
Near-Collapse Buildings and Unsafe Sidewalks as Neglected Urban & Public Health Issue: A Qualitative Study


Abstract
1. Introduction
2. Literature Review
2.1. National, European, and Global Burden of Disease Studies
2.2. Historical Aspects of Urbanism and City-Specific Particularities
2.3. The Structure of Facades, Balconies, and Masonries
2.4. Near-Collapse Buildings: General and Athens-Specific Issues
2.5. Sidewalks
2.6. Building Inspection Method
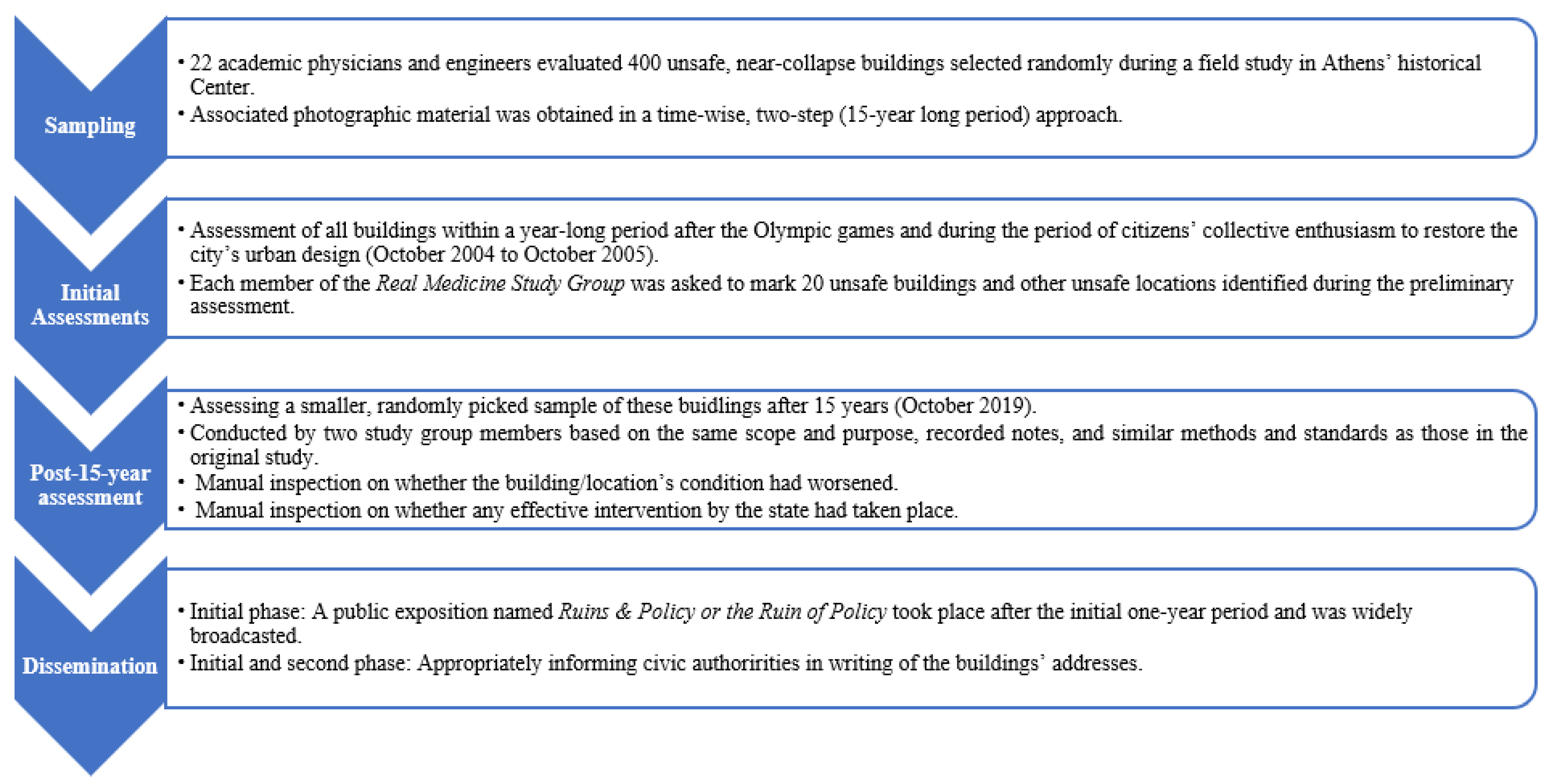
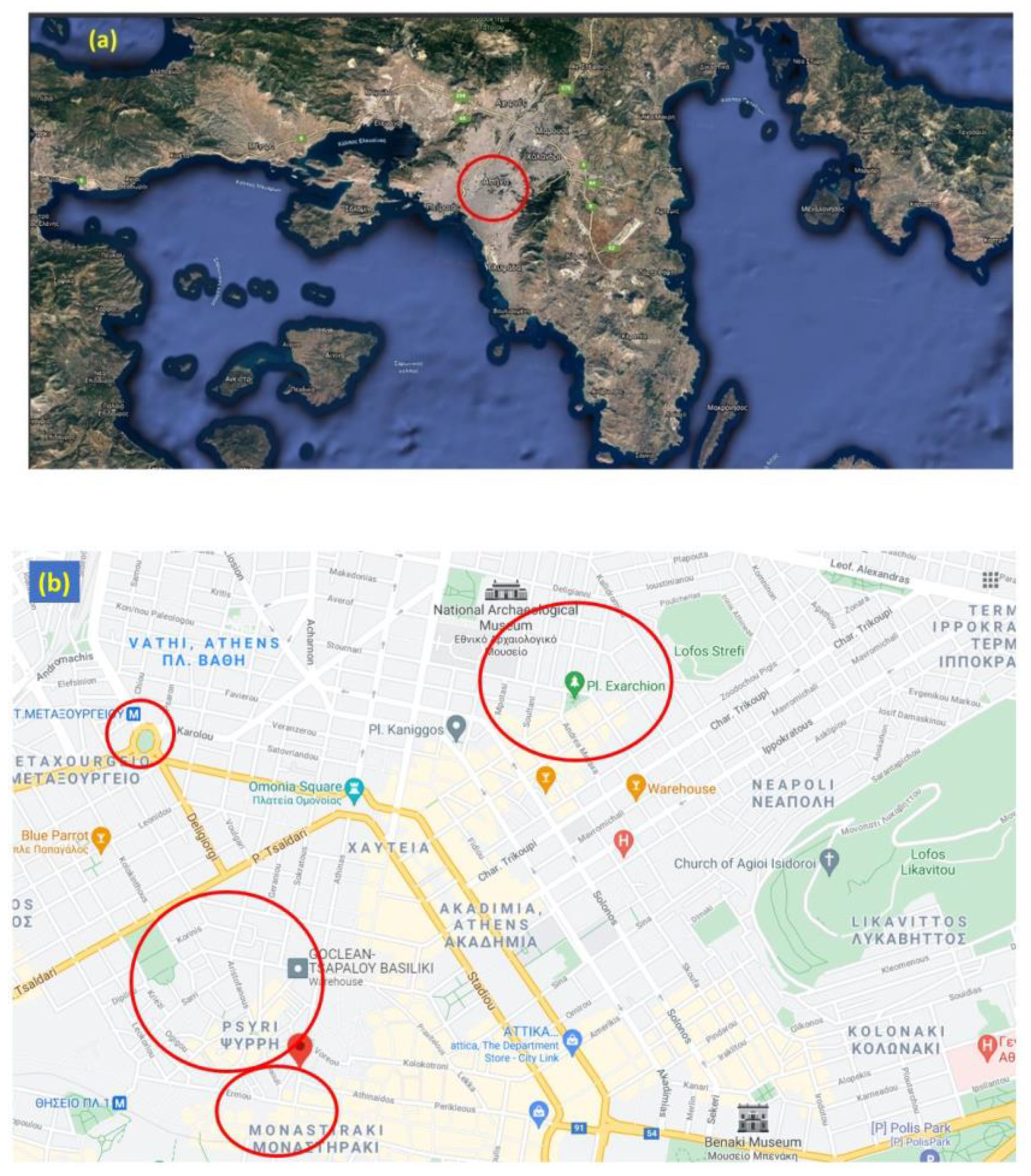
3. Materials and Methods
3.1. Methodology Rationale
3.2. Assessments
4. Results
Analysis of Case Study
5. Discussion
6. Research Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ning, P.; Schwebel, D.C.; Huang, H.; Li, L.; Li, J.; Hu, G. Global progress in road injury mortality since 2010. PLoS ONE 2016, 11, e0164560. [Google Scholar] [CrossRef] [PubMed]
- Ehrenfeucht, R.; Loukaitou-Sideris, A. Constructing the sidewalks: Municipal government and the production of public space in Los Angeles, California, 1880–1920. J. Hist. Geogr. 2007, 33, 104–124. [Google Scholar] [CrossRef]
- Rydin, Y.; Bleahu, A.; Davies, M.; Dávila, J.D.; Friel, S.; De Grandis, G.; Groce, N.; Hallal, P.C.; Hamilton, I.; Howden-Chapman, P. Shaping cities for health: Complexity and the planning of urban environments in the 21st century. Lancet 2012, 379, 2079–2108. [Google Scholar] [CrossRef]
- Halás, M.; Klapka, P.; Bačík, V.; Klobučník, M. The spatial equity principle in the administrative division of the Central European countries. PLoS ONE 2017, 12, e0187406. [Google Scholar] [CrossRef] [PubMed]
- Barton, H.; Grant, M. Urban planning for healthy cities. J. Urban Health 2013, 90, 129–141. [Google Scholar] [CrossRef]
- Barton, H.; Grant, M.; Mitcham, C.; Tsourou, C. Healthy urban planning in European cities. Health Promot. Int. 2009, 24, i91–i99. [Google Scholar] [CrossRef]
- Corburn, J. Confronting the challenges in reconnecting urban planning and public health. Am. J. Public Health 2004, 94, 541–546. [Google Scholar] [CrossRef]
- Barton, H.; Tsourou, C. Healthy Urban Planning; Routledge: London, UK, 2013. [Google Scholar]
- Frumkin, H.; Frank, L.; Frank, L.D.; Jackson, R.J. Urban Sprawl and Public Health: Designing, Planning, and Building for Healthy Communities; Island Press: Washington, DC, USA, 2004. [Google Scholar]
- Corburn, J. Toward the Healthy City: People, Places, and the Politics of Urban Planning; Mit Press: Cambridge, MA, USA, 2009. [Google Scholar]
- Salgado, M.; Madureira, J.; Mendes, A.S.; Torres, A.; Teixeira, J.P.; Oliveira, M.D. Environmental determinants of population health in urban settings. A systematic review. BMC Public Health 2020, 20, 853. [Google Scholar] [CrossRef]
- Perdue, W.C.; Stone, L.A.; Gostin, L.O. The built environment and its relationship to the public’s health: The legal framework. Am. J. Public Health 2003, 93, 1390–1394. [Google Scholar] [CrossRef]
- Zou, P.X. Strategies for minimizing corruption in the construction industry in China. J. Constr. Dev. Ctries 2006, 11, 15–29. [Google Scholar]
- Ambraseys, N.; Bilham, R. Corruption kills. Nature 2011, 469, 153–155. [Google Scholar] [CrossRef]
- Escaleras, M.; Anbarci, N.; Register, C.A. Public sector corruption and major earthquakes: A potentially deadly interaction. Public Choice 2007, 132, 209–230. [Google Scholar] [CrossRef]
- Bouckaert, G.; Peters, B.G.; Verhoest, K. Coordination of Public Sector Organizations; Springer: Berlin/Heidelberg, Germany, 2016. [Google Scholar]
- Giritli, H.; Öney-Yazıcı, E.; Topçu-Oraz, G.; Acar, E. The interplay between leadership and organizational culture in the Turkish construction sector. Int. J. Proj. Manag. 2013, 31, 228–238. [Google Scholar] [CrossRef]
- Chorianopoulos, I.; Pagonis, T.; Koukoulas, S.; Drymoniti, S. Planning, competitiveness and sprawl in the Mediterranean city: The case of Athens. Cities 2010, 27, 249–259. [Google Scholar] [CrossRef]
- Brackbill, R.M.; Thorpe, L.E.; DiGrande, L.; Perrin, M.; Sapp, J.H.; Wu, D.; Campolucci, S.; Walker, D.J.; Cone, J.; Pulliam, P. Surveillance for World Trade Center disaster health effects among survivors of collapsed and damaged buildings. Morb. Mortal. Wkly. Rep. Surveill. Summ. 2006, 55, 1–18. [Google Scholar]
- Gavett, S.H. Physical characteristics and health effects of aerosols from collapsed buildings. J. Aerosol Med. 2006, 19, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Tsouros, A.D. Twenty-seven years of the WHO European Healthy Cities movement: A sustainable movement for change and innovation at the local level. Health Promot. Int. 2015, 30, i3–i7. [Google Scholar] [CrossRef]
- World Health Organization. The power of cities: Tackling Noncommunicable Diseases and Road Traffic Injuries; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Stankūnas, M.; Kaselienė, S.; Girčienė, A.; Tsouros, A.; Avery, M. Is capacity building training effective for changing attitudes toward health inequalities? Experience from a Norway grants project in Lithuania. Medicina 2019, 55, 52. [Google Scholar] [CrossRef]
- Crowe, S.; Cresswell, K.; Robertson, A.; Huby, G.; Avery, A.; Sheikh, A. The case study approach. BMC Med. Res. Methodol. 2011, 11, 100. [Google Scholar] [CrossRef]
- Anonymous. The Registration of All Near-Collapse Buildings in Greece Begins. Available online: https://www.in.gr/2020/11/03/greece/ksekina-katagrafi-olon-ton-etoimorropon-ktirion-stin-ellada/ (accessed on 21 January 2021).
- Anonymous. Mendoni-Tagara Initiative for Dilapidated Buildings: To Protect Human Life and Cultural Heritage. Available online: https://www.iefimerida.gr/politismos/protoboylia-mendoni-gia-etoimorropa-ktiria (accessed on 13 January 2021).
- Boateng, F.G. Knowing What Leads to Building Collapses Can Help Make African Cities Safer. Conversation 2019. Available online: https://www.researchgate.net/publication/334000184_Knowing_what_leads_to_building_collapses_can_help_make_African_cities_safer (accessed on 12 January 2021).
- Zambon, I.; Salvati, L. Metropolitan growth, urban cycles and housing in a Mediterranean country, 1910s–2010s. Cities 2019, 95, 102412. [Google Scholar] [CrossRef]
- Schaffar, A.; Pavleas, S. The evolution of the Greek urban centers: 1951–2011. Rég. Dév. 2014, 39, 87–104. [Google Scholar]
- Petrakos, G.; Pavleas, S.; Anagnostou, A. The Greek Urban System: Concentration or Deconcentration, and estimation of metropolitan concentration. City Reg. 2005, 11, 225–280. [Google Scholar]
- Yannitsaris, Y. The Greek post-war architecture. Archaeol. Arts 2008, 106, 81–87. [Google Scholar]
- Anonymous. From the Apartment Buildings with the Stained Glass Windows into Today—How Urbanisation Shaped the Aesthetics of the Greek Cities. 2020. Available online: www.iefimerida.gr (accessed on 11 January 2021).
- WHO. District Health Facilities: Guidelines for Development and Operations; WHO Regional Office for the Western Pacific: Manila, Philippines, 1998. [Google Scholar]
- Dabaieh, M.; Alwall, J. Building now and building back. Refugees at the centre of an occupant driven design and construction process. Sustain. Cities Soc. 2018, 37, 619–627. [Google Scholar] [CrossRef]
- Gravesen, S.; Nielsen, P.A.; Iversen, R.; Nielsen, K.F. Microfungal contamination of damp buildings--Examples of risk constructions and risk materials. Environ. Health Perspect. 1999, 107, 505–508. [Google Scholar] [CrossRef] [PubMed]
- Sung, D. A new look at building facades as infrastructure. Engineering 2016, 2, 63–68. [Google Scholar] [CrossRef]
- Azimi, E.; Griffis, B. Statistical Analysis of NYC Buildings and Wind Damages. arXiv 2019, arXiv:1901.00103. [Google Scholar]
- Gibson, J.M.; Rodriguez, D.; Dennerlein, T.; Mead, J.; Hasch, T.; Meacci, G.; Levin, S. Predicting urban design effects on physical activity and public health: A case study. Health Place 2015, 35, 79–84. [Google Scholar] [CrossRef]
- Crispim, C.A.; Gaylarde, P.M.; Gaylarde, C.C. Algal and cyanobacterial biofilms on calcareous historic buildings. Curr. Microbiol. 2003, 46, 0079–0082. [Google Scholar] [CrossRef]
- Sing, M.C.; Love, P.E.; Liu, H.J. Rehabilitation of existing building stock: A system dynamics model to support policy development. Cities 2019, 87, 142–152. [Google Scholar] [CrossRef]
- Wallace, D.; Schalliol, D. Testing the temporal nature of social disorder through abandoned buildings and interstitial spaces. Soc. Sci. Res. 2015, 54, 177–194. [Google Scholar] [CrossRef] [PubMed]
- Curl, A.; Fitt, H.; Tomintz, M. Experiences of the built environment, falls and fear of falling outdoors among older adults: An exploratory study and future directions. Int. J. Environ. Res. Public Health 2020, 17, 1224. [Google Scholar] [CrossRef]
- Rafiemanzelat, R.; Emadi, M.I.; Kamali, A.J. City sustainability: The influence of walkability on built environments. Transp. Res. Procedia 2017, 24, 97–104. [Google Scholar] [CrossRef]
- Zapata-Diomedi, B.; Herrera, A.M.M.; Veerman, J.L. The effects of built environment attributes on physical activity-related health and health care costs outcomes in Australia. Health Place 2016, 42, 19–29. [Google Scholar] [CrossRef]
- Jensen, W.A.; Stump, T.K.; Brown, B.B.; Werner, C.M.; Smith, K.R. Walkability, complete streets, and gender: Who benefits most? Health Place 2017, 48, 80–89. [Google Scholar] [CrossRef]
- Yi, L.; Wilson, J.P.; Mason, T.B.; Habre, R.; Wang, S.; Dunton, G.F. Methodologies for assessing contextual exposure to the built environment in physical activity studies: A systematic review. Health Place 2019, 60, 102226. [Google Scholar] [CrossRef]
- Mansfield, T.J.; Peck, D.; Morgan, D.; McCann, B.; Teicher, P. The effects of roadway and built environment characteristics on pedestrian fatality risk: A national assessment at the neighborhood scale. Accid. Anal. Prev. 2018, 121, 166–176. [Google Scholar] [CrossRef]
- Araújo, E.; Martins, L. Environmental risks associated with falls on sidewalks: A systematic review. In Proceedings of the Occupational Safety and Hygiene V: Selected Papers from the International Symposium on Occupational Safety and Hygiene (SHO 2017), Guimarães, Portugal, 10–11 April 2017; CRC Press: Boca Raton, FL, USA, 2017; p. 341. [Google Scholar]
- Gaspar, P.L.; de Brito, J. Quantifying environmental effects on cement-rendered facades: A comparison between different degradation indicators. Build. Environ. 2008, 43, 1818–1828. [Google Scholar] [CrossRef]
- Moghtadernejad, S.; Mirza, S. Performance of Building Facades, 4th Structural Specialty; Canadian Society for Civil Engineers (CSCE): Halifax, NS, Canada, 2014. [Google Scholar]
- Madureira, S.; Flores-Colen, I.; de Brito, J.; Pereira, C. Maintenance planning of facades in current buildings. Constr. Build. Mater. 2017, 147, 790–802. [Google Scholar] [CrossRef]
- Ruiz, F.; Aguado, A.; Serrat, C.; Casas, J.R. Condition assessment of building façades based on hazard to people. Struct. Infrastruct. Eng. 2019, 15, 1346–1365. [Google Scholar] [CrossRef]
- Yau, Y.; Ho, D.C.W.; Chau, K.W. Determinants of the safety performance of private multi-storey residential buildings in Hong Kong. Soc. Indic. Res. 2008, 89, 501–521. [Google Scholar] [CrossRef]
- Tezcan, S.S.; Bal, I.E.; Gulay, F.G. P25 scoring method for the collapse vulnerability assessment of R/C buildings. J. Chin. Inst. Eng. 2011, 34, 769–781. [Google Scholar] [CrossRef]
- Mandeli, K. Public space and the challenge of urban transformation in cities of emerging economies: Jeddah case study. Cities 2019, 95, 102409. [Google Scholar] [CrossRef]
- Agency, F.E.M. Rapid Visual Screening of Buildings for Potential Seismic Hazards: A Handbook; Government Printing Office: Washington, DC, USA, 2017. [Google Scholar]
- Lohman, H.L.; Byers-Connon, S.; Padilla, R. Occupational Therapy with Elders: Strategies for the COTA; Elsevier: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Russell, A.; Van Teijlingen, E.; Lambert, H.; Stacy, R. Social and behavioural science education in UK medical schools: Current practice and future directions. Med. Educ. 2004, 38, 409–417. [Google Scholar] [CrossRef]
- Petermann, M.; Erdly, J. How Safe Are Building Facades? ASTM Stand. News 2003, 31, 24–27. [Google Scholar]
- Smith, H. Forget the Parthenon: How austerity is laying waste to Athens’ modern heritage’. Guardian 2017, 12, 2017. [Google Scholar]
- Carlson, C.; Aytur, S.; Gardner, K.; Rogers, S. Complexity in built environment, health, and destination walking: A neighborhood-scale analysis. J. Urban Health 2012, 89, 270–284. [Google Scholar] [CrossRef]
- Cinderby, S.; Cambridge, H.; Attuyer, K.; Bevan, M.; Croucher, K.; Gilroy, R.; Swallow, D. Co-designing urban living solutions to improve older People’s mobility and well-being. J. Urban Health 2018, 95, 409–422. [Google Scholar] [CrossRef]
- Sohn, E.K.; Stein, L.J.; Wolpoff, A.; Lindberg, R.; Baum, A.; McInnis-Simoncelli, A.; Pollack, K.M. Avenues of influence: The relationship between health impact assessment and determinants of health and health equity. J. Urban Health 2018, 95, 754–764. [Google Scholar] [CrossRef]
- Carmona, M. London’s local high streets: The problems, potential and complexities of mixed street corridors. Prog. Plan. 2015, 100, 1–84. [Google Scholar] [CrossRef]
- Moniruzzaman, M.; Páez, A. A model-based approach to select case sites for walkability audits. Health Place 2012, 18, 1323–1334. [Google Scholar] [CrossRef]
- Anonymous. Hatzidakis: About 9500 Dilapidated Buildings in the Country—His Direct Institutional Interventions. Available online: https://www.iefimerida.gr/ellada/hatzidakis-9500-etoimorropa-parembaseis-ypen (accessed on 16 January 2021).
- Alexandris, A.; Protopapa, E.; Psycharis, I. Collapse mechanisms of masonry buildings derived by the distinct element method. In Proceedings of the 13th World Conference on Earthquake Engineering, Vancouver, BC, Canada, 1–6 August 2004; p. 60. [Google Scholar]
- Carmichael, L.; Prestwood, E.; Marsh, R.; Ige, J.; Williams, B.; Pilkington, P.; Eaton, E.; Michalec, A. Healthy buildings for a healthy city: Is the public health evidence base informing current building policies? Sci. Total Environ. 2020, 719, 137146. [Google Scholar] [CrossRef]
- Johnston, J. Brussels Forces Public Sale of Building after 10 Years of Vacancy. The Brussels Times. 2019. Available online: https://www.brusselstimes.com/brussels/54851/brussels-forces-public-sale-of-building-after-10-years-or-vacancy/ (accessed on 10 January 2021).
- Halonen, J.I.; Pulakka, A.; Pentti, J.; Kallio, M.; Koskela, S.; Kivimäki, M.; Kawachi, I.; Vahtera, J.; Stenholm, S. Cross-sectional associations of neighbourhood socioeconomic disadvantage and greenness with accelerometer-measured leisure-time physical activity in a cohort of ageing workers. BMJ Open 2020, 10, e038673. [Google Scholar] [CrossRef]
- Mao, Q.; Wang, L.; Guo, Q.; Li, Y.; Liu, M.; Xu, G. Evaluating cultural ecosystem services of urban residential green spaces from the perspective of residents’ satisfaction with green space. Front. Public Health 2020, 8, 226. [Google Scholar] [CrossRef]
- Nordh, H.; Østby, K. Pocket parks for people—A study of park design and use. Urban For. Urban Green. 2013, 12, 12–17. [Google Scholar] [CrossRef]
- Bourdakis, E. Low Temperature Heating and High Temperature Cooling Systems Using Phase Change Materials for New Buildings and Energy Renovation of Existing Buildings; Technical University of Denmark: Lyngby, Denmark, 2018. [Google Scholar]
- Anonymous. Recording and Promotion of the 19th and 20th Century’s Buildings in Athens, 2013–2015 Act Report. Available online: https://www.monumenta.org/article.php?IssueID=4&perm=1&ArticleID=1024&CategoryID=23&lang=en (accessed on 8 October 2020).
- De Smith, M.J.; Goodchild, M.F.; Longley, P. Geospatial Analysis: A Comprehensive Guide to Principles, Techniques and Software Tools; Troubador Publishing Ltd.: Leicester, UK, 2007. [Google Scholar]
- Brunauer, W.A.; Lang, S.; Wechselberger, P.; Bienert, S. Additive hedonic regression models with spatial scaling factors: An application for rents in Vienna. J. Real Estate Financ. Econ. 2010, 41, 390–411. [Google Scholar] [CrossRef]
- Chowdhury, R.; Ramond, A.; O’Keeffe, L.M.; Shahzad, S.; Kunutsor, S.K.; Muka, T.; Gregson, J.; Willeit, P.; Warnakula, S.; Khan, H. Environmental toxic metal contaminants and risk of cardiovascular disease: Systematic review and meta-analysis. BMJ 2018, 362, k3310. [Google Scholar] [CrossRef] [PubMed]
- Young, A.F.; Russell, A.; Powers, J.R. The sense of belonging to a neighbourhood: Can it be measured and is it related to health and well being in older women? Soc. Sci. Med. 2004, 59, 2627–2637. [Google Scholar] [CrossRef] [PubMed]
- Higgs, C.; Badland, H.; Simons, K.; Knibbs, L.D.; Giles-Corti, B. The Urban Liveability Index: Developing a policy-relevant urban liveability composite measure and evaluating associations with transport mode choice. Int. J. Health Geogr. 2019, 18, 14. [Google Scholar] [CrossRef] [PubMed]
- Giles-Corti, B.; Zapata-Diomedi, B.; Jafari, A.; Both, A.; Gunn, L. Could smart research ensure healthy people in disrupted cities? J. Transp. Health 2020, 19, 100931. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Cassarino, M.; Setti, A. Environment as ‘Brain Training’: A review of geographical and physical environmental influences on cognitive ageing. Ageing Res. Rev. 2015, 23, 167–182. [Google Scholar] [CrossRef]
- Lombardi, D.; Uslu, B.; Bailey, J.M. Extreme Weather Events and the Climate Crisis: What is the Connection? Earth Sci. 2020, 36, 22–26. [Google Scholar]
- Ståhl, T. Health in All Policies: Prospects and Potentials; Ministry of Social Affairs and Health: Helsinki, Finland, 2006. [Google Scholar]
- Corburn, J.; Curl, S.; Arredondo, G.; Malagon, J. Health in all urban policy: City services through the prism of health. J. Urban Health 2014, 91, 623–636. [Google Scholar] [CrossRef]
- Stuart, E.; Wismar, M.; Ollila, E.; Lahtinen, E.; Leppo, K.; Samman, E. Defining leave no one behind. In Briefing Paper; Overseas Development Institute: London, UK, 2017; Available online: www.odi.org/sites/odi.org.uk/files/resource-documents/11809.pdf (accessed on 8 January 2021).
- Learmonth, A.; Curtis, S. Place shaping to create health and wellbeing using health impact assessment: Health geography applied to develop evidence-based practice. Health Place 2013, 24, 20–22. [Google Scholar] [CrossRef]
- Tsouros, A. City leadership for health and well-being: Back to the future. J. Urban Health 2013, 90, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Tsouros, A. City leadership for health and sustainable development: The World Health Organization European healthy cities network. Health Promot. Int. 2009, 24, i4–i10. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Colantoni, A.; Grigoriadis, E.; Sateriano, A.; Venanzoni, G.; Salvati, L. Cities as selective land predators? A lesson on urban growth, deregulated planning and sprawl containment. Sci. Total Environ. 2016, 545, 329–339. [Google Scholar] [CrossRef] [PubMed]
- Coccossis, H.; Delladetsimas, P.-M.; Katsigianni, X. Disaster Recovery Practices and Resilience Building in Greece. Urban Sci. 2021, 5, 28. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Falling buildings or pieces |
|---|
| Pieces of loose balconies |
| Pieces from long-term uncontrolled tubes used to remove throwing bass in dangerous constructions, which remained unattended and unchecked for years |
| Hanging pots outside balconies (risk of falling). |
| Rotten railings of balconies |
| Various pending accessories (advertisements, signs, hovering light bulbs, or hovering windows) from dilapidated buildings |
| Hovering air conditioners that are near-collapse and placed on the outside of windows, without maintaining any kind of fastening |
| TV antennas |
| TV antennas not fixed to the roof rails |
| No application of the concept of one antenna for the whole building → Indirect results for e-waste oft-exploited by Roma populations—collectors, when the rusty material is placed in the garbage around these buildings |
| No standard fastening of antennas against wind pressures, even though, for example, the air is often strong on the rooves of six-story buildings |
| No care for technical services for the maintenance of antennas |
| Metal mounting rods often become rusty |
| Falls on the same level |
| Poor construction and maintenance of sidewalks Great delay in repair No standardization of constructions with specific objectives (e.g., nonslippery surfaces, duration of construction, ease of repair and maintenance) |
| Slippery ground (unsuitable tiles) |
| Water dripping from balconies (when cleaned), pots (when watered), or attached air conditioners |
| Raised tiles posing great danger for falls due to poor fastening, destruction by car parking or by continuously expanding tree roots |
| Fecal samples from pets that cause sliding |
| Remains of metal poles after their removal by the police |
| Car parking barriers |
Illegally parked motorcycles
|
| Garbage (trash bags)—Abandoned glass or furniture |
| Tree pits |
| Presence of exhibited goods in the road (urban markets) |
| Tables from coffee shops & restaurants |
| Theft of tops of water system counters (where metal is used in old metal trade) causing holes in the sidewalks (with no action from the police) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mentis, A.-F.A.; Papadopulos, J.S. Near-Collapse Buildings and Unsafe Sidewalks as Neglected Urban & Public Health Issue: A Qualitative Study. Urban Sci. 2021, 5, 47. https://doi.org/10.3390/urbansci5020047
Mentis A-FA, Papadopulos JS. Near-Collapse Buildings and Unsafe Sidewalks as Neglected Urban & Public Health Issue: A Qualitative Study. Urban Science. 2021; 5(2):47. https://doi.org/10.3390/urbansci5020047
Chicago/Turabian StyleMentis, Alexios-Fotios A., and Jannis S. Papadopulos. 2021. "Near-Collapse Buildings and Unsafe Sidewalks as Neglected Urban & Public Health Issue: A Qualitative Study" Urban Science 5, no. 2: 47. https://doi.org/10.3390/urbansci5020047
APA StyleMentis, A.-F. A., & Papadopulos, J. S. (2021). Near-Collapse Buildings and Unsafe Sidewalks as Neglected Urban & Public Health Issue: A Qualitative Study. Urban Science, 5(2), 47. https://doi.org/10.3390/urbansci5020047