
Demographic, Epidemiological and Functional Profile Models of Greek CrossFit Athletes in Relation to Shoulder Injuries: A Prospective Study

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Testing Protocol
2.3. Active Range of Motion (ROM)
2.4. Strength
2.5. Sports-Specific Tests
2.6. One-Year Monitoring and Recording Shoulder Injuries
2.7. Statistical Analysis
3. Results
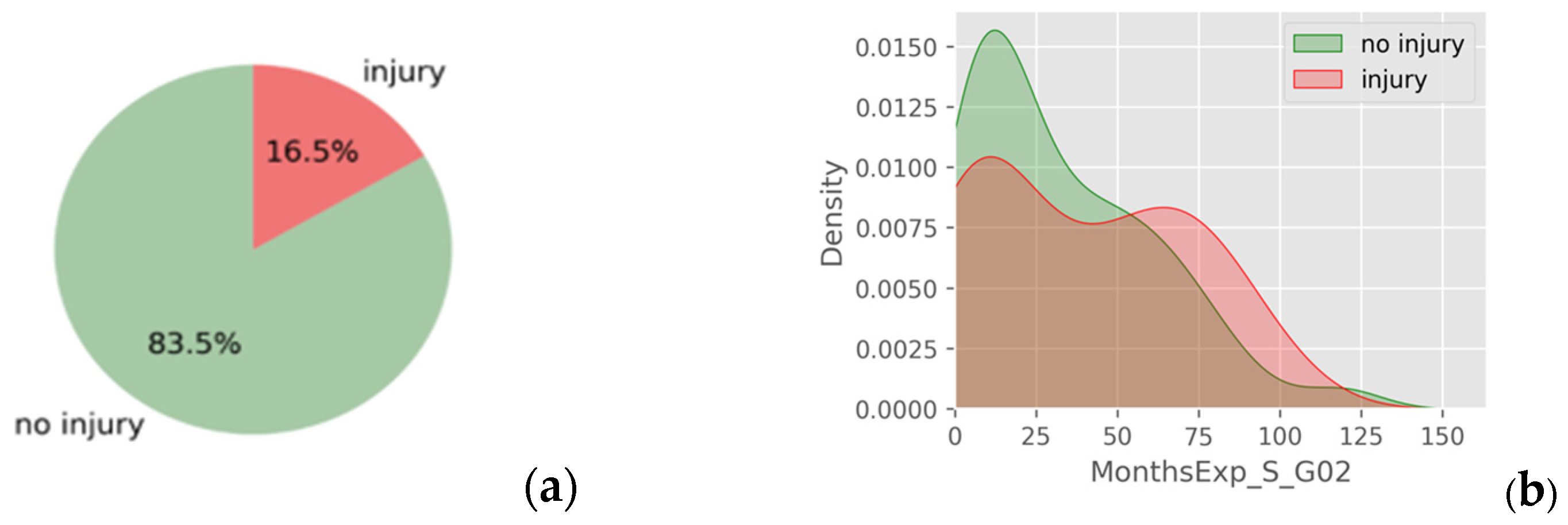
3.1. Demographics and Injury Incidence
3.2. Exploratory Data Analysis and Descriptive Statistics
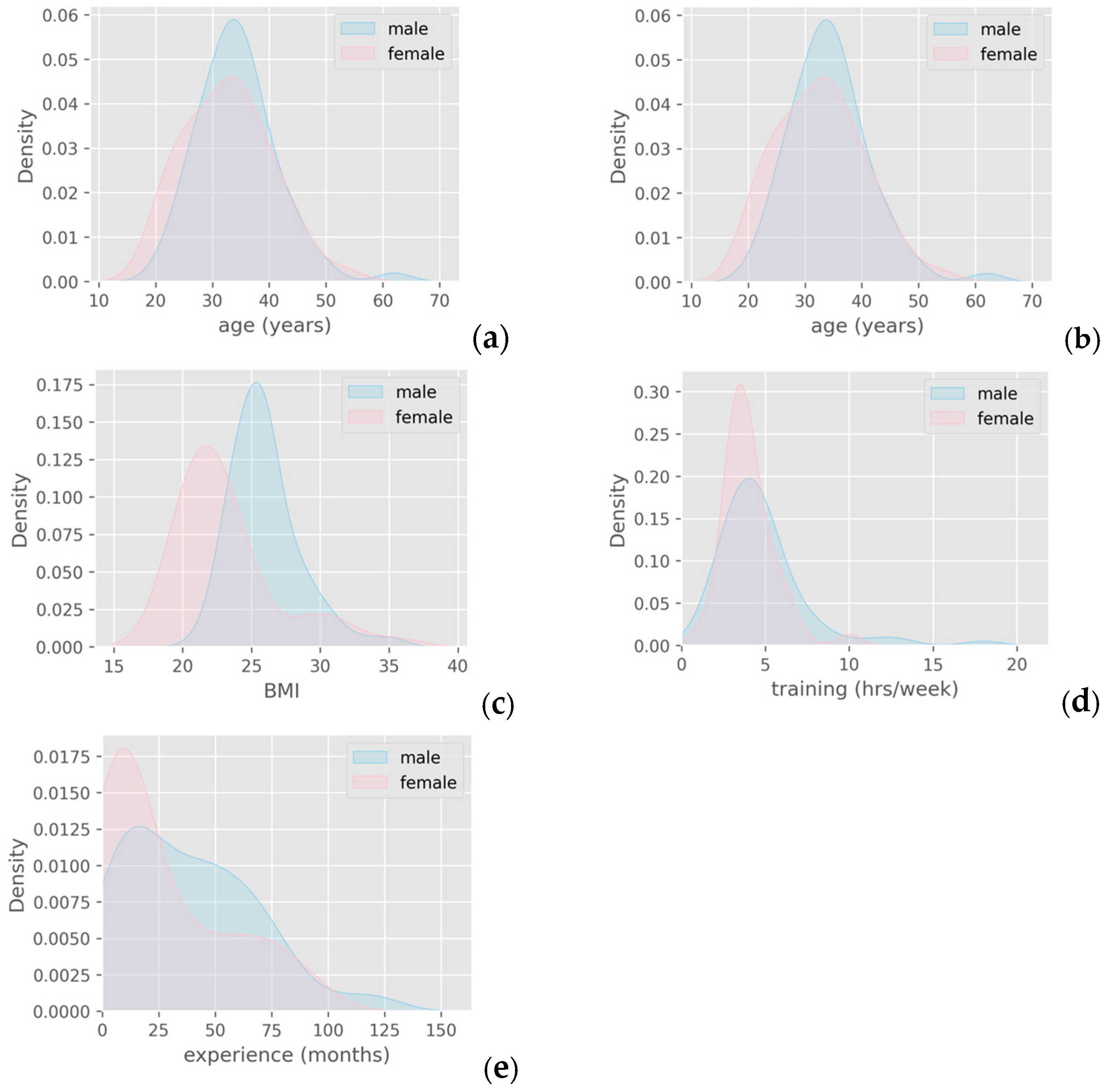
3.2.1. Demographic Data
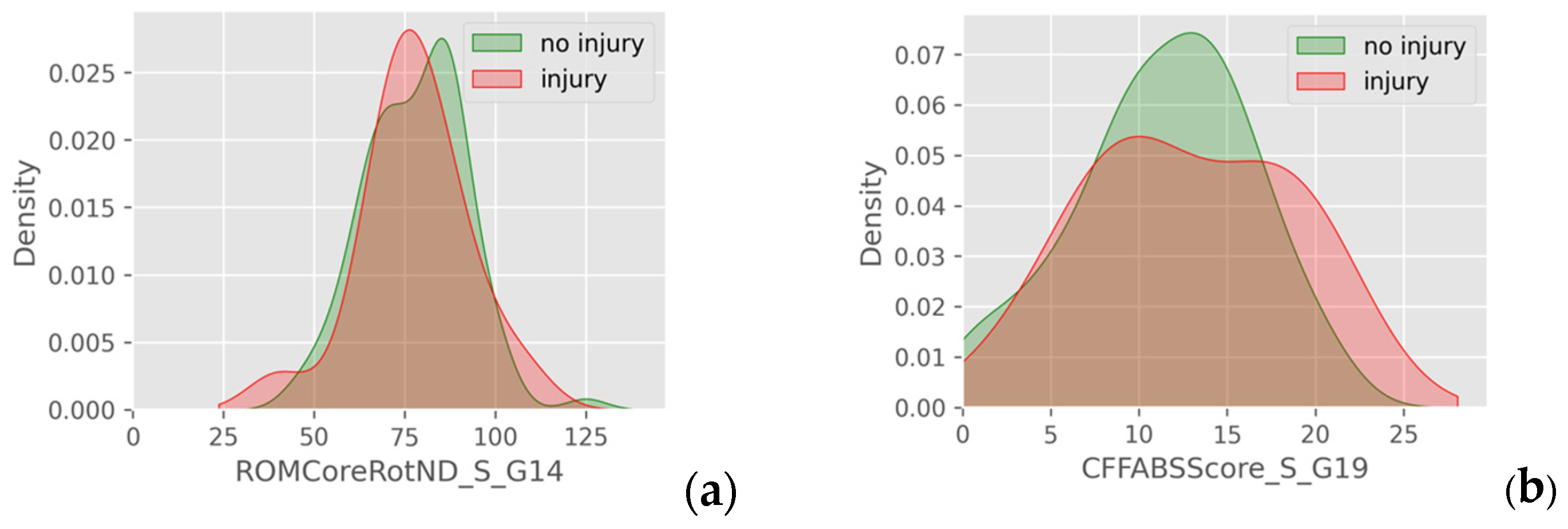
3.2.2. Range of Motion, Strength and Sports-Specific Tests
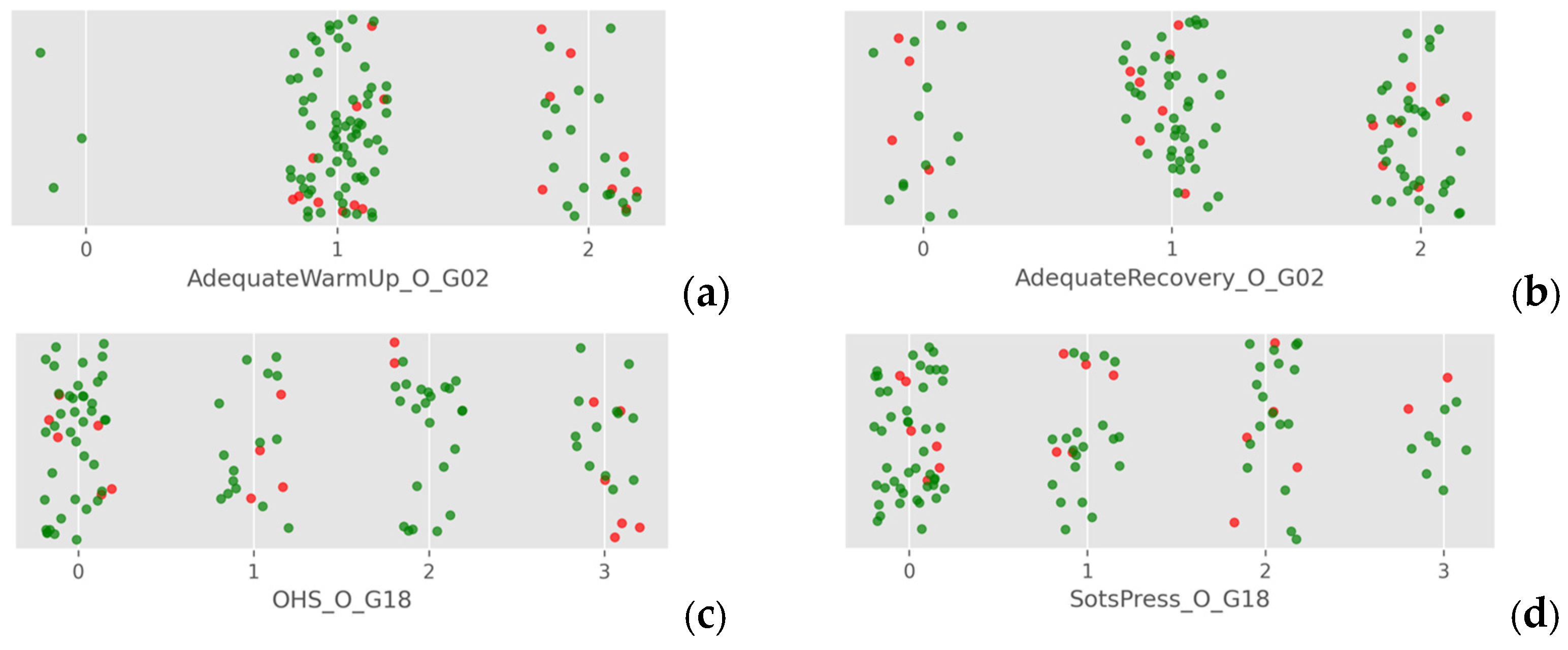
3.2.3. Ordinal Measurements and Data
3.2.4. Nominal Data
3.3. Inferential Statistics
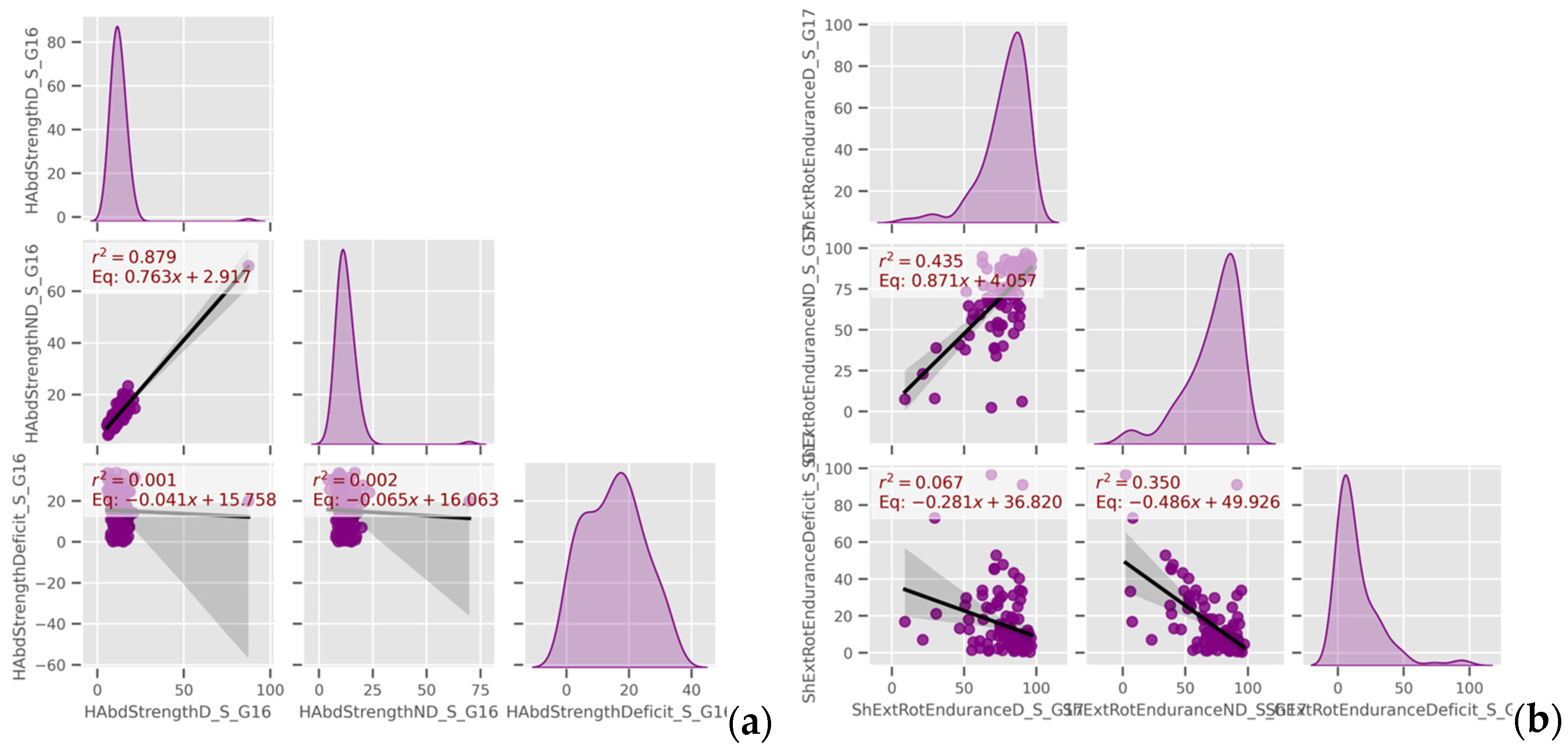
3.4. Understanding the Interactions of the Epidemiological Characteristics and the Functional Tests
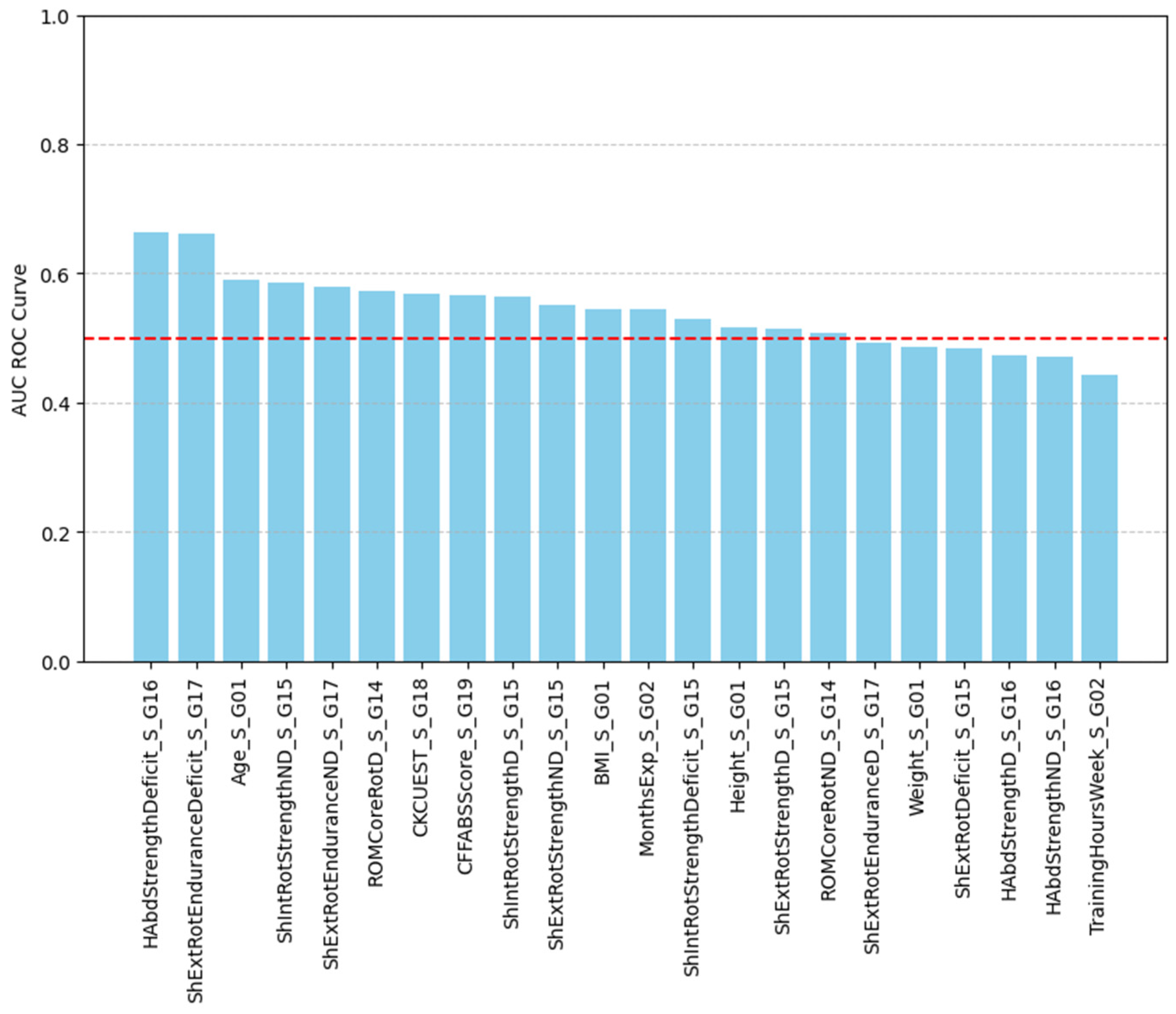
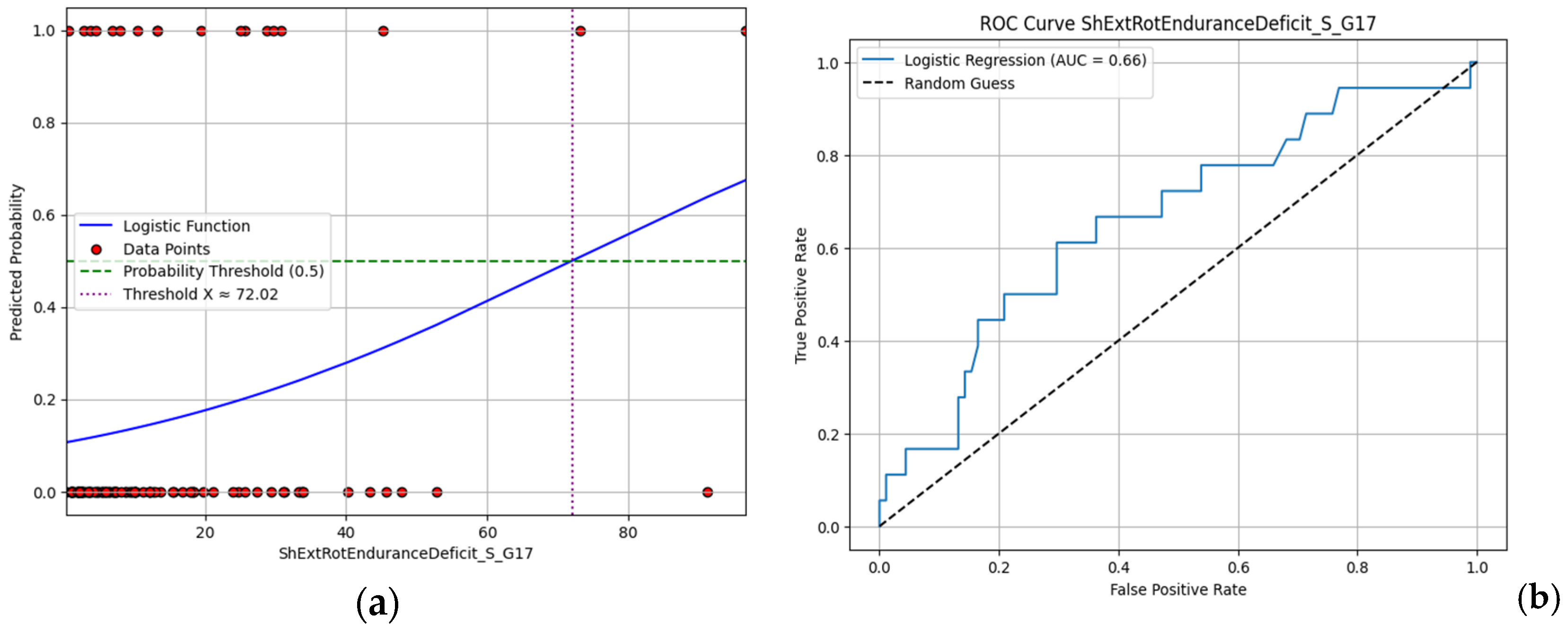
3.5. Modeling and Predicting Shoulder Injuries
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Glassman, G. CrossFit Level 1 Training Guide, 3rd ed.; CrossFit Inc.: Santa Cruz, CA, USA, 2016. [Google Scholar]
- Rios, M.; Becker, K.M.; Cardoso, F.; Pyne, D.B.; Reis, V.M.; Moreira-Gonçalves, D.; Fernandes, R.J. Assessment of Cardiorespiratory and Metabolic Contributions in an Extreme Intensity CrossFit® Benchmark Workout. Sensors 2024, 24, 513. [Google Scholar] [CrossRef] [PubMed]
- Párraga-Montilla, J.A.; Cabrera Linares, J.C.; Jiménez Reyes, P.; Moyano López, M.; Serrano Huete, V.; Morcillo Losa, J.A.; Latorre Román, P.A. Force–Velocity Profiles in CrossFit Athletes: A Cross-Sectional Study Considering Sex, Age, and Training Frequency. Balt. J. Health Phys. Act. 2023, 15, 5. [Google Scholar] [CrossRef]
- Shaffick, M.B.A. Review of the Epidemiology of CrossFit-Related Injuries. Am. J. Health Med. Nurs. Pract. 2023, 8, 33–53. [Google Scholar] [CrossRef]
- Szajkowski, S.; Dwornik, M.; Pasek, J.; Cieślar, G. Risk Factors for Injury in CrossFit®—A Retrospective Analysis. Int. J. Environ. Res. Public Health 2023, 20, 2211. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez, Á.M.; García-Calleja, P.; Terrados, N.; Crespo, I.; Del Valle, M.; Olmedillas, H. Injury in CrossFit®: A Systematic Review of Epidemiology and Risk Factors. Physician Sportsmed. 2022, 50, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Brandsema, C.J.; Mehrab, M.M.; Nina, M.C. Most Common Injuries in Crossfit Training: A Systematic Review. Int. J. Sports Exerc. Med. 2022, 8, 228. [Google Scholar] [CrossRef] [PubMed]
- Boeira, D.; de Brida, L.; Milhomens, Y.; Doyenart, R.; Silva, L.A.D. Injuries in CrossFit Practioner: A Cross-Sectional Study. Mot. Rev. Educ. Fisica. 2023, 29, e10230014322. [Google Scholar] [CrossRef]
- Bernstorff, M.A.; Schumann, N.; Schwake, L.; Somberg, O.; Balke, M.; Schildhauer, T.; Königshausen, M. Shoulder Pathologies in CrossFit: A Magnetic Resonance Imaging Study of 51 Cases. J. Sports Med. Phys. Fit. 2024, 64, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Vanderlei, E.D.S.O.; Santos, A.L.F.D.; Carvalho, N.D.; Carvalho, N.D.; Neves, E.D.A.E.; Lopes-Junior, J.E.G. Muskuloskeletal Injuries in CrossFit Practitioners: An Integrative Review. Braz. J. Clin. Med. Rev. 2023, 1, 25–30. [Google Scholar] [CrossRef]
- Hak, P.T.; Hodzovic, E.; Hickey, B. The Nature and Prevalence of Injury during CrossFit Training. J. Strength Cond. Res. 2013. Publish Ahead of Print. [Google Scholar] [CrossRef] [PubMed]
- Torres-Banduc, M.A.; Jerez-Mayorga, D.; Moran, J.; Keogh, J.W.; Ramírez-Campillo, R. Isokinetic Force-Power Profile of the Shoulder Joint in Males Participating in CrossFit Training and Competing at Different Levels. PeerJ 2021, 9, e11643. [Google Scholar] [CrossRef] [PubMed]
- Kibler, B.W.; Sciascia, A.; Wilkes, T. Scapular Dyskinesis and Its Relation to Shoulder Injury. J. Am. Acad. Orthop. Surg. 2012, 20, 364–372. [Google Scholar] [CrossRef] [PubMed]
- Nicolay, R.W.; Moore, L.K.; DeSena, T.D.; Dines, J.S. Upper Extremity Injuries in CrossFit Athletes—A Review of the Current Literature. Curr. Rev. Musculoskelet. Med. 2022, 15, 402–410. [Google Scholar] [CrossRef] [PubMed]
- Wilson-Smith, A.R.; Muralidaran, S.; Maharaj, M.; Pelletier, M.H.; Beshara, P.; Rao, P.; Pearce, L.M.; Wang, T.; Mobbs, R.J.; Walsh, W.R. Validation of a Novel Range of Motion Assessment Tool for the Cervical Spine: The HALO© Digital Goniometer. J. Spine Surg. 2022, 8, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Olds, M.; McLaine, S.; Magni, N. Validity and Reliability of the Kinvent Handheld Dynamometer in the Athletic Shoulder Test. J. Sport Rehabil. 2023, 32, 764–772. [Google Scholar] [CrossRef] [PubMed]
- Bakaraki, A.; Parmaxizoglou, D.; Gkrilias, P.; Tsekoura, M.; Fousekis, K.; Xergia, S.; Matzaroglou, C.; Tsepis, E. Inter-Rater and Test-Retest Reliability of an Innovative Evaluation Tool: CrossFit Functional Assessment Battery of Tests for the Shoulder Joint. Cureus 2024, 16, e53267. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, G.M.; Calixtre, L.B.; Fialho, H.R.F.; Locks, F.; Kamonseki, D.H. Measurement Properties of Upper Extremity Physical Performance Tests in Athletes: A Systematic Review. Braz. J. Phys. Ther. 2024, 28, 100575. [Google Scholar] [CrossRef] [PubMed]
- Szeles, P.R.D.Q.; Costa, T.S.D.; Cunha, R.A.D.; Hespanhol, L.; Pochini, A.D.C.; Ramos, L.A.; Cohen, M. CrossFit and the Epidemiology of Musculoskeletal Injuries: A Prospective 12-Week Cohort Study. Orthop. J. Sports Med. 2020, 8, 2325967120908884. [Google Scholar] [CrossRef] [PubMed]
- Rosner, B. Fundamentals of Biostatistics, 7th ed.; Brooks/Cole, Cengage Learning: Boston, MA, USA, 2011. [Google Scholar]
- Botev, Z.I.; Grotowski, J.F.; Kroese, D.P. Kernel Density Estimation via Diffusion. Ann. Stat. 2010, 38, 2916–2957. [Google Scholar] [CrossRef]
- Colbrook, M.J.; Botev, Z.I.; Kuritz, K.; MacNamara, S. Kernel Density Estimation with Linked Boundary Conditions. Stud. Appl. Math. 2020, 145, 357–396. [Google Scholar] [CrossRef]
- Abdi, H. The Bonferonni and Šidák Corrections for Multiple Comparisons. Encycl. Meas. Stat. 2007, 7. [Google Scholar]
- James, G.; Witten, D.; Hastie, T.; Tibshirani, R.; Taylor, J. An Introduction to Statistical Learning: With Applications in Python; Springer Texts in Statistics; Springer International Publishing: Cham, Switzerland, 2023. [Google Scholar] [CrossRef]
- How to Classify, Assess, and Coach Aging CrossFit Athletes. Available online: https://www.crossfit.com/pro-coach/classify-assess-coach-aging-crossfit-athletes (accessed on 1 May 2025).
- Kilgore, L. Aging, Performance, and Health: While Physical Capacity Inevitably Declines as Athletes Age, Fitness Has Dramatic Effects on Health and Quality of Life. CrossFit J. 2016, 2–6. Available online: https://library.crossfit.com/free/pdf/CFJ_2015_11_Aging_Kilgore2.pdf (accessed on 22 May 2025).
- Summitt, R.J.; Cotton, R.A.; Kays, A.C.; Slaven, E.J. Shoulder Injuries in Individuals Who Participate in CrossFit Training. Sports Health Multidiscip. Approach 2016, 8, 541–546. [Google Scholar] [CrossRef] [PubMed]
- Montalvo, A.M.; Shaefer, H.; Rodriguez, B.; Li, T.; Epnere, K.; Myer, G.D. Retrospective Injury Epidemiology and Risk Factors for Injury in CrossFit. J. Sports Sci. Med. 2017, 16, 53–59. [Google Scholar] [PubMed]
- Moran, S.; Booker, H.; Staines, J.; Williams, S. Rates and Risk Factors of Injury in CrossFitTM: A Prospective Cohort Study. J. Sports Med. Phys. Fit. 2017, 57, 1147–1153. [Google Scholar] [CrossRef] [PubMed]
- Tafuri, S. CrossFit Athletes Exhibit High Symmetry of Fundamental Movement Patterns. A Cross-Sectional Study. Muscles Ligaments Tendons J. 2016, 6, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Drum, S.N.; Bellovary, B.N.; Jensen, R.L.; Moore, M.T.; Donath, L. Perceived Demands and Postexercise Physical Dysfunction in CrossFit® Compared to an ACSM Based Training Session. J. Sports Med. Phys. Fit. 2017, 57, 604–609. [Google Scholar] [CrossRef] [PubMed]
- Larsen, R.T.; Hessner, A.L.; Ishøi, L.; Langberg, H.; Christensen, J. Injuries in Novice Participants during an Eight-Week Start up CrossFit Program—A Prospective Cohort Study. Sports 2020, 8, 21. [Google Scholar] [CrossRef] [PubMed]
- Minghelli, B.; Vicente, P. Musculoskeletal Injuries in Portuguese CrossFit Practitioners. J. Sports Med. Phys. Fit. 2019, 59, 1213–1220. [Google Scholar] [CrossRef] [PubMed]
- Feito, Y.; Burrows, E.; Tabb, L.; Ciesielka, K.-A. Breaking the Myths of Competition: A Cross-Sectional Analysis of Injuries among CrossFit Trained Participants. BMJ Open Sport Exerc. Med. 2020, 6, e000750. [Google Scholar] [CrossRef] [PubMed]
- Mehrab, M.; Wagner, R.K.; Vuurberg, G.; Gouttebarge, V.; De Vos, R.-J.; Mathijssen, N.M.C. Risk Factors for Musculoskeletal Injury in CrossFit: A Systematic Review. Int. J. Sports Med. 2023, 44, 247–257. [Google Scholar] [CrossRef] [PubMed]
- Bittencourt, N.F.N.; Meeuwisse, W.H.; Mendonça, L.D.; Nettel-Aguirre, A.; Ocarino, J.M.; Fonseca, S.T. Complex Systems Approach for Sports Injuries: Moving from Risk Factor Identification to Injury Pattern Recognition—Narrative Review and New Concept. Br. J. Sports Med. 2016, 50, 1309–1314. [Google Scholar] [CrossRef] [PubMed]
- Van Eetvelde, H.; Mendonça, L.D.; Ley, C.; Seil, R.; Tischer, T. Machine Learning Methods in Sport Injury Prediction and Prevention: A Systematic Review. J. Exp. Orthop. 2021, 8, 27. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Mean | Std. Deviation | Std. Error Mean | Range |
|---|---|---|---|---|
| Age (years) | 33.73 | 7.31 | 0.70 | 20–62 |
| Weight (kg) | 75.24 | 14.57 | 1.40 | 47.50–113.90 |
| Height (meters) | 1.73 | 0.10 | 0.01 | 1.54–1.94 |
| BMI (kg/m2) | 24.89 | 3.34 | 0.32 | 18.79–35.59 |
| Experience (months) | 34.10 | 29.16 | 2.79 | 1–120 |
| Training Volume (hours/week) | 4.48 | 2.36 | 0.23 | 1–18 |
| Seated Trunk Rotation ROM Toward D * Side (Degrees) | 73.32 | 14.07 | 1.35 | 40–105 |
| Seated Trunk Rotation ROM Toward ND ** Side (Degrees) | 77.92 | 13.87 | 1.33 | 40–125 |
| Shoulder External Rotation Strength D (kg) | 6.66 | 2.16 | 0.21 | 2.70–13.40 |
| Shoulder External Rotation Strength ND (kg) | 6.48 | 2.16 | 0.21 | 2.60–12.70 |
| Shoulder External Rotation Strength Deficit (Side-to-Side Difference%) | 11.05 | 7.67 | 0.74 | 0.10–33.70 |
| Shoulder Internal Rotation Strength D (kg) | 6.13 | 2.12 | 0.20 | 2.80–14.70 |
| Shoulder Internal Rotation Strength ND (kg) | 6.22 | 2.22 | 0.21 | 2.80–14.50 |
| Shoulder Internal Rotation Strength Deficit (Side-to-Side Difference%) | 11.01 | 7.80 | 0.75 | 0.10–33.70 |
| Hip Abduction Strength D (kg) | 12.77 | 7.99 | 0.77 | 5.6–87.30 |
| Hip Abduction Strength ND (kg) | 12.66 | 6.50 | 0.62 | 4.30–69.80 |
| Hip Abduction Strength Deficit (Side-to-Side Difference%) | 15.24 | 9.25 | 0.89 | 0.10–34 |
| Shoulder External Rotation Endurance D (%) | 78.37 | 15.98 | 1.53 | 9.10–96.50 |
| Shoulder External Rotation Endurance ND (%) | 72.31 | 21.11 | 2.02 | 2.40–96.90 |
| Shoulder External Rotation Endurance Deficit (Side-to-Side Difference%) | 14.77 | 17.35 | 1.66 | 0.40–96.60 |
| CKCUEST Score (Non-Dimensional) | 24.39 | 5.27 | 0.51 | 13–37 |
| CF FABS Score (Non-Dimensional) | 11.61 | 5.16 | 0.49 | 0–22 |
| Variable | Mean | Std. Deviation | Std. Error Mean | Range |
|---|---|---|---|---|
| VAS Pain Score | 5.15 | 1.69 | 0.38 | 3.0–9.0 |
| SDQ Score (%) | 38.13 | 16.83 | 3.76 | 12.50–87.50 |
| Days Out | 13.75 | 28.04 | 6.27 | 0–108 |
| Variable | T-Statistic | p-Value |
|---|---|---|
| Seated Trunk Rotation ROM Toward D Side (degrees) | −0.8749 | 0.384 |
| Seated Trunk Rotation ROM Toward ND Side (degrees) | −0.1206 | 0.904 |
| Shoulder External Rotation Strength D (kilograms) | 0.4344 | 0.665 |
| Shoulder External Rotation Strength ND (kilograms) | 0.8175 | 0.416 |
| Shoulder External Rotation Strength Deficit (side-to-side difference%) | −0.2284 | 0.820 |
| Shoulder Internal Rotation Strength D (kilograms) | 1.8113 | 0.073 |
| Shoulder Internal Rotation Strength ND (kilograms) | 1.4597 | 0.147 |
| Shoulder Internal Rotation Strength Deficit (side-to-side difference%) | −0.3061 | 0.760 |
| Hip Abduction Strength D (kilograms) | −0.2777 | 0.782 |
| Hip Abduction Strength ND (kilograms) | −0.2952 | 0.768 |
| Hip Abduction Strength Deficit (side-to-side difference%) | −2.2162 | 0.029 * |
| Shoulder External Rotation Endurance D (%) | −0.2963 | 0.768 |
| Shoulder External Rotation Endurance ND (%) | −1.6982 | 0.092 |
| Shoulder External Rotation Endurance Deficit (side-to-side difference%) | 2.6192 | 0.010 * |
| CKCUEST (nd) | −0.7786 | 0.438 |
| CF FABS Score (nd) | 1.0984 | 0.275 |
| Variable | T-Statistic | p-Value | |
|---|---|---|---|
| Epidemiological characteristics | Adequate Warm-Up | 611.0 | 0.029 ** |
| Adequate Recovery | 850.5 | 0.784 | |
| Prior Fitness Level | 903.5 | 0.464 | |
| DUE * Injured Areas | 663.5 | 0.153 | |
| NDUE * Injured Areas | 636.0 | 0.082 | |
| DLE * Injured Areas | 776.5 | 0.691 | |
| NDLE * Injured Areas | 742.0 | 0.442 | |
| Core Injured Areas | 663.5 | 0.153 | |
| All Injured Areas | 509.5 | 0.0097 ** | |
| CF FABS individual tests | Squat | 695.5 | 0.289 |
| Shoulder Rotation D | 825.0 | 0.962 | |
| Shoulder Rotation ND | 680.5 | 0.243 | |
| Wall Angel | 932.0 | 0.326 | |
| OHS | 688.0 | 0.262 | |
| Windmill D | 812.0 | 0.956 | |
| Windmill ND | 651.0 | 0.152 | |
| Sots Press | 684.0 | 0.241 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bakaraki, A.; Tsirogiannis, G.; Matzaroglou, C.; Fousekis, K.; Xergia, S.A.; Tsepis, E. Demographic, Epidemiological and Functional Profile Models of Greek CrossFit Athletes in Relation to Shoulder Injuries: A Prospective Study. J. Funct. Morphol. Kinesiol. 2025, 10, 278. https://doi.org/10.3390/jfmk10030278
Bakaraki A, Tsirogiannis G, Matzaroglou C, Fousekis K, Xergia SA, Tsepis E. Demographic, Epidemiological and Functional Profile Models of Greek CrossFit Athletes in Relation to Shoulder Injuries: A Prospective Study. Journal of Functional Morphology and Kinesiology. 2025; 10(3):278. https://doi.org/10.3390/jfmk10030278
Chicago/Turabian StyleBakaraki, Akrivi, George Tsirogiannis, Charalampos Matzaroglou, Konstantinos Fousekis, Sofia A. Xergia, and Elias Tsepis. 2025. "Demographic, Epidemiological and Functional Profile Models of Greek CrossFit Athletes in Relation to Shoulder Injuries: A Prospective Study" Journal of Functional Morphology and Kinesiology 10, no. 3: 278. https://doi.org/10.3390/jfmk10030278
APA StyleBakaraki, A., Tsirogiannis, G., Matzaroglou, C., Fousekis, K., Xergia, S. A., & Tsepis, E. (2025). Demographic, Epidemiological and Functional Profile Models of Greek CrossFit Athletes in Relation to Shoulder Injuries: A Prospective Study. Journal of Functional Morphology and Kinesiology, 10(3), 278. https://doi.org/10.3390/jfmk10030278