
Screening and Diagnosis Access for Neglected and Tropical Parasitic Diseases in Italy: A National Survey
 , ,
, ,  , , ,
, , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Schistosomiasis
3.2. Strongyloidiasis
3.3. Chagas Disease
3.4. Malaria
3.5. Echinococcosis
3.6. Leishmaniasis
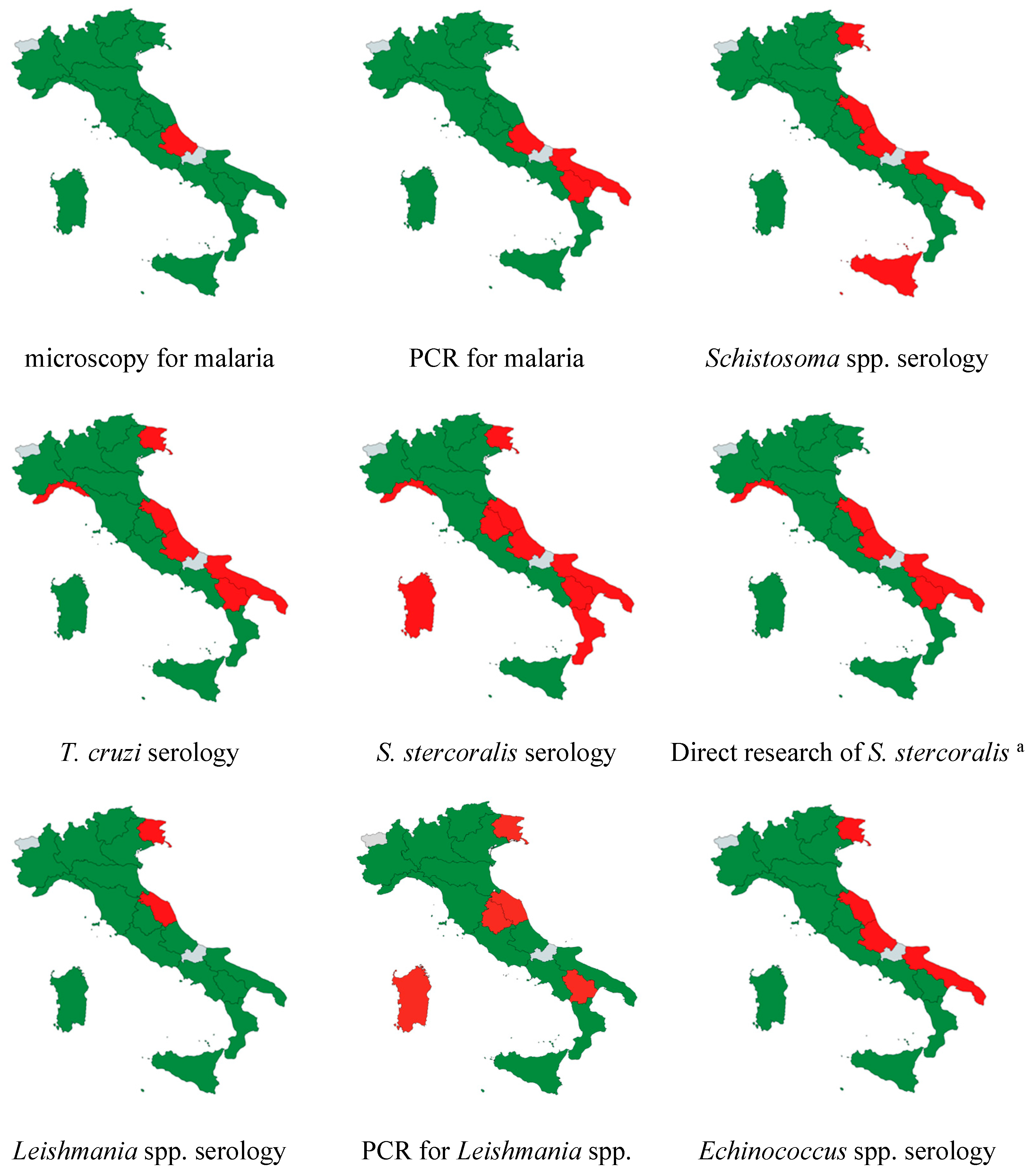
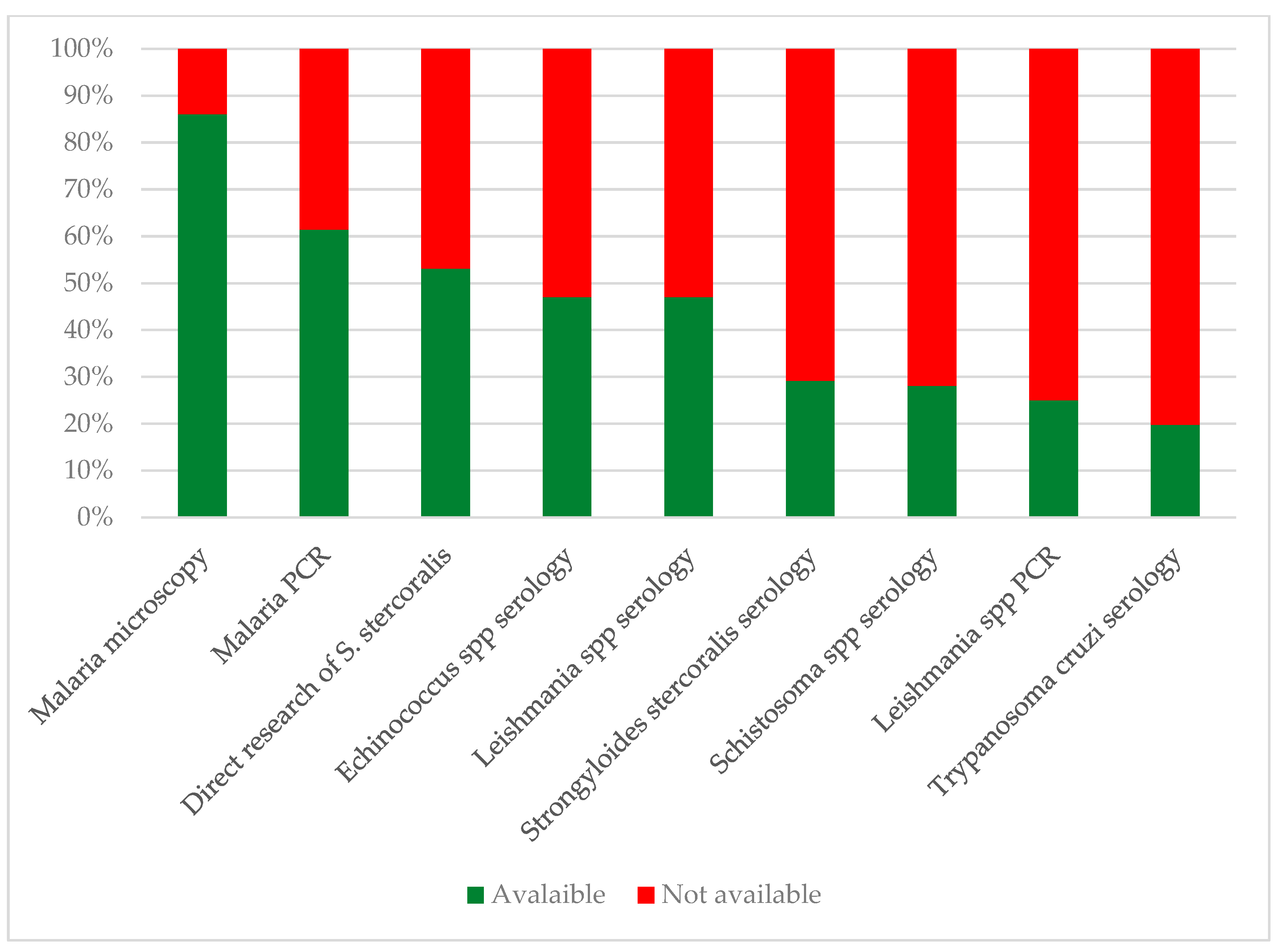
3.7. Geographic Distribution of Tests
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Garcia, L.S. Practical Guide to Diagnostic Parasitology, 3rd ed.; Wiley and sons, Ltd.: Washington, DC, USA, 2021. [Google Scholar]
- ECDC, Public Health Guidance on Screening and Vaccination for Infectious Diseases in Newly Arrived Migrants Within the EU/EEA. 2018. Available online: https://www.ecdc.europa.eu/en/publications-data/public-health-guidance-screening-and-vaccination-infectious-diseases-newly (accessed on 11 December 2024).
- Istituto Nazionale per la Promozione Della Salute Delle Popolazioni Migranti e Per il Contrasto Delle Malattie Della Povertà. I Controlli Alla Frontiera. La Frontiera dei Controlli. Controlli Sanitari All’arrivo e Percorsi di Tutela Per i Migranti Ospiti. Available online: https://www.inmp.it/lg/LG_Migranti-integrata.pdf (accessed on 11 December 2024).
- Zammarchi, L.; Gobbi, F.; Angheben, A.; Spinicci, M.; Buonfrate, D.; Calleri, G.; De Paola, M.; Bevilacqua, N.; Carrara, S.; Attard, L.; et al. Schistosomiasis, strongyloidiasis and Chagas disease: The leading imported neglected tropical diseases in Italy. J. Travel. Med. 2020, 27, taz100. [Google Scholar] [CrossRef]
- Tilli, M.; Botta, A.; Bartoloni, A.; Corti, G.; Zammarchi, L. Hospitalization for Chagas disease, dengue, filariasis, leishmaniasis, schistosomiasis, strongyloidiasis, and Taenia solium taeniasis/cysticercosis, Italy, 2011–2016. Infection 2020, 48, 695–713. [Google Scholar] [CrossRef]
- Gautret, P.; Cramer, J.P.; Field, V.; Caumes, E.; Jensenius, M.; Gkrania-Klotsas, E.; de Vries, P.J.; Grobusch, M.P.; Lopez-Velez, R.; Castelli, F.; et al. Infectious diseases among travellers and migrants in Europe, Eurotravnet 2010. Eurosurveillance 2012, 17, 20205. [Google Scholar] [CrossRef] [PubMed]
- Grobusch, M.P.; Weld, L.; Goorhuis, A.; Hamer, D.H.; Schunk, M.; Jordan, S.; Mockenhaupt, F.P.; Chappuis, F.; Asgeirsson, H.; Caumes, E.; et al. Travel-related infections presenting in Europe: A 20-year analysis of EuroTravNet surveillance data. Lancet Reg. Health—Eur. 2021, 1, 100001. [Google Scholar] [CrossRef]
- Grobusch, M.P.; Mühlberger, N.; Jelinek, T.; Bisoffi, Z.; Corachán, M.; Harms, G.; Matteelli, A.; Fry, G.; Hatz, C.; Gjørup, I.; et al. Imported Schistosomiasis in Europe: Sentinel Surveillance Data from TropNetEurop. J. Travel. Med. 2006, 10, 164–167. [Google Scholar] [CrossRef] [PubMed]
- Tamarozzi, F.; Legnardi, M.; Fittipaldo, A.; Drigo, M.; Cassini, R. Epidemiological distribution of Echinococcus granulosus s.l. infection in human and domestic animal hosts in European Mediterranean and Balkan countries: A systematic review. PLoS Negl. Trop. Dis. 2020, 14, e0008519. [Google Scholar] [CrossRef]
- Casulli, A.; Abela-Ridder, B.; Petrone, D.; Fabiani, M.; Bobić, B.; Carmena, D.; Šoba, B.; Zerem, E.; Gargaté, M.J.; Kuzmanovska, G.; et al. Unveiling the incidences and trends of the neglected zoonosis cystic echinococcosis in Europe: A systematic review from the MEmE project. Lancet Infect. Dis. 2023, 23, e95. [Google Scholar] [CrossRef] [PubMed]
- Tamarozzi, F.; Rossi, P.; Galati, F.; Mariconti, M.; Nicoletti, G.J.; Rinaldi, F.; Casulli, A.; Pozio, E.; Brunetti, E. The Italian registry of cystic echinococcosis (RIEC): The first prospective registry with a European future. Eurosurveillance 2015, 20, 21115. [Google Scholar] [CrossRef]
- Todeschini, R.; Musti, M.A.; Pandolfi, P.; Troncatti, M.; Baldini, M.; Resi, D.; Natalini, S.; Bergamini, F.; Galletti, G.; Santi, A.; et al. Re-emergence of human leishmaniasis in northern Italy, 2004 to 2022: A retrospective analysis. Eurosurveillance 2024, 29, 2300190. [Google Scholar] [CrossRef]
- Berriatua, E.; Jumakanova, Z.; Muñoz, C.; Ortuño, M.; Pérez-Cutillas, P. Surveillance, Prevention and Control of Leishmaniases in the European Union and Its Neighbouring Countries; ECDC: Stockholm Sweden, 2022; Available online: https://www.ecdc.europa.eu/sites/default/files/documents/leishmaniasis-surveillance-eu.pdf (accessed on 11 December 2024).
- George, A.M.; Ansumana, R.; de Souza, D.K.; Niyas, V.K.M.; Zumla, A.; Bockarie, M.J. Climate change and the rising incidence of vector-borne diseases globally. Int. J. Infect. Dis. 2024, 139, 143–145. [Google Scholar] [CrossRef]
- Raele, D.A.; Severini, F.; Toma, L.; Menegon, M.; Boccolini, D.; Tortorella, G.; Di Luca, M.; Cafiero, M.A. Anopheles sacharovi in Italy: First record of the historical malaria vector after over 50 years. Parasit. Vectors 2024, 17, 182. [Google Scholar] [CrossRef] [PubMed]
- CTN Centro Nazionale Trapianti. Valutazione Dell’idoneità del Donatore in Relazione a Patologie Infettive. Revisione 2.0 del 15/02/2024. Available online: https://www.trapianti.salute.gov.it/imgs/C_17_cntPubblicazioni_620_allegato.pdf (accessed on 11 December 2024).
- Requena-Méndez, A.; Chiodini, P.; Bisoffi, Z.; Buonfrate, D.; Gotuzzo, E.; Muñoz, J. The Laboratory Diagnosis and Follow Up of Strongyloidiasis: A Systematic Review. PLoS Negl. Trop. Dis. 2013, 7, e2002. [Google Scholar] [CrossRef]
- Ministero Della Salute Direzione Generale Della Prevenzione Sanitaria. Prevenzione e Controllo Della Malaria in Italia. Available online: https://www.trovanorme.salute.gov.it/norme/renderNormsanPdf?anno=2016&codLeg=57366&parte=1%20&serie=null (accessed on 11 December 2024).
- Gravidanza Fisiologica 2023, xiii, 248 p. Linea Guida 1/2023 SNLG. Available online: https://www.iss.it/documents/20126/9184367/SNLG+1_2023+Gravidanza-fisiologica+Parte-1.pdf/1b3c23be-4578-48f8-277a-88cf0a98de6c?t=1708700731145 (accessed on 11 December 2024).
- Carlier, Y.; Altcheh, J.; Angheben, A.; Freilij, H.; Luquetti, A.O.; Schijman, A.G.; Segovia, M.; Wagner, N.; Vinas, P.A. Congenital Chagas disease: Updated recommendations for prevention, diagnosis, treatment, and follow-up of newborns and siblings, girls, women of childbearing age, and pregnant women. PLoS Negl. Trop. Dis. 2019, 13, e0007694. [Google Scholar] [CrossRef]
- Zammarchi, L.; Vellere, I.; Stella, L.; Bartalesi, F.; Strohmeyer, M.; Bartoloni, A. The diagnosis of neglected tropical diseases (NTDs) in Italy: Reply. Intern. Emerg. Med. 2017, 12, 725–726. [Google Scholar] [CrossRef] [PubMed]
- AMCLI-CoSP, Comitato di Studio per la Parassitologia dell’Associazione Microbiologi Clinici Italiani. Percorso Diagnostico delle Parassitosi Intestinali. 2022. Available online: https://www.amcli.it/wp-content/uploads/2022/03/Percorso-diagnostico-delle-Parassitosi-Intestinali.pdf (accessed on 11 December 2024).
- Martelli, G.; Di Girolamo, C.; Zammarchi, L.; Angheben, A.; Morandi, M.; Tais, S.; Degani, M.; El Hamad, I.; Caligaris, S.; Ciannameo, A.; et al. Seroprevalence of five neglected parasitic diseases among immigrants accessing five infectious and tropical diseases units in Italy: A cross-sectional study. Clin. Microbiol. Infect. 2017, 23, 335.e1–335.e5. [Google Scholar] [CrossRef]
- Tilli, M.; Botta, A.; Mantella, A.; Nuti, B.; Bartoloni, A.; Boccalini, S.; Zammarchi, L. Community-based seroprevalence survey of schistosomiasis and strongyloidiasis by means of Dried Blood Spot testing on Sub-Saharan migrants resettled in Italy. New Microbiol. 2021, 44, 62–65. [Google Scholar] [PubMed]
- Marrone, R.; Mazzi, C.; Ouattara, H.; Cammilli, M.; Pontillo, D.; Perandin, F.; Bisoffi, Z. Screening for Neglected Tropical Diseases and other infections in African refugees and asylum seekers in Rome and Lazio region, Italy. Travel. Med. Infect. Dis. 2023, 56, 102649. [Google Scholar] [CrossRef]
- Buonfrate, D.; Gobbi, F.; Marchese, V.; Postiglione, C.; Badona Monteiro, G.; Giorli, G.; Napoletano, G.; Bisoffi, Z. Extended screening for infectious diseases among newly arrived asylum seekers from Africa and Asia, Verona province, Italy, April 2014 to June 2015. Eurosurveillance 2018, 23, 17-00527. [Google Scholar] [CrossRef]
- Beltrame, A.; Buonfrate, D.; Gobbi, F.; Angheben, A.; Marchese, V.; Monteiro, G.B.; Bisoffi, Z. The hidden epidemic of schistosomiasis in recent African immigrants and asylum seekers to Italy. Eur. J. Epidemiol. 2017, 32, 733–735. [Google Scholar] [CrossRef]
- Buonfrate, D.; Baldissera, M.; Abrescia, F.; Bassetti, M.; Caramaschi, G.; Giobbia, M.; Mascarello, M.; Rodari, P.; Scattolo, N.; Napoletano, G.; et al. Epidemiology of Strongyloides stercoralis in northern Italy: Results of a multicentre case-control study, February 2013 to July 2014. Eurosurveillance 2016, 21, 30310. [Google Scholar] [CrossRef]
- Buonfrate, D.; Marrone, R.; Silva, R.; Mirisola, C.; Ragusa, A.; Mistretta, M.; Perandin, F.; Bisoffi, Z. Prevalence of Strongyloidiasis in a Cohort of Migrants in Italy and Accuracy of a Novel ELISA Assay for S. stercoralis Infection, a Cross-Sectional Study. Microorganisms 2016, 9, 401. [Google Scholar] [CrossRef] [PubMed]
- Di Girolamo, C.; Martelli, G.; Ciannameo, A.; Vocale, C.; Fini, M.; Stefanini, A.; Landini, M.P.; Viale, P.; Verucchi, G. Chagas Disease in a Non-endemic Country: A Multidisciplinary Research, Bologna, Italy. J. Immigr. Minor. Health 2016, 18, 616–623. [Google Scholar] [CrossRef] [PubMed]
- Antinori, S.; Galimberti, L.; Grande, R.; Bianco, R.; Oreni, L.; Traversi, L.; Ricaboni, D.; Bestetti, G.; Lai, A.; Mileto, D.; et al. Chagas disease knocks on our door: A cross-sectional study among Latin American immigrants in Milan, Italy. Clin. Microbiol. Infect. 2018, 24, 1340.e1–1340.e6. [Google Scholar] [CrossRef]
- Pane, S.; Giancola, M.L.; Piselli, P.; Corpolongo, A.; Repetto, E.; Bellagamba, R.; Cimaglia, C.; Carrara, S.; Ghirga, P.; Oliva, A.; et al. Serological evaluation for Chagas disease in migrants from Latin American countries resident in Rome, Italy. BMC Infect. Dis. 2018, 18, 212. [Google Scholar] [CrossRef] [PubMed]
- Mangano, V.D.; Prato, M.; Marvelli, A.; Moscato, G.; Bruschi, F. Screening of at-risk blood donors for Chagas disease in non-endemic countries: Lessons from a 2-year experience in Tuscany, Italy. Transfus. Med. 2021, 31, 63–68. [Google Scholar] [CrossRef]
- Dorrucci, M.; Boccolini, D.; Bella, A.; Lucarelli, C.; D’Amato, S.; Caraglia, A.; Maraglino, F.P.; Severini, C.; Gradoni, L.; Pezzotti, P. Malaria surveillance system and Hospital Discharge Records: Assessing differences in Italy, 2011–2017 database analysis. Travel. Med. Infect. Dis. 2022, 48, 102322. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Malaria Annual Epidemiological Report for 2022; ECDC: Solna, Sweden, 2022. [Google Scholar]
- Naghavi, M. GBD 2021 Italy Subnational Burden of Disease Collaborators. State of health and inequalities among Italian regions from 2000 to 2021: A systematic analysis based on the Global Burden of Disease Study 2021. Lancet Public Health 2025, 10, e309–e320. [Google Scholar] [CrossRef]
- Bradbury, R.S.; Sapp, S.G.H.; Potters, I.; Mathison, B.A.; Frean, J.; Mewara, A.; Sheorey, H.; Tamarozzi, F.; Couturier, M.R.; Chiodini, P.; et al. Where Have All the Diagnostic Morphological Parasitologists Gone? J. Clin. Microbiol. 2022, 60, e0098622. [Google Scholar] [CrossRef]
- Bruschi, F. How parasitology is taught in medical faculties in Europe? Parasitology, lost? Parasitol. Res. 2009, 105, 1759–1762. [Google Scholar] [CrossRef]
- International Organization for Migration (IOM). DTM Italy—Flow Monitoring Surveys with Migrants Arriving to Italy; IOM: Rome, Italy, 2024; Available online: https://dtm.iom.int/sites/g/files/tmzbdl1461/files/reports/DTM_Report_Flow%20Monitoring%20Surveys%20with%20migrants%20arriving%20in%20Italy_2023_1.pdf (accessed on 11 December 2024).
- Decreto del Presidente del Consiglio dei Ministri 12 Gennaio 2017. Definizione e Aggiornamento dei Livelli Essenziali di Assistenza 2017. Available online: https://www.trovanorme.salute.gov.it/norme/dettaglioAtto?id=58669 (accessed on 11 December 2024).
- Decreto del Presidente del Consiglio dei Ministri 2 Novembre 2015. Disposizioni Relative ai Requisiti di Qualita’ e Sicurezza del Sangue e Degli Emocomponenti. Available online: https://www.gazzettaufficiale.it/eli/id/2015/12/28/15A09709/sg (accessed on 11 December 2024).
- Pati, I.; Cruciani, M.; Masiello, F.; Barone, F.; Silvioli, G.; La Raja, M.; Pupella, S.; De Angelis, V. Chagas Disease and Transfusion Risk in Italy: The Results of a National Survey. Pathogens 2022, 1, 1229. [Google Scholar] [CrossRef]
- Calleri, G.; Angheben, A.; Albonico, M. Neglected tropical diseases in Europe: Rare diseases and orphan drugs? Infection 2019, 47, 3–5. [Google Scholar] [CrossRef] [PubMed]
- Comelli, A.; Angheben, A.; Albonico, M.; Calleri, G.; Zammarchi, L.; Napoli, C.; Marrone, R. Schistosomiasis in migrants: Bridging the gap in Italy’s treatment guidelines and access. J. Travel. Med. 2024, 32, taae107. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Schistosomiasis |
|
| Strongyloidiasis |
| Malaria |
|
| Chagas disease |
|
| Leishmaniasis |
|
| Schistosomiasis | In Italy, schistosomiasis is highly prevalent among migrants coming from endemic countries. Zammarchi et al. reported that 1433 out of 4123 NTD cases diagnosed in nine Italian sentinel centres over a seven-year period were due to schistosomiasis [4].Reported seroprevalence ranges from 5.9% to 34% [23,24,25,26,27], with higher prevalence among migrants coming from Mali (63.6% to 72.1%) [25,27] and Ivory Coast (43.1% to 48%) [25,27]. |
| Strongyloidiasis | Strongyloidiasis can affect migrants from a wide geographical area, as well as the elderly from former endemic countries like Italy. Zammarchi et al. reported that 1282 out of 4123 NTD cases diagnosed in nine Italian sentinel centres over a seven-year period were due to strongyloidiasis [4]. Reported seroprevalence ranges from 2.7% to 19.9% [23,26,28,29]. In a study assessing serology among people accidentally presenting with eosinophilia, 8% of Italians (born before 1952) were seropositive [28]. |
| Chagas disease | Zammarchi et al. reported that 581 out of 4123 NTD cases diagnosed in nine Italian sentinel centres over a seven-year period were due to Chagas disease [4].Reported mean seroprevalence ranges from 0.5% among blood donors to 3.9%–9.6% among migrants [23,30,31,32,33]. Seroprevalence among people originating from Bolivia is more than double (23.5% to 30.3%) [30,31,32] |
| Malaria | The last data regarding the number of malaria diagnoses in Italy date back to 2022 [34,35]. Total cases per year ranged from 701 to 888 malaria cases, mainly due to P. falciparum, in the 2013–2017 years report [34]. More than 80% of cases involved non-Italian patients. Most reported cases originated from Northern Italy; however, the comparison between official notifications and hospital discharge records revealed an underreporting from southern and central Italy centres. This highlights the prevalence of imported malaria cases in those regions as well [34]. In line with the reduced volume of international travel during the SARS-CoV-2 pandemic, the cases reported in Italy fell to 181 in 2020 and rapidly increased in the following years with the reopening of movement (571 cases reported in 2022) [35]. |
| Echinococcosis | Since establishing the Italian Registry of Cystic Echinococcosis (RIEC), a more precise estimate of echinococcosis cases has been possible. A first publication in 2015 reported 346 patients enrolled in 11 centres between 2012 and 2014 [11]. A recent systematic review found a total of 15,489 cases of CE between 1997 and 2021 in Italy. As previously mentioned regarding malaria, there is also evident under-notification for CE when compared to HDRs (15,489 cases reported versus 24,651 CE HDRs) [10]. Most cases are diagnosed in patients from southern regions [9,10,11]. A paper detailing the regional distribution from a participating centre in northern Italy revealed that over 70% of native Italian patients were born in southern regions, with the top three being Sicily, Calabria, and Apulia [11] |
| Leishmaniasis | According to the ECDC surveillance system, Italy belongs to European countries with moderate-to-high endemicity for leishmaniases [13]. Overall, 1059 visceral leishmaniasis (VL) cases and 624 cutaneous leishmaniasis (CL) cases were recorded from 2005 to 2020 (autochthonous plus imported cases) [13].When looking at the regional distribution of cases by the HDRs, the highest incidences are from Sicily, Liguria, and Sardinia [13]. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Comelli, A.; Oliva, E.; Bernieri, F.; Zammarchi, L.; Clemente, L.; Petrullo, L.; Calleri, G.; Bruschi, F.; Raglio, A. Screening and Diagnosis Access for Neglected and Tropical Parasitic Diseases in Italy: A National Survey. Trop. Med. Infect. Dis. 2025, 10, 153. https://doi.org/10.3390/tropicalmed10060153
Comelli A, Oliva E, Bernieri F, Zammarchi L, Clemente L, Petrullo L, Calleri G, Bruschi F, Raglio A. Screening and Diagnosis Access for Neglected and Tropical Parasitic Diseases in Italy: A National Survey. Tropical Medicine and Infectious Disease. 2025; 10(6):153. https://doi.org/10.3390/tropicalmed10060153
Chicago/Turabian StyleComelli, Agnese, Ester Oliva, Francesco Bernieri, Lorenzo Zammarchi, Libera Clemente, Luciana Petrullo, Guido Calleri, Fabrizio Bruschi, and Annibale Raglio. 2025. "Screening and Diagnosis Access for Neglected and Tropical Parasitic Diseases in Italy: A National Survey" Tropical Medicine and Infectious Disease 10, no. 6: 153. https://doi.org/10.3390/tropicalmed10060153
APA StyleComelli, A., Oliva, E., Bernieri, F., Zammarchi, L., Clemente, L., Petrullo, L., Calleri, G., Bruschi, F., & Raglio, A. (2025). Screening and Diagnosis Access for Neglected and Tropical Parasitic Diseases in Italy: A National Survey. Tropical Medicine and Infectious Disease, 10(6), 153. https://doi.org/10.3390/tropicalmed10060153