Recent Advances of Computerized Graphical Methods for the Detection and Progress Assessment of Visual Distortion Caused by Macular Disorders



Abstract
1. Introduction
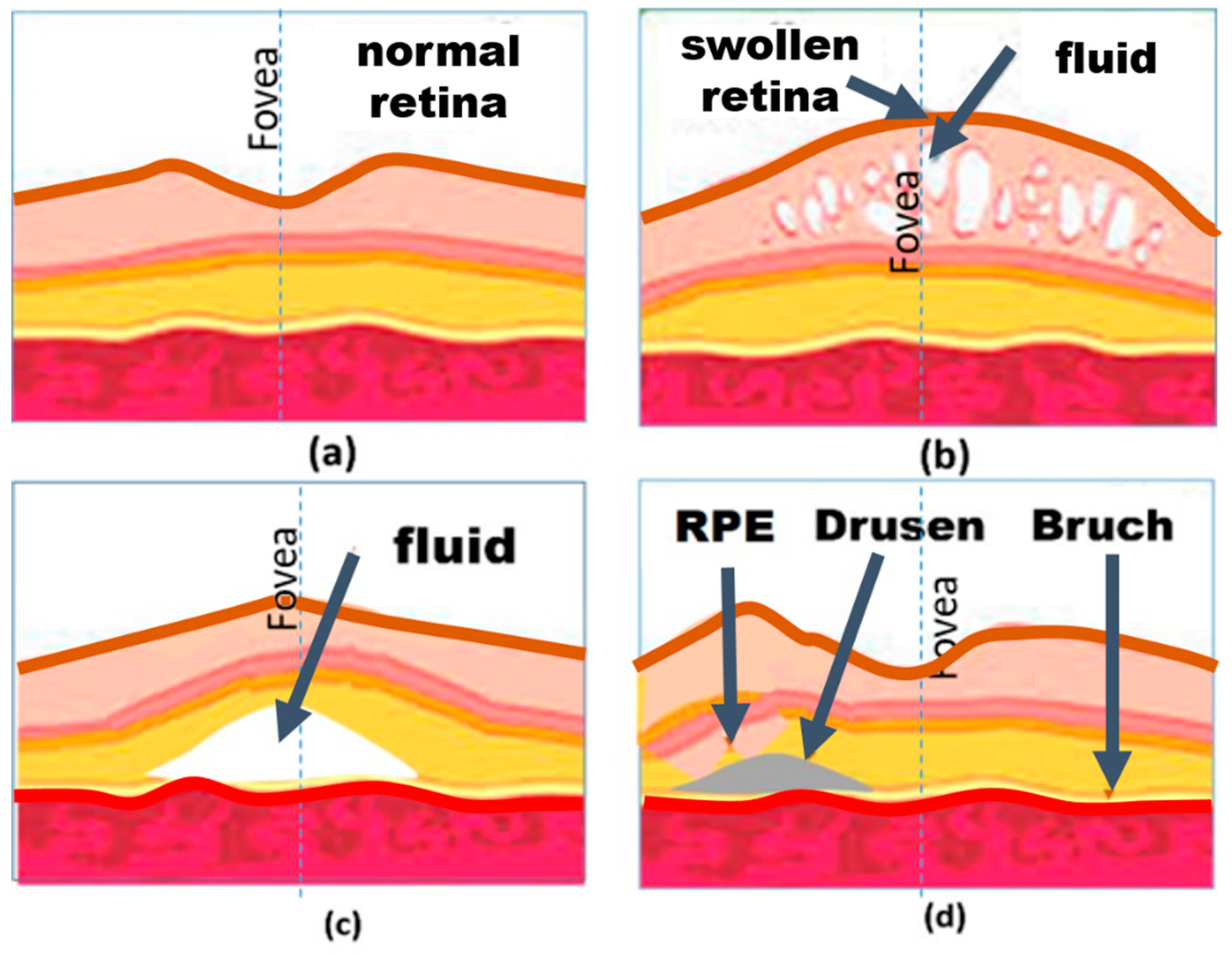
1.1. VD Caused by Macular Disorders
1.2. Related Macular Disorders
1.3. VD Assessment in Patients with Macular Disorders
2. Static VD Assessment Methods
2.1. Enhanced AG Tests
2.2. Threshold Amsler Grid Test
2.3. Accelerated Amsler Grid Test
2.4. Deformable Amsler Grid
2.5. NGRID VD Method
3. Dynamic VD Assessment Methods
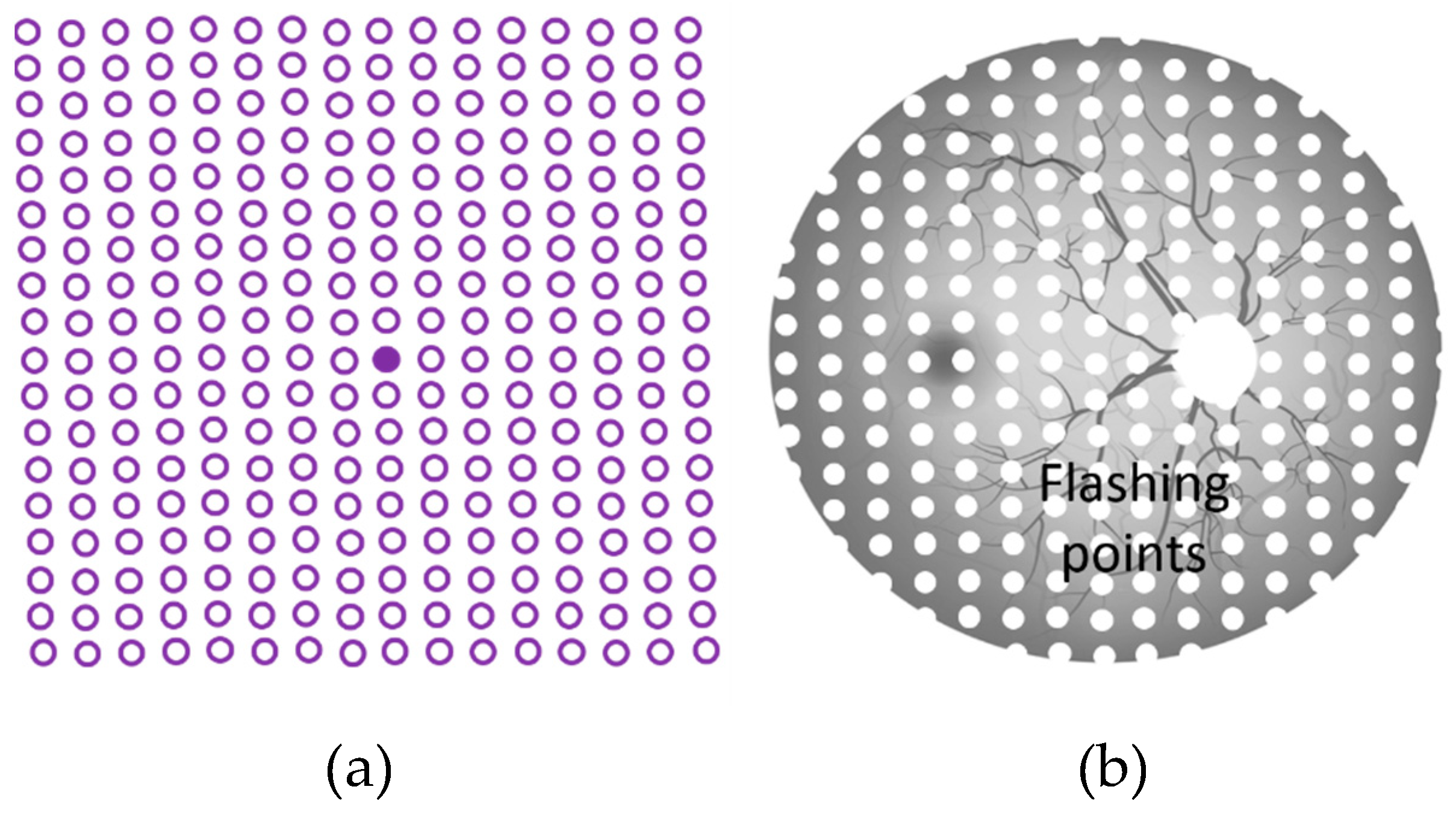
3.1. Preferential Hyperacuity Perimeter (PHP) Test
3.2. D-CTAG Test
3.3. Macular Computerized Psychophysical Test
3.4. M-CHART Score Test
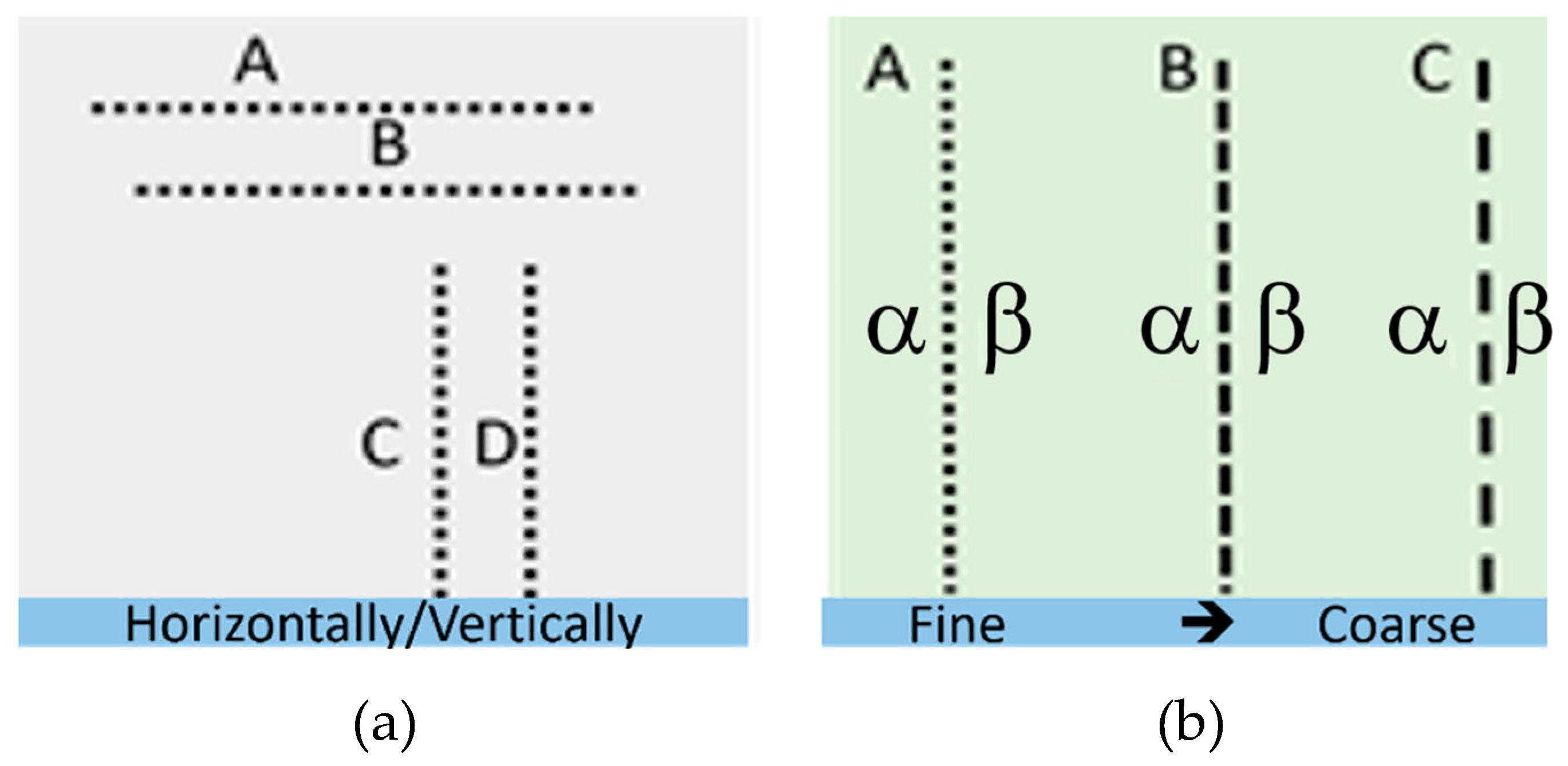
3.5. Shape Discrimination Test
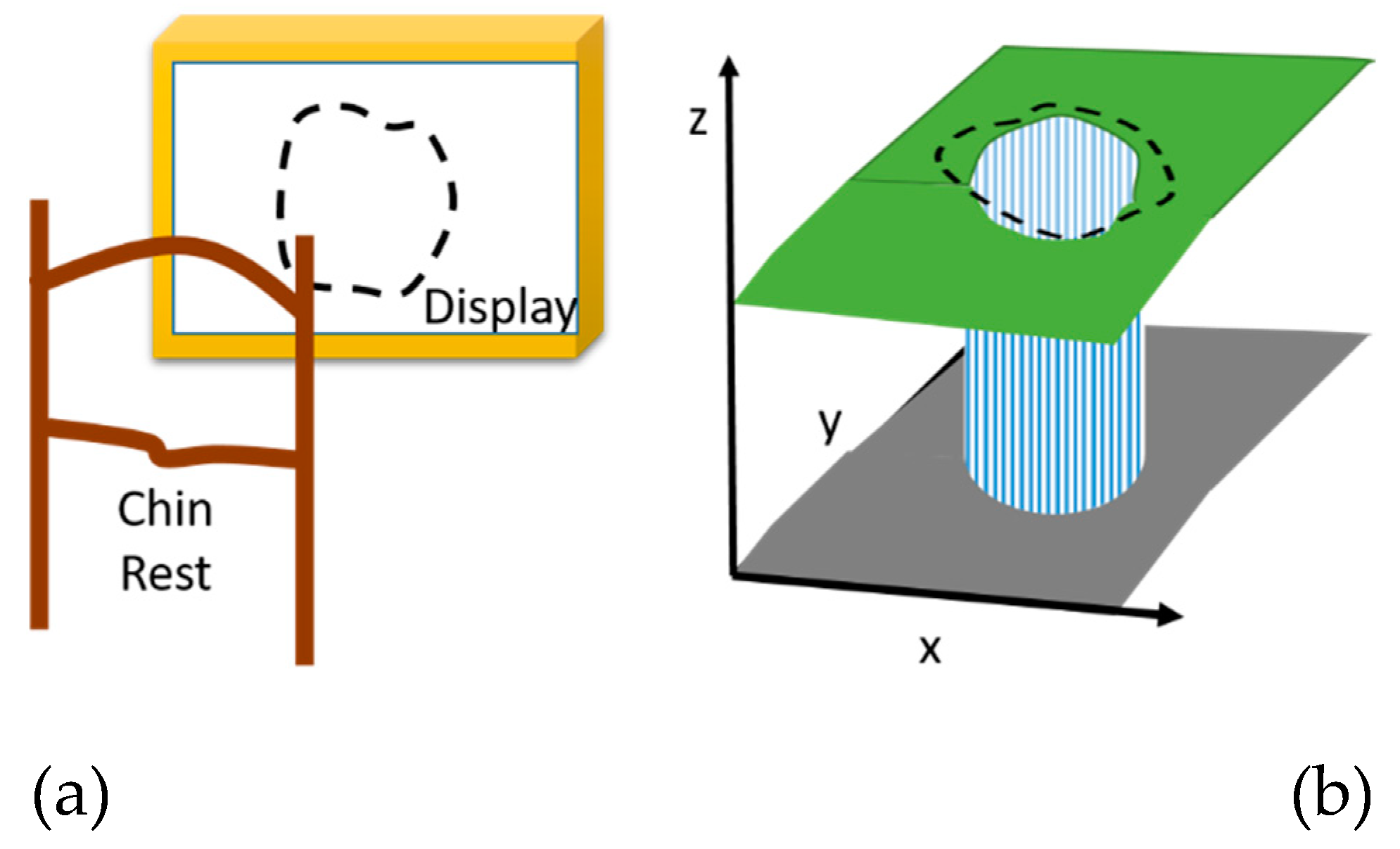
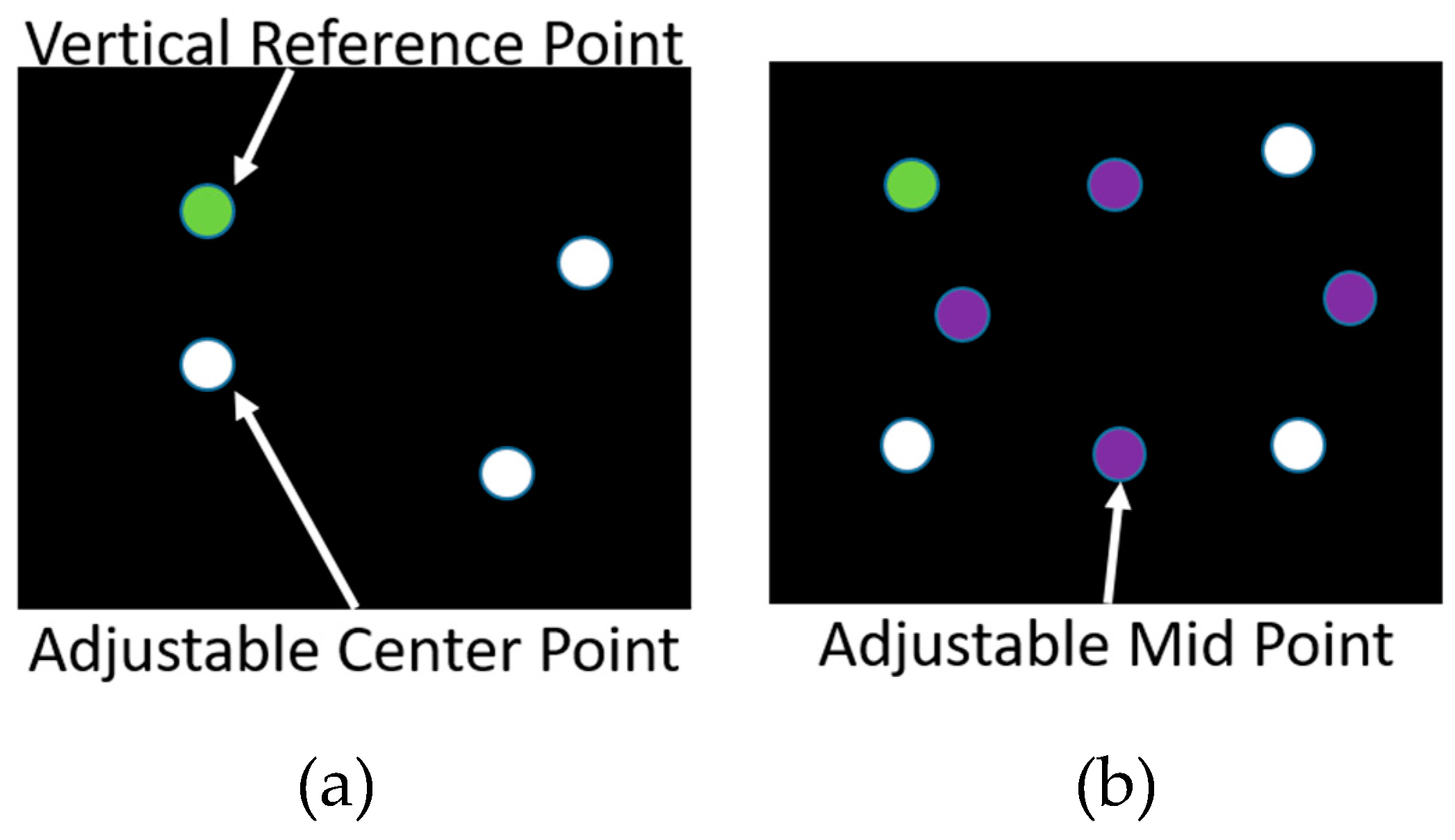
3.6. Positioning Techniques
4. Discussion
5. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- The Eye Diseases Prevalence Research Group, Prevalence of age-related macular degeneration in the United States. Arch. Ophthalmol. 2004, 122, 564–572. [CrossRef]
- Wang, M.; Munch, I.C.; Hasler, P.W.; Prünte, C.; Larsen, M. Central serous chorioretinopathy. Acta Ophthalmol. 2008, 86, 126–145. [Google Scholar] [CrossRef]
- Wong, W.L.; Su, X.; Li, X.; Cheung, C.M.G.; Klein, R.; Cheng, C.Y.; Wong, T.Y. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: A systematic review and meta-analysis. Lancet Glob. Health 2014, 2, e106–e116. [Google Scholar] [CrossRef]
- Taylor, D.J.; Hobby, A.E.; Binns, A.M.; Crabb, D.P. How does age-related macular degeneration affect real-world visual ability and quality of life? A systematic review. BMJ Open 2016, 6, e011504. [Google Scholar] [CrossRef]
- Bressler, N.M.; Bressler, S.B.; Fine, S.L. Age-related macular degeneration. Surv. Ophthalmol. 1988, 32, 375–413. [Google Scholar] [CrossRef]
- The Lancet. Age-related macular degeneration: Treatment at what cost? Lancet 2018, 392, 1090. [Google Scholar] [CrossRef]
- Busch, C.; Wakabayashi, T.; Sato, T.; Fukushima, Y.; Hara, C.; Shiraki, N.; Winegarner, A.; Nishida, K.; Sakaguchi, H.; Nishida, K. Retinal Microvasculature and Visual Acuity after Intravitreal Aflibercept in Diabetic Macular Edema: An Optical Coherence Tomography Angiography Study. Sci. Rep. 2019, 9, 1561. [Google Scholar] [CrossRef]
- Spaide, R.F.; Fujimoto, J.G.; Waheed, N.K.; Sadda, S.R.; Staurenghi, G. Optical coherence tomography angiography. Prog. Retin. Eye Res. 2018, 64, 1–55. [Google Scholar] [CrossRef]
- Rogers, A.H.; Duker, J.S. Retina; Elsevier: Philadelphia, PA, USA, 2008. [Google Scholar]
- Holz, F.G.; Spaide, R.F. Medical Retina: Focus on Retinal Imaging; Springer: New York, NY, USA, 2010. [Google Scholar]
- Midena, E.; Pilotto, E. Microperimetry in age: Related macular degeneration. Eye 2017, 31, 985. [Google Scholar] [CrossRef]
- Midena, E.; Vujosevic, S. Metamorphopsia: An Overlooked Visual Symptom. Ophthalmic Res. 2015, 55, 26–36. [Google Scholar] [CrossRef]
- Besharse, J.C.; Bok, D. The Retina and Its Disorders; Academic Pres: San Diego, CA, USA, 2011. [Google Scholar]
- Emerging Risk Factors Collaboration; Sarwar, N.; Gao, P.; Seshasai, S.R.; Gobin, R.; Kaptoge, S.; Di Angelantonio, E.; Ingelsson, E.; Lawlor, D.A.; Selvin, E.; et al. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: A collaborative meta-analysis of 102 prospective studies. Lancet 2010, 375, 2215–2222. [Google Scholar]
- Bourne, R.R.; Stevens, G.A.; White, R.A.; Smith, J.L.; Flaxman, S.R.; Price, H.; Jonas, J.B.; Keeffe, J.; Leasher, J.; Naidoo, K.; et al. Causes of vision loss worldwide, 1990–2010: A systematic analysis. Lancet Glob. Health 2013, 1, e339–e349. [Google Scholar] [CrossRef]
- Spaide, R.F.; Campeas, L.; Haas, A.; Yannuzzi, L.A.; Fisher, Y.L.; Guyer, D.R.; Slakter, J.S.; Sorenson, J.A.; Orlock, D.A. Central serous chorioretinopathy in younger and older adults. Ophthalmology 1996, 103, 2070–2079; discussion 2079–2080. [Google Scholar] [CrossRef]
- Peiris, T.J.; El Rami, H.E.; Sun, J.K. Central serous chorioretinopathy associated with steroid enema. Retin Cases Brief. Rep. 2018. [Google Scholar] [CrossRef]
- Schlote, T.; Grueb, M.; Mielke, J.; Rohrbach, J.M. Pocket Atlas of Ophthalmology; Georg Thieme Verlag Stuttgart: New York, NY, USA, 2011. [Google Scholar]
- Hogg, R.E.; Chakravarthy, U. Visual function and dysfunction in early and late age-related maculopathy. Prog. Retin. Eye Res. 2006, 25, 249–276. [Google Scholar] [CrossRef]
- Parmet, S.; Lynm, C.; Glass, R.M. Age-related macular degeneration. JAMA 2006, 295, 2438. [Google Scholar] [CrossRef]
- Plainis, S.; Tzatzala, P.; Orphanos, Y.; Tsilimbaris, M.K. A modified ETDRS visual acuity chart for European-wide use. Optom. Vis. Sci. 2007, 84, 647–653. [Google Scholar] [CrossRef]
- Springer, C.; Bültmann, S.; Völcker, H.E.; Rohrschneider, K. Fundus Perimetry with the Micro Perimeter 1 in Normal Individuals: Comparison with Conventional Threshold Perimetry. Ophthalmology 2005, 112, 848–854. [Google Scholar] [CrossRef]
- Ferris, F.L., III; Kassoff, A.; Bresnick, G.H.; Bailey, I. New visual acuity charts for clinical research. Am. J. Ophthalmol. 1982, 94, 91–96. [Google Scholar] [CrossRef]
- Falkenstein, I.A.; Cochran, D.E.; Azen, S.P.; Dustin, L.; Tammewar, A.M.; Kozak, I.; Freeman, W.R. Comparison of Visual Acuity in Macular Degeneration Patients Measured with Snellen and Early Treatment Diabetic Retinopathy Study Charts. Ophthalmology 2008, 115, 319–323. [Google Scholar] [CrossRef]
- Schuchard, R.A. Validity and Interpretation of Amsler Grid Reports. Arch. Ophthalmol. 1993, 111, 776–780. [Google Scholar] [CrossRef]
- Amsler, M. Earliest symptoms of diseases of the macula. Br. J. Ophthalmol. 1953, 37, 521. [Google Scholar] [CrossRef]
- Yoshimura, N. Oct-Atlas, 1st ed.; Springer: New York, NY, USA, 2013. [Google Scholar]
- Patel, P.J.; Chen, F.K.; Ikeji, F.; Xing, W.; Bunce, C.; Da Cruz, L.; Tufail, A. Repeatability of Stratus Optical Coherence Tomography Measures in Neovascular Age-Related Macular Degeneration. Investig. Opthalmol. Vis. Sci. 2008, 49, 1084. [Google Scholar] [CrossRef]
- Thomas, D.; Duguid, G. Optical coherence tomography—A review of the principles and contemporary uses in retinal investigation. Eye 2004, 18, 561–570. [Google Scholar] [CrossRef]
- Macular Degeneration|Lake Travis Eye & Laser Center. Available online: https://laketraviseyecenter.com/macular-degeneration/ (accessed on 20 February 2019).
- Trevino, R. Recent progress in macular function self-assessment. Ophthalmic Physiol. Opt. 2008, 28, 183–192. [Google Scholar] [CrossRef]
- Collazo, E. Portable Electronic Amsler Test. U.S. Patent US8047652B1, 1 November 2011. [Google Scholar]
- Hirji, R. Near Eye Opthalmic Device. U.S. Patent US20080309879, 18 December 2008. [Google Scholar]
- Roser, M.C. Visual and Memory Stimulating Retina Self-Monitoring System. U.S. Patent US7798645, 21 September 2010. [Google Scholar]
- Dowling, J.E. The Retina: An. Approachable Part of the Brain; Belknap Press of Harvard University Press: Cambridge, MA, USA, 1987. [Google Scholar]
- Sadun, A.A.; Wall, M. System and Method of Detecting Visual Field Defects. U.S. Patent US4818091, 4 April 1989. [Google Scholar]
- Fink, W.; Sadun, A.A. Three-dimensional computer-automated threshold Amsler grid test. J. Biomed. Opt. 2004, 9, 149–153. [Google Scholar] [CrossRef]
- Loewenstein, A.; Malach, R.; Goldstein, M.; Leibovitch, I.; Barak, A.; Baruch, E.; Alster, Y.; Rafaeli, O.; Avni, I.; Yassur, Y. Replacing the Amsler grid. Ophthalmology 2003, 110, 966–970. [Google Scholar] [CrossRef]
- Palanker, D. Metamorphopsia Testing and Related Methods. WO2014022850A1, 6 February 2014. [Google Scholar]
- Kohn, W.; Klingshirn, J.A. Characterization and Correction of Macular Distortion. U.S. Patent US8708495, 29 April 2014. [Google Scholar]
- Mohaghegh, N.; Zadeh, E.G.; Magierowski, S. Wearable diagnostic system for age-related macular degeneration. In Proceedings of the 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; IEEE: Piscataway, NJ, USA, 2016; pp. 6006–6009. [Google Scholar]
- Mohaghegh, N.; Ghafar-Zadeh, E.; Munidasa, S.; Magierowski, S. Toward Age-related Macular Degeneration (AMD) Big Data: Hardware and software design and implementation. In Proceedings of the IEEE 30th Canadian Conference on Electrical and Computer Engineering (CCECE), Windsor, ON, Canada, 30 April–3 May 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 1–4. [Google Scholar]
- Mohaghegh, N.; Munidasa, S.; Ziho, X.; Owen, Q.; Magierowski, S.; Ghafar-Zadeh, E. Age-Related Macular Degeneration Diagnostic Tools: Hardware and Software Development. In Proceedings of the IEEE 61st International Midwest Symposium on Circuits and Systems (MWSCAS), Windsor, ON, Canada, 30 April–3 May 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 721–724. [Google Scholar]
- Lakshminarayanan, V.; Enoch, J.M. Vernier acuity and aging. Int. Ophthalmol. 1995, 19, 109–115. [Google Scholar] [CrossRef]
- Kaas, J.H.; Krubitzer, L.A.; Chino, Y.M.; Langston, A.L.; Polley, E.H.; Blair, N. Reorganization of retinotopic cortical maps in adult mammals after lesions of the retina. Science 1990, 248, 229–231. [Google Scholar] [CrossRef]
- Loewenstein, A. The significance of early detection of age-related macular degeneration: Richard & Hinda Rosenthal Foundation lecture, The Macula Society 29th annual meeting. Retina 2007, 27, 873–878. [Google Scholar]
- Lai, Y.; Grattan, J.; Shi, Y.; Young, G.; Muldrew, A.; Chakravarthy, U. Functional and morphologic benefits in early detection of neovascular age-related macular degeneration using the preferential hyperacuity perimeter. Retina 2011, 31, 1620–1626. [Google Scholar] [CrossRef]
- Robison, C.D.; Jivrajka, R.V.; Bababeygy, S.R.; Fink, W.; Sadun, A.A.; Sebag, J. Distinguishing wet from dry age-related macular degeneration using three-dimensional computer-automated threshold Amsler grid testing. Br. J. Ophthalmol. 2011, 95, 1419–1423. [Google Scholar] [CrossRef]
- Loewenstein, A.; Pollack, A.; Schachat, A. Results of a Multicentered, Masked Clinical Trial to Evaluate the Macular Computerized Psychophysical Test (MCPT) for Detection of Age-related Macular Degeneration (AMD). Investig. Ophtalmol. Vis. Sci. 2002, 43, 1213. [Google Scholar]
- Arimura, E.; Matsumoto, C.; Nomoto, H.; Hashimoto, S.; Takada, S.; Okuyama, S.; Shimomura, Y. M-charts as a tool for quantifying metamorphopsia in age-related macular degeneration treated with the bevacizumab injections. BMC Ophthalmol. 2013, 13, 13. [Google Scholar]
- Inami Ltd. Quantitatable Metamorphopsia Chart. 31 October 2015. Available online: http://www.inami.co.jp/english/surgical_instruments/innovations/kdm1 (accessed on 31 October 2015).
- Arimura, E.; Matsumoto, C.; Nomoto, H.; Hashimoto, S.; Takada, S.; Okuyama, S.; Shimomura, Y. Correlations between M-CHARTS and PHP findings and subjective perception of metamorphopsia in patients with macular diseases. Investig. Ophtalmol. Vis. Sci. 2011, 52, 128–135. [Google Scholar] [CrossRef]
- Wang, Y.-Z.; Wilson, E.; Locke, K.G.; Edwards, A.O. Shape discrimination in age-related macular degeneration. Investig. Ophtalmol. Vis. Sci. 2002, 43, 2055–2062. [Google Scholar]
- Enoch, J.M.; Knowles, R.A. Method for Evaluating Metamorphopsia. U.S. Patent US4798456, 17 January 1989. [Google Scholar]
- Wiecek, E.; Lashkari, K.; Dakin, S.; Bex, P.J. Novel Quantitative Assessment of Metamorphopsia in Maculopathy. Investig. Ophtalmol. Vis. Sci. 2014, 56, 494–504. [Google Scholar] [CrossRef]
- Stewart, J.L. System and method for full field oscillating stimulus perimeter. U.S. Patent US6742894, 1 June 2004. [Google Scholar]
- Nazemi, P.P.; Fink, W.; Sadun, A.A.; Francis, B.; Minckler, D. Early detection of glaucoma by means of a novel 3D computer-automated visual field test. Br. J. Ophthalmol. 2007, 91, 1331–1336. [Google Scholar] [CrossRef][Green Version]
- Faes, L.; Bodmer, N.S.; Bachmann, L.M.; Thiel, M.A.; Schmid, M.K. Diagnostic accuracy of the Amsler grid and the preferential hyperacuity perimetry in the screening of patients with age-related macular degeneration: Systematic review and meta-analysis. Eye 2014, 28, 788–796. [Google Scholar] [CrossRef]
- Cocce, K.J.; Stinnett, S.S.; Luhmann, U.F.; Vajzovic, L.; Horne, A.; Schuman, S.G.; Toth, C.A.; Cousins, S.W.; Lad, E.M. Visual Function Metrics in Early and Intermediate Dry Age-related Macular Degeneration for Use as Clinical Trial Endpoints. Am. J. Ophthalmol. 2018, 189, 127–138. [Google Scholar] [CrossRef]
- Bennett, A.G.; Rabbetts, R.B. Proposals for new reduced and schematic eyes. Ophthalmic Physiol. Opt. 1989, 9, 228–230. [Google Scholar] [CrossRef]
- Kitzmann, A.S.; Pulido, J.S.; Diehl, N.N.; Hodge, D.O.; Burke, J.P. The incidence of central serous chorioretinopathy in Olmsted County, Minnesota, 1980–2002. Ophthalmology 2008, 115, 169–173. [Google Scholar] [CrossRef]
- Crossland, M.; Rubin, G. The Amsler chart: Absence of evidence is not evidence of absence. Br. J. Ophthalmol. 2007, 91, 391–393. [Google Scholar] [CrossRef]
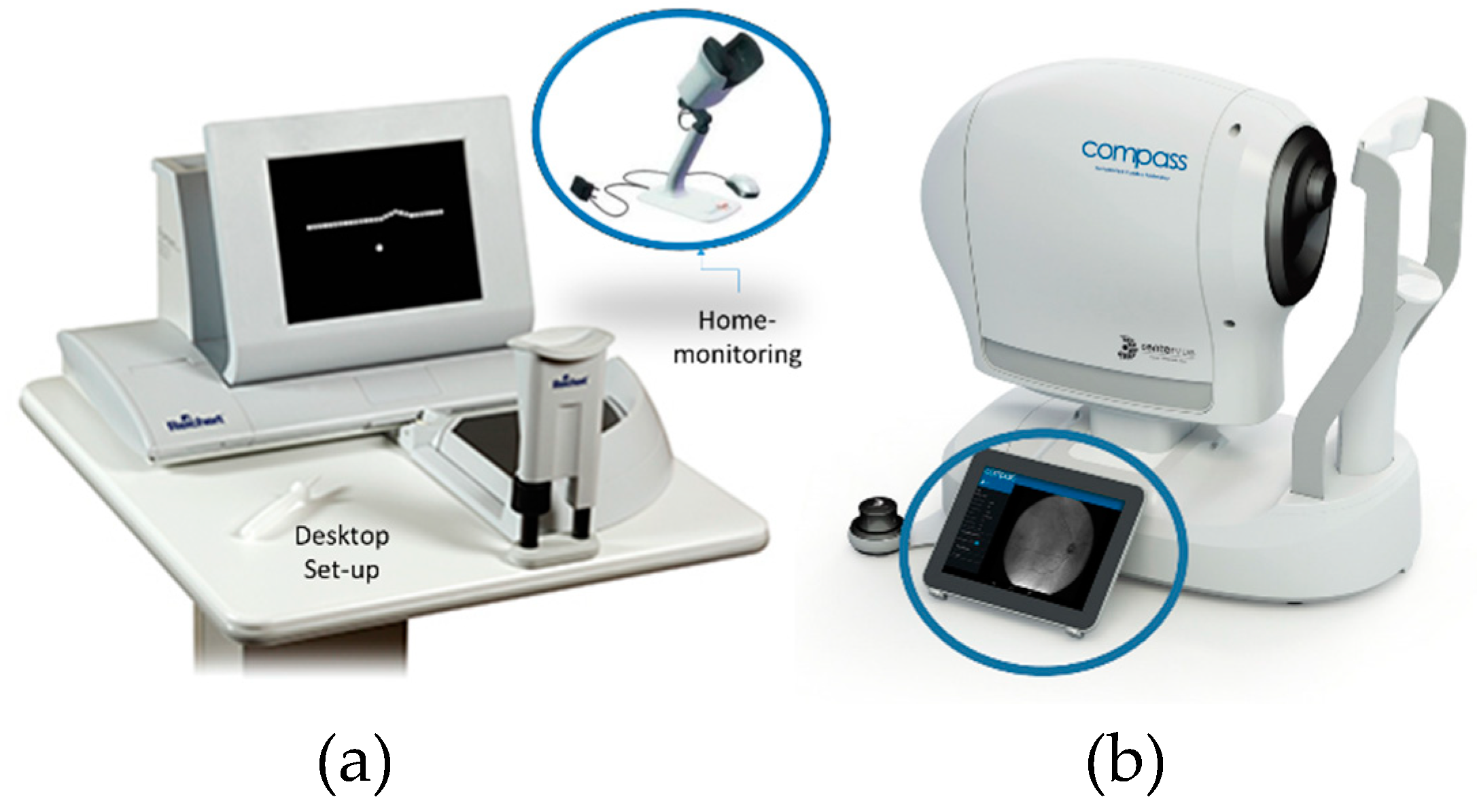
- Notal Vision Inc. ForeseeHome. 31 October 2015. Available online: http://www.foreseehome.com (accessed on 31 October 2015).
- Chew, E.Y.; Traci, E.C.; Susan, B.B.; Michael, J.E.; Ronald, P.D.; Jeffrey, S.; HeierfJudy, E.K.; Richard, A.G. Randomized trial of the ForeseeHome monitoring device for early detection of neovascular age-related macular degeneration. The HOme Monitoring of the Eye (HOME) study design—HOME Study report number 1. Contemp. Clin. Trials 2014, 37, 294–300. [Google Scholar] [CrossRef]
- Han, D.P. The foreseehome device and the home study: A milestone in the self-detection of neovascular age-related macular degeneration. JAMA Ophthalmol. 2014, 132, 1167–1168. [Google Scholar] [CrossRef]
- How the ForeseeHome AMD Monitoring Program Works. ForeseeHome. Available online: https://www.foreseehome.com/hcp/how-it-works-technology/ (accessed on 15 January 2019).
- Compass-Fundus Automated Perimetry. CenterVue. Available online: https://www.centervue.com/products/compass/ (accessed on 15 January 2019).
- Miller, K.P.; Fortun, J.A. Home Monitoring for Age-related Macular Degeneration. Curr. Ophthalmol. Rep. 2018, 6, 53–57. [Google Scholar] [CrossRef]
- Schmid, M.K.; Faes, L.; Bachmann, L.M.; Thiel, M.A. Accuracy of a Self-monitoring Test for Identification and Monitoring of Age-related Macular Degeneration: A Diagnostic Case-control Study. Open Ophthalmol. J. 2018, 12, 19–28. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Term | Acronym |
|---|---|
| Central Serous Retinopathy | CSR |
| Age-related Macular Degeneration | AMD |
| Retinal pigment epithelium | RPE |
| Diabetic Macular Edema | DME |
| Amsler Grid | AG |
| Optical Coherence Tomography | OCT |
| Logarithm of the Minimum Angle of Resolution | LogMAR |
| Visual Distortion | VD |
| Threshold Amsler Grid | TAG |
| Preferential Hyperacuity Perimeter | PHP |
| Three-dimensional Computer-automated Threshold Amsler Grid | 3D-CTAG |
| Macular Computerized Psychophysical Test | MCPT |
| Test | Accuracy | Complexity | Measurement Time | Portability | Ref. |
|---|---|---|---|---|---|
| Amsler Grid (AG) | Low | Low | Low | Good | [25,31] |
| Threshold AG | Medium | Low | Low | Medium | [38] |
| PHP | High | Medium | High | Poor | [38,44,45] |
| PHP Home | High | Medium | High | Good | [63,64,65,66] |
| 3D-CTAG | Medium | Medium | High | Poor | [31,48] |
| MCPT | Medium | High | High | Poor | [38,49] |
| M-CHART | Medium | Medium | Medium | Poor | [50,51] |
| Shape Discrimination | Medium | Low | Medium | Poor | [53] |
| Positioning | Medium | High | High | Poor | [54] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohaghegh, N.; Ghafar-Zadeh, E.; Magierowski, S. Recent Advances of Computerized Graphical Methods for the Detection and Progress Assessment of Visual Distortion Caused by Macular Disorders. Vision 2019, 3, 25. https://doi.org/10.3390/vision3020025
Mohaghegh N, Ghafar-Zadeh E, Magierowski S. Recent Advances of Computerized Graphical Methods for the Detection and Progress Assessment of Visual Distortion Caused by Macular Disorders. Vision. 2019; 3(2):25. https://doi.org/10.3390/vision3020025
Chicago/Turabian StyleMohaghegh, Navid, Ebrahim Ghafar-Zadeh, and Sebastian Magierowski. 2019. "Recent Advances of Computerized Graphical Methods for the Detection and Progress Assessment of Visual Distortion Caused by Macular Disorders" Vision 3, no. 2: 25. https://doi.org/10.3390/vision3020025
APA StyleMohaghegh, N., Ghafar-Zadeh, E., & Magierowski, S. (2019). Recent Advances of Computerized Graphical Methods for the Detection and Progress Assessment of Visual Distortion Caused by Macular Disorders. Vision, 3(2), 25. https://doi.org/10.3390/vision3020025