


Effects of Superimposed Blood Flow Restriction on Isokinetic Knee Extension


 and
and
Abstract
1. Introduction
2. Materials and Methods
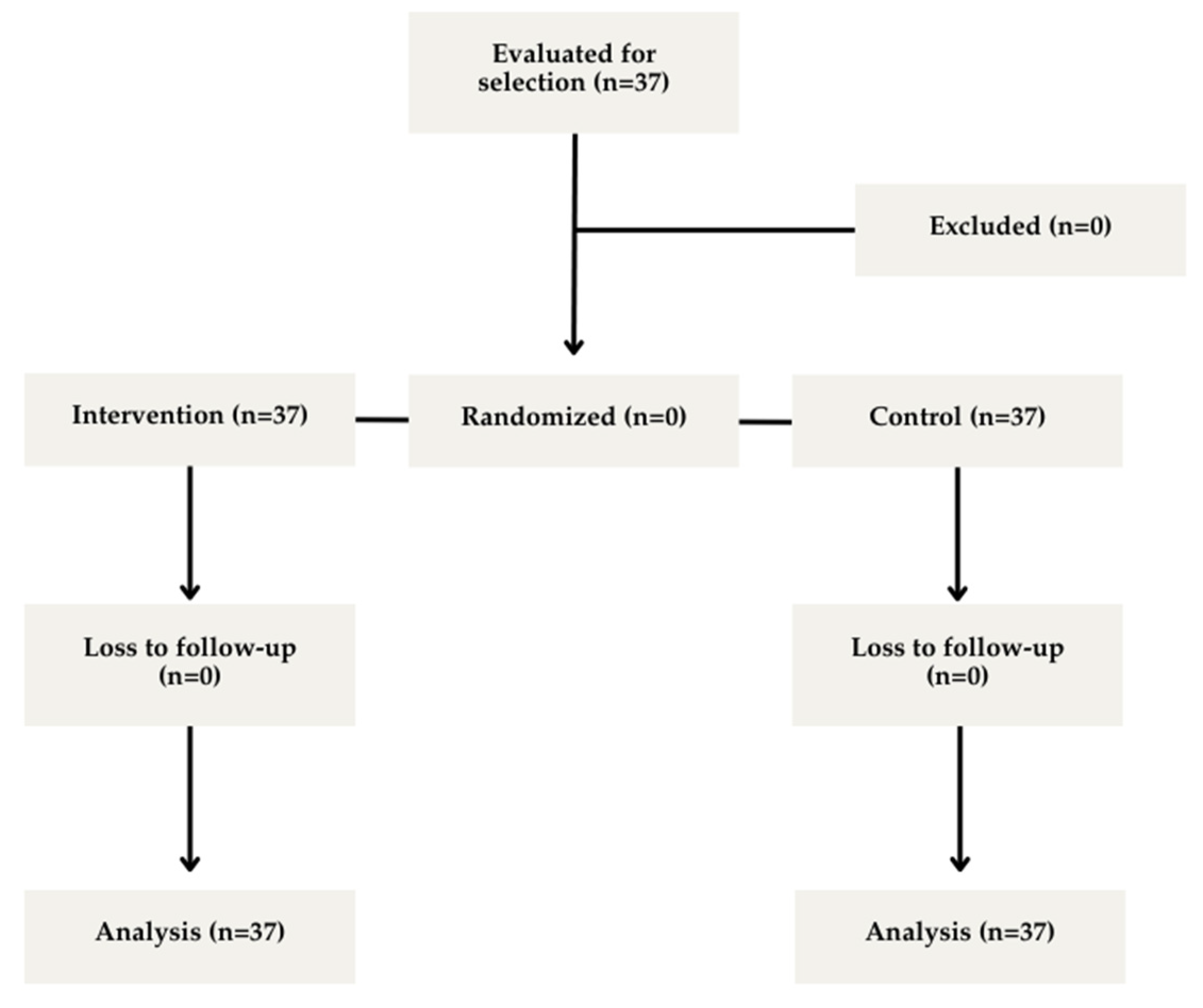
2.1. Participants
2.2. Experimental Design
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Centner, C.; Wiegel, P.; Gollhofer, A.; König, D. Effects of Blood Flow Restriction Training on Muscular Strength and Hypertrophy in Older Individuals: A Systematic Review and Meta-Analysis. Sports Med. 2019, 49, 95–108. [Google Scholar] [CrossRef] [PubMed]
- Grønfeldt, B.M.; Lindberg Nielsen, J.; Mieritz, R.M.; Lund, H.; Aagaard, P. Effect of Blood-flow Restricted Vs Heavy-load Strength Training on Muscle Strength: Systematic Review and Meta-analysis. Scand. J. Med. Sci. Sports 2020, 30, 837–848. [Google Scholar] [CrossRef] [PubMed]
- Lixandrão, M.E.; Ugrinowitsch, C.; Berton, R.; Vechin, F.C.; Conceição, M.S.; Damas, F.; Libardi, C.A.; Roschel, H. Magnitude of Muscle Strength and Mass Adaptations between High-Load Resistance Training Versus Low-Load Resistance Training Associated with Blood-Flow Restriction: A Systematic Review and Meta-Analysis. Sports Med. 2018, 48, 361–378. [Google Scholar] [CrossRef] [PubMed]
- Wortman, R.J.; Brown, S.M.; Savage-Elliott, I.; Finley, Z.J.; Mulcahey, M.K. Blood Flow Restriction Training for Athletes: A Systematic Review. Am. J. Sports Med. 2021, 49, 1938–1944. [Google Scholar] [CrossRef]
- Patterson, S.D.; Hughes, L.; Warmington, S.; Burr, J.; Scott, B.R.; Owens, J.; Abe, T.; Nielsen, J.L.; Libardi, C.A.; Laurentino, G. Blood Flow Restriction Exercise: Considerations of Methodology, Application, and Safety. Front. Physiol. 2019, 10, 448053. [Google Scholar]
- Pearson, S.J.; Hussain, S.R. A Review on the Mechanisms of Blood-Flow Restriction Resistance Training-Induced Muscle Hypertrophy. Sports Med. 2015, 45, 187–200. [Google Scholar] [CrossRef]
- Loenneke, J.P.; Wilson, J.M.; Marín, P.J.; Zourdos, M.C.; Bemben, M.G. Low Intensity Blood Flow Restriction Training: A Meta-Analysis. Eur. J. Appl. Physiol. 2012, 112, 1849–1859. [Google Scholar] [CrossRef]
- Wilk, M.; Krzysztofik, M.; Filip, A.; Szkudlarek, A.; Lockie, R.G.; Zajac, A. Does Post-Activation Performance Enhancement Occur during the Bench Press Exercise Under Blood Flow Restriction? Int. J. Environ. Res. Public Health 2020, 17, 3752. [Google Scholar] [CrossRef]
- Wilk, M.; Gepfert, M.; Krzysztofik, M.; Stastny, P.; Zajac, A.; Bogdanis, G.C. Acute Effects of Continuous and Intermittent Blood Flow Restriction on Movement Velocity during Bench Press Exercise Against Different Loads. Front. Physiol. 2020, 11, 569915. [Google Scholar] [CrossRef]
- De Arce, A.S.; Sánchez, J.C.; Camacho, F.F.; De Arriba, C.C.; Pellico, L.G. Análisis Isocinético De La Flexo-Extensión De La Rodilla Y Su Relación Con La Antropometría Del Miembro Inferior. Rehabilitación 2002, 36, 86–92. [Google Scholar] [CrossRef]
- Doughtie, B.; Calderon, D.; Cruz, G.; Hoppe, N.; Winchester, J.; Ortiz, A. Effectiveness of Blood Flow Restriction Training on Isokinetic Muscle Strength of the Quadriceps. Int. J. Exerc. Sci. Conf. Proc. 2021, 2, 68. [Google Scholar] [CrossRef]
- Rivera, P.M.; Proppe, C.E.; Gonzalez-Rojas, D.; Wizenberg, A.; Hill, E.C. Effects of Load Matched Isokinetic Versus Isotonic Blood Flow Restricted Exercise on Neuromuscular and Muscle Function. Eur. J. Sport Sci. 2023, 23, 1629–1637. [Google Scholar] [CrossRef]
- Tanaka, T.; Kubota, A.; Ozaki, H.; Nishio, H.; Nozu, S.; Takazawa, Y. Effect of Isokinetic Training with Blood Flow Restriction during Rest Interval Versus Exercise on Muscle Strength, Hypertrophy, and Perception: A Pilot Study. Juntendo Med. J. 2023, 69, 477–484. [Google Scholar] [CrossRef]
- Ríos, L.V. Manual de Ecografía Musculoesquelética; Médica Panamericana: Madrid, Spain, 2010. [Google Scholar]
- Laurentino, G.C.; Loenneke, J.P.; Mouser, J.G.; Buckner, S.L.; Counts, B.R.; Dankel, S.J.; Jessee, M.B.; Mattocks, K.T.; Iared, W.; Tavares, L.D. Validity of the Handheld Doppler to Determine Lower-Limb Blood Flow Restriction Pressure for Exercise Protocols. J. Strength Cond. Res. 2020, 34, 2693–2696. [Google Scholar] [CrossRef]
- Tanaka, H.; Monahan, K.D.; Seals, D.R. Age-Predicted Maximal Heart Rate Revisited. J. Am. Coll. Cardiol. 2001, 37, 153–156. [Google Scholar] [CrossRef]
- Jiménez, F.H.; Díaz, J.G.; Montes, J.V. Dinamometría Isocinética. Rehabilitación 2005, 39, 288–296. [Google Scholar] [CrossRef]
- Naclerio, F.J.; Jiménez, A.; Alvar, B.A.; Peterson, M.D. Assessing Strength and Power in Resistance Training. J. Hum. Sport Exerc. 2009, 4, 100–113. [Google Scholar] [CrossRef]
- Morales, J.; Sobonya, S. Use of Submaximal Repetition Tests for Predicting 1-RM Strength in Class Athletes. J. Strength Cond. Res. 1996, 10, 186–189. [Google Scholar]
- Rhea, M.R. Determining the Magnitude of Treatment Effects in Strength Training Research through the use of the Effect Size. J. Strength Cond. Res. 2004, 18, 918–920. [Google Scholar]
- Manini, T.M.; Clark, B.C. Blood Flow Restricted Exercise and Skeletal Muscle Health. Exerc. Sport Sci. Rev. 2009, 37, 78–85. [Google Scholar] [CrossRef]
- Kannus, P. Isokinetic Evaluation of Muscular Performance. Int. J. Sports Med. 1994, 15, S11–S18. [Google Scholar] [CrossRef] [PubMed]
- Bowman, E.N.; Elshaar, R.; Milligan, H.; Jue, G.; Mohr, K.; Brown, P.; Watanabe, D.M.; Limpisvasti, O. Proximal, Distal, and Contralateral Effects of Blood Flow Restriction Training on the Lower Extremities: A Randomized Controlled Trial. Sports Health 2019, 11, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Korkmaz, E.; Dönmez, G.; Uzuner, K.; Babayeva, N.; Torgutalp, Ş.Ş.; Özçakar, L. Effects of Blood Flow Restriction Training on Muscle Strength and Architecture. J. Strength Cond. Res. 2022, 36, 1396–1403. [Google Scholar] [CrossRef]
- Nielsen, J.L.; Frandsen, U.; Prokhorova, T.; Bech, R.D.; Nygaard, T.; Suetta, C.; Aagaard, P. Delayed Effect of Blood Flow-Restricted Resistance Training on Rapid Force Capacity. Med. Sci. Sports Exerc. 2017, 49, 1157–1167. [Google Scholar] [CrossRef] [PubMed]
- Freitas, E.D.; Galletti, B.R.; Koziol, K.J.; Miller, R.M.; Heishman, A.D.; Black, C.D.; Bemben, D.; Bemben, M.G. The Acute Physiological Responses to Traditional vs. Practical Blood Flow Restriction Resistance Exercise in Untrained Men and Women. Front. Physiol. 2020, 11, 577224. [Google Scholar] [CrossRef]
- Rawska, M.; Gepfert, M.; Mostowik, A.; Krzysztofik, M.; Wojdala, G.; Lulinska, A.; Wilk, M. Does Blood Flow Restriction Influence the Maximal Number of Repetitions Performed during the Bench Press? A Pilot Study. Balt. J. Health Phys. Act. 2019, 11, 2. [Google Scholar] [CrossRef]

{kind=link}
| Men | ||||
| Characteristics | N | Mean | SD | CI (95%) |
| Age (years) | 26 | 29.71 | 6.62 | 27.04–32.38 |
| Height (cm) | 26 | 177.71 | 6.97 | 174.89–180.53 |
| Weight (kg) | 26 | 83.04 | 12.75 | 77.89–88.19 |
| BMI (kg/m2) | 26 | 26.13 | 3.59 | 24.68–27.58 |
| % Fat Mass | 26 | 11.63 | 7.32 | 8.67–14.59 |
| % Lean Body Mass | 26 | 67.89 | 6.87 | 65.11–70.67 |
| Women | ||||
| Age (years) | 11 | 28.33 | 7.45 | 23.33–33.33 |
| Height (cm) | 11 | 163.03 | 8.64 | 157.23–168.83 |
| Weight (kg) | 11 | 67.5 | 13.81 | 58.22–76.78 |
| BMI (kg/m2) | 11 | 25.25 | 2.39 | 23.64–26.86 |
| % Fat Mass | 11 | 17.08 | 2.69 | 15.27–18.89 |
| % Lean Body Mass | 11 | 47.85 | 11.08 | 40.41–55.29 |
| 0% BFR | 40% BFR | 80% BFR | |||||||
|---|---|---|---|---|---|---|---|---|---|
| °/s | Median (IQR) | Median (IQR) | p0–40 | d0–40 | Median (IQR) | p0–80 | d0–80 | p40–80 | d40–80 |
| Peak Moment (Nm) | |||||||||
| 120 | 169.45 (55.07) | 161.75 (56.45) | 0.31 | 0.25 | 158.20 (40.90) | 0.13 | 0.37 | 0.51 | 0.09 |
| 210 | 127.75 (37.22) | 131.65 (31.17) | 0.43 | 0.06 | 129.35 (30.00) | 0.19 | 0.15 | 0.33 | 0.03 |
| 300 | 103.35 (36.90) | 109.25 (29.92) | 0.27 | 0.23 | 109.60 (32.52) | 0.26 | 0.13 | 0.39 | 0.09 |
| Average Power (w) | |||||||||
| 120 | 196.80 (64.07) | 193.00 (106.15) | 0.09 | 0.35 | 188.50 (80.15) | 0.35 | 0.41 | 0.18 | 0.01 |
| 210 | 236.25 (111.92) | 243.00 (119.80) | 0.16 | 0.03 | 236.95 (86.10) | 0.21 | 0.15 | 0.21 | 0.13 |
| 300 | 192.28 (110.48) | 250.35 (109.85) | 0.19 | 0.39 | 248.90 (101.10) | 0.27 | 0.37 | 0.29 | 0.02 |
| 0% BFR | 40% BFR | 80% BFR | |||||||
|---|---|---|---|---|---|---|---|---|---|
| °/s | Median (IQR) | Median (IQR) | p0–40 | d0–40 | Median (IQR) | p0–80 | d0–80 | p40–80 | d40–80 |
| Peak Moment (Nm) | |||||||||
| 120 | 113.30 (25.45) | 116.50 (32.00) | 0.13 | 0.39 | 109.09 (21.45) | 0.19 | 0.28 | 0.31 | 0.43 |
| 210 | 87.20 (14.45) | 82.80 (15.90) | 0.11 | 0.15 | 85.39 (13.95) | 0.26 | 0.22 | 0.21 | 0.05 |
| 300 | 74.40 (16.80) | 73.40 (14.35) | 0.20 | 0.24 | 72.90 (10.30) | 0.18 | 0.14 | 0.24 | 0.10 |
| Average Power (w) | |||||||||
| 120 | 143.60 (17.15) | 136.60 (18.50) | 0.23 | 0.19 | 127.80 (20.40) | 0.26 | 0.36 | 0.28 | 0.17 |
| 210 | 153.00 (42.25) | 147.80 (47.70) | 0.21 | 0.45 | 147.40 (33.05) | 0.10 | 0.16 | 0.19 | 0.31 |
| 300 | 149.50 (42.85) | 159.10 (34.90) | 0.27 | 0.23 | 156.90 (42.80) | 0.16 | 0.09 | 0.11 | 0.14 |
| F | p | Eta-Squared | |
|---|---|---|---|
| Peak Moment | 3.72 | 0.027 | 0.096 |
| Average Power | 2.91 | 0.029 | 0.077 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodrigo-Mallorca, D.; Mollá-Sanchis, J.; Chulvi-Medrano, I.; Franco-Grau, L.M. Effects of Superimposed Blood Flow Restriction on Isokinetic Knee Extension. J. Funct. Morphol. Kinesiol. 2025, 10, 167. https://doi.org/10.3390/jfmk10020167
Rodrigo-Mallorca D, Mollá-Sanchis J, Chulvi-Medrano I, Franco-Grau LM. Effects of Superimposed Blood Flow Restriction on Isokinetic Knee Extension. Journal of Functional Morphology and Kinesiology. 2025; 10(2):167. https://doi.org/10.3390/jfmk10020167
Chicago/Turabian StyleRodrigo-Mallorca, Darío, Joaquín Mollá-Sanchis, Iván Chulvi-Medrano, and Luis M. Franco-Grau. 2025. "Effects of Superimposed Blood Flow Restriction on Isokinetic Knee Extension" Journal of Functional Morphology and Kinesiology 10, no. 2: 167. https://doi.org/10.3390/jfmk10020167
APA StyleRodrigo-Mallorca, D., Mollá-Sanchis, J., Chulvi-Medrano, I., & Franco-Grau, L. M. (2025). Effects of Superimposed Blood Flow Restriction on Isokinetic Knee Extension. Journal of Functional Morphology and Kinesiology, 10(2), 167. https://doi.org/10.3390/jfmk10020167