Choroidal Thickness in Correlation with Axial Length and Myopia Degree


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
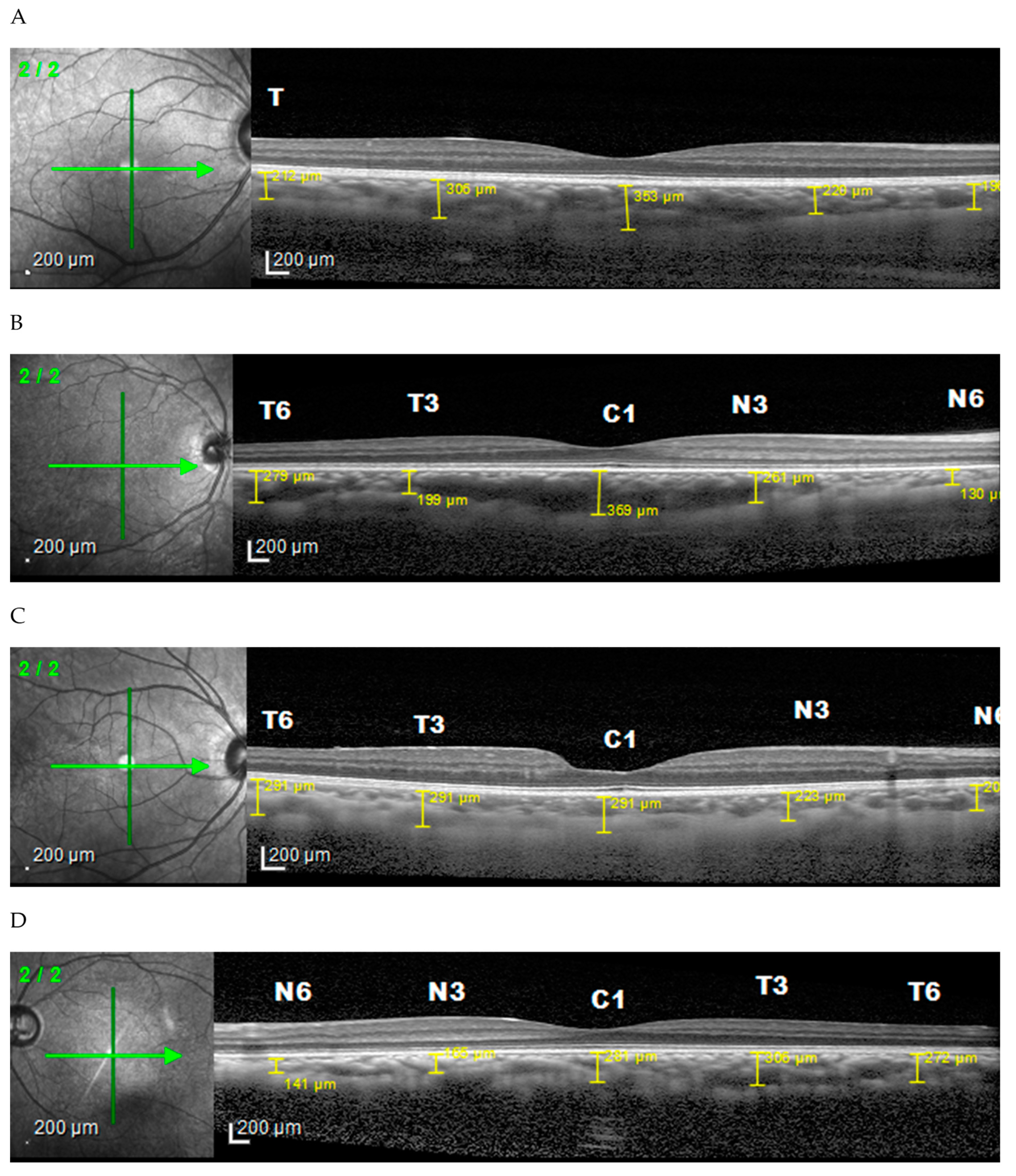
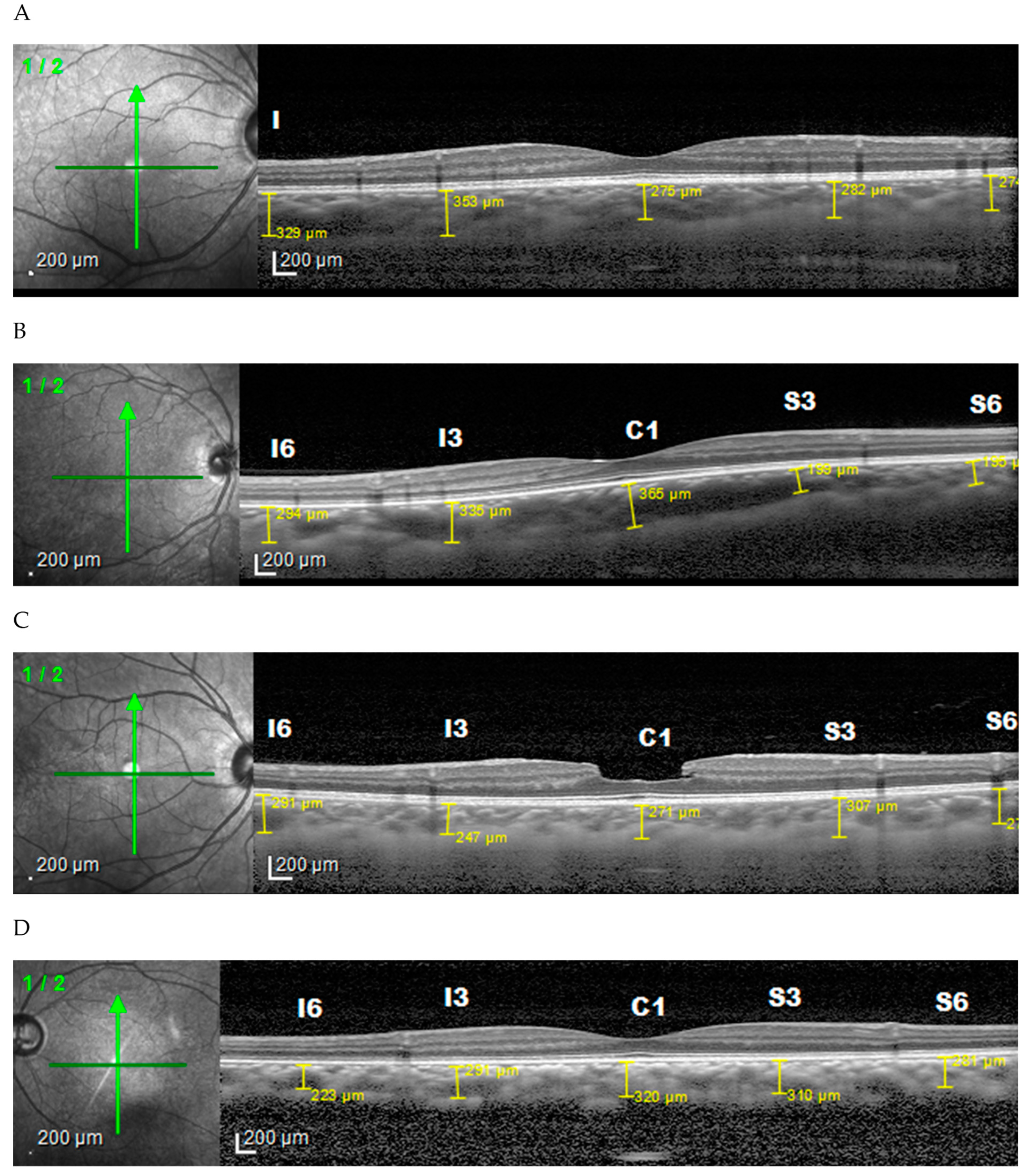
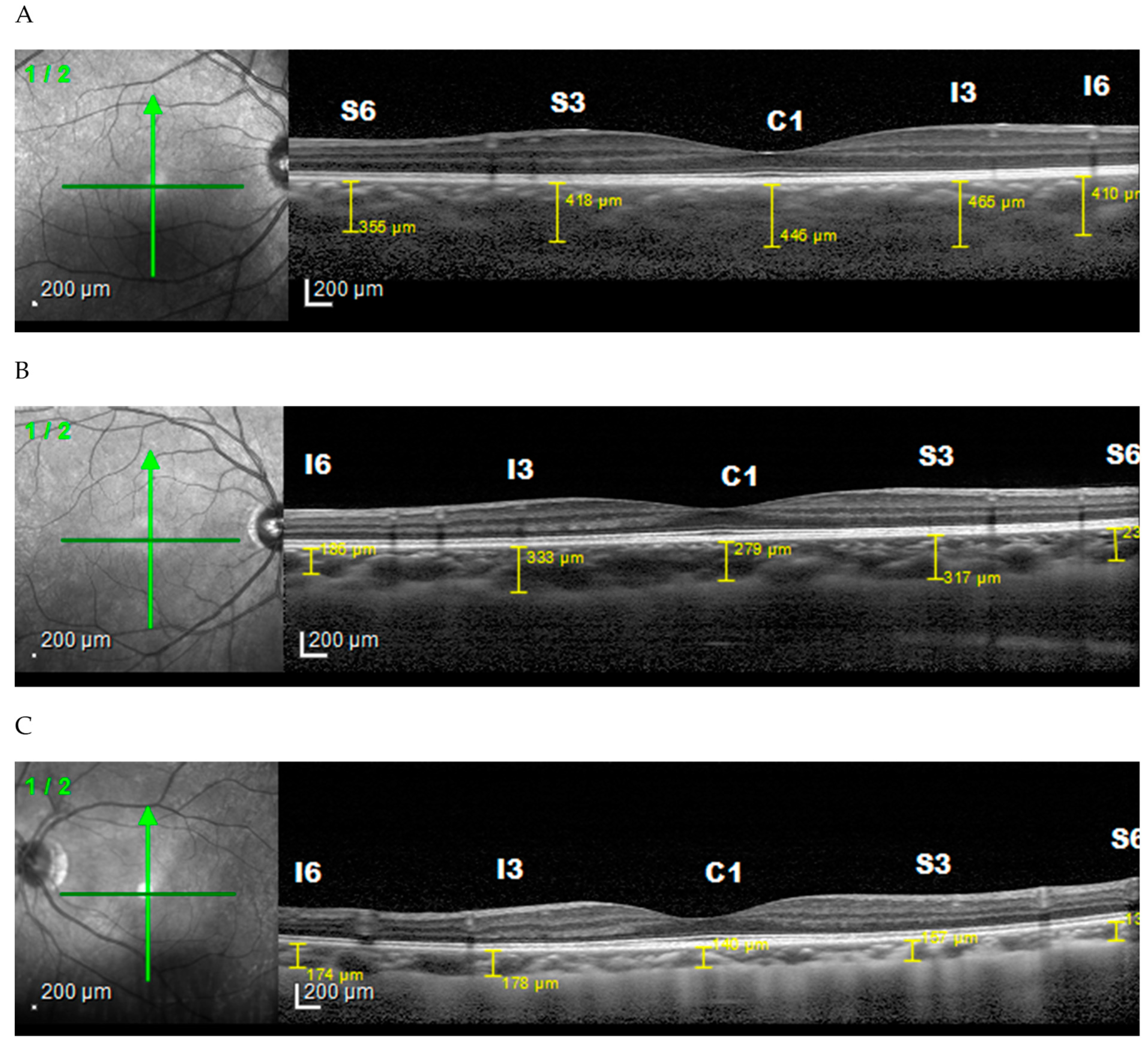
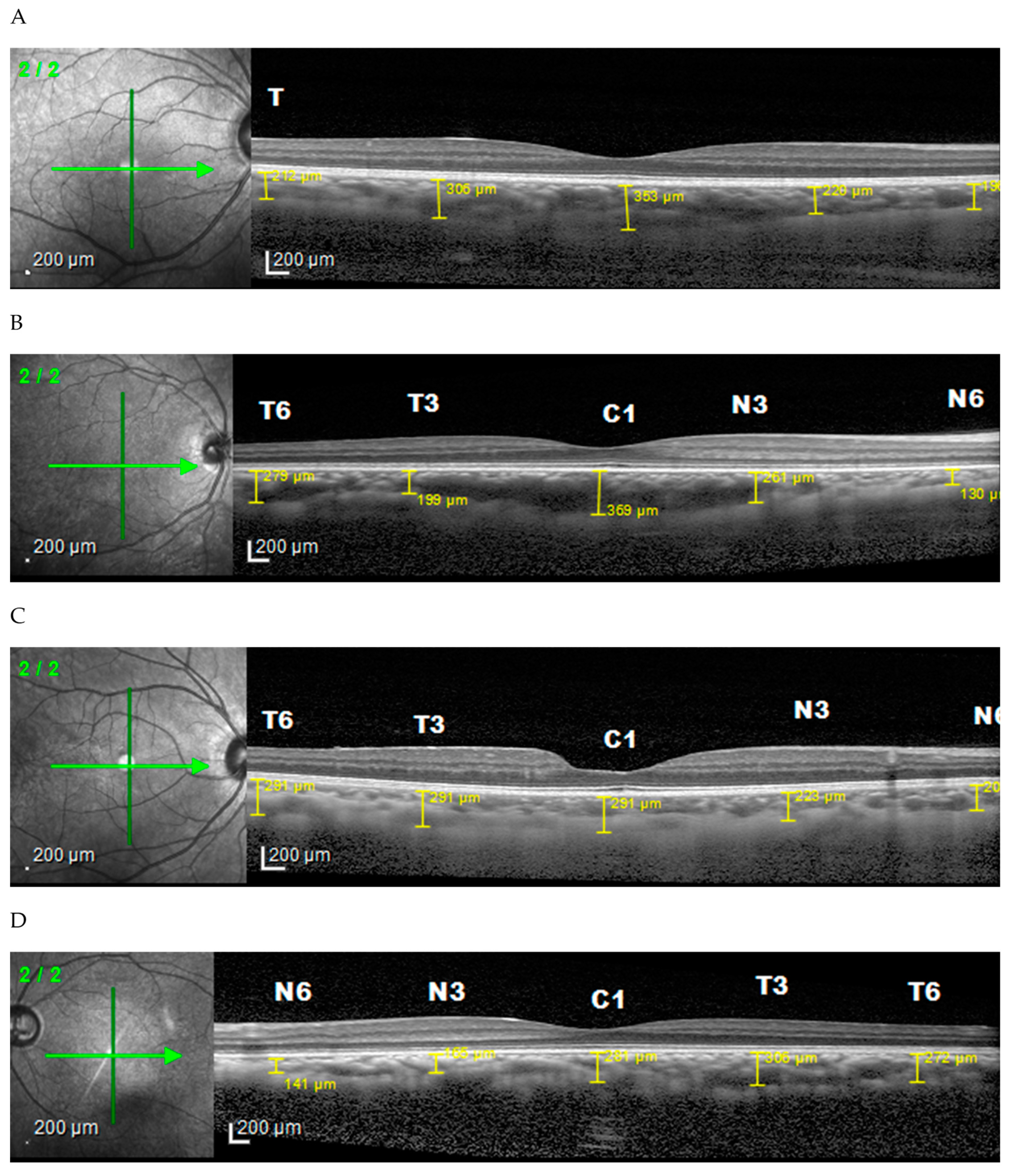
2.2. Ophthalmology Examination
2.3. Data Analysis and Interpretation
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kaur, K.; Gurnani, B.; Kannusamy, V. Myopia: Current concepts and review of literature. TNOA J. Ophthalmic Sci. Res. 2020, 58, 280. [Google Scholar] [CrossRef]
- Holden, B.A.; Fricke, T.R.; Wilson, D.A.; Jong, M.; Naidoo, K.S.; Sankaridurg, P.; Wong, T.Y.; Naduvilath, T.J.; Resnikoff, S. Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. Ophthalmology 2016, 123, 1036–1042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, J.; Tkatchenko, A.V. A Review of Current Concepts of the Etiology and Treatment of Myopia. Eye Contact Lens 2018, 44, 231–247. [Google Scholar] [CrossRef] [PubMed]
- Fredrick, D.R. Myopia. Br. Med. J. 2002, 324, 1195–1199. [Google Scholar] [CrossRef]
- Kaiti, R.; Shyangbo, R.; Sharma, I.P.; Dahal, M. Review on current concepts of myopia and its control strategies. Int. J. Ophthalmol. 2021, 14, 606–615. [Google Scholar] [CrossRef]
- Okafor, F.C.M.; Okoye, O.I.; Eze, B.I. Myopia: A Review of Literature Aetiology Progression of Myopia. Niger. J. Med. 2009, 18, 134–138. [Google Scholar]
- Meng, W.; Butterworth, J.; Malecaze, F.; Calvas, P. Axial length of myopia: A review of current research. Ophthalmologica 2011, 225, 127–134. [Google Scholar] [CrossRef]
- Pugazhendhi, S.; Ambati, B.; Hunter, A.A. Pathogenesis and prevention of worsening axial elongation in pathological myopia. Clin. Ophthalmol. 2020, 14, 853–873. [Google Scholar] [CrossRef] [Green Version]
- Yotsukura, E.; Torii, H.; Ozawa, H.; Hida, R.Y.; Shiraishi, T.; Teixeira, I.C.; Rautha, Y.V.B.L.; Do Nascimento, C.F.M.; Mori, K.; Uchino, M.; et al. Axial length and prevalence of myopia among schoolchildren in the equatorial region of brazil. J. Clin. Med. 2021, 10, 115. [Google Scholar] [CrossRef]
- Teberik, K.; Kaya, M. Retinal and Choroidal Thickness in Patients with High Myopia without Maculopathy. Ocul. Immunol. Inflamm. 2017, 25, 1438–1439. [Google Scholar] [CrossRef]
- Lee, G.Y.; Yu, S.; Kang, H.G.; Kim, J.S.; Lee, K.W.; Lee, J.-H. Choroidal Thickness Variation According to Refractive Error Measured by Spectral Domain-optical Coherence Tomography in Korean Children. Korean J. Ophthalmol. 2017, 31, 151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jin, P.; Zou, H.; Zhu, J.; Xu, X.; Jin, J.; Chang, T.C.; Lu, L.; Yuan, H.; Sun, S.; Yan, B.; et al. Choroidal and Retinal Thickness in Children with Different Refractive Status Measured by Swept-Source Optical Coherence Tomography. Am. J. Ophthalmol. 2016, 168, 164–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujiwara, T.; Imamura, Y.; Margolis, R.; Slakter, J.S.; Spaide, R.F. Enhanced Depth Imaging Optical Coherence Tomography of the Choroid in Highly Myopic Eyes. Am. J. Ophthalmol. 2009, 148, 445–450. [Google Scholar] [CrossRef]
- Wang, S.; Wang, Y.; Gao, X.; Qian, N.; Zhuo, Y. Choroidal thickness and high myopia: A cross-sectional study and meta-analysis Retina. BMC Ophthalmol. 2015, 15, 70. [Google Scholar] [CrossRef] [Green Version]
- Shin, J.W.; Shin, Y.U.; Cho, H.Y.; Lee, B.R. Measurement of choroidal thickness in normal eyes using 3D OCT-1000 spectral domain optical coherence tomography. Korean J. Ophthalmol. 2012, 26, 255–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiong, S.; He, X.; Zhang, B.; Deng, J.; Wang, J.; Lv, M.; Zhu, J.; Zou, H.; Xu, X. Changes in Choroidal Thickness Varied by Age and Refraction in Children and Adolescents: A 1-Year Longitudinal Study. Am. J. Ophthalmol. 2020, 213, 46–56. [Google Scholar] [CrossRef]
- El-Shazly, A.A.; Farweez, Y.A.; Elsebaay, M.E.; El-Zawahry, W.M.A. Correlation between choroidal thickness and degree of myopia assessed with enhanced depth imaging optical coherence tomography. Eur. J. Ophthalmol. 2017, 27, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Deng, J.; Li, X.; Jin, J.; Zhang, B.; Zhu, J.; Zou, H.; Xu, X.; Xie, J.; Wang, L.; Zhu, S.; et al. Distribution Pattern of Choroidal Thickness at the Posterior Pole in Chinese Children With Myopia. Investig. Ophthalmol. Vis. Sci. 2018, 59, 1577–1586. [Google Scholar] [CrossRef]
- Lee, M.W.; Lee, S.E.; Lim, H.B.; Kim, J.Y. Longitudinal changes in axial length in high myopia: A 4-year prospective study. Br. J. Ophthalmol. 2020, 104, 600–603. [Google Scholar] [CrossRef]
- Karahan, E.; Zengin, M.O.; Tuncer, I. Correlation of choroidal thickness with outer and inner retinal layers. Ophthalmic Surg. Lasers Imaging 2013, 44, 544–548. [Google Scholar] [CrossRef]
- Lin, T.N.; Yang, Y.; Lin, J.H.; Zhang, J.H.; Wen, Q.; He, X.L.; Chen, G. A comparative study of macular and choroidal thickness and blood-flow parameters in patients with intermediate and simple juvenile moderate myopia. Int. J. Gen. Med. 2021, 14, 1343–1348. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
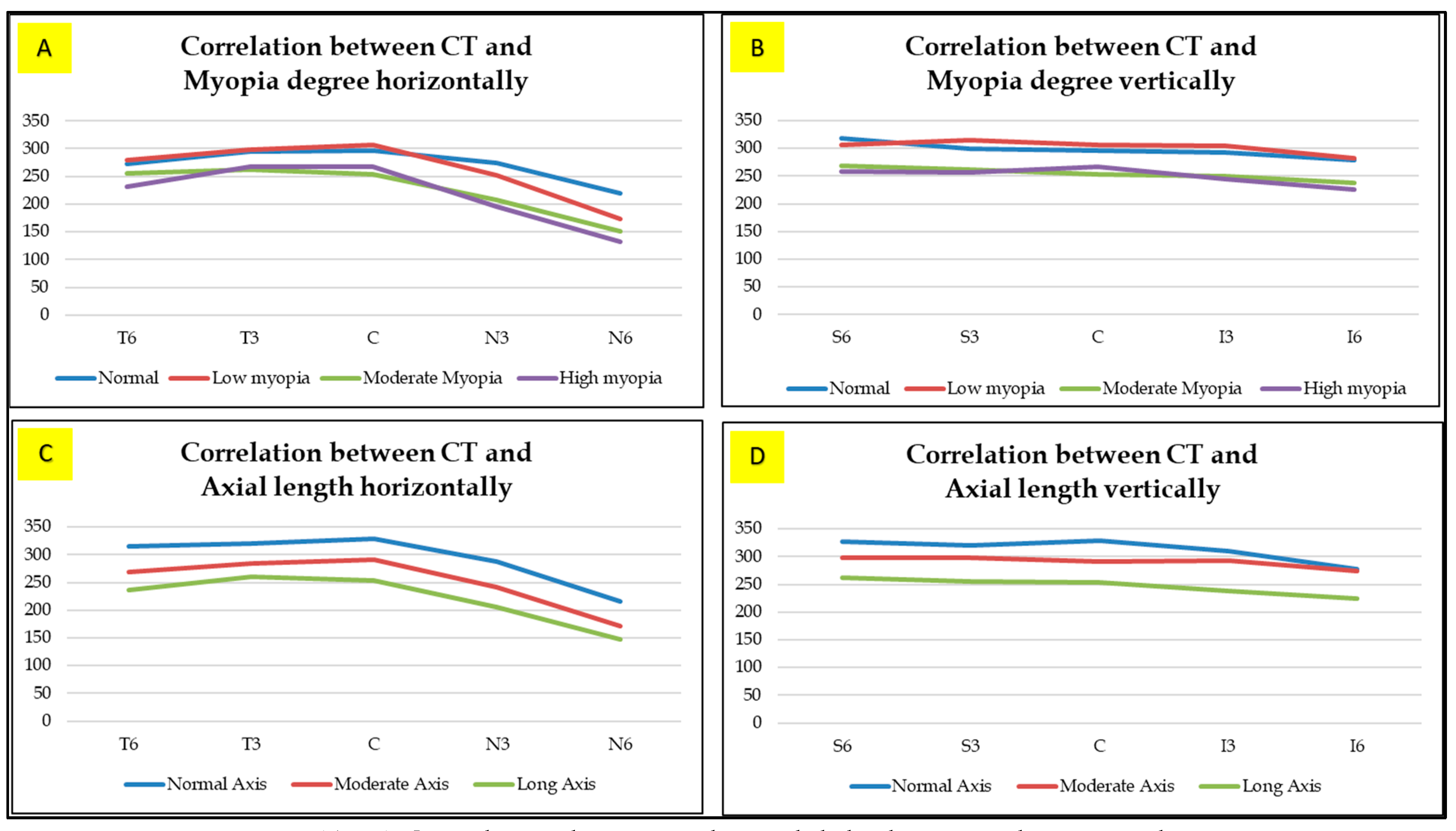
| Choroidal Thickness Based on Area (Mean ± SD) µm | Myopia Degree (D) | p * | |||
|---|---|---|---|---|---|
| Normal (n = 20) | Low Myopia (n = 50) | Moderate Myopia (n = 31) | High Myopia (n = 15) | ||
| C = Sub Fovea | 296.70 ± 69.62 | 307.52 ± 79.30 | 253.39 ± 64.84 | 267.33 ± 104.01 | 0.021 |
| T6 = Temporal 3 | 273.35 ± 46.82 | 280.22 ± 76.18 | 255.06 ± 47.20 | 231.07 ± 59.52 | 0.047 |
| T3 = Temporal 1.5 | 295.45 ± 66.94 | 298.12 ± 78.30 | 262.58 ± 54.02 | 267.80 ± 83.84 | 0.136 |
| N3 = Nasal 1.5 | 274.15 ± 71.70 | 252.50 ± 64.89 | 208.23 ± 48.70 | 196.07 ± 89.16 | 0.001 |
| N6 = Nasal 3 | 219.25 ± 77.72 | 173.00 ± 50.72 | 151.06 ± 47.20 | 132.33 ± 77.61 | 0.001 |
| S6 = Superior 3 | 319.90 ± 84.54 | 306.02 ± 72.50 | 269.13 ± 56.69 | 258.67 ± 89.28 | 0.039 |
| S3 = Superior 1.5 | 299.40 ± 76.45 | 314.18 ± 80.06 | 261.52 ± 52.95 | 257.73 ± 93.38 | 0.008 |
| I3 = Inferior 1.5 | 293.95 ± 77.33 | 307.12 ± 71.74 | 249.97 ± 62.72 | 244.73 ± 76.31 | 0.001 |
| I6 = Inferior 3 | 278.50 ± 86.19 | 282.04 ± 62.99 | 237.84 ± 47.31 | 226.00 ± 65.93 | 0.003 |
| Coroidal Thickness Based on Area (Mean ± SD) µm | Axial Length (mm) | p * | ||
|---|---|---|---|---|
| Normal (n = 6) | Moderate (n = 81) | Long (n = 29) | ||
| C = Sub Fovea | 329.50 ± 27.28 | 291.62 ± 76.94 | 253.28 ± 86.84 | 0.029 |
| T6 = Temporal 3 | 315.17 ± 75.89 | 269.99 ± 62.44 | 236.34 ± 55.72 | 0.006 |
| T3 = Temporal 1.5 | 320.00 ± 37.06 | 285.42 ± 71.87 | 261.76 ± 70.54 | 0.120 |
| N3 = Nasal 1.5 | 288.17 ± 42.97 | 241.38 ± 67.44 | 206.52 ± 71.63 | 0.010 |
| N6 = Nasal 3 | 216.83 ± 60.60 | 171.73 ± 60.47 | 147.93 ± 62.65 | 0.029 |
| S6 = Superior 3 | 327.00 ± 40.71 | 298.06 ± 78.31 | 262.45 ± 72.23 | 0.049 |
| S3 = Superior 1.5 | 320.83 ± 36.40 | 298.53 ± 76.42 | 256.14 ± 79.89 | 0.024 |
| I3 = Inferior 1.5 | 310.50 ± 45.47 | 293.37 ± 73.36 | 239.79 ± 68.67 | 0.002 |
| I6 = Inferior 3 | 278.33 ± 64.76 | 274.07 ± 67.91 | 225.48 ± 56.06 | 0.003 |
| Choroidal Thickness Based on Area (Mean ± SD) µm | Axial Length (mm) | Myopia Degree (D) | ||
|---|---|---|---|---|
| Coefficient Correlation (r) | p * | Coefficient Correlation (r) | p * | |
| C = Sub Fovea | −246 | 0.008 | −175 | 0.060 |
| T6 = Temporal 3 | −293 | 0.001 | −180 | 0.053 |
| T3 = Temporal 1.5 | −190 | 0.041 | −124 | 0.186 |
| N3 = Nasal 1.5 | −278 | 0.003 | −347 | <0.001 |
| N6 = Nasal 3 | −238 | 0.010 | −368 | <0.001 |
| S6 = Superior 3 | −288 | 0.014 | −248 | 0.007 |
| S3 = Superior 1.5 | −249 | 0.007 | −227 | 0.014 |
| I3 = Inferior 1.5 | −310 | 0.001 | −284 | 0.002 |
| I6 = Inferior 3 | −289 | 0.002 | −299 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muhiddin, H.S.; Mayasari, A.R.; Umar, B.T.; Sirajuddin, J.; Patellongi, I.; Islam, I.C.; Ichsan, A.M. Choroidal Thickness in Correlation with Axial Length and Myopia Degree. Vision 2022, 6, 16. https://doi.org/10.3390/vision6010016
Muhiddin HS, Mayasari AR, Umar BT, Sirajuddin J, Patellongi I, Islam IC, Ichsan AM. Choroidal Thickness in Correlation with Axial Length and Myopia Degree. Vision. 2022; 6(1):16. https://doi.org/10.3390/vision6010016
Chicago/Turabian StyleMuhiddin, Habibah Setyawati, Andi Ratna Mayasari, Batari Todja Umar, Junaedi Sirajuddin, Ilhamjaya Patellongi, Itzar Chaidir Islam, and Andi Muhammad Ichsan. 2022. "Choroidal Thickness in Correlation with Axial Length and Myopia Degree" Vision 6, no. 1: 16. https://doi.org/10.3390/vision6010016
APA StyleMuhiddin, H. S., Mayasari, A. R., Umar, B. T., Sirajuddin, J., Patellongi, I., Islam, I. C., & Ichsan, A. M. (2022). Choroidal Thickness in Correlation with Axial Length and Myopia Degree. Vision, 6(1), 16. https://doi.org/10.3390/vision6010016