

A Blood and Biochemical Indicator-Based Prognostic Model Predicting Latent Tuberculosis Infection: A Retrospective Study



Abstract
1. Introduction
2. Materials and Methods
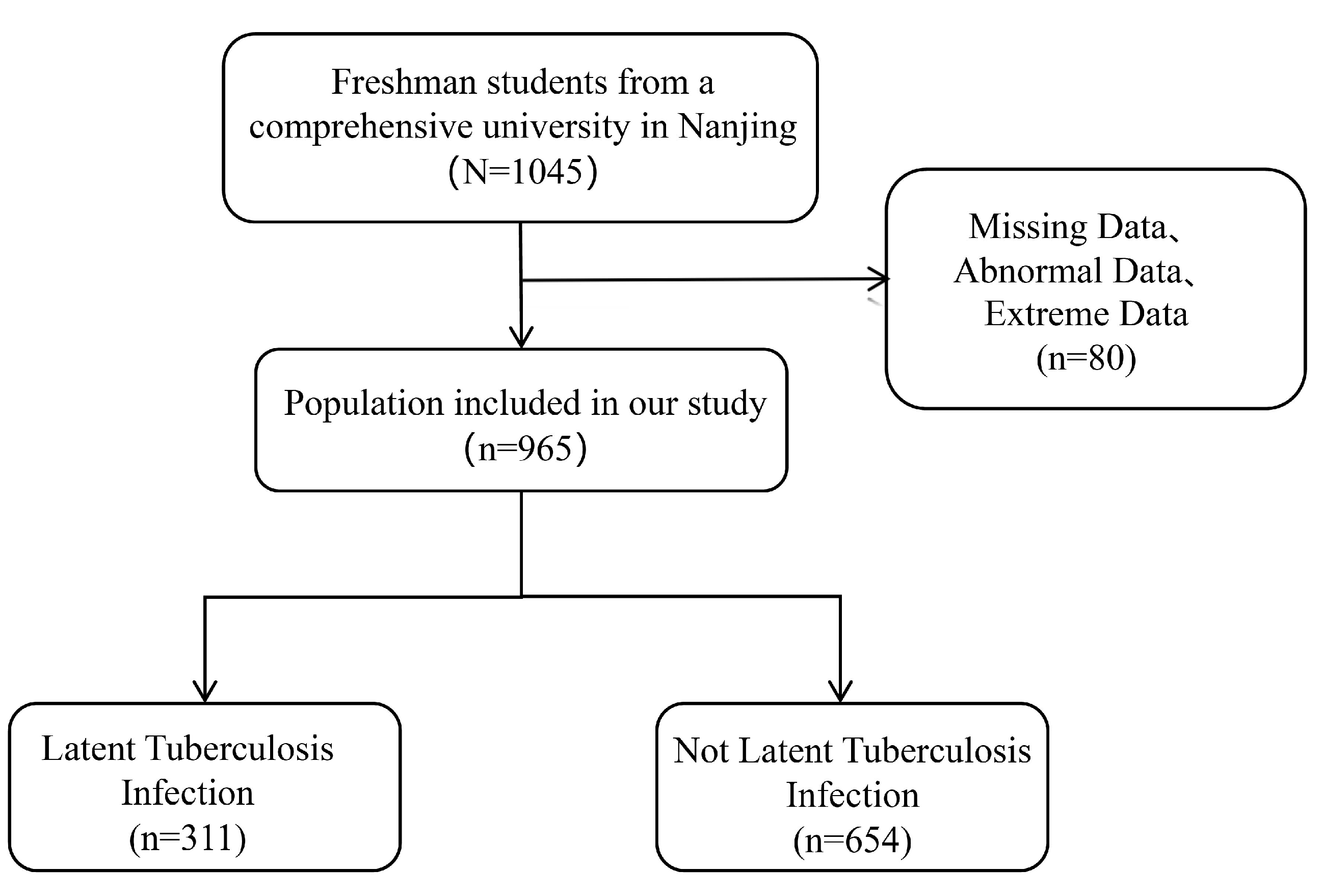
2.1. Study Population and Data Source
2.2. Tuberculin Skin Test (TST)
2.3. Clinical Biochemical Examination
2.4. Statistical Analysis
2.5. Ethics Considerations
3. Results
3.1. Demographic Characteristics of Participants
3.2. Demographic Characteristics and Clinical Information
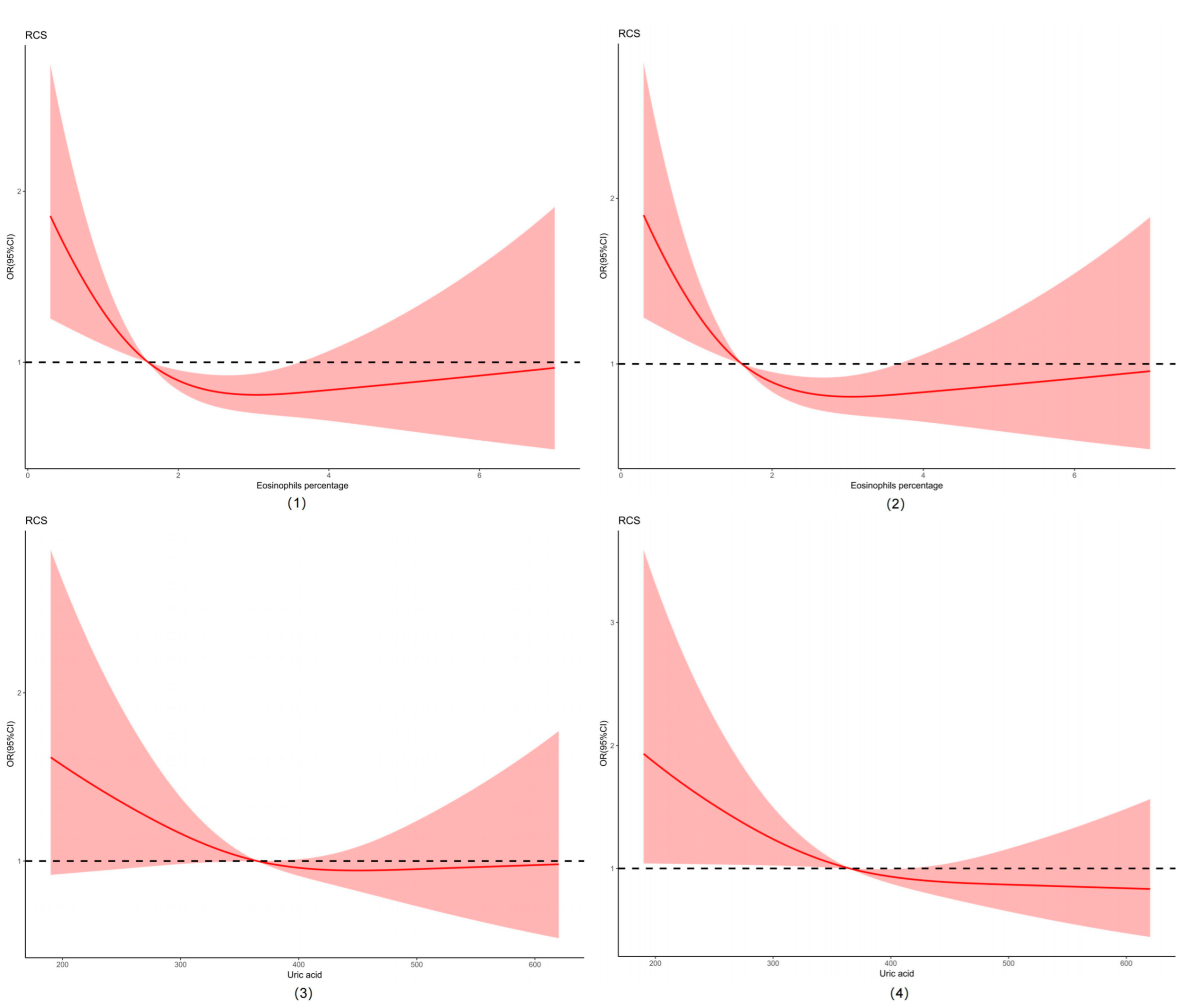
3.3. Factors Related to LTBI
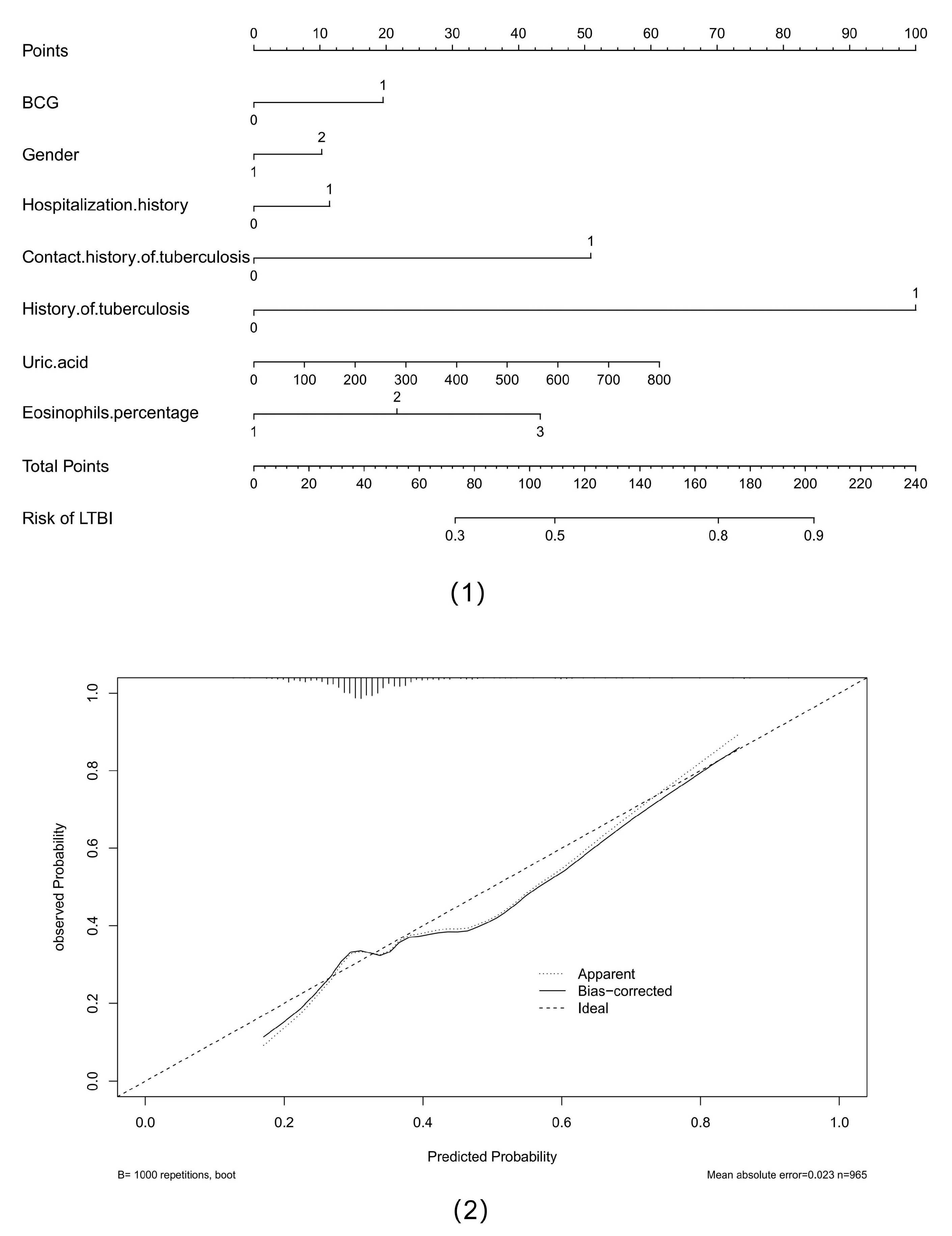
3.4. Prediction of the Risk of LTBI
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report 2024; World Health Organization: Geneva, Switzerland, 2024. [Google Scholar]
- Vasiliu, A.; Martinez, L.; Gupta, R.K.; Hamada, Y.; Ness, T.; Kay, A.; Bonnet, M.; Sester, M.; Kaufmann, S.H.E.; Lange, C.; et al. Tuberculosis prevention: Current strategies and future directions. Clin. Microbiol. Infect. 2023, 30, 1123–1130. [Google Scholar] [CrossRef] [PubMed]
- Houben, R.M.; Dodd, P.J. The Global Burden of Latent Tuberculosis Infection: A Re-estimation Using Mathematical Modelling. PLoS Med. 2016, 13, e1002152. [Google Scholar] [CrossRef] [PubMed]
- Cui, X.; Gao, L.; Cao, B. Management of latent tuberculosis infection in China: Exploring solutions suitable for high-burden countries. Int. J. Infect. Dis. 2020, 92, S37–S40. [Google Scholar] [CrossRef] [PubMed]
- Flynn, J.L.; Chan, J. Tuberculosis: Latency and reactivation. Infect. Immun. 2001, 69, 4195–4201. [Google Scholar] [CrossRef]
- Yang, Q.; Qi, F.; Ye, T.; Li, J.; Xu, G.; He, X.; Deng, G.; Zhang, P.; Liao, M.; Qiao, K.; et al. The interaction of macrophages and CD8 T cells in bronchoalveolar lavage fluid is associated with latent tuberculosis infection. Emerg. Microbes Infect. 2023, 12, 2239940. [Google Scholar] [CrossRef]
- Silver, R.F.; Xia, M.; Storer, C.E.; Jarvela, J.R.; Moyer, M.C.; Blazevic, A.; Stoeckel, D.A.; Rakey, E.K.; Tennant, J.M.; Goll, J.B.; et al. Distinct gene expression signatures comparing latent tuberculosis infection with different routes of Bacillus Calmette-Guerin vaccination. Nat. Commun. 2023, 14, 8507. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhan, B.; Hao, X.; Wang, W.; Zhang, X.; Fang, C.; Wang, M. Factors associated with diagnostic delay of pulmonary tuberculosis among children and adolescents in Quzhou, China: Results from the surveillance data 2011–2021. BMC Infect. Dis. 2023, 23, 541. [Google Scholar] [CrossRef]
- Chen, Q.; Yu, S.; Rui, J.; Guo, Y.; Yang, S.; Abudurusuli, G.; Yang, Z.; Liu, C.; Luo, L.; Wang, M.; et al. Transmissibility of tuberculosis among students and non-students: An occupational-specific mathematical modelling. Infect. Dis. Poverty 2022, 11, 117. [Google Scholar] [CrossRef]
- Jenkins, H.E.; Tolman, A.W.; Yuen, C.M.; Parr, J.B.; Keshavjee, S.; Perez-Velez, C.M.; Pagano, M.; Becerra, M.C.; Cohen, T. Incidence of multidrug-resistant tuberculosis disease in children: Systematic review and global estimates. Lancet 2014, 383, 1572–1579. [Google Scholar] [CrossRef]
- Zhang, M.; Wang, T.; Hou, S.; Ye, J.; Zhou, L.; Zhang, Z.; Deng, Z.; Da, Q.; Li, G.; Li, S. An Outbreak of Multidrug-Resistant Tuberculosis in a Secondary School—Hubei Province, 2019. China CDC Wkly. 2019, 1, 67–69. [Google Scholar] [CrossRef]
- Yuan, Y.; Jin, J.; Bi, X.; Geng, H.; Li, S.; Zhou, C. Factors associated with refusal of preventive therapy after initial willingness to accept treatment among college students with latent tuberculosis infection in Shandong, China. BMC Infect. Dis. 2023, 23, 38. [Google Scholar] [CrossRef]
- Chen, Q.; Wang, X.M.; Qi, Y.; Liu, X.F.; Jiang, L.P.; Hou, W.; Zhou, L.; Lu, X.W. The Impact of Directly Observed Therapy on Preventive Treatment for Latent Tuberculosis Infection among Students in Dalian, China. Biomed. Environ. Sci. 2015, 28, 611–615. [Google Scholar] [PubMed]
- Lonnroth, K.; Migliori, G.B.; Abubakar, I.; D’Ambrosio, L.; de Vries, G.; Diel, R.; Douglas, P.; Falzon, D.; Gaudreau, M.A.; Goletti, D.; et al. Towards tuberculosis elimination: An action framework for low-incidence countries. Eur. Respir. J. 2015, 45, 928–952. [Google Scholar] [CrossRef] [PubMed]
- Getahun, H.; Matteelli, A.; Abubakar, I.; Aziz, M.A.; Baddeley, A.; Barreira, D.; Den Boon, S.; Borroto Gutierrez, S.M.; Bruchfeld, J.; Burhan, E.; et al. Management of latent Mycobacterium tuberculosis infection: WHO guidelines for low tuberculosis burden countries. Eur. Respir. J. 2015, 46, 1563–1576. [Google Scholar] [CrossRef]
- Halliday, A.; Whitworth, H.; Kottoor, S.H.; Niazi, U.; Menzies, S.; Kunst, H.; Bremang, S.; Badhan, A.; Beverley, P.; Kon, O.M.; et al. Stratification of Latent Mycobacterium tuberculosis Infection by Cellular Immune Profiling. J. Infect. Dis. 2017, 215, 1480–1487. [Google Scholar] [CrossRef] [PubMed]
- Sloot, R.; Schim van der Loeff, M.F.; Kouw, P.M.; Borgdorff, M.W. Risk of tuberculosis after recent exposure. A 10-year follow-up study of contacts in Amsterdam. Am. J. Respir. Crit. Care Med. 2014, 190, 1044–1052. [Google Scholar] [CrossRef]
- Drain, P.K.; Bajema, K.L.; Dowdy, D.; Dheda, K.; Naidoo, K.; Schumacher, S.G.; Ma, S.; Meermeier, E.; Lewinsohn, D.M.; Sherman, D.R. Incipient and Subclinical Tuberculosis: A Clinical Review of Early Stages and Progression of Infection. Clin. Microbiol. Rev. 2018, 31, e00021-18. [Google Scholar] [CrossRef]
- LoBue, P.A.; Mermin, J.H. Latent tuberculosis infection: The final frontier of tuberculosis elimination in the USA. Lancet Infect. Dis. 2017, 17, e327–e333. [Google Scholar] [CrossRef]
- Matteelli, A.; Rendon, A.; Tiberi, S.; Al-Abri, S.; Voniatis, C.; Carvalho, A.C.C.; Centis, R.; D’Ambrosio, L.; Visca, D.; Spanevello, A.; et al. Tuberculosis elimination: Where are we now? Eur. Respir. Rev. 2018, 27, 180035. [Google Scholar] [CrossRef]
- Pollock, K.M.; Whitworth, H.S.; Montamat-Sicotte, D.J.; Grass, L.; Cooke, G.S.; Kapembwa, M.S.; Kon, O.M.; Sampson, R.D.; Taylor, G.P.; Lalvani, A. T-cell immunophenotyping distinguishes active from latent tuberculosis. J. Infect. Dis. 2013, 208, 952–968. [Google Scholar] [CrossRef]
- Takenami, I.; Loureiro, C.; Machado, A., Jr.; Emodi, K.; Riley, L.W.; Arruda, S. Blood Cells and Interferon-Gamma Levels Correlation in Latent Tuberculosis Infection. ISRN Pulmonol. 2013, 2013, 256148. [Google Scholar] [CrossRef] [PubMed]
- Potter, N.S.; Harding, C.V. Neutrophils process exogenous bacteria via an alternate class I MHC processing pathway for presentation of peptides to T lymphocytes. J. Immunol. 2001, 167, 2538–2546. [Google Scholar] [CrossRef] [PubMed]
- Svensson, L.; Wenneras, C. Human eosinophils selectively recognize and become activated by bacteria belonging to different taxonomic groups. Microbes Infect. 2005, 7, 720–728. [Google Scholar] [CrossRef]
- Prakash Babu, S.; Narasimhan, P.B.; Babu, S. Eosinophil Polymorphonuclear Leukocytes in TB: What We Know so Far. Front. Immunol. 2019, 10, 2639. [Google Scholar] [CrossRef]
- Bohrer, A.C.; Castro, E.; Tocheny, C.E.; Assmann, M.; Schwarz, B.; Bohrnsen, E.; Makiya, M.A.; Legrand, F.; Hilligan, K.L.; Baker, P.J.; et al. Rapid GPR183-mediated recruitment of eosinophils to the lung after Mycobacterium tuberculosis infection. Cell Rep. 2022, 40, 111144. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Guo, Z.; Wang, W.; Zhang, Q.; Song, S.; Xue, Y.; Zhang, Z.; Wang, J. Prediction of tuberculosis treatment outcomes using biochemical makers with machine learning. BMC Infect. Dis. 2025, 25, 229. [Google Scholar] [CrossRef]
- Sui, X.; Xie, T.; Xu, Y.; Zhang, A.; Zhang, Y.; Gu, F.; Li, L.; Xu, Z.; Chen, J. Protease-Activated Receptor-2 and Phospholipid Metabolism Analysis in Hyperuricemia-Induced Renal Injury. Mediat. Inflamm. 2023, 2023, 5007488. [Google Scholar] [CrossRef]
- Kwan, P.K.W.; Periaswamy, B.; De Sessions, P.F.; Lin, W.; Molton, J.S.; Naftalin, C.M.; Naim, A.N.M.; Hibberd, M.L.; Paton, N.I. A blood RNA transcript signature for TB exposure in household contacts. BMC Infect. Dis. 2020, 20, 403. [Google Scholar] [CrossRef]
- Hu, Y.; Zhao, Q.; Wu, L.; Wang, W.; Yuan, Z.; Xu, B. Prevalence of latent tuberculosis infection and its risk factors in schoolchildren and adolescents in Shanghai, China. Eur. J. Public Health 2013, 23, 1064–1069. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Variables | n | % | |
|---|---|---|---|
| Gender | Male | 467 | 48.39 |
| Female | 498 | 51.61 | |
| Contact history of tuberculosis | Yes | 24 | 2.49 |
| No | 941 | 97.51 | |
| Hospitalization history | Yes | 143 | 14.82 |
| No | 822 | 85.18 | |
| Ethnicity | Han | 701 | 72.64 |
| Non-Han | 264 | 27.36 | |
| History of tuberculosis | Yes | 7 | 0.73 |
| No | 958 | 99.27 | |
| BCG | Yes | 886 | 91.81 |
| Self-statement: None | 79 | 8.19 | |
| Variables | Minimum Value | Q25 | Median Value | Average Value | Q75 | Maximum Value |
|---|---|---|---|---|---|---|
| Neutrophil percentage | 33.70 | 54.75 | 60.10 | 60.08 | 65.20 | 81.30 |
| Eosinophils percentage | 0.10 | 1.00 | 1.60 | 1.94 | 2.50 | 9.90 |
| Basophils percentage | 0.00 | 0.30 | 0.40 | 0.49 | 0.60 | 6.40 |
| Absolute value of lymphocytes | 0.62 | 1.67 | 2.00 | 2.04 | 2.37 | 4.31 |
| Absolute value of monocytes | 0.02 | 0.32 | 0.39 | 0.41 | 0.48 | 1.21 |
| Lymphocytes percentage | 11.30 | 26.40 | 31.10 | 31.28 | 36.00 | 52.80 |
| Monocytes percentage | 2.40 | 5.15 | 6.00 | 6.17 | 7.00 | 9.99 |
| Uric acid | 31.00 | 309.00 | 365.00 | 374.91 | 432.00 | 788.00 |
| Blood urea nitrogen | 1.36 | 3.55 | 4.25 | 4.36 | 5.05 | 9.39 |
| Alanine aminotransferase | 2.50 | 9.60 | 13.30 | 19.26 | 21.25 | 99.99 |
| Creatinine | 39.00 | 58.00 | 68.00 | 68.99 | 79.00 | 116.00 |
| Variables | Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|---|
| cOR (95% CI) | p-Value | aOR (95% CI) | p-Value | ||
| Age | 0.99 (0.81–1.20) | 0.906 | |||
| Gender | Male | 0.97 (0.74–1.27) | 0.836 | 0.78 (0.55–1.10) | 0.150 |
| Female | reference | reference | |||
| Ethnicity | Han | 1.22 (0.89–1.66) | 0.212 | ||
| Non-Han | reference | ||||
| Neutrophil percentage | 1.01 (0.99–1.03) | 0.376 | |||
| Eosinophils percentage | <0.5% | 2.65 (1.33–5.29) | 0.006 | 2.82 (1.39–5.74) | 0.004 * |
| 0.5–5% | 2.75 (1.08–7.00) | 0.034 | 2.78 (1.07–7.23) | 0.036 * | |
| >5% | reference | reference | |||
| Basophils percentage | 0~1% | 1.32 (0.72–2.42) | 0.371 | ||
| >1% | reference | ||||
| Absolute value of lymphocytes | 0.86 (0.66–1.11) | 0.245 | |||
| Absolute value of monocytes | 0.84 (0.30–2.35) | 0.736 | |||
| Lymphocytes percentage | 0.99 (0.97–1.01) | 0.201 | |||
| Monocytes percentage | 0.98 (0.89–1.08) | 0.654 | |||
| Uric Acid | 1.01 (1.00–1.02) | 0.130 | 1.01 (1.00–1.02) | 0.047 * | |
| Blood Urea Nitrogen | 1.03 (0.92–1.16) | 0.578 | |||
| Alanine aminotransferase | 1.00 (0.99–1.01) | 0.984 | |||
| Creatinine | 1.00 (0.99–1.01) | 0.699 | |||
| BCG | Yes | 1.55 (0.91–2.65) | 0.107 | 1.62 (0.94–2.78) | 0.084 |
| Self-statement: None | reference | reference | |||
| History of tuberculosis | Yes | 12.85 (1.54–107.17) | 0.018 | 10.92(1.24–96.08) | 0.031 * |
| No | reference | reference | |||
| Contact history of tuberculosis | Yes | 3.63 (1.57–8.39) | 0.003 | 3.26 (1.39–7.66) | 0.007 * |
| No | reference | reference | |||
| Hospitalization history | Yes | 1.38 (0.96–2.00) | 0.085 | 1.34 (0.91–1.96) | 0.138 |
| No | reference | reference | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qiu, B.; Xu, Z.; Huang, Y.; Miao, R. A Blood and Biochemical Indicator-Based Prognostic Model Predicting Latent Tuberculosis Infection: A Retrospective Study. Trop. Med. Infect. Dis. 2025, 10, 154. https://doi.org/10.3390/tropicalmed10060154
Qiu B, Xu Z, Huang Y, Miao R. A Blood and Biochemical Indicator-Based Prognostic Model Predicting Latent Tuberculosis Infection: A Retrospective Study. Tropical Medicine and Infectious Disease. 2025; 10(6):154. https://doi.org/10.3390/tropicalmed10060154
Chicago/Turabian StyleQiu, Beibei, Zhengyuan Xu, Yanqiu Huang, and Ruifen Miao. 2025. "A Blood and Biochemical Indicator-Based Prognostic Model Predicting Latent Tuberculosis Infection: A Retrospective Study" Tropical Medicine and Infectious Disease 10, no. 6: 154. https://doi.org/10.3390/tropicalmed10060154
APA StyleQiu, B., Xu, Z., Huang, Y., & Miao, R. (2025). A Blood and Biochemical Indicator-Based Prognostic Model Predicting Latent Tuberculosis Infection: A Retrospective Study. Tropical Medicine and Infectious Disease, 10(6), 154. https://doi.org/10.3390/tropicalmed10060154