


From Overweight to Severe Obesity: Physical Activity and Behavioural Profiles in a Large Clinical Cohort

 ,
,  ,
,  , , ,
, , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
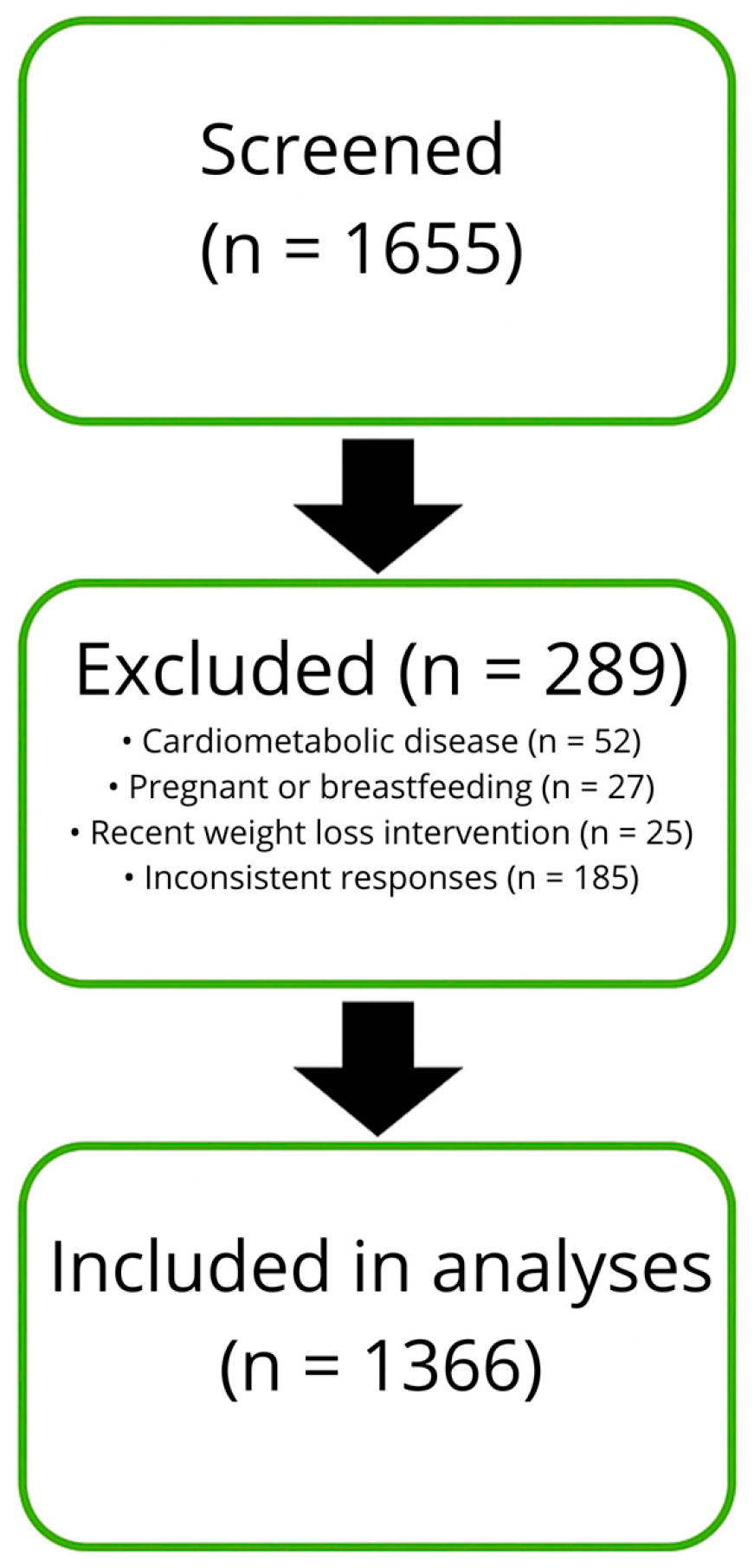
2.1. Subjects
2.2. Questionnaire and Behavioural Assessment
2.3. Body Composition
2.4. Statistical Analysis
3. Results
4. Discussion
4.1. Food Taste
4.2. Eating Behaviours
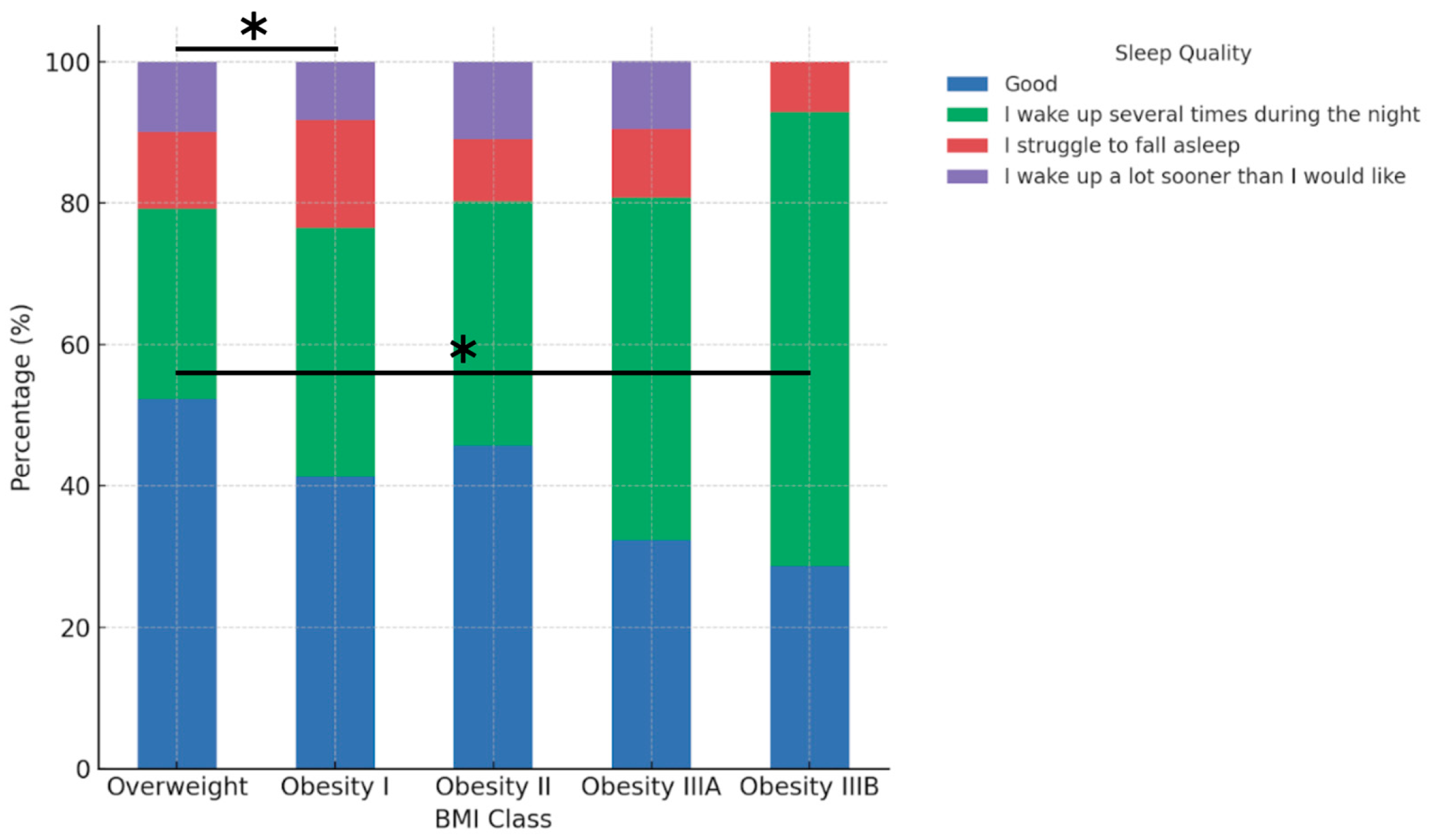
4.3. Sleep Quality
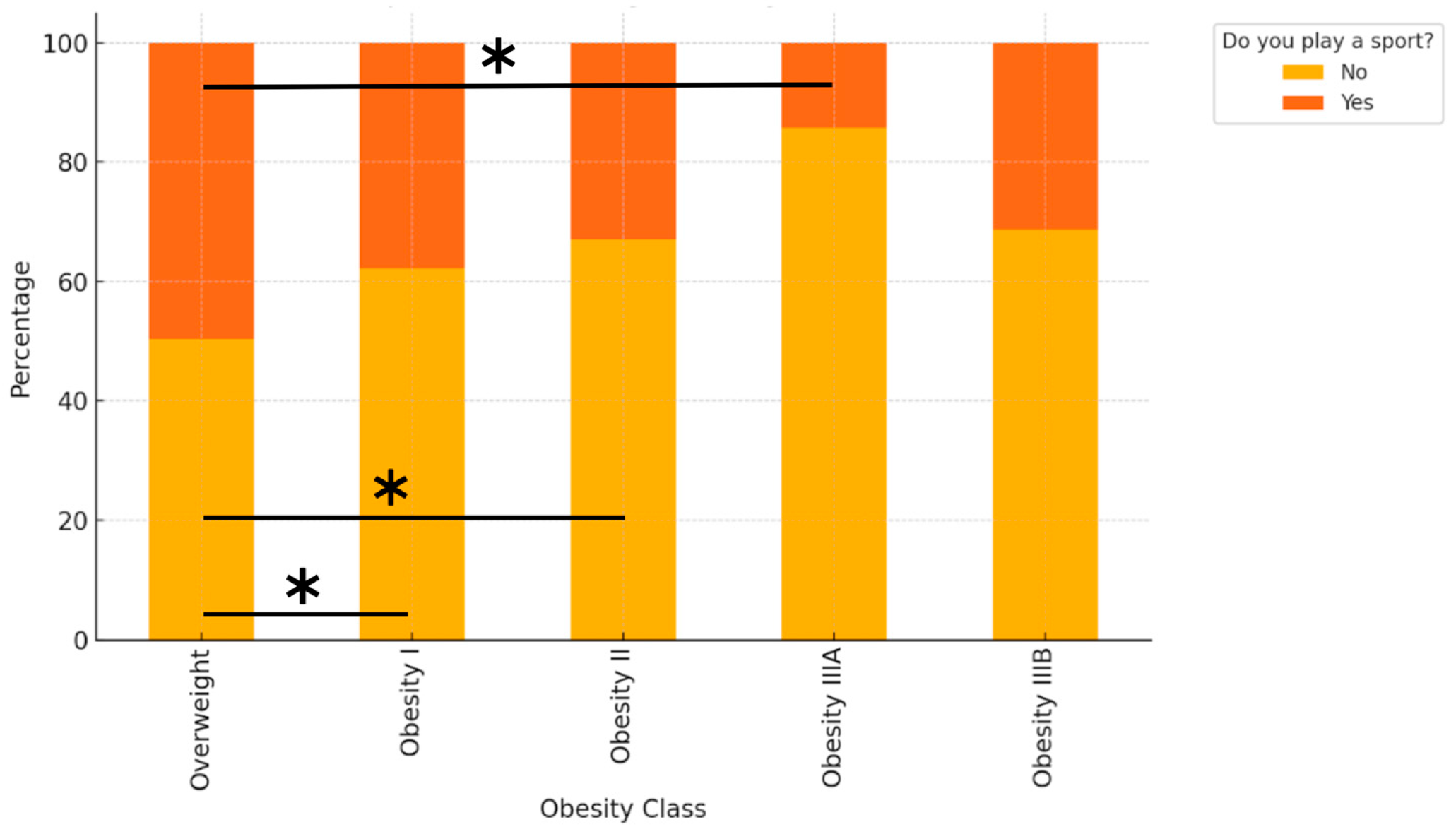
4.4. Physical Activity
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Obesity and Overweight [Internet]; Geneva: World Health Organization: Geneva, Switzerland, 2025; Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 18 July 2025).
- Zandvakili, I.; Pulaski, M.; Pickett-Blakely, O. A phenotypic approach to obesity treatment. Nutr. Clin. Pract. 2023, 38, 959–975. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, S.L.; Coughlin, J.W.; Appel, L.J.; Tyson, C.; Stevens, V.J.; Jerome, G.J.; Dalcin, A.; Brantley, P.J.; Hill-Briggs, F. Application of latent class analysis to identify behavioral patterns of response to behavioral lifestyle interventions in overweight and obese adults. Int. J. Behav. Med. 2015, 22, 471–480. [Google Scholar] [CrossRef] [PubMed]
- Liberali, R.; Del Castanhel, F.; Kupek, E.; Assis, M.D. Latent class analysis of lifestyle risk factors and association with overweight and/or obesity in children and adolescents: Systematic review. Child. Obes. 2020, 17, 2–15. [Google Scholar] [CrossRef] [PubMed]
- Fuente González, C.E.; Chávez-Servín, J.L.; de la Torre-Carbot, K.; Ronquillo González, D.; Aguilera Barreiro, M.L.Á.; Ojeda Navarro, L.R. Relationship between Emotional Eating, Consumption of Hyperpalatable Energy-Dense Foods, and Indicators of Nutritional Status: A Systematic Review. J. Obes. 2022, 2022, 4243868. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wei, Y.; Tang, D.; Lu, J.; Zhang, N.; Hu, Y.; He, R.; Guan, H.; Xu, J.; Wang, S.; et al. Association of major dietary patterns and different obesity phenotypes in Southwest China: The China Multi-Ethnic Cohort (CMEC) Study. Eur. J. Nutr. 2022, 62, 465–476. [Google Scholar] [CrossRef] [PubMed]
- Hendryx, M.; Dinh, P.; Chow, A.; Kroenke, C.H.; Hingle, M.; Shadyab, A.H.; Garcia, L.; Howard, B.V.; Luo, J. Lifestyle and psychosocial patterns and diabetes incidence among women with and without obesity: A prospective latent class analysis. Prev. Sci. 2020, 21, 850–860. [Google Scholar] [CrossRef] [PubMed]
- St-Onge, M.P.; Grandner, M.A.; Brown, D.; Conroy, M.B.; Jean-Louis, G.; Coons, M.; Bhatt, D.L.; American Heart Association Obesity, Behavior Change, Diabetes, and Nutrition Committees of the Council on Lifestyle and Cardiometabolic Health; Council on Cardiovascular Disease in the Young; Council on Clinical Cardiology; et al. Sleep Duration and Quality: Impact on Lifestyle Behaviors and Cardiometabolic Health: A Scientific Statement From the American Heart Association. Circulation 2016, 134, e367–e386. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Raiman, L.; Amarnani, R.; Abdur-Rahman, M.; Marshall, A.; Mani-Babu, S. The role of physical activity in obesity: Let’s actively manage obesity. Clin. Med. 2023, 23, 311–317. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jacob, J.; Isaac, R. Behavioral therapy for management of obesity. Indian J. Endocrinol. Metab. 2012, 16, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Unick, J.; Beavers, D.; Jakicic, J.; Kitabchi, A.; Knowler, W.; Wadden, T.; Wing, R. Effectiveness of lifestyle interventions for individuals with severe obesity and type 2 diabetes. Diabetes Care 2011, 34, 2152–2157. [Google Scholar] [CrossRef] [PubMed]
- Camacho-Barcia, L.; Lucas, I.; Miranda-Olivos, R.; Jiménez-Murcia, S.; Fernández-Aranda, F. Applying psycho-behavioural phenotyping in obesity characterization. Rev. Endocr. Metab. Disord. 2023, 24, 871–883. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cifuentes, L.; Ghusn, W.; Feris, F.; Campos, A.; Sacoto, D.; De la Rosa, A.; McRae, A.; Rieck, T.; Mansfield, S.; Ewoldt, J.; et al. Phenotype tailored lifestyle intervention on weight loss and cardiometabolic risk factors in adults with obesity: A single-centre, non-randomised, proof-of-concept study. EClinicalMedicine 2023, 58, 101923. [Google Scholar] [CrossRef] [PubMed]
- Schulz, C.A.; Oluwagbemigun, K.; Nöthlings, U. Advances in dietary pattern analysis in nutritional epidemiology. Eur. J. Nutr. 2021, 60, 4115–4130. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hooson, J.; Hutchinson, J.; Warthon-Medina, M.; Hancock, N.; Greathead, K.; Knowles, B.; Vargas-Garcia, E.; Gibson, L.E.; Bush, L.A.; Margetts, B.; et al. A systematic review of reviews identifying UK validated dietary assessment tools for inclusion on an interactive guided website for researchers: www.nutritools.org. Crit. Rev. Food. Sci. Nutr. 2020, 60, 1265–1289. [Google Scholar] [CrossRef] [PubMed]
- Carbonneau, E.; Bradette-Laplante, M.; Lamarche, B.; Provencher, V.; Bégin, C.; Robitaille, J.; Desroches, S.; Vohl, M.C.; Corneau, L.; Lemieux, S. Development and validation of the food liking questionnaire in a French-Canadian population. Nutrients 2017, 9, 1337. [Google Scholar] [CrossRef] [PubMed]
- Kushner, R.F.; Hammond, M.M. Using psycho-behavioral phenotyping for overweight and obesity: Confirmation of the 6 factor questionnaire. Obes. Sci. Pract. 2021, 8, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Gnagnarella, P.; Dragà, D.; Misotti, A.M.; Sieri, S.; Spaggiari, L.; Cassano, E.; Baldini, F.; Soldati, L.; Maisonneuve, P. Validation of a short questionnaire to record adherence to the Mediterranean diet: An Italian experience. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 1140–1147. [Google Scholar] [CrossRef] [PubMed]
- Coppini, L.; Waitzberg, D.; Campos, A. Limitations and validation of bioelectrical impedance analysis in morbidly obese patients. Curr. Opin. Clin. Nutr. Metab. Care 2005, 8, 329–332. [Google Scholar] [CrossRef] [PubMed]
- Eales, J.; Lenoir-Wijnkoop, I.; King, S.; Wood, H.; Kok, F.J.; Shamir, R.; Prentice, A.; Edwards, M.; Glanville, J.; Atkinson, R.L. Is Consuming Yoghurt Associated with Weight Management Outcomes? Results from a Systematic Review. Int. J. Obes. 2016, 40, 731–746. [Google Scholar] [CrossRef] [PubMed]
- Sayon-Orea, C.; Martínez-González, M.A.; Ruiz-Canela, M.; Bes-Rastrollo, M. Associations between Yogurt Consumption and Weight Gain and Risk of Obesity and Metabolic Syndrome: A Systematic Review. Adv. Nutr. 2017, 8, 146S–154S. [Google Scholar] [CrossRef] [PubMed]
- Martínez-González, M.A.; Sayon-Orea, C.; Ruiz-Canela, M.; de la Fuente, C.; Gea, A.; Bes-Rastrollo, M. Yogurt Consumption, Weight Change and Risk of Overweight/Obesity: The SUN Cohort Study. Nutr. Metab. Cardiovasc. Dis. 2014, 24, 1189–1196. [Google Scholar] [CrossRef] [PubMed]
- Tucker, L.A. Legume Intake, Body Weight, and Abdominal Adiposity: 10-Year Weight Change and Cross-Sectional Results in 15,185 U.S. Adults. Nutrients 2023, 15, 460. [Google Scholar] [CrossRef] [PubMed]
- Heshmatipour, H.; Hajhashemy, Z.; Mirzaei, S.; Asadi, A.; Akhlaghi, M.; Saneei, P. Association of Legumes and Nuts Consumption with Metabolic Health Status in Iranian Overweight and Obese Adolescents. Sci. Rep. 2023, 13, 5784. [Google Scholar] [CrossRef] [PubMed]
- Peinado, B.R.R.; Frazão, D.R.; Bittencourt, L.O.; de Souza-Rodrigues, R.D.; Vidigal, M.T.C.; da Silva, D.T.; Paranhos, L.R.; Magno, M.B.; Fagundes, N.C.F.; Maia, L.C.; et al. Is Obesity Associated with Taste Alterations? A Systematic Review. Front. Endocrinol. 2023, 14, 1167119. [Google Scholar] [CrossRef] [PubMed]
- Rohrer, J.E.; Vickers-Douglas, K.S.; Stroebel, R.J. Uncontrolled Eating and Obesity in Adult Primary Care Patients. Obes. Res. Clin. Pract. 2009, 3, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Ohkuma, T.; Hirakawa, Y.; Nakamura, U.; Kiyohara, Y.; Kitazono, T.; Ninomiya, T. Association Between Eating Rate and Obesity: A Systematic Review and Meta-Analysis. Int. J. Obes. 2015, 39, 1589–1596. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, R.; Tomi, R.; Shinzawa, M.; Yoshimura, R.; Ozaki, S.; Nakanishi, K.; Ide, S.; Nagatomo, I.; Nishida, M.; Yamauchi-Takihara, K.; et al. Associations of Skipping Breakfast, Lunch, and Dinner with Weight Gain and Overweight/Obesity in University Students: A Retrospective Cohort Study. Nutrients 2021, 13, 271. [Google Scholar] [CrossRef] [PubMed]
- Keramat, S.A.; Alam, K.; Basri, R.; Jansen, M.; Shaikh, M.; Renzaho, A.M.N. Sleep duration, sleep quality and the risk of being obese: Evidence from the Australian panel survey. Sleep Med. 2023, 109, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Yu, T.; Liu, C.; Yang, J.; Yu, J. Poor sleep quality and overweight/obesity in healthcare professionals: A cross-sectional study. Front. Public Health 2024, 12, 1390643. [Google Scholar] [CrossRef] [PubMed]
- Chaput, J.P.; McHill, A.W.; Cox, R.C.; Broussard, J.L.; Dutil, C.; St-Onge, M.P. The role of insufficient sleep and circadian misalignment in obesity. Nat. Rev. Endocrinol. 2023, 19, 82–97. [Google Scholar] [CrossRef] [PubMed]
- Eid, S.W.; Brown, R.F.; Maloney, S.K.; Phillips, J.G.; Touyz, S. Can the relationship between overweight/obesity and sleep quality be explained by affect and behaviour? Eat. Weight. Disord. 2022, 27, 2821–2834. [Google Scholar] [CrossRef] [PubMed]
- Swift, D.L.; McGee, J.E.; Earnest, C.P.; Carlisle, E.; Nygard, M.; Johannsen, N.M. The effects of exercise and physical activity on weight loss and maintenance. Prog Cardiovasc. Dis. 2014, 56, 441–447. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 1366) | Overweight | Obesity I | Obesity II | Obesity IIIA | Obesity IIIB | p-Value | |
|---|---|---|---|---|---|---|---|
| Male (n, %) | 591 (43.3%) | 324 (41.3%) | 174 (45.7%) | 72 (48.0%) | 13 (37.1%) | 8 (50.0%) | 0.3672 |
| Female (n, %) | 775 (56.7%) | 460 (58.7%) | 207 (54.3%) | 78 (52.0%) | 22 (62.9%) | 8 (50.0%) | |
| Age | 42.8 ± 13.2 | 41.4 ± 13.0 | 43.2 ± 13.1 | 46.9 ± 13.3 | 50.0 ± 12.0 | 48.6 ± 13.1 | <0.0001 |
| Weight (kg) | 86.4 ± 16.5 | 77.6 ± 10.0 | 92.1 ± 11.3 | 105.4 ± 13.2 | 115.5 ± 14.4 | 143.8 ± 18.2 | <0.0001 |
| BMI | 30.4 ± 4.7 | 27.3 ± 1.5 | 32.2 ± 1.4 | 37.1 ± 1.4 | 42.1 ± 1.4 | 50.9 ± 5.2 | <0.0001 |
| FM (kg) | 29.4 ± 10.1 | 23.5 ± 5.2 | 33.2 ± 6.0 | 41.4 ± 6.0 | 51.3 ± 6.4 | 70.5 ± 14.4 | <0.0001 |
| FM (%) | 33.8 ± 8.1 | 30.7 ± 7.1 | 36.4 ± 7.0 | 39.7 ± 6.4 | 44.8 ± 6.1 | 49.7 ± 7.3 | <0.0001 |
| AC (cm) | 102.7 ± 11.8 | 95.9 ± 7.4 | 107.8 ± 7.1 | 117.4 ± 8.1 | 124.8 ± 10.9 | 143.2 ± 10.3 | <0.0001 |
| FFM (kg) | 54.0 ± 11.4 | 51.3 ± 10.2 | 55.8 ± 11.2 | 60.7 ± 12.4 | 61.1 ± 13.6 | 67.4 ± 12.3 | <0.0001 |
| BMR (kcal) | 1721.5 ± 345.6 | 1623.2 ± 295.5 | 1789.2 ± 329.5 | 1955.2 ± 381.9 | 1978.8 ± 397.3 | 2270.6 ± 396.1 | <0.0001 |
| Key Findings | |
|---|---|
| Food Preferences | Lower preference for yoghurt and legumes with increasing obesity class. No relevant differences for meat or other dairy products. |
| Taste Preference | No association between BMI class and sweet–salty taste preference. |
| Eating behaviours | Fast eating, uncontrolled eating, and skipping meals increased with BMI class. |
| Sleep Quality | Overweight participants reported better sleep quality; the proportion reporting “Good” sleep declined and night-time awakenings increased with higher obesity class. |
| Sports Participation | The Overweight class was more likely to practice sports than all obesity classes. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campoli, F.; Padua, E.; Caprioli, L.; Edriss, S.; Annino, G.; Bonaiuto, V.; Lombardo, M. From Overweight to Severe Obesity: Physical Activity and Behavioural Profiles in a Large Clinical Cohort. J. Funct. Morphol. Kinesiol. 2025, 10, 283. https://doi.org/10.3390/jfmk10030283
Campoli F, Padua E, Caprioli L, Edriss S, Annino G, Bonaiuto V, Lombardo M. From Overweight to Severe Obesity: Physical Activity and Behavioural Profiles in a Large Clinical Cohort. Journal of Functional Morphology and Kinesiology. 2025; 10(3):283. https://doi.org/10.3390/jfmk10030283
Chicago/Turabian StyleCampoli, Francesca, Elvira Padua, Lucio Caprioli, Saeid Edriss, Giuseppe Annino, Vincenzo Bonaiuto, and Mauro Lombardo. 2025. "From Overweight to Severe Obesity: Physical Activity and Behavioural Profiles in a Large Clinical Cohort" Journal of Functional Morphology and Kinesiology 10, no. 3: 283. https://doi.org/10.3390/jfmk10030283
APA StyleCampoli, F., Padua, E., Caprioli, L., Edriss, S., Annino, G., Bonaiuto, V., & Lombardo, M. (2025). From Overweight to Severe Obesity: Physical Activity and Behavioural Profiles in a Large Clinical Cohort. Journal of Functional Morphology and Kinesiology, 10(3), 283. https://doi.org/10.3390/jfmk10030283