
Postoperative Recurrence of Crohn’s Disease–Is the Early Use of Postoperative Immunomodulators Able to Modify Prognosis?


 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Study Design
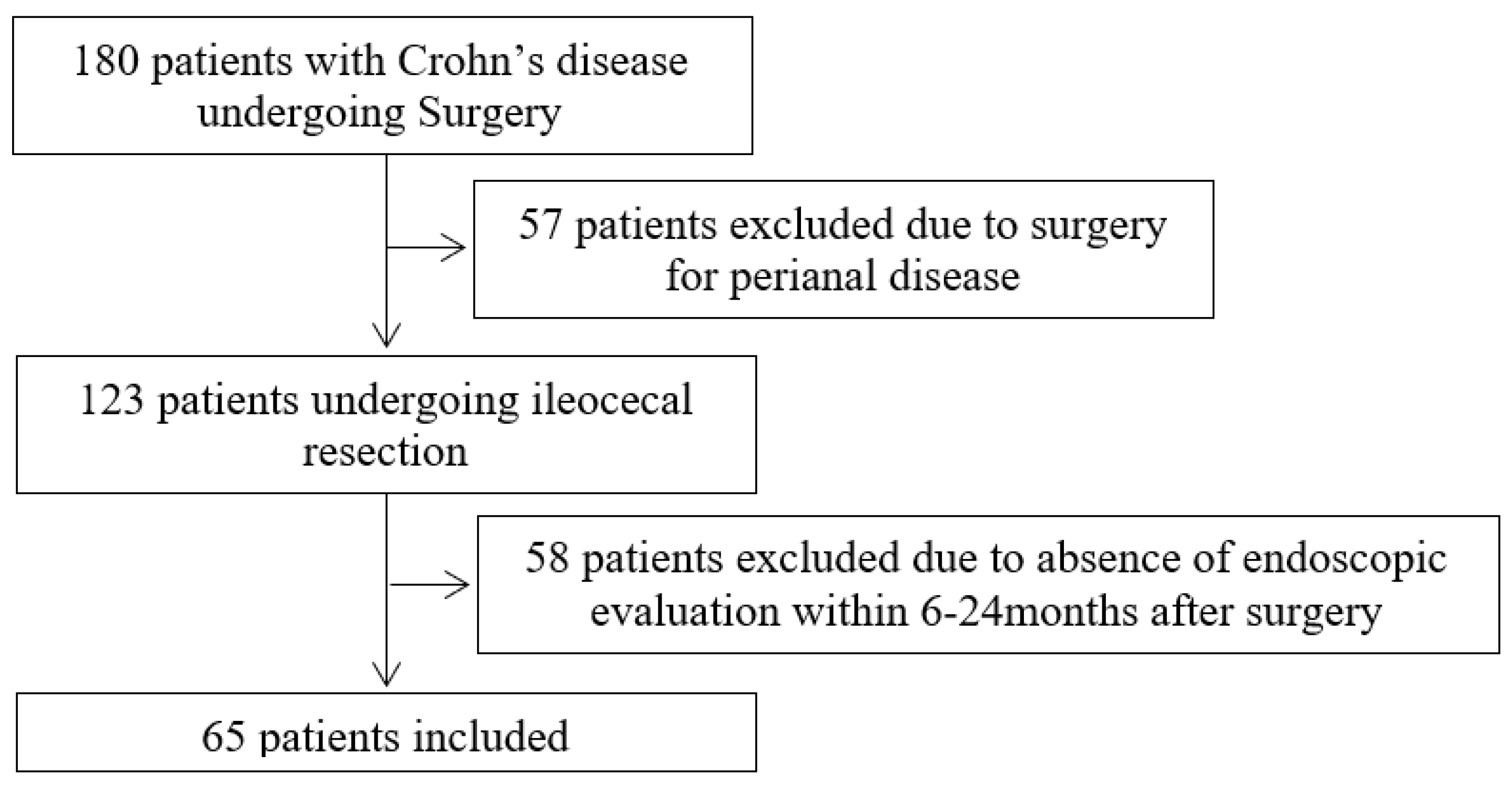
2.2. Study Population
3. Outcomes
3.1. Surgical Procedures
3.2. Histopathological Analysis
3.3. Statistical Analysis
4. Results
4.1. Study’s Population Characteristics
4.2. Univariate Analysis
4.3. Multivariable Analysis
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Statement of Ethics
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Centers for Disease Control and Prevention. Inflammatory Bowel Disease (IBD) 2021. Available online: www.cdc.gov/ibd/#epidIBD (accessed on 1 January 2023).
- Azevedo, L.F.; Magro, F.; Portela, F. Estimating the prevalence of inflammatory bowel disease in Portugal using a pharmaco-epidemiological approach. Pharmacoepidemiol. Drug Saf. 2010, 19, 499–510. [Google Scholar] [CrossRef]
- Torres, J.; Mehandru, S.; Colombel, J.F.; Peyrin-Biroulet, L. Crohn’s disease. Lancet 2017, 389, 1741–1755. [Google Scholar] [CrossRef] [PubMed]
- Buisson, A.; Chevaux, J.B.; Allen, P.B.; Bommelaer, G.; Peyrin-Biroulet, L. Review article: The natural history of postoperative Crohn’s disease recurrence. Aliment. Pharmacol. Ther. 2012, 35, 625–633. [Google Scholar] [CrossRef] [PubMed]
- Adamina, M.; Bonovas, S.; Raine, T.; Spinelli, A.; Warusavitarne, J.; Armuzzi, A.; Bachmann, O.; Bager, P.; Biancone, L.; Bokemeyer, B.; et al. ECCO Guidelines on Therapeutics in Crohn’s Disease: Surgical Treatment. J. Crohn’s Colitis 2020, 14, 155–168. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, T. Factors affecting recurrence after surgery for Crohn’s disease. World J. Gastroenterol. 2005, 11, 3971–3979. [Google Scholar] [CrossRef]
- Rivière, P.; Vermeire, S.; Irles-Depe, M.; Van Assche, G.; Rutgeerts, P.; Denost, Q.; Wolthuis, A.; D’hoore, A.; Laharie, D.; Ferrante, M. Rates of Postoperative Recurrence of Crohn’s Disease and Effects of Immunosuppressive and Biologic Therapies. Clin. Gastroenterol. Hepatol. 2021, 19, 713–720.e1. [Google Scholar] [CrossRef]
- Frolkis, A.D.; Dykeman, J.; Negrón, M.E.; Debruyn, J.; Jette, N.; Fiest, K.M.; Frolkis, T.; Barkema, H.W.; Rioux, K.P.; Panaccione, R.; et al. Risk of surgery for inflammatory bowel diseases has decreased over time: A systematic review and meta-analysis of population-based studies. Gastroenterology 2013, 145, 996–1006. [Google Scholar] [CrossRef]
- O’Connor, A.; Hamlin, P.J.; Taylor, J.; Selinger, C.; Scott, N.; Ford, A.C. Postoperative prophylaxis in Crohn’s disease after intestinal resection: A retrospective analysis. Frontline Gastroenterol. 2017, 8, 203–209. [Google Scholar] [CrossRef]
- Rutgeerts, P.; Geboes, K.; Vantrappen, G.; Beyls, J.; Kerremans, R.; Hiele, M. Predictability of the postoperative course of Crohn’s disease. Gastroenterology 1990, 99, 956–963. [Google Scholar] [CrossRef]
- Rivière, P.; Vermeire, S.; Irles-Depe, M.; Van Assche, G.; Rutgeerts, P.; de Buck van Overstraeten, A.; Denost, Q.; Wolthuis, A.; D’hoore, A.; Laharie, D.; et al. No Change in Determining Crohn’s Disease Recurrence or Need for Endoscopic or Surgical Intervention with Modification of the Rutgeerts’ Scoring System. Clin. Gastroenterol. Hepatol. 2019, 17, 1643–1645. [Google Scholar] [CrossRef]
- Dasharathy, S.S.; Limketkai, B.N.; Sauk, J.S. What’s New in the Postoperative Management of Crohn’s Disease? Dig. Dis. Sci. 2021, 67, 3508–3517. [Google Scholar] [CrossRef] [PubMed]
- Ha, F.J.; Thong, L.; Khalil, H. Quality of Life after Intestinal Resection in Patients with Crohn Disease: A Systematic Review. Dig. Surg. 2017, 34, 355–363. [Google Scholar] [CrossRef]
- Auzolle, C.; Nancey, S.; Tran-Minh, M.L.; Buisson, A.; Pariente, B.; Stefanescu, C.; Fumery, M.; Marteau, P.; Treton, X.; Hammoudi, N.; et al. Male gender, active smoking and previous intestinal resection are risk factors for post-operative endoscopic recurrence in Crohn’s disease: Results from a prospective cohort study. Aliment. Pharmacol. Ther. 2018, 48, 924–932. [Google Scholar] [CrossRef] [PubMed]
- Ryan, W.R.; Allan, R.N.; Yamamoto, T.; Keighley, M.R.B. Crohn’s disease patients who quit smoking have a reduced risk of reoperation for recurrence. Am. J. Surg. 2004, 187, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Reese, G.E.; Nanidis, T.; Borysiewicz, C.; Yamamoto, T.; Orchard, T.; Tekkis, P.P. The effect of smoking after surgery for Crohn’s disease: A meta-analysis of observational studies. Int. J. Color. Dis. 2008, 23, 1213–1221. [Google Scholar] [CrossRef]
- Colombo, F.; Frontali, A.; Baldi, C.; Cigognini, M.; Lamperti, G.; Manzo, C.A.; Maconi, G.; Ardizzone, S.; Foschi, D.; Sampietro, G.M. Repeated surgery for recurrent Crohn’s disease: Does the outcome keep worsening operation after operation? A comparative study of 1224 consecutive procedures. Updates Surg. 2021, 74, 73–80. [Google Scholar] [CrossRef]
- Simillis, C.; Yamamoto, T.; Reese, G.E.; Umegae, S.; Matsumoto, K.; Darzi, A.W.; Tekkis, P.P. A meta-analysis comparing incidence of recurrence and indication for reoperation after surgery for perforating versus nonperforating Crohn’s disease. Am. J. Gastroenterol. 2008, 103, 196–205. [Google Scholar] [CrossRef]
- Raab, Y.; Bergström, R.; Ejerblad, S.; Graf, W.; Påhlman, L. Factors influencing recurrence in Crohn’s disease. An analysis of a consecutive series of 353 patients treated with primary surgery. Dis. Colon Rectum 1996, 39, 918–925. [Google Scholar] [CrossRef]
- Krause, U.; Ejerblad, S.; Bergman, L. A long-term study of the clinical course in 186 patients. Scand. J. Gastroenterol. 1985, 20, 516–524. [Google Scholar] [CrossRef]
- Gionchetti, P.; Dignass, A.; Danese, S.; Dias, F.J.M.; Rogler, G.; Lakatos, P.L.; Adamina, M.; Ardizzone, S.; Buskens, C.J.; Sebastian, S.; et al. 3rd European evidence-based consensus on the diagnosis and management of Crohn’s disease 2016: Part 2: Surgical management and special situations. J. Crohn’s Colitis 2017, 11, 135–149. [Google Scholar] [CrossRef]
- Fornaro, R.; Caratto, E.; Caratto, M.; Fornaro, F.; Caristo, G.; Frascio, M.; Sticchi, C. Post-operative recurrence in Crohn’s disease: Critical analysis of potential risk factors. An update. Surgeon 2015, 13, 330–347. [Google Scholar] [CrossRef] [PubMed]
- Fazio, V.W.; Marchetti, F.; Church, J.M.; Goldblum, J.R.; Lavery, L.C.; Hull, T.L.; Milsom, J.W.; Strong, S.A.; Oakley, J.R.; Secic, M. Effect of resection margins on the recurrence of Crohn’s disease in the small bowel: A randomized controlled trial. Ann. Surg. 1996, 224, 563–573. [Google Scholar] [CrossRef] [PubMed]
- Bernell, O.; Lapidus, A.; Hellers, G. Risk factors for surgery and postoperative recurrence in Crohn’s disease. Ann. Surg. 2000, 231, 38–45. [Google Scholar] [CrossRef]
- Regueiro, M.; Velayos, F.; Greer, J.B.; Bougatsos, C.; Chou, R.; Sultan, S.; Singh, S. American Gastroenterological Association Institute Technical Review on the Management of Crohn’s Disease after Surgical Resection. Gastroenterology 2017, 152, 277–295.e3. [Google Scholar] [CrossRef] [PubMed]
- Sachar, D.B.; Wolfson, D.M.; Greenstein, A.J.; Goldberg, J.; Styczynski, R.; Janowitz, H.D. Risk factors for postoperative recurrence of Crohn’s disease. Gastroenterology 1983, 85, 917–921. [Google Scholar] [CrossRef] [PubMed]
- Bressenot, A.; Peyrin-Biroulet, L. Histologic features predicting postoperative Crohn’s disease recurrence. Inflamm. Bowel Dis. 2015, 21, 468–475. [Google Scholar] [CrossRef] [PubMed]
- Valibouze, C.; Desreumaux, P.; Zerbib, P. Post-surgical recurrence of Crohn’s disease: Situational analysis and future prospects. J. Visc. Surg. 2021, 158, 401–410. [Google Scholar] [CrossRef]
- Tandon, P.; Malhi, G.; Abdali, D.; Pogue, E.; Marshall, J.K.; de Buck van Overstraeten, A.; Riddell, R.; Narula, N. Active Margins, Plexitis, and Granulomas Increase Postoperative Crohn’s Recurrence: Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2021, 19, 451–462. [Google Scholar] [CrossRef]
- Simillis, C.; Jacovides, M.; Reese, G.E.; Yamamoto, T.; Tekkis, P.P. Meta-analysis of the role of granulomas in the recurrence of crohn disease. Dis. Colon Rectum 2010, 53, 177–185. [Google Scholar] [CrossRef]
- Hammoudi, N.; Cazals-Hatem, D.; Auzolle, C.; Gardair, C.; Ngollo, M.; Bottois, H.; Nancey, S.; Pariente, B.; Buisson, A.; Treton, X.; et al. Association between Microscopic Lesions at Ileal Resection Margin and Recurrence after Surgery in Patients with Crohn’s Disease. Clin. Gastroenterol. Hepatol. 2020, 18, 141–149.e2. [Google Scholar] [CrossRef]
- Barreiro-de Acosta, M.; Marín-Jimenez, I.; Rodríguez-Lago, I.; Guarner, F.; Espín, E.; Ferrer Bradley, I.; Gutiérrez, A.; Beltrán, B.; Chaparro, M.; Gisbert, J.P.; et al. Recommendations of the Spanish Working Group on Crohn’s Disease and Ulcerative Colitis (GETECCU) on pouchitis in ulcerative colitis. Part 2: Treatment. Gastroenterol. Hepatol. 2020, 43, 649–658. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, G.C.; Loftus, E.V.; Hirano, I.; Falck-Ytter, Y.; Singh, S.; Sultan, S.; Flamm, S.L.; Lim, J.K.; Rubenstein, J.H.; Smalley, W.E.; et al. American Gastroenterological Association Institute Guideline on the Management of Crohn’s Disease after Surgical Resection. Gastroenterology 2017, 152, 271–275. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.R.; Ow, Z.G.W.; Chin, Y.H.; Lim, W.H.; Kong, G.; Tham, H.Y.; Wong, N.W.; Chong, C.S.; Foo, F.J.; Chan, W.P.W. Quantifying the rate of recurrence of postoperative Crohn’s disease with biological therapy. A meta-analysis. J. Dig. Dis. 2021, 22, 399–407. [Google Scholar] [CrossRef]
- Dulai, P.S.; Singh, S.; Vande Casteele, N.; Boland, B.S.; Rivera-Nieves, J.; Ernst, P.B.; Eckmann, L.; Barrett, K.E.; Chang, J.T.; Sandborn, W.J. Should We Divide Crohn’s Disease into Ileum-Dominant and Isolated Colonic Diseases? Clin. Gastroenterol. Hepatol. 2019, 17, 2634–2643. [Google Scholar] [CrossRef]
- Atreya, R.; Siegmund, B. Location is important: Differentiation between ileal and colonic Crohn’s disease. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 544–558. [Google Scholar] [CrossRef] [PubMed]
- Renna, S.; Cammà, C.; Modesto, I.; Cabibbo, G.; Scimeca, D.; Civitavecchia, G.; Mocciaro, F.; Orlando, A.; Enea, M.; Cottone, M. Meta-Analysis of the Placebo Rates of Clinical Relapse and Severe Endoscopic Recurrence in Postoperative Crohn’s Disease. Gastroenterology 2008, 135, 1500–1509. [Google Scholar] [CrossRef]
- Candia, R.; Bravo-Soto, G.; Monrroy, H.; Hernandez, C.; Nguyen, G.C. Colonoscopy-guided therapy for the prevention of post-operative recurrence of Crohn’s disease. Cochrane Database Syst. Rev. 2020. [Google Scholar] [CrossRef]
- Regueiro, M.; Feagan, B.G.; Zou, B.; Johanns, J.; Blank, M.A.; Chevrier, M.; Plevy, S.; Popp, J.; Cornillie, F.J.; Lukas, M.; et al. Infliximab Reduces Endoscopic, but Not Clinical, Recurrence of Crohn’s Disease after Ileocolonic Resection. Gastroenterology 2016, 150, 1568–1578. [Google Scholar] [CrossRef]
- Kotze, P.G.; Yamamoto, T.; Danese, S.; Suzuki, Y.; Teixeira, F.V.; De Albuquerque, I.C.; Saad-Hossne, R.; de Barcelos, I.F.; da Silva, R.N.; Kotze, L.M.d.S.; et al. Direct retrospective comparison of adalimumab and infliximab in preventing early postoperative endoscopic recurrence after ileocaecal resection for Crohn’s disease: Results from the MULTIPER database. J. Crohn’s Colitis 2015, 9, 541–547. [Google Scholar] [CrossRef]
- Ananthakrishnan, A.N. Surgery for Crohn’s disease: Look harder, act faster. Lancet 2015, 385, 1370–1371. [Google Scholar] [CrossRef]
- Haens, G.R.D.; Geboes, K.; Peeters, M.; Baert, F.; Penninckx, F.; Rutgeerts, P. Early Lesions of Recurrent Crohn’s Disease Caused by Infusion. Gastroenterology 1998, 114, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Rutgeerts, P.; Goboes, K.; Peeters, M.; Hiele, M.; Penninckx, F.; Aerts, R.; Kerremans, R.; Goboes, K. Effect of faecal stream diversion on recurrence of Crohn’s disease in the neoterminal ileum Histological techniques. Lancet 1991, 338, 771–774. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristic | POR (N = 29) | No POR (N = 36) | OR | p-Value | |
|---|---|---|---|---|---|
| Age at the diagnosis (years) median (IQR) | 26 (13) | 24 (12) | 1.02 | 0.22 | |
| Gender (male), % | 48.3% | 50% | 1.07 | 0.89 | |
| Active smoking, % | 53.8% | 30% | 2.72 | 0.074 | |
| Family history of IBD, % | 25% | 11.1% | 2.67 | 0.221 | |
| Behavior of disease (stricturing, penetrating), % | 44.8; 55.2% | 38.9; 41.7% | 2.19 | 0.05 | * |
| Perianal disease, % | 17.2% | 16.7% | 1.04 | 0.951 | |
| Time from diagnosis to surgery (years) median (IQR) | 8.5 (13) | 2 (11) | 0.94 | 0.06 | |
| Previous abdominal surgery for CD, % | 20.7% | 5.9% | 4.17 | 0.097 | |
| Biologics or Azathioprine before the surgery, % | 37.9% | 66.7% | 0.55 | 0.023 | * |
| Extension of resection (centimeters) median (IQR) | 24.5 (21) | 22.5 (18) | 1 | 0.808 | |
| Plexitis, % | 93.1% | 94.4% | 0.79 | 0.823 | |
| Granulomas, % | 20.7% | 38.9% | 0.41 | 0.119 | |
| Transmural inflammation in the margin | 6.9% | 13.9% | 0.46 | 0.375 | |
| Biologics or Azathioprine maintenance or initiation < 8 weeks, % | 55.2% | 55.6% | 0.98 | 0.975 |
| Characteristic | EPI (N = 36) | No EPI (N = 29) | p-Value | |
|---|---|---|---|---|
| Age at the diagnosis (years) median (IQR) | 23 (9.5) | 30 (24) | 0.007 | * |
| Gender (male), % | 47.2% | 50% | 0.524 | |
| Smoking, % | 37.5% | 45.8% | 0.531 | |
| Family history of IBD, % | 20% | 13.6% | 0.564 | |
| Behavior of disease (stricturing, penetrating), % | 30.6%, 61.1% | 55.2%; 31% | 0.039 | * |
| Perianal disease, % | 25% | 6.9% | 0.069 | |
| Previous abdominal surgery for CD, % | 19.4% | 3.5% | 0.083 | |
| Time from diagnosis to surgery (years) median (IQR) | 8.5 (14) | 4 (10) | 0.026 | * |
| Biologics or Azathioprine before the surgery, % | 69.4% | 34.5% | 0.005 | * |
| Extension of resection (centimeters) median (IQR) | 24 (18) | 20 (12) | 0.268 | |
| Plexitis, % | 91.7% | 96.6% | 0.43 | |
| Granulomas, % | 25% | 37.9% | 0.264 |
| Predictor | p-Value | |
|---|---|---|
| Age at the diagnosis (years) (A1 (≤16) vs. A2 (17–39)/A3 (≥40)) | 0.13 | |
| Gender | 0.678 | |
| Active smoking | 0.289 | |
| Family history of IBD | 0.566 | |
| Behavior of disease (Inflammatory vs. Stricturing/Penetrating) | 0.05 | * |
| Perianal disease | 0.862 | |
| Time from diagnosis to surgery (years) < 5 years; ≥5 years | 0.023 | * |
| Previous abdominal surgery for CD | 0.159 | |
| Biologics or Azathioprine before the surgery | 0.007 | * |
| Extension of resection of ileum > 10 cm | 0.057 | |
| Biologics or Azathioprine maintenance or initiation < 3 months; ≥3 months | 0.316 | |
| Plexitis | 0.722 | |
| Granulomas | 0.203 | |
| Transmural inflammation in the margin | 0.879 |
| Logistic Regression | Cox Regression | |||||||
|---|---|---|---|---|---|---|---|---|
| Predictor | OR | 95% CI | p-Value | HR | 95% CI | p-Value | ||
| Age at diagnosis | 1.01 | 0.46–2.22 | 0.979 | |||||
| Smoking | 1.94 | 0.51–7.36 | 0.33 | |||||
| Behavior of disease | 2.49 | 0.73–8.48 | 0.145 | 7.53 | 0.94–60.4 | 0.057 | ||
| Time from diagnosis to surgery (years) | 0.95 | 0.88–1.05 | 0.344 | 0.31 | 0.13–0.74 | 0.008 | * | |
| Previous abdominal surgery for CD | 11.1 | 1.18–104.33 | 0.035 | * | 5.85 | 1.76–19.45 | 0.004 | * |
| Biologics or Azathioprine before the surgery | 0.16 | 0.03–0.78 | 0.025 | * | 0.35 | 0.15–0.8 | 0.013 | * |
| Granulomas | 0.43 | 0.09–1.98 | 0.275 | |||||
| Biologics or Azathioprine maintenance or initiation < 8 weeks; ≥8 weeks | 0.75 | 0.14–4 | 0.738 | 0.67 | 0.28–1.6 | 0.372 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Temido, M.J.; Oliveira, R.C.; Silva, A.; Fontinha, G.N.; Lopes, S.M.F.; Figueiredo, P.; Portela, F. Postoperative Recurrence of Crohn’s Disease–Is the Early Use of Postoperative Immunomodulators Able to Modify Prognosis? Gastrointest. Disord. 2023, 5, 419-430. https://doi.org/10.3390/gidisord5040034
Temido MJ, Oliveira RC, Silva A, Fontinha GN, Lopes SMF, Figueiredo P, Portela F. Postoperative Recurrence of Crohn’s Disease–Is the Early Use of Postoperative Immunomodulators Able to Modify Prognosis? Gastrointestinal Disorders. 2023; 5(4):419-430. https://doi.org/10.3390/gidisord5040034
Chicago/Turabian StyleTemido, Maria José, Rui Caetano Oliveira, Andrea Silva, Guilherme Nogueira Fontinha, Sandra Maria Fernandes Lopes, Pedro Figueiredo, and Francisco Portela. 2023. "Postoperative Recurrence of Crohn’s Disease–Is the Early Use of Postoperative Immunomodulators Able to Modify Prognosis?" Gastrointestinal Disorders 5, no. 4: 419-430. https://doi.org/10.3390/gidisord5040034
APA StyleTemido, M. J., Oliveira, R. C., Silva, A., Fontinha, G. N., Lopes, S. M. F., Figueiredo, P., & Portela, F. (2023). Postoperative Recurrence of Crohn’s Disease–Is the Early Use of Postoperative Immunomodulators Able to Modify Prognosis? Gastrointestinal Disorders, 5(4), 419-430. https://doi.org/10.3390/gidisord5040034