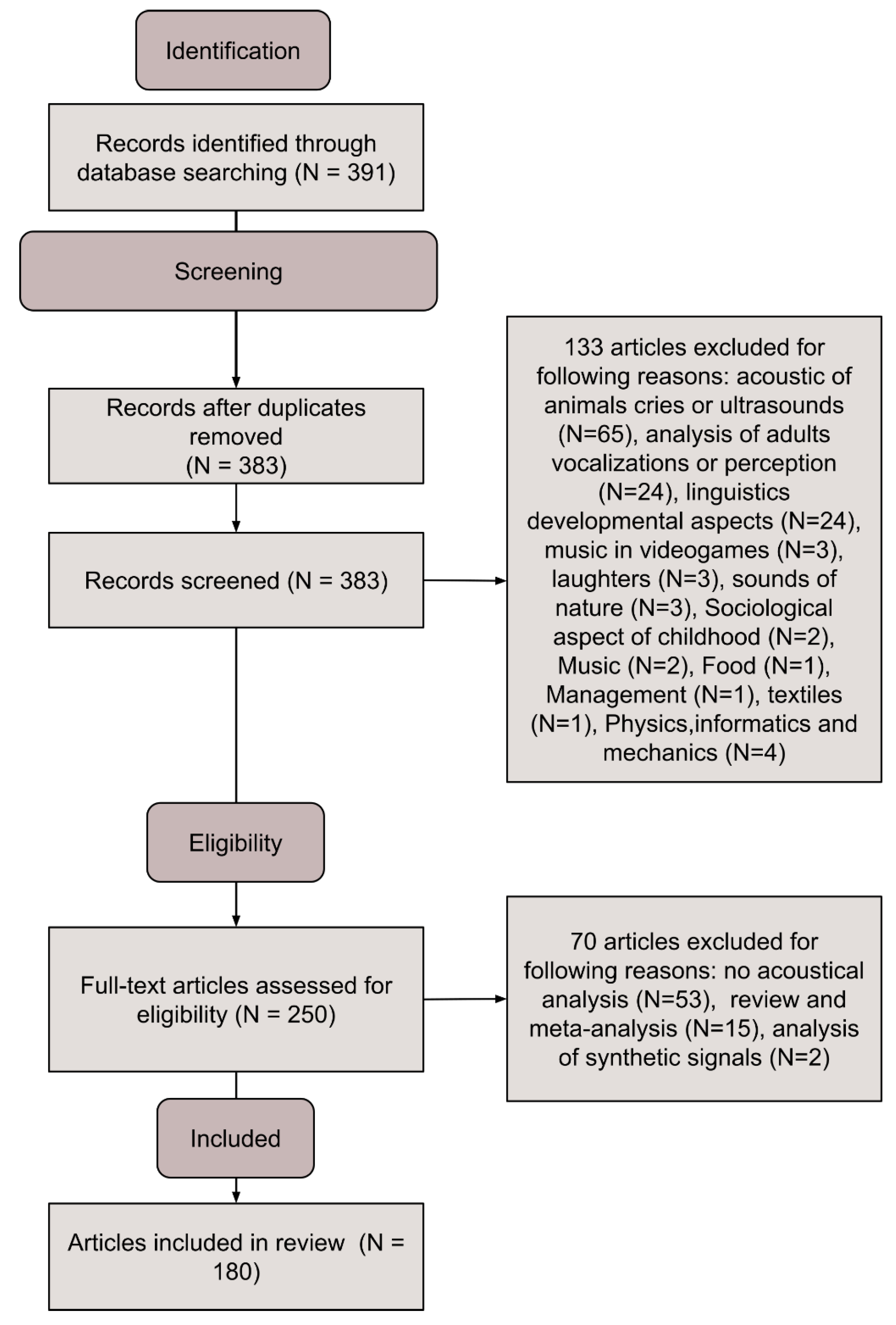
2.2. Search Methods and Results
3. Results
3.1. Participants
3.2. Data Collection
3.3. Methods and Data Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| CNS | Central Nervous System |
| ASD | Autism Spectrum Disorder |
| SIDS | Sudden Infant Death Syndrome |
| F0 | Fundamental Frequency |
| Fn | nth Formant |
| Part | Number of Participants |
| Sam | Number of Samples |
| Age | Participants’ Age |
| Sex | Participants’ Gender |
| Tri | Cry Trigger |
| Pos | Participants’ Position |
| Hea | Participants’ Health Status |
| Mic | Microphones’ Model |
| MTM | Mouth-To-Microphone Distance |
| Env | Recording Environment |
| SR | Sampling Rate |
| FF | File Format |
| PP | Preprocessing Procedure |
| SwHw | Software / Hardware |
| FE | Feature Extraction Methods |
| FR | Frequency Range |
| AF | Analyzed Features |
| Ww | Windows Size |
Appendix A. Supplementary Material—Variable Descriptions
Appendix A.1. Participant Information
Appendix A.1.1. Number of Participants (Part)
Appendix A.1.2. Number of Cry Samples (Sam)
Appendix A.1.3. Age of the Infants (Age)
Appendix A.1.4. Sex of the Infants (Sex)
Appendix A.1.5. Trigger (Tri)
Appendix A.1.6. Position of the Infant during Recording (Pos)
Appendix A.1.7. Health Status of the Infants (Hea)
Appendix A.1.8. Additional Information
Appendix A.2. Data Collection
Appendix A.2.1. Microphone Used for Data Collection (Mic)

Appendix A.2.2. Microphone-to-Mouth Distance (Mtm)
Appendix A.2.3. Recording Environment (Env)
Appendix A.2.4. Sampling Rate of Recorded Signal (Sr)
Appendix A.2.5. File Format Used for Storage (Ff)
- Uncompressed files store the signal as it is, applying no content compression and resulting in files taking more space on digital drives.
- The lossless compressed format encodes in a way that reduces the size of an input file by creating a copy with the same acoustical properties that may have a smaller size, usually in the ratio 2:1 [57].
- To achieve a greater reduction in file space, a lossy compression algorithm can be used. Lossy compression achieves a higher compression ratio, usually around the ratio of 10:1, by reducing the audio quality of the signal. Although quality loss is almost imperceptible to human ears, modification of original signal influences the quality and accuracy of acoustical features estimated from it, such as F0. The most popular lossy file format is the MP3 format, which is widely used for music compression, but it is also employed in the research environment.
Appendix A.3. Methods and Data Analysis Information
Appendix A.3.1. Preprocessing Procedure (Pp)
Appendix A.3.2. Software and Hardware (Swhw)
Appendix A.3.3. Feature Extraction Method (Fe)
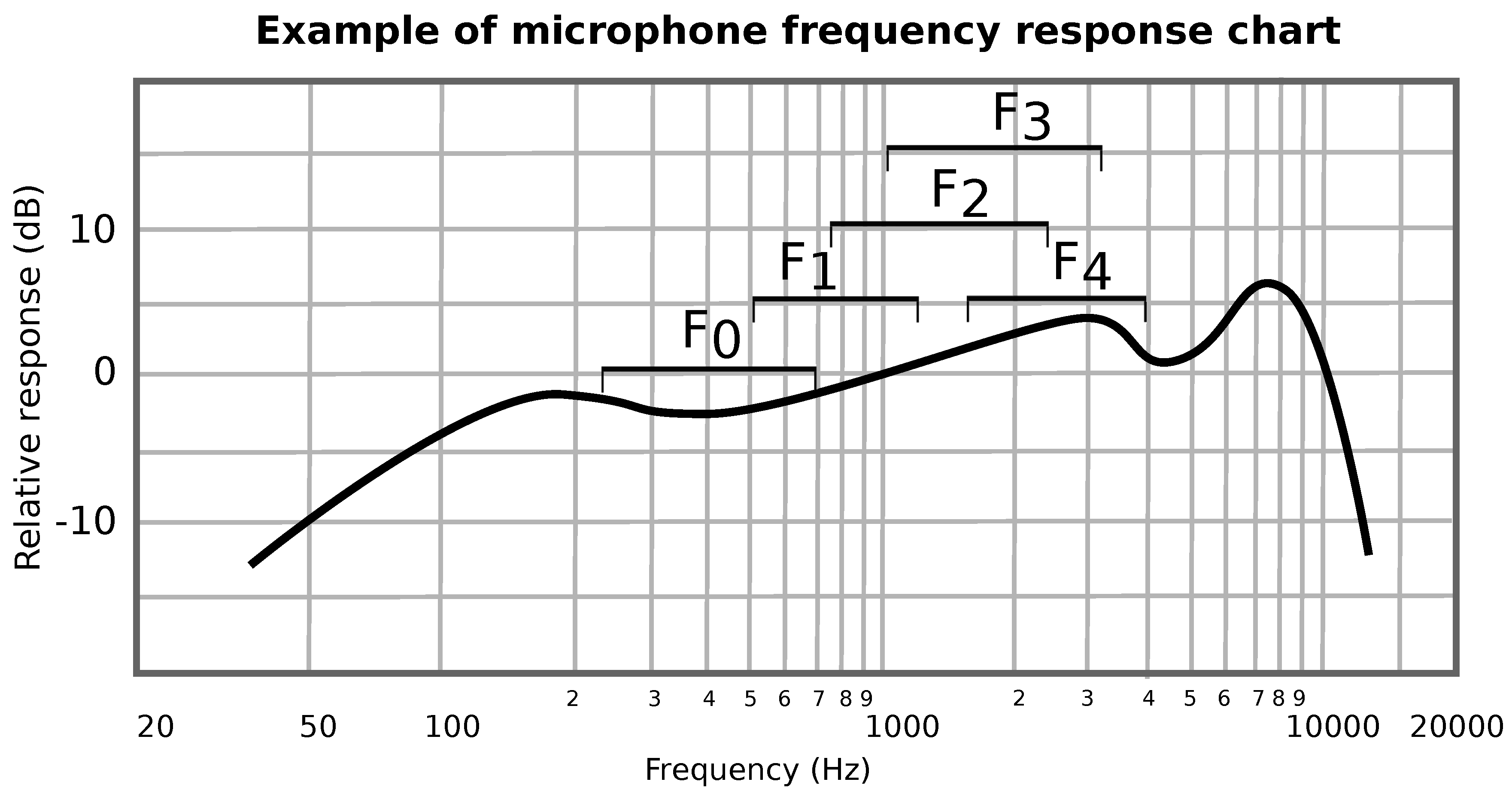
Appendix A.3.4. Analysed Frequency Range (Fr)
Appendix A.3.5. Analyzed Features (Af)
Appendix A.3.6. Window Size of the Signal during Feature Extraction (Ww)
Appendix B. Supplementary Material—Checklist
Appendix B.1. Participants’ Information
- □
- Number of participants: expressed as total number of participants of the study and with clear indication of the number of participants per group (if more than one group is present).
- □
- Number of samples: expressed as total number of samples recorded and with clear indication the number of samples per group (if more than one group is present) and of the number of samples per participant.
- □
- Age of the participants: statistics (mean, std, min, and max) age of the participants of the study for the whole set of participants and for the subset of participants per group (if more than one group is present). If possible, researchers should also indicate the gestational age at birth. Whenever possible, the weight of the participants should be reported as well.
- □
- Gender of the participants: total number of male and female participants and reported per group (if more than one group is present).
- □
- Cry trigger: information about the trigger that has been used to induce crying vocalizations in babies.
- □
- Posture during the recording: information about the position of the babies during the recordings (supine, prone, and seated).
- □
- Additional information: any other additional information that may help giving context to obtained results (e.g., language, ethnicity, and recruitment process).
Appendix B.2. Data Collection
- □
- Microphone model: the model of the microphone(s) used for recording.
- □
- Mouth-to-microphone distance: distance between the infants’ mouths and the microphone.
- □
- Recording environment: environment in which the data have been recorded (clinical or nonclinical). Additional information (e.g., was the baby familiar with the environment? Was the room soundproof and or silent? Was the temperature in room controlled? Was the level of humidity in the room controlled?) should be reported to clarify where data have been collected.
- □
- Sampling rate: Sampling rate of recorded signal (and resolution in bit).
- □
- File Format: format in which the file has been saved.
Appendix B.3. Methods and Analysis
- □
- Preprocessing procedure: detailed information about the preprocessing steps should be reported, included settings and parameters of employed tools and software.
- □
- Software and hardware: information about the software (with versions) and hardware (with model) employed in the research.
- □
- Feature extraction procedure: procedures that have been used to estimate analyzed features (if necessary).
- □
- Region of interest: frequency regions of interest of the signals that have been processed (e.g., between 100 and 4000 Hz).
- □
- Investigated features: list of features that have been analyzed.
- □
- Window size: size of the windows employed in the study, if any, including overlapping and step size.
References
- Esposito, G.; del Carmen Rostagno, M.; Venuti, P.; Haltigan, J.D.; Messinger, D.S. Brief Report: Atypical expression of distress during the separation phase of the strange situation procedure in infant siblings at high risk for ASD. J. Autism Dev. Disord. 2014, 44, 975–980. [Google Scholar] [CrossRef] [PubMed]
- Esposito, G.; Hiroi, N.; Scattoni, M.L. Cry, baby, cry: Expression of distress as a biomarker and modulator in autism spectrum disorder. Int. J. Neuropsychopharmacol. 2017, 20, 498–503. [Google Scholar] [CrossRef] [PubMed]
- Esposito, G.; Venuti, P. Understanding early communication signals in autism: a study of the perception of infants’ cry. J. Intellectual Disabil. Res. 2010, 54, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Ozturk, Y.; Bizzego, A.; Esposito, G.; Furlanello, C.; Venuti, P. Physiological and self-report responses of parents of children with autism spectrum disorder to children crying. Res. Dev. Disabil. 2018, 73, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Colton, R.; Steinschneider, A. The cry characteristics of an infant who died of the sudden infant death syndrome. J. Speech Hearing Disord. 1981, 46, 359–363. [Google Scholar] [CrossRef]
- Hariharan, M.; Yaacob, S.; Awang, S.A. Pathological infant cry analysis using wavelet packet transform and probabilistic neural network. Expert Syst. Appl. 2011, 38, 15377–15382. [Google Scholar] [CrossRef]
- LaGasse, L.L.; Neal, A.R.; Lester, B.M. Assessment of infant cry: acoustic cry analysis and parental perception. Ment. Retard. Dev. Disabil. Res. Rev. 2005, 11, 83–93. [Google Scholar] [CrossRef]
- Lester, B.M.; Corwin, M.; Golub, H. Early detection of the infant at risk through cry analysis. In The Physiological Control of Mammalian Vocalization; Springer: Berlin, Germany, 1988; pp. 395–411. [Google Scholar]
- Manfredi, C.; Bocchi, L.; Orlandi, S.; Spaccaterra, L.; Donzelli, G. High-resolution cry analysis in preterm newborn infants. Med. Eng. Phys. 2009, 31, 528–532. [Google Scholar] [CrossRef]
- Michelsson, K.; Michelsson, O. Phonation in the newborn, infant cry. Int. J. Pediatr. Otorhinolaryngol. 1999, 49, S297–S301. [Google Scholar] [CrossRef]
- Esposito, G.; Nakazawa, J.; Venuti, P.; Bornstein, M.H. Componential deconstruction of infant distress vocalizations via tree-based models: A study of cry in autism spectrum disorder and typical development. Res. Dev. Disabil. 2013, 34, 2717–2724. [Google Scholar] [CrossRef]
- Wasz-Hockert, O. The infant cry: A spectrographic and auditory analysis. Clin. Dev. Med. 1968, 29, 1–42. [Google Scholar]
- Sheinkopf, S.J.; Iverson, J.M.; Rinaldi, M.L.; Lester, B.M. Atypical cry acoustics in 6-month-old infants at risk for autism spectrum disorder. Autism Res. 2012, 5, 331–339. [Google Scholar] [CrossRef] [PubMed]
- Unwin, L.M.; Bruz, I.; Maybery, M.T.; Reynolds, V.; Ciccone, N.; Dissanayake, C.; Hickey, M.; Whitehouse, A.J. Acoustic properties of cries in 12-month old infants at high-risk of autism spectrum disorder. J. Autism Dev. Disord. 2017, 47, 2108–2119. [Google Scholar] [CrossRef] [PubMed]
- Garcia, J.O.; Garcia, C.R. Mel-frequency cepstrum coefficients extraction from infant cry for classification of normal and pathological cry with feed-forward neural networks. In Proceedings of the 2003 IEEE International Joint Conference on Neural Networks, Portland, OR, USA, 20–24 July 2003; Volume 4, pp. 3140–3145. [Google Scholar]
- Várallyay, G. Future prospects of the application of the infant cry in the medicine. Period. Polytech. Electr. Eng. 2006, 50, 47–62. [Google Scholar]
- Etz, T.; Reetz, H.; Wegener, C.; Bahlmann, F. Infant cry reliability: acoustic homogeneity of spontaneous cries and pain-induced cries. Speech Commun. 2014, 58, 91–100. [Google Scholar] [CrossRef]
- Wermke, K.; Mende, W.; Borschberg, H.; Ruppert, R. Changes of voice parameters and melody patterns during the first year of life in human twins. J. Acoust. Soc. Am. 1999, 105, 1303–1304. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Annals Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Esposito, G.; Gabrieli, G. Replication Data for: Are Cry Studies Replicable? An Analysis of Participants, Setups, and Methods Adopted and Reported in Cry Studies; Nanyang Technological University: Singapore, 2019. [Google Scholar]
- Robb, M.P.; Crowell, D.H.; Dunn-Rankin, P. Sudden infant death syndrome: cry characteristics. Int. J. Pediatr. Otorhinolaryngol. 2013, 77, 1263–1267. [Google Scholar] [CrossRef]
- Sahin, M.; Sahin, S.; Sari, F.N.; Tatar, E.C.; Uras, N.; Oguz, S.S.; Korkmaz, M.H. Utilizing Infant Cry Acoustics to Determine Gestational Age. J. Voice 2017, 31, 506.e1. [Google Scholar] [CrossRef]
- Borysiak, A.; Hesse, V.; Wermke, P.; Hain, J.; Robb, M.; Wermke, K. Fundamental frequency of crying in two-month-old boys and girls: Do sex hormones during mini-puberty mediate differences? J. Voice 2017, 31, 128.e21. [Google Scholar] [CrossRef]
- Goberman, A.M.; Whitfield, J.A. Acoustics of Infant Pain Cries: Fundamental Frequency as a Measure of Arousal. Perspect. Speech Sci. Orofac. Disord. 2013, 23, 18–26. [Google Scholar] [CrossRef]
- Reyes-Galaviz, O.F.; Reyes-Garcia, C.A. A system for the processing of infant cry to recognize pathologies in recently born babies with neural networks. In Proceedings of the 9th Conference Speech and Computer, Saint-Petersburg, Russia, 20–22 Septemeber 2004. [Google Scholar]
- Robb, M.P.; Cacace, A.T. Estimation of formant frequencies in infant cry. Int. J. Pediatr. Otorhinolaryngol. 1995, 32, 57–67. [Google Scholar] [CrossRef]
- Hawkins, D.M. The problem of overfitting. J. Chem. Inf. Comput. Sci. 2004, 44, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Hurvich, C.M.; Tsai, C.L. Regression and time series model selection in small samples. Biometrika 1989, 76, 297–307. [Google Scholar] [CrossRef]
- Babyak, M.A. What you see may not be what you get: A brief, nontechnical introduction to overfitting in regression-type models. Psychosom. Med. 2004, 66, 411–421. [Google Scholar]
- Esposito, G.; Venuti, P. Developmental changes in the fundamental frequency (f0) of infants’ cries: A study of children with Autism Spectrum Disorder. Early Child Dev. Care 2010, 180, 1093–1102. [Google Scholar] [CrossRef]
- Cacace, A.T.; Robb, M.P.; Saxman, J.H.; Risemberg, H.; Koltai, P. Acoustic features of normal-hearing pre-term infant cry. Int. J. Pediatr. Otorhinolaryngol. 1995, 33, 213–224. [Google Scholar] [CrossRef]
- Fuller, B.F.; Horii, Y. Spectral energy distribution in four types of infant vocalizations. J. Commun. Dis. 1988, 21, 251–261. [Google Scholar] [CrossRef]
- Sharma, S.; Asthana, S.; Mittal, V.K. A database of infant cry sounds to study the likely cause of cry. In Proceedings of the 12th International Conference on Natural Language Processing, Trivandrum, India, 11–14 December 2015; pp. 112–117. [Google Scholar]
- Parga, J.J.; Lewin, S.; Lewis, J.; Montoya-Williams, D.; Alwan, A.; Shaul, B.; Han, C.; Bookheimer, S.Y.; Eyer, S.; Dapretto, M.; et al. Defining and distinguishing infant behavioral states using acoustic cry analysis: Is colic painful? Pediatr. Res. 2019, 1–6. [Google Scholar] [CrossRef]
- Goberman, A.M.; Johnson, S.; Cannizzaro, M.S.; Robb, M.P. The effect of positioning on infant cries: Implications for sudden infant death syndrome. Int. J. Pediatr. Otorhinolaryngol. 2008, 72, 153–165. [Google Scholar] [CrossRef]
- Goto, K.; Maeda, T.; Mirmiran, M.; Ariagno, R. Effects of prone and supine position on sleep characteristics in preterm infants. Psychiatr. Clin. Neurosci. 1999, 53, 315–317. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.J.; Anderson, G.C.; Lin, C.H. Effects of prone and supine positions on sleep state and stress responses in mechanically ventilated preterm infants during the first postnatal week. J. Adv. Nurs. 2002, 40, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Esposito, G.; Venuti, P. Comparative analysis of crying in children with autism, developmental delays, and typical development. Focus Autism Other Dev. Disabil. 2009, 24, 240–247. [Google Scholar] [CrossRef]
- Woods, J.J.; Wetherby, A.M. Early identification of and intervention for infants and toddlers who are at risk for autism spectrum disorder. Lang. Speech Hearing Serv. Schools 2003, 34, 180–193. [Google Scholar] [CrossRef]
- Sheinkopf, S.J.; Mundy, P.; Oller, D.K.; Steffens, M. Vocal atypicalities of preverbal autistic children. J. Autism Dev. Disord. 2000, 30, 345–354. [Google Scholar] [CrossRef]
- Möller, S.; Schönweiler, R. Analysis of infant cries for the early detection of hearing impairment1. Speech Commun. 1999, 28, 175–193. [Google Scholar] [CrossRef]
- Etz, T.; Reetz, H.; Wegener, C. A classification model for infant cries with hearing impairment and unilateral cleft lip and palate. Folia Phoniatr. Logop. 2012, 64, 254–261. [Google Scholar] [CrossRef]
- Mampe, B.; Friederici, A.D.; Christophe, A.; Wermke, K. Newborns’ cry melody is shaped by their native language. Curr. Biol. 2009, 19, 1994–1997. [Google Scholar] [CrossRef]
- Manfredi, C.; Pieraccini, G.; Viellevoye, R.; Reyes-García, A.T.G.C. Relationships between newborns’cry melody shapes and native language. In Models and Analysis of Vocal Emissions for Biomedical Applications: 10th International Workshop, 13–15 December 2017; Firenze University Press: Firenze, Italy, 2017; Volume 117, p. 47. [Google Scholar]
- Beranek, L.L.; Beranek, L.L.; Beranek, L.L.; Beranek, L.L. Acoustical Measurements; Acoustical Society of America: Melville, NY, USA, 1988. [Google Scholar]
- Eargle, J. The Microphone Book: From Mono to Stereo to Surround-a Guide to Microphone Design and Application; CRC Press: Boca Raton, FL, USA, 2012. [Google Scholar]
- Everest, F.A. Master handbook of acoustics. J. Acoust. Soc. Am. 2001, 110, 1714. [Google Scholar] [CrossRef]
- Kuttruff, H. Room Acoustics; CRC Press: Boca Raton, FL, USA, 2014. [Google Scholar]
- Ross, G.; Kagan, J.; Zelazo, P.; Kotelchuck, M. Separation protest in infants in home and laboratory. Dev. Psychol. 1975, 11, 256. [Google Scholar] [CrossRef]
- Simner, M.L. Newborn’s response to the cry of another infant. Dev. Psychol. 1971, 5, 136. [Google Scholar] [CrossRef]
- Sagi, A.; Hoffman, M.L. Empathic distress in the newborn. Dev. Psychol. 1976, 12, 175. [Google Scholar] [CrossRef]
- Martin, G.B.; Clark, R.D. Distress crying in neonates: Species and peer specificity. Dev. Psychol. 1982, 18, 3. [Google Scholar] [CrossRef]
- Warner, R.M. Spectral Analysis of Time-Series Data; Guilford Press: New York, NY, USA, 1998. [Google Scholar]
- Cook, P.R. Real Sound Synthesis for Interactive Applications; AK Peters/CRC Press: Boca Raton, FL, USA, 2002. [Google Scholar]
- Robin, M.; Gutjahr, A.; Sudicky, E.; Wilson, J. Cross-correlated random field generation with the direct Fourier transform method. Water Resour. Res. 1993, 29, 2385–2397. [Google Scholar] [CrossRef]
- Watkinson, J. Introduction to Digital Audio; Focal Press: Waltham, MA, USA, 2013. [Google Scholar]
- Hans, M.; Schafer, R.W. Lossless compression of digital audio. IEEE Signal Process. Mag. 2001, 18, 21–32. [Google Scholar] [CrossRef]
- Sreedhar, S. The Future of Music. Available online: http://emmanuelderuty.com/pages/dynamics/Biblio/2007_Sreedhar%20The%20Future%20of%20Music%20-%20IEEE%20Spectrum.pdf (accessed on 4 December 2019).
- Laroche, J.; Dolson, M. New phase-vocoder techniques are real-time pitch shifting, chorusing, harmonizing, and other exotic audio modifications. J. Audio Eng. Soc. 1999, 47, 928–936. [Google Scholar]
- Smith, J.O. Introduction to Digital Filters: With Audio Applications; W3K Publishing: Stanford, CA, USA, 2007; Volume 2. [Google Scholar]
- Corwin, M.J.; Lester, B.M.; Golub, H.L. The infant cry: What can it tell us? Curr. Probl. Pediatr. 1996, 26, 313–334. [Google Scholar] [CrossRef]
- Gabrieli, G.; Leck, W.Q.; Bizzego, A.; Esposito, G. Are Praat’s default settings optimal for Infant cry analysis? In Proceedings of the 2019 CCRMA Linux Audio Conference, LAC, Stanford, LA, USA, 23–26 March 2019; pp. 83–88. [Google Scholar]
- Bornstein, M.; Costlow, K.; Truzzi, A.; Esposito, G. Categorizing the cries of infants with ASD versus typically developing infants: A study of adult accuracy and reaction time. Res. Autism Spect. Disord. 2016, 31, 66–72. [Google Scholar] [CrossRef]
- Boersma, P. Praat, a system for doing phonetics by computer. Glot Int. 2002, 5. [Google Scholar]
- Várallyay, G. SSM—A Novel Method to Recognize the Fundamental Frequency in Voice Signals. Iberoamerican Congress on Pattern Recognition; Springer: Berlin, Germany, 2007; pp. 88–95. [Google Scholar]
- Chu, W.; Alwan, A. SAFE: A statistical approach to F0 estimation under clean and noisy conditions. IEEE Trans. Audio Speech Lang. Process. 2012, 20, 933–944. [Google Scholar] [CrossRef]
- Zabidi, A.; Mansor, W.; Khuan, L.Y.; Sahak, R.; Rahman, F.Y.A. Mel-frequency cepstrum coefficient analysis of infant cry with hypothyroidism. In Proceedings of the 5th International Colloquium on IEEE Signal Processing & Its Applications, CSPA 2009, Kuala Lumpur, Malaysia, 6–8 March 2009; pp. 204–208. [Google Scholar]
- Tahon, M.; Devillers, L. Towards a small set of robust acoustic features for emotion recognition: Challenges. IEEE/ACM Trans. Audio Speech Lang. Process. 2016, 24, 16–28. [Google Scholar] [CrossRef]
- Harris, F. Windows, Harmonic Analysis, and the Discrete Fourier Transform; Naval Undersea Center: San Diego, CA, USA, 1969. [Google Scholar]
Sample Availability: The dataset generated for this publication is available on the Data Repository of the Nanyang Technological University https://doi.org/10.21979/N9/UDQBEK [20]. |



{kind=link}
{kind=link}
{kind=link}
| Variable | Abbr. | N | % | |
|---|---|---|---|---|
| Participants | Number of Participants | Part | 161 | 89% |
| Number of Samples | Sam | 122 | 68% | |
| Participants’ Age | Age | 133 | 74% | |
| Participants’ Gender | Sex | 71 | 39% | |
| Cry Trigger | Tri | 121 | 67% | |
| Participants’ Position | Pos | 55 | 30% | |
| Participants’ Health Status | Hea | 73 (77) | 95% | |
| Data Collection | Microphones’ Model | Mic | 112 | 62% |
| Mouth-To-Microphone Distance | MTM | 102 | 57% | |
| Recording Environment | Env | 106 | 59% | |
| Sampling Rate | SR | 115 | 64% | |
| File Format | FF | 69 | 38% | |
| Methods and Analysis | Preprocessing Procedure | PP | 98 | 54% |
| Software/Hardware | SwHw | 140 | 78% | |
| Feature Extraction Methods | FE | 150 | 83% | |
| Frequency Range | FR | 31 | 17% | |
| Analyzed Features | AF | 161 | 89% | |
| Windows Size | Ww | 53 | 29% |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gabrieli, G.; Scapin, G.; Bornstein, M.H.; Esposito, G. Are Cry Studies Replicable? An Analysis of Participants, Procedures, and Methods Adopted and Reported in Studies of Infant Cries. Acoustics 2019, 1, 866-883. https://doi.org/10.3390/acoustics1040052
Gabrieli G, Scapin G, Bornstein MH, Esposito G. Are Cry Studies Replicable? An Analysis of Participants, Procedures, and Methods Adopted and Reported in Studies of Infant Cries. Acoustics. 2019; 1(4):866-883. https://doi.org/10.3390/acoustics1040052
Chicago/Turabian StyleGabrieli, Giulio, Giulia Scapin, Marc H. Bornstein, and Gianluca Esposito. 2019. "Are Cry Studies Replicable? An Analysis of Participants, Procedures, and Methods Adopted and Reported in Studies of Infant Cries" Acoustics 1, no. 4: 866-883. https://doi.org/10.3390/acoustics1040052
APA StyleGabrieli, G., Scapin, G., Bornstein, M. H., & Esposito, G. (2019). Are Cry Studies Replicable? An Analysis of Participants, Procedures, and Methods Adopted and Reported in Studies of Infant Cries. Acoustics, 1(4), 866-883. https://doi.org/10.3390/acoustics1040052