

Correlates of Depression in ART Adherence among Youths in Lilongwe, Malawi


Abstract
:1. Introduction
1.1. ART Services in Malawi
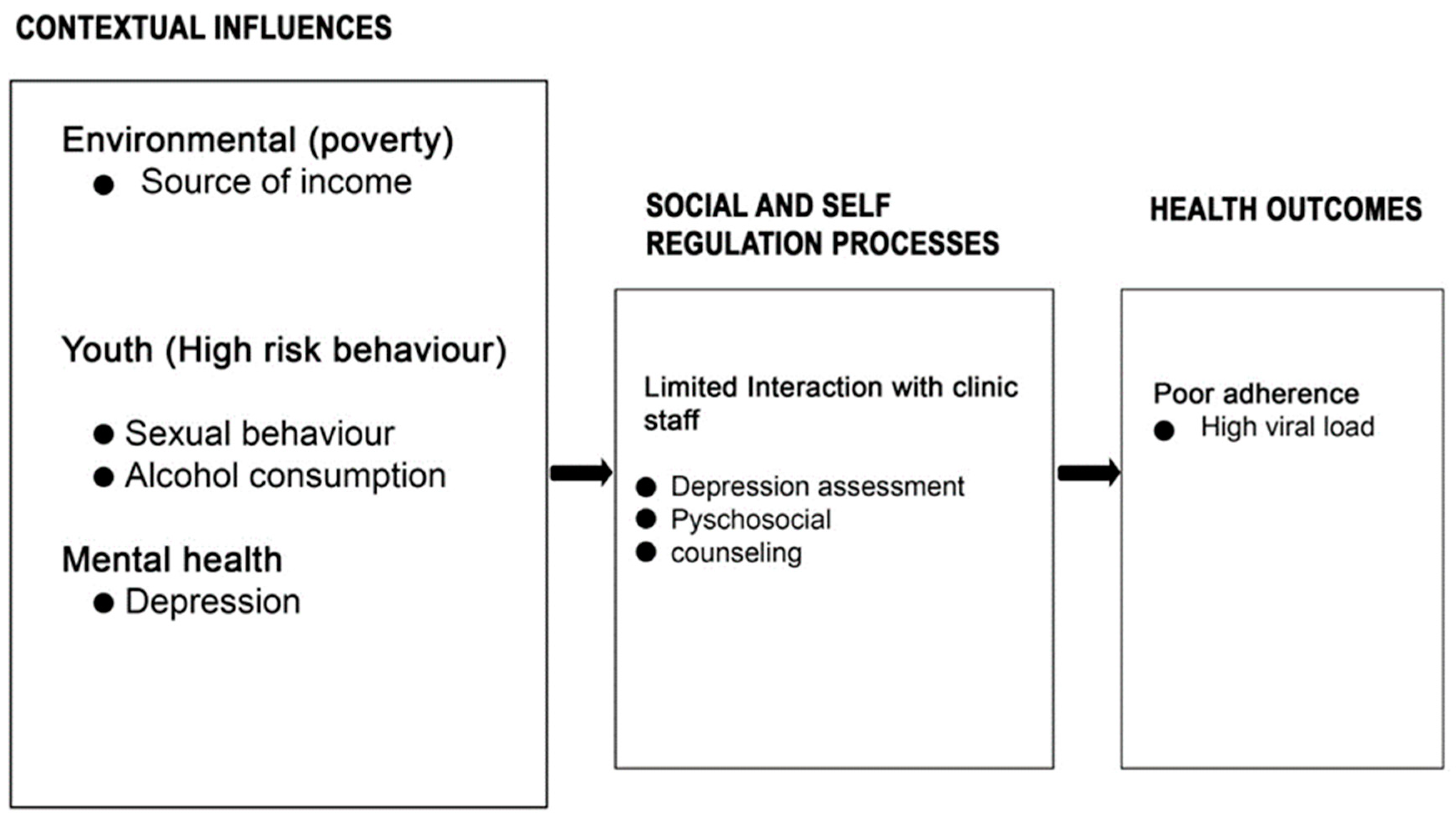
1.2. Conceptual Framework
1.3. Justification
2. Materials and Methods
2.1. Study Design
2.2. Study Place
2.3. Study Population
2.4. Sample Size and Sampling
2.5. Data Collection
2.5.1. Quantitative Method
2.5.2. Qualitative Method
2.6. Data Analysis
2.7. Ethical Considerations
3. Results
3.1. Quantitative Findings
3.1.1. Social and Demographic Characteristics of Study Participants
3.1.2. ART Adherence (Viral Load) Characteristics
3.1.3. Depression among the Youths
3.1.4. Bivariate Analysis
3.1.5. Multivariate Logistic Regression Results
3.2. Qualitative Findings
3.2.1. Explanatory Models for ART Non-Adherence amongst the Youths
Lack of Basic Needs
“Sometimes I am always busy doing peace work to earn money for my daily living, hence forgetting to take my daily medications” (Youth).
Lack of Privacy
“The youths who are in boarding facilities are challenged with privacy as they want to hide that they are on ARV’s and others are in an exploratory phase of different social behaviours, for example, smoking, alcohol and drug use influenced by their peers and later makes them forget taking ARV’s or stops taking ART” (ART Clinician).
“Because ARVs are unlike other drugs, they need strict privacy so that people will not discriminate against you. For instance, in the last six months of ART appointments, I have missed doses three times since I was at school, and there were many friends around me which made me fail to take up my ARV as prescribed” (Youth).
Psychological Trauma
“My relation once disclosed my status to others by speaking bad words such as look at this one. He is HIV positive, and this honestly made me think of stopping taking ARV’s so that I die and follow my parents, and sometimes it’s because of self-disclosure due to angriness that you have tested positive” (Youth)
3.3. Explanatory Models for Depression among the youths
3.3.1. Incomplete HIV Status Disclosure
“They tend to ask why they are the only ones with HIV in their house and why their parents failed to disclose to them when they were alive, which triggers confusion” (Psychosocial counsellor).
3.3.2. Shortage of Psychosocial Providers
“Only those youths presenting with depression symptoms are the ones given a chance to access the services on the adolescent clinic days because of shortage of psychosocial providers which even compromise on the quality of counselling services we do provide to the youths” (Psychosocial counsellor).
3.3.3. Knowledge Deficit of ART Providers to Screen Depression
“Other ART providers are not knowledgeable and skilled on youth’s depression assessments, which compromise the quality of care they receive at the clinic” (Nurse ART provider).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- UNAIDS, 2025 AIDS Targets; World AIDS Day Rep 2020; 2021; pp. 42–68. Available online: https://www.unaids.org/sites/default/files/2025-AIDS-Targets_en.pdf (accessed on 27 August 2023).
- Laurenzi, C.A.; Skeen, S.; Gordon, S.; Akin-Olugbade, O.; Abrahams, N.; Bradshaw, M.; Brand, A.; du Toit, S.; Melendez-Torres, G.J.; Tomlinson, M.; et al. Preventing mental health conditions in adolescents living with HIV: An urgent need for evidence. J. Int. AIDS Soc. 2020, 23, 65–70. [Google Scholar] [CrossRef] [PubMed]
- EGPAF, AIDS Free Generation Z. A Call to Action for Improving Youth-Focused HIV Programming Acknowledgements. Available online: https://www.pedaids.org/wp-content/uploads/2020/07/2020YouthReport_0706.pdf (accessed on 17 August 2023).
- Okonji, E.F.; van Wyk, B.; Mukumbang, F.C.; Hughes, G.D. Determinants of viral suppression among adolescents on antiretroviral treatment in Ehlanzeni district, South Africa: A cross-sectional analysis. AIDS Res. Ther. 2021, 18, 66. [Google Scholar] [CrossRef] [PubMed]
- Elashi, B.A.Y.; Van Wyk, B.E. Factors associated with viral suppression among adolescents on antiretroviral therapy in Free State province, South Africa. South Afr. J. HIV Med. 2022, 23, 1111–1118. [Google Scholar] [CrossRef] [PubMed]
- UNICEF. Support for Adolescents Living with HIV in Eastern and Southern Africa; UNICEF: New York, NY, USA, 2021. [Google Scholar]
- Jackson, C.; Rehman, A.M.; McHugh, G.; Gonzalez-Martinez, C.; Ngwira, L.G.; Bandason, T.; Mujuru, H.; Odland, J.O.; Corbett, E.L.; Ferrand, R.A.; et al. Risk factors for sustained virological non-suppression among children and adolescents living with HIV in Zimbabwe and Malawi: A secondary data analysis. BMC Pediatr. 2022, 22, 340. [Google Scholar] [CrossRef] [PubMed]
- Maccarthy, S.; Saya, U.; Samba, C.; Birungi, J.; Okoboi, S.; Linnemayr, S. “How am I going to live?”: Exploring barriers to ART adherence among adolescents and young adults living with HIV in Uganda. BMC Public Health 2018, 18, 1158. [Google Scholar] [CrossRef] [PubMed]
- Onyango, M.A.; Chergui, H.; Sabin, L.L.; Messersmith, L.J.; Sarkisova, N.; Oyombra, J.; Akello, P.; Kwaro, D.O.; Otieno, J. School-level Barriers of Antiretroviral Therapy Adherence and Interventions to Overcome them Among Adolescents Living with HIV in Western Kenya: A Qualitative Study. Open AIDS J. 2021, 15, 93–107. [Google Scholar] [CrossRef]
- Umar, E.; Levy, J.A.; Bailey, R.C.; Donenberg, G.; Hershow, R.C.; Mackesy-Amiti, M.E. Virological Non-suppression and Its Correlates Among Adolescents and Young People Living with HIV in Southern Malawi. AIDS Behav. 2019, 23, 513–522. [Google Scholar] [CrossRef]
- Wright, J.; Lubben, F.; Mkandawire, M.B. Young Malawians on the interaction between mental health and HIV/AIDS. Afr. J. AIDS Res. 2007, 6, 297–304. [Google Scholar] [CrossRef]
- Vreeman, R.C.; McCoy, B.M.; Lee, S. Mental health challenges among adolescents living with HIV. J. Int. AIDS Soc. 2017, 20 (Suppl. S3), 100–109. [Google Scholar] [CrossRef]
- Todd, J.V.; Cole, S.R.; Pence, B.W.; Lesko, C.R.; Bacchetti, P.; Cohen, M.H.; Feaster, D.J.; Gange, S.; Griswold, M.E.; Mack, W.; et al. Original Contribution Effects of Antiretroviral Therapy and Depressive Symptoms on All-Cause Mortality among HIV-Infected Women. Am. J. Epidemiol. 2017, 185, 869–878. [Google Scholar] [CrossRef]
- Faizi, N.; Kazmi, S. Universal health coverage—There is more to it than meets the eye. J. Fam. Med. Prim. Care 2017, 6, 169–170. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.H.; Mazenga, A.C.; Yu, X.; Devandra, A.; Nguyen, C.; Ahmed, S.; Kazembe, P.N.; Sharp, C. Factors associated with depression among adolescents living with HIV in Malawi. BMC Psychiatry 2015, 15, 264. [Google Scholar] [CrossRef] [PubMed]
- Truong, M.; Rane, M.S.; Govere, S.; Galagan, S.R.; Moosa, M.Y.; Stoep, A.V.; Celum, C.; Drain, P.K. Depression and anxiety as barriers to art initiation, retention in care, and treatment outcomes in KwaZulu-Natal, South Africa. eClinicalMedicine 2021, 31, 100621. [Google Scholar] [CrossRef] [PubMed]
- Uthman, O.A.; Magidson, J.F.; Safren, S.A.; Nachega, J.B. Depression and Adherence to Antiretroviral Therapy in Low-, Middle- and High-Income Countries: A Systematic Review and Meta-Analysis. Curr. HIV/AIDS Rep. 2015, 11, 291–307. [Google Scholar] [CrossRef] [PubMed]
- Ekat, M.H.; Yotebieng, M.; Leroy, V.; Mpody, C.; Diafouka, M.; Loubaki, G.; Nsondé, D.M.; Ossibi Ibara, B.R.; Bernard, C.; Sabin, C.; et al. Association between depressive symptoms and adherence among adolescents living with HIV in the Republic of Congo: A cross sectional study. Medicine 2020, 99, e21606. [Google Scholar] [CrossRef] [PubMed]
- Girma, D.; Assegid, S.; Gezahegn, Y. Depression and associated factors among HIV-positive youths attending antiretroviral therapy clinics in Jimma town, southwest Ethiopia. PLoS ONE 2021, 16, e0244879. [Google Scholar] [CrossRef] [PubMed]
- Oyedokun, G.E. Management Thoughts: The Review of Social Action Theory. SSRN Electron J. 2017. Available online: https://www.researchgate.net/publication/317995900_Management_Thoughts_The_Review_of_Social_Action_Theory/citation/download (accessed on 27 August 2023). [CrossRef]
- Seo, G.; Joseph, J.M.B.; Confident, N.; Jean, E.; Louis, B.; Bell, T.; Riche, R.C.; Belizaire, M.E.; Rouzier, V.; Apollon, A.; et al. The FANMI (“my FAMILY” in Creole) study to evaluate community-based cohort care for adolescent and young women living with HIV in Haiti: Protocol for a randomized controlled trial. BMC Public Health 2019, 19, 1749. [Google Scholar] [CrossRef]
- Farr, B.C. Designing Qualitative Research. Transform. Int. J. Holist. Mission Stud. 2008, 25, 165–166. [Google Scholar] [CrossRef]
- Ahrq, Q. Mixed Methods. AHRQ Publication No. 13-0028-EF March 2013. Available online: https://www.ahrq.gov/sites/default/files/wysiwyg/ncepcr/tools/PCMH/mixed-methods.pdf (accessed on 28 August 2023).
- Wagner, G.J.; Wagner, Z.; Gizaw, M.; Saya, U.; MacCarthy, S.; Mukasa, B.; Wabukala, P.; Linnemayr, S. Increased Depression during COVID-19 Lockdown Associated with Food Insecurity and Antiretroviral Non-Adherence among People Living with HIV in Uganda. AIDS Behav. 2022, 26, 2182–2190. [Google Scholar] [CrossRef]
- Kimera, E.; Vindevogel, S.; Kintu, M.J.; Rubaihayo, J.; De Maeyer, J.; Reynaert, D.; Engelen, A.-M.; Nuwaha, F.; Bilsen, J. Experiences and perceptions of youth living with HIV in Western Uganda on school attendance: Barriers and facilitators. BMC Public Health 2020, 20, 79. [Google Scholar] [CrossRef] [PubMed]
- Kip, E.C.; Udedi, M.; Kulisewa, K.; Go, V.F.; Gaynes, B.N. Stigma and mental health challenges among adolescents living with HIV in selected adolescent-specific antiretroviral therapy clinics in Zomba District, Malawi. BMC Pediatr. 2022, 22, 253. [Google Scholar] [CrossRef] [PubMed]
- Denison, J.A.; Packer, C.; Stalter, R.M.; Banda, H.; Mercer, S.; Nyambe, N.; Katayamoyo, P.; Mwansa, J.K.; McCarraher, D.R. Factors Related to Incomplete Adherence to Antiretroviral Therapy among Adolescents Attending Three HIV Clinics in the Copperbelt, Zambia. AIDS Behav. 2018, 22, 996–1005. [Google Scholar] [CrossRef] [PubMed]
- Joseph, R.S.; Mahiti, G.R.; Frumence, G.; Ulrich, C.M. Qualitative inquiry into adolescents’ experience of ethical challenges during enrollment and adherence to antiretroviral therapy (ART) in Temeke Regional Referral Hospital, Tanzania. BMC Med. Ethics 2022, 23, 22. [Google Scholar] [CrossRef]
- Tesfaye, Y.; Negash, A.; Gebrehiwot, T.T.; Tessema, W.; Anand, S.; Ahmed, G.; Alemu, D. Is There Association between Risky Sexual Behaviors and Depression Symptoms among Youth? A Case of Jimma University Students, Ethiopia. Psychiatry J. 2019, 2019, 3757656. [Google Scholar] [CrossRef]
- Okonji, E.F.; Mukumbang, F.C.; Orth, Z.; Vickerman-Delport, S.A.; Van Wyk, B. Psychosocial support interventions for improved adherence and retention in ART care for young people living with HIV (10–24 years): A scoping review. BMC Public Health 2020, 20, 1841. [Google Scholar] [CrossRef]

{kind=link}
| Characteristic | Frequency (n = 303) |
|---|---|
| Sex | |
| Male | 139 (46%) |
| Female | 164 (54%) |
| Total | 303 (100%) |
| Marital status | |
| Never married | 278 (92%) |
| Married | 22 (7%) |
| Divorced | 3 (1%) |
| Widow | 0 |
| Total | 303 (100%) |
| Religion | |
| Christianity | 273 (90%) |
| Islam | 30 (10%) |
| Total | 303 (100%) |
| Education | |
| None | 1 (0.3%) |
| Primary | 100 (33%) |
| Secondary | 192 (63%) |
| Tertiary | 10 (3%) |
| Total | 303 (100%) |
| Source of income | |
| Self | 45 (15%) |
| Parents | 223 (74%) |
| Guardians | 35 (12%) |
| Total | 303 (100%) |
| Alcohol consumption | |
| No | 271 (89%) |
| Yes | 32 (11%) |
| Total | 303 (100%) |
| Sexual behaviour | |
| None | 271 (89%) |
| One partner | 75 (25%) |
| Two partners | 14 (5%) |
| >Two partners | 7 (2%) |
| Total | 303 (100%) |
| Characteristics | Suppressed (n = 236) n (%) | Unsuppressed (n = 67) n (%) | p-Value |
|---|---|---|---|
| Age | |||
| 15–19 | 65 (28%) | 22 (33%) | |
| 20–24 | 171 (72%) | 45 (67%) | |
| Total | 236 (100%) | 67 (100%) | 0.398 |
| Sex | |||
| Male | 110 (47%) | 28 (42%) | |
| Female | 126 (53%) | 39 (58%) | |
| Total | 236 (100%) | 67 (100%) | 0.485 |
| Marital status | |||
| Never married | 226 (96%) | 63 (94%) | |
| Married | 8 (3%) | 3 (4%) | |
| Divorced | 2 (0.8%) | 1 (2%) | |
| Total | 236 (100%) | 67 (100%) | 0.816 |
| Religion | |||
| Christianity | 215 (91%) | 58 (87%) | |
| Islam | 21 (9%) | 9 (13%) | |
| Total | 236 (100%) | 67 (100%) | 0.273 |
| Education | |||
| None | 0 | 1 (2%) | |
| Primary | 78(33%) | 22 (33%) | |
| Secondary | 150(64%) | 24 (36%) | |
| Tertiary | 8((3%) | 2 (3%) | |
| 0.314 | 236(100%) | 67 (100%) | |
| Source of income | |||
| Self | 35 (15%) | 10 (15%) | |
| Parents | 173 (73%) | 50 (78%) | |
| Guardians | 28 (12%) | 7 (10%) | |
| Total | 236 (100%) | 67 (100%) | 0.950 |
| Alcohol consumption | |||
| No | 212 (90%) | 59 (88%) | |
| Yes | 24 (10%) | 8 (12%) | |
| Total | 236 (100%) | 67 (100%) | 0.677 |
| Sexual behaviour | |||
| None | 159 (67%) | 48 (72%) | |
| One partner | 59 (25%) | 16 (24%) | |
| Two partners | 13 (6%) | 1 (1%) | |
| >two partners | 5 (2%) | 2 (3%) | |
| Total | 236 (100%) | 67(100% | 0.541 |
| Characteristics | None (n = 232) | Mild (n = 51) | Moderate (n = 19) | Severe (n = 1) | p-Value |
|---|---|---|---|---|---|
| Age | |||||
| 15–19 | 72 (31%) | 10 (20%) | 5 (26%) | 0 | |
| 20–24 | 160 (69%) | 41 (80%) | 14 (74%) | 1 (100%) | |
| Total | 232 (100) | 51 (100) | 19 (100) | 1 (100%) | 0.372 |
| Sex | |||||
| Male | 103 (44%) | 27 (53%) | 8 (42%) | 0 | |
| Female | 129 (56%) | 24 (47%) | 11 (58%) | 1 (100%) | |
| Total | 232 (100) | 51 (100) | 19 (100) | 1 (100) | 0.537 |
| Marital status | |||||
| Never married | 220 (95%) | 49 (96%) | 19 (100%) | 1 (100%) | |
| Married | 9 (4%) | 2 (4%) | 0 | 0 | |
| Divorced | 3 (1%) | 0 | 0 | 0 | |
| Total | 232 (100%) | 51 (100%) | 19 (100%) | 1 (100%) | 0.941 |
| Religion | |||||
| Christianity | 210 (91%) | 44 (86%) | 18 (95%) | 1 (100%) | |
| Islam | 22 (9%) | 7(14%) | 1 (5%) | 0 | |
| Total | 232 (100%) | 51 (100%) | 19 (100%) | 1 (100%) | 0.694 |
| Education | |||||
| None | 1 (0.4%) | 0 | 0 | 0 | |
| Primary | 77 (33%) | 16 (31%) | 7 (37%) | 0 | |
| Secondary | 145 (63%) | 35 (69%) | 11 (58%) | 1 (100%) | |
| Tertiary | 9 (4%) | 0 | 1 (5%) | 0 | |
| Total | 232 (100%) | 51 (100%) | 19 (100%) | 1 (100%) | 0.942 |
| Source of income | |||||
| Self | 31 (13%) | 9 (18%) | 5 (26%) | 0 | |
| Parents | 183 (79%) | 29 (57%) | 10 (53%) | 1 (100%) | |
| Guardians | 18 (8%) | 13 (25%) | 4 (21%) | 0 | |
| Total | 232 (100%) | 51 (100%) | 19 (100%) | 1 (100%) | 0.003 |
| Alcohol consumption | |||||
| No | 211 (91%) | 45 (88%) | 15 (79%) | 0 | |
| Yes | 21 (9%) | 6 (12%) | 4 (21%) | 1 (100%) | |
| Total | 232 (100%) | 51 (100%) | 19 (100%) | 1 (100%) | 0.010 |
| Sexual behaviour | |||||
| None | 169 (73%) | 26 (51%) | 12 (63%) | 0 | |
| One partner | 51 (22%) | 17 (33%) | 6 (32%) | 19 (100%) | |
| Two partners | 7 (3%) | 7 (14%) | 0 | 0 | |
| >Two partners | 5 (2%) | 1 (2%) | 1 (5%) | 1 (100%) | |
| Total | 232 (100%) | 51 (100%) | 19 (100%) | 1 (100%) | 0.014 |
| Variable | Odds Ratio | p > [z] | 95% Confidence Level | |
|---|---|---|---|---|
| Source of income | ||||
| Self (reference) | 1 | |||
| Parents | 0.5975 | 0.188 | 0.2777 | 1.2855 |
| Guardians | 2.3149 | 0.08 | 0.904 | 5.9271 |
| Alcohol consumption | ||||
| No (reference) | 1 | |||
| Yes | 1.8993 | 0.142 | 0.8065 | 4.4728 |
| Sexual behaviour | ||||
| None (reference) | 1 | |||
| One partner | 2.01314 | 0.024 | 1.0976 | 3.7596 |
| Two partners | 2.1197 | 0.172 | 0.7211 | 6.2304 |
| More than two | 1.0967 | 0.922 | 0.1729 | 6.9553 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Msefula, M.C.; Umar, E. Correlates of Depression in ART Adherence among Youths in Lilongwe, Malawi. Trop. Med. Infect. Dis. 2024, 9, 2. https://doi.org/10.3390/tropicalmed9010002
Msefula MC, Umar E. Correlates of Depression in ART Adherence among Youths in Lilongwe, Malawi. Tropical Medicine and Infectious Disease. 2024; 9(1):2. https://doi.org/10.3390/tropicalmed9010002
Chicago/Turabian StyleMsefula, Mary Carolyne, and Eric Umar. 2024. "Correlates of Depression in ART Adherence among Youths in Lilongwe, Malawi" Tropical Medicine and Infectious Disease 9, no. 1: 2. https://doi.org/10.3390/tropicalmed9010002
APA StyleMsefula, M. C., & Umar, E. (2024). Correlates of Depression in ART Adherence among Youths in Lilongwe, Malawi. Tropical Medicine and Infectious Disease, 9(1), 2. https://doi.org/10.3390/tropicalmed9010002