Differences in the Prevalence of Non-Communicable Disease between Slum Dwellers and the General Population in a Large Urban Area in Brazil

 ,
, 
 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Site
- (1)
- illegal occupation of the land characterized by construction on the property of others or receipt of land title in the previous 10 years, and
- (2)
- one of the following:
- construction outside of existing municipal patterns, reflected by the presence of narrow and uneven roads, land parcels of inconsistent shape and size, and development not overseen by regulatory agencies, or
- a general scarcity of public services [22].
2.2. Data Collection and Recruitment
2.3. Clinical Definitions
2.4. NCD Survey of Salvador
- 2010 Pau da Lima NCD Survey—Non-random subsample of leptospirosis survey respondents who chose to participate in supplemental NCD survey.
2.5. Statistical Analyses
2.6. Human Participant Protection
3. Results
3.1. Demographic Distribution and Comparison of Surveyed Populations
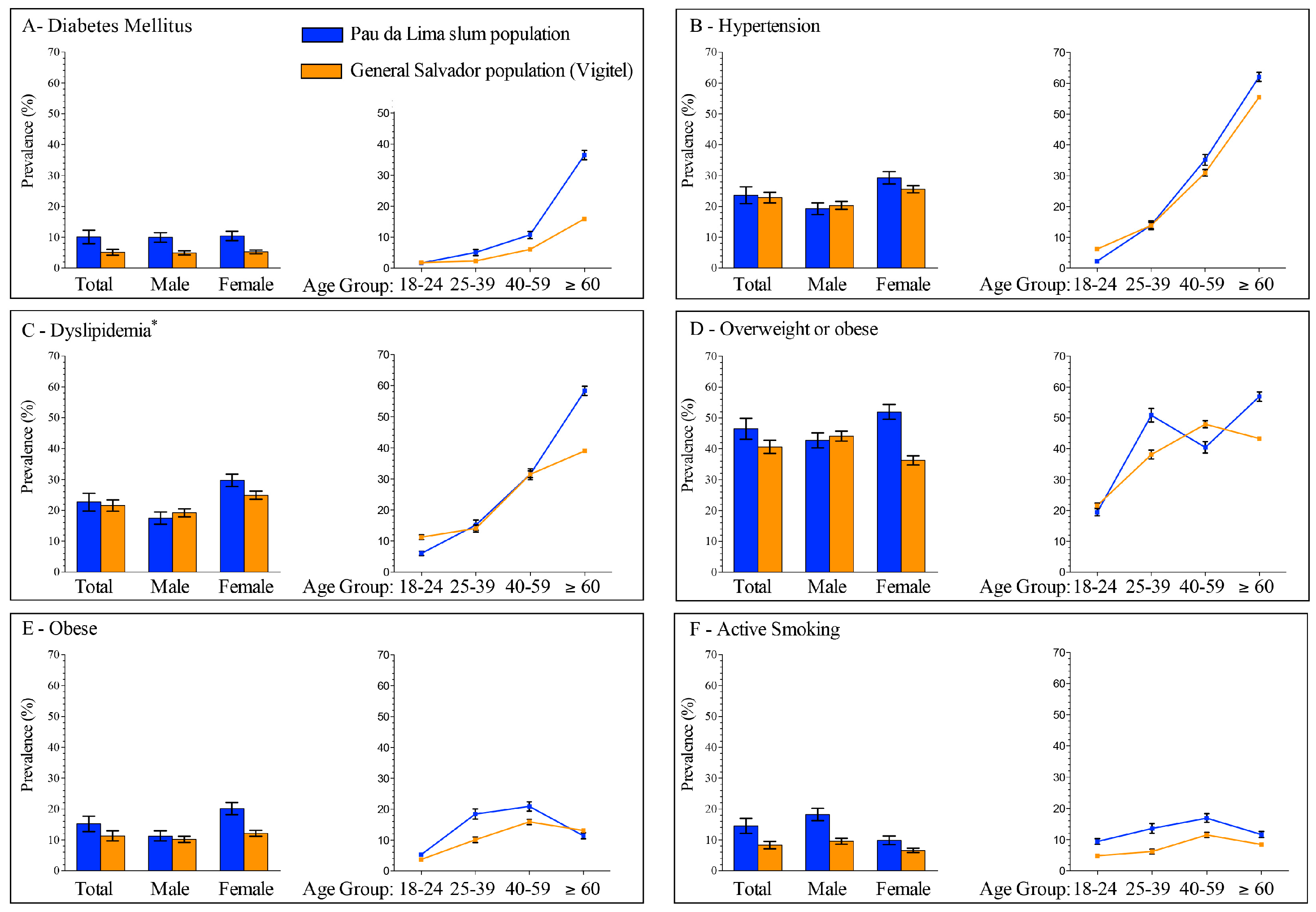
3.2. Prevalence of Non-Communicable Diseases and Risk Factors
3.2.1. Diabetes Mellitus
3.2.2. Hypertension
3.2.3. Dyslipidemia
3.2.4. Overweight and Obese
3.2.5. Smoking
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Murray, C.J.L.; Vos, T.; Lozana, R.; Naghavi, M.; Flaxman, A.D.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2013, 380, 2197–2223. [Google Scholar] [CrossRef]
- Murray, C.J.L.; Barber, R.M.; Foreman, K.J.; Ozgoren, A.A.; Abd-Allah, F.; Abera, S.F.; Aboyans, V.; Abraham, J.P.; Abubakar, I.; Abu-Raddad, L.J.; et al. Global, regional, and national disability-adjusted life years (DALYs) for 306 diseases and injuries and healthy life expectancy (HALE) for 188 countries, 1990–2013: Quantifying the epidemiological transition. Lancet 2015, 386, 2145–2191. [Google Scholar] [CrossRef]
- United Nations Human Settlements Program. State of the World’s Cities 2012/2013; Routledge: London, UK, 2012. [Google Scholar]
- United Nations Human Settlement Program. The Challenge of Slums: Global Report on Human Settlements 2003; Routledge: London, UK, 2003. [Google Scholar]
- Yusuf, S.; Rangarajan, S.; Teo, K.; Islam, S.; Li, W.; Liu, L.; Bo, J.; Lou, Q.; Lu, F.; Liu, T.; et al. Cardiovascular risk and events in 17 low-, middle-, and high-income countries. N. Engl. J. Med. 2014, 371, 818–827. [Google Scholar] [CrossRef] [PubMed]
- Riley, L.W.; Ko, A.I.; Unger, A.; Reis, M.G. Slum health: Diseases of neglected populations. BMC Int. Health Hum. Rights 2007, 7, 2. [Google Scholar] [CrossRef] [PubMed]
- Ayah, R.; Joshi, M.D.; Wanjiru, R.; Njau, E.K.; Otieno, C.F.; Njeru, E.K.; Mutai, K.K. A population-based survey of prevalence of diabetes and correlates in an urban slum community in Nairobi, Kenya. BMC Public Health 2013, 13, 371. [Google Scholar] [CrossRef] [PubMed]
- Daniel, O.J.; Adejumo, O.A.; Adejumo, E.N.; Owolabi, R.S.; Braimoh, R.W. Prevalence of hypertension among urban slum dwellers in Lagos, Nigeria. J. Urban Health 2013, 90, 1016–1025. [Google Scholar] [CrossRef] [PubMed]
- Sitthi-Amorn, C.; Chandraprasert, S.; Bunnag, S.C.; Plengvidhya, C.S. The prevalence and risk factors of hypertension in Klong Toey slum and Klong Toey government apartment houses. Int. J. Epidemiol. 1989, 18, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Van de Vijver, S.J.M.; Oti, S.O.; Agyemang, C.; Gomez, G.B.; Kyobutungi, C. Prevalence, awareness, treatment and control of hypertension among slum dwellers in Nairobi, Kenya. J. Hypertens. 2013, 31, 1018–1024. [Google Scholar] [CrossRef] [PubMed]
- Ettarh, R.; Van de Vijver, S.; Oti, S.; Kyobutungi, C. Overweight, obesity, and perception of body image among slum residents in Nairobi, Kenya, 2008–2009. Prev. Chronic Dis. 2013, 10, 130198. [Google Scholar] [CrossRef] [PubMed]
- Kyobutungi, C.; Ziraba, A.; Ezeh, A.; Yé, Y. The burden of disease profile of residents of Nairobi’s slums: Results from a Demographic Surveillance System. Popul. Health Metr. 2008, 6, 1. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, V.A.; Magalhães, R. Obesidade e pobreza: O aparente paradoxo. Um estudo com mulheres da Favela da Rocinha, Rio de Janeiro, Brasil. Cadernos Saúde Pública 2005, 21, 1792–1800. [Google Scholar] [CrossRef]
- Alves, J.G.; Falcao, R.W.; Pinto, R.A.; Correia, J.B. Obesity patterns among women in a slum area in Brazil. J. Health Popul. Nutr. 2011, 29, 286–289. [Google Scholar] [CrossRef] [PubMed]
- Alves, J.G.B.; Figueiroa, J.N.; Alves, L.V. Prevalence and predictors of physical inactivity in a slum in Brazil. J. Urban Health 2011, 88, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Unger, A.; Felzemburgh, R.D.M.; Snyder, R.E.; Ribeiro, G.S.; Mohr, S.; Costa, V.B.A.; Melendez, A.X.T.O.; Reis, R.B.; Santana, F.S.; Riley, L.W.; et al. Pau da Lima urban health team hypertension in a Brazilian urban slum population. J. Urban Health 2015, 92, 446–459. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, A.; Nikumb, V.B.; Thakur, R.P. Health problems among the elderly: A cross-sectional study. Ann. Med. Health Sci. Res. 2013, 3, 19. [Google Scholar] [CrossRef] [PubMed]
- United Nations Human Settlement Program. State of the World’s Cities 2010/2011; Earthscan: Sterling, VA, USA, 2010. [Google Scholar]
- Schmidt, M.I.; Duncan, B.B.; Menezes, A.M.; Monteiro, C.A.; Barreto, S.M.; Chor, D.; Menezes, P.R. Chronic non-communicable diseases in Brazil: Burden and current challenges. Lancet 2011, 377, 1949–1961. [Google Scholar] [CrossRef]
- World Health Organization. Preventing Chronic Disease: A Vital Investment; World Health Organization: Geneva, Switzerland, 2005. [Google Scholar]
- Moura, E.C.; Pacheco-Santos, L.M.; Peters, L.R.; Serruya, S.J.; Guimarães, R. Research on chronic noncommunicable diseases in Brazil: Meeting the challenges of epidemiologic transition. Rev. Panam. Salud Publica 2012, 31, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Instituto Brasileiro de Geografia e Estatística. Censo Demográfico 2010: Aglomerados Subnormais Primeiros Resultados; IBGE: Rio de Janeiro, Brazil, 2010. [Google Scholar]
- Kikuti, M.; Cunha, G.M.; Paploski, I.A.D.; Kasper, A.M.; Silva, M.M.O.; Tavares, A.S.; Cruz, J.S.; Queiroz, T.L.; Rodrigues, M.S.; Santana, P.M.; et al. Spatial distribution of dengue in a Brazilian urban slum setting: Role of socioeconomic gradient in disease risk. PLoS Negl. Trop. Dis. 2015, 9, e0003937. [Google Scholar] [CrossRef] [PubMed]
- Reis, R.B.; Ribeiro, G.S.; Felzemburgh, R.D.M.; Santana, F.S.; Mohr, S.; Melendez, A.X.T.O.; Queiroz, A.; Santos, A.C.; Ravines, R.R.; Tassinari, W.S.; et al. Impact of environment and social gradient on Leptospira infection in urban slums. PLoS Negl. Trop. Dis. 2008, 2, e228. [Google Scholar] [CrossRef] [PubMed]
- Hagan, J.E.; Moraga, P.; Costa, F.; Capian, N.; Ribeiro, G.S.; Wunder, E.A.; Felzemburgh, R.D.M.; Reis, R.B.; Nery, N.; Santana, F.S.; et al. Spatiotemporal determinants of urban leptospirosis transmission: Four-year prospective cohort study of slum residents in Brazil. PLoS Negl. Trop. Dis. 2016, 10, e0004275. [Google Scholar] [CrossRef] [PubMed]
- Felzemburgh, R.D.M.; Ribeiro, G.S.; Costa, F.; Reis, R.B.; Hagan, J.E.; Melendez, A.X.T.O.; Fraga, D.; Santana, F.S.; Mohr, S.; Santos, dos B.L.; et al. Prospective study of leptospirosis transmission in an urban slum community: Role of poor environment in repeated exposures to the Leptospira agent. PLoS Negl. Trop. Dis. 2014, 8, e2927. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The WHO Global Database on Body Mass Index (BMI). Available online: http://apps.who.int/bmi/index.jsp? (accessed on 3 June 2016).
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2014, 37 (Suppl. 1), S81–S90. [Google Scholar]
- National Heart, Lung, and Blood Institute. Third Report of the Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (ATP III Final Report); NIH Publication: Washington, DC, USA, 2002. [Google Scholar]
- Secretaria de Vigilância em Saúde. Vigitel Brasil 2006: Vigilância de Fatores de Risco e Proteção Para Doenças Crônicas Por Inquérito Telefônico; Ministério da Saúde: Brasília, Brazil, 2007.
- Vigitel-Brasil. In: Vigitel-Brasil. Brasília, DF, Brazil; Ministério da Saúde, Secretaria de Gestão Estratégica e Participativa, Secretaria de Vigilância em Saúde. c2006–2014. Available online: http://portalsaude.saude.gov.br/index.php/o-ministerio/principal/leia-mais-o-ministerio/673-secretaria-svs/vigilancia-de-a-a-z/doencas-cronicas-nao-transmissiveis/l2-doencas-cronicas-nao-transmissiveis/14128-vigitel-2006-a-2013 (accessed on 11 November 2015).
- Secretaria de Vigilância em Saúde. Vigitel Brasil 2010: Vigilância de Fatores de Risco e Proteção Para Doenças Crônicas Por Inquérito Telefônico; Ministério da Saúde: Brasília, Brazil, 2011.
- Secretaria de Vigilância em Saúde. Vigitel Brasil 2013 Vigilância de Fatores de Risco e Proteção Para Doenças Crônicas Por Inquérito Telefônico; Ministério da Saúde: Brasília, Brazil, 2014.
- Keyfitz, N. Sampling variance of standardized mortality rates. Hum. Biol. 1966, 38, 309–317. [Google Scholar] [PubMed]
- Heitzinger, K.; Montano, S.M.; Hawes, S.E.; Alarcón, J.O.; Zunt, J.R. A community-based cluster randomized survey of noncommunicable disease and risk factors in a peri-urban shantytown in Lima, Peru. BMC Int. Health Hum. Rights 2014, 14, 19. [Google Scholar] [CrossRef] [PubMed]
- Joshi, M.; Ayah, R.; Njau, E.; Wanjiru, R.; Kayima, J.; Njeru, E.; Mutai, K. Prevalence of hypertension and associated cardiovascular risk factors in an urban slum in Nairobi, Kenya: A population-based survey. BMC Public Health 2014, 14, 1177. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Noncommunicable Diseases: Country Profiles 2011: Brazil; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Snyder, R.E.; Jaimes, G.; Riley, L.W.; Faerstein, E. A comparison of social and spatial determinants of health between formal and informal settlements in a large metropolitan setting in Brazil. J. Urban Health 2014, 91, 432–445. [Google Scholar] [CrossRef] [PubMed]
- Unger, A.; Riley, L.W. Slum health: From understanding to action. PLoS Med. 2007, 4, 1561–1566. [Google Scholar] [CrossRef] [PubMed]
- Zaluar, A. Crimes and Violence Trends in Rio de Janeiro, Brazil. In Case Study Prepared for Enhancing Urban Safety and Security: Global Report on Human Settlements; Earthscan Publishers: Sterling, VA, USA, 2007. [Google Scholar]
- Kessels, R. Patients’ memory for medical information. J. R. Soc. Med. 2003, 96, 219–222. [Google Scholar] [CrossRef] [PubMed]
- Wilson, P.W.F.; D’Agostino, R.B.; Levy, D.; Belanger, A.M.; Silbershatz, H.; Kannel, W.B. Prediction of coronary heart disease using risk factor categories. Circulation 1998, 97, 1837–1847. [Google Scholar] [CrossRef] [PubMed]
- Lim, L.L.; Seubsman, S.-A.; Sleigh, A. Validity of self-reported weight, height, and body mass index among university students in Thailand: Implications for population studies of obesity in developing countries. Popul. Health Metr. 2009, 7, 1111–1118. [Google Scholar] [CrossRef] [PubMed]
- Thawornchaisit, P.; De Looze, F.; Reid, C.M.; Seubsman, S.-A.; Sleigh, A. Thai Cohort Study Team T. Validity of self-reported hypertension: Findings from the Thai cohort study compared to physician telephone interview. Glob. J. Health Sci. 2013, 6, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Papier, K.; Jordan, S.; D’Este, C.; Bain, C.; Peungson, J.; Banwell, C.; Yiengprugsawan, V.; Seubsman, S.; Sleigh, A. Incidence and risk factors for type 2 diabetes mellitus in transitional Thailand: Results from the Thai cohort study. BMJ Open 2016, 6, e014102–e014108. [Google Scholar] [CrossRef] [PubMed]
- Schneider, F. Size and Measurement of the Informal Economy in 110 Countries; Workshop of Australian National Tax Centre: Canberra, Australian, 2002; Available online: http://www.amnet.co.il/attachments/informal_economy110.pdf (accessed on 29 September 2015).
- Bloom, D.E.; Cafiero, E.T.; Jané-Llopis, E.; Abrahams-Gessel, S.; Bloom, L.; Fathima, S.; Feigl, A.; Gaziano, T.; Hamandi, A.; Mowafi, M.; et al. The Global Economic Burden of Noncommunicable Diseases; World Economic Forum: Geneva, Switzerland, 2011. [Google Scholar]
- UN Millenium Project. Investing in Development: A Practical Plan to Achieve the Millennium Development Goals; Earthscan: New York, NY, USA, 2005. [Google Scholar]
- Huffman, M.D.; Rao, K.D.; Pichon-Riviere, A.; Zhao, D.; Harikrishnan, S.; Ramaiya, K.; Ajay, V.S.; Goenka, S.; Calcagno, J.I.; Caporale, J.E.; et al. A cross-sectional study of the microeconomic impact of cardiovascular disease hospitalization in four low- and middle-income countries. PLoS ONE 2011, 6, e20821. [Google Scholar] [CrossRef] [PubMed]
- Engelgau, M.; Rosenhouse, S.; El-Saharty, S.; Mahal, A. The economic effect of noncommunicable diseases on households and nations: A review of existing evidence. J. Health Commun. 2011, 16 (Suppl. 2), 75–81. [Google Scholar] [CrossRef] [PubMed]
- Krieger, N. Epidemiology and the web of causation: Has anyone seen the spider? Soc. Sci. Med. 1994, 39, 887–903. [Google Scholar] [CrossRef]
- World Health Organization. Global Strategy for the Prevention and Control of Noncommunicable Diseases; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]


{kind=link}
| NCD Survey (n: 792) | Pau da Lima Favela Cohort (n: 1539) | p-Value | ||
|---|---|---|---|---|
| Female sex | 511 (64.5%) | 911 (58.1%) | <0.01 | |
| Age group (years) | 18–24 | 128 (16.1%) | 309 (19.7%) | 0.01 |
| 25–39 | 316 (39.9%) | 649 (41.4%) | ||
| 40–59 | 287 (36.2%) | 506 (32.3%) | ||
| ≥60 | 61 (7.7%) | 105 (6.7%) | ||
| Race | Black | 436 (55.4%) | 861 (55.1%) | 0.84 |
| Mixed | 300 (38.2%) | 594 (38.0%) | ||
| Other | 51 (6.5%) | 107 (6.9%) | ||
| Schooling (years) | 0–3 | 156 (19.7%) | 273 (17.4%) | 0.50 |
| 4–7 | 227 (28.6%) | 484 (30.9%) | ||
| 8–13 | 409 (51.6%) | 812 (51.8%) | ||
| Daily per-capita income (2010 US$) | <2.00 | 128 (17.5%) | 338 (23.6%) | <0.01 |
| 2.00–3.99 | 213 (29.1%) | 518 (36.2%) | ||
| 4.00–5.99 | 159 (21.8%) | 311 (21.7%) | ||
| ≥6.00 | 231 (31.6%) | 264 (18.5%) | ||
| Total | Sex | Age | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | 18–24 | 25–39 | 40–59 | ≥60 | |||||||||
| (%) | 95% CI | (%) | 95% CI | (%) | 95% CI | (%) | 95% CI | (%) | 95% CI | (%) | 95% CI | (%) | 95% CI | |
| Diabetes mellitus | 8.8 | 6.8, 10.8 | 9.8 | 6.4, 13.2 | 8.3 | 5.9, 10.7 | 1.6 | 0, 3.5 | 4.8 | 2.4, 7.2 | 10.6 | 7.1, 14.1 | 36.7 | 24.6, 48.7 |
| Hypertension | 23.8 | 20.8, 28.2 | 19.9 | 15.3, 24.6 | 26.0 | 22.3, 29.8 | 2.3 | 0.0, 4.7 | 14.2 | 10.3, 18.2 | 35.9 | 30.2, 41.6 | 62.3 | 49.8, 74.8 |
| Dyslipidemia | 23.4 | 20.4, 26.5 | 17.2 | 12.8, 21.6 | 26.8 | 22.9, 30.7 | 6.3 | 2.2, 10.5 | 14.7 | 10.7, 18.7 | 33.1 | 27.8, 38.4 | 59.0 | 46.8, 71.3 |
| Overweight or obese 1 | 49.0 | 45.5, 52.5 | 43.4 | 37.6, 49.2 | 52.1 | 47.8, 56.5 | 23.5 | 13.8, 33.2 | 51.0 | 44.0, 58.1 | 60.1 | 54.0, 67.6 | 48.7 | 33.1, 64.4 |
| Obese 2 | 17.3 | 14.8, 19.9 | 10.7 | 7.2, 14.2 | 21.0 | 47.8, 56.5 | 5.9 | 0.3, 11.4 | 13.4 | 8.7, 18.1 | 12.4 | 7.7, 17.1 | 12.8 | 2.4, 23.2 |
| Active smoker | 13.4 | 11.1, 15.7 | 18.1 | 13.7, 22.6 | 10.8 | 8.2, 13.5 | 8.6 | 3.8, 13.4 | 12.7 | 8.9, 16.4 | 16.7 | 12.3–21.1 | 11.5 | 3.3–19.6 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Snyder, R.E.; Rajan, J.V.; Costa, F.; Lima, H.C.A.V.; Calcagno, J.I.; Couto, R.D.; Riley, L.W.; Reis, M.G.; Ko, A.I.; Ribeiro, G.S. Differences in the Prevalence of Non-Communicable Disease between Slum Dwellers and the General Population in a Large Urban Area in Brazil. Trop. Med. Infect. Dis. 2017, 2, 47. https://doi.org/10.3390/tropicalmed2030047
Snyder RE, Rajan JV, Costa F, Lima HCAV, Calcagno JI, Couto RD, Riley LW, Reis MG, Ko AI, Ribeiro GS. Differences in the Prevalence of Non-Communicable Disease between Slum Dwellers and the General Population in a Large Urban Area in Brazil. Tropical Medicine and Infectious Disease. 2017; 2(3):47. https://doi.org/10.3390/tropicalmed2030047
Chicago/Turabian StyleSnyder, Robert E., Jayant V. Rajan, Federico Costa, Helena C. A. V. Lima, Juan I. Calcagno, Ricardo D. Couto, Lee W. Riley, Mitermayer G. Reis, Albert I. Ko, and Guilherme S. Ribeiro. 2017. "Differences in the Prevalence of Non-Communicable Disease between Slum Dwellers and the General Population in a Large Urban Area in Brazil" Tropical Medicine and Infectious Disease 2, no. 3: 47. https://doi.org/10.3390/tropicalmed2030047
APA StyleSnyder, R. E., Rajan, J. V., Costa, F., Lima, H. C. A. V., Calcagno, J. I., Couto, R. D., Riley, L. W., Reis, M. G., Ko, A. I., & Ribeiro, G. S. (2017). Differences in the Prevalence of Non-Communicable Disease between Slum Dwellers and the General Population in a Large Urban Area in Brazil. Tropical Medicine and Infectious Disease, 2(3), 47. https://doi.org/10.3390/tropicalmed2030047