Abstract
Multiple sclerosis (MS) is a disease that affects the central nervous system, which consists of the brain and spinal cord. Although this condition cannot be cured, proper treatment of persons with MS (PwMS) can help control and manage the relapses of several symptoms. In this survey article, we focus on the different technologies used for the assessment and rehabilitation of motor impairments for PwMS. We discuss sensor-based and robot-based solutions for monitoring, assessment and rehabilitation. Among MS symptoms, fatigue is one of the most disabling features, since PwMS may need to put significantly more intense effort toward achieving simple everyday tasks. While fatigue is a common symptom across several neurological chronic diseases, it remains poorly understood for various reasons, including subjectivity and variability among individuals. To this end, we also investigate recent methods for fatigue detection and monitoring. The result of this survey will provide both clinicians and researchers with valuable information on assessment and rehabilitation technologies for PwMS, as well as providing insights regarding fatigue and its effect on performance in daily activities for PwMS.
1. Introduction
Multiple Sclerosis (MS) is a disease in which the immune system attacks the neurons of the central nervous system causing inflammation that damages the myelin, the fatty substance that surround the axons [1]. It is incurable and is the most prevalent inflammatory disease affecting nearly 2 million people worldwide and around 400,000 in the United States [2]. There are several different subtypes of MS: Clinically Isolated Syndrome (CIS), Relapsing-Remitting MS (RRMS), Secondary Progressive MS (SPMS) and Primary Progressive MS (PPMS) [3]. CIS is the first clinical presentation of the disease which shows characteristics of inflammatory demyelination in the central nervous system and it must last for at least 24 h to be classified as a sign indicating MS. A person exhibiting CIS may or may not go on to develop MS [4]. RRMS is the most commonly diagnosed subtype and is characterized by exacerbation of the disease in which some aspect of function (e.g., walking) is compromised (a ‘relapse’), followed by a remission of the disease in which the function is regained to near pre-exacerbation levels. After an initial period of RRMS, SPMS typically follows [4]; this is characterized by less recovery after attacks, gradually worsening attacks and shorter periods of remission. PPMS is characterized by steady progression of disability once a person is affected (i.e., without the cycle of relapses and remissions seen in RRMS) [4]. There are no straightforward tests or symptoms to diagnose MS. It usually involves several strategies to make sure that the various symptoms are not due to a different underlying problem. The most commonly used tests for this purpose include Magnetic Resonance Imaging (MRI), Evoked Potentials (EP) and spinal fluid analysis apart from a meticulous medical history and a neurological exam. A widely used standard for the diagnosis of MS is the McDonald Criteria, which has been developed and enhanced over the past decade [5]. There are several options within this criteria including dissemination of lesions (detected using MRI scans) in time and space.
One of the most important symptoms of MS is motor impairment. According to one of the composite scales for quantifying disability in MS, the Multiple Sclerosis Functional Composite (MSFC), several components are recommended for assessment including measurement of leg function/ambulation, arm/hand function and cognitive function [6]. It is clear that the assessment of motor impairments in PwMS is very important in the treatment of this condition. Impairments can manifest as tremors, spasticity, paroxysmal, dystonia, ballism, chorea and paroxysmal kinesigenic dyskinesia among others [7]. These impairments can be explained by muscle dysfunction which is both neural and muscular in origin [8]. The most common movement defects in PwMS are gait and balance abnormalities and upper-limb impairments. These defects deter proper day-to-day functioning of PwMS. Such functional impairments require both specialized assessments and interventions by rehabilitation specialists. Multiple studies have been conducted to assess movement deficits in terms of gait and manual dexterity and several assessments are available. Studies have indicated that PwMS have a higher gait variability and lower walking velocity than people without MS [9,10]. With developments in sensor-based technology and assistive robots, several of these assessments have incorporated sensors and robots to assist clinicians and physical therapists in providing targeted assessments and rehabilitation interventions. Our main objective is to provide both clinicians and researchers with a survey of sensor-based and robot-based assistive technologies for both assessment and rehabilitation approaches for such common motor impairments in PwMS. Hence, for our survey, we include research studies and papers in which assistive technologies have been already proposed and evaluated for assessment and rehabilitation for PwMS. Our search in Google Scholar included terms related to “Multiple Sclerosis AND sensors”, “Multiple Sclerosis AND wearables OR rehabilitation robots AND fatigue analysis OR fatigue monitoring” and “Multiple Sclerosis AND wearables OR rehabilitation robots AND upper limb assessment OR upper limb rehabilitation”. We then refined, enhanced and validated our results by using the following databases: PubMed, Science Direct, ProQuest and Medline.
The main purpose of such a survey is to present the available assistive technologies used in MS, providing researchers and clinicians with the different approaches (sensors, robots) used to augment both assessment and rehabilitation approaches for different types of motor impairments (lower/upper body). Towards this, we provide a description of well-established assessment tests used by clinicians (Section 2) for upper limb motor function assessment, as well as balance and gait assessment. We discuss the need for assistive technologies in the domain of MS assessment (Section 3), providing a description of sensor technologies and robotic devices, used to augment and enhance traditional assessments, as well as assistive technologies and approaches for rehabilitation, training and intervention for PwMS (Section 4). Since fatigue is a commonly reported symptom for PwMS, we discuss existing methods to estimate and assess fatigue, including both traditional methods (e.g., questionnaires, scales), as well as multimodal fatigue detection and analysis approaches and their application to rehabilitation and training for PwMS (Section 5). Finally, we conclude by providing a summary of the paper, as well as a set of discussion points towards improving existing assistive technologies for the assessment, rehabilitation and training for PwMS (Section 6).
2. Tests for Motor Function Assessment in Multiple Sclerosis
Diagnosis for MS has evolved over the years from being only a clinical symptom-based assessment [11,12] to including MRI to the diagnostic criteria [13]. This advancement in the diagnostic criteria has helped in the timely diagnosis of the condition. For long-term well-being, early treatment is highly advised since it has been shown that it can slow down disease progression. The main problem is that due to the multitude of symptoms, most people find it difficult to know when to start treatment [14]. In the following sections, we present some of the commonly used tests for the assessment of motor function, including gait, balance and walking difficulty, as well as upper limb motor function in PwMS.
2.1. Tests for Gait and Balance Assessment
Gait, balance and walking ability are critical in the maintenance of independence and several tests have been developed to assess these abilities in MS. Some of the most commonly used tests are Manual Muscle Tests, Timed Walking Tests, balance and gait analyses, vestibular and sensory/proprioceptive assessments, and safety evaluations [15]. In this section, we elaborate on some of the most explored and researched tests for assessing balance and walking difficulties.
In Manual Muscle Testing, patients are instructed to hold the corresponding limb or appropriate body part to be tested at the end of its available range of motion while the practitioner provides opposing manual resistance. Different methods have been proposed to grade muscle strength like the Oxford Muscle Strength Scale and the Medical Research Council (MRC) Scale [16]. The most commonly used scale is a 6 point numeric grading system where 0 implies complete paralysis and 5 implies full strength [17,18]. While it is not a highly accurate assessment, administering this test at the appropriate time can provide physical therapists with valuable insights regarding the progress of the treatment and can assist in planning proper intervention or modification to the current track of treatment.
Timed walking tests, such as the Timed 10-m, 30-m and Timed Up-and-Go tests are designed and regularly used and recommended by physiotherapists for assessing and rehabilitating walking defects [19]. The timed walking tests help measure the disability and the effectiveness of physiotherapy intervention for PwMS [20]. In these tests, the patients are asked to walk a set distance like 3, 10 or 30 m as quickly and safely as possible. The Timed Up-and-Go test is used to assess balance and physical mobility. In this test, the patients rise from a chair walk a distance of 3 m, turn around, walk back 3 m and sit down again and the time taken for this activity is recorded [21]. Tests with shorter distance like the timed 25-foot walking test and the timed up-and-go test have been identified as important measures to assess leg function and ambulation [22].
Gait is defined as the manner in which a person walks. Gait impairment is a very common defect in PwMS. The degree of gait impairment depends on the severity of the defects in the neurological system. Several factors like muscle power loss, level of spasticity, degree of instability due to impaired coordination and degree of sensory impairment have been identified to induce gait variability in PwMS [23]. Several studies have been conducted to monitor and assess gait deterioration [24,25,26,27]. In a study by Kaufman et al. [28], the Timed 25-foot walk was used to assess gait deterioration and it is reported that an increase of 20% in the walking time between two trials signifies a clinically-relevant deterioration of gait. Several other spatiotemporal parameters like decreased velocity, step length, cadence and asymmetric gait with a difference between right and left stance periods, increased hip and knee flexion, increased overall sagittal range of motion (ROM) in the hip joint and decreased overall ankle sagittal ROM [25,29] have been reported as indicators of gait abnormality in a person with MS.
2.2. Tests for Upper Limb Motor Function Assessment
Upper limb motor function is important for activities of daily living (ADL), such as cooking or writing. Deterioration in hand dexterity, strength and coordination are common in PwMS [30]. In this section, we describe some of the tests commonly used to assess dexterity and upper limb motor function.
The Nine Hole Peg Test (NHPT) is a brief, standardized and quantitative test which measures manual dexterity and is considered as a “gold standard” assessment. It has been widely used for measuring dexterity for PwMS [31,32,33], patients with Parkinson’s disease [34], children [35] and the elderly [36]. NHPT is a timed test in which the patients are asked to transfer pegs from a container to a block with 9 holes as quickly as possible. Figure 1 shows an example NHPT (left). The test is done on both the dominant and non-dominant arms twice consecutively and the time taken to complete the run is recorded. Several studies have been done to check the test’s reliability for healthy and post-stroke subjects and have concluded that NHPT has high inter-rater and test-retest reliability [37,38,39]. One drawback of this test is that NHPT may be sensitive to practice effects. Hence, it is recommended that a few rounds should be administered before a baseline assessment [40,41].
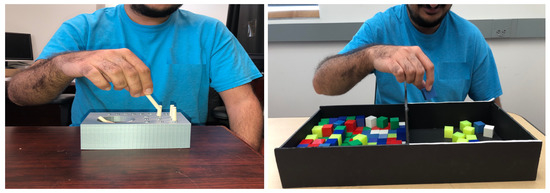
Figure 1.
Subject taking the custom built nine hole peg board test (left). Subject taking the custom built box and blocks test (right).
The Box and Blocks Test assesses manual dexterity in physically challenged individuals [36]. The test usually involves participants moving blocks, from one side of a box to another in 60 s, in a setup as shown in Figure 1 (right side). Several studies have concluded that the test has high inter-rater and test-retest reliability [36,42] and recommend this test for assessment of manual dexterity [40].
The Purdue Pegboard Test is also extensively researched and widely used and measures gross movements of arms and hands as well as finger dexterity [40,43]. This test involves four sub-tests where participants are asked to place small pegs, washers, and collars into holes on a pegboard or perform an assembly task using pins and washers. The participants perform this test using both dominant and non-dominant hand one after the other, using both hands simultaneously or using both hands alternately. The user has to perform the task within 30 s and is evaluated on the number of pegs placed in the holes or the number of pairs assembled [44].
Other tests for manual dexterity include the Crawford Small Parts Dexterity Test, the Functional Dexterity Test, the Grooved Pegboard Test, the Jebsen-Taylor Test of Hand Function, the Minnesota Rate of Manipulation Test, the Moberg Pick-Up test, the O’Connor Finger Dexterity Test, the Sequential Occupational Therapy Dexterity Assessment and the Wolf Motor Function Test. These tests are considered to lack psychometric soundness due to limited research establishing their reliability and validity and must be used cautiously [40].
3. Assistive Technologies for Assessment in Multiple Sclerosis
Loss of motor function is a common problem faced by people suffering from MS, diabetes, the elderly and patients suffering from other neurodegenerative diseases. Traditionally, motor impairment and deterioration have been measured using rating scales like the Ambulation Index, the Functional Systems Score, the Expanded Disability Status Scale (EDSS) and many others and tests in a clinical setup like the Timed 25-foot Walking Test, Timed Up-and-Go Test and the NHPT among others. These tests are usually administered in person by an expert usually a neurologist, whose observations are used as input. These tests often lack precision and might require patient input and/or clinician’s expertise to administer the tests and interpret the results [45]. In recent years, several sensors and assistive robots have been developed to provide an accurate measure of body movement and physical activity early in the disease progression [46]. In this section, we discuss several sensor-based and robot-based assessment technologies used for assessment and treatment of MS. We present the different methods and approaches for multimodal gait analysis, for balance monitoring and for the assessment of upper limb motor function and manual dexterity. We present the different technologies, sensors used and procedures followed for assessment of both the lower and upper limb motor function.
3.1. Multimodal Gait and Balance Monitoring
Difficulty in walking or gait variability is one of the symptoms most commonly reported by PwMS. Gait is defined as the manner in which a person walks and gait variability is defined as stride-to-stride fluctuations in walking [47]. There are several factors that affect the gait of a person which include fatigue, balance, weakness, spasticity and sensory deficit [48]. PwMS have greater variability in their hip, knee and ankle joint angle movement compared to healthy subjects [9]. While objective quantification of disability is routine in clinical trials/clinical visits, traditional methods for gait assessment are semi-subjective, carried out by specialists who observe the quality of a patient’s gait as they walk. Patients may also be surveyed to provide the specialist with a subjective evaluation of their gait. The disadvantage of the subjective nature of the measurements is limited accuracy and precision [46]. In contrast to traditional methods, progress in new technologies has given rise to devices and techniques which allow a quantitative evaluation and analysis of different gait parameters, resulting in more objective measurements and quantitative information related to patients’ gait, potentially reducing error compared to subjective approaches. Several studies have shown the reliability and the ability of these sensor-based setups to effectively measure gait parameters.
In a study by Sun et al. [49], static balance assessment is done by measuring the postural sway by using lightweight inertial sensors and accurately measuring sway metrics like sway area, sway path length, root mean square (RMS) sway amplitude along the anterior-posterior and medial-lateral axis, mean velocity and jerk (an indicator of the smoothness of postural sway). Postural sway refers to the horizontal movement around the center of gravity of the human body. The balance assessment consists of two 30 s quiet standing trials in three different conditions: eyes open on a firm surface, eyes closed on a firm surface, and eyes open on a foam surface. Statistical analysis of sway metrics from BioStamp inertial sensors have shown a strong correlation with MTx sensor data and its capability to distinguish PwMS from healthy subjects. This study considered PwMs with mild MS who had EDSS score between 2 and 4 and severe MS with EDSS score ≥6. Another study by Filli et al. [50] characterized MS-related gait pathology, aimed at defining and detecting specific gait patterns in patients and monitored deterioration of walking function over a period of one year. PwMS recruited for this study had a mean EDSS score of 4.5 ± 1.0. Patients showed a bilateral reduction in step length, associated with diminished ROM in the leg joints. While ROM of the hip was preserved, significant reductions in the extent of the movement were observed at the knee as well as at the ankle joint. The study also showed that more pronounced restriction of ROM at the knee and ankle joint of the weakest leg resulted in substantial left-right asymmetry. These kinematic gait parameters were measured using the Nexus 2.2.3 Motion Capture Software to generate a set of full-body gait profiles based on a comprehensive set of upper and lower extremity and trunk kinematic parameters.
Spain et al. [24] sought to determine if body-worn sensors could detect differences in gait and balance between PwMS who had normal walking speeds and healthy controls. The system consisted of six small, body-worn sensors (Xsens [51]) each housing a 3-dimensional gyroscope and tri-axial accelerometer sensors. In this study, the authors compared different timed mobility tests like Timed 25-Foot Walk, Timed Up-and-Go test and the Quiet Standing test for balance assessment with 31 PwMS, with a median EDSS score of 3 and 28 age and sex matched control subjects while wearing the Xsens sensor. They found that the traditional stopwatch-timed mobility tests with experts were insensitive to mild MS. Whereas, the portable motion analysis system using the Xsens sensor showed significant differences in balance and gait parameters in MS.
Another study conducted by Greene et al. [52] conducted a cross-sectional study with early-stage MS patients to measure the reliability of manual and automatic mobility measures derived from shank-mounted inertial sensors during the Timed Up-and-Go test. In this study, the authors tried to see if a patient’s disease status can be explained with measurements from the inertial sensors and distinguish them with measurements from healthy subjects. The mobility of 38 patients diagnosed with relapsing-remitting MS, with a mean EDSS score of 1.3 and 33 healthy controls was assessed using the Timed Up-and-Go test while the sensors were mounted on both the shanks. A total of 36 (out of 53) mobility parameters obtained during the Timed Up-and-Go showed excellent intra-session reliability, while 9 (out of 53) parameters showed moderate reliability. This compared favorably with the reliability of the mobility parameters in healthy controls, and mobility parameters of early-stage PwMS could be distinguished from healthy subjects with 96.9% accuracy.
Considering mobility impairment in PwMS, a study by Moon et al. [27] proposed a wireless, skin-mounted and conformal inertial sensor to assess mobility under controlled conditions. During the test, PwMS were instrumented with BioStampRC [53] and MTx [51] sensors on their shanks, as well as an activity monitor GT3X [54] on their non-dominant hip. Shank angular velocity was simultaneously measured with the inertial sensors. Step number and temporal gait parameters were calculated from the data recorded by each sensor. The study concluded that the BioStampRC sensor can accurately and precisely measure gait parameters in PwMS across different diverse walking impairment levels and detected differences in gait characteristics specific to disability level. There were three groups of PwMS recruited for this study, PwMS with mild disability had EDSS score between 0 and 2.5, PwMS with moderate disability had EDSS score between 3.5 and 6 and PwMS with severe disability had EDSS score between 5.5 and 6.
Following a computational approach, Gong, Goldman and Lach [26] proposed a Deep Convolutional Neural Network (DCNN) to learn the temporal and spectral associations among the time-series motion data captured by inertial body sensors. A simulated model was developed to train the CNN, and then the trained model assessed gait performance in a pilot dataset with 41 subjects, 28 PwMS who had an EDSS score <4.5 and 13 healthy controls. Five inertial body sensors, equipped with a 3-D gyroscope and a tri-axial accelerometer were used to capture the body motion of walking subjects. The authors reported that their proposed approach outperformed previous efforts to detect differences between healthy controls and PwMS.
While it is not clear which factors influence the prognosis of MS, psycological stress has long been suspected of aggravating progression. Lopez and Picard [55] discuss the opportunities for wearable sensors in the management of stress in PwMS. To accurately gather measurements of autonomic responses in the midst of daily activity, cumbersome electronics such as electrodes placed on the chest have usually been required. In this work, the authors claim that wearable biosensors that can accurately and unobtrusively measure autonomic responses have become available and can be used for stress management. Electrodermal Activity (EDA) biosensors measure electrical conductance changes in the skin, reflecting eccrine sweat-gland activity, while Blood Volume Pulse (BVP) signals obtained from wrist photoplethysmograph (PPG) sensors measure heart and blood circulation changes.
Another study by Muro, Garcia and Mendez [56] presents a review of some sensors being used for human gait recognition and analysis, including Echo5D with the GAITRite CIR-Face (GC) sensor [57], M3D Force Plate [58], XSens MVN [51], Zebris FDM-T System [59], FootScan [60], MatScan [61], Kistler Force Plate [62] and Or6-7 Platform [63]. Dobkin and Dorsch [64] also introduce two other sensors, the DynaPort Minimod [65] and IDDEA Lifegate sensor [66] to analyze different activities for gait analysis, including walking, sitting and standing. The GAITRite CIRFace (GC) sensor was also configured as a straight path for electronic gait analysis by Bethoux et al. [67].
Based on the studies presented above, it is evident that an inertial sensor-based setup is most commonly used in several studies [24,26,27,49,50,52] and measurements from these sensors have also been proven to be reliable to categorize patients to a specific disease state and differentiate an MS patient from a healthy subject [52]. An inertial sensor like the BioStamp sensor or the Xsens sensor usually consists of a 3-dimensional gyroscope and tri-axial accelerometer sensors. Positions of these sensors usually vary based on the kind of tests performed. For example, for timed walking tests like the Timed Up-and-Go test and the Timed 25-Foot Walk test, sensors can be mounted on each shank [27] while for a balance test like the Quiet Standing task, the sensors could be placed on the posterior trunk at L5 vertebrae [49]. The sensor placement also differed based on the kind of parameters to be measured. It is important to note that there is a need for remote monitoring of patients to accommodate longitudinal monitoring of gait and balance impairments in PwMS [50]. Most of these sensors being wearable and lightweight provides an avenue for development of remote monitoring systems which would help clinicians and health care providers make better treatment and rehabilitation plan. Table 1 summarizes the sensors and wearables that have been used for gait analysis and balance assessment.

Table 1.
Summary of sensor technology used for gait assessment.
3.2. Multimodal Assessment of Upper Limb Motor Function
Several studies indicate that impairment in the upper limb motor function should be considered as an important aspect of MS disease progression and management [68,69]. Dysfunction in the upper limbs includes reduced manual dexterity, tremors, numbness, weakness in the muscles and difficulty in slow movements. Such effects cause difficulty in completing common ADL like eating or dressing. There are tests like the NHPT and Hand-Grip Strength Test (HGS) that are used to assess upper limb mobility, but these are limited by being relatively insensitive to subtle changes in motor skills. This has led to the development of sensor and robotic technologies, towards enabling medical and research specialists to detect and analyze changes in motor skills and abilities. Examples of such sensors include motion capture technologies, haptic interfaces and mechanical environments.
In a study conducted by Corona et al., researchers recruited 20 PwMS with a mean EDSS score of 5.4 ± 1.3 in order to perform a Hand-To-Mouth (HTM) test while recording data for kinematic analysis using the SMART-D system, a motion capture system [68]. The SMART-D system consists of 8 infrared cameras that track movement using retro reflective markers positioned on specific points on the upper arm. The task included sitting in front of a table with a neutral posture and moving the fingertips to the mouth after a verbal signal. The task was self-paced and repeated at least 6 times. It was evaluated using an Arm Profile Score (APS) which was derived as the root mean square difference between the kinematic data of a healthy subject and a PwMS. Their finding was that PwMS showed greater difficulty in reaching their mouth, for both their dominant and non dominant arms. They also established that APS was suitable to discriminate movements between PwMS and healthy subjects.
Another study investigated the effectiveness of an accelerometer-based wrist-worn movement sensor to measure and analyze tremors [70]. All participants were diagnosed with MS and were clinically identified or self-reported to have tremors in one or both upper limbs. The study quantified tremors in the impaired limb on a zero to four scale based on the Fahn-Tolosa-Marin clinical rating scale [71]. Participants carried out several tasks, including several from the Fahn scale, a self-selected daily activity affected by tremor and several from activities from the Action Research Arm Test (ARAT) [72] another established performance test for upper arm function. Activities included maintaining posture against gravity with both arms extended at a 90 degree angle, picking up a wooden cube and placing it on a shelf or pouring water from one container to another. An algorithm was developed to predict the presence of tremors based on the wrist monitor data. Overall, the algorithm was able to predict 98.2% of the tremor cases with high specificity and sensitivity. This categorization was in agreement with the judgment of an experienced therapist present during each session.
Carpinella et al. conducted a study to quantify the assessment of the upper limb during ARAT. Subjects were asked to perform all of the ARAT subtasks [73]. Users were monitored while sitting upright on a chair with no armrests using an inertial sensor attached on their wrist and used the most affected arm to perform each test. PwMS recruited for this study had EDSS score between 2 and 8.5 while the median score was 7. ARAT tests were categorized into 4 groups (grasp, grip, pinch and gross).The Xsens sensor, which consists of an accelerometer, a 3D gyroscope and a 3D magnetometer, was placed on the dorsal side of the wrist. After data collection, data segmentation and analysis were carried out in MATLAB. Clustering analysis of clinical parameters revealed three sub-groups of PwMS with different levels of upper limb impairments: mild, moderate and severe. Instrumental parameters extracted from the sensor revealed slower movements and jerks in PwMS in comparison to the control group. Most of the difficulties PwMS had were during the manipulation phase of the task. Overall, the proposed method was shown to be effective in a clinical setting for identifying differences in PwMS. This approach could also detect the level of tremor in a patient and subtle changes in motor skill conditions that cannot be detected using typical medical test scores.
In subsequent work Carpinella et al. focused on improving the analysis of inertial sensor data by implementing the Hilbert-Huang transform (HHT) [74]. They quantified the Finger-to-Nose Test (FNT) by attaching a single Xsens inertial measurement unit to the hand of each patient’s most affected arm. The participants were asked to lift their arm, maintaining a 90 degree angle in shoulder abduction, while keeping the other arm in a neutral position. When asked, the participants would touch the index finger of the arm in abduction to their nose. This movement was divided into two parts the acceleration and the deceleration phase. The FNT test was performed at a self-paced rate and was repeated five times, after which the HHT method was used to classify the collected data. The HHT consists of an Empirical Mode Decomposition (EMD) to extract the oscillatory modes of a signal by breaking down the signal into finite sets of waveforms, and a Hilbert transform to compute their instantaneous frequencies. The resulting signal was then classified into voluntary movement, noise or tremors, based on its frequency. The raw signal was also processed using a Butterworth Bandpass Filter to extract tremors. Once tremors were identified, a tremor index was calculated as the shown in Equation (1). Here, TI indicates the tremor index, k indicates the dimension of the signal, i represents the acceleration or deceleration phase, TR is the extracted tremors and A indicates the normalized angular velocity. The study demonstrated the use of HHT method to identify the tremors and to distinguish them from noise. PwMS recruited for this study had EDSS score < 9 while the mean EDSS score was 6.2. One of the most important observations of this study was that the tremor index in PwMS was greater during the deceleration phase compared to the acceleration phase, while moving towards the nose in any directions. They also found that the tremor index for the deceleration phase correlated significantly with the Fahn-Toloso-Marin tremor rating scale.
Haptic interfaces have also been used to detect and assess upper limb impairments. A study conducted by Bardorfer et al. used a haptic interface called PHANTOM [75], implemented on a 3 degree of freedom (DOF) robot. This device has a pen-like end effector which the subjects hold and is used as a positional device and delivers a force feedback to the user. During testing, the subject traverses a randomly generated labyrinth, viewed on a screen, with the help of the robot. Tactile information about the labyrinth is provided as haptic feedback, and the system records and analyzes the user’s movement and traversal using kinematic data. The authors evaluated their interface with 13 subjects with four types of neurological disorders: Parkinson’s disease, MS, muscular dystrophy and Friedreich ataxia. They concluded that this device is appropriate for such an assessment and that the kinematic parameters collected can be analyzed to provide a quantitative assessment of the impairment.
Another study conducted by Pellegrino et al. focused on upper limb impairment in MS subjects while interacting with different mechanical environments [76]. They aimed to define and characterize upper limb behavioral parameters, muscle activity and muscle synergy. They used a robotic device which subjects would hold and move in two dimensions. Subjects were asked to control a cursor and hit targets appearing on a screen by moving the end effector. While the subject performed the task, data were recorded using force sensors and EMG electrodes. From these, multiple parameters were obtained and analyzed, including movement duration, average speed, normalized jerk index, aiming error, endpoint error, linearity error and lateral deviation. In addition, a muscle synergy measure that quantifies the usage of a group of muscles to perform a task was extracted using non-negative matrix factorization. The authors compared performance between control subjects and PwMS with a EDSS score ≤ 7 and found that the number of trajectory corrections was higher for PwMS during the deceleration phase of the task; also the time taken for the MS subjects to complete the task was longer with lower average speed and less smooth trajectories. However, when assistive forces were provided, there were no significant differences in performance between the two groups. Although both groups changed their organization of muscle synergies for different tasks, this change was greater in MS subjects. The study identified behavioral and muscular features sensitive to MS that may be useful in developing a further understanding of upper limb motor impairments and in creating personalized and more effective interventions and rehabilitation plans.
From the studies discussed above, it is evident that among the sensor-based setups, the accelerometer is one of the most commonly used sensors for assessing and monitoring upper limb motor impairments [70,73,74]. An accelerometer is usually attached to the wrist and is used to collect data while the user performs physical tasks and exercises, such as the ARAT or NHPT. Analysis of accelerometer data has proven useful to identify tremors and to distinguish between PwMS and healthy subjects [70,73]. Results and measures from such approaches are highly correlated with clinical measures for identifying tremors, including Fahn’s tremor rating scale. HHT-based analysis [74] has shown better performance than traditional filtering-based method [70] and shows a better correlation to the clinical measures. Although these studies have successfully shown the validity of this sensor, the number of subjects and types of MS considered in these studies were limited. Apart from accelerometer data analysis, vision-based tracking has been also used in similar settings [68]. Such a methodology was shown to be effective in assessing arm kinematics and identifying impairments. Haptic interfaces have also been successful in identifying upper arm impairments [75,76]. These devices analyzed the arm movements while restricting the subject’s movement path. Subtle changes and tremors could be detected using these devices. EMG in tandem with robotic manipulandum has been used to identify behavioral and muscular features in upper arm impairments. Features like muscle synergies extracted from EMG data have been shown to be an important biomarker for assessing impairments and designing rehabilitative treatments [76]. Although haptic and robotic interfaces are shown to be effective in identifying upper arm impairments, they are expensive and they require a clinical setup and technical assistance for setup and monitoring. Table 2 provides a summary of all the technologies discussed in this section.
Table 2.
Summary of technologies used for upper limb motor assessment.
4. Assistive Technologies for Rehabilitation and Intervention
According to The World Health Organization’s 2011 world report on disability, rehabilitation is defined as “a set of measures that assist individuals who experience disability to achieve and maintain optimal physical, sensory, intellectual, psychological and social functioning in interaction with their environment” [77]. MS is a complex condition where the patients present several different symptoms that can be related to motor, cognitive or behavioral systems. It is therefore very important to provide personalized long-term rehabilitation plan. In the following section, we discuss several sensor-based and robot-based technologies used during rehabilitation and interventions for patients with MS. We present different technologies that have been proposed to assist PwMS during rehabilitation and treatment, including robot-assisted training systems for movement rehabilitation (gait rehabilitation, balance improvement, upper limb rehabilitation and robot-assisted training to improve reaching and manipulation skills). We present the different approaches, considering both hardware (sensors, rehabilitation robotics, exoskeletons, etc.), data collection and analysis, highlighting different user studies which evaluate the effectiveness of robot-assisted rehabilitation and training systems.
4.1. Robot-Assisted Gait Training and Rehabilitation
One of the most common robots used for gait rehabilitation is Lokomat [78]. Lokomat is a lower limb exoskeleton robot attached to a harness. A study conducted by Beer et al. evaluated the effect of robot-assisted gait training in 35 PwMS [79]. The subject population was divided into two groups, one of which performed rehabilitation using a robot (19) and the other without (16). PwMS recruited for each group had severe walking disabilities with a EDSS score between 6 and 7.5 while the median EDSS score was 6.5. The subjects in both groups underwent a treatment session of one hour daily for five days per week, over a period of three weeks. Walking velocity, walking distance, stride length and knee-extensor strength were recorded, as well as clinical measures like activities of daily living and Extended Barthel Index were measured. The study’s findings indicated the feasibility of robot-assisted gait training for PwMS, although the authors noted that a larger subject population was required for significant effect.
Another study conducted by Straudi et al. arrived at a similar result [80] using the Lokomat robotic device with 16 subjects. They conducted a study comparing robot-assisted rehabilitation (8) and conventional walking training (8). PwMS recruited for the first group had a mean EDSS score of 5.8 ± 0.8 and 5.7 ± 0.7 for the second group. The effect of the two rehabilitation techniques was analyzed by conducting a Six Minute Walk test, a Timed Up-and-Go test and using Fatigue Severity Scale (FSS). To achieve this, gait kinematic data were collected using the VICON 460 system one week before treatment, one week after treatment and three months after treatment. The authors concluded that robot-assisted gait training is effective in increasing walking competency; in particular, they found a significant difference in gait speed and walking endurance improvement in the subjects who underwent robot-assisted training compared to those experiencing conventional walking training. They also hypothesized that robotic training could help to improve and/or restore hip and pelvis movement.
Lokomat has also been used in conjunction with other technologies like virtual reality (VR). A study conducted by Brütsch et al. combined the assistance of Lokomat with a VR setup to provide motivation [81]. They conducted the study on 18 children, 10 with cerebral palsy, spinal cord injury and MS among other neurological disorders and 8 healthy subjects. They investigated the rehabilitation measures in four conditions: without any assistance, with a therapist’s assistance, with VR and with a combination of VR and therapist. The VR setup was designed as a soccer game. Force feedback from hip and knee joints were collected, as well as self-reports on experience with the system. The authors observed that the motor output among PwMS using VR was similar to when they were motivated by a therapist and concluded that active participation, through encouragement, resulted in a better motor output than a passive condition. A therapist or VR or a combination of both could be used to provide this encouragement.
Another lower limb exoskeleton robot called PK 100, a lightweight and portable exoskeleton robot that covers the leg from thigh to foot, has been designed to assist in rehabilitation of lower limb impairment [82]. The actuators present in the exoskeleton are used to apply forces to the knee in order to assist in walking, providing an active knee orthosis. The robot has a force sensor at the foot to assist in this actuation. The data from this sensor were used to determine whether the patient required extra assistance for sit-to-stand motions or to climb stairs. The device has four modes: automatic, manual, continuous passive and robotic therapy. In automatic mode the actuator provides assistance based on the sensor data, in manual mode the patient has to press a button for the device to provide assistance, in continuous passive mode the robot provides assistance for both flexion and extension movement of the leg and in robotic therapy mode the robot provides assistance if it senses that the patient needs it. Early studies showed improvement in walking speed for people who used this robot.
Robot-assisted gait training has been shown to be an effective technique for gait rehabilitation. Multiple studies highlight the benefits of robot-assisted gait training over conventional walking training [79,80,83]. A study conducted by Husemann et al. showed that post stroke subjects who used a Lokomat for training had an increase in muscle mass [84]. There is some evidence of robot-assisted training improving spatiotemporal parameters of gait, as well as improving overall mobility [79,80]. Studies have also indicated that task-oriented training is more effective in preserving white matter integrity in the brain than passive training [85]. VR can be used to provide task-oriented training while performing the exercise using a robot [81] and can also improve the experience of therapy as it can motivate and encourage the user during rehabilitation [86]. One of the common drawbacks in studies that have looked at Lokomat and its effect on gait rehabilitation has been the limited size of subject samples [79,80,81]. A post-hoc power analysis showed that a sample size of N = 106 is required for significant effect [79]. It must also be noted that VR studies are sensitive to practice effects [81]. Overall, robot-assisted rehabilitation in conjunction with active rehabilitation techniques have shown promising results in gait rehabilitation. Table 3 provides a summary of all the technologies discussed in this section.
Table 3.
Summary of Robot-Assisted Gait Training and Rehabilitation.
4.2. Upper Limb Training and Rehabilitation
According to a cross-sectional study [69], which considered 219 PwMS, to find the concurrent presence of disability, 76% of the population were found to be suffering from manual dexterity issues. Studies have shown the effect of robotic upper limb rehabilitation on PwMS. One such study conducted by Carpinella et al. evaluated the feasibility of an upper limb robotic rehabilitation system for reaching tasks [87]. In this work, the authors proposed using Braccio di Ferro, a planar robotic manipulandum. This robot has an end effector that subjects hold to perform a set of reaching movements. The study team recruited 16 subjects: 7 MS subjects with a mean EDSS score of 5.71 and 9 healthy controls. The subjects controlled a cursor on a screen using the end effector and were asked to hit targets as they appeared on the screen. During the exercise, the system recorded three trajectory parameters: trajectory duration, jerk metric and lateral deviation. The protocol included a NHPT, Tremor Sensitivity test and transfer test, all both before and after the exercise. The transfer test was performed by asking the subjects to track a figure-of-8. This was done to verify if the improvements noted was specific to the task during rehabilitation or can be observed in other movements as well. The authors observed that prior to rehabilitation there were significant differences between the two groups in all three trajectory parameters. Over the course of 8 sessions of treatment, they observed an improvement in the quality of movements, especially during the first three sessions. Through the figure-of-8 tracking test, they showed that the improvement was generalized and not task specific. Overall, their results suggest the viability of a robot-based upper limb rehabilitation and therapy approach.
Carpinella et al. also conducted a study in which they compared two protocols for robot-based rehabilitation [88]. As in their earlier work, they used the Braccio di Ferro robot for a reaching task. A splint in which the subject would suspend their arm was added to the end effector for use in reaching and manipulation tasks. PwMS recruited for this study had EDSS score < 9 with a mean EDSS score of 6.7. For the reaching task, the participants used a cursor and target setup as described above, and for the manipulation task they were asked to manipulate real objects like LEGOs, bottles and jars. Two types of forces were applied by the robot: perturbing forces that acted in the perpendicular direction to the movement and resistive forces that opposed the movement. Kinematic assessments like reaching duration, manipulation duration, jerk index, mean and maximum lateral duration, normalized path length and learning index and also clinical assessments like the NHPT and ARAT were analyzed. The authors found that the proposed robotic therapy approach reduced arm tremor and improved arm kinematics and functional ability. They also found that MS subjects had the ability to adapt to the perturbing forces generated by the robot, which suggests that the PwMS were able to learn an internal model to account for these forces. While prior to the treatment the MS subjects had difficulty counteracting resistive forces, this ability improved when tested post treatment.
Another study by Sampson et al. combined robotic rehabilitation with functional electric stimulation (FES) and VR [89]. FES is a method in which a low level electrical stimulation is applied to a muscle in order to artificially contract it. In this study, stimulation was applied to the anterior deltoid and triceps. The authors proposed using an upper limb exoskeleton to provide passive support during a set of tracking tasks, which were tested in 5 PwMS. The authors analyzed the accuracy of the tracking task, as well as measures from clinical tasks like the ARAT, NHPT, Manual Ability Measure and Fugl-Meyer assessment (FM). The study concluded that a combined system of FES plus a passive robot could improve upper arm movement and control. They also found that none of the participants reported an increase in muscle fatigue.
Upper limb training using a robot in a VR environment was also studied by Feys et al. [90]. They aimed to compare the effect of robot-assisted upper limb training compared to conventional training. To achieve this, they used HapticMaster, a 3 DOF robot with a gimbal at the end within which the subject’s hand is suspended using a brace. A VR system, using I-TRAVEL, was designed to engage subjects with games while performing exercises. Both clinical assessment measures and robot-based task measures were gathered and analyzed. As clinical assessments, Motricity Index (MI), FM, ARAT and Motor Activity Log (MAL) were used. MI gives an indication of limb strength, FM is a performance-based measurement for impairment, ARAT was used here to quantify the subject’s ability to handle different objects and MAL was used to examine the performance of limbs. For task-based parameters, active ROM, movement duration velocity and quality were analyzed. Two groups of MS subjects were recruited, and one, with median EDSS score of 8, was given robot-assisted training while the other, with a median EDSS score of 7.3, received conventional training. The duration of the study was 8 weeks, and data were gathered at the start and the 8th week. No significant changes were found in the clinical measures for either group. However, improvements in the task-based parameters did occur in the robot-assisted training group, specifically in the speed and time of movements and the trajectories for reaching tasks.
Studies have shown that PwMS display a slower and less smooth upper arm trajectories during reaching tasks [87]. These impairments can often manifest as ataxia, tremors, muscle weakness or coordination deficits. Upper limb rehabilitation has been shown to have a positive effect on upper-arm functioning in persons with progressive MS [91]. Robots, like Braccio di Ferro and HapticMaster [87,88,90], have been used to assist users in rehabilitation by providing them the ability to perform multiple exercises with specific mechanical constraints. These robots can provide different kinds of forces to the its end effector, which the subjects would hold, to simulate different mechanical constraints. Apart from these, passive robotic support in tandem with FES has also been studied by Sampson et al. [89]. In that work, a robotic exoskeleton system was used to support the subject’s arm while FES provided assistance during rehabilitation exercises.
In another study, improvement in the quality of reaching movements has been noted following robot-assisted upper arm rehabilitation where the subjects performed the figure-of-8 tracking task, pre and post rehabilitation [87]. One important observation during robotic rehabilitation is that PwMS retained the ability to adapt to disturbing forces [88]. An improvement in the clinical measures pertaining to upper limb movement was observed by Carpinella et al., though not by Feys et al., perhaps because the task chosen by Feys et al. focused mainly on proximal upper limb movements while Carpinella et al. focused on reaching tasks and reaching and manipulation tasks. This indicates a need for selecting appropriate rehabilitation and assessment tasks when designing robotic rehabilitation systems. Studies have shown that task-oriented training is more effective than passive training during rehabilitation to retain the white matter integrity of the brain [85]. As with gait rehabilitation, VR has also been used with upper limb rehabilitation [89,90]. Table 4 provides a summary of all the technologies discussed in this section.
Table 4.
Summary of upper limb training and rehabilitation.
5. Monitoring Fatigue in Persons with Multiple Sclerosis
Fatigue is very a commonly reported symptom by PwMS, and many consider it to be the worst symptom of MS as it may lead to unemployment and disrupt the social functioning of patients [92]. Several studies indicate that fatigue in MS has a major impact by reducing the quality of life of patients but it remains poorly understood, principally because it is subjective and its etiology varies both across individuals and across different stages of disease progression [93,94,95].
5.1. Fatigue Measurement Scales
Several questionnaires have been developed to measure fatigue, and different clinicians and physical therapists may use different questionnaires, in part due to working with different populations. While there is no “gold standard” fatigue measurement standard for PwMS, Braley and Chervin [94] review some of the most commonly used questionnaires for PwMS. They discuss some of the widely used and researched scales, including The Chalder Fatigue Scale (CFS), Fatigue Severity Scale (FSS) and the Modified Fatigue Impact Scale (MFIS). CFS includes 14 questions, each of which is rated with a numeric Likert scale. A total score is calculated and a higher value indicates more severe fatigue. The main advantage of this test is its brevity and ease of use. The authors also state that while this test lacks assessments of validity and consistency, it is considered valuable for clinical studies. FSS is a survey that includes 9 questions, each of which is rated on a 7-point Likert scale that focuses primarily on physical fatigue. MFIS is a survey originally derived from a 40-item survey, the Fatigue Impact Scale. The MFIS survey consists of 21 questions assessing aspects of fatigue on a 0–4 point Likert scale (“never” to “always”). In scoring, answers contribute to three categories: physical fatigue (9 questions), cognitive fatigue (10 questions), and psychological fatigue (2 questions). A total MFIS score is also obtained by summing all responses. The advantages of this scale include ease of use, reproducibility, and a high correlation with the FSS metrics. All three of these scales assess “trait fatigue”, or the fatigue experienced by PwMS over an extended period of time (e.g., over the past month), and not the complementary “state fatigue” component. It is also important to note that some researchers have adopted the use of Visual Analogue Scale (VAS) in their surveys to get a more precise value for statistical analysis. The VAS has been used to measure the severity of pain or fatigue and correlate it to depression in PwMS [96]. This scale provides the users with a scale of 100 mm horizontal line where, one extreme (0 mm) is “not fatigued at all” to another extreme (100 mm) representing “extremely fatigued”. This scale helps to measure the level of fatigue a patient is experiencing at a given point in time. In other words, it helps measure the “state fatigue” component.
5.2. Multimodal Fatigue Detection and Analysis
The scales discussed above provide a subjective measure of fatigue in PwMS, based on self-reports. These kinds of tests are always susceptible to human error, like overestimation or underestimation by the patient, indicating a need for objective measurement and analysis of fatigue [95]. Towards this goal, several studies have attempted to measure fatigue using physiological data. In this section, we discuss some of the sensor-based technologies used by researchers to monitor and assess fatigue levels in patients.
A study by Sehle et al. [95], looked into the detection of motor fatigue using kinematic gait analysis in PwMS. They developed the Fatigue Kliniken Schmieder (FKS) index to classify patients as fatigued or non-fatigued. The study was conducted with 20 healthy subjects and 40 PwMS with a mean EDSS score of 3.4 ± 1.3, all between the ages of 18 and 65 years. Participants were asked to walk on a treadmill for a maximum of 60 minutes or until they were completely exhausted. The treadmill speed was set 10% higher than their preferred speed or a maximum of 5 km/h. Though there was no explicit screening based on disease course or disability level, the MS group was required to walk without aids or assistance as a recruitment criteria. Gait data was recorded for one minute at the beginning and one minute at the end using an AS200 motion analysis device and gait parameters including step length, width and height, bilateral leg circumduction, bilateral knee flexion angle and medio-lateral trunk sway were recorded. Blood samples were taken during the start and the end of the exercise to measure blood lactate levels using a lactate analyzer (Arkray Lactate Pro LT-17810) and lactate strip. Heart rate was measured using a chest mounted Garmin Forerunner heart rate monitor. Based on the FKS value computed, patients with a value of 4 and above were classified as having fatigue and others as non-fatigued. The authors reported that the FKS scale was a more sensitive and reliable measure of motor fatigue than traditional methods where an expert would rate a PwMS. Also, based on the lactate levels they concluded that the motor fatigue in MS is not related to muscle fatigue. It is important to note that the sensors used for assessment involved a complex setup, including a harness to support MS patients as they walked on the treadmill, as a safety measure and blood samples were also drawn. Thus, this type of experiment is difficult to replicate without access to clinical facilities.
In a more recent work by Barrios et al. [97], the use of sensors capable of measuring heart rate through changes in blood volume and electrodermal activity (EDA) were explored using wearable Empatica E4 and Everion devices. The authors attempted to verify whether these devices were able to accurately monitor the functions of the autonomic nervous system by comparing their output to a medical-grade Holter monitor. Their results showed that the tested devices may be capable of monitoring motor fatigue, though they lacked psychometric soundness. However, there is limited research backing of reliability and validity of the methods used.
Several other wearable non-invasive sensors have been explored by researchers for fatigue assessment. An advantage of such sensors is that they can be used for long term data monitoring at home or at work to better assess improvement or deterioration. For instance, Yu et al. [98] developed a wireless Fatigue Monitoring System (FAMOS), to monitor physiological and functional parameters like ECG, EMG, body-skin temperature and motion. This system was capable of recording data during cognitive and functional tests, as well as during activities of daily living. The signals recorded were transferred to a laptop via a wireless router. They tested this system in a sample of 17 fatigued PwMS, who had a EDSS score <5.5 and 9 control subjects to see if they were able to distinguish the groups. Participants wore a temperature sensor on the back near the L5 vertebra of the spine to measure body temperature, motion sensors on the shank, ECG electrodes on the sides of the thorax under the arms and EMG electrodes on the quadriceps and below the eye to measure muscle activity and eye movement respectively. Participants in the study also received several cognitive and functional tests. Based on the data calculated from these tests, the authors were able to distinguish healthy controls from fatigued PwMS. Although the main aim of the study was to build a wireless system, it was limited to indoor setup as the system required WiFi to store data to a cloud-based data store.
Fatigue monitoring related to driving has been a specific area of some interest. A study by Chipchase et al. [99] looked at 75 MS patients and 63 control subjects and found that fatigue along with other factors like leg problems, numbness and eye problems were a significant cause for driving impairment. A study by Nayak et al. [100], found an effective way to score driver fatigue by integrating EEG parameters, heart rate variability and blood biomarkers, but lack psychometric soundness.
In summary, it is clear from these studies that fatigue is a very important aspect of MS, and that it needs more research to build assessment and monitoring systems. Although several wireless sensor-based setups were developed [95,97,98], it is still the general consensus that subjective measures generally give a more accurate measure of fatigue a person experiences, regardless of the drawbacks. Several researchers propose a task based framework to monitor fatigue while performing a physical or cognitive task [101]. Care must be taken to decide what parameters are required for monitoring fatigue and what kind of sensors are to be used.
5.3. Measuring and Analyzing Fatigue in Rehabilitation
Developing rehabilitation strategies to treat MS-related symptoms is critical in helping PwMS achieve a better quality of life. Although several pharmacological treatments are available to control MS symptoms, assessments and rehabilitation using physical therapies have proven to help improve the quality of life [102]. Fatigue is an important factor to consider during rehabilitation and in designing rehabilitation plans [103], as studies have shown a decline in performance during rehabilitation tasks due to fatigue [104,105]. In this section, we discuss several techniques investigated by researchers for monitoring and detecting fatigue during rehabilitation.
Several research studies have been conducted to assess the relationship between rehabilitation and fatigability in PwMS. One study conducted by Severijns et al. looked at the fatigue induced by robot-mediated arm training in PwMS and healthy controls [105]. 16 control subjects and 16 MS subjects, with a median EDSS score of 6, participated in the study. The two groups performed repetitive anteflexion movements using a HapticMaster robot. During the exercise, EMG data were recorded from the anterior deltoid, middle deltoid, biceps brachii and upper trapezius muscles using a Delsys sensor. Fatigue was recorded using a Visual Analogue Scale, which provided a subjective measure of state fatigue. Fatigue was also recorded by analyzing the RMS and median frequency of the EMG signal as well as Maximum Voluntary Contraction (MVC) of each muscle. Although the authors found no relationship between subjective feeling of fatigue and objective measures, they did find a higher increase in RMS values of healthy individuals compared to PwMS, accompanied by an 8% decrease in median frequency in healthy control compared to a 5.4% decrease in PwMS. In general, a drop in the mean frequency of greater than 8% is used as an indication of fatigue [106,107]. The authors caution against overinterpreting the differences in median frequency as they found that the on an average a 5.4% change in the median frequency was observed for PwMS. The study also found that objectively measured fatigue was present in both groups after robot-mediated training. PwMS with hand grip weakness displayed a larger increase in subjective fatigue level than PwMS with normal hand grip strength, and the authors concluded that objective signs of fatigue were less obvious in weaker PwMS. Changes in MVC were correlated with subjective feelings of fatigue in PwMS, though this relationship was not observed in healthy controls.
Octavia et al. evaluated muscle fatigue during robot-mediated upper limb rehabilitation as PwMS and healthy control subjects were performing five sessions of lifting and transporting exercises using a HapticMaster robot and an I-Travel system [104]. While performing the tasks EMG was recorded from the anterior deltoid and trapezius muscles, filtered using Infinite Impulse Response and Butterworth bandpass filters and then rectified using an RMS sliding window approach. Analysis of the EMG measures also incorporated performance measures and subjective fatigue measures captured with a visual analog scale. The authors observed an increase in the EMG amplitude in the muscles responsible for the exercise accompanied by a decrease in performance and an increase in the perception of fatigue. There were 20.29% and 15.25% increases in EMG amplitude in PwMS and control subjects respectively between the first and the final session, which was taken as evidence of greater muscle fatigue in PwMS.
A study conducted by Wier et al. examined the effect of robot-assisted body-weight-supported treadmill training (BWSTT) on the quality of life (QOL) for PwMS [108]. In robot assisted BWSTT, gait training is conducted on a treadmill, where the user is suspended and assistance is provided to them through an exoskeleton robot. The authors compared the effects of training done with a Lokomat robotic device to training without. To assess QOL measures, they used the Multiple Sclerosis Quality of Life Inventory (MSQLI), which is a 36-item short form survey incorporating the MFIS and a Pain Effect Scale (PES) to measure the effect of pain on the subject’s mood, physical and psychosocial functions. The subjects were divided into two groups, each of which performed training with the robot in one of two sessions with a six-week rest period between them. PwMS recruited for this study had a mean EDSS score of 4.9 ± 1.2. Questionnaires were collected at baseline, after the first session, after the six-week rest period and after completing the second session. Participants in both groups showed a significant overall improvement in a few of the QOL measures including MFIS items. In all subjects, regardless of whether robot training occurred in the first or second session, there were significant improvements in FSS, MFIS and PES following the first session. However, there were no significant differences in improvement between the two groups. Within the groups there were significant improvements in some of the measures, but across groups, only one measure showed a significant difference, suggesting that the order of training sessions (with the robot and without) did not matter. However, the number of participants was small (6 subjects used the robot in session 1 and 7 subjects used it in session 2).
Straudi et al. analyzed the effects of robot-assisted gait training on subjects with progressive MS by comparing subjects using a Lokomat robot, who had a mean EDSS score of 6.43 ± 0.38, with subjects who performed conventional walking therapy, who had a mean EDSS score of 6.46 ± 0.43 [109]. Both groups performed multiple tests including the FSS and were evaluated at the start of the study, after 3 weeks, after the end of the treatment and during a 3-month follow up. Overall, the authors found that robot-assisted gait training might be beneficial to people with progressive MS. However, none of the treatment methodologies had a significant effect on perceived fatigue, which differs from other studies [83,108]. One explanation advanced by the authors is that the FSS might not be reliable while measuring high levels of fatigue.
Pompa et al. studied the effect of robot-assisted gait training in PwMS with high disability in comparison to conventional walking training [83]. During this study the researchers recorded parameters for walking capacity and ability using the Rivermed Mobility Index and a modified Barthel Index VAS to measure lower limb spasticity and the FSS to measure perceived fatigue. They found that the improvement in walking using robot-assisted training was comparable with that from conventional walking training. When they looked at the effect of the two training methodologies on fatigue, however, they found that subjects in the robot-assisted group reported lower fatigue severity than the subjects in the conventional training group, who showed no significant improvements. The authors suggested that robot-assisted gait training should therefore be considered as an add-on to conventional training.
One of the most important and detrimental phenomena during rehabilitation is fatigue. The performance during rehabilitation has shown to worsen due to fatigue. Many studies have directly or indirectly tried to account for fatigue. Octavia et al. aimed to evaluate muscular fatigue during robot mediated upper limb rehabilitation [104]. Here, they found that during rehabilitation there was an increase in the subjective fatigue which was accompanied by a decrease in performance. This could have a negative impact on the rehabilitation. An increase in the EMG amplitude was observed with the increase in subjective fatigue, indicating its usability to objectively measure fatigue. Serverijns et al. also observed an increase in fatigue during robot mediated upper limb training [105]. They found a correlation between the force applied by the PwMS and subjective feeling of fatigue, however, such a relationship could not be observed between subjective fatigue and EMG parameters. Although, an 8% and 5.4% decline in median frequency was observed for healthy and PwMS subjects respectively during the exercise. Apart from upper limb rehabilitation, the effect of fatigue on gait rehabilitation has also been studied. Wier et al. examined the QOL measures during robot assisted BWSTT [108]. Among other metrics, fatigue was also examined. An overall improvement in subjective feeling of fatigue was observed both with and without robot assisted BWSTT. There was limited evidence to support the use of robot assisted BWSTT over conventional BWSTT. A study conducted by Pompa et al. found similar result with robot assisted gait training. Although, people who underwent conventional walking training did not show an improvement in subjective fatigue [83]. Straudi et al. on the other hand did not find significant improvement in the perceived fatigue during robot assisted gait training [109]. Overall, studies have shown that fatigue is an important aspect to be considered while designing rehabilitation protocols for PwMS.
6. Concluding Remarks
In this paper, we present a survey of assistive technologies used for assessment and rehabilitation for PwMS, with a focus on movement defects in the upper and lower body. Multiple sensors and devices like robots have been used to detect movement defects in upper limbs as well as gait defects. Wearable and lightweight sensors and devices can enable the development of remote monitoring systems which would enhance the decision making of clinicians and health care providers for treatment and rehabilitation plans. One of the most common types of sensor used in analyzing gait defects is the inertial sensor. BioStamp and MTx are two of the most common inertial sensors used in gait assessment. For gait rehabilitation, robot-assisted gait training has shown some advantages over conventional walking training. The Lokomat is one of the most common robots used for robot-assisted training. Robot-assisted rehabilitation in conjunction with active rehabilitation techniques have shown promising results in gait rehabilitation. Along with gait, upper limb rehabilitation and assessment have also benefited from robotics. Multiple robots like the PHANTOM, HapticMaster and Braccio di Ferro among others have been developed for this purpose. Although haptic and robotic interfaces are shown to be effective in identifying upper arm impairments, they are expensive and require a clinical setup and technical assistance for setup and monitoring.
Taking the several applications mentioned in this survey into consideration, we would like to highlight the need for selecting appropriate rehabilitation and assessment tasks when designing sensor-based and robotic rehabilitation systems. Clinicians and researchers should take into consideration each patient’s specific needs while selecting an assessment or rehabilitation strategy (tests, sensors). The selection and design of assistive technologies (e.g., sensors, robots) should be made considering both user experience (e.g., non-invasive sensors) and efficiency (clinical outcomes). Studies have shown that task-oriented training is more effective than passive training during rehabilitation. Moreover, user involvement (patients, caregivers and clinicians) should be considered during both system design and evaluation [110]. Successful design and selection of sensor-based technologies for PwMS can enable the development of sensor-based experimental testbeds for research in MS and analysis of multisensing data during assessment and rehabilitation of PwMS towards improving such technologies and treatment plans.
Since fatigue is such a commonly reported symptom, it should be considered during assessment and rehabilitation of PwMS. Towards this, we provide a survey of recent research in this area that highlights the importance of measuring and accounting for fatigue in assessing PwMS, in general daily living and in rehabilitation. Since fatigue, as well as its impact on user behavior and performance, is highly subjective and varies across users, there is a need to combine both subjective and objective fatigue measures to enable both patients and caregivers to provide reports and expert input in order to develop reliable personalized fatigue measurement and detection tools that can be used to provide PwMS with personalized rehabilitation plans towards improving their treatments and thus their quality of life. Moreover, designing sensor-based assessment and rehabilitation systems which take fatigue into account, could lead to valuable multimodal data for physical and cognitive fatigue analysis [101]. The variety of the available assistive technologies for MS, as presented in this survey, can provide researchers and clinicians with insights about performance of PwMS in daily activities, assessment and rehabilitation, and how it is affected by fatigue, mood and other cognitive–behavioral factors [111].
Author Contributions
A.R., V.K., and D.C. searched for papers then refined, enhanced and validated the search results. M.G. was responsible for materials related to Multimodal Gait and Balance Monitoring (Section 3.1). D.C. was responsible for content on Multimodal Assessment of Upper Limb Motor Function (Section 3.2). K.T. was accountable for materials related to Introduction, Conclusion and helped by supervising the work and assisted with the overall structure of the paper. A.R. and V.K. wrote the article and coordinated the work. M.A. and M.P. helped with writing and proofreading the manuscript. J.C.F., G.W., and F.M. managed the work and contributed to the manuscript preparation.
Funding
This work is based upon research supported by NSF under award numbers NSF-CHS 1565328, NSF-PFI 1719031.
Conflicts of Interest
The authors declare no conflict of interest.
References
- National MS Society. Definition of MS. Available online: https://www.nationalmssociety.org/What-is-MS/Definition-of-MS (accessed on 12 December 2018).
- Reich, D.S.; Lucchinetti, C.F.; Calabresi, P.A. Multiple Sclerosis. N. Engl. J. Med. 2018, 378, 169–180. [Google Scholar] [CrossRef] [PubMed]
- Lublin, F.D.; Reingold, S.C.; Cohen, J.A.; Cutter, G.R.; Sørensen, P.S.; Thompson, A.J.; Wolinsky, J.S.; Balcer, L.J.; Banwell, B.; Barkhof, F.; et al. Defining the clinical course of multiple sclerosis: The 2013 revisions. Neurology 2014, 83, 278–286. [Google Scholar] [CrossRef]
- National MS Society. Types of MS. Available online: https://www.nationalmssociety.org/What-is-MS/Types-of-MS (accessed on 12 December 2018).
- Polman, C.H.; Reingold, S.C.; Banwell, B.; Clanet, M.; Cohen, J.A.; Filippi, M.; Fujihara, K.; Havrdova, E.; Hutchinson, M.; Kappos, L.; et al. Diagnostic criteria for multiple sclerosis: 2010 Revisions to the McDonald criteria. Ann. Neurol. 2011, 69, 292–302. [Google Scholar] [CrossRef]
- Cutter, G.R.; Baier, M.L.; Rudick, R.A.; Cookfair, D.L.; Fischer, J.S.; Petkau, J.; Syndulko, K.; Weinshenker, B.G.; Antel, J.P.; Confavreux, C.; et al. Development of a multiple sclerosis functional composite as a clinical trial outcome measure. Brain 1999, 122, 871–882. [Google Scholar] [CrossRef] [PubMed]
- Mehanna, R.; Jankovic, J. Movement disorders in multiple sclerosis and other demyelinating diseases. J. Neurol. Sci. 2013, 328, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kjølhede, T.; Vissing, K.; Dalgas, U. Multiple sclerosis and progressive resistance training: A systematic review. Mult. Scler. J. 2012, 18, 1215–1228. [Google Scholar] [CrossRef]
- Dilokthornsakul, P.; Valuck, R.J.; Nair, K.V.; Corboy, J.R.; Allen, R.R.; Campbell, J.D. Multiple sclerosis prevalence in the United States commercially insured population. Neurology 2016, 86, 1014–1021. [Google Scholar] [CrossRef]
- Sosnoff, J.J.; Sandroff, B.M.; Motl, R.W. Quantifying gait abnormalities in persons with multiple sclerosis with minimal disability. Gait Post. 2012, 36, 154–156. [Google Scholar] [CrossRef] [PubMed]
- Schumacher, G.A.; Beebe, G.; Kibler, R.F.; Kurland, L.T.; Kurtzke, J.F.; McDowell, F.; Nagler, B.; Sibley, W.A.; Tourtellotte, W.W.; Willmon, T.L. Problems of experimental trials of therapy in multiple sclerosis: Report by the panel on the evaluation of experimental trials of therapy in multiple sclerosis. Ann. N. Y. Acad. Sci. 1965, 122, 552–568. [Google Scholar] [CrossRef] [PubMed]
- Poser, C.M.; Paty, D.W.; Scheinberg, L.; McDonald, W.I.; Davis, F.A.; Ebers, G.C.; Johnson, K.P.; Sibley, W.A.; Silberberg, D.H.; Tourtellotte, W.W. New diagnostic criteria for multiple sclerosis: Guidelines for research protocols. Ann. Neurol. 1983, 13, 227–231. [Google Scholar] [CrossRef] [PubMed]
- McDonald, W.I.; Compston, A.; Edan, G.; Goodkin, D.; Hartung, H.P.; Lublin, F.D.; McFarland, H.F.; Paty, D.W.; Polman, C.H.; Reingold, S.C.; et al. Recommended diagnostic criteria for multiple sclerosis: Guidelines from the international panel on the diagnosis of multiple sclerosis. Ann. Neurol. 2001, 50, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Catherine Lovering, A.S.L. Why It Pays to Start MS Treatment Early. Available online: https://www.healthline.com/health/multiple-sclerosis/recently-diagnosed-why-start-ms-treatment-early (accessed on 12 December 2018).
- National MS Society. Assessment and Interventions in MS. Available online: https://www.nationalmssociety.org/For-Professionals/Clinical-Care/Managing-MS/Rehabilitation/Rehabilitation-Paradigm/Assessment-and-Intervention (accessed on 12 December 2018).
- Schwartz, S.; Cohen, M.E.; Herbison, G.J.; Shah, A. Relationship between two measures of upper extremity strength: Manual muscle test compared to hand-held myometry. Arch. Phys. Med. Rehabil. 1992, 73, 1063–1068. [Google Scholar] [PubMed]
- Prohealthcare.com. Manual Muscle Testing Grading and Procedures. Available online: https://www.prohealthcareproducts.com/blog/manual-muscle-testing-grading-and-procedures/ (accessed on 12 December 2018).
- Hoang, P.D.; Gandevia, S.C.; Herbert, R.D. Prevalence of joint contractures and muscle weakness in people with multiple sclerosis. Disab. Rehabil. 2014, 36, 1588–1593. [Google Scholar] [CrossRef] [PubMed]
- Nilsagard, Y.; Lundholm, C.; Gunnarsson, L.G.; Denison, E. Clinical relevance using timed walk tests and ‘timed up and go’ testing in persons with Multiple Sclerosis. Physiother. Res. Int. 2007, 12, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Vaney, C.; Blaurock, H.; Gattlen, B.; Meisels, C. Assessing mobility in multiple sclerosis using the Rivermead Mobility Index and gait speed. Clin. Rehabil. 1996, 10, 216–226. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The Timed “Up & Go”: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef]
- Fischer, J.S.; Rudick, R.A.; Cutter, G.R.; Reingold, S.C.; National MS Society Clinical Outcomes Assessment Task Force. The Multiple Sclerosis Functional Composite measure (MSFC): An integrated approach to MS clinical outcome assessment. Mult. Scler. J. 1999, 5, 244–250. [Google Scholar] [CrossRef]
- Givon, U.; Zeilig, G.; Achiron, A. Gait analysis in multiple sclerosis: Characterization of temporal—Spatial parameters using GAITRite functional ambulation system. Gait Post. 2009, 29, 138–142. [Google Scholar] [CrossRef]
- Spain, R.; George, R.S.; Salarian, A.; Mancini, M.; Wagner, J.; Horak, F.; Bourdette, D. Body-worn motion sensors detect balance and gait deficits in people with multiple sclerosis who have normal walking speed. Gait Post. 2012, 35, 573–578. [Google Scholar] [CrossRef]
- Gehlsen, G.; Beekman, K.; Assmann, N.; Winant, D.; Seidle, M.; Carter, A. Gait characteristics in multiple sclerosis: Progressive changes and effects of exercise on parameters. Arch. Phys. Med. Rehabil. 1986, 67, 536–539. [Google Scholar]
- Gong, J.; Goldman, M.D.; Lach, J. Deepmotion: A deep convolutional neural network on inertial body sensors for gait assessment in multiple sclerosis*. In Proceedings of the 2016 IEEE Wireless Health (WH), Bethesda, MD, USA, 25–27 October 2016; pp. 1–8. [Google Scholar] [CrossRef]
- Moon, Y.; McGinnis, R.S.; Seagers, K.; Motl, R.W.; Sheth, N.; Wright, J.A., Jr.; Ghaffari, R.; Sosnoff, J.J. Monitoring gait in multiple sclerosis with novel wearable motion sensors. PLoS ONE 2017, 12, 1–19. [Google Scholar] [CrossRef]
- Kaufman, M.; Moyer, D.; Norton, J. The significant change for the Timed 25-Foot Walk in the Multiple Sclerosis Functional Composite. Mult. Scler. J. 2000, 6, 286–290. [Google Scholar] [CrossRef]
- Benedetti, M.G.; Piperno, R.; Simoncini, L.; Bonato, P.; Tonini, A.; Giannini, S. Gait abnormalities in minimally impaired multiple sclerosis patients. Mult. Scler. J. 1999, 5, 363–368. [Google Scholar] [CrossRef]
- Health Care Journey. Loss of hand Dexterity and Coordination. Available online: http://www.healthcarejourney.com/loss-of-hand-dexterity-and-coordination.html (accessed on 12 December 2018).
- Feys, P.; Lamers, I.; Francis, G.; Benedict, R.; Phillips, G.; LaRocca, N.; Hudson, L.D.; Rudick, R.; Multiple Sclerosis Outcome Assessments Consortium. The Nine-Hole Peg Test as a manual dexterity performance measure for multiple sclerosis. Mult. Scler. J. 2017, 23, 711–720. [Google Scholar] [CrossRef]
- Alusi, S.H.; Worthington, J.; Glickman, S.; Findley, L.J.; Bain, P.G. Evaluation of three different ways of assessing tremor in multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2000, 68, 756–760. [Google Scholar] [CrossRef] [PubMed]
- Yozbatıran, N.; Baskurt, F.; Baskurt, Z.; Ozakbas, S.; Idiman, E. Motor assessment of upper extremity function and its relation with fatigue, cognitive function and quality of life in multiple sclerosis patients. J. Neurol. Sci. 2006, 246, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Earhart, G.M.; Cavanaugh, J.T.; Ellis, T.; Ford, M.P.; Foreman, K.B.; Dibble, L. The 9-hole PEG test of upper extremity function: average values, test-retest reliability, and factors contributing to performance in people with Parkinson disease. J. Neurol. Phys. Ther. 2011, 35, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Poole, J.L.; Burtner, P.A.; Torres, T.A.; McMullen, C.K.; Markham, A.; Marcum, M.L.; Anderson, J.B.; Qualls, C. Measuring dexterity in children using the Nine-hole Peg Test. J. Hand Ther. 2005, 18, 348–351. [Google Scholar] [CrossRef]
- Mathiowetz, V.; Volland, G.; Kashman, N.; Weber, K. Adult norms for the Box and Block Test of manual dexterity. Am. J. Occup. Ther. 1985, 39, 386–391. [Google Scholar] [CrossRef]
- Chen, H.M.; Chen, C.C.; Hsueh, I.P.; Huang, S.L.; Hsieh, C.L. Test-Retest Reproducibility and Smallest Real Difference of 5 Hand Function Tests in Patients with Stroke. Neurorehabil. Neural Repair 2009, 23, 435–440. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.C.; Magasi, S.R.; Bohannon, R.W.; Reuben, D.B.; McCreath, H.E.; Bubela, D.J.; Gershon, R.C.; Rymer, W.Z. Assessing Dexterity Function: A Comparison of Two Alternatives for the NIH Toolbox. J. Hand Ther. 2011, 24, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Grice, K.O.; Vogel, K.A.; Le, V.; Mitchell, A.; Muniz, S.; Vollmer, M.A. Adult norms for a commercially available Nine Hole Peg Test for finger dexterity. Am. J. Occup. Ther. 2003, 57, 570–573. [Google Scholar] [CrossRef]
- Yancosek, K.E.; Howell, D. A Narrative Review of Dexterity Assessments. J. Hand Ther. 2009, 22, 258–270. [Google Scholar] [CrossRef]
- National MS Society. Nine Hole Peg Test. Available online: https://www.nationalmssociety.org/For-Professionals/Researchers/Resources-for-Researchers/Clinical-Study-Measures/9-Hole-Peg-Test-(9-HPT) (accessed on 12 December 2018).
- Platz, T.; Pinkowski, C.; van Wijck, F.; Kim, I.H.; di Bella, P.; Johnson, G. Reliability and validity of arm function assessment with standardized guidelines for the Fugl-Meyer Test, Action Research Arm Test and Box and Block Test: A multicentre study. Clin.Rehabil. 2005, 19, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Guralnik, J.M.; Fried, L.P.; Simonsick, E.M.; Lafferty, M.E.; Kasper, J.D. The Women’s Health and Aging Study: Health and Social Characteristics of Older Women With Disability; DIANE Publishing: Collingdale, PA, USA, 1995. [Google Scholar]
- Gallus, J.; Mathiowetz, V. Test-retest reliability of the Purdue Pegboard for persons with multiple sclerosis. Am. J. Occup. Ther. 2003, 57, 108–111. [Google Scholar] [CrossRef]
- Najafi, B.; Horn, D.; Marclay, S.; Crews, R.T.; Wu, S.; Wrobel, J.S. Assessing Postural Control and Postural Control Strategy in Diabetes Patients Using Innovative and Wearable Technology. J. Diabetes Sci. Technol. 2010, 4, 780–791. [Google Scholar] [CrossRef] [PubMed]
- Fjeldstad, C.; Pardo, G.; Frederiksen, C.; Bemben, D.; Bemben, M. Assessment of Postural Balance in Multiple Sclerosis. Int. J. MS Care 2009, 11, 1–5. [Google Scholar] [CrossRef]
- Hausdorff, J.M. Gait variability: Methods, modeling and meaning. J. NeuroEng. Rehabil. 2005, 2, 19. [Google Scholar] [CrossRef]
- Natioanl MS Society. Walking Difficulties. Available online: https://www.nationalmssociety.org/Symptoms-Diagnosis/MS-Symptoms/Walking-Gait-Balance-Coordination (accessed on 12 December 2018).
- Sun, R.; Moon, Y.; McGinnis, R.S.; Seagers, K.; Motl, R.W.; Sheth, N.; Wright, J.A.; Ghaffari, R.; Patel, S.; Sosnoff, J.J. Assessment of Postural Sway in Individuals with Multiple Sclerosis Using a Novel Wearable Inertial Sensor. Digit. Biomark. 2018, 2, 1–10. [Google Scholar] [CrossRef]
- Filli, L.; Sutter, T.; Easthope, C.S.; Killeen, T.; Meyer, C.; Reuter, K.; Lörincz, L.; Bolliger, M.; Weller, M.; Curt, A.; et al. Profiling walking dysfunction in multiple sclerosis: Characterisation, classification and progression over time. Sci. Rep. 2018, 8, 4984. [Google Scholar] [CrossRef]
- MTx. Xsens Technologies B.V. Available online: https://www.xsens.com/technologytech/mtx/ (accessed on 12 December 2018).
- Greene, B.R.; Rutledge, S.; McGurgan, I.; McGuigan, C.; O’Connell, K.; Caulfield, B.; Tubridy, N. Assessment and Classification of Early-Stage Multiple Sclerosis With Inertial Sensors: Comparison Against Clinical Measures of Disease State. IEEE J. Biomed. Health Inform. 2015, 19, 1356–1361. [Google Scholar] [CrossRef] [PubMed]
- BioStamp. MC10 Inc.: Lexington, MA, USA. Available online: https://www.mc10inc.com/our-products/biostamprc (accessed on 12 December 2018).
- GT3X. Actigraph, Inc. Available online: https://www.actigraphcorp.com/support/activity-monitors/gt3x/ (accessed on 12 December 2018).
- Lopez Martinez, D.; Picard, R. Wearable technologies for multiple sclerosis: The future role of wearable stress measurement in improving quality of life. In Proceedings of the Second International Conference on Smart Portable, Wearable, Implantable and Disability-Oriented Devices and Systems (SPWID’16), Valencia, Spain, 22–26 May 2016. [Google Scholar]
- Muro-de-la Herran, A.; Garcia-Zapirain, B.; Mendez-Zorrilla, A. Gait Analysis Methods: An Overview of Wearable and Non-Wearable Systems, Highlighting Clinical Applications. Sensors 2014, 14, 3362–3394. [Google Scholar] [CrossRef] [PubMed]
- GAITRite. CIR Systems, Inc. Available online: https://www.gaitrite.com/ (accessed on 12 December 2018).
- M3D Force Plate. CTec Gihan Co., Ltd. Available online: http://www.tecgihan.co.jp/en/products/m3d_forceplate/ (accessed on 12 December 2018).
- Zebris FDM-T System. Zebris Medical GmbH. Available online: https://www.zebris.de/en/medical/products-solutions/gait-analysis-fdm-t/ (accessed on 12 December 2018).
- FootScan. RSscan International NV. Available online: https://www.rsscan.com/es/footscan/ (accessed on 12 December 2018).
- MatScan. Tekscan, Inc. Available online: https://www.tekscan.com/products-solutions/systems/matscan (accessed on 12 December 2018).
- Kistler Force Plate. Kistler Instrument Corp. Available online: https://www.kistler.com/en/applications/sensor-technology/biomechanics-and-force-plate/ (accessed on 12 December 2018).
- OR6-7 Force Platform. AMTI Force and Motion. Available online: http://www.amti.uk.com/products/or6-7-force-platform.php (accessed on 12 December 2018).
- Dobkin, B.H.; Dorsch, A. The Promise of mHealth: Daily Activity Monitoring and Outcome Assessments by Wearable Sensors. Neurorehabil. Neural Repair 2011, 25, 788–798. [Google Scholar] [CrossRef] [PubMed]
- DynaPort. McRoberts B.V. Available online: https://www.rsscan.com/es/footscan/ (accessed on 12 December 2018).
- IDDEA LifeGait. MiniSun LLC: Fresno, California, USA. Available online: http://www.minisun.com/LifeGait.htm (accessed on 12 December 2018).
- Bethoux, F.; Varsanik, J.S.; Chevalier, T.W.; Halpern, E.F.; Stough, D.; Kimmel, Z.M. Walking speed measurement with an Ambient Measurement System (AMS) in patients with multiple sclerosis and walking impairment. Gait Post. 2018, 61, 393–397. [Google Scholar] [CrossRef] [PubMed]
- Corona, F.; Gervasoni, E.; Coghe, G.; Cocco, E.; Ferrarin, M.; Pau, M.; Cattaneo, D. Validation of the Arm Profile Score in assessing upper limb functional impairments in people with multiple sclerosis. Clin. Biomech. 2018, 51, 45–50. [Google Scholar] [CrossRef]
- Johansson, S.; Ytterberg, C.; Claesson, I.M.; Lindberg, J.; Hillert, J.; Andersson, M.; Widén Holmqvist, L.; von Koch, L. High concurrent presence of disability in multiple sclerosis. J. Neurol. 2007, 254, 767. [Google Scholar] [CrossRef] [PubMed]
- Teufl, S.; Preston, J.; van Wijck, F.; Stansfield, B. Objective identification of upper limb tremor in multiple sclerosis using a wrist-worn motion sensor: Establishing validity and reliability. Br. J. Occup. Ther. 2017, 80, 596–602. [Google Scholar] [CrossRef]
- Fahn, S.; Tolosa, E.; Marín, C. Clinical rating scale for tremor. Parkinson’s Dis. Mov. Disord. 1993, 2, 271–280. [Google Scholar]
- Lyle, R.C. A performance test for assessment of upper limb function in physical rehabilitation treatment and research. Int. J. Rehabil. Res. 1981, 4, 483–492. [Google Scholar] [CrossRef]
- Carpinella, I.; Cattaneo, D.; Ferrarin, M. Quantitative assessment of upper limb motor function in Multiple Sclerosis using an instrumented Action Research Arm Test. J. NeuroEng. Rehabil. 2014, 11, 67. [Google Scholar] [CrossRef]
- Carpinella, I.; Cattaneo, D.; Ferrarin, M. Hilbert-Huang transform based instrumental assessment of intention tremor in multiple sclerosis. J. Neural Eng. 2015, 12, 046011. [Google Scholar] [CrossRef]
- Bardorfer, A.; Munih, M.; Zupan, A.; Primozic, A. Upper limb motion analysis using haptic interface. IEEE/ASME Trans. Mechatron. 2001, 6, 253–260. [Google Scholar] [CrossRef]
- Pellegrino, L.; Coscia, M.; Muller, M.; Solaro, C.; Casadio, M. Evaluating upper limb impairments in multiple sclerosis by exposure to different mechanical environments. Sci. Rep. 2018, 8, 2110. [Google Scholar] [CrossRef]
- World Health Organization. World Report on Disability; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Jezernik, S.; Colombo, G.; Keller, T.; Frueh, H.; Morari, M. Robotic Orthosis Lokomat: A Rehabilitation and Research Tool. Neuromodulation Technol. Neural Interface 2003, 6, 108–115. [Google Scholar] [CrossRef]
- Beer, S.; Aschbacher, B.; Manoglou, D.; Gamper, E.; Kool, J.; Kesselring, J. Robot-assisted gait training in multiple sclerosis: A pilot randomized trial. Mult. Scler. J. 2008, 14, 231–236. [Google Scholar] [CrossRef]
- Straudi, S.; Benedetti, M.; Venturini, E.; Manca, M.; Foti, C.; Basaglia, N. Does robot-assisted gait training ameliorate gait abnormalities in multiple sclerosis? A pilot randomized-control trial. NeuroRehabilitation 2013, 33, 555–563. [Google Scholar]
- Brütsch, K.; Schuler, T.; Koenig, A.; Zimmerli, L.; (-Koeneke), S.M.; Lünenburger, L.; Riener, R.; Jäncke, L.; Meyer-Heim, A. Influence of virtual reality soccer game on walking performance in robotic assisted gait training for children. J. NeuroEng. Rehabil. 2010, 7, 15. [Google Scholar] [CrossRef]
- Horst, R.W. A bio-robotic leg orthosis for rehabilitation and mobility enhancement. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; pp. 5030–5033. [Google Scholar] [CrossRef]
- Pompa, A.; Morone, G.; Iosa, M.; Pace, L.; Catani, S.; Casillo, P.; Clemenzi, A.; Troisi, E.; Tonini, A.; Paolucci, S.; et al. Does robot-assisted gait training improve ambulation in highly disabled multiple sclerosis people? A pilot randomized control trial. Mult. Scler. J. 2017, 23, 696–703. [Google Scholar] [CrossRef]
- Husemann, B.; Müller, F.; Krewer, C.; Heller, S.; Koenig, E. Effects of Locomotion Training with Assistance of a Robot-Driven Gait Orthosis in Hemiparetic Patients After Stroke. Stroke 2007, 38, 349–354. [Google Scholar] [CrossRef]
- Bonzano, L.; Tacchino, A.; Brichetto, G.; Roccatagliata, L.; Dessypris, A.; Feraco, P.; Carvalho, M.L.L.D.; Battaglia, M.A.; Mancardi, G.L.; Bove, M. Upper limb motor rehabilitation impacts white matter microstructure in multiple sclerosis. NeuroImage 2014, 90, 107–116. [Google Scholar] [CrossRef]
- Streicher, M.C.; Alberts, J.L.; Sutliff, M.H.; Bethoux, F. Effects and feasibility of virtual reality system vs traditional physical therapy training in multiple sclerosis patients. Int. J. Ther. Rehabil. 2018, 25, 522–528. [Google Scholar] [CrossRef]
- Carpinella, I.; Cattaneo, D.; Abuarqub, S.; Ferrarin, M. Robot-Based Rehabilitation of the Upper Limbs in Multiple Sclerosis: Feasibility and Preliminary Results. J. Rehabil. Med. 2009, 41, 966–970. [Google Scholar] [CrossRef]
- Carpinella, I.; Cattaneo, D.; Bertoni, R.; Ferrarin, M. Robot Training of Upper Limb in Multiple Sclerosis: Comparing Protocols With or WithoutManipulative Task Components. IEEE Trans. Neural Syst. Rehabil. Eng. 2012, 20, 351–360. [Google Scholar] [CrossRef]
- Sampson, P.; Freeman, C.; Coote, S.; Demain, S.; Feys, P.; Meadmore, K.; Hughes, A. Using Functional Electrical Stimulation Mediated by Iterative Learning Control and Robotics to Improve Arm Movement for People With Multiple Sclerosis. IEEE Trans. Neural Syst. Rehabil. Eng. 2016, 24, 235–248. [Google Scholar] [CrossRef]
- Feys, P.; Coninx, K.; Kerkhofs, L.; De Weyer, T.; Truyens, V.; Maris, A.; Lamers, I. Robot-supported upper limb training in a virtual learning environment: A pilot randomized controlled trial in persons with MS. J. NeuroEng. Rehabil. 2015, 12, 60. [Google Scholar] [CrossRef]
- Mark, V.; Taub, E.; Bashir, K.; Uswatte, G.; Delgado, A.; Bowman, M.; Bryson, C.; McKay, S.; Cutter, G. Constraint-Induced Movement therapy can improve hemiparetic progressive multiple sclerosis. Preliminary findings. Mult. Scler. J. 2008, 14, 992–994. [Google Scholar] [CrossRef]
- Krupp, L.B. Fatigue in Multiple Sclerosis. CNS Drugs 2003, 17, 225–234. [Google Scholar] [CrossRef]
- Johansson, S.; Kottorp, A.; Lee, K.A.; Gay, C.L.; Lerdal, A. Can the Fatigue Severity Scale 7-item version be used across different patient populations as a generic fatigue measure—A comparative study using a Rasch model approach. Health Qual. Life Outcomes 2014, 12, 24. [Google Scholar] [CrossRef]
- Braley, T.J.; Chervin, R.D. Fatigue in Multiple Sclerosis: Mechanisms, Evaluation, and Treatment. Sleep 2010, 33, 1061–1067. [Google Scholar] [CrossRef]
- Sehle, A.; Vieten, M.; Sailer, S.; Mündermann, A.; Dettmers, C. Objective assessment of motor fatigue in multiple sclerosis: The Fatigue index Kliniken Schmieder (FKS). J. Neurol. 2014, 261, 1752–1762. [Google Scholar] [CrossRef]
- Krupp, L.B.; Alvarez, L.A.; LaRocca, N.G.; Scheinberg, L.C. Fatigue in multiple sclerosis. Arch. Neurol. 1988, 45, 435–437. [Google Scholar] [CrossRef]
- Barrios, L.; Oldrati, P.; Santini, S.; Lutterotti, A. Recognizing Digital Biomarkers for Fatigue Assessment in Patients with Multiple Sclerosis. In Proceedings of the 12th EAI International Conference on Pervasive Computing Technologies for Healthcare; PervasiveHealth 2018; EAI: New York, NY, USA, 2018. [Google Scholar] [CrossRef]
- Yu, F.; Bilberg, A.; Stenager, E.; Rabotti, C.; Zhang, B.; Mischi, M. A wireless body measurement system to study fatigue in multiple sclerosis. Physiol. Meas. 2012, 33, 2033. [Google Scholar] [CrossRef]
- Chipchase, S.; Lincoln, N.B.; Radford, K.A. A survey of the effects of fatigue on driving in people with multiple sclerosis. Disab. Rehabil. 2003, 25, 712–721. [Google Scholar] [CrossRef]
- Nayak, B.P.; Kar, S.; Routray, A.; Padhi, A.K. A biomedical approach to retrieve information on driver’s fatigue by integrating EEG, ECG and blood biomarkers during simulated driving session. In Proceedings of the 4th International Conference on Intelligent Human Computer Interaction (IHCI), Kharagpur, India, 27–29 December 2012; pp. 1–6. [Google Scholar] [CrossRef]
- Tsiakas, K.; Papakostas, M.; Ford, J.C.; Makedon, F. Towards a Task-driven Framework for Multimodal Fatigue Analysis During Physical and Cognitive Tasks. In Proceedings of the 5th International Workshop on Sensor-based Activity Recognition and Interaction, Berlin, Germany, 20–21 September 2018. [Google Scholar] [CrossRef]
- Dalgas, U.; Stenager, E.; Jakobsen, J.; Petersen, T.; Hansen, H.; Knudsen, C.; Overgaard, K.; Ingemann-Hansen, T. Fatigue, mood and quality of life improve in MS patients after progressive resistance training. Mult. Scler. J. 2010, 16, 480–490. [Google Scholar] [CrossRef]
- National MS Society. Multiple Sclerosis–Rehabilitaion. Available online: https://www.nationalmssociety.org/Treating-MS/Rehabilitation (accessed on 12 December 2018).
- Octavia, J.R.; Feys, P.; Coninx, K. Development of activity-related muscle fatigue during robot-mediated upper limb rehabilitation training in persons with multiple sclerosis: A pilot trial. Mult. Scler. Int. 2015, 2015. [Google Scholar] [CrossRef]
- Severijns, D.; Octavia, J.R.; Kerkhofs, L.; Coninx, K.; Lamers, I.; Feys, P. Investigation of Fatigability during Repetitive Robot-Mediated Arm Training in People with Multiple Sclerosis. PLoS ONE 2015, 10, 1–15. [Google Scholar] [CrossRef]
- Öberg, T.; Sandsjö, L.; Kadefors, R. Electromyogram mean power frequency in non-fatigued trapezius muscle. Eur. J. Appl. Physiol. Occup. Physiol. 1990, 61, 362–369. [Google Scholar] [CrossRef]
- Szucs, K.; Navalgund, A.; Borstad, J.D. Scapular muscle activation and co-activation following a fatigue task. Med. Biol. Eng. Comput. 2009, 47, 487–495. [Google Scholar] [CrossRef]
- Wier, L.M.; Hatcher, M.S.; Lo, A.C. Effect of robot-assisted versus conventional body-weight-supported treadmill training on quality of life for people with multiple sclerosis. J. Rehabil. Res. Dev. 2011, 48, 483. [Google Scholar] [CrossRef]
- Straudi, S.; Fanciullacci, C.; Martinuzzi, C.; Pavarelli, C.; Rossi, B.; Chisari, C.; Basaglia, N. The effects of robot-assisted gait training in progressive multiple sclerosis: A randomized controlled trial. Mult. Scler. J. 2016, 22, 373–384. [Google Scholar] [CrossRef]
- Holt, R.; Makower, S.; Jackson, A.; Culmer, P.; Levesley, M.; Richardson, R.; Cozens, A.; Williams, M.M.; Bhakta, B. User involvement in developing Rehabilitation Robotic devices: An essential requirement. In Proceedings of the IEEE 10th International Conference on Rehabilitation Robotics, Noordwijk, The Netherlands, 13–15 June 2007; pp. 196–204. [Google Scholar] [CrossRef]
- Rudroff, T.; Kindred, J.H.; Ketelhut, N.B. Fatigue in multiple sclerosis: Misconceptions and future research directions. Front. Neurol. 2016, 7, 122. [Google Scholar] [CrossRef]

© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).