

Physical Activity as a Central Pillar of Lifestyle Modification in the Management of Chronic Musculoskeletal Pain: A Narrative Review




Abstract
1. Introduction
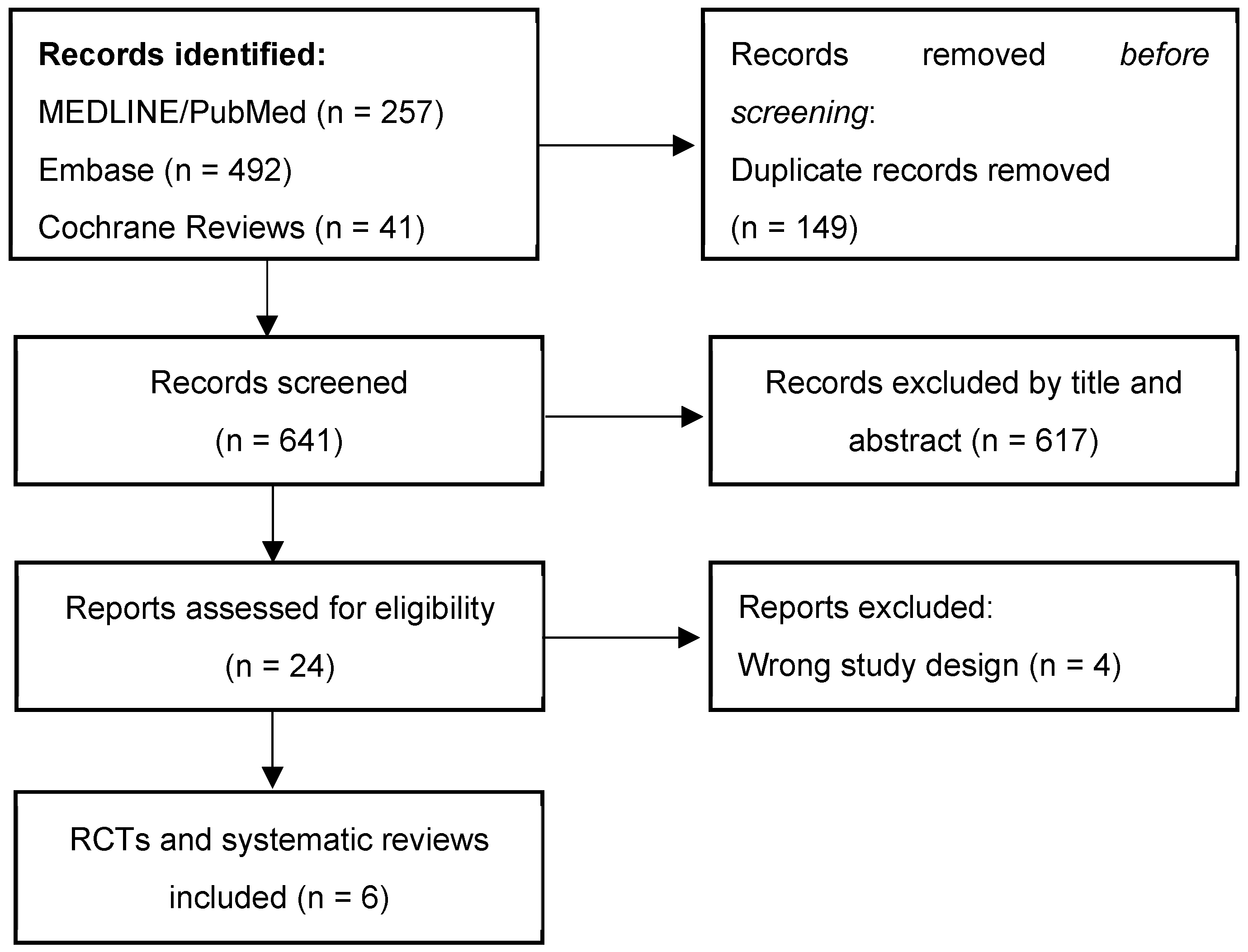
2. Materials and Methods
3. Results
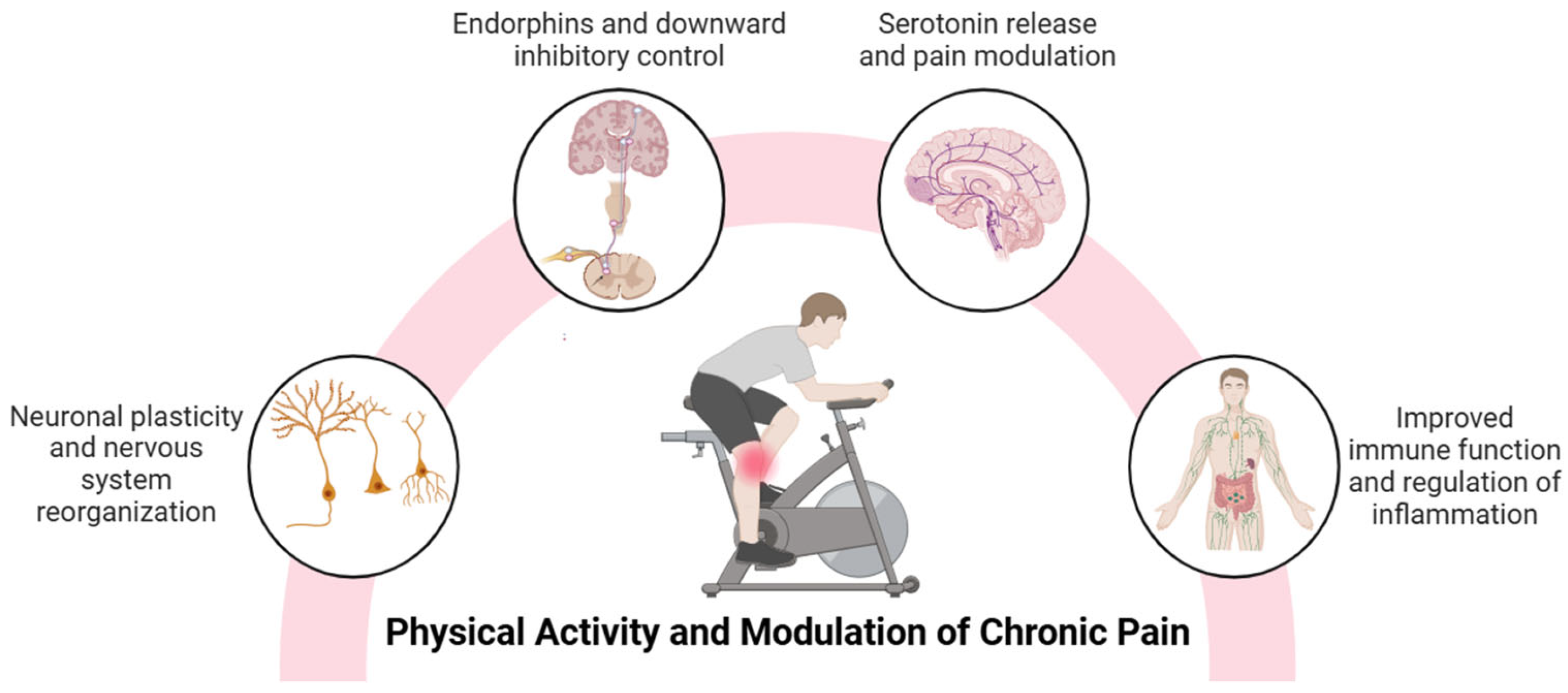
3.1. Physical Activity and Modulation of Chronic Pain
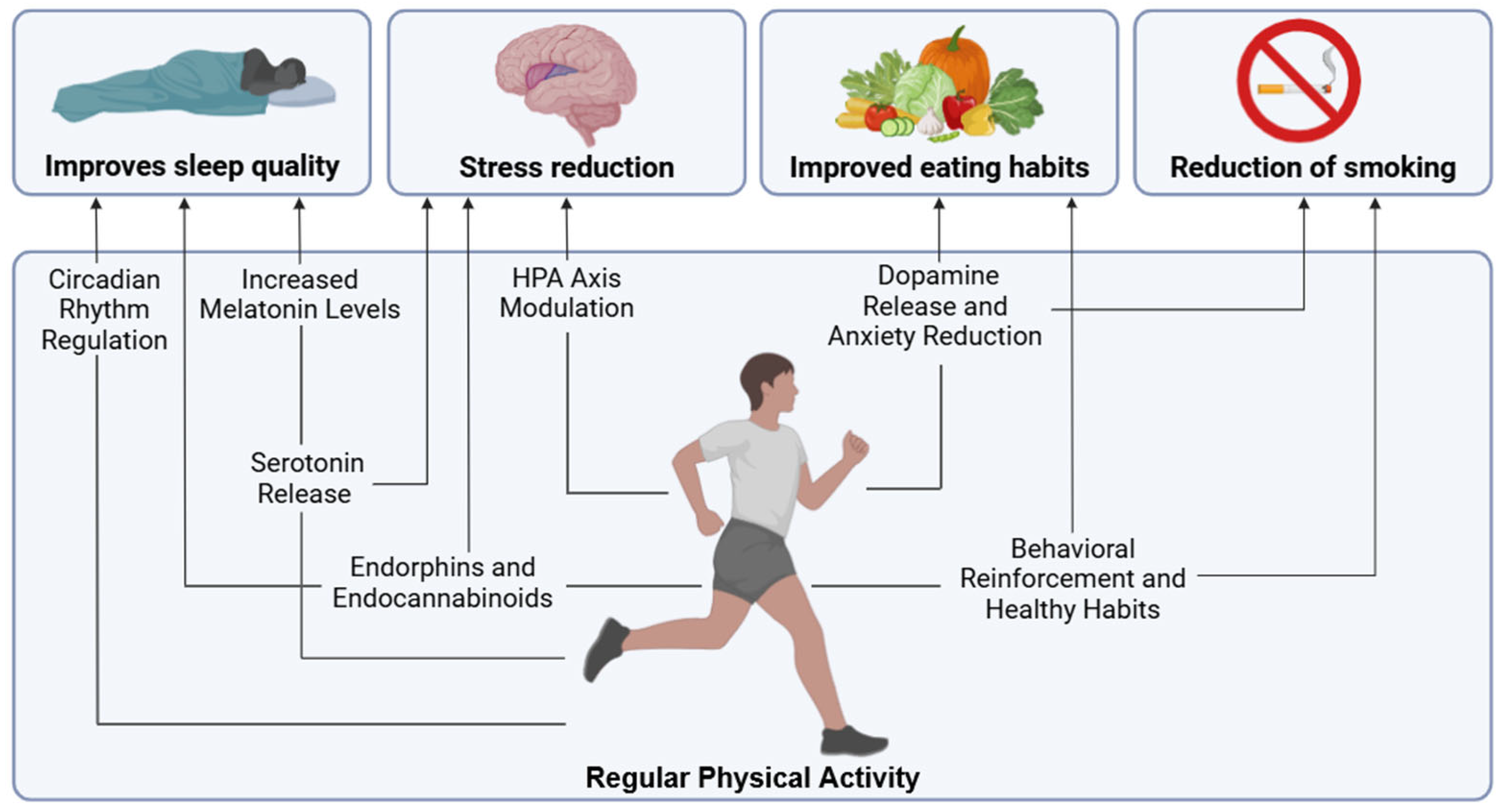
3.2. Physical Activity and Improvement of Sleep Quality
3.3. Physical Activity to Reduce Stress
3.4. Impact on Diet and Metabolic Regulation
3.5. Physical Activity and Smoking Reduction
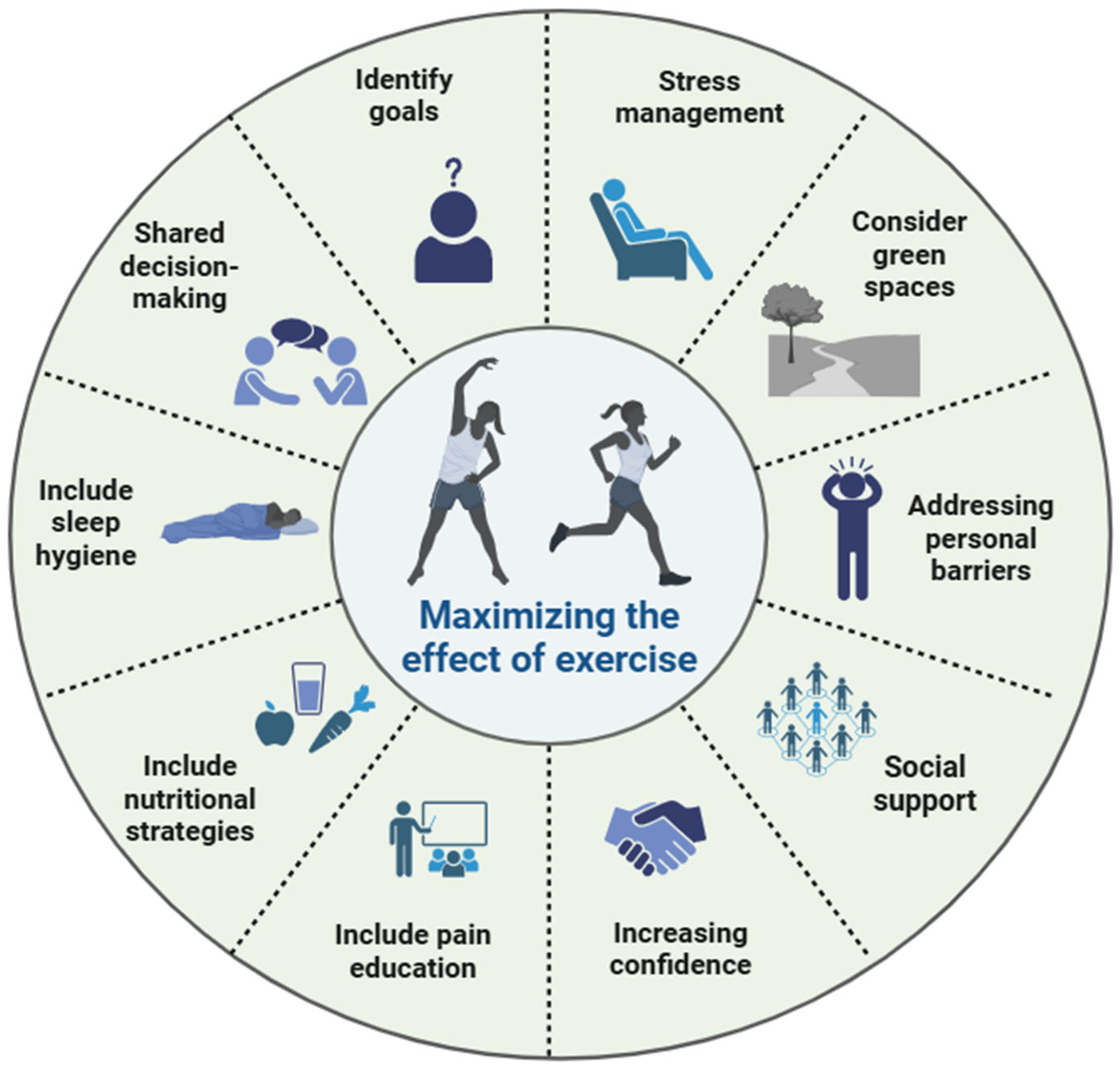
4. Comprehensive Intervention Proposal
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BDNF | Brain-derived neurotrophic factor |
| HPA | Hypothalamic–pituitary–adrenal |
| NMDA | N-Methyl-D-Aspartate |
| IL-6 | Interleukin-6 |
| IL-8 | Interleukin-8 |
| TNF-α | Tumor necrosis factor alpha |
| REM | Rapid eye movement |
| GLP-1 | Glucagon-like peptide-1 |
| CCK | Cholecystokinin |
| GABA | Gamma-aminobutyric acid |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pubmed/MEDLINE | |
|---|---|
| #1 | “chronic pain”[MeSH Terms] OR “chronic pain”[Title/Abstract] |
| #2 | “physical activity”[Title/Abstract] OR “exercise”[Title/Abstract] OR “exercise”[MeSH Terms] |
| #3 | “sleep”[MeSH Terms] OR “sleep”[Title/Abstract] OR “insomnia”[Title/Abstract] OR “stress”[Title/Abstract] OR “diet”[MeSH Terms] OR “diet”[Title/Abstract] OR “nutrition”[Title/Abstract] OR “smoking”[MeSH Terms] OR “smoking”[Title/Abstract] |
| #4 | #1 AND #2 AND #3 |
| #5 | Filters applied: Meta-Analysis, Randomized Controlled Trial, Review, Systematic Review. |
| Embase | |
| #1 | (‘chronic pain’:ab,ti) |
| #2 | (‘physical activity’:ab,ti OR exercise:ab,ti) |
| #3 | (sleep:ab,ti OR insomnia:ab,ti OR stress:ab,ti OR diet:ab,ti OR nutrition:ab,ti OR smoking:ab,ti) |
| #4 | #1 AND #2 AND #3 |
| #5 | #4 AND (‘article’/it OR ‘clinical trial’/it OR ‘review’/it) |
| Cochrane Reviews | |
| #1 | “chronic pain” |
| #2 | “physical activity” OR “exercise” |
| #3 | “sleep” OR “insomnia” OR “stress” OR “diet” OR “nutrition” OR “smoking” |
| #4 | #1 AND #2 AND #3 |
| Study | Design | Population | Topic | Type of Physical Activity | Main Findings |
|---|---|---|---|---|---|
| Chang et al. 2024 [53] | Systematic review with network meta-analysis (107 RCTs) | 8121 adults with chronic musculoskeletal pain | Sleep | Aerobic exercise, resistance training, mind–body (e.g., Tai Chi) | Exercise and mind–body exercise significantly improved sleep quality. |
| Navarro-Ledesma et al. 2024 [55] | Systematic review (17 RCTs) | Adults with chronic musculoskeletal pain (n = 591) | Sleep | Aerobic, resistance, Pilates, mind–body | Therapeutic exercise showed positive effects on sleep quality. More research is needed to determine optimal exercise parameters. |
| Calvo et al. 2023 [54] | Systematic review with meta-analysis (6 RCTs, 4 in meta-analysis) | 636 adults with chronic pain and sleep disturbance (mean age 54 ± 9.7) | Sleep | Neck stabilization, Pilates, walking, yoga, aerobics, supervised group exercise | Most interventions improved sleep and pain in the qualitative synthesis, but the meta-analysis showed no statistically significant effects. A correlation between pain and sleep improvements was noted. |
| Rotter et al. 2022 [85] | RCT | 55 adults (82% women) with chronic low back pain (VAS ≥ 40 mm) | Stress | Mindful walking (8 weekly 60 min guided sessions with mindfulness training and self-practice) | No statistically or clinically significant differences were found in terms of pain, stress, or function after 8 weeks. A slight improvement tendency was noted at 12 weeks. |
| Aykut and Şevgin 2025 [84] | RCT | 46 women (18–35) with premenstrual syndrome | Stress | Home-based Pilates (video-guided, 2x/week for 8 weeks) | Pilates significantly reduced symptoms of central sensitization, perceived stress, and pain in the intervention group compared to controls. |
| Verbrugghe et al. 2023 [86] | Secondary analysis of RCT | 51 adults (mean age 43.6) with chronic non-specific low back pain | Stress | High-intensity interval training: aerobic + resistance/core strength training | Exercise reduced perceived stress at 6 months. Stronger effects were observed in participants with clinically elevated CSI scores. A small but significant correlation with improvements in disability and pain was observed. |
| Messier et al. 2013 [103] | RCT (18 months, 3 arms) | 454 overweight/obese older adults (≥55 años) with knee osteoarthritis | Diet and inflammation | Aerobic + strength (3x/sem) combined with diet | The diet plus exercise group showed greater improvements in pain, function, IL-6 levels, physical quality of life, and weight loss than those with diet or exercise alone. |
References
- Cohen, S.P.; Vase, L.; Hooten, W.M. Chronic Pain: An Update on Burden, Best Practices, and New Advances. Lancet 2021, 397, 2082–2097. [Google Scholar] [CrossRef] [PubMed]
- Breivik, H.; Eisenberg, E.; O’Brien, T.; OPENMinds. The Individual and Societal Burden of Chronic Pain in Europe: The Case for Strategic Prioritisation and Action to Improve Knowledge and Availability of Appropriate Care. BMC Public Health 2013, 13, 1229. [Google Scholar] [CrossRef] [PubMed]
- GBD 2021 Other Musculoskeletal Disorders Collaborators Global, Regional, and National Burden of Other Musculoskeletal Disorders, 1990-2020, and Projections to 2050: A Systematic Analysis of the Global Burden of Disease Study 2021. Lancet Rheumatol. 2023, 5, e670–e682. [CrossRef] [PubMed]
- Macfarlane, G.J.; Barnish, M.S.; Jones, G.T. Persons with Chronic Widespread Pain Experience Excess Mortality: Longitudinal Results from UK Biobank and Meta-Analysis. Ann. Rheum. Dis. 2017, 76, 1815–1822. [Google Scholar] [CrossRef]
- Classification of Chronic Pain. Descriptions of Chronic Pain Syndromes and Definitions of Pain Terms. Prepared by the International Association for the Study of Pain, Subcommittee on Taxonomy. Pain Suppl. 1986, 3, S1–S226. [Google Scholar]
- Hemington, K.S.; Rogachov, A.; Cheng, J.C.; Bosma, R.L.; Kim, J.A.; Osborne, N.R.; Inman, R.D.; Davis, K.D. Patients with Chronic Pain Exhibit a Complex Relationship Triad between Pain, Resilience, and within- and Cross-Network Functional Connectivity of the Default Mode Network. Pain 2018, 159, 1621–1630. [Google Scholar] [CrossRef]
- Nijs, J.; George, S.Z.; Clauw, D.J.; Fernández-de-Las-Peñas, C.; Kosek, E.; Ickmans, K.; Fernández-Carnero, J.; Polli, A.; Kapreli, E.; Huysmans, E.; et al. Central Sensitisation in Chronic Pain Conditions: Latest Discoveries and Their Potential for Precision Medicine. Lancet Rheumatol. 2021, 3, e383–e392. [Google Scholar] [CrossRef]
- Nijs, J.; D’Hondt, E.; Clarys, P.; Deliens, T.; Polli, A.; Malfliet, A.; Coppieters, I.; Willaert, W.; Tumkaya Yilmaz, S.; Elma, Ö.; et al. Lifestyle and Chronic Pain across the Lifespan: An Inconvenient Truth? PM R. 2020, 12, 410–419. [Google Scholar] [CrossRef]
- Nijs, J.; Lahousse, A.; Malfliet, A. A Paradigm Shift from a Tissue- and Disease-Based Approach towards Multimodal Lifestyle Interventions for Chronic Pain: 5 Steps to Guide Clinical Reasoning. Braz. J. Phys. Ther. 2023, 27, 100556. [Google Scholar] [CrossRef]
- Nicholls, D.A. The Active Future for the Passive Therapist. J. Orthop. Sports Phys. Ther. 2021, 51, 318–321. [Google Scholar] [CrossRef]
- Fjeld, M.K.; Årnes, A.P.; Engdahl, B.; Morseth, B.; Hopstock, L.A.; Horsch, A.; Stubhaug, A.; Strand, B.H.; Nielsen, C.S.; Steingrímsdóttir, Ó.A. Consistent Pattern between Physical Activity Measures and Chronic Pain Levels: The Tromsø Study 2015 to 2016. Pain 2023, 164, 838–847. [Google Scholar] [CrossRef] [PubMed]
- Geneen, L.J.; Moore, R.A.; Clarke, C.; Martin, D.; Colvin, L.A.; Smith, B.H. Physical Activity and Exercise for Chronic Pain in Adults: An Overview of Cochrane Reviews. Cochrane Database Syst. Rev. 2017, 1, CD011279. [Google Scholar] [PubMed]
- Daenen, L.; Varkey, E.; Kellmann, M.; Nijs, J. Exercise, Not to Exercise, or How to Exercise in Patients with Chronic Pain? Applying Science to Practice. Clin. J. Pain 2015, 31, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.; Ning, J.; Chuter, V.H.; Taylor, J.B.; Christophe, D.; Meng, Z.; Xu, Y.; Jiang, L. Exercise Alone and Exercise Combined with Education Both Prevent Episodes of Low Back Pain and Related Absenteeism: Systematic Review and Network Meta-Analysis of Randomised Controlled Trials (RCTs) Aimed at Preventing Back Pain. Br. J. Sports Med. 2020, 54, 766–770. [Google Scholar] [CrossRef]
- Cotman, C.W.; Berchtold, N.C. Exercise: A Behavioral Intervention to Enhance Brain Health and Plasticity. Trends Neurosci. 2002, 25, 295–301. [Google Scholar] [CrossRef]
- Voss, M.W.; Vivar, C.; Kramer, A.F.; van Praag, H. Bridging Animal and Human Models of Exercise-Induced Brain Plasticity. Trends Cogn. Sci. 2013, 17, 525–544. [Google Scholar] [CrossRef]
- Coelho, F.M.; Pereira, D.S.; Lustosa, L.P.; Silva, J.P.; Dias, J.M.D.; Dias, R.C.D.; Queiroz, B.Z.; Teixeira, A.L.; Teixeira, M.M.; Pereira, L.S.M. Physical Therapy Intervention (PTI) Increases Plasma Brain-Derived Neurotrophic Factor (BDNF) Levels in Non-Frail and Pre-Frail Elderly Women. Arch. Gerontol. Geriatr. 2012, 54, 415–420. [Google Scholar] [CrossRef]
- Ateaque, S.; Merkouris, S.; Barde, Y.-A. Neurotrophin Signalling in the Human Nervous System. Front. Mol. Neurosci. 2023, 16, 1225373. [Google Scholar] [CrossRef]
- Zarza-Rebollo, J.A.; López-Isac, E.; Rivera, M.; Gómez-Hernández, L.; Pérez-Gutiérrez, A.M.; Molina, E. The Relationship between BDNF and Physical Activity on Depression. Prog. Neuropsychopharmacol. Biol. Psychiatry 2024, 134, 111033. [Google Scholar] [CrossRef]
- Da Silva Santos, R.; Galdino, G. Endogenous Systems Involved in Exercise-Induced Analgesia. J. Physiol. Pharmacol. 2018, 69, 3–13. [Google Scholar]
- Zhou, Y.-S.; Meng, F.-C.; Cui, Y.; Xiong, Y.-L.; Li, X.-Y.; Meng, F.-B.; Niu, Z.-X.; Zheng, J.-X.; Quan, Y.-Q.; Wu, S.-X.; et al. Regular Aerobic Exercise Attenuates Pain and Anxiety in Mice by Restoring Serotonin-Modulated Synaptic Plasticity in the Anterior Cingulate Cortex. Med. Sci. Sports Exerc. 2022, 54, 566–581. [Google Scholar] [CrossRef] [PubMed]
- Puts, S.; Liberman, K.; Leysen, L.; Forti, L.; Muyldermans, E.; Vaes, P.; Nijs, J.; Beckwée, D.; Bautmans, I. Exercise-Induced Effects on Inflammatory Markers and Brain-Derived Neurotrophic Factor in Patients with Knee Osteoarthritis. A Systematic Review with Meta-Analysis. Exerc. Immunol. Rev. 2023, 29, 22–53. [Google Scholar] [PubMed]
- Sluka, K.A.; Danielson, J.; Rasmussen, L.; DaSilva, L.F. Exercise-Induced Pain Requires NMDA Receptor Activation in the Medullary Raphe Nuclei. Med. Sci. Sports Exerc. 2012, 44, 420–427. [Google Scholar] [CrossRef] [PubMed]
- Ji, R.-R.; Nackley, A.; Huh, Y.; Terrando, N.; Maixner, W. Neuroinflammation and Central Sensitization in Chronic and Widespread Pain. Anesthesiology 2018, 129, 343–366. [Google Scholar] [CrossRef]
- Loggia, M.L.; Chonde, D.B.; Akeju, O.; Arabasz, G.; Catana, C.; Edwards, R.R.; Hill, E.; Hsu, S.; Izquierdo-Garcia, D.; Ji, R.-R.; et al. Evidence for Brain Glial Activation in Chronic Pain Patients. Brain 2015, 138, 604–615. [Google Scholar] [CrossRef]
- He, W.; Wang, Y.; Zhang, Y.; Zhang, Y.; Zhou, J. The Status of Knowledge on Migraines: The Role of Microglia. J. Neuroimmunol. 2023, 381, 578118. [Google Scholar] [CrossRef]
- Grace, P.M.; Hutchinson, M.R.; Maier, S.F.; Watkins, L.R. Pathological Pain and the Neuroimmune Interface. Nat. Rev. Immunol. 2014, 14, 217–231. [Google Scholar] [CrossRef]
- Omoigui, S. The Biochemical Origin of Pain—Proposing a New Law of Pain: The Origin of All Pain Is Inflammation and the Inflammatory Response. Part 1 of 3—A Unifying Law of Pain. Med. Hypotheses 2007, 69, 70–82. [Google Scholar] [CrossRef]
- Zhang, J.-M.; An, J. Cytokines, Inflammation, and Pain. Int. Anesthesiol. Clin. 2007, 45, 27–37. [Google Scholar] [CrossRef]
- Wang, H.; Moser, M.; Schiltenwolf, M.; Buchner, M. Circulating Cytokine Levels Compared to Pain in Patients with Fibromyalgia—A Prospective Longitudinal Study over 6 Months. J. Rheumatol. 2008, 35, 1366–1370. [Google Scholar]
- Mendieta, D.; De la Cruz-Aguilera, D.L.; Barrera-Villalpando, M.I.; Becerril-Villanueva, E.; Arreola, R.; Hernández-Ferreira, E.; Pérez-Tapia, S.M.; Pérez-Sánchez, G.; Garcés-Alvarez, M.E.; Aguirre-Cruz, L.; et al. IL-8 and IL-6 Primarily Mediate the Inflammatory Response in Fibromyalgia Patients. J. Neuroimmunol. 2016, 290, 22–25. [Google Scholar] [CrossRef] [PubMed]
- González-Álvarez, M.E.; Riquelme-Aguado, V.; González-Pérez, Á.; Murillo-Llergo, R.; Manjón-Olmedillas, M.; Turroni, S.; Rossettini, G.; Villafañe, J.H. Association Between Systemic Neuroinflammation, Pain Perception and Clinical Status in Fibromyalgia Patients: Cross-Sectional Study. Cells 2024, 13, 1719. [Google Scholar] [CrossRef] [PubMed]
- Puts, S.; Njemini, R.; Bilterys, T.; Lefeber, N.; Scheerlinck, T.; Nijs, J.; Beckwée, D.; Bautmans, I. Linking Intra-Articular Inflammatory Biomarkers with Peripheral and Central Sensitization in Late-Stage Knee Osteoarthritis Pain: A Pilot Study. J. Clin. Med. 2024, 13, 5212. [Google Scholar] [CrossRef]
- Scheffer, D. da L.; Latini, A. Exercise-Induced Immune System Response: Anti-Inflammatory Status on Peripheral and Central Organs. Biochim. Biophys. Acta Mol. Basis Dis. 2020, 1866, 165823. [Google Scholar] [CrossRef]
- Chow, L.S.; Gerszten, R.E.; Taylor, J.M.; Pedersen, B.K.; van Praag, H.; Trappe, S.; Febbraio, M.A.; Galis, Z.S.; Gao, Y.; Haus, J.M.; et al. Exerkines in Health, Resilience and Disease. Nat. Rev. Endocrinol. 2022, 18, 273–289. [Google Scholar] [CrossRef]
- Suso-Martí, L.; Núñez-Cortés, R.; Sánchez-Sabater, A.; Garrigós-Pedrón, M.; Ferrer-Sargues, F.J.; López-Bueno, R.; Calatayud, J. Effects of Exercise-Based Interventions on Inflammatory Markers in Patients with Fibromyalgia: A Systematic Review and Meta-Analysis. Semin. Arthritis Rheum. 2024, 65, 152377. [Google Scholar] [CrossRef]
- Hadjispyrou, S.; Dinas, P.C.; Delitheos, S.M.; Koumprentziotis, I.-A.; Chryssanthopoulos, C.; Philippou, A. The Effect of High-Intensity Interval Training on Mitochondrial-Associated Indices in Overweight and Obese Adults: A Systematic Review and Meta-Analysis. Front. Biosci. (Landmark Ed.) 2023, 28, 281. [Google Scholar] [CrossRef]
- Azizbeigi, K.; Azarbayjani, M.A.; Atashak, S.; Stannard, S.R. Effect of Moderate and High Resistance Training Intensity on Indices of Inflammatory and Oxidative Stress. Res. Sports Med. 2015, 23, 73–87. [Google Scholar] [CrossRef]
- Runge, N.; Ahmed, I.; Saueressig, T.; Perea, J.; Labie, C.; Mairesse, O.; Nijs, J.; Malfliet, A.; Verschueren, S.; Van Assche, D.; et al. The Bidirectional Relationship between Sleep Problems and Chronic Musculoskeletal Pain: A Systematic Review with Meta-Analysis. Pain 2024, 165, 2455–2467. [Google Scholar] [CrossRef]
- Bilterys, T.; Siffain, C.; De Maeyer, I.; Van Looveren, E.; Mairesse, O.; Nijs, J.; Meeus, M.; Ickmans, K.; Cagnie, B.; Goubert, D.; et al. Associates of Insomnia in People with Chronic Spinal Pain: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 3175. [Google Scholar] [CrossRef]
- Whibley, D.; AlKandari, N.; Kristensen, K.; Barnish, M.; Rzewuska, M.; Druce, K.L.; Tang, N.K.Y. Sleep and Pain: A Systematic Review of Studies of Mediation. Clin. J. Pain 2019, 35, 544–558. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Laksono, I.; Selvanathan, J.; Saripella, A.; Nagappa, M.; Pham, C.; Englesakis, M.; Peng, P.; Morin, C.M.; Chung, F. Prevalence of Sleep Disturbances in Patients with Chronic Non-Cancer Pain: A Systematic Review and Meta-Analysis. Sleep Med. Rev. 2021, 57, 101467. [Google Scholar] [CrossRef] [PubMed]
- Haack, M.; Simpson, N.; Sethna, N.; Kaur, S.; Mullington, J. Sleep Deficiency and Chronic Pain: Potential Underlying Mechanisms and Clinical Implications. Neuropsychopharmacology 2020, 45, 205–216. [Google Scholar] [CrossRef]
- Nijs, J.; Loggia, M.L.; Polli, A.; Moens, M.; Huysmans, E.; Goudman, L.; Meeus, M.; Vanderweeën, L.; Ickmans, K.; Clauw, D. Sleep Disturbances and Severe Stress as Glial Activators: Key Targets for Treating Central Sensitization in Chronic Pain Patients? Expert. Opin. Ther. Targets 2017, 21, 817–826. [Google Scholar] [CrossRef]
- Navarro-Ledesma, S.; Gonzalez-Muñoz, A.; García Ríos, M.C.; de la Serna, D.; Pruimboom, L. Circadian Variation of Blood Pressure in Patients with Chronic Musculoskeletal Pain: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19. [Google Scholar] [CrossRef]
- Segal, J.P.; Tresidder, K.A.; Bhatt, C.; Gilron, I.; Ghasemlou, N. Circadian Control of Pain and Neuroinflammation. J. Neurosci. Res. 2018, 96, 1002–1020. [Google Scholar] [CrossRef]
- Herrero Babiloni, A.; De Koninck, B.P.; Beetz, G.; De Beaumont, L.; Martel, M.O.; Lavigne, G.J. Sleep and Pain: Recent Insights, Mechanisms, and Future Directions in the Investigation of This Relationship. J. Neural Transm. 2020, 127, 647–660. [Google Scholar] [CrossRef]
- Masruha, M.R.; Lin, J.; de Souza Vieira, D.S.; Minett, T.S.C.; Cipolla-Neto, J.; Zukerman, E.; Vilanova, L.C.P.; Peres, M.F.P. Urinary 6-Sulphatoxymelatonin Levels Are Depressed in Chronic Migraine and Several Comorbidities. Headache 2010, 50, 413–419. [Google Scholar] [CrossRef]
- Nijs, J.; Mairesse, O.; Neu, D.; Leysen, L.; Danneels, L.; Cagnie, B.; Meeus, M.; Moens, M.; Ickmans, K.; Goubert, D. Sleep Disturbances in Chronic Pain: Neurobiology, Assessment, and Treatment in Physical Therapist Practice. Phys. Ther. 2018, 98, 325–335. [Google Scholar] [CrossRef]
- Vanderlinden, J.; Boen, F.; van Uffelen, J.G.Z. Effects of Physical Activity Programs on Sleep Outcomes in Older Adults: A Systematic Review. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 11. [Google Scholar] [CrossRef]
- Dolezal, B.A.; Neufeld, E.V.; Boland, D.M.; Martin, J.L.; Cooper, C.B. Interrelationship between Sleep and Exercise: A Systematic Review. Adv. Prev. Med. 2017, 2017, 1364387. [Google Scholar] [PubMed]
- Kelley, G.A.; Kelley, K.S. Exercise and Sleep: A Systematic Review of Previous Meta-Analyses. J. Evid.-Based. Med. 2017, 10, 26–36. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.R.; Cheung, Y.K.; Sharma, S.; Li, S.X.; Tao, R.R.; Lee, J.L.C.; Sun, E.R.; Pinto, S.M.; Zhou, Z.; Fong, H.; et al. Comparative Effectiveness of Non-Pharmacological Interventions on Sleep in Individuals with Chronic Musculoskeletal Pain: A Systematic Review with Network Meta-Analysis. Sleep Med. Rev. 2024, 73, 101867. [Google Scholar] [CrossRef]
- Calvo, S.; González, C.; Lapuente-Hernández, D.; Cuenca-Zaldívar, J.N.; Herrero, P.; Gil-Calvo, M. Are Physical Therapy Interventions Effective in Improving Sleep in People with Chronic Pain? A Systematic Review and Multivariate Meta-Analysis. Sleep Med. 2023, 111, 70–81. [Google Scholar] [CrossRef]
- Navarro-Ledesma, S.; Hamed-Hamed, D.; Gonzalez-Muñoz, A.; Pruimboom, L. Impact of Physical Therapy Techniques and Common Interventions on Sleep Quality in Patients with Chronic Pain: A Systematic Review. Sleep Med. Rev. 2024, 76, 101937. [Google Scholar] [CrossRef]
- Chennaoui, M.; Arnal, P.J.; Sauvet, F.; Léger, D. Sleep and Exercise: A Reciprocal Issue? Sleep Med. Rev. 2015, 20, 59–72. [Google Scholar] [CrossRef]
- Uchida, S.; Shioda, K.; Morita, Y.; Kubota, C.; Ganeko, M.; Takeda, N. Exercise Effects on Sleep Physiology. Front. Neurol. 2012, 3, 48. [Google Scholar] [CrossRef]
- Buman, M.P.; King, A.C. Exercise as a Treatment to Enhance Sleep. Am. J. Lifestyle Med. 2010, 4, 500–514. [Google Scholar] [CrossRef]
- Santos, R.V.T.; Tufik, S.; De Mello, M.T. Exercise, Sleep and Cytokines: Is There a Relation? Sleep Med. Rev. 2007, 11, 231–239. [Google Scholar] [CrossRef]
- Zagaar, M.; Dao, A.; Alhaider, I.; Alkadhi, K. Regular Treadmill Exercise Prevents Sleep Deprivation-Induced Disruption of Synaptic Plasticity and Associated Signaling Cascade in the Dentate Gyrus. Mol. Cell. Neurosci. 2013, 56, 375–383. [Google Scholar] [CrossRef]
- Nay, K.; Smiles, W.J.; Kaiser, J.; McAloon, L.M.; Loh, K.; Galic, S.; Oakhill, J.S.; Gundlach, A.L.; Scott, J.W. Molecular Mechanisms Underlying the Beneficial Effects of Exercise on Brain Function and Neurological Disorders. Int. J. Mol. Sci. 2021, 22, 4052. [Google Scholar] [CrossRef] [PubMed]
- Deuschle, M.; Schredl, M.; Wisch, C.; Schilling, C.; Gilles, M.; Geisel, O.; Hellweg, R. Serum Brain-Derived Neurotrophic Factor (BDNF) in Sleep-Disordered Patients: Relation to Sleep Stage N3 and Rapid Eye Movement (REM) Sleep across Diagnostic Entities. J. Sleep Res. 2018, 27, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Ditmer, M.; Gabryelska, A.; Turkiewicz, S.; Białasiewicz, P.; Małecka-Wojciesko, E.; Sochal, M. Sleep Problems in Chronic Inflammatory Diseases: Prevalence, Treatment, and New Perspectives: A Narrative Review. J. Clin. Med. 2021, 11, 67. [Google Scholar] [CrossRef]
- Lee, H.; Kim, S.; Kim, D. Effects of Exercise with or without Light Exposure on Sleep Quality and Hormone Reponses. J. Exerc. Nutr. Biochem. 2014, 18, 293–299. [Google Scholar] [CrossRef]
- Lee, B.H.; Hille, B.; Koh, D.-S. Serotonin Modulates Melatonin Synthesis as an Autocrine Neurotransmitter in the Pineal Gland. Proc. Natl. Acad. Sci. USA 2021, 118, e2113852118. [Google Scholar] [CrossRef]
- Xie, Z.; Chen, F.; Li, W.A.; Geng, X.; Li, C.; Meng, X.; Feng, Y.; Liu, W.; Yu, F. A Review of Sleep Disorders and Melatonin. Neurol. Res. 2017, 39, 559–565. [Google Scholar] [CrossRef]
- Kim, N.; Ka, S.; Park, J. Effects of Exercise Timing and Intensity on Physiological Circadian Rhythm and Sleep Quality: A Systematic Review. Phys. Act. Nutr. 2023, 27, 52–63. [Google Scholar] [CrossRef]
- Secondulfo, C.; Mazzeo, F.; Pastorino, G.M.G.; Vicidomini, A.; Meccariello, R.; Operto, F.F. Opioid and Cannabinoid Systems in Pain: Emerging Molecular Mechanisms and Use in Clinical Practice, Health, and Fitness. Int. J. Mol. Sci. 2024, 25, 9407. [Google Scholar] [CrossRef]
- Matei, D.; Trofin, D.; Iordan, D.A.; Onu, I.; Condurache, I.; Ionite, C.; Buculei, I. The Endocannabinoid System and Physical Exercise. Int. J. Mol. Sci. 2023, 24, 1989. [Google Scholar] [CrossRef]
- Desai, D.; Momin, A.; Hirpara, P.; Jha, H.; Thaker, R.; Patel, J. Exploring the Role of Circadian Rhythms in Sleep and Recovery: A Review Article. Cureus 2024, 16, e61568. [Google Scholar] [CrossRef]
- Vlahoyiannis, A.; Aphamis, G.; Eddin, D.A.; Giannaki, C.D. The Effect of Evening Cycling at Different Intensities on Sleep in Healthy Young Adults with Intermediate Chronobiological Phenotype: A Randomized, Cross-over Trial. J. Sports Sci. 2021, 39, 192–199. [Google Scholar] [CrossRef]
- Thomas, C.; Jones, H.; Whitworth-Turner, C.; Louis, J. High-Intensity Exercise in the Evening Does Not Disrupt Sleep in Endurance Runners. Eur. J. Appl. Physiol. 2020, 120, 359–368. [Google Scholar] [CrossRef] [PubMed]
- Stutz, J.; Eiholzer, R.; Spengler, C.M. Effects of Evening Exercise on Sleep in Healthy Participants: A Systematic Review and Meta-Analysis. Sports Med. 2019, 49, 269–287. [Google Scholar] [CrossRef] [PubMed]
- Skarpsno, E.S.; Mork, P.J.; Nilsen, T.I.L.; Jørgensen, M.B.; Holtermann, A. The Joint Association of Musculoskeletal Pain and Domains of Physical Activity with Sleep Problems: Cross-Sectional Data from the DPhacto Study, Denmark. Int. Arch. Occup. Environ. Health 2019, 92, 491–499. [Google Scholar] [CrossRef] [PubMed]
- Malfliet, A.; De Baets, L.; Bilterys, T.; Van Looveren, E.; Mairesse, O.; Cagnie, B.; Meeus, M.; Moens, M.; Goubert, D.; Munneke, W.; et al. Cognitive Behavioral Therapy for Insomnia in Pain Management for Nonspecific Chronic Spinal Pain: A Randomized Clinical Trial. JAMA Netw. Open 2024, 7, e2425856. [Google Scholar] [CrossRef]
- Wyns, A.; Hendrix, J.; Lahousse, A.; De Bruyne, E.; Nijs, J.; Godderis, L.; Polli, A. The Biology of Stress Intolerance in Patients with Chronic Pain-State of the Art and Future Directions. J. Clin. Med. 2023, 12, 2245. [Google Scholar] [CrossRef]
- Gaab, J.; Baumann, S.; Budnoik, A.; Gmünder, H.; Hottinger, N.; Ehlert, U. Reduced Reactivity and Enhanced Negative Feedback Sensitivity of the Hypothalamus-Pituitary-Adrenal Axis in Chronic Whiplash-Associated Disorder. Pain 2005, 119, 219–224. [Google Scholar] [CrossRef]
- Heuser, I.; Lammers, C.-H. Stress and the Brain. Neurobiol. Aging 2003, 24 (Suppl. 1), S69–S76; discussion S81–S82. [Google Scholar] [CrossRef]
- Nijs, J.; Wyns, A.; Hendrix, J. The Importance of Stress in the Paradigm Shift from a Tissue- and Disease-Based Pain Management Approach towards Multimodal Lifestyle Interventions for Chronic Pain. Braz. J. Phys. Ther. 2024, 28, 101061. [Google Scholar] [CrossRef]
- Van Oosterwijck, J.; Marusic, U.; De Wandele, I.; Meeus, M.; Paul, L.; Lambrecht, L.; Moorkens, G.; Danneels, L.; Nijs, J. Reduced Parasympathetic Reactivation during Recovery from Exercise in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. J. Clin. Med. 2021, 10, 4527. [Google Scholar] [CrossRef]
- Katayama, K.; Saito, M. Muscle Sympathetic Nerve Activity during Exercise. J. Physiol. Sci. 2019, 69, 589–598. [Google Scholar] [CrossRef] [PubMed]
- Whitworth, J.A.; Williamson, P.M.; Mangos, G.; Kelly, J.J. Cardiovascular Consequences of Cortisol Excess. Vasc. Health Risk Manag. 2005, 1, 291–299. [Google Scholar] [CrossRef]
- Nowacka-Chmielewska, M.; Grabowska, K.; Grabowski, M.; Meybohm, P.; Burek, M.; Małecki, A. Running from Stress: Neurobiological Mechanisms of Exercise-Induced Stress Resilience. Int. J. Mol. Sci. 2022, 23, 13348. [Google Scholar] [CrossRef]
- Aykut, Ş.; Sevgin, O. Effect of Video-Based Exercise on Premenstrual Symptoms: A Randomized Controlled Trial. Ginekol. Pol. 2025, 96, 102–108. [Google Scholar] [CrossRef]
- Rotter, G.; Ortiz, M.; Binting, S.; Tomzik, J.; Reese, F.; Roll, S.; Brinkhaus, B.; Teut, M. Mindful Walking in Patients with Chronic Low Back Pain: A Randomized Controlled Trial. J. Integr. Complement. Med. 2022, 28, 474–483. [Google Scholar] [CrossRef]
- Verbrugghe, J.; Agten, A.; Stevens, S.; Vandenabeele, F.; Roussel, N.; Verbunt, J.; Goossens, N.; Timmermans, A. High Intensity Training Improves Symptoms of Central Sensitization at Six-Month Follow-up in Persons with Chronic Nonspecific Low Back Pain: Secondary Analysis of a Randomized Controlled Trial. Braz. J. Phys. Ther. 2023, 27, 100496. [Google Scholar] [CrossRef]
- Stanhope, J.; Breed, M.F.; Weinstein, P. Exposure to Greenspaces Could Reduce the High Global Burden of Pain. Environ. Res. 2020, 187, 109641. [Google Scholar] [CrossRef]
- Nijs, J.; Mostaqim, K.; Oostendorp, R. Exercise Therapy and Physical Activity in the Paradigm Shift from a Tissue- and Disease-Based Pain Management Approach towards Multimodal Lifestyle Interventions for Chronic Pain. Braz. J. Phys. Ther. 2024, 28, 101101. [Google Scholar] [CrossRef]
- Hasenbring, M.I.; Andrews, N.E.; Ebenbichler, G. Overactivity in Chronic Pain, the Role of Pain-Related Endurance and Neuromuscular Activity: An Interdisciplinary, Narrative Review. Clin. J. Pain 2020, 36, 162–171. [Google Scholar] [CrossRef]
- Hasenbring, M.I.; Hallner, D.; Klasen, B.; Streitlein-Böhme, I.; Willburger, R.; Rusche, H. Pain-Related Avoidance versus Endurance in Primary Care Patients with Subacute Back Pain: Psychological Characteristics and Outcome at a 6-Month Follow-Up. Pain 2012, 153, 211–217. [Google Scholar] [CrossRef]
- Elma, Ö.; Yilmaz, S.T.; Deliens, T.; Coppieters, I.; Clarys, P.; Nijs, J.; Malfliet, A. Do Nutritional Factors Interact with Chronic Musculoskeletal Pain? A Systematic Review. J. Clin. Med. 2020, 9, 702. [Google Scholar] [CrossRef]
- Elma, Ö.; Brain, K.; Dong, H.-J. The Importance of Nutrition as a Lifestyle Factor in Chronic Pain Management: A Narrative Review. J. Clin. Med. 2022, 11, 5950. [Google Scholar] [CrossRef]
- Zhou, R.; Zhang, L.; Sun, Y.; Yan, J.; Jiang, H. Causal Associations between Dietary Habits and Chronic Pain: A Two-Sample Mendelian Randomization Study. Nutrients 2023, 15, 3709. [Google Scholar] [CrossRef] [PubMed]
- Hodges, S.; Guler, S.; Sacca, V.; Vangel, M.; Orr, S.; Pace-Schott, E.; Wen, Y.; Ge, T.; Kong, J. Associations among Acute and Chronic Musculoskeletal Pain, Sleep Duration, and C-Reactive Protein (CRP): A Cross-Sectional Study of the UK Biobank Dataset. Sleep Med. 2023, 101, 393–400. [Google Scholar] [CrossRef]
- Matsuda, M.; Huh, Y.; Ji, R.-R. Roles of Inflammation, Neurogenic Inflammation, and Neuroinflammation in Pain. J. Anesth. 2019, 33, 131–139. [Google Scholar] [CrossRef]
- Shabbir, F.; Patel, A.; Mattison, C.; Bose, S.; Krishnamohan, R.; Sweeney, E.; Sandhu, S.; Nel, W.; Rais, A.; Sandhu, R.; et al. Effect of Diet on Serotonergic Neurotransmission in Depression. Neurochem. Int. 2013, 62, 324–329. [Google Scholar] [CrossRef] [PubMed]
- Goodson, N.J.; Smith, B.H.; Hocking, L.J.; McGilchrist, M.M.; Dominiczak, A.F.; Morris, A.; Porteous, D.J.; Goebel, A. Generation Scotland Cardiovascular Risk Factors Associated with the Metabolic Syndrome Are More Prevalent in People Reporting Chronic Pain: Results from a Cross-Sectional General Population Study. Pain 2013, 154, 1595–1602. [Google Scholar] [CrossRef]
- Blundell, J.E.; Gibbons, C.; Caudwell, P.; Finlayson, G.; Hopkins, M. Appetite Control and Energy Balance: Impact of Exercise. Obes. Rev. 2015, 16 (Suppl. 1), 67–76. [Google Scholar] [CrossRef]
- Hopkins, M.; Blundell, J.E. Energy Balance, Body Composition, Sedentariness and Appetite Regulation: Pathways to Obesity. Clin. Sci. 2016, 130, 1615–1628. [Google Scholar] [CrossRef]
- Kraemer, W.J.; Ratamess, N.A. Hormonal Responses and Adaptations to Resistance Exercise and Training. Sports Med. 2005, 35, 339–361. [Google Scholar] [CrossRef]
- Garland, T., Jr.; Schutz, H.; Chappell, M.A.; Keeney, B.K.; Meek, T.H.; Copes, L.E.; Acosta, W.; Drenowatz, C.; Maciel, R.C.; van Dijk, G.; et al. The Biological Control of Voluntary Exercise, Spontaneous Physical Activity and Daily Energy Expenditure in Relation to Obesity: Human and Rodent Perspectives. J. Exp. Biol. 2011, 214, 206–229. [Google Scholar] [CrossRef] [PubMed]
- Annesi, J.J. Effects of Cardiovascular Exercise on Eating Behaviours: Accounting for Effects on Stress, Depression-, and Anger-Related Emotional Eating in Women with Obesity. Stress Health 2024, 40, e3364. [Google Scholar] [CrossRef] [PubMed]
- Messier, S.P.; Mihalko, S.L.; Legault, C.; Miller, G.D.; Nicklas, B.J.; DeVita, P.; Beavers, D.P.; Hunter, D.J.; Lyles, M.F.; Eckstein, F.; et al. Effects of Intensive Diet and Exercise on Knee Joint Loads, Inflammation, and Clinical Outcomes among Overweight and Obese Adults with Knee Osteoarthritis: The IDEA Randomized Clinical Trial. JAMA 2013, 310, 1263–1273. [Google Scholar] [CrossRef]
- Elma, Ö.; Nijs, J.; Malfliet, A. The Importance of Nutritional Factors on the Road toward Multimodal Lifestyle Interventions for Persistent Pain. Braz. J. Phys. Ther. 2024, 28, 101119. [Google Scholar] [CrossRef]
- Turnagöl, H.H.; Koşar, Ş.N.; Güzel, Y.; Aktitiz, S.; Atakan, M.M. Nutritional Considerations for Injury Prevention and Recovery in Combat Sports. Nutrients 2021, 14, 53. [Google Scholar] [CrossRef]
- Zvolensky, M.J.; McMillan, K.; Gonzalez, A.; Asmundson, G.J.G. Chronic Pain and Cigarette Smoking and Nicotine Dependence among a Representative Sample of Adults. Nicotine Tob. Res. 2009, 11, 1407–1414. [Google Scholar] [CrossRef]
- Mundal, I.; Gråwe, R.W.; Bjørngaard, J.H.; Linaker, O.M.; Fors, E.A. Psychosocial Factors and Risk of Chronic Widespread Pain: An 11-Year Follow-up Study—The HUNT Study. Pain 2014, 155, 1555–1561. [Google Scholar] [CrossRef]
- van Oostrom, S.H.; Monique Verschuren, W.M.; de Vet, H.C.W.; Picavet, H.S.J. Ten Year Course of Low Back Pain in an Adult Population-Based Cohort—The Doetinchem Cohort Study. Eur. J. Pain 2011, 15, 993–998. [Google Scholar] [CrossRef]
- John, U.; Hanke, M.; Meyer, C.; Völzke, H.; Baumeister, S.E.; Alte, D. Tobacco Smoking in Relation to Pain in a National General Population Survey. Prev. Med. 2006, 43, 477–481. [Google Scholar] [CrossRef]
- Vogt, M.T.; Hanscom, B.; Lauerman, W.C.; Kang, J.D. Influence of Smoking on the Health Status of Spinal Patients: The National Spine Network Database. Spine (Phila Pa 1976) 2002, 27, 313–319. [Google Scholar] [CrossRef]
- Girdler, S.S.; Maixner, W.; Naftel, H.A.; Stewart, P.W.; Moretz, R.L.; Light, K.C. Cigarette Smoking, Stress-Induced Analgesia and Pain Perception in Men and Women. Pain 2005, 114, 372–385. [Google Scholar] [CrossRef] [PubMed]
- Ussher, M.H.; Faulkner, G.E.J.; Angus, K.; Hartmann-Boyce, J.; Taylor, A.H. Exercise Interventions for Smoking Cessation. Cochrane Database Syst. Rev. 2019, 2019, CD002295. [Google Scholar] [CrossRef] [PubMed]
- Klinsophon, T.; Thaveeratitham, P.; Sitthipornvorakul, E.; Janwantanakul, P. Effect of Exercise Type on Smoking Cessation: A Meta-Analysis of Randomized Controlled Trials. BMC Res. Notes 2017, 10, 442. [Google Scholar] [CrossRef]
- Santos, C.P.; Proença, M.; Gouveia, T.D.S.; Soares de Oliveira, C.B.; Tacao, G.Y.; Trevisan, I.B.; Ramos, E.M.C.; Ramos, D. Effectiveness of Aerobic Exercise on Smoking Cessation in Adults: A Systematic Review and Meta-Analysis. J. Phys. Act. Health 2021, 18, 230–242. [Google Scholar] [CrossRef]
- Taylor, A.H.; Thompson, T.P.; Greaves, C.J.; Taylor, R.S.; Green, C.; Warren, F.C.; Kandiyali, R.; Aveyard, P.; Ayres, R.; Byng, R.; et al. A Pilot Randomised Trial to Assess the Methods and Procedures for Evaluating the Clinical Effectiveness and Cost-Effectiveness of Exercise Assisted Reduction Then Stop (EARS) among Disadvantaged Smokers. Health Technol. Assess. 2014, 18, 1–324. [Google Scholar] [CrossRef]
- Everson, E.S.; Daley, A.J.; Ussher, M. The Effects of Moderate and Vigorous Exercise on Desire to Smoke, Withdrawal Symptoms and Mood in Abstaining Young Adult Smokers. Ment. Health Phys. Act. 2008, 1, 26–31. [Google Scholar] [CrossRef]
- Fox, K.R. The Influence of Physical Activity on Mental Well-Being. Public Health Nutr. 1999, 2, 411–418. [Google Scholar] [CrossRef]
- Steptoe, A.; Edwards, S.; Moses, J.; Mathews, A. The Effects of Exercise Training on Mood and Perceived Coping Ability in Anxious Adults from the General Population. J. Psychosom. Res. 1989, 33, 537–547. [Google Scholar] [CrossRef]
- Salmon, P. Effects of Physical Exercise on Anxiety, Depression, and Sensitivity to Stress: A Unifying Theory. Clin. Psychol. Rev. 2001, 21, 33–61. [Google Scholar] [CrossRef]
- Purani, H.; Friedrichsen, S.; Allen, A.M. Sleep Quality in Cigarette Smokers: Associations with Smoking-Related Outcomes and Exercise. Addict. Behav. 2019, 90, 71–76. [Google Scholar] [CrossRef]
- Correa, M.; Pardo, M.; Carratalá-Ros, C.; Martínez-Verdú, A.; Salamone, J.D. Preference for Vigorous Exercise versus Sedentary Sucrose Drinking: An Animal Model of Anergia Induced by Dopamine Receptor Antagonism. Behav. Pharmacol. 2020, 31, 553–564. [Google Scholar] [CrossRef] [PubMed]
- Spanagel, R. Cannabinoids and the Endocannabinoid System in Reward Processing and Addiction: From Mechanisms to Interventions. Dialogues Clin. Neurosci. 2020, 22, 241–250. [Google Scholar] [CrossRef] [PubMed]
- Flack, K.; Pankey, C.; Ufholz, K.; Johnson, L.; Roemmich, J.N. Genetic Variations in the Dopamine Reward System Influence Exercise Reinforcement and Tolerance for Exercise Intensity. Behav. Brain Res. 2019, 375, 112148. [Google Scholar] [CrossRef]
- Greenwood, B.N.; Foley, T.E.; Le, T.V.; Strong, P.V.; Loughridge, A.B.; Day, H.E.W.; Fleshner, M. Long-Term Voluntary Wheel Running Is Rewarding and Produces Plasticity in the Mesolimbic Reward Pathway. Behav. Brain Res. 2011, 217, 354–362. [Google Scholar] [CrossRef]
- Park, S.-S.; Shin, M.-S.; Park, H.-S.; Kim, T.-W.; Kim, C.-J.; Lim, B.-V. Treadmill Exercise Ameliorates Nicotine Withdrawal-Induced Symptoms. J. Exerc. Rehabil. 2019, 15, 383–391. [Google Scholar] [CrossRef]
- Thomas, A.M.; Ostroumov, A.; Kimmey, B.A.; Taormina, M.B.; Holden, W.M.; Kim, K.; Brown-Mangum, T.; Dani, J.A. Adolescent Nicotine Exposure Alters GABA Receptor Signaling in the Ventral Tegmental Area and Increases Adult Ethanol Self-Administration. Cell Rep. 2018, 23, 68–77. [Google Scholar] [CrossRef]
- Fischer-Smith, K.D.; Houston, A.C.W.; Rebec, G.V. Differential Effects of Cocaine Access and Withdrawal on Glutamate Type 1 Transporter Expression in Rat Nucleus Accumbens Core and Shell. Neuroscience 2012, 210, 333–339. [Google Scholar] [CrossRef]
- Ni, Y.; Li, L.; Qu, Y.; Chen, S.; Zhang, H.; Wang, H. Advances in the Study of Neural Mechanisms Associated with Exercise to Ameliorate Nicotine Addiction. Adv. Phys. Educ. 2022, 12, 126–141. [Google Scholar] [CrossRef]
- Matthias, M.S.; Henry, S.G. Reducing Frustration and Improving Management of Chronic Pain in Primary Care: Is Shared Decision-Making Sufficient? J. Gen. Intern. Med. 2022, 37, 227–228. [Google Scholar] [CrossRef]
- Salazar-Méndez, J.; Núñez-Cortés, R.; Suso-Martí, L.; Ribeiro, I.L.; Garrido-Castillo, M.; Gacitúa, J.; Mendez-Rebolledo, G.; Cruz-Montecinos, C.; López-Bueno, R.; Calatayud, J. Dosage Matters: Uncovering the Optimal Duration of Pain Neuroscience Education to Improve Psychosocial Variables in Chronic Musculoskeletal Pain. A Systematic Review and Meta-Analysis with Moderator Analysis. Neurosci. Biobehav. Rev. 2023, 153, 105328. [Google Scholar] [CrossRef]
- Núñez-Cortés, R.; Salazar-Méndez, J.; Calatayud, J.; Malfliet, A.; Lluch, E.; Mendez-Rebolledo, G.; Guzmán-Muñoz, E.; López-Bueno, R.; Suso-Martí, L. The Optimal Dose of Pain Neuroscience Education Added to an Exercise Programme for Patients with Chronic Spinal Pain: A Systematic Review and Dose-Response Meta-Analysis. Pain 2024, 165, 1196–1206. [Google Scholar] [CrossRef] [PubMed]
- Núñez-Cortés, R.; Salazar-Méndez, J.; Calatayud, J.; Lluch, E.; López-Bueno, R.; Horment-Lara, G.; Cruz-Montecinos, C.; Suso-Martí, L. How Do the Target Concepts of Pain Science Education Combined with Exercise Contribute to the Effect on Pain Intensity and Disability in Patients with Chronic Spinal Pain? A Systematic Review and Meta-Analysis with Moderator Analysis. Neurosci. Biobehav. Rev. 2024, 163, 105740. [Google Scholar] [CrossRef] [PubMed]
- Inayat, S.; Qandeel; Nazariahangarkolaee, M.; Singh, S.; McNaughton, B.L.; Whishaw, I.Q.; Mohajerani, M.H. Low Acetylcholine during Early Sleep Is Important for Motor Memory Consolidation. Sleep 2020, 43, zsz297. [Google Scholar] [CrossRef]
- Salazar-Méndez, J.; Viscay-Sanhueza, N.; Pinto-Vera, C.; Oyarce-Contreras, F.; Parra-Vera, M.-F.; Suso-Martí, L.; Guzmán-Muñoz, E.; López-Bueno, R.; Núñez-Cortés, R.; Calatayud, J. Cognitive Behavioral Therapy for Insomnia in People with Chronic Musculoskeletal Pain. A Systematic Review and Dose-Response Meta-Analysis. Sleep Med. 2024, 122, 20–26. [Google Scholar] [CrossRef]
- Jackman, P.C.; Cooke, S.; George, T.; Blackwell, J.; Middleton, G. Physical Activity Experiences of Community-Dwelling Older Adults with Physical Disabilities: A Scoping Review of Qualitative Research. Disabil. Rehabil. 2024, 46, 3564–3576. [Google Scholar] [CrossRef]
- Koho, P.; Orenius, T.; Kautiainen, H.; Haanpää, M.; Pohjolainen, T.; Hurri, H. Association of Fear of Movement and Leisure-Time Physical Activity among Patients with Chronic Pain. J. Rehabil. Med. 2011, 43, 794–799. [Google Scholar] [CrossRef]
- Vader, K.; Doulas, T.; Patel, R.; Miller, J. Experiences, Barriers, and Facilitators to Participating in Physical Activity and Exercise in Adults Living with Chronic Pain: A Qualitative Study. Disabil. Rehabil. 2021, 43, 1829–1837. [Google Scholar] [CrossRef]
- Núñez-Cortés, R.; Lluch, E.; Cruz-Montecinos, C. Democratizing Access to Physical Therapy to Address the Challenge of Chronic Pain. Braz. J. Phys. Ther. 2024, 28, 101084. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Núñez-Cortés, R.; Salazar-Méndez, J.; Nijs, J. Physical Activity as a Central Pillar of Lifestyle Modification in the Management of Chronic Musculoskeletal Pain: A Narrative Review. J. Funct. Morphol. Kinesiol. 2025, 10, 183. https://doi.org/10.3390/jfmk10020183
Núñez-Cortés R, Salazar-Méndez J, Nijs J. Physical Activity as a Central Pillar of Lifestyle Modification in the Management of Chronic Musculoskeletal Pain: A Narrative Review. Journal of Functional Morphology and Kinesiology. 2025; 10(2):183. https://doi.org/10.3390/jfmk10020183
Chicago/Turabian StyleNúñez-Cortés, Rodrigo, Joaquín Salazar-Méndez, and Jo Nijs. 2025. "Physical Activity as a Central Pillar of Lifestyle Modification in the Management of Chronic Musculoskeletal Pain: A Narrative Review" Journal of Functional Morphology and Kinesiology 10, no. 2: 183. https://doi.org/10.3390/jfmk10020183
APA StyleNúñez-Cortés, R., Salazar-Méndez, J., & Nijs, J. (2025). Physical Activity as a Central Pillar of Lifestyle Modification in the Management of Chronic Musculoskeletal Pain: A Narrative Review. Journal of Functional Morphology and Kinesiology, 10(2), 183. https://doi.org/10.3390/jfmk10020183