
Spondyloarthritis and Strength Training: A 4-Year Report

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Characteristics and Questionnaires
2.2. Nutritional Plans
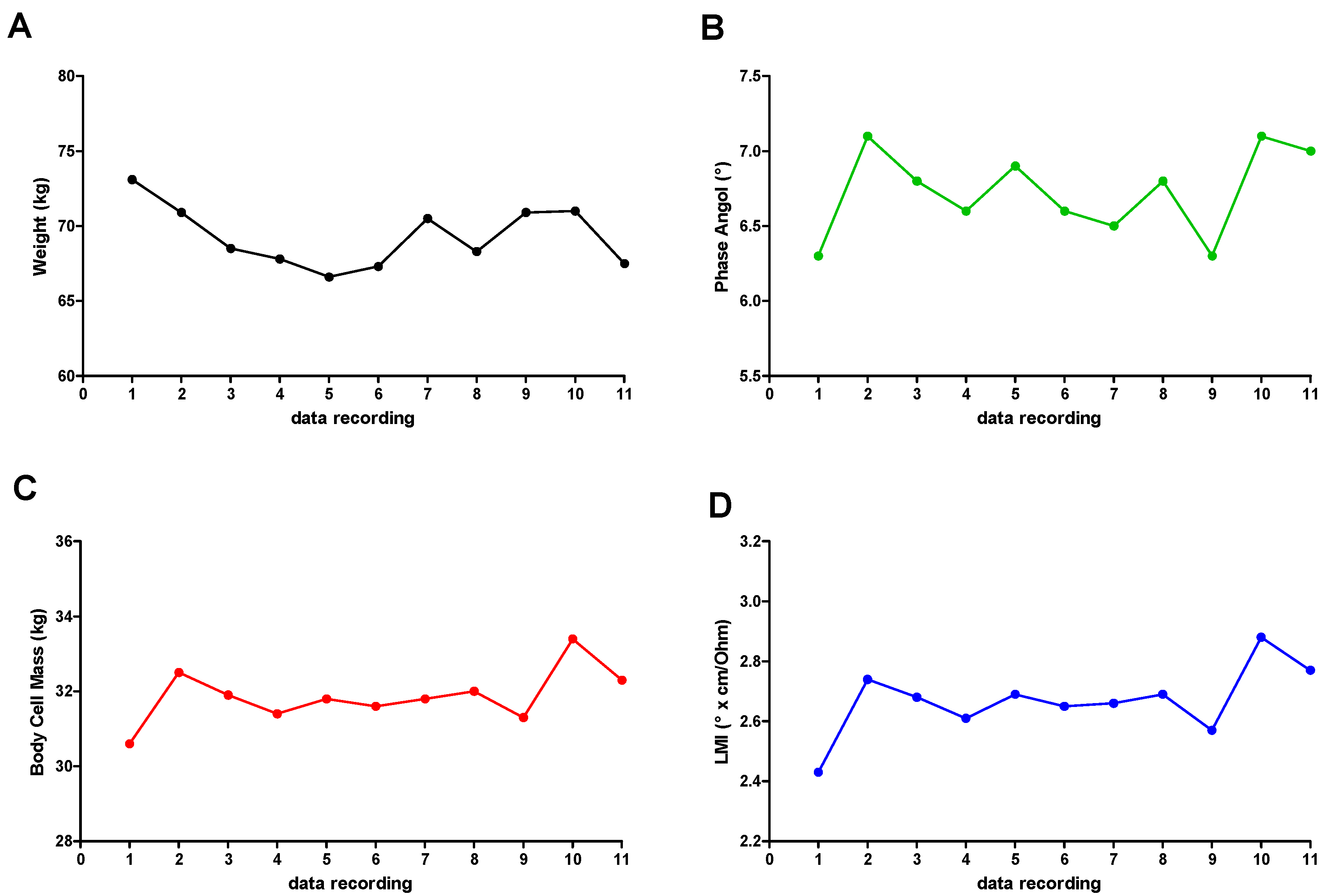
2.3. Bioimpedance Analysis
2.4. Training Program
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Kiltz, U.; Baraliakos, X.; Braun, J. Spondyloarthritiden-das neue Konzept. Eine Einführung zu Diagnostik und Therapie der axialen Spondyloarthritis [Spondyloarthritis-the novel concept. An introduction to the diagnosis and treatment of axial spondyloarthritis]. Dtsch. Med. Wochenschr. 2012, 137, 1745–1747. [Google Scholar] [CrossRef] [PubMed]
- Fejzić, E.; Eminović, I.; Karamehić, J.; Šahović, A.; Šišić, S.; Suljević, D. Association Between Human Leukocyte Antigen-B*27 and Pathogenesis in Seronegative Spondyloarthropathies in Federation of Bosnia and Herzegovina. Arch. Rheumatol. 2018, 34, 166–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rudwaleit, M. Spondyloarthritiden [Spondyloarthritides]. Z. Rheumatol. 2017, 76, 889–903. [Google Scholar] [CrossRef] [PubMed]
- Flórez García, M.T.; Carmona, L.; Almodóvar, R.; Fernández de Las Peñas, C.; García Pérez, F.; Pérez Manzanero, M.Á.; García García, J.M.; Soriano Segarra, L.; Jiménez Díaz, J.F.; Mendoza Laiz, N.; et al. Recommendations for the prescription of physical exercise for patients with spondyloarthritis. Reumatol. Clin. 2019, 15, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- McDonald, M.T.; Siebert, S.; Coulter, E.H.; McDonald, D.A.; Paul, L. Level of adherence to prescribed exercise in spondyloarthritis and factors affecting this adherence: A systematic review. Rheumatol. Int. 2019, 39, 187–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sveaas, S.H.; Dagfinrud, H.; Berg, I.J.; Provan, S.A.; Johansen, M.W.; Pedersen, E.; Bilberg, A. High-Intensity Exercise Improves Fatigue, Sleep, and Mood in Patients with Axial Spondyloarthritis: Secondary Analysis of a Randomized Controlled Trial. Phys. Ther. 2020, 100, 1323–1332. [Google Scholar] [CrossRef] [PubMed]
- Malorgio, A.; Malorgio, M.; Benedetti, M.; Casarosa, S.; Cannataro, R. High intensity resistance training as intervention method to knee osteoarthritis. Sports Med. Health Sci. 2021, 3, 46–48. [Google Scholar] [CrossRef]
- American College of Rheumatology. Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)—General Description; ACR: Atlanta, GA, USA, 2012. [Google Scholar]
- Yi, H.; Shin, K.; Shin, C. Development of the sleep quality scale. J. Sleep Res. 2006, 15, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Hays, R.D.; Sherbourne, C.D.; Mazel, R.M. The RAND 36-Item Health Survey 1.0. Health Econ. 1993, 2, 217–227. [Google Scholar] [CrossRef] [PubMed]
- Lukaski, H.C.; Bolonchuk, W.W.; Hall, C.B.; Siders, W.A. Validation of tetrapolar bioelectrical impedance method to assess human body composition. J. Appl. Physiol. 1986, 60, 1327–1332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gómez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.C.; Pirlich, M.; et al. Composition of the ESPEN Working Group. Bioelectrical impedance analysis—Part I: Review of principles and methods. Clin. Nutr. 2004, 23, 1226–1243. [Google Scholar] [CrossRef] [PubMed]
- Cannataro, R.; Perri, M.; Gallelli, L.; Caroleo, M.C.; De Sarro, G.; Cione, E. Ketogenic Diet Acts on Body Remodeling and MicroRNAs Expression Profile. MicroRNA. 2019, 8, 116–126. [Google Scholar] [CrossRef] [PubMed]
- Cannataro, R.; Caroleo, M.C.; Fazio, A.; La Torre, C.; Plastina, P.; Gallelli, L.; Lauria, G.; Cione, E. Ketogenic Diet and microRNAs Linked to Antioxidant Biochemical Homeostasis. Antioxidants 2019, 8, 269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, M.S.; Callahan, D.M.; Tourville, T.W.; Slauterbeck, J.R.; Kaplan, A.; Fiske, B.R.; Savage, P.D.; Ades, P.A.; Beynnon, B.D.; Toth, M.J. Moderate-intensity resistance exercise alters skeletal muscle molecular and cellular structure and function in inactive older adults with knee osteoarthritis. J. Appl. Physiol. 2017, 122, 775–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berardinelli, A.; D’Antona, G. Physiological aspects of muscular adaptations to training translated to neuromuscular diseases. Acta Mol. 2019, 38, 197–206. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| WOMAC | Pain | Stiffness | Impact on Quality of Life | Sleep Quality |
|---|---|---|---|---|
| T0 2017 | 18 | 8 | 60 | 64 |
| T1 2019 | 6 | 3 | 26 | 40 |
| T2 2020 | 10 | 5 | 35 | 45 |
| T3 2021 | 1 | 1 | 4 | 15 |
| % Reduction T0 vs. T3 | −95 | −87.5 | −93.3 | −76.6 |
| Data Recording | |
|---|---|
| 1 | 14/04/2017 |
| 2 | 10/05/2017 |
| 3 | 12/06/2017 |
| 4 | 13/07/2017 |
| 5 | 28/11/2017 |
| 6 | 21/02/2018 |
| 7 | 25/07/2018 |
| 8 | 24/01/2019 |
| 9 | 28/02/2020 |
| 10 | 16/07/2020 |
| 11 | 27/03/2021 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cannataro, R.; Di Maio, L.; Malorgio, A.; Levi Micheli, M.; Cione, E. Spondyloarthritis and Strength Training: A 4-Year Report. J. Funct. Morphol. Kinesiol. 2021, 6, 58. https://doi.org/10.3390/jfmk6030058
Cannataro R, Di Maio L, Malorgio A, Levi Micheli M, Cione E. Spondyloarthritis and Strength Training: A 4-Year Report. Journal of Functional Morphology and Kinesiology. 2021; 6(3):58. https://doi.org/10.3390/jfmk6030058
Chicago/Turabian StyleCannataro, Roberto, Lorenzo Di Maio, Andrea Malorgio, Matteo Levi Micheli, and Erika Cione. 2021. "Spondyloarthritis and Strength Training: A 4-Year Report" Journal of Functional Morphology and Kinesiology 6, no. 3: 58. https://doi.org/10.3390/jfmk6030058
APA StyleCannataro, R., Di Maio, L., Malorgio, A., Levi Micheli, M., & Cione, E. (2021). Spondyloarthritis and Strength Training: A 4-Year Report. Journal of Functional Morphology and Kinesiology, 6(3), 58. https://doi.org/10.3390/jfmk6030058