A Brief History of the Major Rickettsioses in the Asia–Australia–Pacific Region: A Capstone Review for the Special Issue of TMID

 ,
,  , ,
, , 

Abstract
1. Introduction
2. History of Typhus
2.1. Early Accounts and History of “Typhus”
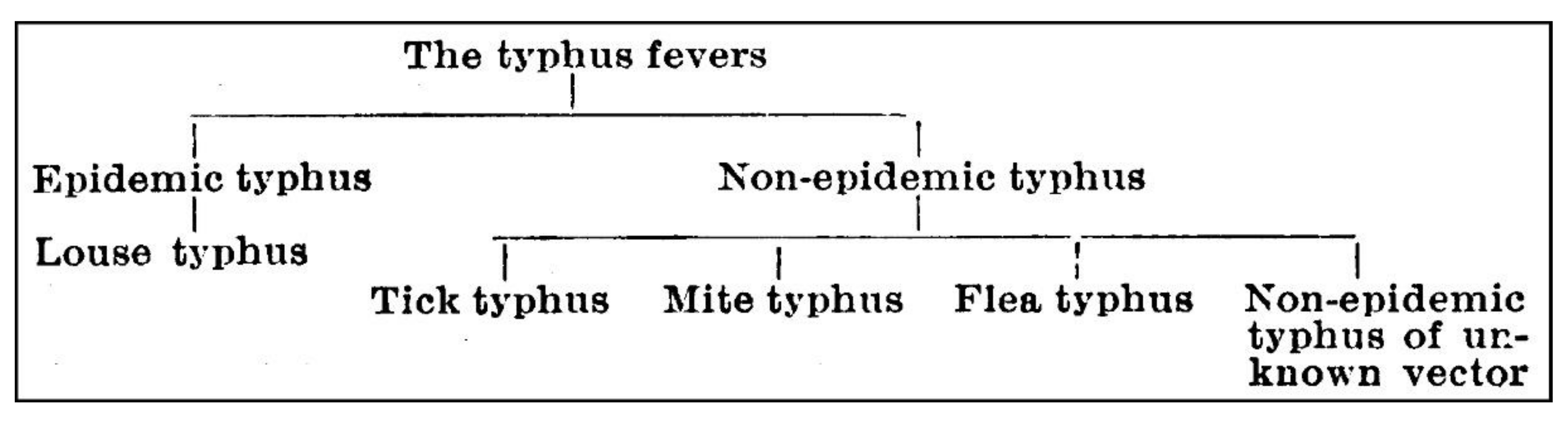
2.2. The Confusion of “Typhus”
3. Evolution of Scrub Typhus and Rickettsial Diagnostics
3.1. Weil–Felix Test
3.2. Complement Fixation Test
3.3. Indirect Immunofluorescence Assay
3.4. Rapid Diagnostic Tests
3.5. Rickettsial ELISA
4. Diagnosis in the Era of Recombinant Proteins, DNA Sequencing and PCR (1987 to Present)
4.1. Rickettsial ELISA Transformation: The Recombinants
4.2. IgM ELISA
4.3. Polymerase Chain Reaction (PCR) Diagnostics and Strain Typing
4.4. Gene Sequence Analysis
4.5. Quantitative PCR as an Emerging Diagnostic Tool
4.6. How Diagnostic Tools were Utilized in Studies Reported in the Special Issue
5. Evolution of Prevention and Treatments; Antibiotics and Rickettsial Vaccines in the AAP
5.1. Antibiotic Treatment of Scrub Typhus
5.2. Vaccines
6. Molecular Variation of Scrub Typhus and Murine Typhus
6.1. Use of Single Genes versus Multiple Locus Sequence Typing (MLST)
6.2. Genome Evolution within Rickettsial Species
6.3. Geographic Patterns of Genome Differentiation
6.4. Geographical Patterns of Single-Gene Differentiation
6.5. Transmission Factors That Affect Geographic Gene Differentiation
7. Where Are We in Our Study of Rickettsiology
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Zinsser, H. Rats, Lice and History; Little, Brown: Boston, MA, USA, 1935; p. 301. [Google Scholar]
- Bavaro, M.F.; Kelly, D.J.; Dasch, G.A.; Hale, B.R.; Olson, P. History of U.S. military contributions to the study of rickettsial diseases. Mil. Med. 2005, 170, 49–60. [Google Scholar] [CrossRef] [PubMed]
- Kelly, D.J.; Richards, A.L.; Temenak, J.; Strickman, D.; Dasch, G.A. The past and present threat of rickettsial diseases to military medicine and international public health. Clin. Infect. Dis. 2002, 34, S145–S169. [Google Scholar] [CrossRef] [PubMed]
- Luce-Fedrow, A.; Lehman, M.L.; Kelly, D.J.; Mullins, K.; Maina, A.N.; Stewart, R.L.; Ge, H.; John, H.S.; Jiang, J.; Richards, A.L. A review of scrub typhus (Orientia tsutsugamushi and related organisms): Then, now, and tomorrow. Trop. Med. Infect. Dis. 2018, 3, 8. [Google Scholar] [CrossRef] [PubMed]
- Abdad, M.Y.; Abou Abdallah, R.; Fournier, P.; Stenos, J.; Vasoo, S. A concise review of the epidemiology and diagnostics of rickettsioses: Rickettsia and Orientia spp. J. Clin. Microbiol. 2018, 56, 1728. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Richards, A.L. Scrub typhus: No longer restricted to the tsutsugamushi triangle. Trop. Med. Infect. Dis. 2018, 3, 11. [Google Scholar] [CrossRef] [PubMed]
- Richards, A.L.; Jiang, J. Scrub typhus: Historic perspective and current status of the worldwide presence of Orientia species. Trop. Med. Infect. Dis. 2020, 5, 49. [Google Scholar] [CrossRef] [PubMed]
- Fuller, H.S.; Smadel, J.E. Rickettsial diseases and the Korean conflict. In Medical Science Publication no. 4; U.S. Army Medical Department, Office of Medical History: Washington, DC, USA, 1954; Volume II, pp. 304–310. [Google Scholar]
- Blacksell, S.; Kingston, H.; Tanganuchitcharnchai, A.; Phanichkrivalkosil, M.; Hossain, M.; Hossain, A.; Ghose, A.; Leopold, S.; Dondorp, A.; Day, N.; et al. Diagnostic accuracy of the InBios Scrub Typhus Detect™ ELISA for the detection of IgM antibodies in Chittagong, Bangladesh. Trop. Med. Infect. Dis. 2018, 3, 95. [Google Scholar] [CrossRef] [PubMed]
- Evans, S.; Adcox, H.; VieBrock, L.; Green, R.; Luce-Fedrow, A.; Chattopadhyay, S.; Jiang, J.; Marconi, R.; Paris, D.; Richards, A.; et al. Outer membrane protein A conservation among Orientia tsutsugamushi isolates suggests its potential as a protective antigen and diagnostic target. Trop. Med. Infect. Dis. 2018, 3, 63. [Google Scholar] [CrossRef]
- Kelly, D.J.; Fuerst, P.A.; Richards, A.L. The historical case for and the future study of antibiotic-resistant scrub typhus. Trop. Med. Infect. Dis. 2017, 2, 63. [Google Scholar] [CrossRef]
- Kelly, D.J.; Fuerst, P.A.; Richards, A.L. Origins, importance and genetic stability of the prototype strains Gilliam, Karp and Kato of Orientia tsutsugamushi. Trop. Med. Infect. Dis. 2019, 4, 75. [Google Scholar] [CrossRef]
- Naoi, T.; Morita, M.; Kawakami, T.; Fujimoto, S. Hemophagocytic lymphohistiocytosis associated with scrub typhus: Systematic review and comparison between pediatric and adult cases. Trop. Med. Infect. Dis. 2018, 3, 19. [Google Scholar] [CrossRef] [PubMed]
- Sando, E.; Ariyoshi, K.; Fujita, H. Serological cross-reactivity among Orientia tsutsugamushi serotypes but not with Rickettsia japonica in Japan. Trop. Med. Infect. Dis. 2018, 3, 74. [Google Scholar] [CrossRef] [PubMed]
- Tshokey, T.; Stenos, J.; Durrheim, D.; Eastwood, K.; Nguyen, C.; Vincent, G.; Graves, S. Rickettsial infections and Q fever amongst febrile patients in Bhutan. Trop. Med. Infect. Dis. 2018, 3, 12. [Google Scholar] [CrossRef] [PubMed]
- Gautam, R.; Parajuli, K.; Sherchand, J.B. Epidemiology, risk factors and seasonal variation of scrub typhus fever in central Nepal. Trop. Med. Infect. Dis. 2019, 4, 27. [Google Scholar] [CrossRef]
- Aung, A.K.; Spelman, D.W.; Murray, R.J.; Graves, S. Rickettsial infections in Southeast Asia: Implications for local populace and febrile returned travelers. Am. J. Trop. Med. Hyg. 2014, 91, 451–460. [Google Scholar] [CrossRef]
- Robinson, M.T.; Satjanadumrong, J.; Hughes, T.; Stenos, J.; Blacksell, S.D. Diagnosis of spotted fever group rickettsia infections: The Asian perspective. Epidemiol. Infect. 2019, 147, e286. [Google Scholar] [CrossRef]
- Satjanadumrong, J.; Robinson, M.T.; Hughes, T.; Blacksell, S.D. Distribution and ecological drivers of spotted fever group Rickettsia in Asia. EcoHealth 2019, 16, 611–626. [Google Scholar] [CrossRef]
- Campbell, R.W.; Domrow, R. Rickettsioses in Australia: Isolation of Rickettsia tsutsugamushi and R. australis from naturally infected arthropods. Trans. R. Soc. Trop. Med. Hyg. 1974, 68, 397–402. [Google Scholar] [CrossRef]
- Stewart, A.; Armstrong, M.; Graves, S.; Hajkowicz, K. Clinical manifestations and outcomes of Rickettsia australis infection: A 15-year retrospective study of hospitalized patients. Trop. Med. Infect. Dis. 2017, 2, 19. [Google Scholar] [CrossRef]
- Salgado Lynn, M.; William, T.; Tanganuchitcharnchai, A.; Jintaworn, S.; Thaipadungpanit, J.; Lee, M.; Jalius, C.; Daszak, P.; Goossens, B.; Hughes, T. Spotted fever rickettsiosis in a wildlife researcher in Sabah, Malaysia: A case study. Trop. Med. Infect. Dis. 2018, 3, 29. [Google Scholar] [CrossRef]
- Shirai, A.; Bozeman, F.M.; Humphries, J.W.; Elisberg, B.L.; Faber, J.E. Experimental infection of the cotton rat Sigmodon hispidus with Rickettsia rickettsii. J. Bacteriol. 1967, 94, 1334–1339. [Google Scholar] [CrossRef] [PubMed]
- Sirisanthana, T.; Pinyopornpanit, V.; Sirisanthana, V.; Strickman, D.; Kelly, D.J.; Dasch, G.A. First cases of spotted fever group rickettsiosis in Thailand. Am. J. Trop. Med. Hyg. 1994, 50, 682–686. [Google Scholar] [CrossRef] [PubMed]
- Stenos, J.; Roux, V.; Walker, D.; Raoult, D. Rickettsia honei sp. nov., the aetiological agent of Flinders Island spotted fever in Australia. Int. J. Syst. Evol. Microbiol. 1998, 48, 1399–1404. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Sangkasuwan, V.; Lerdthusnee, K.; Sukwit, S.; Chuenchitra, T.; Rozmajzl, P.J.; Eamsila, C.; Jones, J.W.; Richards, A.L. Human infection with Rickettsia honei, Thailand. Emerg. Infect. Dis. 2005, 11, 1473. [Google Scholar] [CrossRef]
- Uchida, T.; Uchiyama, T.; Kumano, K.; Walker, D.H. Rickettsia japonica sp. nov., the etiological agent of spotted fever group rickettsiosis in Japan. Int. J. Syst. Evol. Microbiol. 1992, 42, 303–305. [Google Scholar] [CrossRef]
- Yuhana, Y.; Tanganuchitcharnchai, A.; Sujariyakul, P.; Sonthayanon, P.; Chotivanich, K.; Paris, D.H.; Pukrittayakamee, S.; Blacksell, S.D.; Hanboonkunupakarn, B. Diagnosis of murine typhus by serology in peninsular Malaysia: A case report where rickettsial illnesses, leptospirosis and dengue co-circulate. Trop. Med. Infect. Dis. 2019, 4, 23. [Google Scholar] [CrossRef]
- Lewis, G. Lest We Forget Tropical Typhus; 19th AGM/Seminar; The Malaysian Society of Parasitology and Tropical Medicine: Kuala Lumpur, Malaysia, 1983; pp. 1–6. Available online: https://cpb-us-w2.wpmucdn.com/u.osu.edu/dist/c/37470/files/2019/09/George-Lewis-tropical-typhus-lecture.pdf (accessed on 3 September 2020).
- Chadwick, J.; Mann, W.N. The Medical Works of Hippocrates: A New Translation from the Original Greek Made Especially for English Readers; Blackwell: Oxford, UK, 1950; p. 301. [Google Scholar]
- Weiss, K. The role of rickettsioses in history. In Biology of Rickettsial Diseases, Volume I; Walker, D.H., Ed.; CRC Press: Boca Raton, FL, USA, 2008; pp. 1–14. [Google Scholar]
- Dupont, H.T. Histoire du typhus. Méd. Mal. Infect. 1995, 25, 823–829. [Google Scholar] [CrossRef]
- Gerhard, W.W. ARTICLE I. On the typhus fever which occurred at Philadelphia in the Spring and Summer of 1836. Am. J. Med. Sci. 1837, 40, 289–321. [Google Scholar] [CrossRef]
- Gerhard, W.W. Art. I. On the typhus fever, which occurred at Philadelphia in the Spring and Summer of 1836; illustrated by clinical observations at the Philadelphia Hospital; showing the distinction between this form of disease and dothinenteritis or the typhoid fever with alteration of the follicles of the small intestine. Am. J. Med Sci. 1837, 19, 288–315. [Google Scholar]
- Hansen, W.; Freney, J. Le typhus épidémique, sa transmission et la découverte de l’agent étiologique. Lyon Pharm. 1996, 3, 130–138. [Google Scholar]
- Weil, E.; Felix, A. Zur serologischen diagnose des fleckfiebers. Wien. Klin. Wschr. 1916, 29, 33–36. [Google Scholar]
- Fletcher, W.; Lesslar, J.E. Tropical Typhus in the Federated Malay States with a Compilation on Epidemic Typhus. Bull. Inst. Med. Res. 1925, 2, 88. [Google Scholar]
- Fletcher, W.; Lesslar, J.E. Tropical typhus and brill’s disease. J. Trop. Med. Hyg. 1926, 29, 374–378. [Google Scholar]
- Hone, F.S. A series of cases closely resembling typhus fever. Med. J. Aust. 1922, 1, 1–13. [Google Scholar] [CrossRef]
- Fletcher, W. Tropical typhus. Br. Med. J. 1932, 2, 1140–1141. [Google Scholar] [CrossRef] [PubMed]
- Felix, A. Technique and interpretation of the Weil-Felix test in typhus fever. Trans. R. Soc. Trop. Med. Hyg. 1944, 37, 321–341. [Google Scholar] [CrossRef]
- Fletcher, W.; Lesslar, J.E.; Lewthwaite, R. The aetiology of the tsutsugamushi disease and tropical typhus in the Federated Malay States. part II. Trans. R. Soc. Trop. Med. Hyg. 1929, 23, 57–70. [Google Scholar] [CrossRef]
- Fletcher, W. Typhus-like fevers of unknown ætiology, with special reference to the Malay states. Proc. R. Soc. Med. 1930, 23, 1021–1030. [Google Scholar] [CrossRef]
- Megaw, J. The typhus group of fevers. Indian Med Gaz. 1924, 59, 68–75. [Google Scholar]
- Megaw, J. A typhus-like fever in India, possibly transmitted by ticks. Indian Med. Gaz. 1921, 56, 361–371. [Google Scholar]
- Megaw, J. Typhus fevers in the tropics. Br. Med. J. 1934, 2, 244–246. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, W. Tropical typhus in a training camp. J. R. Army Med. Corps 1925, 45, 274–284. [Google Scholar]
- Fletcher, W.; Lesslar, J.E.; Lewthwaite, R. The ætiology of the tsutsugamushi disease and tropical typhus in the Federated Malay States: A preliminary note. part I. Trans. R. Soc. Trop. Med. Hyg. 1928, 22, 161–174. [Google Scholar] [CrossRef]
- Maxcy, K.F.; Havens, L.C. A series of cases giving a positive Weil-Felix reaction. Am. J. Trop. Med. Hyg. 1923, 3, 495–507. [Google Scholar] [CrossRef]
- Maxcy, K.F. An epidemiological study of endemic typhus (Brill’s disease) in the southeastern United States: With special reference to its mode of transmission. Public Health Rep. 1926, 41, 2967–2995. [Google Scholar] [CrossRef]
- Philip, C.B. Tsutsugamushi disease (scrub typhus) in World War II. J. Parasitol. 1948, 34, 169–191. [Google Scholar] [CrossRef]
- Philip, C.B. Scrub typhus and scrub itch. In Communicable Diseases: Arthropod-borne Diseases Other Than Malaria; Coates, J.B., Jr., Hoff, E.B., Eds.; Medical Department, United States Army, Office of the Surgeon General, Department of the Army: Washington, DC, USA, 1964; Volume VII, pp. 275–348. [Google Scholar]
- Zarafonetis, C.J.D.; Baker, M.P. Scrub typhus. In Internal Medicine in World War II. Volume II: Infectious Diseases; Coates, J.B.J., Ed.; Medical Department, United States Army: Washington, DC, USA, 1963; pp. 111–142. [Google Scholar]
- Zarafonetis, C.J.D. The typhus fevers. In Internal Medicine in World War II. Volume II: Infectious Diseases; Coates, J.B.J., Ed.; Medical Department, United States Army: Washington, DC, USA, 1963; pp. 143–224. [Google Scholar]
- Azad, A.F. Epidemiology of murine typhus. Annu. Rev. Entomol. 1990, 35, 553–570. [Google Scholar] [CrossRef]
- Barrett, O.N.J.; Stark, F.R. Rickettsial Diseases and Leptospirosis. In Internal Medicine in Vietnam. Volume II; Ongibene, A.J., Barrett, O.N.J., Eds.; Medical Department, United States Army: Washington, DC, USA, 1982; pp. 133–163. [Google Scholar]
- Kawamura, R. Studies on Tsutsugamushi Disease (Japanese Blood Fever); Spokesman Printing Company: Cincinnati, OH, USA, 1926; p. 229. [Google Scholar]
- Mackie, T.T. Observations on tsutsugamushi disease (scrub typhus) in Assam and Burma preliminary report. Trans. R. Soc. Trop. Med. Hyg. 1946, 40, 15–56. [Google Scholar] [CrossRef]
- Audy, J.R.; Harrison, J.L. A review of investigations of mite typhus in Burma and Malaya, 1945–1950. Trans. R. Soc. Trop. Med. Hyg. 1951, 44, 371–404. [Google Scholar] [CrossRef]
- Bengtson, I.A. Apparent serological heterogeneity among strains of tsutsugamushi disease (scrub typhus). Public Health Rep. 1945, 60, 1483–1488. [Google Scholar] [CrossRef]
- Audy, J.R. Red Mites and Typhus; University of London, Athlone Press: London, UK, 1968; p. 191. [Google Scholar]
- Paris, D.H.; Dumler, J.S. State of the art of diagnosis of rickettsial diseases: The use of blood specimens for diagnosis of scrub typhus, spotted fever group rickettsiosis, and murine typhus. Curr. Opin. Infect. Dis. 2016, 29, 433–439. [Google Scholar] [CrossRef]
- Kelly, D.J.; Wong, P.W.; Gan, E.; Lewis, G.E., Jr. Comparative evaluation of the indirect immunoperoxidase test for the serodiagnosis of rickettsial disease. Am. J. Trop. Med. Hyg. 1988, 38, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Luce-Fedrow, A.; Mullins, K.; Kostik, A.P.; St John, H.K.; Jiang, J.; Richards, A.L. Strategies for detecting rickettsiae and diagnosing rickettsial diseases. Future Microbiol. 2015, 10, 537–564. [Google Scholar] [CrossRef] [PubMed]
- Bengtson, I.A.; Topping, N.H. Complement-fixation in rickettsial diseases. Am. J. Public Health 1942, 32, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Plotz, H. Complement fixation in rickettsial diseases. Science 1943, 97, 20–21. [Google Scholar] [CrossRef] [PubMed]
- Eisen, H.N. Complement (appendix). In Microbiology, 3rd ed.; Davis, B.D., Dulbecco, R., Eisen, H.N., Ginsberg, H.S., Eds.; Harper & Row: Philadelphia, PA, USA, 1980; pp. 463–466. [Google Scholar]
- Robinson, D.M.; Brown, G.; Gan, E.; Huxsoll, D.L. Adaptation of a microimmunofluorescence test to the study of human Rickettsia tsutsugamushi antibody. Am. J. Trop. Med. Hyg. 1976, 25, 900–905. [Google Scholar] [CrossRef] [PubMed]
- Bozeman, F.M.; Elisberg, B.L. Serological diagnosis of scrub typhus by indirect immunofluorescence. Proc. Soc. Exp. Biol. Med. 1963, 112, 568–573. [Google Scholar] [CrossRef]
- Kelly, D.J.; Wong, P.W.; Gan, E.; Chye, C.T.; Cowan, D.; Lewis, G.E., Jr. Multi-laboratory evaluation of a scrub typhus diagnostic kit. Am. J. Trop. Med. Hyg. 1990, 43, 301–307. [Google Scholar] [CrossRef]
- Kelly, D.J.; Chan, C.T.; Paxton, H.; Thompson, K.; Howard, R.; Dasch, G.A. Comparative evaluation of a commercial enzyme immunoassay for the detection of human antibody to Rickettsia typhi. Clin. Diagn. Lab. Immunol. 1995, 2, 356–360. [Google Scholar] [CrossRef]
- Pradutkanchana, J.; Silpapojakul, K.; Paxton, H.; Pradutkanchana, S.; Kelly, D.J.; Strickman, D. Comparative evaluation of four serodiagnostic tests for scrub typhus in Thailand. Trans. R. Soc. Trop. Med. Hyg. 1997, 91, 425–428. [Google Scholar] [CrossRef]
- Halle, S.; Dasch, G.A.; Weiss, E. Sensitive enzyme-linked immunosorbent assay for detection of antibodies against typhus rickettsiae, Rickettsia prowazekii and Rickettsia typhi. J. Clin. Microbiol. 1977, 6, 101–110. [Google Scholar] [PubMed]
- Dasch, G.A.; Halle, S.; Bourgeois, A.L. Sensitive microplate enzyme-linked immunosorbent assay for detection of antibodies against the scrub typhus rickettsia, Rickettsia tsutsugamushi. J. Clin. Microbiol. 1979, 9, 38–48. [Google Scholar]
- Clements, M.L.; Dumler, J.S.; Fiset, P.; Wisseman, C.L., Jr.; Snyder, M.J.; Levine, M.M. Serodiagnosis of rocky mountain spotted fever: Comparison of IgM and IgG enzyme-linked immunosorbent assays and indirect fluorescent antibody test. J. Infect. Dis. 1983, 148, 876–880. [Google Scholar] [CrossRef] [PubMed]
- Oaks, E.V.; Stover, C.K.; Rice, R.M. Molecular cloning and expression of Rickettsia tsutsugamushi genes for two major protein antigens in Escherichia coli. Infect. Immun. 1987, 55, 1156–1162. [Google Scholar] [CrossRef] [PubMed]
- Stover, C.K.; Marana, D.P.; Carter, J.M.; Roe, B.A.; Mardis, E.; Oaks, E.V. The 56-kilodalton major protein antigen of Rickettsia tsutsugamushi: Molecular cloning and sequence analysis of the sta56 gene and precise identification of a strain-specific epitope. Infect. Immun. 1990, 58, 2076–2084. [Google Scholar] [CrossRef] [PubMed]
- Stover, C.K.; Marana, D.P.; Dasch, G.A.; Oaks, E.V. Molecular cloning and sequence analysis of the Sta58 major antigen gene of Rickettsia tsutsugamushi: Sequence homology and antigenic comparison of Sta58 to the 60-kilodalton family of stress proteins. Infect. Immun. 1990, 58, 1360–1368. [Google Scholar] [CrossRef] [PubMed]
- Carl, M.; Tibbs, C.W.; Dobson, M.E.; Paparello, S.; Dasch, G.A. Diagnosis of acute typhus infection using the polymerase chain reaction. J. Infect. Dis. 1990, 161, 791–793. [Google Scholar] [CrossRef] [PubMed]
- Kelly, D.J.; Marana, D.P.; Stover, C.K.; Oaks, E.V.; Carl, M. Detection of Rickettsia tsutsugamushi by gene amplification using polymerase chain reaction techniques. Ann. N. Y. Acad. Sci. 1990, 590, 564–571. [Google Scholar] [CrossRef]
- Ching, W.; Rowland, D.; Zhang, Z.; Bourgeois, A.L.; Kelly, D.; Dasch, G.A.; Devine, P.L. Early diagnosis of scrub typhus with a rapid flow assay using recombinant major outer membrane protein antigen (r56) of Orientia tsutsugamushi. Clin. Diagn. Lab. Immunol. 2001, 8, 409–414. [Google Scholar] [CrossRef]
- Blacksell, S.D.; Tanganuchitcharnchai, A.; Nawtaisong, P.; Kantipong, P.; Laongnualpanich, A.; Day, N.P.J.; Paris, D.H. Diagnostic accuracy of the InBios scrub typhus detect enzyme-linked immunoassay for the detection of IgM antibodies in northern Thailand. Clin. Vaccine Immunol. 2016, 23, 148–154. [Google Scholar] [CrossRef]
- Saraswati, K.; Phanichkrivalkosil, M.; Day, N.P.J.; Blacksell, S.D. The validity of diagnostic cut-offs for commercial and in-house scrub typhus IgM and IgG ELISAs: A review of the evidence. PLoS Negl. Trop. Dis. 2019, 13, e0007158. [Google Scholar] [CrossRef] [PubMed]
- Scrub Typhus Diagnostics. 2014. Available online: http://inbios.com/wp-content/uploads/2016/06/Scrub-Typhus-ELISA-and-Rapid-develop.-05.16.pdf (accessed on 3 September 2020).
- Webb, L.; Carl, M.; Malloy, D.C.; Dasch, G.A.; Azad, A.F. Detection of murine typhus infection in fleas by using the polymerase chain reaction. J. Clin. Microbiol. 1990, 28, 530–534. [Google Scholar] [CrossRef] [PubMed]
- Wittwer, C.T.; Herrmann, M.G.; Moss, A.A.; Rasmussen, R.P. Continuous fluorescence monitoring of rapid cycle DNA amplification. BioTechniques 1997, 22, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Higuchi, R.; Fockler, C.; Dollinger, G.; Watson, R. Kinetic PCR analysis: Real-time monitoring of DNA amplification reactions. BioTechnology 1993, 11, 1026–1030. [Google Scholar] [CrossRef]
- Reller, M.E.; Dumler, J.S. Development and clinical validation of a multiplex real-time quantitative PCR assay for human infection by Anaplasma phagocytophilum and Ehrlichia chaffeensis. Trop. Med. Infect. Dis. 2018, 3. [Google Scholar] [CrossRef]
- Naimi, W.A.; Green, R.S.; Cockburn, C.L.; Carlyon, J.A. Differential susceptibility of male versus female laboratory mice to Anaplasma phagocytophilum infection. Trop. Med. Infect. Dis. 2018, 3, 78. [Google Scholar] [CrossRef]
- Yelin, I.; Aharony, N.; Shaer-Tamar, E.; Argoetti, A.; Messer, E.; Berenbaum, D.; Shafran, E.; Kuzli, A.; Gandali, N.; Hashimshony, T. Evaluation of COVID-19 RT-qPCR test in multi-sample pools. Clin. Infect. Dis. 2020, in press. [Google Scholar] [CrossRef]
- Bustin, S.; Nolan, T. Talking the talk, but not walking the walk: RT-qPCR as a paradigm for the lack of reproducibility in molecular research. Eur. J. Clin. Investig. 2017, 47, 756–774. [Google Scholar] [CrossRef]
- Legendre, K.P.; Macaluso, K.R. Rickettsia felis: A review of transmission mechanisms of an emerging pathogen. Trop. Med. Infect. Dis. 2017, 2, 64. [Google Scholar] [CrossRef]
- Minahan, N.T.; Chao, C.; Tsai, K. The re-emergence and emergence of vector-borne rickettsioses in Taiwan. Trop. Med. Infect. Dis. 2018, 3, 1. [Google Scholar] [CrossRef]
- Hardstone Yoshimizu, M.; Billeter, S.A. Suspected and confirmed vector-borne rickettsioses of North America associated with human diseases. Trop. Med. Infect. Dis. 2018, 3, 2. [Google Scholar] [CrossRef] [PubMed]
- Bonell, A.; Lubell, Y.; Newton, P.N.; Crump, J.A.; Paris, D.H. Estimating the burden of scrub typhus: A systematic review. PLoS Negl. Trop. Dis. 2017, 11, e0005838. [Google Scholar] [CrossRef] [PubMed]
- Smadel, J.E.; Woodward, T.E.; Ley Jr, H.L.; Philip, C.B.; Traub, R.; Lewthwaite, R.; Savoor, S.R. Chloromycetin in the treatment of scrub typhus. Science 1948, 160–161. [Google Scholar] [CrossRef] [PubMed]
- Sheehy, T.W.; Hazlett, D.; Turk, R.E. Scrub typhus: A comparison of chloramphenicol and tetracycline in its treatment. Arch. Intern. Med. 1973, 132, 77–80. [Google Scholar] [CrossRef]
- Brown, G.W.; Saunders, J.P.; Singh, S.; Huxsoll, D.L.; Shirai, A. Single dose doxycycline therapy for scrub typhus. Trans. R. Soc. Trop. Med. Hyg. 1978, 72, 412–416. [Google Scholar] [CrossRef]
- Raoult, D.; Drancourt, M. Antimicrobial therapy of rickettsial diseases. Antimicrob. Agents Chemother. 1991, 35, 2457. [Google Scholar] [CrossRef]
- Cross, R.; Ling, C.; Day, N.P.J.; McGready, R.; Paris, D.H. Revisiting doxycycline in pregnancy and early childhood-time to rebuild its reputation? Expert Opin. Drug Saf. 2016, 15, 367–382. [Google Scholar] [CrossRef]
- Watt, G.; Chouriyagune, C.; Ruangweerayud, R.; Watcharapichat, P.; Phulsuksombati, D.; Jongsakul, K.; Teja-Isavadharm, P.; Bhodhidatta, D.; Corcoran, K.D.; Dasch, G.A. Scrub typhus infections poorly responsive to antibiotics in northern Thailand. Lancet 1996, 348, 86–89. [Google Scholar] [CrossRef]
- Tanskul, P.; Linthicum, K.J.; Watcharapichat, P.; Phulsuksombati, D.; Mungviriya, S.; Ratanatham, S.; Suwanabun, N.; Sattabongkot, J.; Watt, G. A new ecology for scrub typhus associated with a focus of antibiotic resistance in rice farmers in Thailand. J. Med. Entomol. 1998, 35, 551–555. [Google Scholar] [CrossRef]
- Kelly, D.J. Orientia tsutsugamushi. In Antimicrobial Chemotherapy; Yu, V.L., Merigan, T.C., Barriere, S.L., Eds.; Williams & Wilkins Inc: Baltimore, MD, USA, 1999; pp. 551–554. [Google Scholar]
- Wangrangsimakul, T.; Phuklia, W.; Newton, P.N.; Richards, A.L.; Day, N.P.J. Scrub typhus and the misconception of doxycycline resistance. Clin. Infect. Dis. 2019, ciz972. [Google Scholar] [CrossRef]
- Berge, T.O.; Gauld, R.L.; Kitaoka, M. A field trial of a vaccine prepared from the volner strain of Rickettsia tsutsugamushi. Am. J. Hyg. 1949, 50, 337–342. [Google Scholar] [CrossRef]
- Card, W.I.; Walker, J.M. Scrub-typhus vaccine: Field trial in South-east Asia. Lancet 1947, 252, 481–483. [Google Scholar] [CrossRef]
- Rapmund, G. Rickettsial diseases of the Far East: New perspectives. J. Infect. Dis. 1984, 149, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Chattopadhyay, S.; Jiang, J.; Chan, T.; Manetz, T.S.; Chao, C.; Ching, W.; Richards, A.L. Scrub typhus vaccine candidate kp r56 induces humoral and cellular immune responses in Cynomolgus monkeys. Infect. Immun. 2005, 73, 5039–5047. [Google Scholar] [CrossRef] [PubMed]
- Chattopadhyay, S.; Richards, A.L. Scrub typhus vaccines: Past history and recent developments. Hum. Vaccines 2007, 3, 73–80. [Google Scholar] [CrossRef]
- Roux, V.; Rydkina, E.; Eremeeva, M.; Raoult, D. Citrate synthase gene comparison, a new tool for phylogenetic analysis, and its application for the rickettsiae. Int. J. Syst. Evol. Microbiol. 1997, 47, 252–261. [Google Scholar] [CrossRef]
- Fournier, P.; Roux, V.; Raoult, D. Phylogenetic analysis of spotted fever group rickettsiae by study of the outer surface protein rOmpA. Int. J. Syst. Evol. Microbiol. 1998, 48, 839–849. [Google Scholar] [CrossRef]
- Anderson, B.E.; Tzianabos, T. Comparative sequence analysis of a genus-common rickettsial antigen gene. J. Bacteriol. 1989, 171, 5199–5201. [Google Scholar] [CrossRef]
- Eremeeva, M.E.; Dasch, G.A. Rickettsia. In Molecular Detection of Human Bacterial Pathogens; Liu, D., Ed.; CRC Press-TaylorR & Francis Group: Boca Raton, FL, USA, 2011; pp. 683–700. [Google Scholar]
- Kelly, D.J.; Fuerst, P.A.; Ching, W.; Richards, A.L. Scrub typhus: The geographic distribution of phenotypic and genotypic variants of Orientia tsutsugamushi. Clin. Infect. Dis. 2009, 48, S203–S230. [Google Scholar] [CrossRef]
- Fournier, P.; Raoult, D. Current knowledge on phylogeny and taxonomy of Rickettsia spp. Ann. N. Y. Acad. Sci. 2009, 1166, 1–11. [Google Scholar] [CrossRef]
- Batty, E.M.; Chaemchuen, S.; Blacksell, S.; Richards, A.L.; Paris, D.; Bowden, R.; Chan, C.; Lachumanan, R.; Day, N.; Donnelly, P. Long-read whole genome sequencing and comparative analysis of six strains of the human pathogen Orientia tsutsugamushi. PLoS Negl. Trop. Dis. 2018, 12, e0006566. [Google Scholar] [CrossRef]
- Duong, V.; Blassdell, K.; May, T.T.X.; Sreyrath, L.; Gavotte, L.; Morand, S.; Frutos, R.; Buchy, P. Diversity of Orientia tsutsugamushi clinical isolates in Cambodia reveals active selection and recombination process. Infect. Genet. Evol. 2013, 15, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Fleshman, A.; Mullins, K.; Sahl, J.; Hepp, C.; Nieto, N.; Wiggins, K.; Hornstra, H.; Kelly, D.; Chan, T.; Phetsouvanh, R.; et al. Comparative pan-genomic analyses of Orientia tsutsugamushi reveal an exceptional model of bacterial evolution driving genomic diversity. Microb. Genom. 2018, 4, 000199. [Google Scholar] [CrossRef]
- Nakayama, K.; Kurokawa, K.; Fukuhara, M.; Urakami, H.; Yamamoto, S.; Yamazaki, K.; Ogura, Y.; Ooka, T.; Hayashi, T. Genome comparison and phylogenetic analysis of Orientia tsutsugamushi strains. DNA Res. 2010, 17, 281–291. [Google Scholar] [CrossRef] [PubMed]
- Phetsouvanh, R.; Sonthayanon, P.; Pukrittayakamee, S.; Paris, D.H.; Newton, P.N.; Feil, E.J.; Day, N.P.J. The diversity and geographical structure of Orientia tsutsugamushi strains from scrub typhus patients in Laos. PLoS Negl. Trop. Dis. 2015, 9, e0004024. [Google Scholar] [CrossRef] [PubMed]
- Sonthayanon, P.; Peacock, S.J.; Chierakul, W.; Wuthiekanun, V.; Blacksell, S.D.; Holden, M.T.G.; Bentley, S.D.; Feil, E.J.; Day, N.P.J. High rates of homologous recombination in the mite endosymbiont and opportunistic human pathogen Orientia tsutsugamushi. PLoS Negl. Trop. Dis. 2010, 4, e752. [Google Scholar] [CrossRef] [PubMed]
- Wongprompitak, P.; Duong, V.; Anukool, W.; Sreyrath, L.; Mai, T.T.X.; Gavotte, L.; Moulia, C.; Cornillot, E.; Ekpo, P.; Suputtamongkol, Y. Orientia tsutsugamushi, agent of scrub typhus, displays a single metapopulation with maintenance of ancestral haplotypes throughout continental South East Asia. Infect. Genet. Evol. 2015, 31, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Cho, N.; Kim, H.; Lee, J.; Kim, J.; Cha, S.; Kim, S.; Darby, A.C.; Fuxelius, H.; Yin, J. The Orientia tsutsugamushi genome reveals massive proliferation of conjugative type IV secretion system and host–cell interaction genes. Proc. Natl. Acad. Sci. USA 2007, 104, 7981–7986. [Google Scholar] [CrossRef]
- Rapmund, G.; Dohany, A.L.; Manikumaran, C.; Chan, T.C. Transovarial transmission of Rickettsia tsutsugamushi in Leptotrombidium (leptotrombidium) arenicola traub (acarina: Trombiculidae). J. Med. Entomol. 1972, 9, 71–72. [Google Scholar] [CrossRef]
- Frances, S.P.; Watcharapichat, P.; Phulsuksombati, D.; Tanskul, P. Transmission of Orientia tsutsugamushi, the aetiological agent for scrub typhus, to co-feeding mites. Parasitology 2000, 120, 601–607. [Google Scholar] [CrossRef]
- Frances, S.P.; Watcharapichat, P.; Phulsuksombati, D. Vertical transmission of Orientia tsutsugamushi in two lines of naturally infected Leptotrombidium deliense (acari: Trombiculidae). J. Med. Entomol. 2001, 38, 17–21. [Google Scholar] [CrossRef] [PubMed]
- Frances, S.P. Potential for horizontal transmission of Orientia tsutsugamushi by chigger mites (acari: Trombiculidae). Int. J. Acarol. 2005, 31, 75–82. [Google Scholar] [CrossRef]
- Phasomkusolsil, S.; Tanskul, P.; Ratanatham, S.; Watcharapichat, P.; Phulsuksombati, D.; Frances, S.P.; Lerdthusnee, K.; Linthicum, K.J. Transstadial and transovarial transmission of Orientia tsutsugamushi in Leptotrombidium imphalum and Leptotrombidium chiangraiensis (acari: Trombiculidae). J. Med. Entomol. 2009, 46, 1442–1445. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.; Ha, N.; Min, C.; Kim, H.; Yen, N.T.H.; Lee, K.; Oh, I.; Kang, J.; Choi, M.; Kim, I.; et al. Diversification of Orientia tsutsugamushi genotypes by intragenic recombination and their potential expansion in endemic areas. PLoS Negl. Trop. Dis. 2017, 11, e0005408. [Google Scholar] [CrossRef]
- Allman, E.S.; Kubatko, L.S.; Rhodes, J.A. Split scores: A tool to quantify phylogenetic signal in genome-scale data. Syst. Biol. 2017, 66, 620–636. [Google Scholar] [CrossRef]
- Huang, H.; He, Q.; Kubatko, L.S.; Knowles, L.L. Sources of error inherent in species-tree estimation: Impact of mutational and coalescent effects on accuracy and implications for choosing among different methods. Syst. Biol. 2010, 59, 573–583. [Google Scholar] [CrossRef]
- Tian, Y.; Kubatko, L.S. Gene tree rooting methods give distributions that mimic the coalescent process. Mol. Phylogenet. Evol. 2014, 70, 63–69. [Google Scholar] [CrossRef]
- Long, C.; Kubatko, L. The effect of gene flow on coalescent-based species-tree inference. Syst. Biol. 2018, 67, 770–785. [Google Scholar] [CrossRef]
- McLeod, M.P.; Qin, X.; Karpathy, S.E.; Gioia, J.; Highlander, S.K.; Fox, G.E.; McNeill, T.Z.; Jiang, H.Y.; Muzny, D.; Jacob, L.S.; et al. Complete genome sequence of Rickettsia typhi and comparison with sequences of other rickettsiae. J. Bacteriol. 2004, 186, 5842–5855. [Google Scholar] [CrossRef]
- Seto, J.; Suzuki, Y.; Otani, K.; Qiu, Y.; Nakao, R.; Sugimoto, C.; Abiko, C. Proposed vector candidate: Leptotrombidium palpale for Shimokoshi type Orientia tsutsugamushi. Microbiol. Immunol. 2013, 57, 111–117. [Google Scholar] [CrossRef]
- Azad, A.F. Relationship of vector biology and epidemiology of louse-and flea-borne rickettsioses. In Biology of Rickettsial Diseases. Volume 1; Walker, D., Ed.; CRC Press: Boca Raton, FL, USA, 1988; pp. 51–62. [Google Scholar]
- Azad, A.F.; Beard, C.B. Rickettsial pathogens and their arthropod vectors. Emerg. Infect. Dis. 1998, 4, 179. [Google Scholar] [CrossRef]
- Takhampunya, R.; Tippayachai, B.; Korkusol, A.; Promsathaporn, S.; Leepitakrat, S.; Sinwat, W.; Schuster, A.L.; Richards, A.L. Transovarial transmission of co-existing Orientia tsutsugamushi genotypes in laboratory-reared Leptotrombidium imphalum. Vector Borne Zoonotic Dis. 2016, 16, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Elliott, I.; Pearson, I.; Dahal, P.; Thomas, N.V.; Roberts, T.; Newton, P.N. Scrub typhus ecology: A systematic review of Orientia in vectors and hosts. Parasites Vectors 2019, 12, 513. [Google Scholar] [CrossRef] [PubMed]
- Takhampunya, R.; Korkusol, A.; Promsathaporn, S.; Tippayachai, B.; Leepitakrat, S.; Richards, A.L.; Davidson, S.A. Heterogeneity of Orientia tsutsugamushi genotypes in field-collected trombiculid mites from wild-caught small mammals in Thailand. PLoS Negl. Trop. Dis. 2018, 12, e0006632. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Zhao, Z.; Wang, X.; Li, Z.; Ding, L.; Ding, S.; Yang, L. Mixed scrub typhus genotype, Shandong, China, 2011. Emerg. Infect. Dis. 2014, 20, 484. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.R.; Heo, S.T.; Kang, J.; Park, D.; Kim, J.S.; Bae, J.H.; Woo, J.J.; Kim, S.; Lee, K.H. Mixed infection with severe fever with thrombocytopenia syndrome virus and two genotypes of scrub typhus in a patient, South Korea, 2017. Am. J. Trop. Med. Hyg. 2018, 99, 287–290. [Google Scholar] [CrossRef] [PubMed]
- Le-Viet, N.; Phan, D.; Le-Viet, N.; Trinh, S.; To, M.; Raoult, D.; Parola, P. Dual genotype Orientia tsutsugamushi infection in patient with rash and eschar, Vietnam, 2016. Emerg. Infect. Dis. 2018, 24, 1520. [Google Scholar] [CrossRef]
- Da Pham, X.; Suzuki, H.; Otsuka, Y.; Takaoka, H. Trombiculid fauna and seasonal occurrence of Leptotrombidium scutellare and Leptotrombidium pallidum in endemic and non-endemic areas for tsutsugamushi disease in Oita prefecture, Japan. Med. Entomol. Zool. 1999, 50, 303–312. [Google Scholar] [CrossRef][Green Version]
- Kitazawa, T. Fauna and seasonal fluctuation of larval trombiculid mites in northern Kyushu, Japan. Med. Entomol. Zool. 1993, 44, 327–334. [Google Scholar] [CrossRef]
- Noda, S.; Yamamoto, S.; Uchikawa, K. Seasonal occurrence of larval trombiculid mites and distribution of Leptotrombidium scutellare in residential area and farmland in Kagoshima prefecture. Med. Entomol. Zool. 1996, 47, 339–346. [Google Scholar] [CrossRef]
- Ogawa, M.; Hagiwara, T.; Kishimoto, T.; Shiga, S.; Yoshida, Y.; Furuya, Y.; Kaiho, I.; Ito, T.; Nemoto, H.; Yamamoto, N. Scrub typhus in Japan: Epidemiology and clinical features of cases reported in 1998. Am. J. Trop. Med. Hyg. 2002, 67, 162–165. [Google Scholar] [CrossRef] [PubMed]
- Frances, S.P.; Watcharapichat, P.; Phulsuksombati, D.; Tanskul, P.; Linthicum, K.J. Seasonal occurrence of Leptotrombidium deliense (acari: Trombiculidae) attached to sentinel rodents in an orchard near Bangkok, Thailand. J. Med. Entomol. 1999, 36, 869–874. [Google Scholar] [CrossRef] [PubMed]
- Kitaoka, M.; Asanuma, K.; Otsuji, J. Transmission of Rickettsia orientalis to man by Leptotrombidium akamushi at a scrub typhus endemic area in Akita prefecture, Japan. Am. J. Trop. Med. Hyg. 1974, 23, 993–999. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Kakkar, R.; Kaore, S.N.; Yadav, V.K.; Sharma, R. Geographical distribution, effect of season & life cycle of scrub typhus. JK Sci. 2010, 12, 63. [Google Scholar]
- Wei, Y.; Huang, Y.; Luo, L.; Xiao, X.; Liu, L.; Yang, Z. Rapid increase of scrub typhus: An epidemiology and spatial-temporal cluster analysis in Guangzhou city, southern China, 2006–2012. PLoS ONE 2014, 9, e101976. [Google Scholar] [CrossRef]
- Kumlert, R.; Chaisiri, K.; Anantatat, T.; Stekolnikov, A.A.; Morand, S.; Prasartvit, A.; Makepeace, B.L.; Sungvornyothin, S.; Paris, D.H. Autofluorescence microscopy for paired-matched morphological and molecular identification of individual chigger mites (acari: Trombiculidae), the vectors of scrub typhus. PLoS ONE 2018, 13, e0193163. [Google Scholar] [CrossRef]
- Paris, D.H.; Stephan, F.; Bulder, I.; Wouters, D.; Van der Poll, T.; Newton, P.N.; Day, N.P.; Zeerleder, S. Increased nucleosomes and neutrophil activation link to disease progression in patients with scrub typhus but not murine typhus in laos. PLoS Negl. Trop. Dis. 2015, 9, e0003990. [Google Scholar] [CrossRef]
- Kingston, H.W.; Blacksell, S.D.; Tanganuchitcharnchai, A.; Laongnualpanich, A.; Basnyat, B.; Day, N.P.; Paris, D.H. Comparative accuracy of the InBios scrub typhus detect IgM rapid test for the detection of IgM antibodies by using conventional serology. Clin. Vaccine Immunol. 2015, 22, 1130–1132. [Google Scholar] [CrossRef]
- Paris, D.H.; Chattopadhyay, S.; Jiang, J.; Nawtaisong, P.; Lee, J.S.; Tan, E.; Cruz, E.D.; Burgos, J.; Abalos, R.; Blacksell, S.D. A nonhuman primate scrub typhus model: Protective immune responses induced by pKarp47 DNA vaccination in cynomolgus macaques. J. Immunol. 2015, 194, 1702–1716. [Google Scholar] [CrossRef]


{kind=link}
| Genotype | Cambodia | India | Japan | Korea | Laos | PRC | Taiwan | Thailand | Viet Nam |
|---|---|---|---|---|---|---|---|---|---|
| Karp or Karp related | 11 | 8 | 2 | 4 | 5 | 6 | 40 | 50 | 19 |
| Jp-1 or Jp-2 | 2 | - | 48 | 6 | - | 3 | 6 | 4 | 1 |
| Saitama | - | - | 7 | 8 | - | - | 4 | - | - |
| Kuroki | - | - | 6 | 214 | - | - | 2 | - | - |
| Gilliam | 1 | 1 | - | 1 | - | 4 | 1 | - | - |
| TA763 | 1 | 2 | - | - | - | - | 30 | 19 | 2 |
| Kawasaki | - | - | 7 | 58 | - | 91 | 2 | - | - |
| JG | 8 | 2 | 10 | 7 | 6 | 2 | 4 | 3 | - |
| JG-v | - | 4 | 1 | - | - | - | 27 | 22 | 3 |
| Kato | 4 | - | - | 2 | - | - | 10 | 1 | - |
| Kato-v | 2 | 24 | - | - | - | 1 | 16 | 7 | - |
| Shimokoshi | - | - | 9 | - | - | 1 | - | - | - |
| Divergent | - | - | 8 | - | - | 5 | - | - | - |
| Total | 29 | 41 | 98 | 300 | 11 | 113 | 142 | 106 | 25 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paris, D.H.; Kelly, D.J.; Fuerst, P.A.; Day, N.P.J.; Richards, A.L. A Brief History of the Major Rickettsioses in the Asia–Australia–Pacific Region: A Capstone Review for the Special Issue of TMID. Trop. Med. Infect. Dis. 2020, 5, 165. https://doi.org/10.3390/tropicalmed5040165
Paris DH, Kelly DJ, Fuerst PA, Day NPJ, Richards AL. A Brief History of the Major Rickettsioses in the Asia–Australia–Pacific Region: A Capstone Review for the Special Issue of TMID. Tropical Medicine and Infectious Disease. 2020; 5(4):165. https://doi.org/10.3390/tropicalmed5040165
Chicago/Turabian StyleParis, Daniel H., Daryl J. Kelly, Paul A. Fuerst, Nicholas P. J. Day, and Allen L. Richards. 2020. "A Brief History of the Major Rickettsioses in the Asia–Australia–Pacific Region: A Capstone Review for the Special Issue of TMID" Tropical Medicine and Infectious Disease 5, no. 4: 165. https://doi.org/10.3390/tropicalmed5040165
APA StyleParis, D. H., Kelly, D. J., Fuerst, P. A., Day, N. P. J., & Richards, A. L. (2020). A Brief History of the Major Rickettsioses in the Asia–Australia–Pacific Region: A Capstone Review for the Special Issue of TMID. Tropical Medicine and Infectious Disease, 5(4), 165. https://doi.org/10.3390/tropicalmed5040165