
Surveillance of Soil-Transmitted Helminth Infection in Preschool Child Population: Do Changes in Behavior and Immunological Responses Affect Prevalence?

 ,
,
Abstract
1. Introduction
2. Materials and Methods
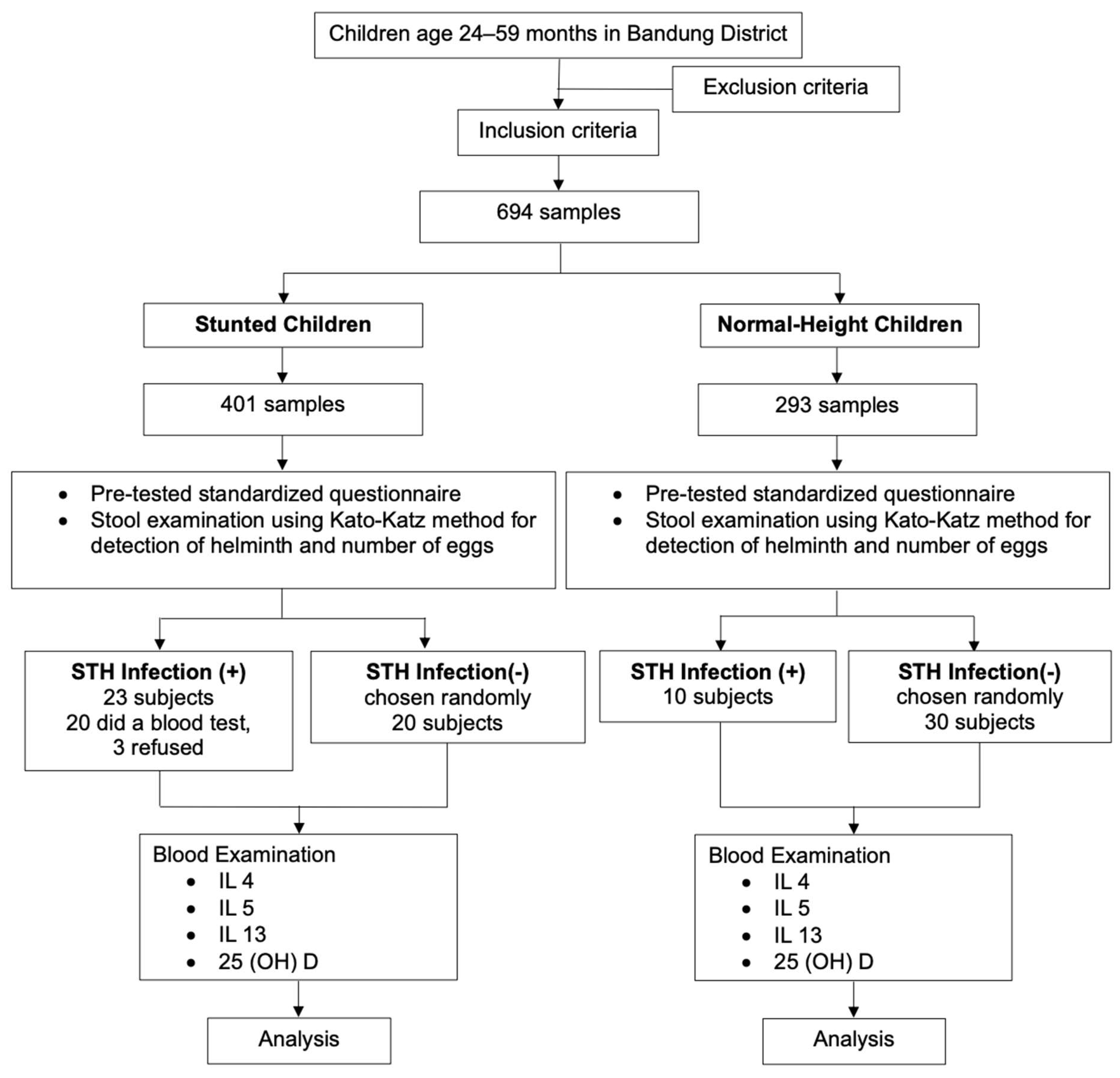
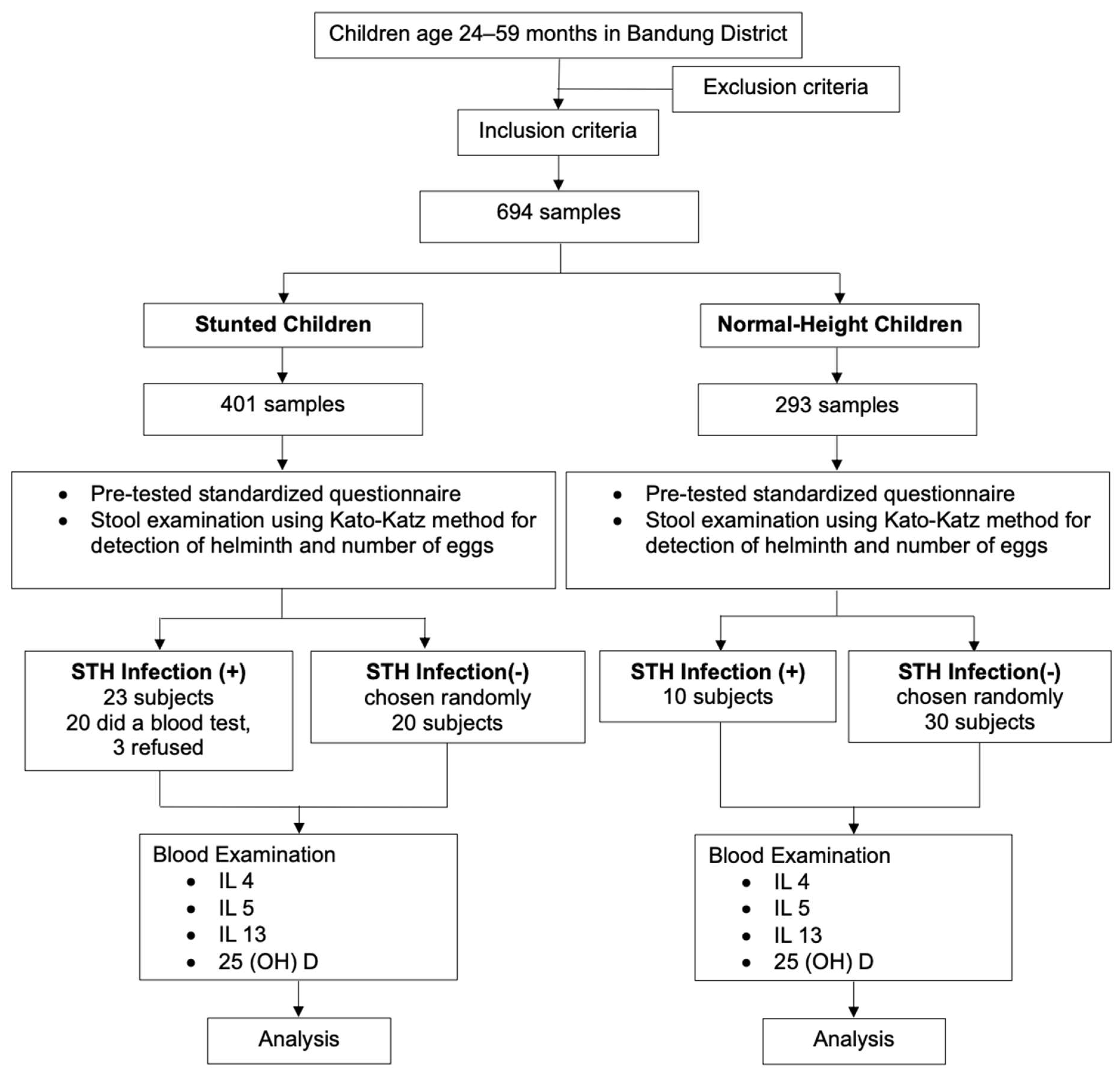
2.1. Study Design
2.2. Study Site and Population
2.3. Study Size and Sampling
2.4. Variables Measurement
2.5. Data Management and Analysis
3. Results
3.1. Participant Characteristics
3.2. Comparison of the Severity Levels of STH Infection in Normal Children and Stunted Children Based on Etiology
3.3. Correlation of 25(OH)D, IL-5, and IL-13 Levels with STH Infection
4. Discussion
5. Conclusions
6. Study Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hotez, P.J.; Lo, N.C. Neglected tropical diseases: Public health control programs and mass drug administration. In Hunter’s Tropical Medicine and Emerging Infectious Diseases; Tenth, E., Ed.; Elsevier: London, UK, 2020; pp. 209–213. [Google Scholar] [CrossRef]
- Reducing Stunting in Children: Equity Considerations for Achieving the Global Nutrition Targets 2025; World Health Organization: Geneva, Switzerland, 2018.
- Kurscheid, J.; Laksono, B.; Park, M.J.; Clements, A.C.A.; Sadler, R.; McCarthy, J.S.; Nery, S.V.; Soares-Magalhaes, R.; Halton, K.; Hadisaputro, S.; et al. Epidemiology of soil-transmitted helminth infections in Semarang, Central Java, Indonesia. PLoS Neglected Trop. Dis. 2020, 14, e0008907. [Google Scholar] [CrossRef]
- Water, Sanitation and Hygiene (WASH). Available online: https://www.who.int/health-topics/water-sanitation-and-hygiene-wash#tab=tab_1 (accessed on 4 October 2023).
- Novianty, S.; Dimyati, Y.; Pasaribu, S.; Pasaribu, A.P. Risk Factors for Soil-Transmitted Helminthiasis in Preschool Children Living in Farmland, North Sumatera, Indonesia. J. Trop. Med. 2018, 2018, 6706413. [Google Scholar] [CrossRef]
- Indonesia. Ministry of Health. Regulation of Minister of Health No. 15/2017. Helmenthiasis Control. 2017. Available online: http://hukor.kemkes.go.id/uploads/produk_hukum/PMK_No._15_ttg_Penanggulangan_Cacingan_.pdf (accessed on 20 January 2019).
- Hall, A. Micronutrient Supplements for Children after Deworming. Lancet Infect. Dis. 2007, 7, 297–302. [Google Scholar] [CrossRef]
- Hall, A.; Hewitt, G.; Tuffrey, V.; de Silva, N. A Review and Meta-Analysis of the Impact of Intestinal Worms on Child Growth and Nutrition. Matern. Child Nutr. 2008, 4 (Suppl. 1), 118–236. [Google Scholar] [CrossRef] [PubMed]
- Hesham, M.S.; Edariah, A.B.; Norhayati, M. Intestinal Parasitic Infections and Micronutrient Deficiency: A Review. Med. J. Malays. 2004, 59, 284–293. [Google Scholar]
- Manousaki, D.; Paternoster, L.; Standl, M.; Moffatt, M.F.; Farrall, M.; Bouzigon, E.; Strachan, D.P.; Demenais, F.; Lathrop, M.; Cookson, W.O.C.M.; et al. Vitamin D Levels and Susceptibility to Asthma, Elevated Immunoglobulin E Levels, and Atopic Dermatitis: A Mendelian Randomization Study. PLoS Med. 2017, 14, e1002294. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, S.P.; Chougule, A.A. Correlation of Serum Vitamin D Levels and Anemia in Childhood Pneumonia: A Case Control Study from Rural Area. Int. J. Contemp. Pediatr. 2017, 4, 756. [Google Scholar] [CrossRef]
- Jia, K.P.; Zhao, L.F.; Feng, N.; Ma, K.; Li, Y.X. Lower Level of Vitamin D3 Is Associated with Susceptibility to Acute Lower Respiratory Tract Infection (ALRTI) and Severity: A Hospital Based Study in Chinese Infants. Int. J. Clin. Exp. Med. 2017, 10, 7997–8003. [Google Scholar]
- Chowdhury, R.; Taneja, S.; Bhandari, N.; Sinha, B.; Upadhyay, R.P.; Bhan, M.K.; Strand, T.A. Vitamin-D Deficiency Predicts Infections in Young North Indian Children: A Secondary Data Analysis. PLoS ONE 2017, 12, e0170509. [Google Scholar] [CrossRef] [PubMed]
- Colombo, S.A.P.; Grencis, R.K. Immunity to Soil-Transmitted Helminths: Evidence From the Field and Laboratory Models. Front. Immunol. 2020, 11, 1286. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Soil Transmitted Helminth Infections. 2017. Available online: www.Who.Int/Intestinal_worms (accessed on 12 January 2020).
- Adrizain, R.; Setiabudi, D.; Faridah, L.; Fauziah, N.; Setiabudiawan, B. Challenges for national deworming policy in Indonesia: Experience from Bandung district West Java province. J. Public Health. 2022, 30, 1613–1618. [Google Scholar] [CrossRef]
- Schluter, P.J.; Kokaua, J.; Tautolo, E.-S.; Iusitini, L.; Richards, R.; Ruhe, T. Parental education related to their children’s health in late childhood and early adolescence for Pacific families within New Zealand. Sci. Rep. 2022, 12, 5313. [Google Scholar] [CrossRef]
- Wysocki, T.; Gavin, L. Paternal Involvement in the Management of Pediatric Chronic Diseases: Associations with Adherence, Quality of Life, and Health Status. J. Pediatr. Psychol. 2006, 31, 501–511. [Google Scholar] [CrossRef] [PubMed]
- Binga, W.E.; Houmsou, R.S.; Garba, L.C.; Amuta, E.U.; Santaya, K.L. Use of rivers’ water, inadequate hygiene, and sanitation as exposure of internally displaced persons (IDPs) to urogenital schistosomiasis and soil-transmitted helminthiasis in Jalingo Local Government Area (LGA), Taraba State, Nigeria. J. Water Sanit. Hyg. Dev. 2022, 12, 792–802. [Google Scholar] [CrossRef]
- Gizaw, Z.; Addisu, A.; Dagne, H. Effects of Water, Sanitation and Hygiene (WASH) Education on Childhood Intestinal Parasitic Infections in Rural Dembiya, Northwest Ethiopia: An Uncontrolled before-and-after Intervention Study. Environ. Health Prev. Med. 2019, 24, 16. [Google Scholar] [CrossRef] [PubMed]
- Faridah, L.; Fauziah, N.; Adrizain, R. Knowledge of Helminthiasis of People Living in Slum Areas of Bandung District, Indonesia. Maj. Kedokt. Bdg. 2021, 53, 223–228. [Google Scholar] [CrossRef]
- de Lima Corvino, D.F.; Horrall, S. Ascariasis. StatPearls. 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK430796/ (accessed on 24 January 2024).
- Hajare, S.T.; Mulu, T.; Upadhye, V.J.; Chauhan, N.M.; Eriso, F. Prevalence of Ascaris lumbricoides infections among elementary school children and associated risk factors from Southern Ethiopia. J. Parasit. Dis. 2022, 46, 643–652. [Google Scholar] [CrossRef]
- Phuphisut, O.; Poodeepiyasawat, A.; Yoonuan, T.; Watthanakulpanich, D.; Chotsiri, P.; Reamtong, O.; Mousley, A.; Gobert, G.N.; Adisakwattana, P. Transcriptome profiling of male and female Ascaris lumbricoides reproductive tissues. Parasites Vectors 2022, 15, 477. [Google Scholar] [CrossRef]
- Viswanath, A.; Yarrarapu, S.N.S.; Williams, M. Trichuris Trichiura Infection; StatPearls: Treasure Island, FL, USA, 2023. [Google Scholar]
- Tang, Y.T.; Gao, X.; Rosa, B.A.; Abubucker, S.; Hallsworth-Pepin, K.; Martin, J.; Tyagi, R.; Heizer, E.; Zhang, X.; Bhonagiri-Palsikar, V.; et al. Genome of the human hookworm Necator americanus. Nat. Genet. 2014, 46, 261–269. [Google Scholar] [CrossRef]
- Holland, C.; Sepidarkish, M.; Deslyper, G.; Abdollahi, A.; Valizadeh, S.; Mollalo, A.; Mahjour, S.; Ghodsian, S.; Ardekani, A.; Behniafar, H.; et al. Global prevalence of Ascaris infection in humans (2010–2021): A systematic review and meta-analysis. Infect. Dis. Poverty 2022, 11, 113. [Google Scholar] [CrossRef]
- García, O.P.; Zavala, G.A.; Campos-Ponce, M.; Polman, K. Nutrition and parasitism. In Encyclopedia of Human Nutrition, 4th ed.; Elsevier: Amsterdam, The Netherlands, 2023; Volume 1–4, pp. 541–548. [Google Scholar] [CrossRef]
- Wacker, M.; Holick, M.F. Sunlight and Vitamin D: A global perspective for health. Dermato-Endocrinology 2013, 5, 51–108. [Google Scholar] [CrossRef] [PubMed]
- Easton, A.V.; Raciny-Aleman, M.; Liu, V.; Ruan, E.; Marier, C.; Heguy, A.; Yasnot, M.F.; Rodriguez, A.; Loke, P. Immune Response and Microbiota Profiles during Coinfection with Plasmodium vivax and Soil-Transmitted Helminths. mBio 2020, 11, 10–1128. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, A.L.; Mahoney, D.L.; Gabrie, J.A. Interleukin-10 and soil-transmitted helminth infections in Honduran children. BMC Res. Notes 2015, 8, 55. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristic | STH Infection | p Value * | ||
|---|---|---|---|---|
| Positive (n = 33) | Negative (n = 661) | |||
| 1. | Sex | 0.491 | ||
| Male | 19 (57.5%) | 340 (51%) | ||
| Female | 14 (42.5%) | 321 (49%) | ||
| 2. | Body height | 0.156 | ||
| Stunted | 23 (5.7%) | 378 (94.3%) | ||
| Normal | 10 (3.4%) | 283 (96.6%) | ||
| 3. | Mother’s education: | 0.138 | ||
| Elementary school | 12 (9.2%) | 119 (90.8%) | ||
| Junior high school | 12 (4.0%) | 291 (96.0%) | ||
| Senior high school | 8 (3.4%) | 228 (96.6%) | ||
| Bachelor’s degree | 1 (4.2%) | 23 (95.8%) | ||
| 4. | Father’s education: | <0.001 | ||
| Elementary school | 15 (12.5%) | 105 (87.5%) | ||
| Junior high school | 7 (2.4%) | 281 (97.6%) | ||
| Senior high school | 9 (3.5%) | 250 (96.5%) | ||
| Bachelor’s degree | 2 (7.4%) | 25 (92.6%) | ||
| 5. | Nutritional status: | 0.674 | ||
| Severely underweight | 8 (4.3%) | 178 (95.7%) | ||
| Underweight | 9 (7.3%) | 114 (92.7%) | ||
| Normal | 16 (4.2%) | 366 (95.8%) | ||
| Overweight | 0 | 2 (100%) | ||
| Obese | 0 | 1 (100%) | ||
| 6. | Water sources | 0.009 | ||
| Tap water | 3 (1.8%) | 164 (98.2%) | ||
| Water well | 5 (3.5%) | 136 (96.5%) | ||
| Water pump | 3 (3.3%) | 87 (96.7%) | ||
| Water electric pump | 22 (8.4%) | 239 (91.6%) | ||
| Spring water | 0 | 35 (100%) | ||
| 7. | Distance between water sources and toilet | 0.002 | ||
| Less than 10 m | 23 (7.6%) | 280 (92.4%) | ||
| More than 10 m | 10 (2.6%) | 381 (97.4%) | ||
| 8. | Hand washing habit | 0.580 | ||
| With water only | 14 (4.3%) | 313 (95.7%) | ||
| With water and soap | 19 (5.2%) | 348 (94.8%) | ||
| 9. | Cleanliness of toenails | 0.013 | ||
| Clean | 23 (3.9%) | 566 (96.1%) | ||
| Dirty | 10 (9.5%) | 95 (90.5%) | ||
| Children Infected by Ascaris lumbricoides | ||||
|---|---|---|---|---|
| Subject | Species | Number of Eggs (epg) | Severity Levels of STH | Height per Age |
| Patient 4 | Ascaris lumbricoides | 250 epg | Mild | Normal |
| Patient 7 | Ascaris lumbricoides | 600 epg | Mild | Normal |
| Patient 8 | Ascaris lumbricoides | 2.000 epg | Mild | Normal |
| Patient 9 | Ascaris lumbricoides | 2676 epg | Mild | Normal |
| Patient 3 | Ascaris lumbricoides | 3.450 epg | Mild | Normal |
| Patient 5 | Ascaris lumbricoides | 22.600 epg | Moderate | Normal |
| Patient 6 | Ascaris lumbricoides | 33.450 epg | Moderate | Normal |
| Patient 2 | Ascaris lumbricoides | 37.250 epg | Moderate | Normal |
| Patient 1 | Ascaris lumbricoides | 172.250 epg | Severe | Normal |
| Patient 28 | Ascaris lumbricoides | 59 epg | Mild | Stunted |
| Patient 25 | Ascaris lumbricoides | 117 epg | Mild | Stunted |
| Patient 29 | Ascaris lumbricoides | 118 epg | Mild | Stunted |
| Patient 22 | Ascaris lumbricoides | 147 epg | Mild | Stunted |
| Patient 27 | Ascaris lumbricoides | 235 epg | Mild | Stunted |
| Patient 30 | Ascaris lumbricoides | 293 epg | Mild | Stunted |
| Patient 21 | Ascaris lumbricoides | 513 epg | Mild | Stunted |
| Patient 17 | Ascaris lumbricoides | 700 epg | Mild | Stunted |
| Patient 24 | Ascaris lumbricoides | 882 epg | Mild | Stunted |
| Patient 16 | Ascaris lumbricoides | 1.450 epg | Mild | Stunted |
| Patient 11 | Ascaris lumbricoides | 1.500 epg | Mild | Stunted |
| Patient 18 | Ascaris lumbricoides | 2.950 epg | Mild | Stunted |
| Patient 12 | Ascaris lumbricoides | 3.150 epg | Mild | Stunted |
| Patient 15 | Ascaris lumbricoides | 3.850 epg | Mild | Stunted |
| Patient 31 | Ascaris lumbricoides | 4.841 epg | Mild | Stunted |
| Patient 14 | Ascaris lumbricoides | 6.700 epg | Moderate | Stunted |
| Patient 26 | Ascaris lumbricoides | 19.450 epg | Moderate | Stunted |
| Patient 23 | Ascaris lumbricoides | 25.470 epg | Moderate | Stunted |
| Patient 13 | Ascaris lumbricoides | 28.500 epg | Moderate | Stunted |
| Patient 19 | Ascaris lumbricoides | 53.350 epg | Severe | Stunted |
| Patient 10 | Ascaris lumbricoides | 64.500 epg | Severe | Stunted |
| Patient 20 | Ascaris lumbricoides | 64.550 epg | Severe | Stunted |
| Variable | Group | p Value | |||
|---|---|---|---|---|---|
| A (n = 20) | B (n = 20) | C (n = 10) | D (n = 30) | ||
| 25(OH)D (ng/mL) | 28.773 (8.462) | 32.757 (12.432) | 32.128 (12.038) | 30.927 (11.248) | 0.701 |
| A vs. B | 0.258 | ||||
| A vs. C | 0.435 | ||||
| A vs. D | 0.501 | ||||
| B vs. C | 0.884 | ||||
| B vs. D | 0.568 | ||||
| C vs. D | 0.767 | ||||
| IL-5 (pg/mL) | 60.886 (21.812–216.271) | 89.508 (25.050–199.098) | 71.575 (18.624–190.132 | 81.262 (10.867–309.279) | 0.080 |
| A vs. B | 0.006 | ||||
| A vs. C | 0.397 | ||||
| A vs. D | 0.104 | ||||
| B vs. C | 0.183 | ||||
| B vs. D | 0.452 | ||||
| C vs. D | 0.656 | ||||
| IL-13 (pg/mL) | 5.456 (0.612–76.351) | 15.455 (0.853–386.627) | 11.839 (1.149–495.728) | 11.724 (1.637–222.731) | 0.063 |
| A vs. B | 0.010 | ||||
| A vs. C | 0.397 | ||||
| A vs. D | 0.022 | ||||
| B vs. C | 0.713 | ||||
| B vs. D | 0.362 | ||||
| C vs. D | 0.939 | ||||
| Characteristics | STH Infection | p Value | ||
|---|---|---|---|---|
| Positive (n = 20) | Negative (n = 20) | |||
| 1. | Sex | 0.527 | ||
| Male | 11 | 9 | ||
| Female | 9 | 11 | ||
| 2. | Mother’s education: | 0.604 | ||
| Elementary school | 6 | 9 | ||
| Junior high school | 10 | 7 | ||
| Senior high school | 4 | 3 | ||
| Bachelor’s degree | 0 | 1 | ||
| 3. | Father’s Education: | 0.187 | ||
| Elementary school | 10 | 4 | ||
| Junior high school | 5 | 9 | ||
| Senior high school | 5 | 6 | ||
| Bachelor’s degree | 0 | 1 | ||
| 4. | Nutritional Status: | 0.618 | ||
| Severely underweight | 9 | 7 | ||
| Underweight | 6 | 9 | ||
| Normal | 5 | 4 | ||
| 5. | Water sources | 0.020 | ||
| Tap water | 1 | 6 | ||
| Water well | 4 | 5 | ||
| Water pump | 3 | 6 | ||
| Water electric pump | 12 | 0 | ||
| Spring water | 0 | 3 | ||
| 6. | Distance between water sources and toilet | 0.011 | ||
| Less than 10 me | 14 | 6 | ||
| More than 10 m | 6 | 14 | ||
| 7. | Hand-washing habits | 0.744 | ||
| With water only | 7 | 8 | ||
| With water and soap | 13 | 12 | ||
| 8. | Cleanliness of toenails | 0.525 | ||
| Clean | 12 | 10 | ||
| Dirty | 8 | 10 | ||
| Variable | Cut-Off Point | AUROC (95% CI) |
|---|---|---|
| 25(OH)D (ng/mL) | ≤42.202 | 0.605 (0.438–0.756) |
| IL-5 (pg/mL) | ≤62.774 | 0.750 (0.588–0.873) |
| IL-13 (pg/mL) | ≤6.708 | 0.735 (0.572–0.862) |
| Variable | STH Infection | p Value * | OR (95% CI) | |
|---|---|---|---|---|
| Negative (n = 20) | Positive (n = 20) | |||
| 25(OH)D (ng/mL) | 0.020 ** | - | ||
| ≤42.202 | 20 | 14 | ||
| >42.202 | 0 | 6 | ||
| IL-5 (pg/mL) | 0.008 | 6.93 (1.53–31.38) | ||
| ≤62.774 | 11 | 3 | ||
| >62.774 | 9 | 17 | ||
| IL-13 (pg/mL) | <0.001 | 16.71 (2.98–93.88) | ||
| ≤6.708 | 13 | 2 | ||
| >6.708 | 7 | 19 | ||
| Variable | Coef B | SE (B) | p Value | ORadj (95% CI) |
|---|---|---|---|---|
| IL-5 (≤62.774) | 2.239 | 1.287 | 0.041 | 9.38 (1.13–77.88) |
| IL-13 (≤6.708) | 3.166 | 1.290 | 0.007 | 23.71 (2.84–197.94) |
| Distance between water sources with toilet (<10 m) | 2.380 | 1.173 | 1.173 | 10.81 (1.57–74.40) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adrizain, R.; Nagari, M.V.; Sukandar, H.; Berbudi, A.; Setiabudi, D.; Setiabudiawan, B. Surveillance of Soil-Transmitted Helminth Infection in Preschool Child Population: Do Changes in Behavior and Immunological Responses Affect Prevalence? Trop. Med. Infect. Dis. 2024, 9, 33. https://doi.org/10.3390/tropicalmed9020033
Adrizain R, Nagari MV, Sukandar H, Berbudi A, Setiabudi D, Setiabudiawan B. Surveillance of Soil-Transmitted Helminth Infection in Preschool Child Population: Do Changes in Behavior and Immunological Responses Affect Prevalence? Tropical Medicine and Infectious Disease. 2024; 9(2):33. https://doi.org/10.3390/tropicalmed9020033
Chicago/Turabian StyleAdrizain, Riyadi, Monika Verena Nagari, Hadyana Sukandar, Afiat Berbudi, Djatnika Setiabudi, and Budi Setiabudiawan. 2024. "Surveillance of Soil-Transmitted Helminth Infection in Preschool Child Population: Do Changes in Behavior and Immunological Responses Affect Prevalence?" Tropical Medicine and Infectious Disease 9, no. 2: 33. https://doi.org/10.3390/tropicalmed9020033
APA StyleAdrizain, R., Nagari, M. V., Sukandar, H., Berbudi, A., Setiabudi, D., & Setiabudiawan, B. (2024). Surveillance of Soil-Transmitted Helminth Infection in Preschool Child Population: Do Changes in Behavior and Immunological Responses Affect Prevalence? Tropical Medicine and Infectious Disease, 9(2), 33. https://doi.org/10.3390/tropicalmed9020033