1. Introduction
Percutaneous nephrolithotomy (PCNL) is the standard procedure for treating large kidney stones, especially those measuring over 20 mm or staghorn stones [
1,
2]. The accurate placement of the tract into the renal collecting system is crucial for achieving complete stone removal and minimizing complications such as bleeding, organ injuries, and access failure. PCNL punctures can lead to serious complications. In some cases, percutaneous access may rely on interventional radiologists, which may not always be ideal for stone clearance, especially when there is no preoperative communication between groups [
3].
To improve PCNL outcomes, various advancements have been made in renal access techniques over the past decade. Computer-assisted navigation systems, such as the one developed by Rassweiler et al. in 2012 [
4], have allowed surgeons to visualize the relationship between calyceal anatomy and surgical instruments using radio-opaque markers and 3D-reconstructed preoperative computed tomography (CT) images. While these systems have improved access efficiency, they do not account for real-time kidney position during respiratory movements, which has led to the development of automated devices.
In 1997, Cadeddu, Stoianovici. et al. from the Urobotics Laboratory at Johns Hopkins Medical Institutions introduced the PAKY-RCM system [
4,
5], demonstrating its feasibility in a clinical trial involving 23 PCNL patients [
6]. Another automated device developed by the same laboratory, called AcuBot, was shown to outperform computer-assisted navigation systems and manual operation in percutaneous ablative targeting, as reported by Pollock et al. in 2010 [
7]. However, these systems have limitations, including their high cost, bulkiness, and complexity, which have hindered their widespread use in clinical settings.
A new system called ANT-X, developed by NDR Medical Technology, offers an efficient solution for percutaneous needle placement in PCNL. It is compact, user-friendly, and specifically designed for urologists performing PCNL. Animal studies using a pig model have demonstrated that the ANT-X device reduces radiation exposure and complications after the procedure [
8]. A human trial has shown that the use of the ANT-X device can achieve percutaneous access on the first attempt [
8].
In this study, we conducted a benchtop evaluation using a phantom kidney model to assess whether the ANT-X device offers advantages over traditional free-hand puncture, specifically in terms of reducing access time and radiation exposure to both the patient and the surgeon. Our choice to focus on percutaneous renal access as the first step in PCNL was based on the critical importance of precise needle access to a chosen nodule in this procedure.
By evaluating the performance of the ANT-X device in comparison to free-hand puncture, we aim to provide valuable insights into the potential benefits of incorporating this robotic-assisted system into PCNL procedures. The findings from this benchtop study will contribute to the understanding of the device’s efficacy, paving the way for future research and clinical trials involving live patients.
2. Study Objective
To compare the free-hand puncture technique with robotic-assisted puncture during fluoroscopy-guided PCNL on phantom kidney model in terms of efficiency (puncture time) and safety (fluoroscopy exposure). The surgeon’s self-assessment of confidence levels after each puncture was recorded as well.
3. Material and Methods
3.1. Study Design
This prospective single-center benchtop study was conducted at the University Malaya Medical Centre (UMMC), involving four urological residents from UMMC as participants. The study utilized renal phantom models, which were provided by NDR Medical Technology (Senai, Malaysia). The research was carried out in the urology suite at UMMC over a period of three months, from January to March 2022. Ethical approval by Malaysia Research Ethical Committee (202124-9805).
The study design aimed to evaluate the efficacy and potential advantages of the ANT-X system compared to traditional free-hand puncture techniques. By involving urological residents, who are in the early stages of their training and may have limited experience in PCNL needle puncture, the study aimed to assess the device’s usability and its potential to improve procedural outcomes for less-experienced surgeons.
Throughout the three-month study period, the participants performed multiple needle punctures using both free-hand and ANT-X methods on the renal phantom models. Data on puncture time, radiation exposure, and self-assessment of confidence levels were collected and analyzed.
The utilization of phantom models and a controlled environment allowed for standardized testing conditions, ensuring consistency and reproducibility in the evaluation of the ANT-X device’s performance.
3.2. Phantom Models
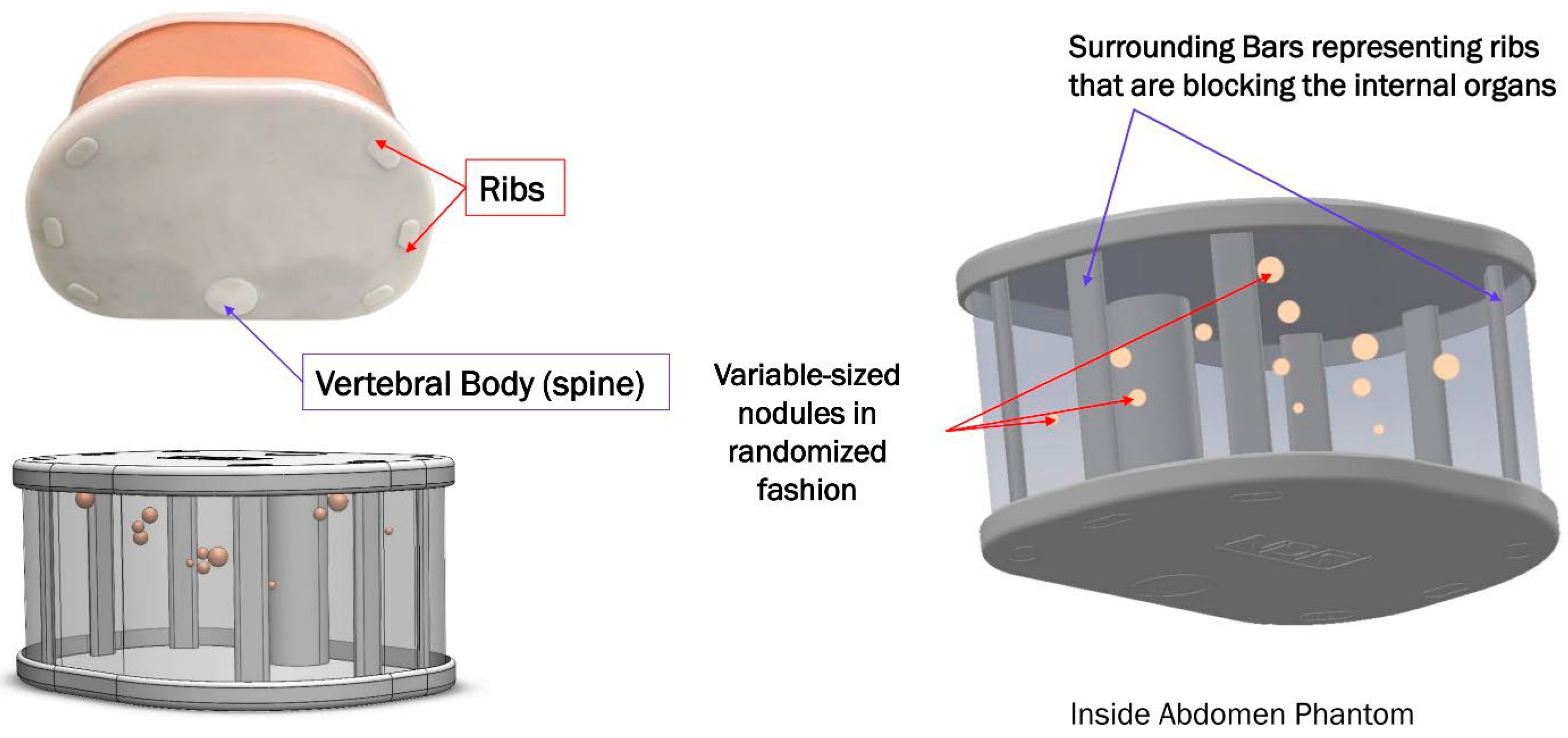
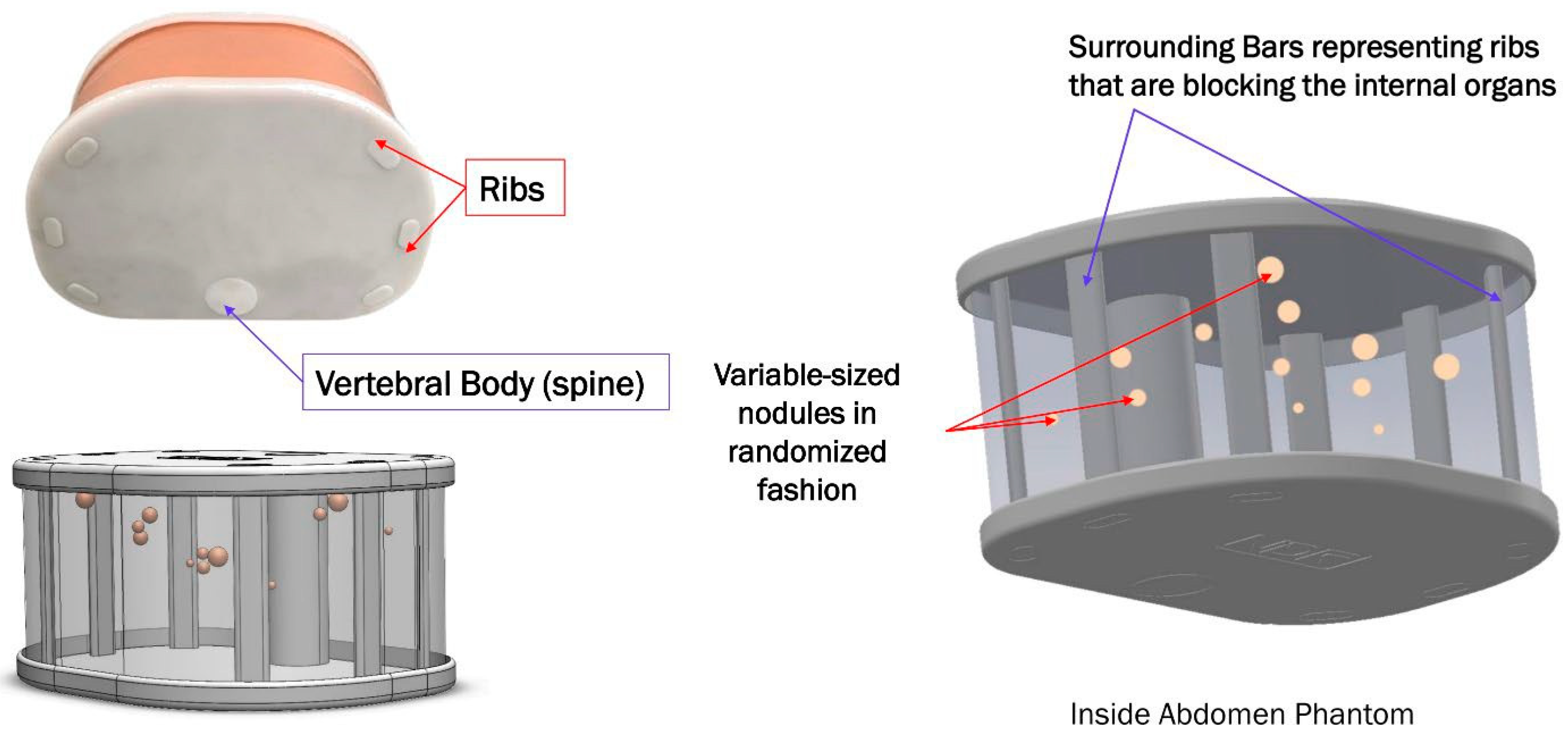
Accugel abdomen phantom is representative of a small adult abdomen and can be imaged under CT, Fluoroscopy, and ultrasound. It simulates the abdomen with ribs surrounding it, and materials provide contrast between the structures under all imaging modalities. The phantom is made of gelatin with nodules that are made of RTV rubber. The overlying surface is covered with skin to increase validity (texture and resistance) and prevent direct visualization of the kidney. The posterior cover of the phantom can be removed for the direct visualization and evaluation of the needle position following each puncture.
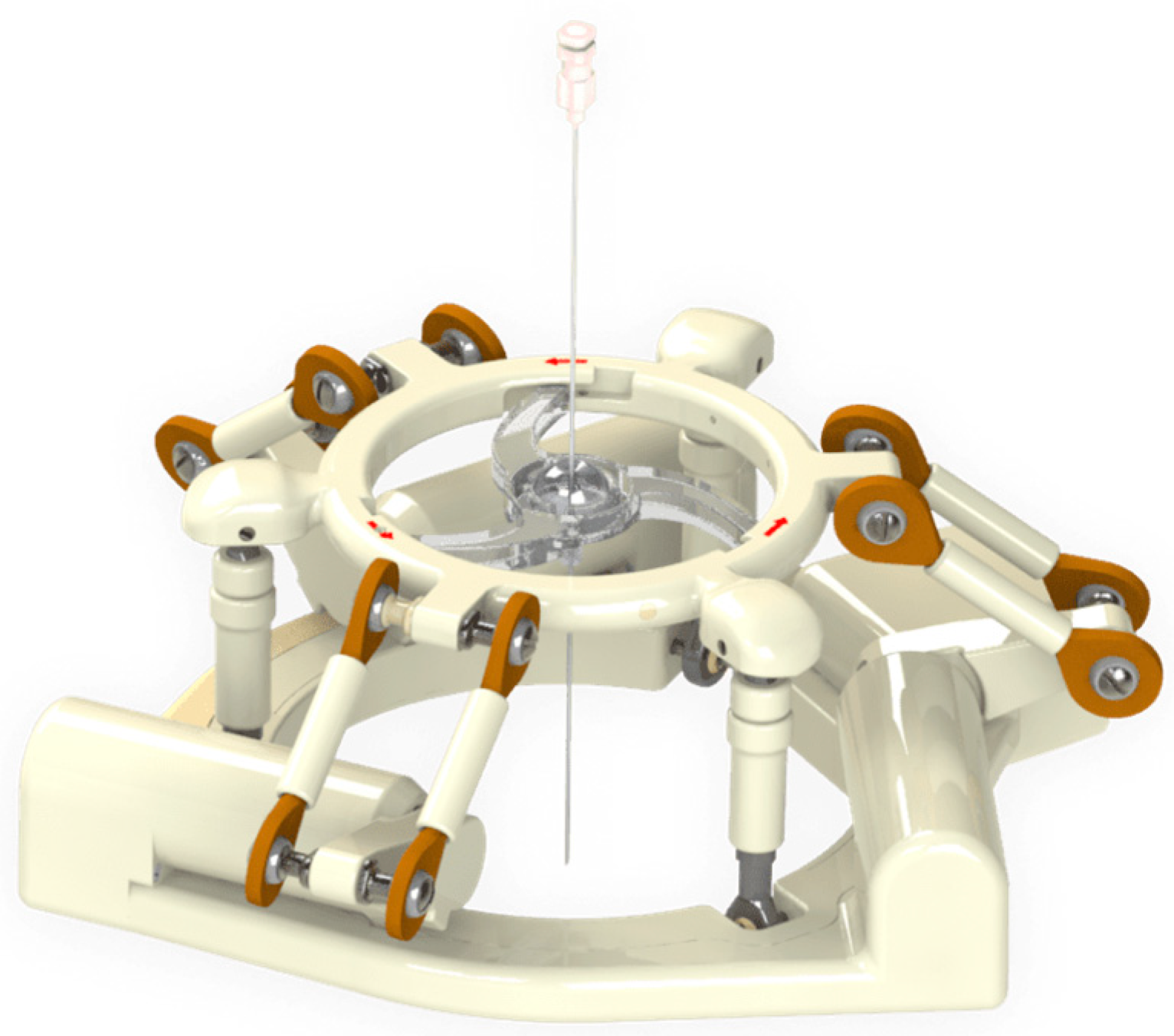
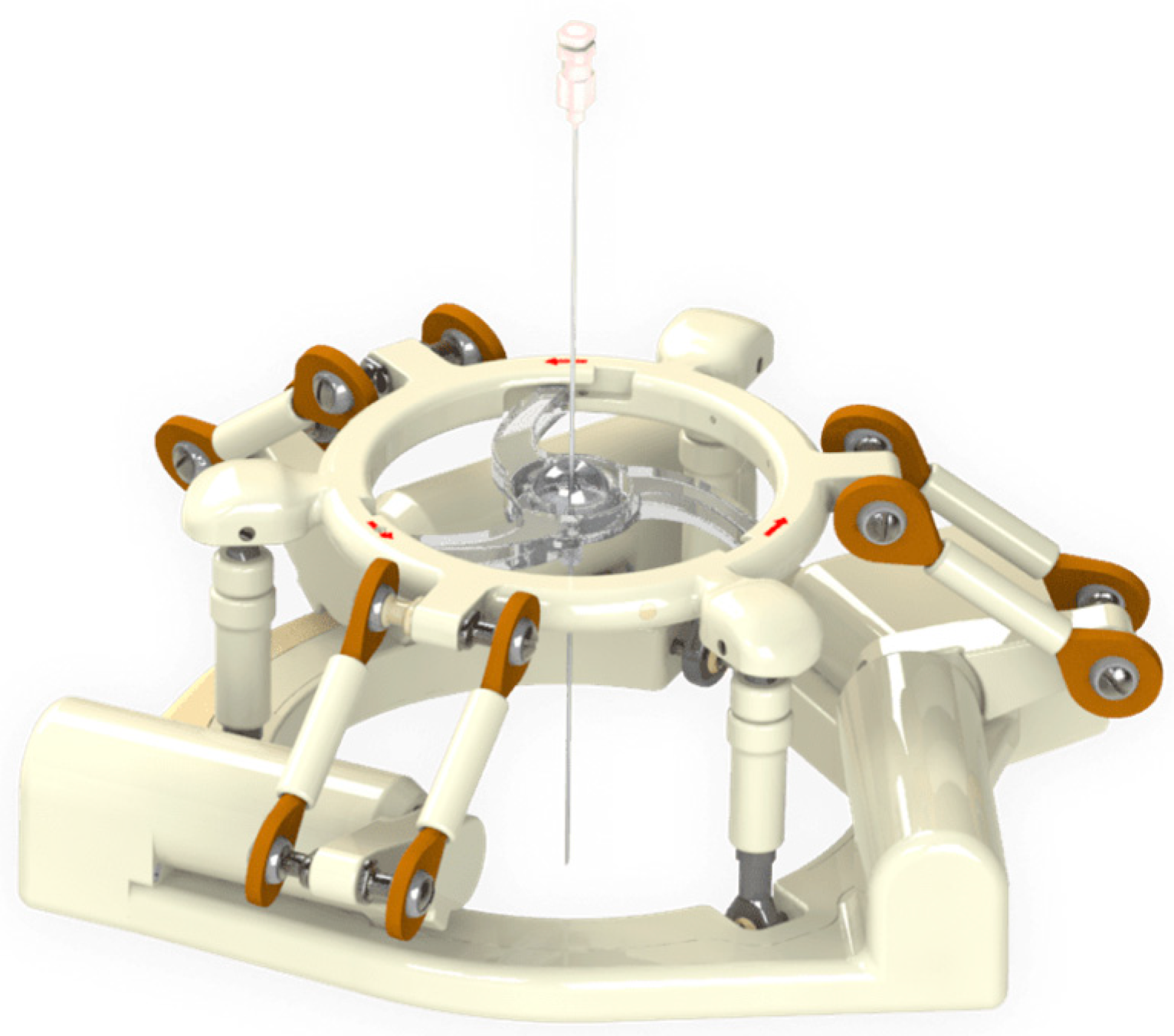
The system consists of a single-use ball-joint needle holder placed within the ANT-X device (
Figure 1) with an articulated arm mounted on the operating table. The ANT-X device and the fluoroscopic arm are connected to the computer system to form a closed-loop feedback system (
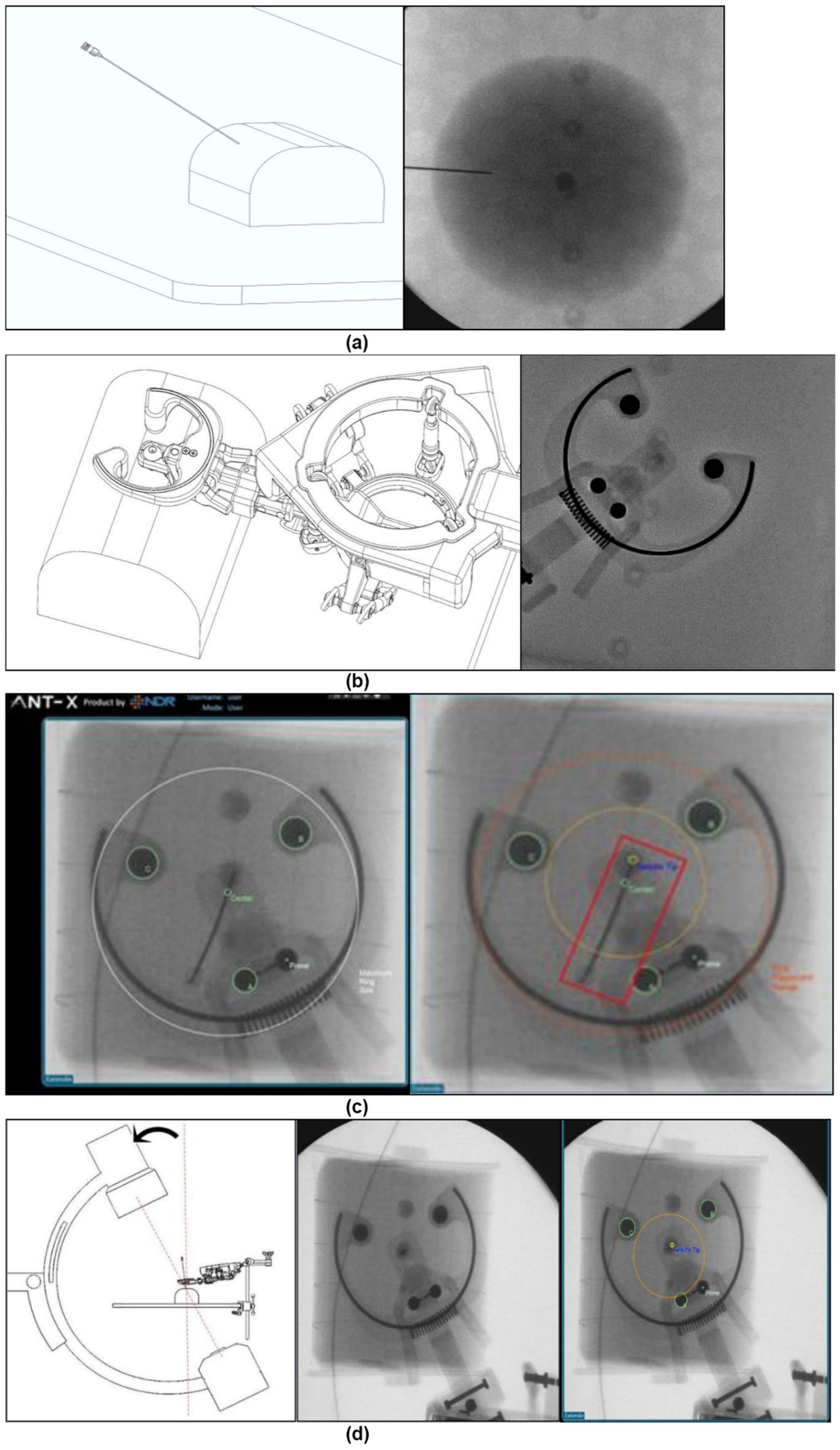
Figure 2). ANT-X works on the following principles:
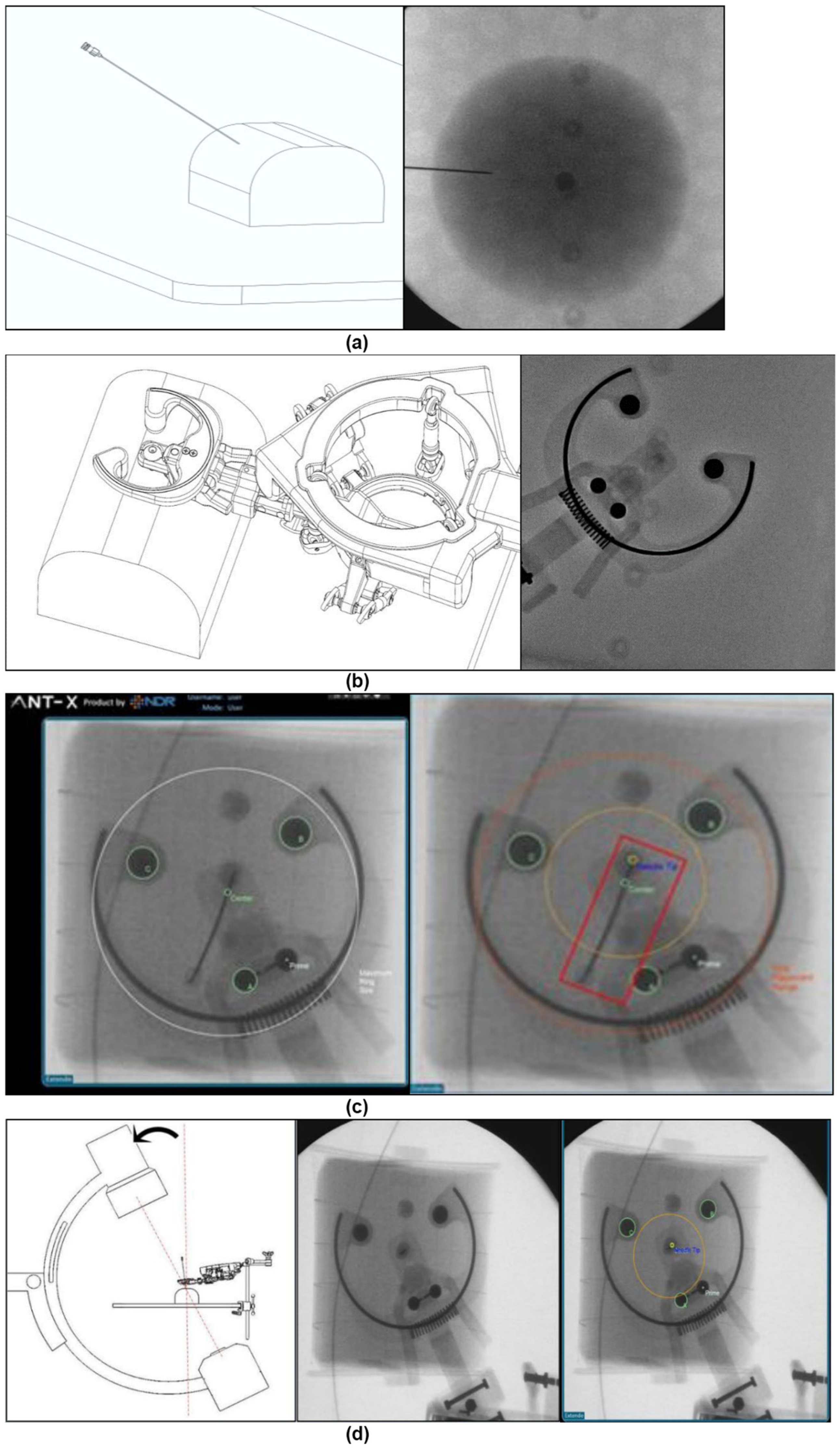
The desired nodule within the phantom is identified via fluoroscopy. In humans, the collecting system is lit up via retrograde pyelogram, and the surgeon chooses the appropriate calyx for entry by placing a skin stab incision over the area.
The needle holder ring is positioned near the point of entry.
The needle is inserted into the needle holder and pivoted on the incision site.
Fluoroscopic images are obtained by the C-arm at 30 degrees and imported to the system using DICOM or any other video output methods deployed by the common C-arms available in the market.
ANT-X integrates the images with the real-time position of the needle mounted on the device by using transformative projection. The needle is automatically aligned for puncture into the chosen nodule based on the correlation of these coordinates. In humans, there is no compensation for respiration movement.
Once auto-alignment is completed, the needle holder keeps the needle angle stable as the surgeon advances the needle into the desired nodule manually. Fluoroscopy with C-arm at 0 degrees is used to gauge the depth of puncture. For phantom puncture, the direct visualization and evaluation of the needle position can be achieved via the posterior of the phantom.
3.3. Participants and Procedures
In this study, four urological residents participated and performed phantom punctures using both the free-hand bull’s eye technique and the automated needle targeting system with X-ray (ANT-X). Each resident performed a total of 60 punctures on the renal phantom models, with 30 punctures using the free-hand technique and 30 punctures using the ANT-X robotic-assisted system.
The residents underwent training and familiarization with the ANT-X system and traditional bull’s eye puncture for a total duration of 2 h before performing the punctures. The punctures were carried out on the renal phantom models, mimicking the anatomical features and complexities of the renal collecting system. The residents followed the standard protocols and techniques for each puncture method, ensuring consistency and accuracy in their approach. Successful puncture was confirmed using fluoroscopy and direct visualization. By performing an equal number of punctures using both the free-hand and ANT-X groups, the study sought to establish a direct comparison between the two methods.
The background experience in PCNL renal access of the participants is summarized in
Table 1.
Each participant will complete a total of 60 punctures, distributed over six sessions with a minimum one-week gap between each session. In each session, the participants will perform 10 needle punctures on a standardized phantom, alternating between the free-hand technique and the ANT-X robotic-assisted puncture group. The nodule to puncture will be standardized to minimize bias.
For the traditional free-hand puncture, the participants will employ a prone fluoroscopy-guided PCNL approach using the bull’s eye technique. On the other hand, for the ANT-X puncture, the participants will utilize the ANT-X system, which integrates an articulated reusable arm mounted on the operating table and a computer system connected to a standard C-arm. This system will provide automated needle positioning for accessing target balls. The principles and description of the ANT-X system have been previously documented.
During the study, several parameters will be recorded for analysis, including the total time taken to achieve renal access, the total dose of radiation exposure (measured in mGy/s), and the trainee’s confidence level.
The software activation and robotic arm attachment to the operation table were completed beforehand. The workflow of the robotic-assisted puncture is shown below (
Figure 3).
3.4. Statistical Analysis
Continuous normally distributed variables were expressed as means (standard deviation), whereas non-normally distributed variables were expressed as medians (25% and 75% interquartile range). Categorical variables were presented as frequency (percentage). The Mann–Whitney U test was used to identify differences between groups. Differences were considered statistically significant at a <0.05.
Data that were captured are time to access, radiation exposure, and confidence level.
4. Results
A total of 240 needle insertions were conducted, with 120 in the ANT-X group and 120 in the free-hand group. The success rate of needle insertions was 100% in both groups, indicating the safety and feasibility of both groups.
Needle Puncture Time: the study revealed that the ANT-X group required, on average, an additional 51 s for needle puncture compared to the free-hand group (
p < 0.001) (
Table 2).
Fluoroscopic Exposure: notably, the study found that the ANT-X group exhibited significantly lower fluoroscopic exposure compared to the free-hand group (0.50 mGy/s vs. 0.87 mGy/s, respectively;
p < 0.001) (
Table 3).
Sub-analysis of total puncture time and radiation exposure was conducted between the free-hand and ANT-X groups. The results revealed interesting findings related to participant experience and changes in radiation exposure throughout the sessions.
Puncture time: The average puncture time of the four participants did not reduce despite using the free-hand and ANT-X groups (p = 0.040). This suggests that regardless of the technique employed, the participants’ puncture time remained relatively consistent.
Fluoroscopic screening time: The sub-analysis indicated that the average fluoroscopic screening time decreased as the participants gained more puncture experience. This suggests that with increasing proficiency and familiarity with the procedure, participants required less time for fluoroscopic guidance. This finding highlights the potential for skill development and improved efficiency over time.
Radiation exposure in the first session: In the first session, the average radiation exposure of the four participants was significantly higher in the free-hand group (1.876 mGy/s) compared to the ANT-X group (0.609 mGy/s) (
p < 0.001). This indicates that the use of the ANT-X resulted in significantly lower radiation exposure during initial sessions (
Table 4).
Radiation exposure in the last session: In the last session, the average radiation exposure of the four participants was significantly lower in both the free-hand and ANT-X groups compared to the first session. However, the free-hand group still had a higher average radiation exposure (0.714 mGy/s) compared to the ANT-X group (0.413 mGy/s) (
p < 0.001). This suggests that as participants gained experience, both groups resulted in reduced radiation exposure, with the ANT-X group consistently providing lower exposure levels (
Table 5).
The high level of confidence elicited in this study regarding needle puncture is indeed surprising, considering that each participant had limited experience in PCNL needle puncture. The self-assessment scores of 88.3%, indicating a confidence level of more than 7 on a scale of 1–10, suggest that the participants felt quite confident in their ability to perform the puncture.
5. Discussion
The development of robot-assisted devices for various purposes has been hindered by their complexity, bulkiness, and high cost. Therefore, it is crucial to adopt a more practical approach using readily available imaging modalities to improve the technique for robot-assisted renal access in urinary stone disease. The ANT-X robotic system presented in this study offers a feasible and effective solution thanks to its compact size, user-friendly interface, and fully automated navigation system. Moreover, it can be integrated with low-cost C-arm fluoroscopic devices commonly available in operating theatres.
Despite the participating surgeons having limited experience in fluoroscopy-guided renal access, they were able to perform needle puncture effectively. The median needle puncture time with the ANT-X system, including fluoroscopic confirmation, was 24% slower than a free-hand puncture. However, the radiation exposure was 32% lower with ANT-X compared to free-hand puncture. This is likely due to ANT-X’s ability to achieve and maintain precise positioning during needle puncture, resulting in reduced radiation exposure. These findings highlight the potential advantages of the ANT-X device in reducing radiation exposure during PCNL puncture. By minimizing radiation exposure, the ANT-X offers enhanced safety for both patients and medical staff.
As the surgeons gained more experience with needle puncture using both free-hand and ANT-X on the phantom model, a significant reduction in radiation dose was observed within each group. For the free-hand group, the radiation dose decreased by 61.9% between the last and first sessions, while for the ANT-X group, the reduction was 32.1%. Although this study does not definitively prove that ANT-X reduces the learning curve in free-hand puncture, it does demonstrate the important role of ANT-X in assisting surgeons to achieve the bull’s eye position and stabilize the needle during advancement, thereby fulfilling the ALARA (as low as reasonably achievable) principle, even for beginners [
9,
10,
11].
Surgeons’ self-assessment of confidence levels indicated a high level of confidence in needle puncture. The combination of free-hand and ANT-X boosted surgeons’ self-confidence, as evidenced by the study’s findings of 88.3% of participants reporting a confidence level greater than 7 (on a scale of 1–10) despite their lack of experience in PCNL needle puncture. The ability of surgeons to grasp the concept and appreciate the bull’s eye technique, whether performing free-hand or assisted by ANT-X, contributes to their confidence. This training will undoubtedly aid surgeons in initiating renal puncture in human patients.
The primary limitation of this study is the use of a phantom model that may not fully mimic the anatomy and physiological aspects of an actual kidney. Additionally, the absence of respiratory and kidney movement in the phantom model introduces discrepancies. Given that this research is a benchtop study, the findings should be validated in actual patients with renal stones, which is currently ongoing. Lastly, the surgeons’ self-assessment represents a subjective evaluation of the procedure and may be influenced by individual biases.
Further research and clinical studies are necessary to confirm and expand upon the findings of this study, particularly in live patient settings, which is currently ongoing. Validating the outcomes in real-world scenarios will provide more robust evidence regarding the efficacy and safety of the ANT-X system for robot-assisted renal access in PCNL procedures.
6. Conclusions
Our benchtop study comparing the efficacy and safety between free-hand and ANT-X phantom punctures revealed comparable results for mimicked renal access during PCNL. The needle puncture technique facilitated by the ANT-X system showed promising results in terms of reducing fluoroscopic exposure, albeit at the cost of longer operative times.
This technology holds promise for novice surgeons who are in the early stages of their learning curve and might be useful for experienced surgeons looking to reduce radiation exposure.
Author Contributions
Conceptualization, J.Z.K.L., C.C.A. and W.S.Y.; methodology, K.K. and A.K.P.; software, K.K. and A.N.; validation, S.K. and T.A.O.; formal analysis, J.Z.K.L.; investigation, J.Z.K.L.; resources, C.C.A. and W.S.Y.; data curation, J.Z.K.L. and C.C.A.; writing—original draft preparation, J.Z.K.L.; writing—review and editing, J.Z.K.L., C.C.A. and W.S.Y.; visualization, W.S.Y.; supervision, A.N. and W.S.Y.; project administration, J.Z.K.L. and C.C.A.; funding acquisition, C.C.A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. The robotic device and phantom kidney are donated by NDR Medical Technology.
Institutional Review Board Statement
Ethical approval by Malaysia Research Ethical Committee (202124-9805).
Informed Consent Statement
This study did not involve humans.
Data Availability Statement
Data is generated using IPSS and available to public.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Assimos, D.; Krambeck, A.; Miller, N.L.; Monga, M.; Murad, M.H.; Nelson, C.P.; Pace, K.T.; Pais, V.M.; Pearle, M.S.; Preminger, G.M.; et al. Surgical management of stones: American Urological Association/ Endourological Society Guideline. Part II. J. Urol. 2016, 196, 1161–1169. [Google Scholar] [CrossRef] [PubMed]
- Türk, C.; Petřík, A.; Sarica, K.; Seitz, C.; Skolarikos, A.; Straub, M.; Knoll, T. EAU guidelines on interventional treatment for urolithiasis. Eur. Urol. 2016, 69, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Tomaszewski, J.J.; Ortiz, T.D.; Gayed, B.A.; Smaldone, M.C.; Jackman, S.V.; Averch, T.D. Renal access by urologist or radiologist during percutaneous nephrolithotomy. J. Endourol. 2010, 24, 1733–1737. [Google Scholar] [CrossRef] [PubMed]
- Rassweiler, J.J.; Müller, M.; Fangerau, M.; Klein, J.; Goezen, A.S.; Pereira, P.; Meinzer, H.P.; Teber, D. IPadassisted percutaneous access to the kidney using marker-based navigation. Eur. Urol. 2012, 6, 13–22. [Google Scholar]
- Cadeddu, J.A.; Bzostek, A.; Schreiner, S.; Barnes, A.C.; Roberts, W.W.; Anderson, J.H.; Taylor, R.H.; Kavoussi, L.R. A robotic system for percutaneous renal access. J. Urol. 1997, 158, 1589–1593. [Google Scholar] [CrossRef]
- Cadeddu, J.A.; Soianovici, D.; Roland, N.C.; Moore, R.G.; Kavoussi, L.R. Stereotactic Mechanical Percutaneous Renal Access. J. Endourol. 1998, 12, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Su, L.-M.; Stoianovici, D.; Jarrett, T.W.; Patriciu, A.; Roberts, W.W.; Cadeddu, J.A.; Ramakumar, S.; Solomon, S.B.; Kavoussi, L.R. Robotic percutaneous access to the kidney: Comparison with standard manual access. J. Endourol. 2002, 16, 471–475. [Google Scholar] [CrossRef] [PubMed]
- Pollock, R.; Mozer, P.; Guzzo, T.J.; Marx, J.; Matlaga, B.; Petrisor, D.; Vigaru, B.; Badaan, S.; Stoianovici, D.; Allaf, M.E. Prospects in Percutaneous Ablative Targeting: Comparison of a Computer-Assisted Navigation System and the AcuBot Robotic System. J. Endourol. 2010, 24, 1269–1272. [Google Scholar] [CrossRef]
- Oo, M.M.; Gandhi, H.R.; Chong, K.T.; Goh, J.Q.; Ng, K.W.; Hein, A.T.; Tan, Y.K. Automated Needle Targeting with X-ray (ANT-X)—Robot-assisted device for percutaneous nephrolithotomy (PCNL) with its first successful use in human. J. Endourol. 2021, 35, e919. [Google Scholar] [CrossRef] [PubMed]
- Kyriazis, I.; Liatsikos, E.; Sopilidis, O.; Kallidonis, P.; Skolarikos, A.; European Section of Urotechnology (ESUT). European Section of Urotechnology educational video on fluoroscopic-guided puncture in percutaneous nephrolithotomy: All techniques step by step. BJU Int. 2017, 120, 739–741. [Google Scholar] [CrossRef] [PubMed]
- Blair, B.; Huang, G.; Arnold, D.; Li, R.; Schlaifer, A.; Anderson, K.; Engebretsen, S.; Wallner, C.; Olgin, G.; Baldwin, D.D. Reduced fluoroscopy protocol for percutaneous nephrostolithotomy: Feasibility, outcomes and effects on fluoroscopy time. J. Urol. 2013, 190, 2112–2116. [Google Scholar] [CrossRef] [PubMed]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).

 ,
, 

{kind=link}
{kind=link}
{kind=link}