

Clinical Diagnosis of Chikungunya Infection: An Essential Aid in a Primary Care Setting Where Serological Confirmation Is Not Available
 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. WHO CHIKV Infection Case Definition [31]
2.3. CHIKV Serological Analysis
2.4. Statistical Analysis
2.5. Agreement Consensus
3. Results
3.1. Study Participants
3.2. Demographics
3.3. Clinical Characteristics
3.4. Univariate Analysis
3.5. Agreement and Expert Consensus Results
3.6. Multiple Logistic Regression Analysis and ROC Curve
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Powers, A.M.; Brault, A.C.; Tesh, R.B.; Weaver, S.C. Re-emergence of chikungunya and o’nyong-nyong viruses: Evidence for distinct geographical lineages and distant evolutionary relationships. J. Gen. Virol. 2000, 81, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Tsetsarkin, K.A.; Vanlandingham, D.L.; McGee, C.E.; Higgs, S. A single mutation in Chikungunya virus affects vector specificity and epidemic potential. PLoS Pathog. 2007, 3, 1895–1906. [Google Scholar] [CrossRef] [PubMed]
- The Pan American Health Organization. Number of Reported Cases of Chikungunya Fever in the Americas, by Country or Territory Cumulative Cases (Updated 15 May 2015) Data Source: Cases Reported by IHR NFPs to PAHO/WHO and/or through Member States Websites or Official News Publication; The Pan American Health Organization: Washington, DC, USA, 2015; Volume 2015, p. 2048. [Google Scholar]
- Padilla, J.C.; Lizarazo, F.E.; Murillo, O.L.; Mendigaña, F.A.; Pachón, E.; Vera, M.J. Epidemiología de las principales enfermedades transmitidas por vectores en Colombia, 1990–2016. Biomédica 2017, 37, 27. [Google Scholar] [CrossRef]
- Rodas, J.D.; Kautz, T.; Camacho, E.; Paternina, L.; Guzmán, H.; Díaz, F.J.; Blanco, P.; Tesh, R.; Weaver, S.C. Genetic Characterization of Northwestern Colombian Chikungunya Virus Strains from the 2014–2015 Epidemic. Am. J. Trop. Med. Hyg. 2016, 95, 639–646. [Google Scholar] [CrossRef] [PubMed]
- Cassadou, S.; Boucau, S.; Petit-Sinturel, M.; Huc, P.; Leparc-Goffart, I.; Ledrans, M. Emergence of chikungunya fever on the French side of Saint Martin island, October to December 2013. Eurosurveillance 2014, 19, 20752. [Google Scholar] [CrossRef] [PubMed]
- Dengue Around the World|Dengue|CDC. Available online: https://www.cdc.gov/dengue/areaswithrisk/around-the-world.html (accessed on 4 December 2019).
- Geographic Distribution|Chikungunya Virus|CDC. Available online: https://www.cdc.gov/chikungunya/geo/index.html (accessed on 4 December 2019).
- Zika Travel Information|Travelers’ Health|CDC. Available online: https://wwwnc.cdc.gov/travel/page/zika-information (accessed on 4 December 2019).
- Kularatne, S.A.M.; Gihan, M.C.; Weerasinghe, S.C.; Gunasena, S. Concurrent outbreaks of Chikungunya and Dengue fever in Kandy, Sri Lanka, 2006–2007: A comparative analysis of clinical and laboratory features. Postgrad. Med. J. 2009, 85, 342–346. [Google Scholar] [CrossRef]
- Sissoko, D.; Ezzedine, K.; Moendandzé, A.; Giry, C.; Renault, P.; Malvy, D. Field evaluation of clinical features during chikungunya outbreak in Mayotte, 2005–2006. Trop. Med. Int. Heal. 2010, 15, 600–607. [Google Scholar] [CrossRef]
- Macpherson, C.; Noël, T.; Fields, P.; Jungkind, D.; Yearwood, K.; Simmons, M.; Widjaja, S.; Mitchell, G.; Noel, D.; Bidaisee, S.; et al. Clinical and serological insights from the asian lineage Chikungunya outbreak in Grenada, 2014: An observational study. Am. J. Trop. Med. Hyg. 2016, 95, 890–893. [Google Scholar] [CrossRef]
- Bloch, D.; Roth, N.M.; Caraballo, E.V.; Muñoz-Jordan, J.; Hunsperger, E.; Rivera, A.; Pérez-Padilla, J.; Rivera Garcia, B.; Sharp, T.M. Use of Household Cluster Investigations to Identify Factors Associated with Chikungunya Virus Infection and Frequency of Case Reporting in Puerto Rico. PLoS Negl. Trop. Dis. 2016, 10, e0005075. [Google Scholar] [CrossRef]
- van Genderen, F.T.; Krishnadath, I.; Sno, R.; Grunberg, M.G.; Zijlmans, W.; Adhin, M.R. First Chikungunya Outbreak in Suriname; Clinical and Epidemiological Features. PLoS Negl. Trop. Dis. 2016, 10, e0004625. [Google Scholar] [CrossRef]
- Anaya, J.-M.; Rodríguez, Y.; Monsalve, D.M.; Vega, D.; Ojeda, E.; González-Bravo, D.; Rodríguez-Jiménez, M.; Pinto-Díaz, C.A.; Chaparro, P.; Gunturiz, M.L.; et al. A comprehensive analysis and immunobiology of autoimmune neurological syndromes during the Zika virus outbreak in Cúcuta, Colombia. J. Autoimmun. 2017, 77, 123–138. [Google Scholar] [CrossRef]
- Godaert, L.; Bartholet, S.; Najioullah, F.; Hentzien, M.; Fanon, J.L.; Césaire, R.; Dramé, M. Screening for Chikungunya virus infection in aged people: Development and internal validation of a new score. PLoS ONE 2017, 12, e0181472. [Google Scholar] [CrossRef]
- Braga, J.U.; Bressan, C.; Dalvi, A.P.R.; Calvet, G.A.; Daumas, R.P.; Rodrigues, N.; Wakimoto, M.; Nogueira, R.M.R.; Nielsen-Saines, K.; Brito, C.; et al. Accuracy of Zika virus disease case definition during simultaneous Dengue and Chikungunya epidemics. PLoS ONE 2017, 12, e0179725. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.M.; Tauro, L.B.; Kikuti, M.; Anjos, R.O.; Santos, V.C.; Gonçalves, T.S.F.; Paploski, I.A.D.; Moreira, P.S.S.; Nascimento, L.C.J.; Campos, G.S.; et al. Concomitant transmission of dengue, chikungunya and Zika viruses in Brazil: Clinical and epidemiological findings from surveillance for acute febrile illness. Clin. Infect. Dis. 2019, 69, 1353–1359. [Google Scholar] [CrossRef] [PubMed]
- Carabali, M.; Lim, J.K.; Palencia, D.C.; Lozano-Parra, A.; Gelvez, R.M.; Lee, K.S.; Florez, J.P.; Herrera, V.M.; Kaufman, J.S.; Rojas, E.M.; et al. Burden of dengue among febrile patients at the time of chikungunya introduction in Piedecuesta, Colombia. Trop. Med. Int. Heal. 2018, 23, 1231–1241. [Google Scholar] [CrossRef]
- Sánchez-Carbonel, J.; Tantaléan-Yépez, D.; Aguilar-Luis, M.A.; Silva-Caso, W.; Weilg, P.; Vásquez-Achaya, F.; Costa, L.; Martins-Luna, J.; Sandoval, I.; del Valle-Mendoza, J. Identification of infection by Chikungunya, Zika, and Dengue in an area of the Peruvian coast. Molecular diagnosis and clinical characteristics. BMC Res. Notes 2018, 11, 175. [Google Scholar] [CrossRef] [PubMed]
- Azeredo, E.L.; Hoscher Romanholi, I.; Badolato-Corrêa, J.; Cunha, R.; Barbosa, L.S.; de-Oliveira-Pinto, L.M.; Dal Fabbro, M.; dos Santos, F.B.; Sánchez-Arcila, J.C.; Nunes, P.C.G.; et al. Clinical and Laboratory Profile of Zika and Dengue Infected Patients: Lessons Learned From the Co-circulation of Dengue, Zika and Chikungunya in Brazil. PLoS Curr. 2018, 10. [Google Scholar] [CrossRef] [PubMed]
- Lee, V.J.; Chow, A.; Zheng, X.; Carrasco, L.R.; Cook, A.R.; Lye, D.C.; Ng, L.C.; Leo, Y.S. Simple Clinical and Laboratory Predictors of Chikungunya versus Dengue Infections in Adults. PLoS Negl. Trop. Dis. 2012, 6, e1786. [Google Scholar] [CrossRef]
- Vega, F.L.R.; Bezerra, J.M.T.; Said, R.F.d.C.; da Gama Neto, A.N.; Cotrim, E.C.; Mendez, D.; Amâncio, F.F.; Carneiro, M. Emergence of chikungunya and Zika in a municipality endemic to dengue, Santa Luzia, MG, Brazil, 2015–2017. Rev. Soc. Bras. Med. Trop. 2019, 52, 1–9. [Google Scholar] [CrossRef]
- Taraphdar, D.; Sarkar, A.; Mukhopadhyay, B.B.; Chatterjee, S. A Comparative Study of Clinical Features between Monotypic and Dual Infection Cases with Chikungunya Virus and Dengue Virus in West Bengal, India. Am. J. Trop. Med. Hyg. 2012, 86, 720–723. [Google Scholar] [CrossRef]
- Mohd Zim, M.A.; Sam, I.-C.; Omar, S.F.S.; Chan, Y.F.; AbuBakar, S.; Kamarulzaman, A. Chikungunya infection in Malaysia: Comparison with dengue infection in adults and predictors of persistent arthralgia. J. Clin. Virol. 2013, 56, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Thiberville, S.D.; Boisson, V.; Gaudart, J.; Simon, F.; Flahault, A.; de Lamballerie, X. Chikungunya Fever: A Clinical and Virological Investigation of Outpatients on Reunion Island, South-West Indian Ocean. PLoS Negl. Trop. Dis. 2013, 7, e2004. [Google Scholar] [CrossRef] [PubMed]
- Sahadeo, N.; Mohammed, H.; Allicock, O.M.; Auguste, A.J.; Widen, S.G.; Badal, K.; Pulchan, K.; Foster, J.E.; Weaver, S.C.; Carrington, C.V.F. Molecular Characterisation of Chikungunya Virus Infections in Trinidad and Comparison of Clinical and Laboratory Features with Dengue and Other Acute Febrile Cases. PLoS Negl. Trop. Dis. 2015, 9, e0004199. [Google Scholar]
- Waggoner, J.J.; Gresh, L.; Vargas, M.J.; Ballesteros, G.; Tellez, Y.; Soda, K.J.; Sahoo, M.K.; Nuñez, A.; Balmaseda, A.; Harris, E.; et al. Viremia and Clinical Presentation in Nicaraguan Patients Infected With Zika Virus, Chikungunya Virus, and Dengue Virus. Clin. Infect. Dis. 2016, 63, 1584–1590. [Google Scholar] [CrossRef] [PubMed]
- Romero, C.; Zogbi, H.; Carvalho, M.S.; de Souza, R.V.; Calvet, G.A.; Brasil, P.; de Filippis, A.M.B.; Bressan, C.d.S.; de Mendonça, M.C.L.; Alves, S.S.; et al. Zika Virus Outbreak in Rio de Janeiro, Brazil: Clinical Characterization, Epidemiological and Virological Aspects. PLoS Negl. Trop. Dis. 2016, 10, e0004636. [Google Scholar]
- Danis-Lozano, R.; Díaz-González, E.E.; Trujillo-Murillo, K.d.C.; Caballero-Sosa, S.; Sepúlveda-Delgado, J.; Malo-García, I.R.; Canseco-Ávila, L.M.; Salgado-Corsantes, L.M.; Domínguez-Arrevillaga, S.; Torres-Zapata, R.; et al. Clinical characterization of acute and convalescent illness of confirmed chikungunya cases from Chiapas, S. Mexico: A cross sectional study. PLoS ONE 2017, 12, e0186923. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Chikungunya: Case definitions for acute, atypical and chronic cases. Conclusions of an expert consultation, Managua, Nicaragua, 20–21 May. Relev. Epidemiol. Hebd. 2015, 90, 410–414. [Google Scholar]
- Petti, C.A.; Polage, C.R.; Quinn, T.C.; Ronald, A.R.; Sande, M.A. Laboratory Medicine in Africa: A Barrier to Effective Health Care. Clin. Infect. Dis. 2006, 42, 377–382. [Google Scholar] [CrossRef]
- Salas Botero, D. Informe Final del Evento Chikungunya, Colombia 2014. Available online: https://www.ins.gov.co/buscador-eventos/Paginas/Info-Evento.aspx (accessed on 24 May 2018).
- Salas Botero, D. Informe Final del Evento Chikungunya, Colombia 2015. Available online: https://www.ins.gov.co/buscador-eventos/Paginas/Info-Evento.aspx (accessed on 24 May 2018).
- Pinilla Farias, A. Informe del Evento Chikungunya Periodo Epidemiológico XIII, Colombia 2016. Available online: https://www.ins.gov.co/buscador-eventos/Paginas/Info-Evento.aspx (accessed on 24 May 2018).
- Rodriguez Reyes, A.J. Informe del Evento Chikungunya, Colombia 2017. Available online: https://www.ins.gov.co/buscador-eventos/Paginas/Info-Evento.aspx (accessed on 24 May 2018).
- Instituto Nacional de Salud. Boletín Epidemiológico Semanal Semana Epidemiológica 52 23 al 29 de Diciembre de 2018; Instituto Nacional de Salud: Bogotá, Colombia, 2018. [Google Scholar]
- Instituto Nacional de Salud. Semana Epidemiológica 44; Instituto Nacional de Salud: Bogotá, Colombia, 2019. [Google Scholar]
- Rueda, J.C.; Santos, A.M.; Angarita, J.I.; Giraldo, R.B.; Saldarriaga, E.L.; Ballesteros Muñoz, J.G.; Forero, E.; Valencia, H.; Somoza, F.; Martin-Arsanios, D.; et al. Demographic and clinical characteristics of chikungunya patients from six Colombian cities, 2014–2015. Emerg. Microbes Infect. 2019, 8, 1490–1500. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Ávila, D.G.; Rojas, M.X.; Rosselli, D. Delphi method in rheumatology research: Are we doing well? Rev. Colomb. Reumatol. 2019, 27, 177–189. [Google Scholar]
- Trevethan, R. Sensitivity, Specificity, and Predictive Values: Foundations, Pliabilities, and Pitfalls in Research and Practice. Front. Public Heal. 2017, 5, 307. [Google Scholar] [CrossRef] [PubMed]
- OMS. Zika virus disease: Interim case definitions. In Who/Zikv/Sur/16.1 2016; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- World Health Organization. Dengue: Guidelines for Diagnosis Treatment Prevention and Control (New Edition 2009); World Health Organization: Geneva, Switzerland, 2009; ISBN 978-92-4-154787-1. [Google Scholar]
- Cleton, N.B.; Reusken, C.B.E.M.; Wagenaar, J.F.P.; van der Vaart, E.E.; Reimerink, J.; van der Eijk, A.A.; Koopmans, M.P.G. Syndromic Approach to Arboviral Diagnostics for Global Travelers as a Basis for Infectious Disease Surveillance. PLoS Negl. Trop. Dis. 2015, 9, e0004073. [Google Scholar] [CrossRef] [PubMed]
- Borgherini, G.; Poubeau, P.; Staikowsky, F.; Lory, M.; Moullec, N.L.; Becquart, J.P.; Wengling, C.; Michault, A.; Paganin, F. Outbreak of Chikungunya on Reunion Island: Early Clinical and Laboratory Features in 157 Adult Patients. Clin. Infect. Dis. 2007, 44, 1401–1407. [Google Scholar] [CrossRef]
- Kumar, R.; Sharma, M.; Jain, S.; Yadav, S.; Singhal, A. Cutaneous manifestations of chikungunya fever: Observations from an outbreak at a Tertiary Care Hospital in Southeast Rajasthan, India. Indian Dermatol. Online J. 2017, 8, 336. [Google Scholar] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Positive CHIKV Serology † (n = 295) | Negative CHIKV Serology ‡ (n = 253) | p Value | |
|---|---|---|---|
| Age in Years (mean ± SD) | 48.3 ± 17.4 | 49.6 ± 17.6 | |
| Gender | |||
| Female | 208 (70.5%) | 174 (68.8%) | |
| Male | 87 (29.5%) | 79 (31.2%) | |
| Age-group in Years | |||
| 18–29 | 60 (20.3%) | 37 (14.6%) | |
| 30–39 | 43 (14.6%) | 47 (18.6%) | |
| 40–49 | 42 (14.2%) | 45 (17.8%) | |
| 50–59 | 60 (20.3%) | 44 (17.4%) | |
| 60–69 | 56 (19.0%) | 44 (17.4%) | |
| 70–79 | 26 (8.8%) | 25 (9.9%) | |
| ≥80 | 8 (2.7%) | 11 (4.3%) | |
| WHO acute clinical case [31] | |||
| Fulfill criteria | 149 (50.5%) | 26 (10.3%) | <0.001 |
| Do not fulfill criteria | 146 (49.5%) | 227 (89.7%) | <0.001 |
| Positive CHIKV Serology † (n = 295) | Negative CHIKV Serology ‡ (n = 253) | Total (n = 548) | OR (CI) | p Value | |
|---|---|---|---|---|---|
| Systemic | |||||
| Fever | 151 (85.3%) | 26 (14.7%) | 177 (32.3%) | 9.1 (5.7–14.6) | <0.001 |
| Myalgia | 139 (85.8%) | 23 (14.2%) | 162 (29.6%) | 8.9 (5.5–14.5) | <0.001 |
| Whole body | 40 (95.2%) | 2 (4.8%) | 42 (7.7%) | 19.7 (4.7–82.3) | <0.001 |
| Extremities | 96 (82.1%) | 21 (17.9%) | 117 (21.4%) | 5.3 (3.2–8.9) | <0.001 |
| Back | 22 (84.6%) | 4 (15.4%) | 26 (4.7%) | 5.0 (1.7–14.7) | 0.001 |
| Fatigue | 173 (85.2%) | 30 (14.8%) | 203 (37.0%) | 10.5 (6.7–16.5) | <0.001 |
| Joint | |||||
| Arthralgia | 270 (57.0%) | 204 (43.0%) | 474 (86.5%) | 2.6 (1.5–4.3) | <0.001 |
| Symmetric | 240 (62.8%) | 142 (37.2%) | 382 (69.7%) | 3.4 (2.3–5.0) | <0.001 |
| Hands | 158 (68.4%) | 73 (31.6%) | 231 (42.2%) | 2.8 (1.9–4.0) | <0.001 |
| Wrists | 93 (67.9%) | 44 (32.1%) | 137 (25.0%) | 2.1 (1.4–3.3) | <0.001 |
| Elbows | 74 (66.7%) | 37 (33.3%) | 111 (20.3%) | 1.9 (1.3–3.0) | 0.002 |
| Shoulders | 81 (56.6%) | 62 (43.4%) | 143 (26.1%) | 1.2 (0.8–1.7) | 0.433 |
| Knees | 184 (62.6%) | 110 (37.4%) | 294 (53.6%) | 2.1 (1.5–3.0) | <0.001 |
| Ankles | 137 (74.1%) | 48 (25.9%) | 185 (33.8%) | 3.7 (2.5–5.4) | <0.001 |
| Feet | 104 (67.1%) | 51 (32.9%) | 155 (28.3%) | 2.2 (1.5–3.2) | <0.001 |
| Arthritis | 99 (91.7%) | 9 (8.3%) | 108 (19.7%) | 13.7 (6.7–27.8) | <0.001 |
| Symmetric | 90 (93.8%) | 6 (6.3%) | 96 (17.5%) | 18.1 (7.8–42.1) | <0.001 |
| Hands | 47 (95.9%) | 2 (4.1%) | 49 (8.9%) | 23.8 (5.7–99.0) | <0.001 |
| Wrists | 19 (95.0%) | 1 (5.0%) | 20 (3.6%) | 17.3 (2.3–130.5) | <0.001 |
| Elbows | 11 (91.7%) | 1 (8.3%) | 12 (2.2%) | 9.7 (1.2–76.1) | 0.008 |
| Shoulders | 9 (100.0%) | 0 (0.0%) | 9 (1.6%) | ||
| Knees | 22 (88.0%) | 3 (12.0%) | 25 (4.6%) | 6.7 (2.0–22.7) | <0.001 |
| Ankles | 47 (94.0%) | 3 (6.0%) | 50 (9.1%) | 15.8 (4.8–51.4) | <0.001 |
| Feet | 45 (97.8%) | 1 (2.2%) | 46 (8.4%) | 45.4 (6.2–332.0) | <0.001 |
| Dermatologic | |||||
| Rash | 132 (87.4%) | 19 (12.6%) | 151 (27.6%) | 9.9 (6.0–16.8) | <0.001 |
| Face | 94 (88.7%) | 12 (11.3%) | 106 (19.3%) | 9.4 (5.0–17.6) | <0.001 |
| Thorax | 84 (91.3%) | 8 (8.7%) | 92 (16.8%) | 12.2 (5.8–25.6) | <0.001 |
| Abdomen | 84 (92.3%) | 7 (7.7%) | 91 (16.6%) | 14.0 (6.3–31.0) | <0.001 |
| Back | 73 (91.3%) | 7 (8.7%) | 80 (14.6%) | 11.5 (5.2–25.6) | <0.001 |
| Extremities | 91 (86.7%) | 14 (13.3%) | 105 (19.2%) | 7.6 (4.2–13.7) | <0.001 |
| Pruritus | 87 (86.1%) | 14 (13.9%) | 101 (18.4%) | 7.1 (3.9–13.0) | <0.001 |
| Mucosa | 12 (85.7%) | 2 (14.3%) | 14 (2.6%) | 5.3 (1.2–24.0) | 0.015 |
| Oral | 9 (90.0%) | 1 (10.0%) | 10 (1.8%) | 7.9 (1.0–63.0) | 0.021 |
| Genital | 11 (84.6%) | 2 (15.4%) | 13 (2.4%) | 4.9 (1.1–22.1) | 0.024 |
| Gastrointestinal | |||||
| Diarrhea | 75 (83.3%) | 15 (16.7%) | 90 (16.4%) | 5.4 (3.0–9.6) | <0.001 |
| Emesis | 33 (82.5%) | 7 (17.5%) | 40 (7.3%) | 4.4 (1.9–10.1) | <0.001 |
| Nausea | 34 (85.0%) | 6 (15.0%) | 40 (7.3%) | 5.6 (2.2–13.0) | <0.001 |
| Abdominal pain | 23 (76.7%) | 7 (23.3%) | 30 (5.5%) | 3.0 (1.2–7.0) | 0.010 |
| Do You Consider as Clinical Criteria? | Totally Agree | Agree | Not Agree or Disagree | Disagree | Totally Disagree | Type of Agreement (Total) |
|---|---|---|---|---|---|---|
| Symmetrical joint involvement | 100 | 0 | 0 | 0 | 0 | Agree (100) |
| Abrupt onset of symptoms | 100 | 0 | 0 | 0 | 0 | Agree (100) |
| Fever | 38 | 50 | 12 | 0 | 0 | Agree (78) |
| Rash | 13 | 75 | 0 | 12 | 0 | Agree (88) |
| Mucosal involvement | 0 | 0 | 0 | 63 | 37 | Disagree (100) |
| Myalgia | 25 | 75 | 0 | 0 | 0 | Agree (100) |
| Fatigue | 63 | 25 | 12 | 0 | 0 | Agree (88) |
| Gastrointestinal involvement | 0 | 12 | 0 | 25 | 63 | Disagree (88) |
| Shoulder arthralgia | 0 | 25 | 12 | 38 | 25 | Disagree (63) |
| Shoulder arthritis | 0 | 0 | 0 | 38 | 62 | Disagree (100) |
| Elbow arthralgia | 0 | 0 | 0 | 88 | 12 | Disagree (100) |
| Elbow arthritis | 0 | 0 | 0 | 25 | 75 | Disagree (100) |
| Wrist arthralgia | 50 | 25 | 13 | 0 | 12 | Agree (75) |
| Wrist arthritis | 75 | 13 | 0 | 12 | 0 | Agree (88) |
| Hand arthralgia | 88 | 12 | 0 | 0 | 0 | Agree (100) |
| Hand arthritis | 88 | 12 | 0 | 0 | 0 | Agree (100) |
| Knee arthralgia | 13 | 63 | 0 | 12 | 12 | Agree (76) |
| Knee arthritis | 13 | 63 | 12 | 0 | 12 | Agree (76) |
| Ankle arthralgia | 100 | 0 | 0 | 0 | 0 | Agree (100) |
| Ankle arthritis | 100 | 0 | 0 | 0 | 0 | Agree (100) |
| Foot arthralgia | 50 | 38 | 0 | 12 | 0 | Agree (88) |
| Foot arthritis | 75 | 13 | 0 | 12 | 0 | Agree (88) |
| Odds Ratio | 95% Confidence Interval | p Value | Point Value | |
|---|---|---|---|---|
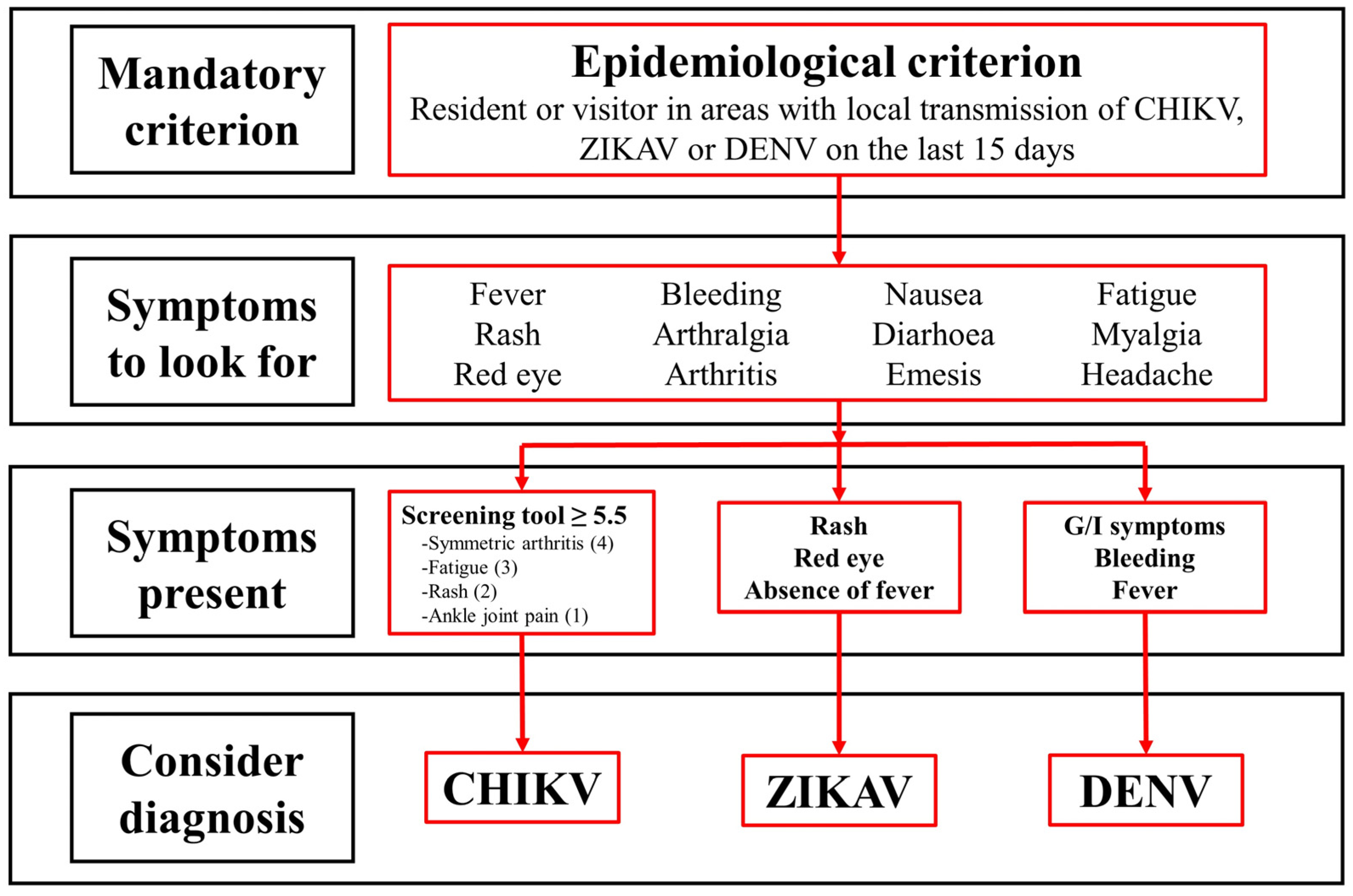
| Symmetric arthritis | 4.75 | 1.88–11.98 | 0.001 | 4 |
| Fatigue | 3.47 | 1.91–6.32 | <0.001 | 3 |
| Rash | 2.70 | 1.37–5.31 | 0.004 | 2 |
| Ankle joint pain | 1.69 | 1.06–2.68 | 0.026 | 1 |
| Sensitivity % (CI) | Specificity % (CI) | PPV % (CI) | NPV % (CI) | AUC (CI) | Accuracy % (CI) | YI % | |
|---|---|---|---|---|---|---|---|
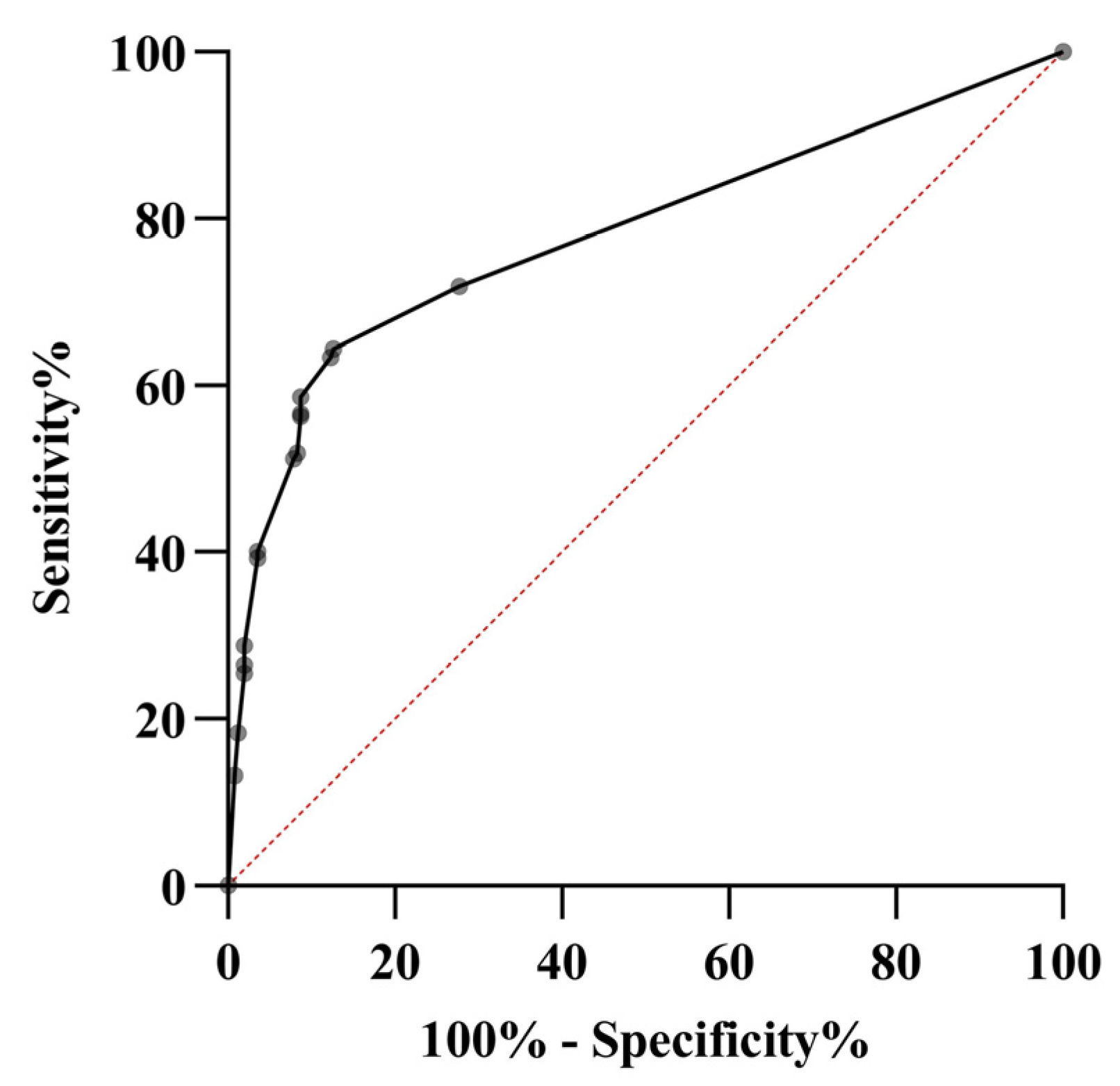
| Proposed screening tool (Score ≥ 5.5) | 64.4 (58.5–69.8) | 87.3 (82.6–91.1) | 85.5 (80.9–89.2) | 67.7 (64.1–71.1) | 0.72 (0.67–0.76) | 75.0 (71.1–78.5) | 52 |
| CHIKV WHO case definition (2015) [31] Fever + arthralgia | 51.2 (45.3–57.0) | 85.3 (85.3–93.1) | 85.3 (79.9–89.5) | 61.2 (58.2–64.1) | 0.71 (0.67–0.75) | 68.9 (64.9–72.8) | 36 |
| Sissoko (2010) [11] | |||||||
| Fever + arthralgia | 51.2 | 85.3 | 85.3 | 61.2 | 0.71 | 68.9 | 36 |
| (45.3–57.0) | (85.3–93.1) | (79.9–89.5) | (58.2–64.1) | (0.67–0.75) | (64.9–72.8) | ||
| Fever + myalgia | 62.3 | 88.9 | 86.7 | 66.9 | 0.75 | 74.6 | 51 |
| (56.5–67.9) | (84.4–92.5) | (82.1–90.4) | (63.4–70.2) | (0.71–0.79) | (70.7–78.2) | ||
| Thiberville (2013) [26] | |||||||
| Fever + arthralgia hands + | 62.3 (56.5–67.9) | 88.9 (84.4–92.5) | 86.7 (82.1–90.4) | 66.9 (63.4–70.2) | 0.76 (0.72–0.81) | 74.6 (70.7–78.2) | 51 |
| arthralgia wrists + | |||||||
| no myalgia | |||||||
| Cleton syndromic approach (2015) [40] | 57.2 | 90.5 | 87.5 | 64.5 | 0.74 | 72.6 | 48 |
| Arthritis + rash | (51.4–63.0) | (86.2–93.8) | (82.6–91.2) | (61.2–67.6) | (0.70–0.78) | (68.6–76.3) | |
| Macpherson (2016) [12] | |||||||
| Arthralgia + myalgia | 47.1 | 90.9 | 85.8 | 59.6 | 0.71 | 67.3 | 38 |
| (41.3–52.9) | (86.6–94.1) | (80.1–90.1) | (56.8–62.3) | (0.66–0.74) | (63.2–71.2) | ||
| Arthralgia + rash | 44.7 | 92.4 | 87.4 | 58.9 | 0.70 | 66.7 | 38 |
| (38.9–50.6) | (88.5–95.4) | (81.5–91.6) | (56.2–61.5) | (0.66–0.74) | (62.6–70.7) | ||
| Arthralgia + fever | 51.2 | 85.3 | 85.3 | 61.2 | 0.71 | 68.9 | 36 |
| (45.3–57.0) | (85.3–93.1) | (79.9–89.5) | (58.2–64.1) | (0.67–0.75) | (64.9–72.8) | ||
| ZIKAV WHO case definition (2016) [41] | |||||||
| Rash + fever + arthralgia | 58.8 | 87.7 | 84.8 | 64.7 | 0.74 | 72.2 | 46 |
| (53.1–64.6) | (83.1–91.5) | (79.9–88.7) | (61.3–67.9) | (0.70–0.78) | (68.3–75.9) | ||
| Rash + fever + arthritis | 62.3 | 86.5 | 84.4 | 66.3 | 0.76 | 73.5 | 49 |
| (56.5–67.9) | (81.7–90.5) | (79.6–88.2) | (62.8–69.7) | (0.72–0.80) | (69.6–77.1) | ||
| Rash + arthralgia | 44.7 | 92.4 | 87.4 | 58.9 | 0.70 | 66.7 | 38 |
| (38.9–50.6) | (88.5–95.4) | (81.5–91.6) | (56.2–61.5) | (0.66–0.74) | (62.6–70.7) | ||
| Rash + arthritis | 57.2 | 90.5 | 87.5 | 64.5 | 0.74 | 72.6 | 48 |
| (51.4–63.0) | (86.2–93.8) | (82.6–91.2) | (61.2–67.6) | (0.70–0.78) | (68.6–76.3) | ||
| Fever + arthralgia | 51.2 | 85.3 | 85.3 | 61.2 | 0.71 | 68.9 | 36 |
| (45.3–57.0) | (85.3–93.1) | (79.9–89.5) | (58.2–64.1) | (0.67–0.75) | (64.9–72.8) | ||
| Fever + arthritis | 57.2 | 87.7 | 84.5 | 63.7 | 0.73 | 71.3 | 45 |
| (51.4–63.0) | (83.1–91.5) | (79.4–88.4) | (60.5–66.9) | (0.69–0.77) | (67.3–75.1) | ||
| Braga ZIKAV (2017) [17] | |||||||
| No fever + rash | 58.9 | 87.7 | 84.8 | 64.7 | 0.74 | 72.2 | 47 |
| (53.1–64.6) | (83.1–91.5) | (79.9–88.7) | (61.3–67.9) | (0.69–0.78) | (68.3–75.9) | ||
| Rash + pruritus | 44.7 | 92.4 | 87.4 | 58.9 | 0.68 | 66.7 | 37 |
| (38.9–50.6) | (88.5–95.4) | (81.5–91.6) | (56.2–61.5) | (0.64–0.73) | (62.6–70.7) | ||
| No fever + pruritus | 55.9 | 88.9 | 85.4 | 63.3 | 0.72 | 71.1 | 45 |
| (50.0–61.6) | (84.4–92.5) | (80.3–89.4) | (60.1–66.4) | (0.68–0.76) | (67.1–74.9) | ||
| DENV WHO case definition (2009) [42] | |||||||
| Fever + nausea + rash | 60.7 | 87.7 | 85.2 | 65.6 | 0.74 | 73.1 | 48 |
| (54.8–66.2) | (83.1–91.5) | (80.3–89.0) | (62.2–68.9) | (0.70–0.78) | (69.2–76.8) | ||
| Fever + nausea + arthralgia | 55.2 | 89.3 | 85.7 | 63.1 | 0.72 | 70.9 | 45 |
| (49.3–61.0) | (84.8–92.8) | (80.6–89.7) | (59.9–66.1) | (0.68–0.77) | (66.9–74.7) | ||
| Fever + rash + arthralgia | 58.8 | 87.7 | 84.8 | 64.7 | 0.74 | 72.2 | 46 |
| (53.1–64.6) | (83.1–91.5) | (79.9–88.7) | (61.3–67.9) | (0.70–0.78) | (68.3–75.9) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rueda, J.C.; Peláez-Ballestas, I.; Angarita, J.-I.; Santos, A.M.; Pinzon, C.; Saldarriaga, E.-L.; Rueda, J.M.; Forero, E.; Saaibi, D.L.; Pavía, P.X.; et al. Clinical Diagnosis of Chikungunya Infection: An Essential Aid in a Primary Care Setting Where Serological Confirmation Is Not Available. Trop. Med. Infect. Dis. 2023, 8, 213. https://doi.org/10.3390/tropicalmed8040213
Rueda JC, Peláez-Ballestas I, Angarita J-I, Santos AM, Pinzon C, Saldarriaga E-L, Rueda JM, Forero E, Saaibi DL, Pavía PX, et al. Clinical Diagnosis of Chikungunya Infection: An Essential Aid in a Primary Care Setting Where Serological Confirmation Is Not Available. Tropical Medicine and Infectious Disease. 2023; 8(4):213. https://doi.org/10.3390/tropicalmed8040213
Chicago/Turabian StyleRueda, Juan C., Ingris Peláez-Ballestas, Jose-Ignacio Angarita, Ana M. Santos, Carlos Pinzon, Eugenia-Lucia Saldarriaga, Jorge M. Rueda, Elias Forero, Diego L. Saaibi, Paula X. Pavía, and et al. 2023. "Clinical Diagnosis of Chikungunya Infection: An Essential Aid in a Primary Care Setting Where Serological Confirmation Is Not Available" Tropical Medicine and Infectious Disease 8, no. 4: 213. https://doi.org/10.3390/tropicalmed8040213
APA StyleRueda, J. C., Peláez-Ballestas, I., Angarita, J.-I., Santos, A. M., Pinzon, C., Saldarriaga, E.-L., Rueda, J. M., Forero, E., Saaibi, D. L., Pavía, P. X., Mantilla, M. J., Rodríguez-Salas, G., Santacruz, J. C., Rueda, I., Cardiel, M. H., & Londono, J. (2023). Clinical Diagnosis of Chikungunya Infection: An Essential Aid in a Primary Care Setting Where Serological Confirmation Is Not Available. Tropical Medicine and Infectious Disease, 8(4), 213. https://doi.org/10.3390/tropicalmed8040213