
A Novel Approach for Diabetic Retinopathy Screening Using Asymmetric Deep Learning Features

 , ,
, ,  and
and 
Abstract
1. Introduction
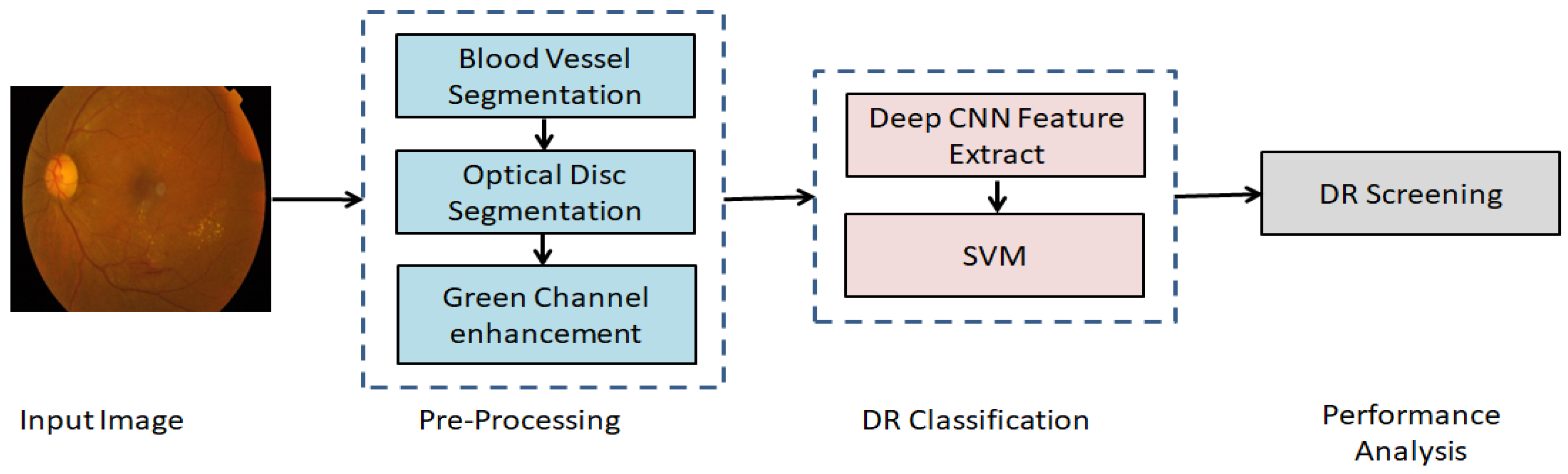
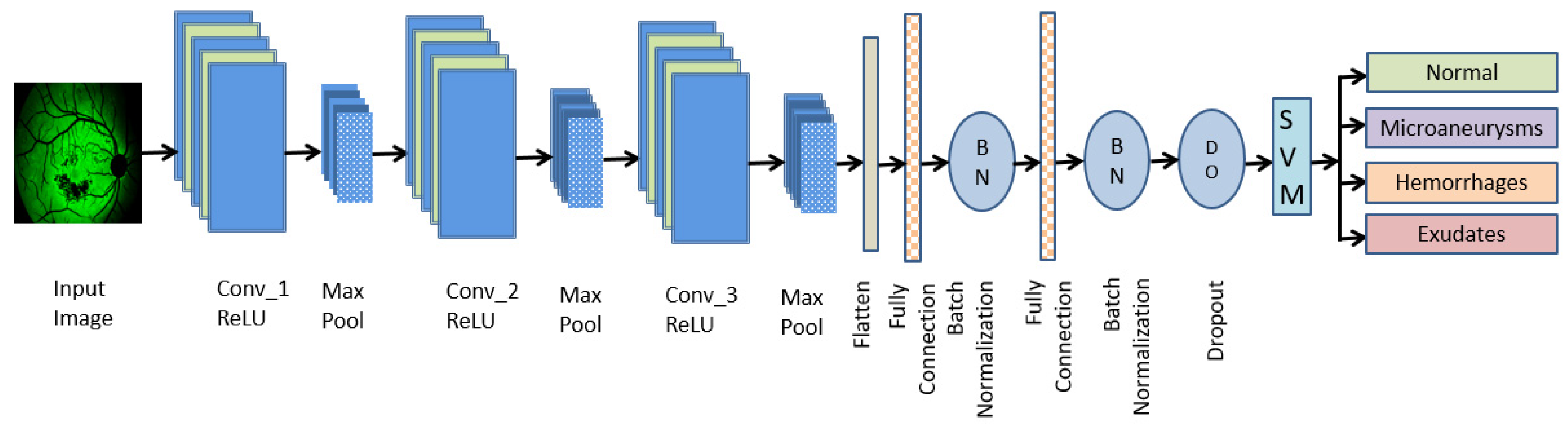
- An asymmetric deep learning approach is for the classification of diabetic retinopathy into Normal, MAs, HMs, and EXs.
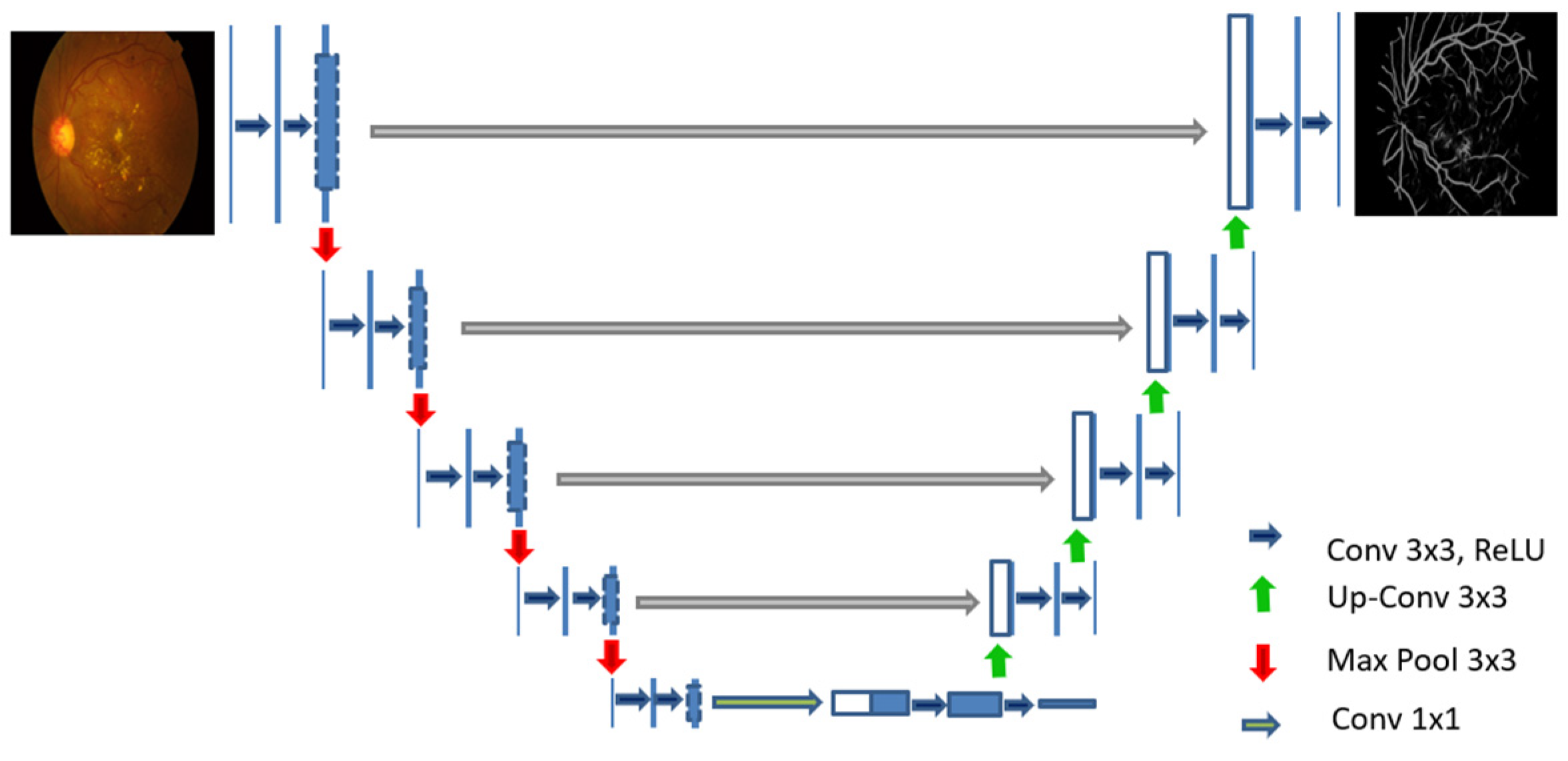
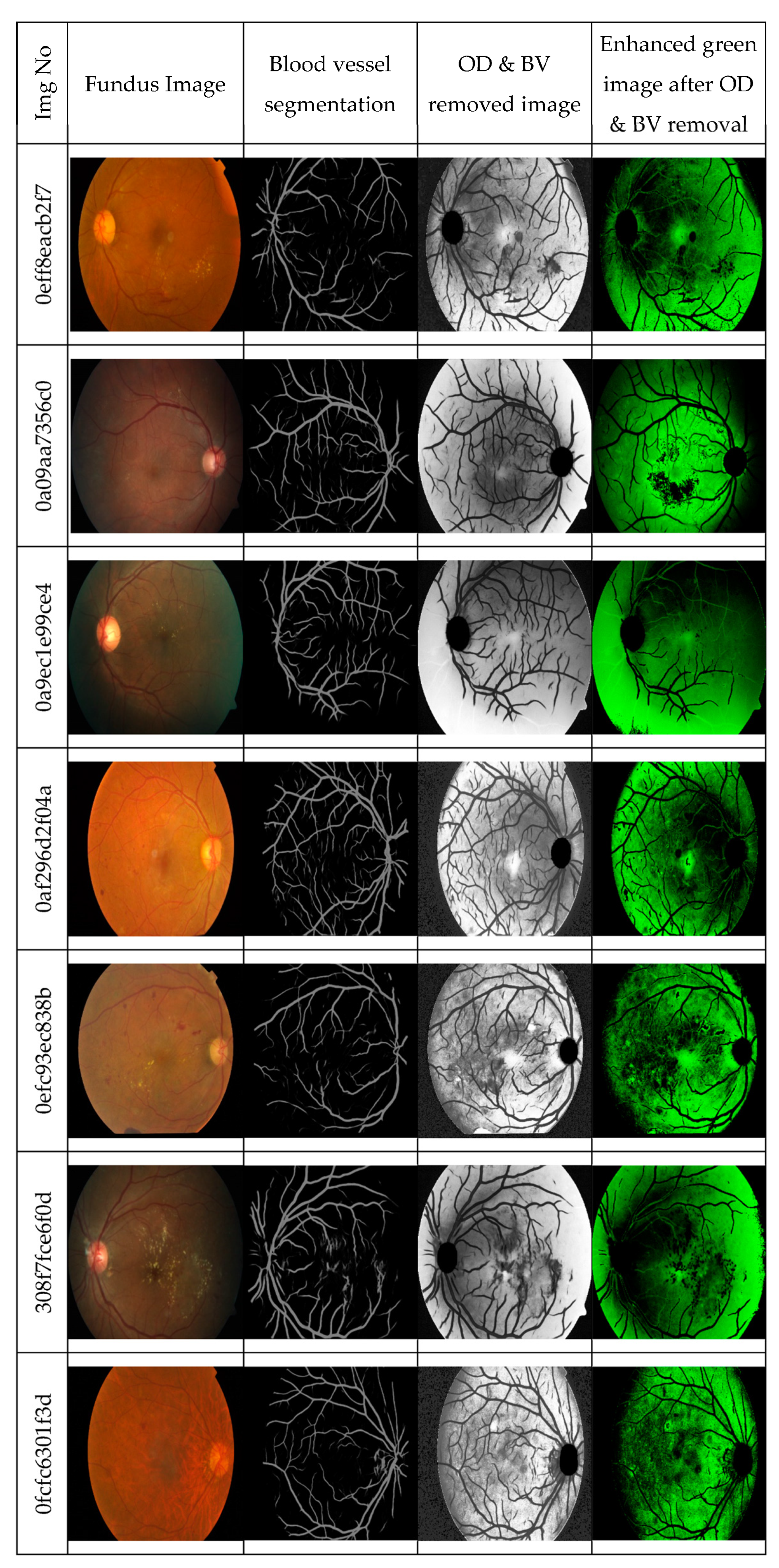
- Two U-Nets are trained through supervised learning for the retinal vessel segmentation, i.e., the U-Net_OD for optic-disc segmentation and the U-Net_BV for blood vessel segmentation, to enhance the individual learning performance.
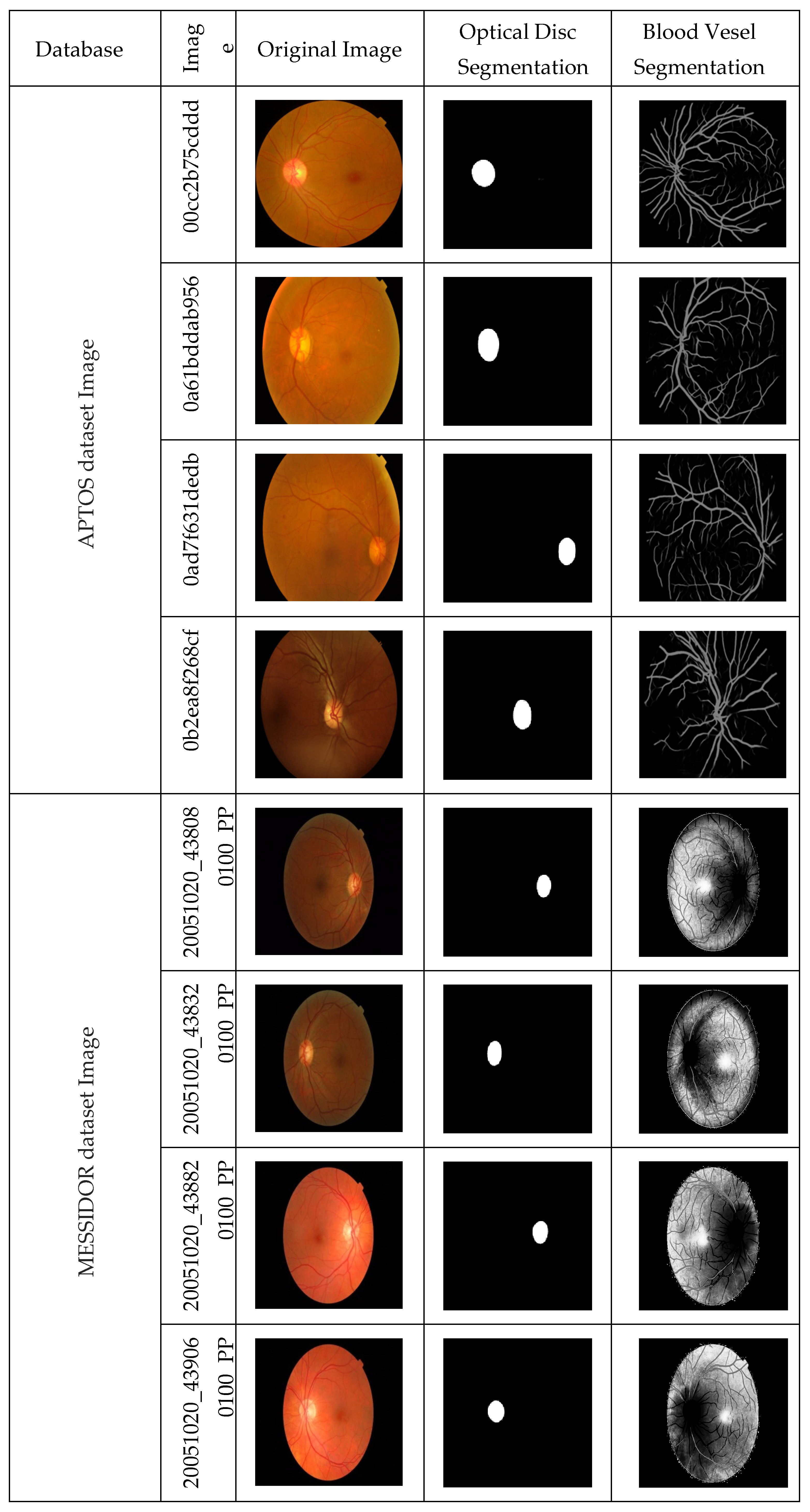
- DR classification is done using CNN and SVM on the APTOS and MESSIDOR fundus image datasets, which are public datasets and can be downloaded with prior registration.
- The APTOS dataset consists of 3662 fundus images, out of which 1805 images are Normal, 370 images belong to MAs, 999 images are of HMs types, and 295 images belong to the EXs category.
- The MESSIDOR dataset consists of 1200 fundus images, out of which 548 images are Normal, 152 images belong to MAs, 246 images are of HMs types, and 254 images belong to the EXs category.
2. Related Work
3. Proposed Model
3.1. Segmentation Using U-Net

3.2. Performance Measures
4. Results and Discussions
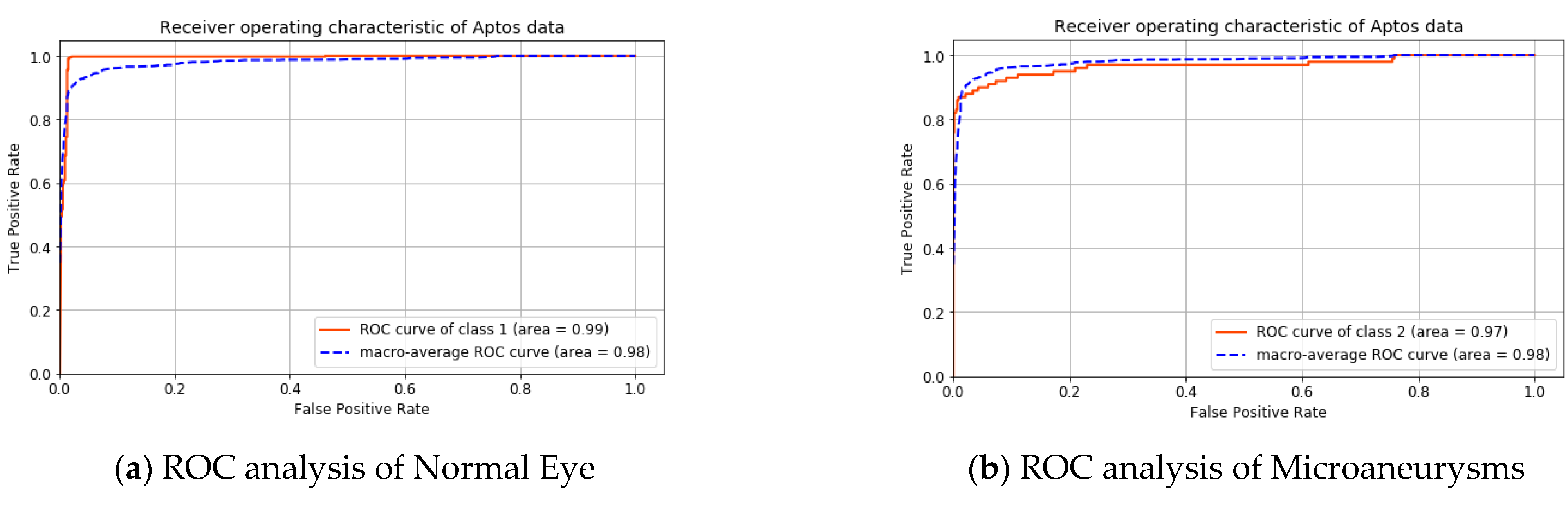
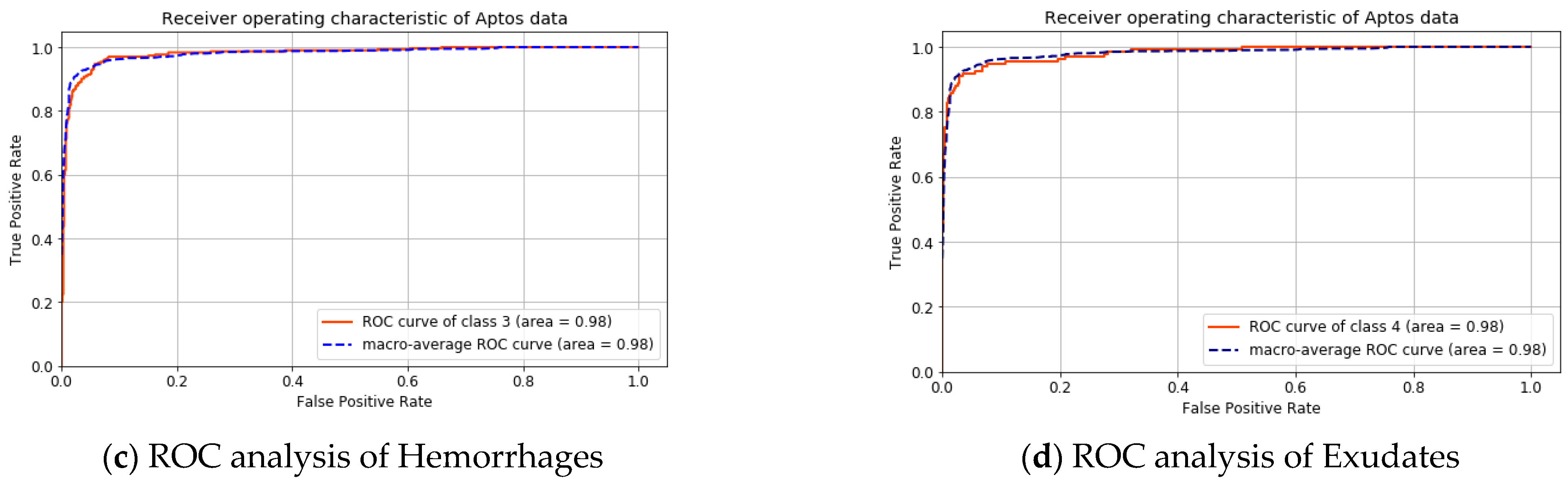
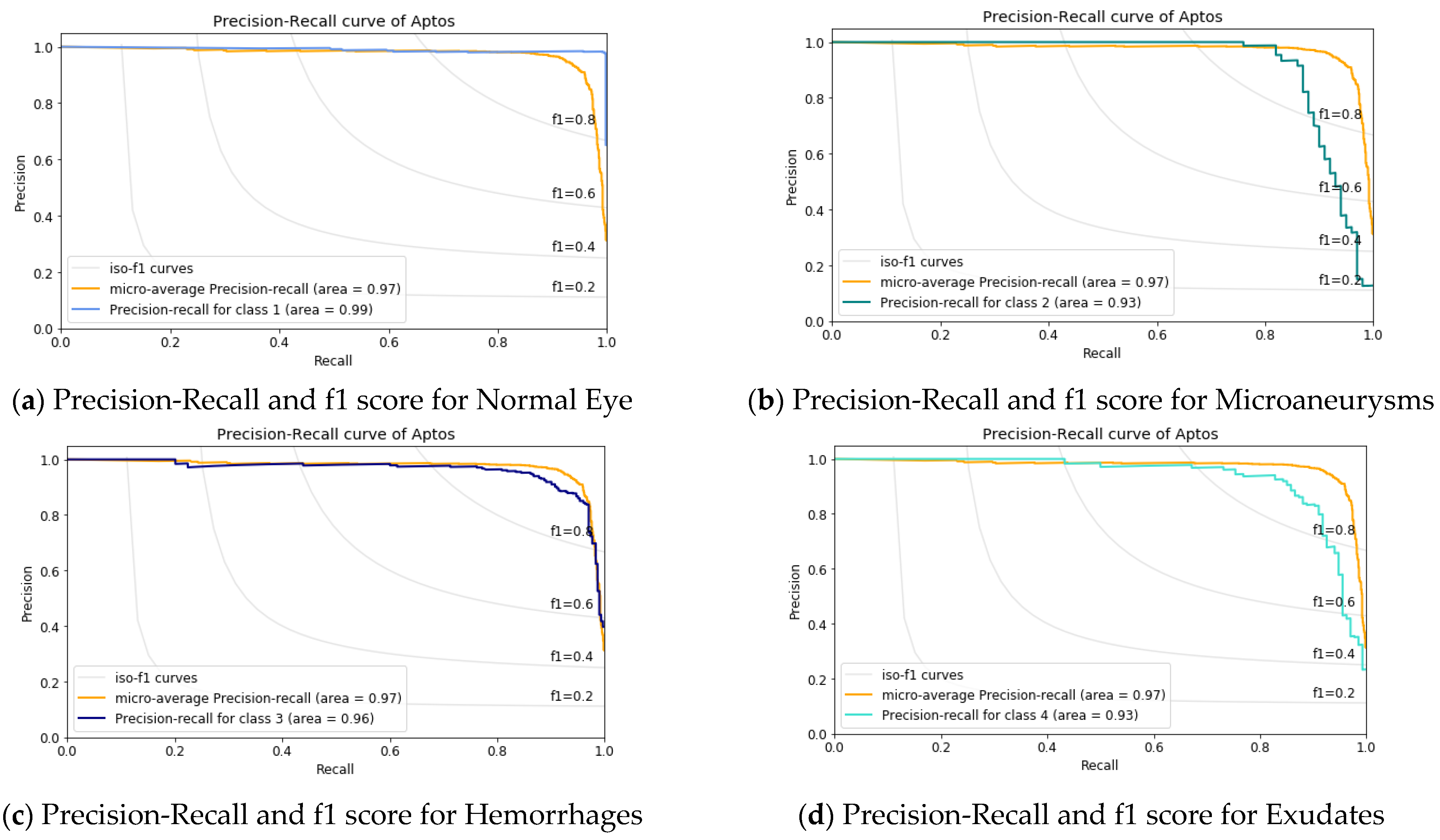
4.1. Result Analysis Using Aptos Dataset
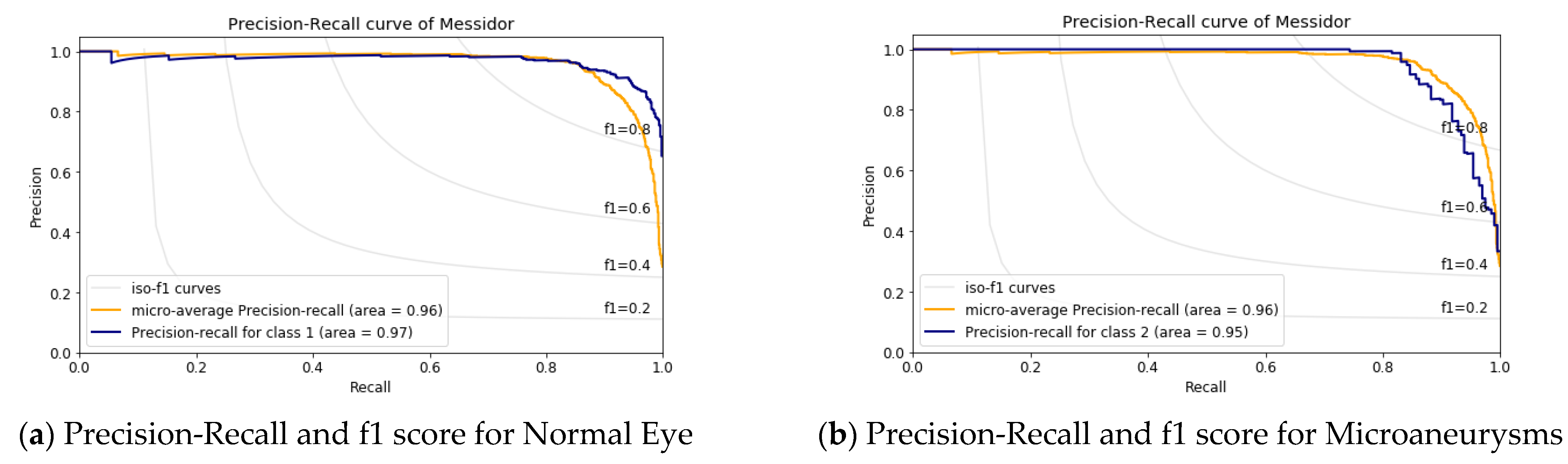
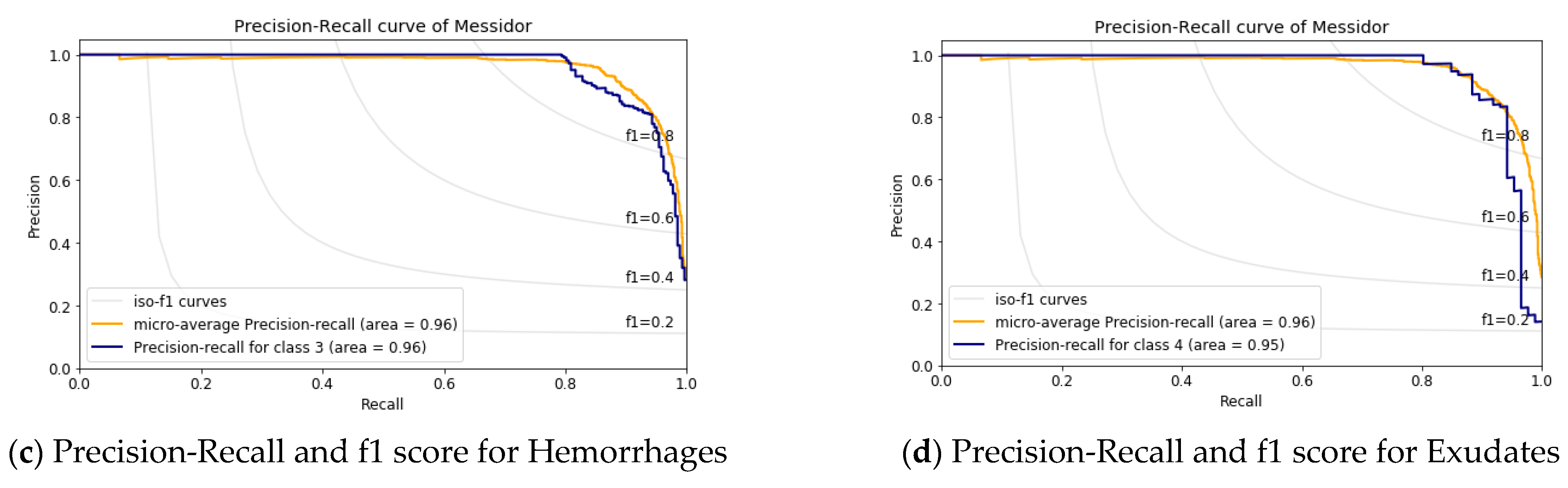
4.2. Result Analysis Using Messidor Dataset
4.3. Performance Comparison
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, L.; Gu, J.; Chen, Y.; Liang, Y.; Zhang, W.; Pu, J.; Chen, H. Automated segmentation of the optic disc from fundus images using an asymmetric deep learning network. Pattern Recognit. 2021, 112, 107810. [Google Scholar] [CrossRef] [PubMed]
- Rahim, S.S.; Jayne, C.; Palade, V.; Shuttleworth, J. Automatic detection of microaneurysms in colour fundus images for diabetic retinopathy screening. Neural Comput. Appl. 2015, 27, 1149–1164. [Google Scholar] [CrossRef]
- Asiri, N.; Hussain, M.; Al Adel, F.; Alzaidi, N. Deep learning based computer-aided diagnosis systems for diabetic retinopathy: A survey. Artif. Intell. Med. 2019, 99, 101701. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Adarsh, A.; Kumar, B.; Singh, A.K. An automated early diabetic retinopathy detection through improved blood vessel and optic disc segmentation. Opt. Laser Technol. 2019, 121, 105815. [Google Scholar] [CrossRef]
- Júnior, S.B.; Welfer, D. Automatic Detection of Microaneurysms and Hemorrhages in Color Eye Fundus Images. Int. J. Comput. Sci. Inf. Technol. 2013, 5, 21–37. [Google Scholar] [CrossRef]
- Zhu, C.; Zou, B.; Zhao, R.; Cui, J.; Duan, X.; Chen, Z.; Liang, Y. Retinal vessel segmentation in colour fundus images using Extreme Learning Machine. Comput. Med. Imaging Graph. 2017, 55, 68–77. [Google Scholar] [CrossRef]
- Khojasteh, P.; Júnior, L.A.P.; Carvalho, T.; Rezende, E.; Aliahmad, B.; Papa, J.P.; Kumar, D.K. Exudate detection in fundus images using deeply-learnable features. Comput. Biol. Med. 2018, 104, 62–69. [Google Scholar] [CrossRef]
- Nayak, D.R.; Das, D.; Majhi, B.; Bhandary, S.V.; Acharya, U.R. ECNet: An evolutionary convolutional network for automated glaucoma detection using fundus images. Biomed. Signal Process. Control. 2021, 67, 102559. [Google Scholar] [CrossRef]
- Perdomo, O.; Otalora, S.; Rodríguez, F.; Arevalo, J.; González, F.A. A novel machine learning model based on ex-udate localization to detect diabetic macular edema. Lect. Notes Comput. Sci. 2016, 1, 137–144. [Google Scholar]
- Sengupta, S.; Singh, A.; Leopold, H.A.; Gulati, T.; Lakshminarayanan, V. Ophthalmic diagnosis using deep learning with fundus images—A critical review. Artif. Intell. Med. 2019, 102, 101758. [Google Scholar] [CrossRef]
- Zhao, R.; Li, S. Multi-indices quantification of optic nerve head in fundus image via multitask collaborative learning. Med. Image Anal. 2019, 60, 101593. [Google Scholar] [CrossRef] [PubMed]
- Akram, M.U.; Khalid, S.; Tariq, A.; Khan, S.A.; Azam, F. Detection and classification of retinal lesions for grading of diabetic retinopathy. Comput. Biol. Med. 2014, 45, 161–171. [Google Scholar] [CrossRef] [PubMed]
- Deepak, S.; Ameer, P. Brain tumor classification using deep CNN features via transfer learning. Comput. Biol. Med. 2019, 111, 103345. [Google Scholar] [CrossRef] [PubMed]
- Nazir, T.; Irtaza, A.; Shabbir, Z.; Javed, A.; Akram, U.; Mahmood, M.T. Diabetic retinopathy detection through novel tetragonal local octa patterns and extreme learning machines. Artif. Intell. Med. 2019, 99, 101695. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Yin, Y.; Cao, G.; Wei, B.; Zheng, Y.; Yang, G. Hierarchical retinal blood vessel segmentation based on feature and ensemble learning. Neurocomputing 2015, 149, 708–717. [Google Scholar] [CrossRef]
- Wu, J.; Zhang, S.; Xiao, Z.; Zhang, F.; Geng, L.; Lou, S.; Liu, M. Hemorrhage detection in fundus image based on 2D Gaussian fitting and human visual characteristics. Opt. Laser Technol. 2018, 110, 69–77. [Google Scholar] [CrossRef]
- Leontidis, G.; Al-Diri, B.; Hunter, A. A new unified framework for the early detection of the progression to diabetic retinopathy from fundus images. Comput. Biol. Med. 2017, 90, 98–115. [Google Scholar] [CrossRef] [PubMed]
- Lahiri, A.; Roy, A.G.; Sheet, D.; Biswas, P.K. Deep neural ensemble for retinal vessel segmentation in fundus images towards achieving label-free angiography. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 6–10 August 2016; pp. 1340–1343. [Google Scholar]
- Orlando, J.I.; Prokofyeva, E.; del Fresno, M.; Blaschko, M.B. An ensemble deep learning based approach for red lesion detection in fundus images. Comput. Methods Programs Biomed. 2018, 153, 115–127. [Google Scholar] [CrossRef]
- Zhang, D.; Wang, J.; Noble, J.H.; Dawant, B.M. HeadLocNet: Deep convolutional neural networks for accurate classification and multi-landmark localization of head CTs. Med. Image Anal. 2020, 61, 101659. [Google Scholar] [CrossRef]
- Alyoubi, W.L.; Abulkhair, M.F.; Shalash, W.M. Diabetic retinopathy fundus image classification and lesions lo-calization system using deep learning. Sensors 2021, 21, 3704. [Google Scholar] [CrossRef]
- Amit, Y. Deep Learning With Asymmetric Connections and Hebbian Updates. Front. Comput. Neurosci. 2019, 13, 18. [Google Scholar] [CrossRef] [PubMed]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In International Conference on Medical Image Computing and Computer-Assisted Intervention; Springer: Cham, Switzerland, 2015; pp. 234–241. [Google Scholar]
- Dunnhofer, M.; Antico, M.; Sasazawa, F.; Takeda, Y.; Camps, S.; Martinel, N.; Micheloni, C.; Carneiro, G.; Fontanarosa, D. Siam-U-Net: Encoder-decoder siamese network for knee cartilage tracking in ultrasound images. Med. Image Anal. 2020, 60, 101631. [Google Scholar] [CrossRef] [PubMed]
- Karimi, D.; Zeng, Q.; Mathur, P.; Avinash, A.; Mahdavi, S.; Spadinger, I.; Abolmaesumi, P.; Salcudean, S.E. Accurate and robust deep learning-based segmentation of the prostate clinical target volume in ultrasound images. Med. Image Anal. 2019, 57, 186–196. [Google Scholar] [CrossRef]
- Prusty, S.; Dash, S.K.; Patnaik, S. A Novel Transfer Learning Technique for Detecting Breast Cancer Mammograms Using VGG16 Bottleneck Feature. ECS Trans. 2022, 107, 733–746. [Google Scholar] [CrossRef]
- Prusty, S.; Patnaik, S.; Dash, S.K. SKCV: Stratified K-fold cross-validation on ML classifiers for predicting cervical cancer. Front. Nanotechnol. 2022, 4, 972421. [Google Scholar] [CrossRef]
- Zhou, Q.; Yang, W.; Gao, G.; Ou, W.; Lu, H.; Chen, J.; Latecki, L.J. Multi-scale deep context convolutional neural networks for semantic segmentation. World Wide Web 2018, 22, 555–570. [Google Scholar] [CrossRef]
- Savelli, B.; Bria, A.; Molinara, M.; Marrocco, C.; Tortorella, F. A multi-context CNN ensemble for small lesion de-tection. Artif. Intell. Med. 2020, 103, 101749. [Google Scholar] [CrossRef]
- Aslani, S.; Sarnel, H. A new supervised retinal vessel segmentation method based on robust hybrid features. Biomed. Signal Process. Control. 2016, 30, 1–12. [Google Scholar] [CrossRef]
- Lim, G.; Cheng, Y.; Hsu, W.; Lee, M.L. Integrated optic disc and cup segmentation with deep learning. In Proceedings of the 2015 IEEE 27th International Conference on Tools with Artificial Intelligence (ICTAI), Vietri sul Mare, Italy, 9–11 November 2015; pp. 162–169. [Google Scholar]
- Mahum, R.; Rehman, S.U.; Okon, O.D.; Alabrah, A.; Meraj, T.; Rauf, H.T. A Novel Hybrid Approach Based on Deep CNN to Detect Glaucoma Using Fundus Imaging. Electronics 2021, 11, 26. [Google Scholar] [CrossRef]
- Antal, B.; Hajdu, A. An Ensemble-Based System for Microaneurysm Detection and Diabetic Retinopathy Grading. IEEE Trans. Biomed. Eng. 2012, 59, 1720–1726. [Google Scholar] [CrossRef]
- Adal, K.M.; Sidibé, D.; Ali, S.; Chaum, E.; Karnowski, T.P.; Mériaudeau, F. Automated detection of microaneurysms using scale-adapted blob analysis and semi-supervised learning. Comput. Methods Programs Biomed. 2014, 114, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Mansour, R.F. Deep-learning-based automatic computer-aided diagnosis system for diabetic retinopathy. Biomed. Eng. Lett. 2017, 8, 41–57. [Google Scholar] [CrossRef] [PubMed]
- Tzelepi, M.; Tefas, A. Deep convolutional learning for Content Based Image Retrieval. Neurocomputing 2018, 275, 2467–2478. [Google Scholar] [CrossRef]
- Wang, X.; Jiang, X.; Ren, J. Blood vessel segmentation from fundus image by a cascade classification framework. Pattern Recognit. 2018, 88, 331–341. [Google Scholar] [CrossRef]
- Saha, S.K.; Xiao, D.; Bhuiyan, A.; Wong, T.Y.; Kanagasingam, Y. Color fundus image registration techniques and applications for automated analysis of diabetic retinopathy progression: A review. Biomed. Signal Process. Control. 2018, 47, 288–302. [Google Scholar] [CrossRef]
- Kobat, S.G.; Baygin, N.; Yusufoglu, E.; Baygin, M.; Barua, P.D.; Dogan, S.; Yaman, O.; Celiker, U.; Yildirim, H.; Tan, R.-S.; et al. Automated Diabetic Retinopathy Detection Using Horizontal and Vertical Patch Division-Based Pre-Trained DenseNET with Digital Fundus Images. Diagnostics 2022, 12, 1975. [Google Scholar] [CrossRef]
- Ali, R.; Hardie, R.C.; Narayanan, B.N.; Kebede, T.M. IMNets: Deep Learning Using an Incremental Modular Network Synthesis Approach for Medical Imaging Applications. Appl. Sci. 2022, 12, 5500. [Google Scholar] [CrossRef]
- Sharifrazi, D.; Alizadehsani, R.; Roshanzamir, M.; Joloudari, J.H.; Shoeibi, A.; Jafari, M.; Hussain, S.; Sani, Z.A.; Hasanzadeh, F.; Khozeimeh, F.; et al. Fusion of convolution neural network, support vector machine and Sobel filter for accurate detection of COVID-19 patients using X-ray images. Biomed. Signal Process. Control. 2021, 68, 102622. [Google Scholar] [CrossRef]
- Guo, Y.; Zhang, Z.; Tang, F. Feature selection with kernelized multi-class support vector machine. Pattern Recognit. 2021, 117, 107988. [Google Scholar] [CrossRef]
- Jena, P.K.; Khuntia, B.; Palai, C.; Pattanaik, S.R. Content based image retrieval using adaptive semantic signature. In Proceedings of the 2019 IEEE 5th International Conference for Convergence in Technology (I2CT), Pune, India, 29–30 March 2019; pp. 1–4. [Google Scholar]
- Jena, P.K.; Khuntia, B.; Anand, R.; Patnaik, S.; Palai, C. Significance of texture feature in NIR face recog-nition. In Proceedings of the 2020 First International Conference on Power, Control and Computing Technologies (ICPC2T), Raipur, India, 3–5 January 2020; pp. 21–26. [Google Scholar]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Class | Precision% | Recall% | f1-Score% | Specificity% | Accuracy% |
|---|---|---|---|---|---|
| 1 | 97.66 | 99.35 | 98.50 | 97.95 | 98.60 |
| 2 | 92.55 | 87.00 | 89.69 | 99.22 | 98.00 |
| 3 | 93.00 | 92.08 | 92.54 | 96.99 | 95.50 |
| 4 | 88.15 | 88.81 | 88.48 | 98.15 | 96.90 |
| Macro Avg | 92.84 | 91.81 | 92.30 | 98.08 | 97.25 |
| Class | Precision% | Recall% | f1-Score% | Specificity% | Accuracy% |
|---|---|---|---|---|---|
| 1 | 88.80 | 93.65 | 91.16 | 90.06 | 91.90 |
| 2 | 82.78 | 88.72 | 85.64 | 95.53 | 95.40 |
| 3 | 91.88 | 82.06 | 86.69 | 97.43 | 93.60 |
| 4 | 96.00 | 83.72 | 89.44 | 99.67 | 98.30 |
| Macro Avg | 89.86 | 87.04 | 88.23 | 95.67 | 94.80 |
| References | Dataset | Methods Used | Avg. Sensitivity% | Avg. Specificity% |
|---|---|---|---|---|
| Kumar S. et al. [4] | DIABET DB1 | RBFN Network | 87 | 93 |
| Rahim S.S. et al. [2] | DIABET DB0 & DB1 | Circular Hough Transform | 80 | 55 |
| Kedir M. Adal et al. [34] | DIABET DB1 | KNN Classifier | 81.08 | 92.3 |
| Kobat, S. G [39] | APTOS | DenseNET | 80.6 | - |
| Our proposed method | APTOS | UNet and CNN with SVM | 91.81 | 98.08 |
| Our proposed method | MESSIDOR | UNet and CNN with SVM | 87.04 | 95.67 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jena, P.K.; Khuntia, B.; Palai, C.; Nayak, M.; Mishra, T.K.; Mohanty, S.N. A Novel Approach for Diabetic Retinopathy Screening Using Asymmetric Deep Learning Features. Big Data Cogn. Comput. 2023, 7, 25. https://doi.org/10.3390/bdcc7010025
Jena PK, Khuntia B, Palai C, Nayak M, Mishra TK, Mohanty SN. A Novel Approach for Diabetic Retinopathy Screening Using Asymmetric Deep Learning Features. Big Data and Cognitive Computing. 2023; 7(1):25. https://doi.org/10.3390/bdcc7010025
Chicago/Turabian StyleJena, Pradeep Kumar, Bonomali Khuntia, Charulata Palai, Manjushree Nayak, Tapas Kumar Mishra, and Sachi Nandan Mohanty. 2023. "A Novel Approach for Diabetic Retinopathy Screening Using Asymmetric Deep Learning Features" Big Data and Cognitive Computing 7, no. 1: 25. https://doi.org/10.3390/bdcc7010025
APA StyleJena, P. K., Khuntia, B., Palai, C., Nayak, M., Mishra, T. K., & Mohanty, S. N. (2023). A Novel Approach for Diabetic Retinopathy Screening Using Asymmetric Deep Learning Features. Big Data and Cognitive Computing, 7(1), 25. https://doi.org/10.3390/bdcc7010025