
A Comprehensive Survey on Data Utility and Privacy: Taking Indian Healthcare System as a Potential Case Study




Abstract
1. Introduction
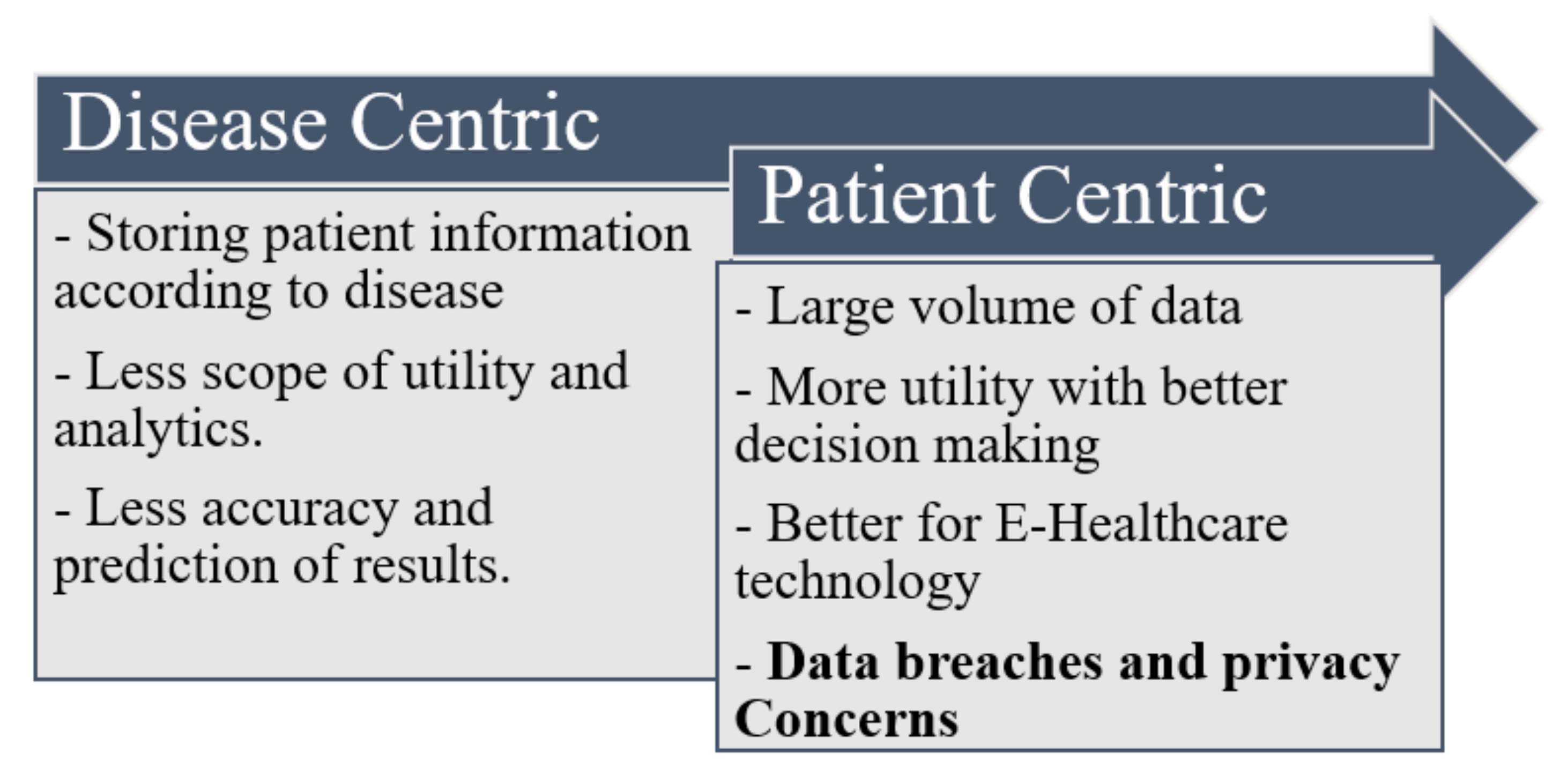
- The health data are centrally stored according to diseases (type, symptoms, and remedial medicines).
- Electronic health records (EHRs) are assessments and analyses conducted according to diseases. For example, we can analyze the patient data of the past ten years in a hospital with diabetes, malaria, or another joint disease.
- Disease-centric databases present less scope for data analysis because they do not focus on individual traits and symptoms. Some diseases are related to a person’s behavior, lifestyle, and geographical location. For example, suppose a person is treated for two or three similar diseases from different hospitals in the past ten years. In that case, we must analyze his treatment records, family records, and habits, which are unavailable in the disease-centric database or may be available in heterogeneous databases, wherein a combined analysis is complex. Some data values are spread across multiple datasets maintained separately by hospitals or may have incomplete values, resulting in inappropriate/wrong prediction. The data quality is questionable to be used for analysis.
- The data volume generated is considerably larger and stored according to the individual patient; hence, the data quality and utility are highly satisfactory in appropriate decision making.
- Because an individual’s data are collected from multiple devices and sensors or through sources, maintaining the individual’s privacy is challenging.
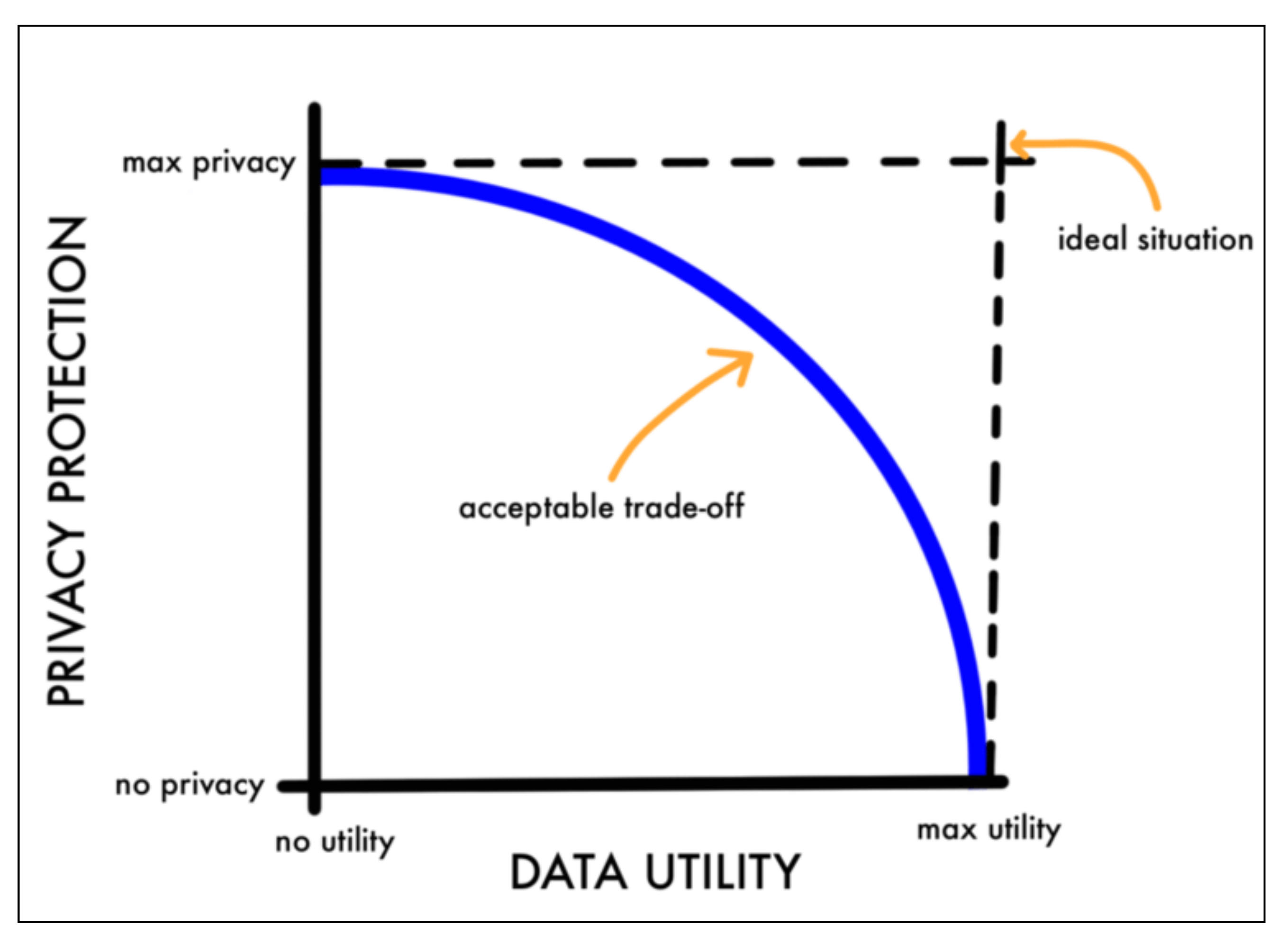
- Can one pursue high data utility while maintaining acceptable privacy?
- Because privacy concerns are different for different healthcare organizations, how is the trade-off between privacy protection and data utility balanced for computing?
- Provide insights into Indian healthcare systems with applications, trends, and advantages.
- Describe policies that drive Indian healthcare systems
- Specify technological inventions used in Indian healthcare systems.
- List the various privacy issues concerning the Indian healthcare system that needs to be addressed first.
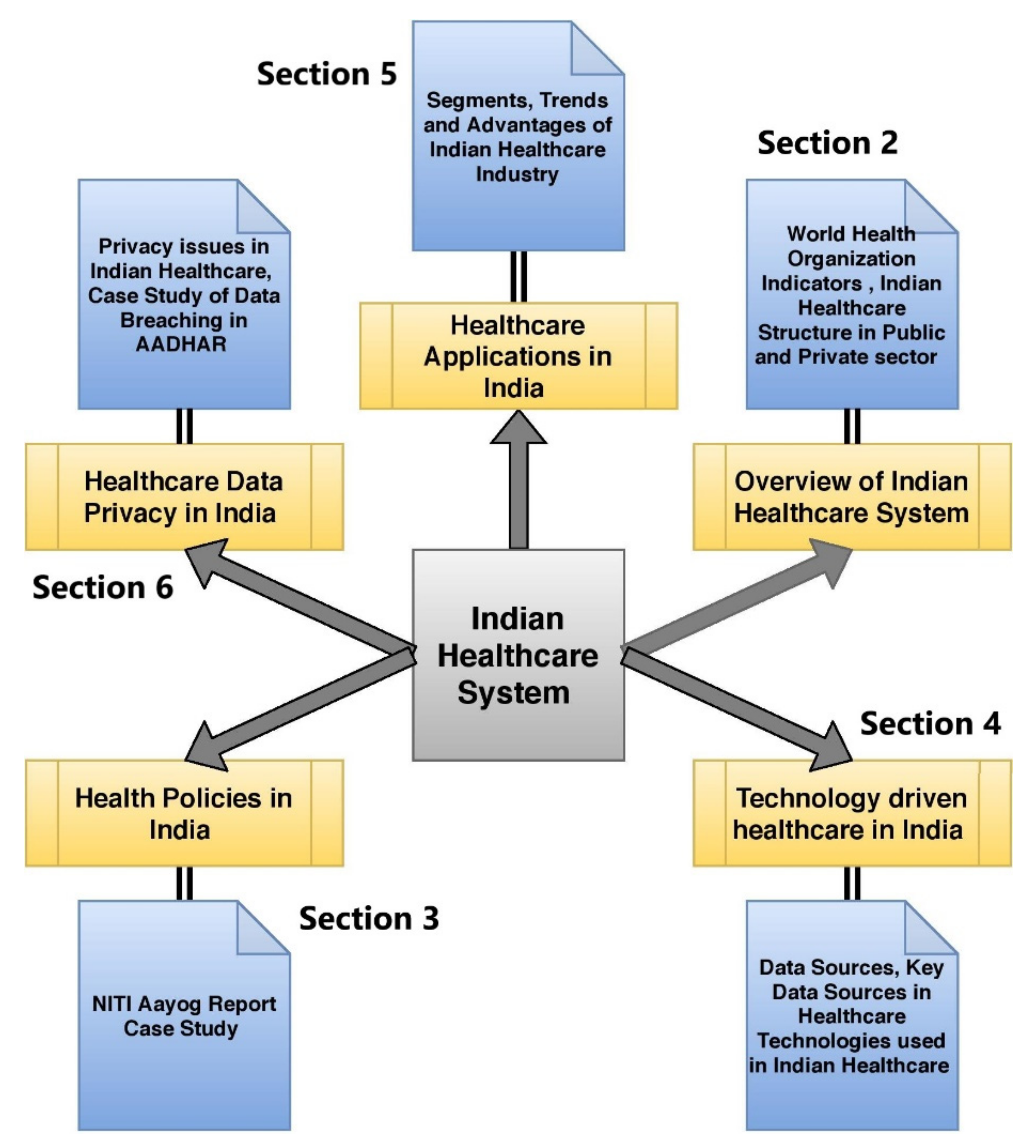
Structure of Paper
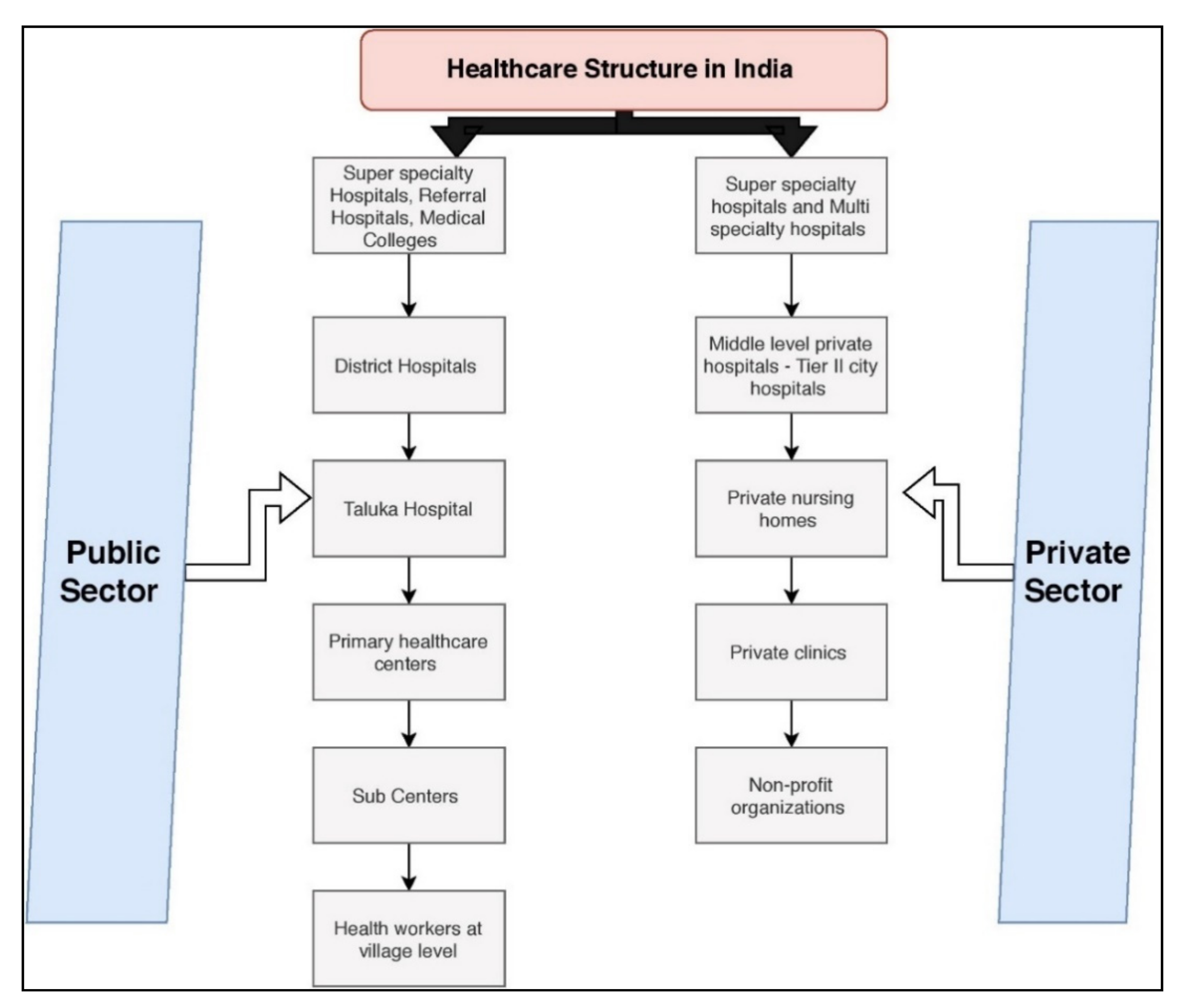
2. Indian Healthcare Systems: Overview
3. Healthcare in India: Reformation in Policies
Case Study: Healthcare Sector in India: NITI Aayog Report
- ✓
- Strong economic foundation and policy implementation for transforming the healthcare industry, which is currently underperforming.
- ✓
- Healthcare system improvisation can decrease mortality and poverty rates and accelerate economic growth.
- ✓
- Unnecessary and non-uniform health sector fragmentation is the main problem of healthcare industries in India.
- Protect the healthcare data from a third-party unauthorized entity;
- Have uniformity in centralized health systems.
4. Healthcare Industry and Applications in India
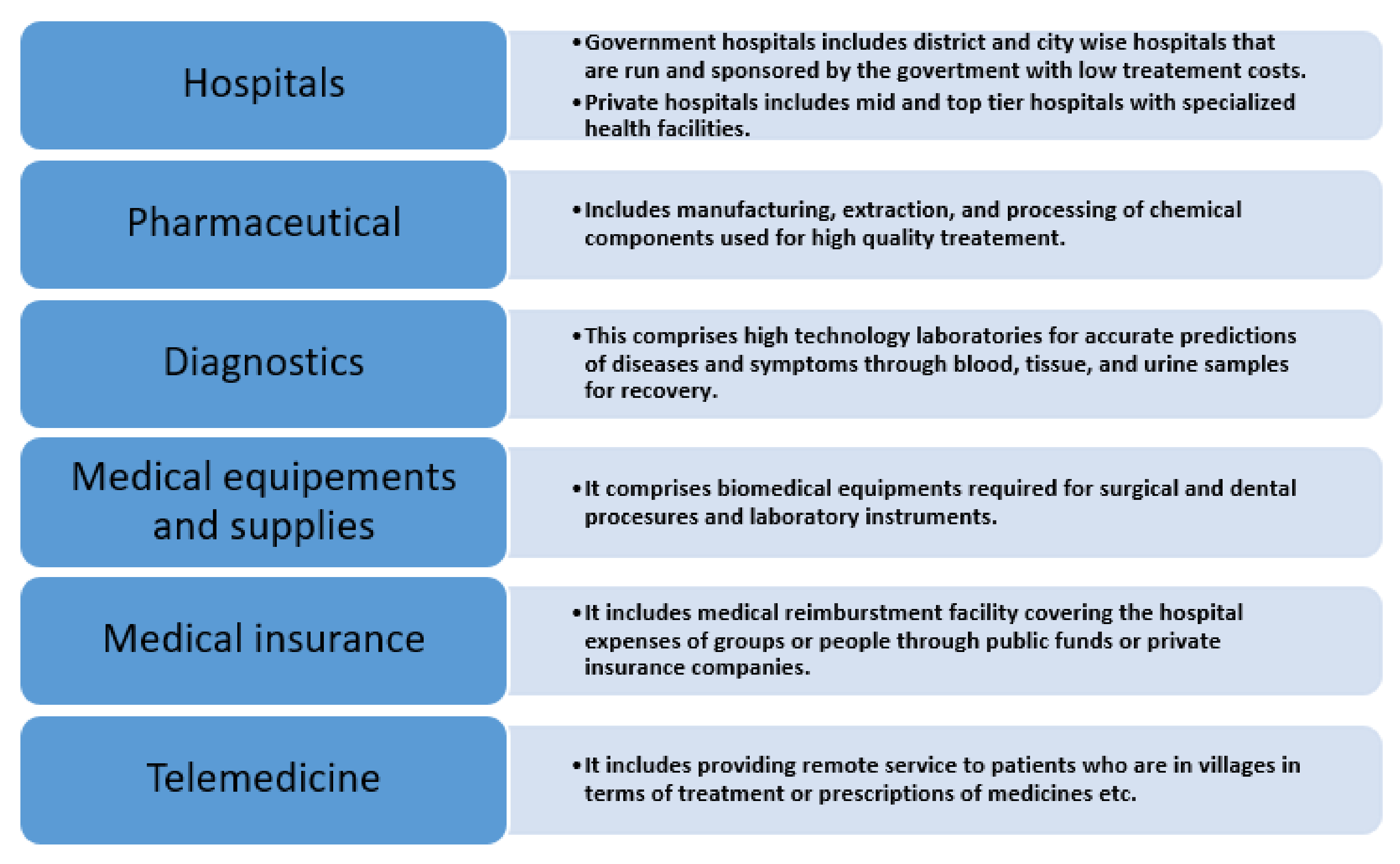
4.1. Segments of Indian Healthcare Industry
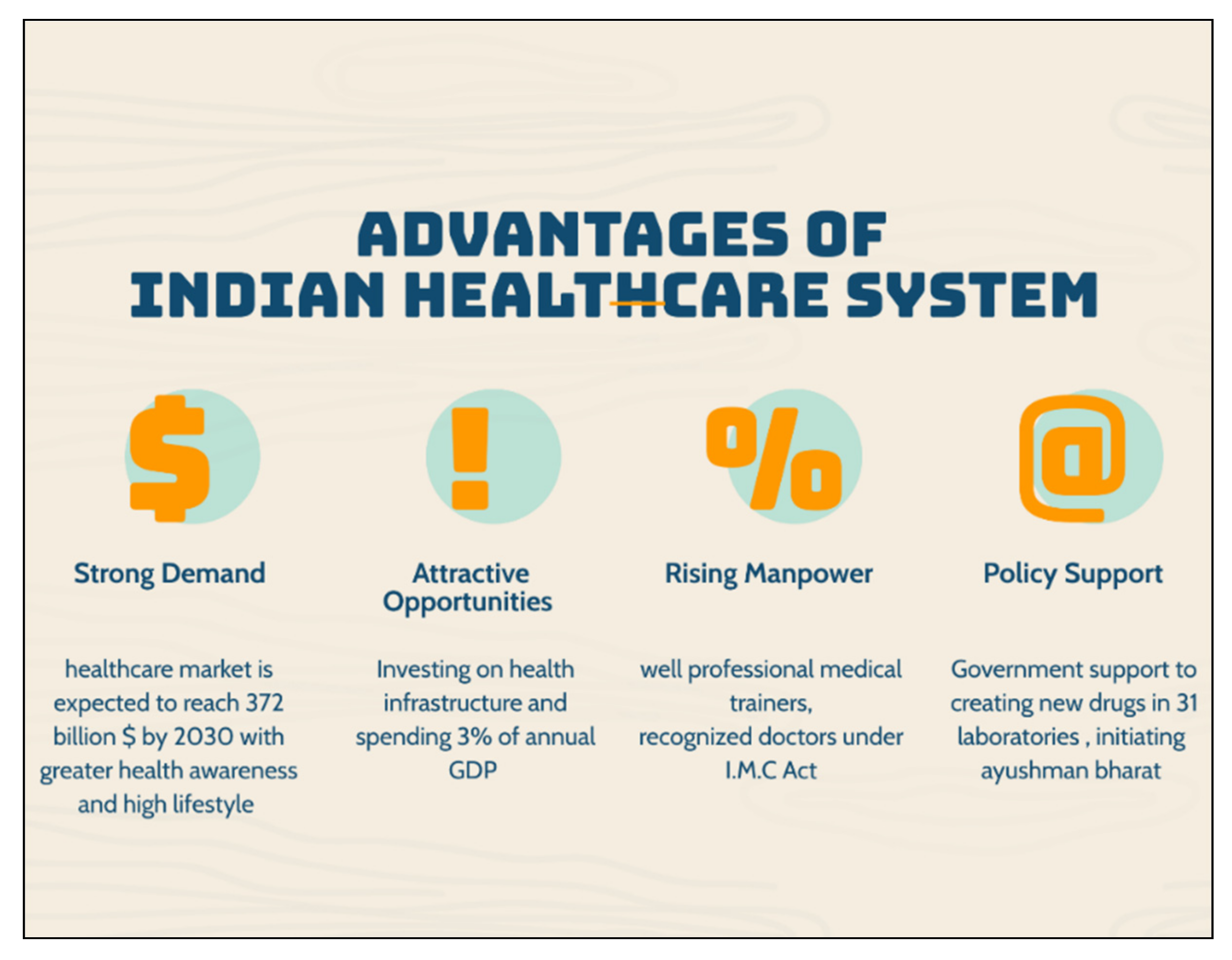
4.2. Advantages of the New Indian Healthcare Industry
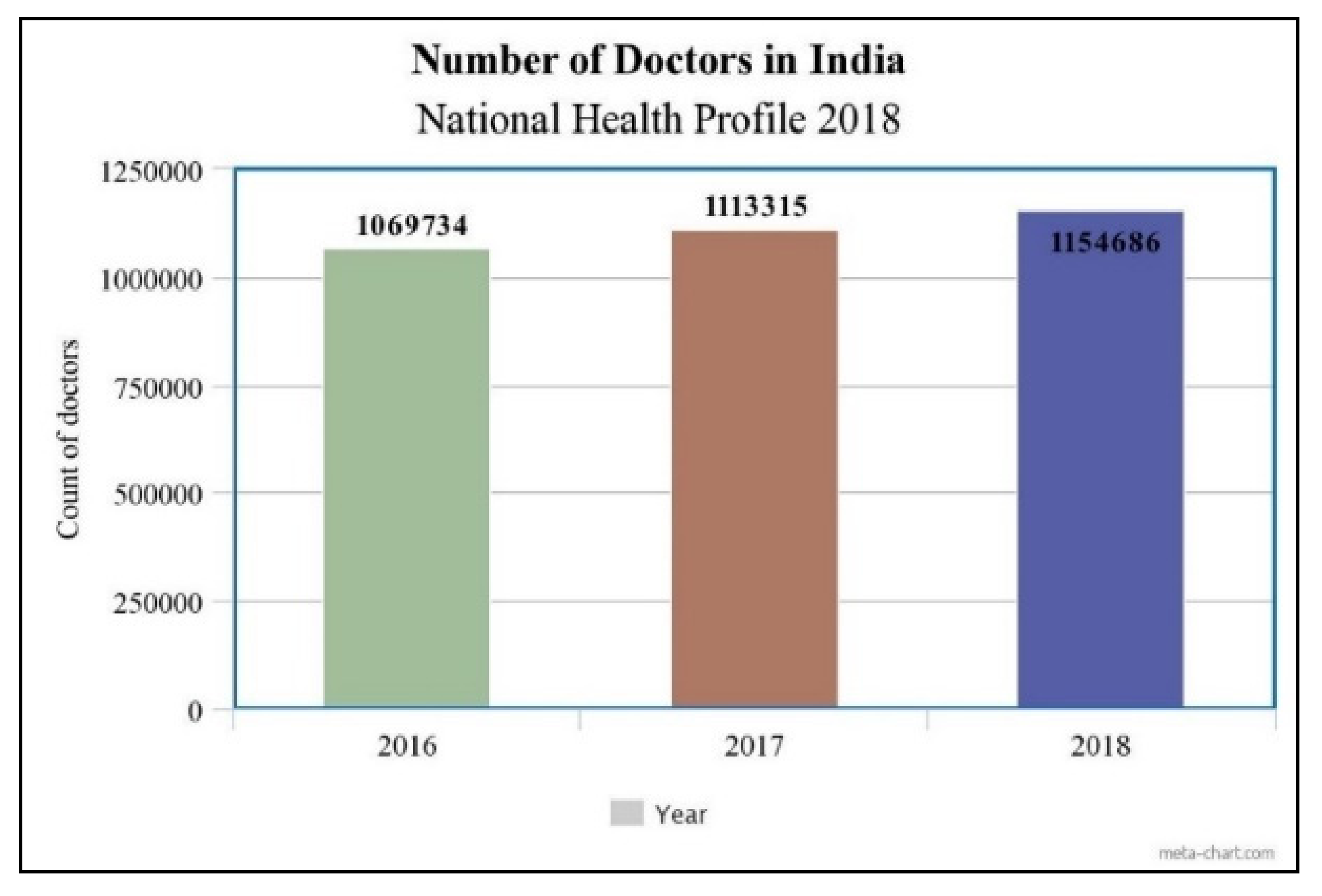
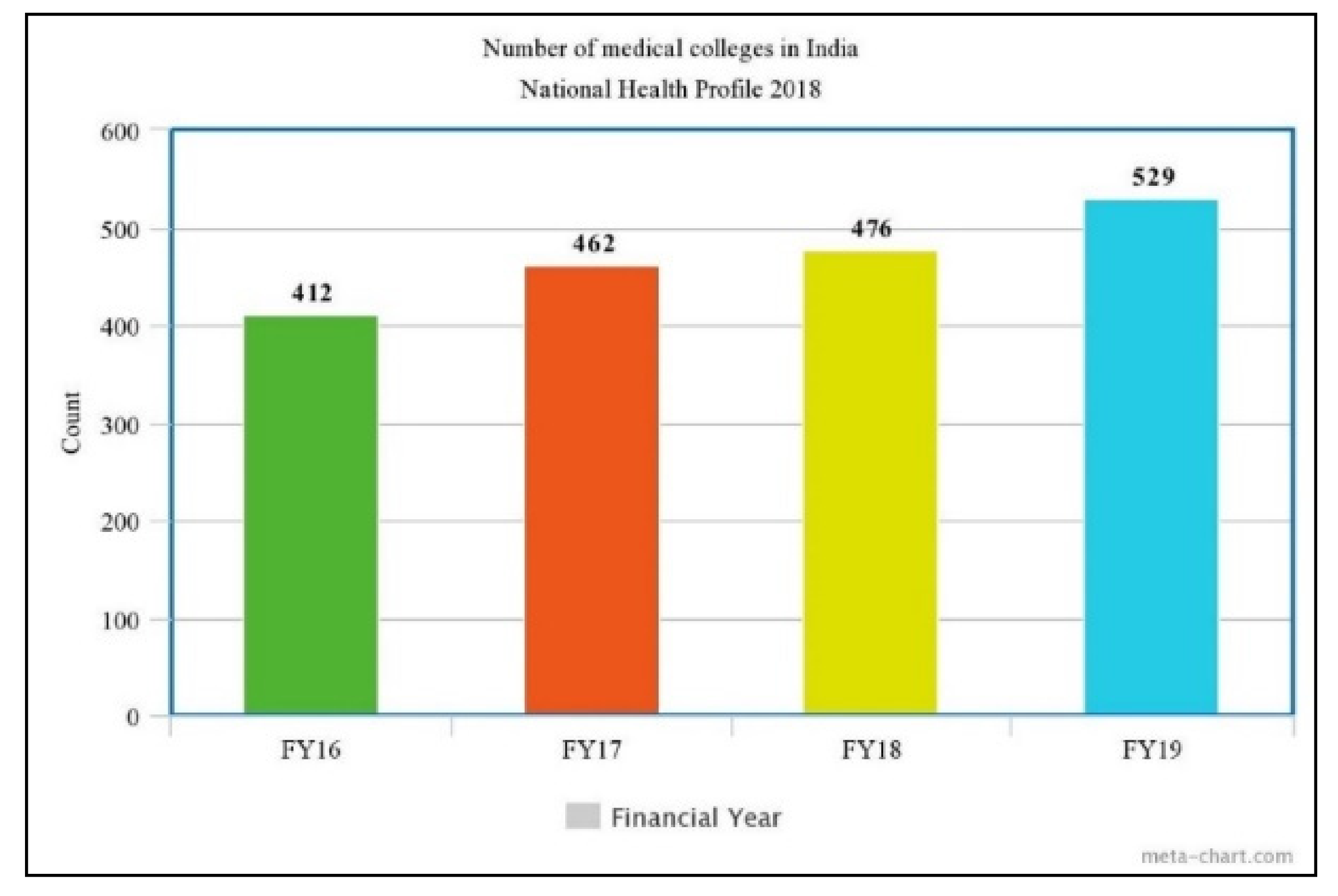
4.3. Rise in Healthcare Infrastructure in India
4.4. Trends in Indian Healthcare System
4.5. Popular Healthcare Hubs/Startups in India
5. Healthcare Data Utility: Context of India
- What are the different data sources of the Indian healthcare industry?
- How are the Indian healthcare data classified?
- What are the different intelligent platforms used for healthcare data analysis?
- Which technologies drive the Indian healthcare system?
5.1. Sources of Indian Healthcare Data
- Exogenous Data
- Genomic Data
5.2. Types of Healthcare Data
5.3. Key Data Sources of Health Information of India
5.4. Technologies Used in Healthcare Data: Indian Perspective
5.4.1. Data Mining/Analysis of Indian Health Data
- Clustering: Clustering is a type of unsupervised learning and is slightly different from classification. In clustering, many datasets are divided into small chunks (clusters) based on some similarity. The Euclidian distance is used to calculate the relation/distance between two data values. K-means clustering is a prevalent method of clustering; however, it is time-consuming and slow.
- Classification: Classification comprises training and testing data. Training is required as it helps create classification rules. For high accuracy, providing maximum data for training is an optimal practice. The accuracy of a classification model depends on the degree of classifying rules being true, which is estimated using the test data.
- Association: Association is an exciting mining method in which frequent and usual patterns in a dataset are determined. It is also known as the market basket analysis because it can identify the association among purchased items or unknown customer sales patterns in a transaction database. Association rule mining is widely used for identifying the relationships among various symptoms with similar causes of particular diseases.
- Regression: Regression is used to find the correlation among various attributes defined over a particular function. For regression, a mathematical model is constructed with the training data with dependent and independent variables. Regression can be linear and nonlinear. Linear regression identifies the relationship between a dependent variable and one or more independent variables. Logistic regression, a nonlinear regression type, can accept the categorical data and predict the probability through the logit function.
5.4.2. Artificial Intelligence, Machine Learning, and Deep Learning in Indian Health Data
5.4.3. Data Visualization of Indian Health Data
5.4.4. Augmented and Virtual Reality in Indian Health Data
6. Healthcare Data Privacy in India
- -
- Information privacy involves establishing rules governing collecting and handling personal data such as credit information and medical and government records. It is also known as data protection;
- -
- Bodily privacy concerns the protection of people’s physical selves against invasive procedures such as genetic tests, drug testing, and cavity searches;
- -
- Privacy of communications covers the security and privacy of mail, telephones, e-mails, and other forms of communication; and
- -
- Territorial privacy concerns the setting of limits on intrusion into the domestic and other environments such as the workplace or public space. This includes searches, video surveillance, and ID checks—Australian law reform commission.
- The law must be flexible and adhere to changing technologies.
- Law must be applied to public and private sector entities.
- Entities controlling the data should be accountable for data processing.
- Consent must be structured and genuine.
- Data processing and analysis must be minimal.
- A high-powered statutory authority should enforce the data protection framework.
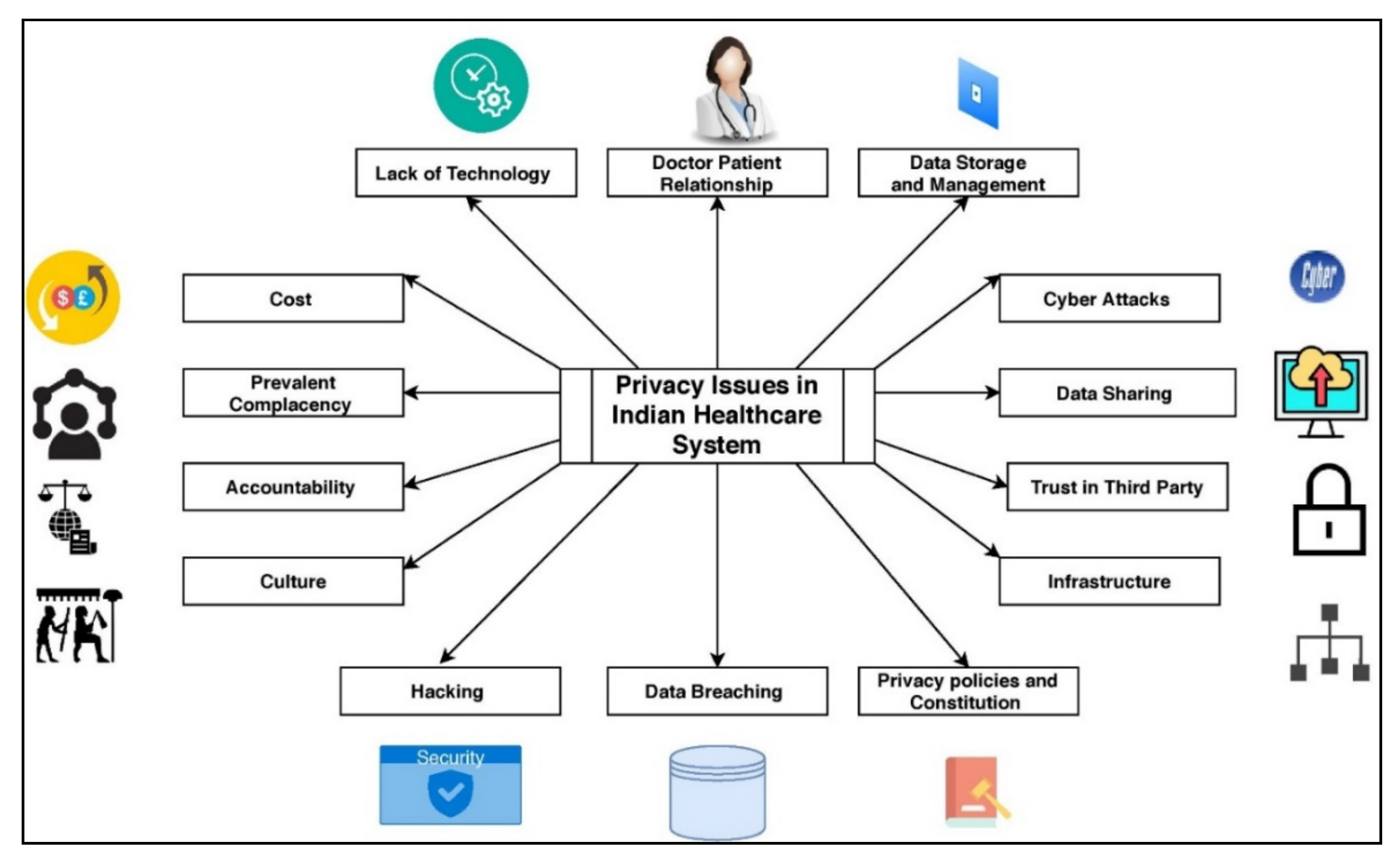
Privacy Issues in the Indian Healthcare System
- A.
- Lack of Technology and Infrastructure
- B.
- Doctor–Patient Relationship
- C.
- Data Storage and Management
- D.
- Cyber Attacks and Hacking
- E.
- Data Sharing Trust in the Third Party
- F.
- Lack of Policy and Constitutional Limitations
- Who owns and accesses patient records and why?
- What type of data with what granularity level must be collected?
- Where must the data be stored (central warehouse or hospital)?
- Who can view medical records?
- Who is responsible for disclosing medical records?
- Which consent must be acquired while deleting patient records?
- G.
- Data Breaching
- Brocken access and authentication.
- Flawed service level agreements by organizations.
- Poor backup and recovery plans in case of data loss.
- Reverse engineering methods.
- H.
- Culture
- I.
- Prevalent Complacency
- J.
- Cost
7. Open Issues and Further Discussions
7.1. Key Performance Indicators in the Context of Privacy in the Indian Healthcare System
- Forced Trust vs. Control: A forced trust is a trust in which an individual has no choice but to trust any healthcare system. On the other hand, control is a systematic view of obtaining trust and assuring each individual that their sensitive personal data will not be shared with the third party without any consent. In the Indian healthcare context, the ratio of forced trust to control is high. People tend to have less trust in any healthcare system because of constitutional limitations. This is one of the significant KPIs in the context of Indian Healthcare privacy.
- Content Viewed by Whom: Though there is limited access to any EHR and only authenticated people can view or access the sensitive data, there is still the possibility that unauthorized entities may access health records. Weak passwords, inappropriate security policies, conflict in access controls, and sharing passwords to untrusted persons are the possible reasons sensitive data may be misused. In India, the healthcare system is not very structured and centralized. Local hospitals keep their records on local servers, which are highly vulnerable to various attacks. Data breaching primarily happens in tier 2 and tier 3 cities and village hospitals.
- Tacit Knowledge: Even if the healthcare system ensures maximum protection against data breaches for healthcare data, the metadata or tacit information may reveal more information than basic health information. Using reverse engineering techniques or social media analysis, it is easy to gain personal information. In India, there are many cases reported against criminals who seek sensitive information through social media accounts. Unfortunately, there is no control over the protection against such information.
- Laws and Regulation: Limited regulation and law in the constitution are essential KPI in the Indian healthcare field. As per the latest data of 2019, Indian healthcare generates 1021 gigabytes of data per year. Managing such a massive amount of data by protecting sensitive content must prioritize the Indian government.
- Use of new Data Protection Technologies: The newer technologies like blockchain, two-factor authentication, machine learning, AI, and attribute-based anonymization is only implemented in high-end industries or healthcare organizations. Small sector health organizations, village, or tier 3 hospitals do not have funds to support the protection of such data, and hence newer technologies cannot be used.
- Researcher’s Satisfaction: Since there is a massive generation of healthcare data, it is an excellent opportunity to analyze the data for research purposes. Healthcare analytics is the emerging field of computing and is rising exponentially in India. More restricted and policy-imposed data are not suitable for analytics purposes, and data quality gets degraded.
- Industry-academia collaboration exists for privacy preservation mechanisms: There is a huge gap between industry and academia in India. Despite having good researchers in the privacy field, their work is not reaching the industry.
- Doctors and Healthcare Professionals/practitioners (DH): Five doctors are selected from all tier cities and villages who manage patient records through the digital and paper-based modes.
- Hospital administrative staff (HA): Five administrative staff are taken from various hospitals from all tier cities and villages, maintaining patient records for future communication.
- Researchers and Scientist (RS): Five Researchers from healthcare data analytics and data privacy are selected to work in a new development in healthcare data science and data privacy.
- Academicians in the computer science field (AC): Five Academicians in the Computer Science field are selected to either teach data analytics courses or security courses in their curriculum.
7.2. Future of Data Privacy in India
- The law must be flexible and must be adhered to changing technologies.
- Law must be applied to public and private sector entities.
- Entities controlling the data should be accountable for any data processing.
- Consent must be structured and genuine.
- Processing and analysis of data must be minimal.
- Enforcement of the data protection framework should be carried out by a high-powered statutory authority.
7.3. Data Utility-Privacy Trade-Off in Personal Data Protection Bill
8. Conclusions and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Healthcare System for New India: Building Blocks—Potential Pathway to Reform. November 2019. Available online: https://niti.gov.in/sites/default/files/2019-11/NitiAayogBook_compressed.pdf (accessed on 1 August 2020).
- Fullman, N.; Yearwood, J.; Abay, S.M.; Abbafati, C.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; Abebe, Z.; Abebo, T.A.; Aboyans, V.; et al. Measuring performance on the Healthcare Access and Quality Index for 195 countries and territories and selected subnational locations: A systematic analysis from the Global Burden of Disease Study 2016. Lancet 2018, 391, 2236–2271. [Google Scholar] [CrossRef]
- Klecun, E. Transforming healthcare: Policy discourses of IT and patient-centred care. Eur. J. Inf. Syst. 2016, 25, 64–76. [Google Scholar] [CrossRef]
- Top 40 Medical and Healthcare Startups in India. February 2020. Available online: https://www.medicalstartups.org/country/India/ (accessed on 1 August 2020).
- Liu, X.; Deng, R.H.; Choo, K.-K.R.; Yang, Y. Privacy-Preserving Reinforcement Learning Design for Patient-Centric Dynamic Treatment Regimes. IEEE Trans. Emerg. Top. Comput. 2021, 9, 456–470. [Google Scholar] [CrossRef]
- Vora, J.; Devmurari, P.; Tanwar, S.; Tyagi, S.; Kumar, N.; Obaidat, M.S. Blind Signatures Based Secured E-Healthcare System. In Proceedings of the 2018 International Conference on Computer, Information and Telecommunication Systems (CITS), Alsace, Colmar, France, 11–13 July 2018; pp. 1–5. [Google Scholar]
- Pussewalage, H.S.G.; Oleshchuk, V.A. Privacy preserving mechanisms for enforcing security and privacy requirements in E-health solutions. Int. J. Inf. Manag. 2016, 36, 1161–1173. [Google Scholar] [CrossRef]
- Dey, N.; Hassanien, A.E.; Bhatt, C.; Ashour, A.; Satapathy, S.C. (Eds.) Internet of Things and Big Data Analytics toward Next-Generation Intelligence; Springer: Berlin, Germany, 2018; pp. 3–549. [Google Scholar]
- Kaur, G.; Tomar, P.; Singh, P. Design of Cloud-Based Green IoT Architecture for Smart Cities. In Internet of Things and Big Data Analytics toward Next-Generation Intelligence; Springer: Cham, Switzerland, 2018; pp. 315–333. [Google Scholar]
- Valdez, A.C.; Ziefle, M. The users’ perspective on the privacy-utility trade-offs in health recommender systems. Int. J. Hum. Comput. Stud. 2019, 121, 108–121. [Google Scholar] [CrossRef]
- Churi, P.P.; Pawar, A.V. Jestr r. J. Eng. Sci. Technol. Rev. 2019, 12, 17–25. [Google Scholar] [CrossRef]
- Sánchez, D.; Batet, M.; Viejo, A. Utility-preserving privacy protection of textual healthcare documents. J. Biomed. Inform. 2014, 52, 189–198. [Google Scholar] [CrossRef]
- Rastogi, V.; Suciu, D.; Hong, S. The boundary between privacy and utility in data publishing. In Proceedings of the 33rd International Conference on Very Large Data Bases, Vienna, Austria, 23–28 September 2007; pp. 531–542. [Google Scholar]
- Talib, F.; Rahman, Z. Current Health of Indian Healthcare and Hospitality Industries: A Demographic Study. Int. J. Bus. Res. Dev. 2013, 2, 1–17. [Google Scholar] [CrossRef]
- Available online: https://www.ibef.org/industry/healthcare-india.aspx (accessed on 13 June 2020).
- Sachdeva, S.; Batra, S.; Bhalla, S. Evolving large scale healthcare applications using open standards. Health Policy Technol. 2017, 6, 410–425. [Google Scholar] [CrossRef]
- Available online: http://www.cbhidghs.nic.in/Ebook/National%20Health%20Profile-2018%20(e-Book)/files/assets/common/downloads/files/NHP%202018.pdf (accessed on 14 June 2020).
- Ganesan, L.; Veena, S.R. ‘Make In India’ For Healthcare Sector in India: A SWOT Analysis on Current Status and Future Prospects. Int. J. Health Sci. Res. 2018, 8, 258–265. [Google Scholar]
- Shankar, D. Health sector reforms for 21st century healthcare. J. Ayurveda Integr. Med. 2015, 6, 4. [Google Scholar] [CrossRef]
- IRDA, CII, Grant Thornton, Gartner, Technopak, TechSci Research. Available online: https://www.ibef.org/download/Healthcare-July-2019.pdf (accessed on 14 June 2020).
- Available online: https://mea.gov.in/images/pdf/22899_India_in_Business.pdf (accessed on 14 June 2020).
- Basu, S.; Andrews, J.; Kishore, S.; Panjabi, R.; Stuckler, D. Comparative performance of private and public healthcare systems in low-and middle-income countries: A systematic review. PLoS Med. 2012, 9, e1001244. [Google Scholar] [CrossRef]
- Gupta, Y.; Joshi, A.; Kale, G. Healthcare Analytics Systems: An Overview. Int. J. Eng. Sci. 2018, 8, 18898. [Google Scholar]
- Boric-Lubecke, O.; Gao, X.; Yavari, E.; Baboli, M.; Singh, A.; Lubecke, V.M. E-healthcare: Remote monitoring, privacy, and security. In Proceedings of the 2014 IEEE MTT-S International Microwave Symposium (IMS2014), Tampa, FL, USA, 1–6 June 2014; pp. 1–3. [Google Scholar]
- Morilla, M.D.R.; Sans, M.; Casasa, A.; Giménez, N. Implementing technology in healthcare: Insights from physicians. BMC Med. Inform. Decis. Mak. 2017, 17, 92. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, V.; Singh, R.; Reddy, R.; Churi, P. Privacy Issues in Wearable Technology: An Intrinsic Review. 2020. SSRN 3566918. Available online: https://ssrn.com/abstract=3566918 (accessed on 20 June 2021). [CrossRef]
- Vassy, J.L.; Korf, B.R.; Green, R.C. How to know when physicians are ready for genomic medicine. Sci. Transl. Med. 2015, 7, 287fs19. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Ishwaran, H. Random forests for genomic data analysis. Genomics 2012, 99, 323–329. [Google Scholar] [CrossRef]
- Das, A.K.; Kedia, A.; Sinha, L.; Goswami, S.; Chakrabarti, T.; Chakrabarti, A. Data mining techniques in Indian healthcare: A short review. In Proceedings of the 2015 International Conference on Man and Machine Interfacing (MAMI), Bhubaneswar, India, 17–19 December 2015; pp. 1–7. [Google Scholar]
- Pandey, A.; Roy, N.; Bhawsar, R.; Mishra, R.M. Health Information System in India: Issues of data availability and quality. Demogr. India 2010, 39, 111–128. [Google Scholar]
- Patel, S.; Patel, H. Survey of Data Mining Techniques used in Healthcare Domain. Int. J. Inf. 2016, 6, 53–60. [Google Scholar] [CrossRef]
- Rojas, E.; Munoz-Gama, J.; Sepúlveda, M.; Capurro, D. Process mining in healthcare: A literature review. J. Biomed. Inform. 2016, 61, 224–236. [Google Scholar] [CrossRef]
- Tomar, D.; Agarwal, S. A survey on Data Mining approaches for Healthcare. Int. J. Bio-Sci. Bio-Technol. 2013, 5, 241–266. [Google Scholar] [CrossRef]
- Kalaiselvi, C. Diagnosing of heart diseases using average k-nearest neighbor algorithm of data mining. In Proceedings of the 2016 3rd International Conference on Computing for Sustainable Global Development (INDIACom), New Delhi, India, 16–18 March 2016; pp. 3099–3103. [Google Scholar]
- Kala, V.C.; Kiran, L.V.; Prasad, P.S. Prediction of diseases with pathological characteristics classification using data mining. In Proceedings of the 2019 International Conference on Vision Towards Emerging Trends in Communication and Networking (ViTECoN), Vellore, India, 30–31 March 2019; pp. 1–5. [Google Scholar]
- Chauhan, D.; Jaiswal, V. An efficient data mining classification approach for detecting lung cancer disease. In Proceedings of the 2016 International Conference on Communication and Electronics Systems (ICCES), Coimbatore, India, 21–22 October 2016; pp. 1–8. [Google Scholar]
- Khan, S.I.; Islam, A.; Hossen, A.; Zahangir, T.I.; Hoque, A.S.M.L. Supporting the Treatment of Mental Diseases using Data Mining. In Proceedings of the 2018 International Conference on Innovations in Science, Engineering and Technology (ICISET), Chittagong, Bangladesh, 27–28 October 2018; pp. 339–344. [Google Scholar]
- Alonso, S.G.; De La Torre-Díez, I.; Hamrioui, S.; López-Coronado, M.; Barreno, D.C.; Nozaleda, L.M.; Franco, M. Data Mining Algorithms and Techniques in Mental Health: A Systematic Review. J. Med. Syst. 2018, 42, 161. [Google Scholar] [CrossRef]
- Dubey, A.K.; Gupta, U.; Jain, S. Epidemiology of lung cancer and approaches for its prediction: A systematic review and analysis. Chin. J. Cancer 2016, 35, 71. [Google Scholar] [CrossRef]
- Swapna, K.; Babu, M.S.P. A Critical Study on Cluster Analysis Methods to Extract Liver Disease Patterns in Indian Liver Patient Data. Int. J. Comput. Intell. Res. 2017, 13, 2379–2390. [Google Scholar]
- Pasha, M.; Fatima, M. Comparative Analysis of Meta Learning Algorithms for Liver Disease Detection. J. Softw. 2017, 12, 923–933. [Google Scholar] [CrossRef]
- Abdar, M.; Zomorodi-Moghadam, M.; Das, R.; Ting, I.-H. Performance analysis of classification algorithms on early detection of liver disease. Expert Syst. Appl. 2017, 67, 239–251. [Google Scholar] [CrossRef]
- Wu, H.; Yang, S.; Huang, Z.; He, J.; Wang, X. Type 2 diabetes mellitus prediction model based on data mining. Inform. Med. Unlocked 2018, 10, 100–107. [Google Scholar] [CrossRef]
- Verma, L.; Srivastava, S.; Negi, P.C. A Hybrid Data Mining Model to Predict Coronary Artery Disease Cases Using Non-Invasive Clinical Data. J. Med. Syst. 2016, 40, 178. [Google Scholar] [CrossRef] [PubMed]
- Goswami, T.; Dabhi, V.K.; Prajapati, H.B. Skin Disease Classification from Image—A Survey. In Proceedings of the 2020 6th International Conference on Advanced Computing and Communication Systems (ICACCS), Coimbatore, India, 6–7 March 2020; pp. 599–605. [Google Scholar]
- Induja, S.; Raji, C. Computational Methods for Predicting Chronic Disease in Healthcare Communities. In Proceedings of the 2019 International Conference on Data Science and Communication (IconDSC), Bangalore, India, 1–2 March 2019; pp. 1–6. [Google Scholar]
- Jain, D.; Singh, V. Feature selection and classification systems for chronic disease prediction: A review. Egypt. Inform. J. 2018, 19, 179–189. [Google Scholar] [CrossRef]
- Chaurasia, V.; Pal, S. A novel approach for breast cancer detection using data mining techniques. Int. J. Innov. Res. Comput. Commun. Eng. 2017, 2. [Google Scholar]
- Kadam, K.; Kamat, P.V.; Malav, A.P. Cardiovascular Disease Prediction Using Data Mining Techniques: A Proposed Framework Using Big Data Approach. In Coronary and Cardiothoracic Critical Care: Breakthroughs in Research and Practice; IGI Global: Hershey, PA, USA, 2019; pp. 246–264. [Google Scholar]
- Miljkovic, D.; Aleksovski, D.; Podpečan, V.; Lavrač, N.; Malle, B.; Holzinger, A. Machine Learning and Data Mining Methods for Managing Parkinson’s disease. In Machine Learning for Health Informatics; Springer: Cham, Switzerland, 2016; pp. 209–220. [Google Scholar]
- Manogaran, G.; Lopez, D. A survey of big data architectures and machine learning algorithms in Healthcare. Int. J. Biomed. Eng. Technol. 2017, 25, 182–211. [Google Scholar] [CrossRef]
- Yu, K.-H.; Beam, A.L.; Kohane, I.S. Artificial intelligence in healthcare. Nat. Biomed. Eng. 2018, 2, 719–731. [Google Scholar] [CrossRef] [PubMed]
- Simonite, T. Google’s AI Eye Doctor Gets Ready to Go to Work in India. WIRED. Available online: https://www.wired.com/2017/06/googles-ai-eye-doctor-gets-ready-go-work-india/ (accessed on 18 June 2020).
- Waghade, S.S.; Karandikar, A.M. A comprehensive study of healthcare fraud detection based on machine learning. Int. J. Appl. Eng. Res. 2018, 13, 4175–4178. [Google Scholar]
- Baid, U.; Baheti, B.; Dutande, P.; Talbar, S. Detection of Pathological Myopia and Optic Disc Segmentation with Deep Convolutional Neural Networks. In Proceedings of the TENCON 2019-2019 IEEE Region 10 Conference (TENCON), Kochi, India, 17–20 October 2019; pp. 1345–1350. [Google Scholar]
- Mandal, T.; Rao, K.S. Glottal Closure Instants Detection From Pathological Acoustic Speech Signal Using Deep Learning. arXiv 2018, arXiv:1811.09956. [Google Scholar]
- Gupta, N.; Ahuja, N.; Malhotra, S.; Bala, A.; Kaur, G. Intelligent heart disease prediction in cloud environment through ensembling. Expert Syst. 2017, 34, e12207. [Google Scholar] [CrossRef]
- Abdar, M.; Yen, N.Y.; Hung, J.C.-S. Improving the Diagnosis of Liver Disease Using Multilayer Perceptron Neural Network and Boosted Decision Trees. J. Med. Biol. Eng. 2018, 38, 953–965. [Google Scholar] [CrossRef]
- Patnaik, S.K.; Sidhu, M.S.; Gehlot, Y.; Sharma, B.; Muthu, P. Automated Skin Disease Identification using Deep Learning Algorithm. Biomed. Pharmacol. J. 2018, 11, 1429–1437. [Google Scholar] [CrossRef]
- Kaur, H.; Kumari, V. Predictive modelling and analytics for diabetes using a machine learning approach. Appl. Comput. Inform. 2020. [Google Scholar] [CrossRef]
- Kumar, R.; Arora, R.; Bansal, V.; Sahayasheela, V.J.; Buckchash, H.; Imran, J.; Narayanan, N.; Pandian, G.N.; Raman, B. Accurate Prediction of COVID-19 using Chest X-Ray Images through Deep Feature Learning model with SMOTE and Machine Learning Classifiers. medRxiv 2020. [Google Scholar] [CrossRef]
- Kakileti, S.T.; Madhu, H.J.; Manjunath, G.; Wee, L.; Dekker, A.; Sampangi, S. Personalized risk prediction for breast cancer pre-screening using artificial intelligence and thermal radiomics. Artif. Intell. Med. 2020, 105, 101854. [Google Scholar] [CrossRef]
- Ko, I.; Chang, H. Interactive data visualization based on conventional statistical findings for antihypertensive prescriptions using National Health Insurance claims data. Int. J. Med. Inform. 2018, 116, 1–8. [Google Scholar] [CrossRef]
- Ledesma, A.; Bidargaddi, N.; Strobel, J.; Schrader, G.; Nieminen, H.; Korhonen, I.; Ermes, M. Health timeline: An insight-based study of a timeline visualization of clinical data. BMC Med. Inform. Decis. Mak. 2019, 19, 170. [Google Scholar] [CrossRef]
- Ulahannan, J.P.; Narayanan, N.; Thalhath, N.; Prabhakaran, P.; Chaliyeduth, S.; Suresh, S.P.; Mohammed, M.; Rajeevan, E.; Joseph, S.; Balakrishnan, A.; et al. A citizen science initiative for open data and visualization of COVID-19 outbreak in Kerala, India. J. Am. Med. Inform. Assoc. 2020, 27, 1913–1920. [Google Scholar] [CrossRef]
- Tandon, H.; Ranjan, P.; Chakraborty, T.; Suhag, V. Coronavirus (COVID-19): ARIMA based time-series analysis to forecast near future. arXiv 2020, arXiv:2004.07859. [Google Scholar]
- Gupta, S.; Raghuwanshi, G.S.; Chanda, A. Effect of weather on COVID-19 spread in the US: A prediction model for India in 2020. Sci. Total Environ. 2020, 728, 138860. [Google Scholar] [CrossRef]
- Basu, S.; Mitra, S.; Saha, N. Deep Learning for Screening COVID-19 using Chest X-Ray Images. In Proceedings of the 2020 IEEE Symposium Series on Computational Intelligence (SSCI), Canberra, ACT, Australia, 1–4 December 2020; pp. 2521–2527. [Google Scholar]
- Pasa, F.; Golkov, V.; Pfeiffer, F.; Cremers, D. Efficient Deep Network Architectures for Fast Chest X-Ray Tuberculosis Screening and Visualization. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef]
- Olshannikova, E.; Ometov, A.; Koucheryavy, Y.; Olsson, T. Visualizing Big Data with augmented and virtual reality: Challenges and research agenda. J. Big Data 2015, 2, 22. [Google Scholar] [CrossRef]
- Schuemie, M.J.; Van Der Straaten, P.; Krijn, M.; Van Der Mast, C.A. Research on Presence in Virtual Reality: A Survey. Cyberpsychol. Behav. 2001, 4, 183–201. [Google Scholar] [CrossRef] [PubMed]
- Prakaash, D.; Kodagahally, R.R.; Honnaiah, M. Virtual reality: A railroad for structural bioinformatics towards advanced cancer research. PeerJ Prepr. 2017, 5, e2960v1. [Google Scholar]
- Ayoub, A.; Pulijala, Y. The application of virtual reality and augmented reality in Oral & Maxillofacial Surgery. BMC Oral Health 2019, 19, 238. [Google Scholar] [CrossRef]
- Chamberlain, D.; Jimenez-Galindo, A.; Fletcher, R.R.; Kodgule, R. Applying Augmented Reality to Enable Automated and Low-Cost Data Capture from Medical Devices. In Proceedings of the Eighth International Conference on Information and Communication Technologies and Development; ACM: New York, NY, USA, 2016; pp. 1–4. [Google Scholar]
- Bhatti, R.; Grandison, T. Towards Improved Privacy Policy Coverage in Healthcare Using Policy Refinement. In Workshop on Secure Data Management; Springer: Berlin/Heidelberg, Germany, 2007; pp. 158–173. [Google Scholar]
- Parker, R.B. A definition of privacy. Rutgers L. Rev. 1973, 27, 275. [Google Scholar]
- Mireku, K.K.; Zhang, F.; Komlan, G.; Kingsford, K.M.; FengLi, Z. Patient knowledge and data privacy in healthcare records system. In Proceedings of the 2017 2nd International Conference on Communication Systems, Computing and IT Applications (CSCITA), Mumbai, India, 7–April 2017; pp. 154–159. [Google Scholar]
- Cheng, V.S.; Hung, P.C. Health Insurance Portability and Accountability Act (HIPPA) Compliant access control model for web services. Int. J. Healthc. Inf. Syst. Inform. 2006, 1, 22–39. [Google Scholar] [CrossRef]
- Cho, S. A Study on Privacy Protection in the EU’s GDPR and Korea’s Personal Information Protection Act. Law J. 2018, 61, 117–148. [Google Scholar]
- Akpojivi, U. Rethinking information privacy in a “connected” world. In Censorship, Surveillance, and Privacy: Concepts, Methodologies, Tools, and Applications; IGI Global: Hershey, PA, USA, 2019; pp. 1–18. [Google Scholar]
- Churi, P.P.; Pawar, A.V. A Systematic Review on Privacy Preserving Data Publishing Techniques. J. Eng. Sci. Technol. Rev. 2019, 12, 17–25. [Google Scholar] [CrossRef]
- Srinivas, N.; Biswas, A. Protecting patient information in India: Data privacy law and its challenges. NUJS L. Rev. 2012, 5, 411. [Google Scholar]
- Jalali, M.S.; Landman, A.; Gordon, W.J. Telemedicine, privacy, and information security in the age of COVID-19. J. Am. Med. Inform. Assoc. 2021, 28, 671–672. [Google Scholar] [CrossRef]
- Kagalwalla, N.; Garg, T.; Churi, P.; Pawar, A. A survey on implementing Privacy in Healthcare: An indian perspective. Int. J. Adv. Trends Comput. Sci. Eng. 2019, 8, 963–982. [Google Scholar] [CrossRef]
- Meingast, M.; Roosta, T.; Sastry, S. Security and privacy issues with health care information technology. In Proceedings of the 2006 International Conference of the IEEE Engineering in Medicine and Biology Society, New York, NY, USA, 30 August–3 September 2006; pp. 5453–5458. [Google Scholar]
- Mishra, N.N.; Parker, L.S.; Nimgaonkar, V.L.; Deshpande, S.N. Privacy and the Right to Information Act, 2005. Indian J. Med. Ethics 2008, 5, 158–161. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Berger, D. Corruption ruins the doctor-patient relationship in India. BMJ 2014, 348, g3169. [Google Scholar] [CrossRef] [PubMed]
- Ion, I.; Sachdeva, N.; Kumaraguru, P.; Čapkun, S. Home is safer than the cloud! Privacy concerns for consumer cloud storage. In Proceedings of the Seventh Symposium on Usable Privacy and Security; 2011; pp. 1–20. [Google Scholar] [CrossRef]
- Priya, R.; Sivasankaran, S.; Ravisasthiri, P.; Sivachandiran, S. A survey on security attacks in electronic healthcare systems. In Proceedings of the 2017 International Conference on Communication and Signal Processing (ICCSP), Chennai, India, 6–8 April 2017; pp. 0691–0694. [Google Scholar]
- Kumar, P.R.; Raj, P.H.; Jelciana, P. Exploring Data Security Issues and Solutions in Cloud Computing. Procedia Comput. Sci. 2018, 125, 691–697. [Google Scholar] [CrossRef]
- Carol, Y.; Cheung, Y. Data without borders. Lancet 2019, 393, 1331–1384. [Google Scholar]
- Bartoletti, I. AI in Healthcare: Ethical and Privacy Challenges. In Conference on Artificial Intelligence in Medicine in Europe; Springer: Cham, Switzerland, 2019; pp. 7–10. [Google Scholar]
- Bhattacharya, P.; Tanwar, S.; Bodke, U.; Tyagi, S.; Kumar, N. BinDaaS: Blockchain-Based Deep-Learning as-a-Service in Healthcare 4.0 Applications. IEEE Trans. Netw. Sci. Eng. 2019, 1. [Google Scholar] [CrossRef]
- Hathaliya, J.J.; Tanwar, S.; Tyagi, S.; Kumar, N. Securing electronics healthcare records in Healthcare 4.0: A biometric-based approach. Comput. Electr. Eng. 2019, 76, 398–410. [Google Scholar] [CrossRef]
- Kumari, A.; Tanwar, S.; Tyagi, S.; Kumar, N. Fog computing for Healthcare 4.0 environment: Opportunities and challenges. Comput. Electr. Eng. 2018, 72, 1–13. [Google Scholar] [CrossRef]
- Vora, J.; Nayyar, A.; Tanwar, S.; Tyagi, S.; Kumar, N.; Obaidat, M.S.; Rodrigues, J.J.P.C. BHEEM: A Blockchain-Based Framework for Securing Electronic Health Records. In Proceedings of the 2018 IEEE Globecom Workshops (GC Wkshps), Abu Dhabi, United Arab Emirates, 9–13 December 2018; pp. 1–6. [Google Scholar]
- Vora, J.; Tanwar, S.; Tyagi, S.; Kumar, N.; Rodrigues, J.J.P.C. FAAL: Fog computing-based patient monitoring system for ambient assisted living. In Proceedings of the 2017 IEEE 19th International Conference on e-Health Networking, Applications and Services (Healthcom), Dalian, China, 12–15 October 2017; pp. 1–6. [Google Scholar]
- Vora, J.; Tanwar, S.; Tyagi, S.; Kumar, N.; Rodrigues, J.J.P.C. Home-based exercise system for patients using IoT enabled smart speaker. In Proceedings of the 2017 IEEE 19th International Conference on e-Health Networking, Applications and Services (Healthcom), Dalian, China, 12–15 October 2017; pp. 1–6. [Google Scholar]
- Hathaliya, J.J.; Tanwar, S. An exhaustive survey on security and privacy issues in Healthcare 4. Comput. Commun. 2020, 153, 311–335. [Google Scholar] [CrossRef]
- Hathaliya, J.J.; Tanwar, S.; Evans, R. Securing electronic healthcare records: A mobile-based biometric authentication approach. J. Inf. Secur. Appl. 2020, 53, 102528. [Google Scholar] [CrossRef]
- Madhisetty, S.; Williams, M.-A. Managing Privacy Through Key Performance Indicators When Photos and Videos Are Shared via Social Media. In Science and Information Conference; Springer: Cham, Switzerland, 2018; pp. 1103–1117. [Google Scholar]
- Singh, R.G.; Ruj, S. A Technical Look at the Indian Personal Data Protection Bill. arXiv 2020, arXiv:2005.13812. [Google Scholar]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Sub-Category | Description and Indicators | The Public Sector in India | The Private Sector in India |
|---|---|---|---|---|
| Access and response | Availability | 24 × seven healthcare service availability to people without any hesitation | Moderate | Good |
| Timeliness of service | Less waiting time to initial screening and subsequent testing, providing results, and follow-up | Moderate | Excellent | |
| Hospitality | Highly responsive feedback system, facility, and maintenance of healthcare system | Moderate | Good | |
| Quality | The comprehensiveness of healthcare services | Availability of all the components of WHO service packages | Poor | Good |
| Diagnostic | Accurate diagnosis of retrospective review | Moderate | Excellent | |
| Management standards | Rate of conformity to international disease-specific management standards | Poor | Good | |
| Client retention | Rate of failure to follow-up or rate of appropriate patient return | Moderate | Moderate | |
| Outcomes | Treatment success rates | Rate of therapy success, controlling of population characteristics, and delayed presentation | Moderate | Good |
| Population coverage | The proportion of the catchment population reached through dedicated campaigns (e.g., vaccination rates) | Excellent | Moderate | |
| Morbidity | Rate of disability to patients and controlling of population characteristics | Moderate | Less | |
| Mortality | Rate of patient death and controlling of population characteristics | Moderate | Less | |
| Accountability, transparency, and regulation. | Data accessibility and quality | Availability of data and appropriate use of indicators and statistics | Poor | Good |
| Public health functions | Contribution of healthcare systems to core public health system functions (e.g., reporting of critical diseases and preventative care) | Good | Good | |
| Reform capacity | Results of quality improvement initiatives | Poor | Good | |
| Fairness and equity | Financial barriers to care | User fees, bribes, and pharmaceutical costs | Very less | High |
| Distributive justice | Healthcare availability commensurate with requirements | Moderate | Good | |
| Efficiency | Cost | Absolute dollars spent for a given indication | Very less | High |
| Redundancy | Repetition of diagnostic time, testing, supply chains, and therapy delivery | Moderate | Good | |
| Fragmentation | Separation of core healthcare system functions and generating sluggish management | Poor | Poor | |
| Delays | The time between the ordering of tests or therapies and their execution | Poor | Good |
| India | China | Sri Lanka | Indonesia | Egypt | Philippines | |
|---|---|---|---|---|---|---|
| Total health expenditures as % GDP | 4.0% | 5.5% | 4% | 3% | 5% | 4% |
| Fiscal health expenditures as % GDP | 0.9% | 3.2% | 2% | 1% | 1% | 1.3% |
| Per-capita health expenditures (PPP) | 239 | 761 | 491 | 363 | 516 | 342 |
| Level of out-of-pocket (% Total health expenditures) | 64% | 36% | 50% | 60% | 62% | 54% |
| Neo-natal mortality 1980 | 60 | 65 | 24 | 41 | 53 | 27 |
| Neo-natal mortality 2016 | 25 | 5 | 7 | 13 | 12 | 13 |
| Global healthcare rank | 145 | 92 | 71 | 138 | 111 | 124 |
| The burden of disease (DALYs per 100,000 population) | 34,000 | 26,300 | 24,000 | 28,900 | 28,000 | 31,000 |
| Trends | Description | Privacy Implications |
|---|---|---|
| Community disease to personal- and lifestyle-related diseases | Due to urbanization and technology use in our daily lives, specific lifestyle-related diseases have led to community diseases. These diseases include cholesterol, blood pressure, diabetes, liver problems caused by overconsumption of products such as alcohol. This trend requires customized medicines and treatment with personal health and self-care. | In general, diseases are less harmful and can be treated by a local doctor or healthcare professionals. The record of such diseases and treatment is stored by individual hospitals in digital form. Local hospitals are not trustworthy enough to store such sensitive information, and hence it may invite data breaching issues due to insecure storage of EHR [20,21,22]. |
| Healthcare expansion to Indian cities | The privatization of Healthcare by the government helped expand Healthcare to tier II and III cities. Hospitals are also built-in villages and rural areas to provide Healthcare to middle and lower-class people. The government is reducing taxes for the first five years for such businesses to encourage healthcare expansion in the private sector. | Hospitals built in rural areas mostly use paper-based prescription records; using these records lacks electricity and the Internet to run digital equipment. Paper-based records can be easily stolen and are most vulnerable to stealing personal information than digitally stored information. |
| Telemedicine | Many healthcare startups such as Apollo and AIIMS are adopting telemedicine services. Telemedicine can bridge the rural-urban gap to provide medical facilities, low-cost consultation, and diagnosis facilities to the remotest of areas through the high-speed Internet and telecommunication. | Research says that protection against privacy concerns is more in telemedicine, Which requires a multi-disciplinary and multi-stakeholder approach. Most of the employees working in the telemedicine industry are either very busy with workload or are less trained about security and privacy violations. This invites data breaching attacks, phishing attacks, unauthorized access, and so on [23]. |
| AI in Healthcare | The adoption and use of AI-based healthcare applications are rapidly growing. AI helps solve the problems of patients, doctors, hospitals, and the overall healthcare industry. | AI ensures that the disease prediction is way faster than an actual spread of disease due to prediction technology. However, with the massive use of data for training purpose (which contains sensitive data), privacy issues of identifying individual rises [24]. |
| Home healthcare [24] | Home healthcare provides Healthcare at affordable prices at patients’ homes. It saves the traveling costs of doctors/patients, and treatment is provided with minimum logistic interventions. | - |
| Growth of health insurance | Health insurance is gaining momentum in India. The trust of people in India in health insurance and the assurance by health insurance has increased in past years. Many companies such as Aditya Birla and LIC provide health insurance to people. | There are massive amounts of data generated in the health insurance and needs to be protected. The sensitive information such as personal details, disease details, past health history is being recorded and shared with the third party by insurance companies without individual consent. Most of the data shared with the third party are non-anonymous; it is straightforward to predict the identity of individual human beings. |
| Mobile-based health delivery | The mobile solid technology infrastructure and the launch of 4G can drive mobile-based health initiatives in the country. It enables fast health-related services with reduced costs and superior reach [21,22]. | - |
| Technology for health | Technological intervention is increasing in India. According to [21], India’s medical technology sector can reach US $9.60 billion by 2022. Various advent technologies are used in the healthcare domain, such as machine learning algorithms for prediction of specific health parameters/data/diseases/behavior and the Internet of things-based healthcare systems [22] | - |
| Luxurious living and health | Luxurious services, including pick and drop facilities, doctor visits at homes, online prescriptions, have become a part of the Indian healthcare industry. | - |
| Health Care Providers | Statistics | Description |
|---|---|---|
| Apollo Hospitals | 9844 beds 70 hospitals 8500+ doctors Total income was Rs 9648.88 crore (US $1.38 billion) in FY 19 and Rs 8347.39 crore (US $1.19 billion) during 20 | Apollo healthcare has hospitals and pharmacies across India. Moreover, the company provides project consultancy services, health insurance services, education and training programs, and research services. It also operates birthing centers, day surgery centers, and dental clinics. |
| Thyrocare Technologies Limited | Over 1200 employees 571 cities Consolidated total income of Rs 412.86 crore (US $59.07 million) in FY 19 and Rs 337.43 crore (US $48.28 million) in 9 MFY 20 | Thyrocare is the first completely automated diagnostics laboratory. The company offers cancer and HIV diagnostics centers, chemotherapy, and dialysis centers across India. |
| Fortis Healthcare | 36 healthcare facilities Approximately 9000 beds 415 diagnostic centers Total consolidated revenue of Rs 4469.35 crore (US $639.48 million) in FY 19 and Rs 2379.79 crore (US $340.51 million) in H1FY 20. | Fortis healthcare is considered an integrated healthcare delivery service provider in India. Fortis memorial research institute (FMRI) ranked second in a study of 30 most technologically advanced hospitals in the world conducted by topmastersinhealthcare.com. 19 August 2020 |
| Net meds | 14 logistic centers across the country 24 × seven online portal and mobile application Three million downloads (till 2018) with more than $512 million profit; it is projected to earn $3.645 billion by 2022. | Netmeds is an online platform for the pharmacy industry. It offers significant pharmacy products through online shipments. It is also called “India ki pharmacy.” The mobile application is well-equipped with voice chats, e-mailing services, and 24 × seven customer care services. |
| Practo | Free services for doctors and patients Focused website and 1 lac doctor profiles in India | Practo is the world’s leading healthcare platform and works as an independent medical portal, connecting doctors and hospitals across India and the globe. Although the reach of Practo is global, it was founded in 2008 in Bangalore. Practo provides its users with diagnostic search features on its web-based platform through high-quality photographs and filter options. Practo is suitable for private doctors who independently run hospitals in rural and urban areas. |
| Type | Description | Examples | Clinical Data | Exogenous Data | Genetic Data |
|---|---|---|---|---|---|
| Structured | The data arranged in a structured format are considered structured data. Such data are primarily arranged in rows and columns. The structured data are mostly easy for analysis but have considerable sensitive information and direct identifiers. | Blood reports, sugar reports, billing information of patients, and Indian census information. Primarily clinical data can be categorized as structured data. | Yes | No | Yes |
| Semi-structured | The data that is minimally structured and requires scripts for extraction ate classified as semi-structured data. Such data are generally captured from wearable devices, which monitor a person’s response to particular medicine and activity. | XML-, JSON-extracted reports are considered semi-structured. The exogenous data are generally considered semi-structured data. | No | Yes | Yes |
| Unstructured | The data with no uniform format or structure are classified as unstructured data. Human written prescriptions and reports are considered unstructured data. | The doctor’s written prescription on a notepad, images, videos, or time series reports is considered unstructured. | Yes | Yes | Yes |
| Data type | Direct/ Indirect | Description | Strengths | Limitations |
|---|---|---|---|---|
| Population census | Indirect | Population census is about storing information on the population of India. The vast database comprises social, geographical, and demographic information of people collected every ten years. | It covers small information for people across India. In terms of analysis, the data are most helpful with proper predictions of literacy rates, social-cultural activities, and food consumption habits. | Population census is conducted every ten years by the government of India. The health-related information is considerably low. Providing health analytics on census datasets is challenging. |
| Civil registration system | Indirect | The count and details of the population are obtained in certain situations, such as the birth and death of a person and from lost and found records. | Primarily the data related to time and location are recorded. | Death-related information is documented correctly. For example, minor details such as the cause of death (crime, health issue, and aging), city information, the place of death (can be different from the place of living) are not correctly stored, and hence the data are not productive for analysis. Inadequate information or columns are generally filled by some random values, which cause wrong/improper prediction of specific facts. |
| Public surveys | Direct | The data generated by companies, work organizations, health insurance companies, and third parties are considered the survey data. | The data are primarily structured for a particular party collecting data. The data are collected through digital mediums, including online forms, SAP systems, web portals, and social media. | The irregular and impure data are obtained most of the time. Mostly, the data are not accurate because not all people provide correct information. The data quality is low. The data remain moderately analytical. |
| Service records | Direct | The data captured directly from people about their health, work, and other demographic aspect. Work organizations generally capture the data, and data use is limited to organization scopes and limits. The organization must acquire consent from its employees for sharing, using, and publishing such data on a public platform or with a third-party service provider. | This is exclusively used for service management. The data quality is excellent and reliable. The data can be captured in limited time intervals of months or days (depending on data captured). | Mainly, data duplication and inconsistency problems arise because the data are not always at the centralized place. |
| Administrative records | Direct | It contains information regarding family details, financial planning, personality, and emotional details. | The data are captured as a single data source and generally are in a suitable quality format. These data are highly analytical but are generally substantially private. | The privacy problems and data breaching probability are maximum. The data require uniform and secure policies to access, use, share and publish. |
| Types of Disease | Type of Data | Data Mining Technique | References |
|---|---|---|---|
| Data Mining of Indian Health Data | |||
| Conventional pathology data | Structured | Support vector machine classification | [32,33,34] |
| Heart disease | Structured and unstructured | Naïve Bayes, decision tree, and K-nearest neighbor | [35] |
| Lymphoma disease and lung cancer | Unstructured (image dataset) | Support vector machine | [36,37] |
| Psychiatric diseases | Structured and semi-structured | Random forest, support vector machine (SVM), K-nearest neighbor | [38,39] |
| Liver diseases | Structured | k-means (KM) clustering algorithm, agglomerative nesting (AGNES), clustering algorithm, density-based spatial clustering of applications with a noise clustering algorithm, ordering points to identify the clustering structure, clustering algorithm, and exception maximization clustering algorithm | [40,41,42] |
| Skin disease | No paper found on the Indian dataset | [43] | |
| Diabetes | Structured | Improved K-means algorithm and logistic regression | [44] |
| Chest disease | Unstructured (image dataset) | Risk factor identification through correlation-based feature subset selection with particle swarm optimization search method and K-means clustering algorithms. Supervised learning algorithms such as multilayer perceptron, multinomial logistic regression, fuzzy unordered rule induction algorithm, and C4.5 classification algorithm | [45] |
| Chronic disease | Structured | Naïve Bayes, K-nearest neighbor, and decision tree | [46,47] |
| Breast cancer | No paper found on the Indian dataset | [48] | |
| Cardiovascular diseases | No paper found on the Indian dataset | [49] | |
| Parkinson disease | No paper found on the Indian dataset | [50] | |
| AI/machine learning/deep learning in the Indian health data | |||
| Conventional pathology data | Unstructured (image data) | Convolutional neural network on pathological myopia disease for vision blindness. Classification-based glottal closure instants detection from pathological acoustic speech signals | [51,52,53,54,55,56] |
| Heart disease | Structured | Naïve Bayes. Decision tree and random forest | [57] |
| Lymphoma disease and lung cancer | No paper found on the Indian dataset | ||
| Psychiatric diseases | No paper was found on the Indian dataset. | ||
| Liver diseases | Structured | Multilayer perceptron neural network algorithm based on various decision trees algorithms such as See5 (C5.0), chi-square automatic interaction detector, and classification and regression tree with boosting technique | [58] |
| Skin disease | Unstructured (image dataset) | Deep learning algorithms: (inception_ v3, MobileNet, resnet, exception | [59] |
| Diabetes | Structured | Linear kernel SVM, radial basis function kernel SVM, k-nearest neighbor, artificial neural network, and multifactor dimensionality reduction | [60] |
| Chest disease | Unstructured (image dataset) | Random forest | [61] |
| Chronic disease | No paper found on the Indian dataset | ||
| Breast cancer | Unstructured | Thermolytic risk score framework | [62,63,64] |
| Cardiovascular diseases | No paper found on the Indian dataset | - | |
| Parkinson disease | No paper was found on the Indian dataset. | - | |
| Data visualization of the Indian health data | |||
| Covid 19 dataset (open research dataset of India) | Structured | - | [65,66,67] |
| Covid 19 dataset (open research dataset of India) | Unstructured (X-ray image dataset) | - | [68,69,70] |
| Tuberculosis screening | Unstructured (X-ray image dataset) | - | [71,72,73] |
| Augmented and virtual reality in Indian Healthcare | |||
| Automated data capturing from medical devices | Unstructured | - | [74] |
| Cyber Attacks on Data Gathering Phase | Cyber Attacks at Network Phase | Cyber Attacks at Storage Phase |
|---|---|---|
| Phishing attack | Eavesdropping of health record | Cross-site scripting attack |
| Log access attack | Man-in-the-middle attack | Weak authentication attack |
| Social engineering attack | Data tampering | SQL injection attack. |
| Brute force attack (on passwords) | Denial of the service attack | |
| Data interception | ||
| Spoofing and sniffing attack |
| Type of Healthcare | Privacy Issues Stated in the Indian Healthcare System. | ||||||
|---|---|---|---|---|---|---|---|
| Type of Sector | Lack of Technology | Doctor-Patient Relationship | Data Storage and Management | Cyberattacks | Data Sharing | Trust in the Third Party | |
| Super specialty hospital | Public | Very good | Trustworthy | Very good | Minimal risk | Drafted Policies for consent | Strict |
| Medical institutes/colleges | Public | Adequate | Trustworthy | Good | Minimal risk | With good consent | Easy |
| District and taluka hospitals | Public | Adequate | Bit trustworthy | Adequate | High risk | Minimal consent | Easy |
| Primary healthcare centers | Public | Poor | Bit trustworthy | Poor | High risk | Without consent | Easy |
| Village hospitals | Public | Poor | Not trustworthy | Poor | High risk | Without consent | Easy |
| Super and multispecialty hospitals | Private | Excellent | Most Trustworthy | Very good | Minimal risk | Drafted Policies for consent | Strict |
| Tier II and III city hospitals | Private | Very good | Most Trustworthy | Very good | Minimal risk | Drafted Policies for consent | Strict |
| Private clinics | Private | Very good | Trustworthy | Very good | Minimal risk | Drafted Policies for consent | Strict |
| Non-profit organizations | Private | good | Trustworthy | Very good | Minimal risk | Minimal consent | Strict |
| Pharmaceutical industry | Private | Excellent | - | Very good | Minimal risk | Drafted Policies for consent | Strict |
| Health insurance company | Private | Excellent | - | Excellent | Minimal risk | Drafted Policies for consent | Strict |
| Private organizations | Private | Excellent | - | Excellent | Minimal risk | Minimal Consent | Easy |
| Type of Healthcare | Privacy Issues Stated in the Indian Healthcare System. | |||||||
|---|---|---|---|---|---|---|---|---|
| Type | Infrastructure | Privacy Policies | Data Breaching | Hacking | Accountability | Cultural Interventions | Cost | |
| Super specialty hospital | Public | Excellent | Well defined and followed | Less probability | Less probability | Yes | No | Average |
| Medical institutes/colleges | Public | Adequate | Well defined and followed | Adequate probability | Adequate probability | Yes | No | Low |
| District and taluka hospitals | Public | Poor | Well defined but not followed | High probability | High probability | No | Yes | considerably low/no cost |
| Primary healthcare centers | Public | Considerably poor | Well defined but not followed | High probability | High probability | No | Yes | considerably low/no cost |
| Village hospitals | Public | Considerably poor | Not defined | High probability | High probability | No | Yes | No cost |
| Super and multispecialty hospitals | Private | Excellent | Well defined and followed | Less probability | Less probability | Yes | No | Very high |
| Tier II and III city hospitals | Private | Excellent | Well defined and followed | Less probability | Less probability | Yes | No | High/considerably high |
| Private clinics | Private | Excellent | Well defined and followed | Less probability | Less probability | Yes | No | High |
| Non-profit organizations | Private | Excellent | Well defined and followed | Less probability | Less probability | Yes | No | Low |
| Pharmaceutical industry | Private | Excellent | Well defined and followed | Less probability | Less probability | Yes | No | NA |
| Health insurance company | Private | Excellent | Well defined and followed | Less probability | Less probability | Yes | No | NA |
| Private organizations | Private | Excellent | Well defined and followed | Less probability | Less probability | Yes | No | NA |
| KPI | Doctors and Healthcare Professionals/Practitioners | Hospital Administrative Staff | Researchers and Scientist | Academicians in the Computer Science Field | Mean | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Samples | DH1 | DH2 | DH3 | DH4 | DH5 | HA1 | HA2 | HA3 | HA4 | HA5 | RS1 | RS2 | RS3 | RS4 | RS5 | AC1 | AC2 | AC3 | AC4 | AC5 | |
| Forced Trust Vs. Control | 1 | 2 | 2 | 3 | 3 | 2 | 2 | 2 | 2 | 4 | 1 | 1 | 1 | 2 | 1 | 2 | 2 | 1 | 1 | 2 | 1.85 |
| Content Viewed by Whom | 3 | 3 | 4 | 2 | 1 | 3 | 2 | 4 | 1 | 2 | 1 | 1 | 1 | 1 | 1 | 2 | 1 | 3 | 1 | 2 | 1.95 |
| Tacit Knowledge | 3 | 3 | 3 | 4 | 2 | 2 | 2 | 2 | 3 | 1 | 1 | 1 | 1 | 3 | 2 | 2 | 3 | 2 | 3 | 1 | 2.2 |
| Laws and Regulation | 1 | 1 | 2 | 1 | 2 | 1 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 2 | 1 | 3 | 1 | 1 | 3 | 1.4 |
| Use of new Data Protection Technologies | 3 | 3 | 3 | 3 | 1 | 3 | 2 | 2 | 3 | 4 | 2 | 2 | 2 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 2 |
| Researcher’s Satisfaction | 4 | 4 | 4 | 4 | 2 | 5 | 5 | 4 | 4 | 4 | 2 | 2 | 2 | 3 | 1 | 1 | 1 | 1 | 1 | 2 | 2.8 |
| Industry-academia collaboration exists for privacy preservation mechanisms | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 2 | 2 | 2 | 1 | 1 | 1 | 2 | 1 | 2 | 2 | 2.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Churi, P.; Pawar, A.; Moreno-Guerrero, A.-J. A Comprehensive Survey on Data Utility and Privacy: Taking Indian Healthcare System as a Potential Case Study. Inventions 2021, 6, 45. https://doi.org/10.3390/inventions6030045
Churi P, Pawar A, Moreno-Guerrero A-J. A Comprehensive Survey on Data Utility and Privacy: Taking Indian Healthcare System as a Potential Case Study. Inventions. 2021; 6(3):45. https://doi.org/10.3390/inventions6030045
Chicago/Turabian StyleChuri, Prathamesh, Ambika Pawar, and Antonio-José Moreno-Guerrero. 2021. "A Comprehensive Survey on Data Utility and Privacy: Taking Indian Healthcare System as a Potential Case Study" Inventions 6, no. 3: 45. https://doi.org/10.3390/inventions6030045
APA StyleChuri, P., Pawar, A., & Moreno-Guerrero, A.-J. (2021). A Comprehensive Survey on Data Utility and Privacy: Taking Indian Healthcare System as a Potential Case Study. Inventions, 6(3), 45. https://doi.org/10.3390/inventions6030045