
The Effects of High-Intensity Interval Exercise on Skeletal Muscle and Cerebral Oxygenation during Cycling and Isokinetic Concentric and Eccentric Exercise


 ,
,  ,
,  ,
, 
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Procedures
2.3. High-Intensity Interval Cycling Exercise Protocol
2.4. High-Intensity Interval Isokinetic Exercise Protocol
2.5. Skeletal Muscle and Cerebral Oxygenation
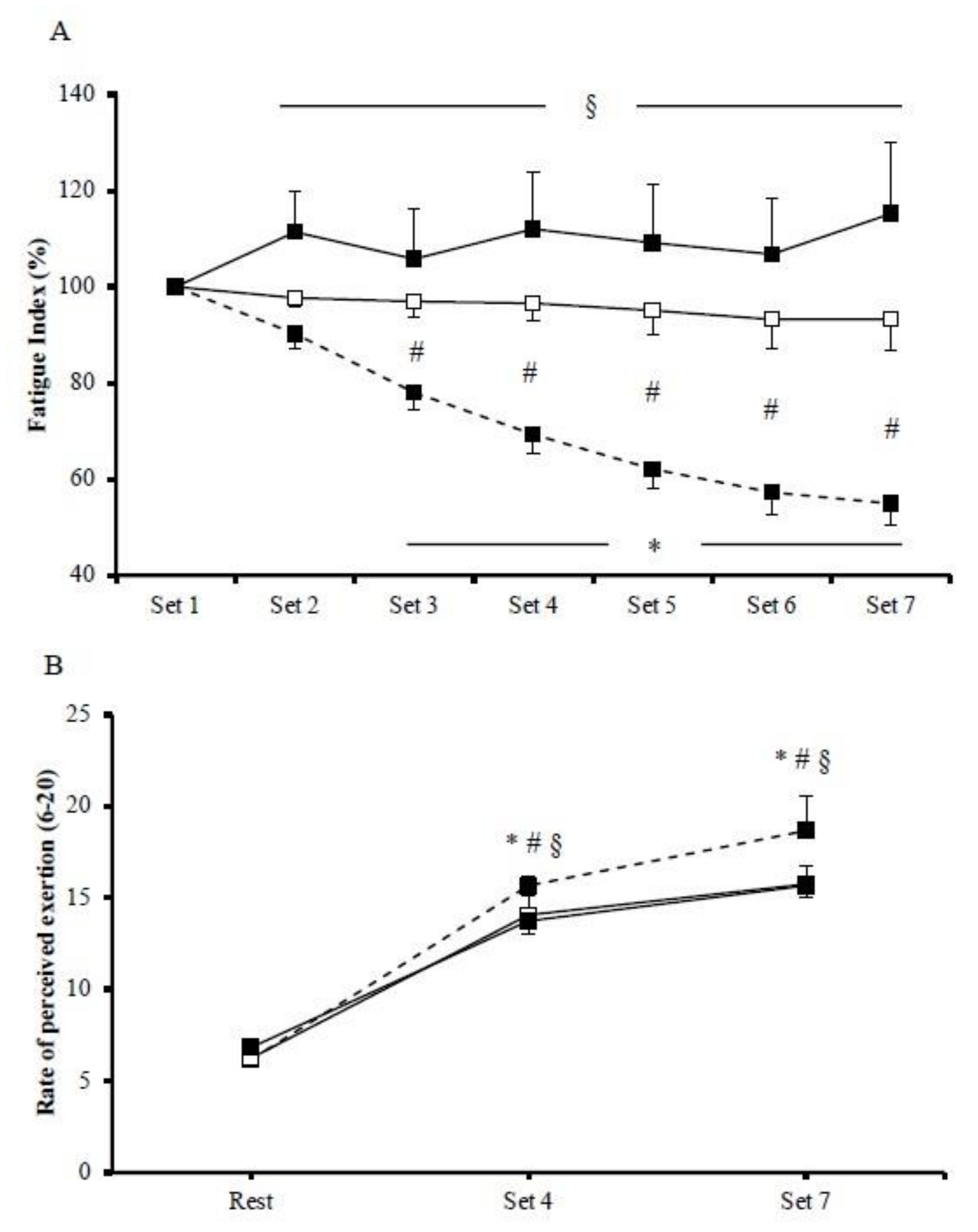
2.6. Rate of Perceived Exertion
2.7. Statistical Analysis
3. Results
3.1. Exercise Performance
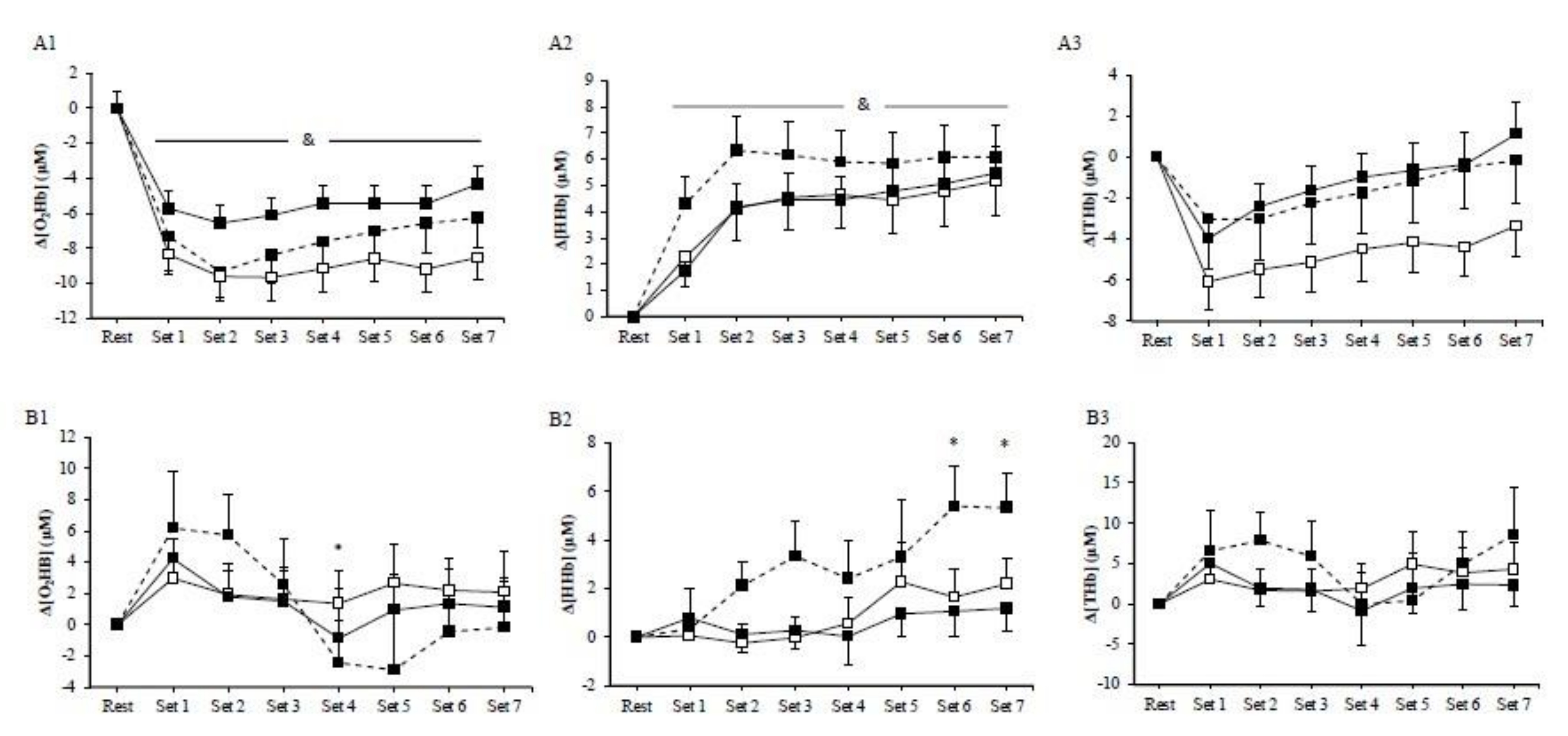
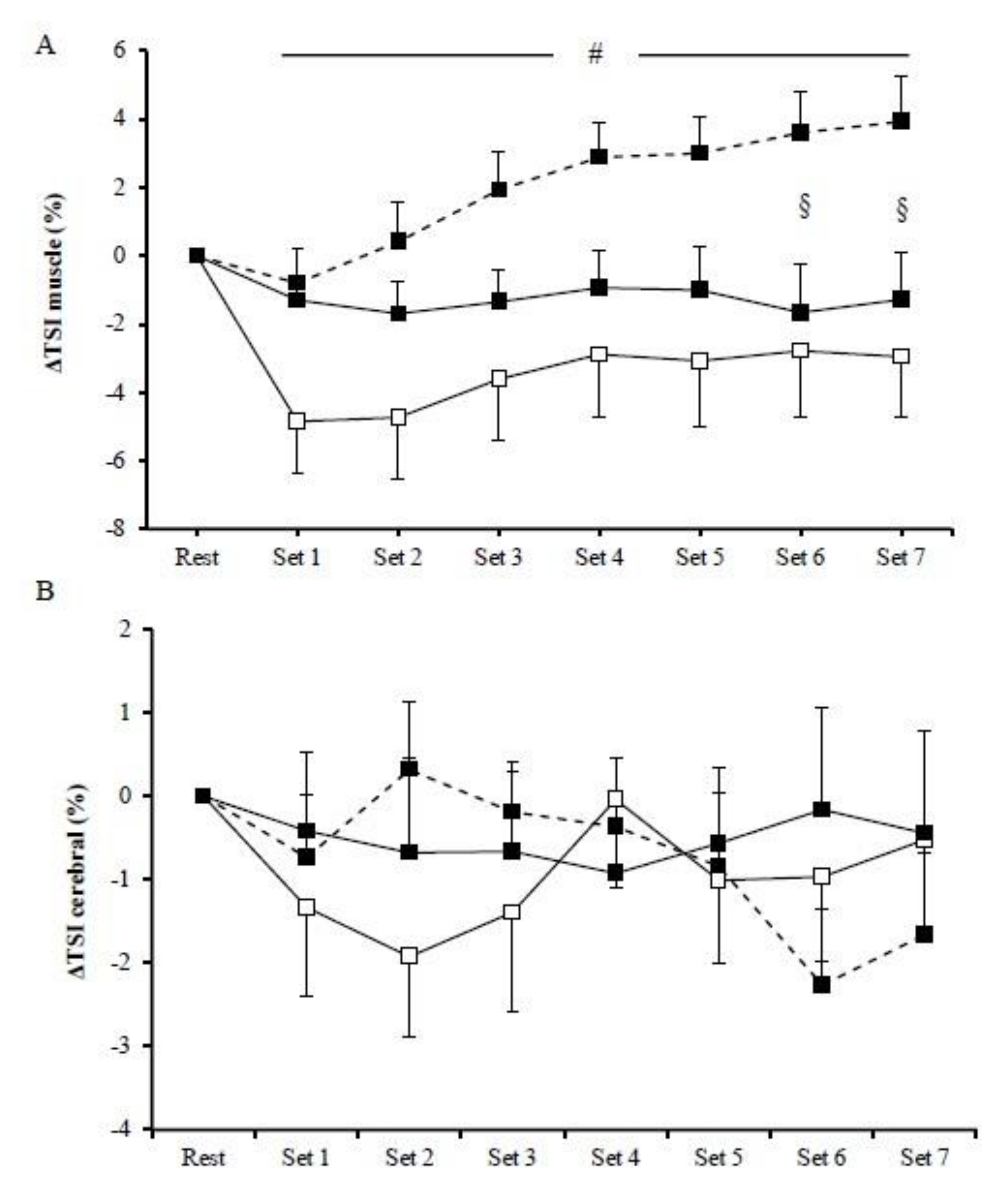
3.2. Muscle Oxygenation
3.3. Cerebral Oxygenation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Billat, L.V. Interval training for performance: A scientific and empirical practice. Special recommendations for middle- and long-distance running. Part II: Anaerobic interval training. Sports Med. 2001, 31, 75–90. [Google Scholar] [CrossRef]
- Billat, L.V. Interval training for performance: A scientific and empirical practice. Special recommendations for middle- and long-distance running. Part I: Aerobic interval training. Sports Med. 2001, 31, 13–31. [Google Scholar] [CrossRef]
- Engel, F.A.; Ackermann, A.; Chtourou, H.; Sperlich, B. High-Intensity Interval Training Performed by Young Athletes: A Systematic Review and Meta-Analysis. Front Physiol. 2018, 9, 1012. [Google Scholar] [CrossRef]
- Gibala, M.J.; Jones, A.M. Physiological and performance adaptations to high-intensity interval training. Nestle Nutr Inst Workshop Ser 2013, 76, 51–60. [Google Scholar] [CrossRef]
- Gist, N.H.; Fedewa, M.V.; Dishman, R.K.; Cureton, K.J. Sprint interval training effects on aerobic capacity: A systematic review and meta-analysis. Sports Med. 2014, 44, 269–279. [Google Scholar] [CrossRef]
- Ni Cheilleachair, N.J.; Harrison, A.J.; Warrington, G.D. HIIT enhances endurance performance and aerobic characteristics more than high-volume training in trained rowers. J. Sports Sci. 2017, 35, 1052–1058. [Google Scholar] [CrossRef]
- Batacan, R.B., Jr.; Duncan, M.J.; Dalbo, V.J.; Tucker, P.S.; Fenning, A.S. Effects of high-intensity interval training on cardiometabolic health: A systematic review and meta-analysis of intervention studies. Br. J. Sports Med. 2017, 51, 494–503. [Google Scholar] [CrossRef]
- Daussin, F.N.; Zoll, J.; Dufour, S.P.; Ponsot, E.; Lonsdorfer-Wolf, E.; Doutreleau, S.; Mettauer, B.; Piquard, F.; Geny, B.; Richard, R. Effect of interval versus continuous training on cardiorespiratory and mitochondrial functions: Relationship to aerobic performance improvements in sedentary subjects. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2008, 295, R264–R272. [Google Scholar] [CrossRef]
- Gibala, M.J.; Little, J.P.; van Essen, M.; Wilkin, G.P.; Burgomaster, K.A.; Safdar, A.; Raha, S.; Tarnopolsky, M.A. Short-term sprint interval versus traditional endurance training: Similar initial adaptations in human skeletal muscle and exercise performance. J. Physiol. 2006, 575, 901–911. [Google Scholar] [CrossRef]
- Gibala, M.J.; McGee, S.L. Metabolic adaptations to short-term high-intensity interval training: A little pain for a lot of gain? Exerc. Sport Sci. Rev. 2008, 36, 58–63. [Google Scholar] [CrossRef]
- Gillen, J.B.; Gibala, M.J. Is high-intensity interval training a time-efficient exercise strategy to improve health and fitness? Appl. Physiol. Nutr. Metab. 2014, 39, 409–412. [Google Scholar] [CrossRef]
- Nybo, L.; Sundstrup, E.; Jakobsen, M.D.; Mohr, M.; Hornstrup, T.; Simonsen, L.; Bulow, J.; Randers, M.B.; Nielsen, J.J.; Aagaard, P.; et al. High-intensity training versus traditional exercise interventions for promoting health. Med. Sci. Sports Exerc. 2010, 42, 1951–1958. [Google Scholar] [CrossRef]
- Adolfo, J.R.; Dhein, W.; Sbruzzi, G. Intensity of physical exercise and its effect on functional capacity in COPD: Systematic review and meta-analysis. J. Bras. Pneumol. 2019, 45, e20180011. [Google Scholar] [CrossRef]
- Giallauria, F.; Smart, N.A.; Cittadini, A.; Vigorito, C. Exercise training modalities in chronic heart failure: Does high intensity aerobic interval training make the difference? Monaldi Arch. Chest. Dis. 2016, 86, 754. [Google Scholar] [CrossRef][Green Version]
- Iellamo, F.; Caminiti, G.; Sposato, B.; Vitale, C.; Massaro, M.; Rosano, G.; Volterrani, M. Effect of High-Intensity interval training versus moderate continuous training on 24-h blood pressure profile and insulin resistance in patients with chronic heart failure. Intern. Emerg. Med. 2014, 9, 547–552. [Google Scholar] [CrossRef]
- Spee, R.F.; Niemeijer, V.M.; Wijn, P.F.; Doevendans, P.A.; Kemps, H.M. Effects of high-intensity interval training on central haemodynamics and skeletal muscle oxygenation during exercise in patients with chronic heart failure. Eur. J. Prev. Cardiol. 2016, 23, 1943–1952. [Google Scholar] [CrossRef]
- Viana, R.B.; de Lira, C.A.B.; Naves, J.P.A.; Coswig, V.S.; Del Vecchio, F.B.; Ramirez-Campillo, R.; Vieira, C.A.; Gentil, P. Can We Draw General Conclusions from Interval Training Studies? Sports Med. 2018, 48, 2001–2009. [Google Scholar] [CrossRef]
- Komi, P.V.; Linnamo, V.; Silventoinen, P.; Sillanpaa, M. Force and EMG power spectrum during eccentric and concentric actions. Med. Sci. Sports Exerc. 2000, 32, 1757–1762. [Google Scholar] [CrossRef]
- Margaritelis, N.V.; Theodorou, A.A.; Chatzinikolaou, P.N.; Kyparos, A.; Nikolaidis, M.G.; Paschalis, V. Eccentric exercise per se does not affect muscle damage biomarkers: Early and late phase adaptations. Eur. J. Appl. Physiol. 2020. [Google Scholar] [CrossRef]
- Paschalis, V.; Nikolaidis, M.G.; Theodorou, A.A.; Panayiotou, G.; Fatouros, I.G.; Koutedakis, Y.; Jamurtas, A.Z. A weekly bout of eccentric exercise is sufficient to induce health-promoting effects. Med. Sci. Sports Exerc. 2011, 43, 64–73. [Google Scholar] [CrossRef]
- Theodorou, A.A.; Panayiotou, G.; Paschalis, V.; Nikolaidis, M.G.; Kyparos, A.; Mademli, L.; Grivas, G.V.; Vrabas, I.S. Stair descending exercise increases muscle strength in elderly males with chronic heart failure. BMC Res. Notes 2013, 6, 87. [Google Scholar] [CrossRef]
- Franchi, M.V.; Reeves, N.D.; Narici, M.V. Skeletal Muscle Remodeling in Response to Eccentric vs. Concentric Loading: Morphological, Molecular, and Metabolic Adaptations. Front. Physiol. 2017, 8, 447. [Google Scholar] [CrossRef]
- Groeber, M.; Reinhart, L.; Kornfeind, P.; Baca, A. The Contraction Modalities in a Stretch-Shortening Cycle in Animals and Single Joint Movements in Humans: A Systematic Review. J. Sports Sci. Med. 2019, 18, 604–614. [Google Scholar]
- Abbott, B.C.; Bigland, B.; Ritchie, J.M. The physiological cost of negative work. J. Physiol. 1952, 117, 380–390. [Google Scholar] [CrossRef]
- Beltman, J.G.; Sargeant, A.J.; van Mechelen, W.; de Haan, A. Voluntary activation level and muscle fiber recruitment of human quadriceps during lengthening contractions. J. Appl. Physiol. 2004, 97, 619–626. [Google Scholar] [CrossRef]
- Bigland-Ritchie, B.; Woods, J.J. Integrated electromyogram and oxygen uptake during positive and negative work. J. Physiol. 1976, 260, 267–277. [Google Scholar] [CrossRef] [PubMed]
- Dufour, S.P.; Lampert, E.; Doutreleau, S.; Lonsdorfer-Wolf, E.; Billat, V.L.; Piquard, F.; Richard, R. Eccentric cycle exercise: Training application of specific circulatory adjustments. Med. Sci. Sports Exerc. 2004, 36, 1900–1906. [Google Scholar] [CrossRef] [PubMed]
- Joumaa, V.; Herzog, W. Energy cost of force production is reduced after active stretch in skinned muscle fibres. J. Biomech. 2013, 46, 1135–1139. [Google Scholar] [CrossRef] [PubMed]
- Lombardi, V.; Piazzesi, G. The contractile response during steady lengthening of stimulated frog muscle fibres. J. Physiol. 1990, 431, 141–171. [Google Scholar] [CrossRef] [PubMed]
- Penailillo, L.; Blazevich, A.; Numazawa, H.; Nosaka, K. Metabolic and muscle damage profiles of concentric versus repeated eccentric cycling. Med. Sci. Sports Exerc. 2013, 45, 1773–1781. [Google Scholar] [CrossRef] [PubMed]
- Perrey, S.; Betik, A.; Candau, R.; Rouillon, J.D.; Hughson, R.L. Comparison of oxygen uptake kinetics during concentric and eccentric cycle exercise. J. Appl. Physiol. 2001, 91, 2135–2142. [Google Scholar] [CrossRef]
- Ryschon, T.W.; Fowler, M.D.; Wysong, R.E.; Anthony, A.; Balaban, R.S. Efficiency of human skeletal muscle in vivo: Comparison of isometric, concentric, and eccentric muscle action. J. Appl. Physiol. 1997, 83, 867–874. [Google Scholar] [CrossRef]
- Fortuna, R.; Groeber, M.; Seiberl, W.; Power, G.A.; Herzog, W. Shortening-induced force depression is modulated in a time- and speed-dependent manner following a stretch-shortening cycle. Physiol. Rep. 2017, 5. [Google Scholar] [CrossRef] [PubMed]
- Fukutati, A.; Misaki, J.; Isaka, T. Both the elongation of attached crossbridges and residual force enhancement contribute to joint torque enhancement by the stretch-shortening cycle. R. Soc. Open Sci. 2017, 4, 161036. [Google Scholar]
- Herzog, W. The multiple roles of titin in muscle contraction and force production. Biophys. Rev. 2018, 10, 1187–1199. [Google Scholar] [CrossRef] [PubMed]
- Lindstedt, S.L.; La Stayo, P.C.; Reich, T.E. When active muscles lengthen: Properties and consequences of eccentric contractions. News Physiol. Sci. 2001, 16, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Barstow, T.J. Understanding near infrared spectroscopy and its application to skeletal muscle research. J. Appl. Physiol. 2019, 126, 1360–1376. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, M.; Mottola, L.; Quaresima, V. Principles, techniques, and limitations of near infrared spectroscopy. Can. J. Appl. Physiol. 2004, 29, 463–487. [Google Scholar] [CrossRef]
- Buchheit, M.; Cormie, P.; Abbiss, C.R.; Ahmaidi, S.; Nosaka, K.K.; Laursen, P.B. Muscle deoxygenation during repeated sprint running: Effect of active vs. passive recovery. Int. J. Sports Med. 2009, 30, 418–425. [Google Scholar] [CrossRef]
- Kriel, Y.; Kerherve, H.A.; Askew, C.D.; Solomon, C. The Effect of Active versus Passive Recovery Periods during High Intensity Intermittent Exercise on Local Tissue Oxygenation in 18–30 Year Old Sedentary Men. PLoS One 2016, 11, e0163733. [Google Scholar] [CrossRef]
- Racinais, S.; Bishop, D.; Denis, R.; Lattier, G.; Mendez-Villaneuva, A.; Perrey, S. Muscle deoxygenation and neural drive to the muscle during repeated sprint cycling. Med. Sci. Sports Exerc. 2007, 39, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.J.; Billaut, F. Tissue oxygenation in men and women during repeated-sprint exercise. Int. J. Sports Physiol. Perform. 2012, 7, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Woorons, X.; Dupuy, O.; Mucci, P.; Millet, G.P.; Pichon, A. Cerebral and Muscle Oxygenation during Repeated Shuttle Run Sprints with Hypoventilation. Int. J. Sports Med. 2019, 40, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Zafeiridis, A.; Kounoupis, A.; Dipla, K.; Kyparos, A.; Nikolaidis, M.G.; Smilios, I.; Vrabas, I.S. Oxygen Delivery and Muscle Deoxygenation during Continuous, Long- and Short-Interval Exercise. Int. J. Sports Med. 2015, 36, 872–880. [Google Scholar] [CrossRef] [PubMed]
- Denis, R.; Bringard, A.; Perrey, S. Vastus lateralis oxygenation dynamics during maximal fatiguing concentric and eccentric isokinetic muscle actions. J. Electromyogr. Kinesiol. 2011, 21, 276–282. [Google Scholar] [CrossRef]
- Muthalib, M.; Lee, H.; Millet, G.Y.; Ferrari, M.; Nosaka, K. Comparison between maximal lengthening and shortening contractions for biceps brachii muscle oxygenation and hemodynamics. J. Appl. Physiol. 2010, 109, 710–720. [Google Scholar] [CrossRef]
- Okamoto, T.; Masuharab, M.; Ikutac, K. Differences of muscle oxygenation during eccentric and concentric contraction. Iso. Exerc. Sci. 2006, 14, 207–212. [Google Scholar] [CrossRef]
- Secher, N.H.; Seifert, T.; Van Lieshout, J.J. Cerebral blood flow and metabolism during exercise: Implications for fatigue. J. Appl. Physiol. 2008, 104, 306–314. [Google Scholar] [CrossRef]
- Subudhi, A.W.; Dimmen, A.C.; Roach, R.C. Effects of acute hypoxia on cerebral and muscle oxygenation during incremental exercise. J. Appl. Physiol. 2007, 103, 177–183. [Google Scholar] [CrossRef]
- Rupp, T.; Perrey, S. Prefrontal cortex oxygenation and neuromuscular responses to exhaustive exercise. Eur. J. Appl. Physiol. 2008, 102, 153–163. [Google Scholar] [CrossRef]
- Shibuya, K.; Kuboyama, N. Decreased activation in the primary motor cortex area during middle-intensity hand grip exercise to exhaustion in athlete and nonathlete participants. Percept. Mot. Ski. 2010, 111, 19–30. [Google Scholar] [CrossRef]
- Shibuya, K.; Tanaka, J.; Kuboyama, N.; Ogaki, T. Cerebral oxygenation during intermittent supramaximal exercise. Respir. Physiol. Neurobiol. 2004, 140, 165–172. [Google Scholar] [CrossRef]
- Beam, W.C.; Adams, G.M. Exercise Physiology Laboratory Manual, 8th ed.; McGraw Hill: Champaign, IL, USA, 2002; pp. 107–119. [Google Scholar]
- Dolopikou, C.F.; Kourtzidis, I.A.; Margaritelis, N.V.; Vrabas, I.S.; Koidou, I.; Kyparos, A.; Theodorou, A.A.; Paschalis, V.; Nikolaidis, M.G. Acute nicotinamide riboside supplementation improves redox homeostasis and exercise performance in old individuals: A double-blind cross-over study. Eur. J. Nutr. 2020, 59, 505–515. [Google Scholar] [CrossRef] [PubMed]
- Grassi, B.; Quaresima, V. Near-infrared spectroscopy and skeletal muscle oxidative function in vivo in health and disease: A review from an exercise physiology perspective. J. Biomed. Opt. 2016, 21, 091313. [Google Scholar] [CrossRef] [PubMed]
- Matcher, S.J.; Elwell, C.E.; Cooper, C.E.; Cope, M.; Delpy, D.T. Performance comparison of several published tissue near-infrared spectroscopy algorithms. Anal. Biochem. 1995, 227, 54–68. [Google Scholar] [CrossRef]
- Cardinale, M.; Ferrari, M.; Quaresima, V. Gastrocnemius medialis and vastus lateralis oxygenation during whole-body vibration exercise. Med. Sci. Sports Exerc. 2007, 39, 694–700. [Google Scholar] [CrossRef]
- van Beekvelt, M.C.; Borghuis, M.S.; van Engelen, B.G.; Wevers, R.A.; Colier, W.N. Adipose tissue thickness affects in vivo quantitative near-IR spectroscopy in human skeletal muscle. Clin. Sci. 2001, 101, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Borg, G.A. Perceived exertion: A note on "history" and methods. Med. Sci. Sports 1973, 5, 90–93. [Google Scholar] [CrossRef]
- Buchheit, M.; Abbiss, C.R.; Peiffer, J.J.; Laursen, P.B. Performance and physiological responses during a sprint interval training session: Relationships with muscle oxygenation and pulmonary oxygen uptake kinetics. Eur. J. Appl. Physiol. 2012, 112, 767–779. [Google Scholar] [CrossRef] [PubMed]
- Burgomaster, K.A.; Heigenhauser, G.J.; Gibala, M.J. Effect of short-term sprint interval training on human skeletal muscle carbohydrate metabolism during exercise and time-trial performance. J. Appl. Physiol. 2006, 100, 2041–2047. [Google Scholar] [CrossRef]
- Gonzalez-Izal, M.; Lusa Cadore, E.; Izquierdo, M. Muscle conduction velocity, surface electromyography variables, and echo intensity during concentric and eccentric fatigue. Muscle Nerve 2014, 49, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Paulus, J.; Croisier, J.L.; Kaux, J.F.; Bury, T. Eccentric versus Concentric - Which Is the Most Stressful Cardiovascularly and Metabolically? Curr. Sports Med. Rep. 2019, 18, 477–489. [Google Scholar] [CrossRef] [PubMed]
- Billaut, F.; Davis, J.M.; Smith, K.J.; Marino, F.E.; Noakes, T.D. Cerebral oxygenation decreases but does not impair performance during self-paced, strenuous exercise. Acta Physiol. 2010, 198, 477–486. [Google Scholar] [CrossRef] [PubMed]
- Monroe, D.C.; Gist, N.H.; Freese, E.C.; O’Connor, P.J.; McCully, K.K.; Dishman, R.K. Effects of Sprint Interval Cycling on Fatigue, Energy, and Cerebral Oxygenation. Med. Sci. Sports Exerc. 2016, 48, 615–624. [Google Scholar] [CrossRef] [PubMed]
- Santos-Concejero, J.; Billaut, F.; Grobler, L.; Olivan, J.; Noakes, T.D.; Tucker, R. Brain oxygenation declines in elite Kenyan runners during a maximal interval training session. Eur. J. Appl. Physiol. 2017, 117, 1017–1024. [Google Scholar] [CrossRef]
- Puhan, M.A.; Büsching, G.; Schünemann, H.J.; VanOort, E.; Zaugg, C.; Frey, M. Interval versus continuous high-intensity exercise in chronic obstructive pulmonary disease: A randomized trial. Ann. Intern. Med. 2006, 145, 816–825. [Google Scholar] [CrossRef]
- Davies, R.C.; Eston, R.G.; Poole, D.C.; Rowlands, A.V.; DiMenna, F.; Wilkerson, D.P.; Twist, C.; Jones, A.M. Effect of eccentric exercise-induced muscle damage on the dynamics of muscle oxygenation and pulmonary oxygen uptake. J. Appl. Physiol. 2008, 105, 1413–1421. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perentis, P.A.; Cherouveim, E.D.; Malliou, V.J.; Margaritelis, N.V.; Chatzinikolaou, P.N.; Koulouvaris, P.; Tsolakis, C.; Nikolaidis, M.G.; Geladas, N.D.; Paschalis, V. The Effects of High-Intensity Interval Exercise on Skeletal Muscle and Cerebral Oxygenation during Cycling and Isokinetic Concentric and Eccentric Exercise. J. Funct. Morphol. Kinesiol. 2021, 6, 62. https://doi.org/10.3390/jfmk6030062
Perentis PA, Cherouveim ED, Malliou VJ, Margaritelis NV, Chatzinikolaou PN, Koulouvaris P, Tsolakis C, Nikolaidis MG, Geladas ND, Paschalis V. The Effects of High-Intensity Interval Exercise on Skeletal Muscle and Cerebral Oxygenation during Cycling and Isokinetic Concentric and Eccentric Exercise. Journal of Functional Morphology and Kinesiology. 2021; 6(3):62. https://doi.org/10.3390/jfmk6030062
Chicago/Turabian StylePerentis, Panagiotis A., Evgenia D. Cherouveim, Vassiliki J. Malliou, Nikos V. Margaritelis, Panagiotis N. Chatzinikolaou, Panayiotis Koulouvaris, Charilaos Tsolakis, Michalis G. Nikolaidis, Nickos D. Geladas, and Vassilis Paschalis. 2021. "The Effects of High-Intensity Interval Exercise on Skeletal Muscle and Cerebral Oxygenation during Cycling and Isokinetic Concentric and Eccentric Exercise" Journal of Functional Morphology and Kinesiology 6, no. 3: 62. https://doi.org/10.3390/jfmk6030062
APA StylePerentis, P. A., Cherouveim, E. D., Malliou, V. J., Margaritelis, N. V., Chatzinikolaou, P. N., Koulouvaris, P., Tsolakis, C., Nikolaidis, M. G., Geladas, N. D., & Paschalis, V. (2021). The Effects of High-Intensity Interval Exercise on Skeletal Muscle and Cerebral Oxygenation during Cycling and Isokinetic Concentric and Eccentric Exercise. Journal of Functional Morphology and Kinesiology, 6(3), 62. https://doi.org/10.3390/jfmk6030062